Skin Care [1 ed.] 9781622570317, 9781612095684
This new book presents topical research in the study of skin care, including healthy infant skin and proper cleansing; n
176 14 5MB
English Pages 186 Year 2011
Polecaj historie


![Wound Care and Skin Infections - 2023 [19 ed.]](https://dokumen.pub/img/200x200/wound-care-and-skin-infections-2023-19nbsped.jpg)






![Skin Care [1 ed.]
9781622570317, 9781612095684](https://dokumen.pub/img/200x200/skin-care-1nbsped-9781622570317-9781612095684.jpg)
Citation preview
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved. Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved. Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
DERMATOLOGY - LABORATORY AND CLINICAL RESEARCH
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
SKIN CARE
No part of this digital document may be reproduced, stored in a retrieval system or transmitted in any form or by any means. The publisher has taken reasonable care in the preparation of this digital document, but makes no expressed or implied warranty of any kind and assumes no responsibility for any errors or omissions. No liability is assumed for incidental or consequential damages in connection with or arising out of information contained herein. This digital document is sold with the clear understanding that the publisher is not engaged in rendering legal, medical or any other professional services. Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
DERMATOLOGY - LABORATORY AND CLINICAL RESEARCH Additional books in this series can be found on Nova’s website under the Series tab.
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Additional E-books in this series can be found on Nova’s website under the E-books tab.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
DERMATOLOGY - LABORATORY AND CLINICAL RESEARCH
SKIN CARE
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
SANDRA M. HAYES EDITOR
Nova Biomedical Books New York Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011 by Nova Science Publishers, Inc. All rights reserved. No part of this book may be reproduced, stored in a retrieval system or transmitted in any form or by any means: electronic, electrostatic, magnetic, tape, mechanical photocopying, recording or otherwise without the written permission of the Publisher. For permission to use material from this book please contact us: Telephone 631-231-7269; Fax 631-231-8175 Web Site: http://www.novapublishers.com NOTICE TO THE READER The Publisher has taken reasonable care in the preparation of this book, but makes no expressed or implied warranty of any kind and assumes no responsibility for any errors or omissions. No liability is assumed for incidental or consequential damages in connection with or arising out of information contained in this book. The Publisher shall not be liable for any special, consequential, or exemplary damages resulting, in whole or in part, from the readers’ use of, or reliance upon, this material. Any parts of this book based on government reports are so indicated and copyright is claimed for those parts to the extent applicable to compilations of such works.
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Independent verification should be sought for any data, advice or recommendations contained in this book. In addition, no responsibility is assumed by the publisher for any injury and/or damage to persons or property arising from any methods, products, instructions, ideas or otherwise contained in this publication. This publication is designed to provide accurate and authoritative information with regard to the subject matter covered herein. It is sold with the clear understanding that the Publisher is not engaged in rendering legal or any other professional services. If legal or any other expert assistance is required, the services of a competent person should be sought. FROM A DECLARATION OF PARTICIPANTS JOINTLY ADOPTED BY A COMMITTEE OF THE AMERICAN BAR ASSOCIATION AND A COMMITTEE OF PUBLISHERS. Additional color graphics may be available in the e-book version of this book. Library of Congress Cataloging-in-Publication Data Skin care / editor, Sandra M. Hayes. p. ; cm. Includes bibliographical references and index. ISBN 978-1-62257-031-7 (E-Book) 1. Skin--Care and hygiene. 2. Skin--Diseases--Treatment. I. Hayes, Sandra M. [DNLM: 1. Skin Care. 2. Skin Diseases--therapy. WR 650] RL87.S555 2011 616.5--dc23 2011024895
Published by Nova Science Publishers, Inc. † New York
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Contents vii
Preface
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Chapter I
Keeping Infant Skin Healthy through Proper Cleansing Georgios N. Stamatas, Russel M. Walters and Lorena S. Telofski
1
Chapter II
Novel Approaches for Wound Repair Therapies Gerd G. Gauglitz and Marc G. Jeschke
31
Chapter III
Skin Care: Chronic Ulcer Management P. C. Leung
59
Chapter IV
The Role of Nonprescription Topical Treatment on the Skin Diana Badiu,, Rafael Luque and Dănuţ Dincă
79
Current Preventive Strategies to Reduce Surgical Site Infections by the Endogenous Flora Pascal M. Dohmen
99
Chapter V
Chapter VI
Recent Innovations in Topical Skin Care Patrick C. Angelos and Stephen M. Weber
117
Chapter VII
Acne Vulgaris and Adolescence Donald E. Greydanus and Dilip R. Patel
133
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
vi Chapter VIII
Contents Keloids and Hypertrophic Scars after Surgery in Cancer Patients D. Franck, A. De Mey and W. D. Boeckx
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Index
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
147 159
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Preface This new book presents topical research in the study of skin care, including healthy infant skin and proper cleansing; novel technologies for improving wound healing capacities; chronic ulcer management; nonprescription topical treatment of the skin; strategies to reduce surgical site infections by endogenous flora; acne vulgaris in adolescence and keloids and hypertrophic scars after surgery in cancer patients. Chapter 1 – Keeping the skin clean is essential to the overall good health of an individual. This statement is even more relevant in the case of infants, since infant skin structure, function, and composition are still developing, underscoring the need for special care. Skin cleansing essentially means removing unwanted substances, including irritants from sources such as saliva, nasal secretions, urine, feces, and dirt. These irritants include salts, lipolytic and proteolytic enzymes, infectious microbial species, as well as potential allergens. Keeping the diaper area clean helps prevent skin barrier breakdown and therefore rash (diaper dermatitis) and infection (candidiasis). Keeping hands clean, particularly in the case of babies with their hand-to-mouth behaviors, can help reduce or prevent oral transmission of microbial contaminants. Special attention should also be paid to the facial area, where vulnerable skin can be irritated by milk, saliva, and nasal mucosa, all of which have higher pH relative to skin which can be detrimental to skin barrier. Similarly skin folds and creases (prominent in infant skin) should be kept clean. Proper formulation of personal care products intended for use on infants and young children is essential and should take into account the unique properties of infant skin as well as infant behaviors. Proper cleansing products should therefore be mild to both infant skin and eyes. Although the need for and benefits of good skin hygiene are clear, optimal cleansing and bathing practices still remain debated, from the baby’s first bath through infancy and
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
viii
Preface
early childhood. In spite of this debate, evidence-based practice guidelines should form the basis of proper cleansing approaches. Chapter 2 – Treatment of non-healing wounds has remained difficult, in spite of better understanding of pathophysiologic principles. Gene therapy, initially developed for treatment of congenital defects, represents a novel option for enhancing wound repair. In order to accelerate wound closure, genes encoding for growth factors or cytokines have showed most potential. The majority of gene delivery systems are based on viral transfection, naked DNA application, high pressure injection, and liposomal vectors. Besides advances stemming from breakthroughs in recombinant growth factors and bioengineered skin, early data suggest the use of multipotent stem cells in order to accelerate wound healing. Cutaneous wound healing requires a wellorchestrated integration of the complex biological and molecular events of cell migration and proliferation, as well as extracellular matrix deposition, angiogenesis, and remodeling. Stem cells, due to their ability to differentiate into various tissue types by asymmetric replication thus represent a promising tissue repair strategy. A variety of sources, such as bone marrow, peripheral blood, umbilical cord blood, adipose tissue and skin/ hair follicles, have been utilized to isolate stem cells to modulate the healing response of acute and chronic wounds. Recent data have demonstrated the feasibility of autologous ASC therapy in cutaneous repair and regeneration. Very recently, the combination of gene and stem cell therapy has emerged and could provide a promising approach for future treatment of chronic and acute wounds. The aim of this review is to discuss the use and the potential of these novel technologies in order to improve wound healing capacities. Chapter 3 – Chronic ulcers are related to vascular, neurological or metabolic problems that either initiate the formation of the ulcers themselves or prevent the usual healing processes. With the aging population, chronic ulcers occur in larger numbers of population in the first place, and give the elderlies disabling disturbances in a lot of circumstances. Chronic ulcers are treated with standard procedures which include basic wound care and surgery, ranging from skin grafting, flap closure and reconstructive measures. Unfortunately, the chronicity is resistant to conservative treatment and either the age or the co-existing morbid conditions are unfavorable for special surgical measures. In recent years, with the development of molecular biology, growth factors are included into the treatment options. Stem cell research has also brought a new area of application to chronic ulcers. These new measures, however, remain in their experimental stage short of general application. On the other hand, traditional
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Preface
ix
herbal medicine might have something special to offer in chronic situations resistant to treatment. Chapter 4 – Natural and holistic treatments have been found to be extremely beneficial for maintaining problem-free and healthy skin. Treatments with cosmeceutical products such as herbal and homeopathic remedies are a safe and gentle alternative without the harmful side effects of synthetic chemicals often found in topical prescription medication. Several products are being manufactured today with the use of cosmeceutical ingredients, such as moisturizers and anti-aging treatments. Cosmeceuticals are likely to contain active ingredients like retinoids, hidroxy acids, antioxidants and other important constituents. These ingredients are a great aid in improving the appearance and delivery of essential nutrients to the skin that help maintaining the skin’s vitality. This chapter review many interesting topics and ideas with the aim to improve the knowledge of chemists and/or physicians who desire to better understand the meaning of this unusual created word cosmeceutical. Chapter 5 – Surgical site infection is a mean issue in cardiac surgery, leading to prolonged hospitalization, and substantially increased morbidity and mortality. In the literature the incidence to develop sternal surgical site infection varies from 1.3 to 12.8%. One source of pathogens is the endogenous flora of the patient’s skin, which can contaminate the surgical site. A number of preoperative skin care strategies are performed to reduce bacterial contamination like preoperative antiseptic showering, hair removal, disinfection of the skin, adhesive barrier drapes, and antimicrobial prophylaxis. Furthermore we can also support the natural host defense by optimal intra-operative management of oxygen supply, glycemia, and temperature. This review overviews the recent literature about preventing SSIs in cardiac surgery. Chapter 6 – Skin care has undergone significant developments over the past decade with many companies now marketing skin care products directly to consumers. Few over-the-counter (OTC) products have data to support their efficacy at a clinical level. Current evidence supports a basic regimen for preventative skin care including twice-daily facial cleansing and twice-daily moisturizer application. Daily sunscreen use represents the most effective means of preventing photoaging and development of non-melanoma skin cancers. This article will focus on preventative therapies as well as additional topical treatments directed at maintenance and repair of photoaged skin. Chapter 7 – Acne vulgaris is a common disorder of adolescents and young adults that can be very severe especially in those with concomitant
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
x
Preface
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
hyperandrogenic conditions. The pathophysiology of acne vulgaris is reviewed along with its differential diagnosis, including acne variants. Management of acne is also reviewed including use of topical and oral anti-acne agents such as benzoyl peroxide, retinoids, and antibiotics (topical and oral). Treatment of severe acne includes management of underlying disorders (as endocrine conditions) along with oral isotretinoin. Other medications that may be useful in selective cases include oral contraceptives, low dose prednisone, antiandrogens (as spironolactone or cyproterone acetate), or gonadotropinreleasing hormone agonists. Chapter 8 – After a dermal injury, the biochemical process of wound repair initiates a complex series of events that results in the deposition of a collagen-rich matrix. The wound healing process is divided in three distinct phases, inflammatory-proliferative-remodeling, and can take months to complete. At the end of the process, although the mature scar has not the high degree of organization as the normal dermis, it has the aspect of a fine-line.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
In: Skin Care Editor: Sandra M. Hayes, pp. 1-29
ISBN 978-1-61209-568-4 © 2011 Nova Science Publishers, Inc.
Chapter I
Keeping Infant Skin Healthy through Proper Cleansing
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Georgios N. Stamatas1, Russel M. Walters2 and Lorena S. Telofski2 Johnson & Johnson Consumer France, Issy les Moulineaux, France, and others
Abstract Keeping the skin clean is essential to the overall good health of an individual. This statement is even more relevant in the case of infants, since infant skin structure, function, and composition are still developing, underscoring the need for special care. Skin cleansing essentially means removing unwanted substances, including irritants from sources such as saliva, nasal secretions, urine, feces, and dirt. These irritants include salts, lipolytic and proteolytic enzymes, infectious microbial species, as well as potential allergens. Keeping the diaper area clean helps prevent skin barrier breakdown and therefore rash (diaper dermatitis) and infection (candidiasis). Keeping hands clean, particularly in the case of babies with 1
Corresponding author: Georgios N Stamatas, PhD, Johnson and Johnson Santé Beauté France. 1, rue Camille Desmoulins, 92787 Issy-les-Moulineaux, France. Tel: +33 1 55 00 46 52. Email: [email protected]. 1 Johnson and Johnson Santé Beauté France, Issy les Moulineaux, France 2 Johnson and Johnson Consumer Companies Inc, Skillman, NJ, USA
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
2
Georgios N. Stamatas, Russel M. Walters and Lorena S. Telofski their hand-to-mouth behaviors, can help reduce or prevent oral transmission of microbial contaminants. Special attention should also be paid to the facial area, where vulnerable skin can be irritated by milk, saliva, and nasal mucosa, all of which have higher pH relative to skin which can be detrimental to skin barrier. Similarly skin folds and creases (prominent in infant skin) should be kept clean. Proper formulation of personal care products intended for use on infants and young children is essential and should take into account the unique properties of infant skin as well as infant behaviors. Proper cleansing products should therefore be mild to both infant skin and eyes. Although the need for and benefits of good skin hygiene are clear, optimal cleansing and bathing practices still remain debated, from the baby’s first bath through infancy and early childhood. In spite of this debate, evidence-based practice guidelines should form the basis of proper cleansing approaches.
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Keywords: Skin cleansing, skin barrier function, surfactants, diaper dermatitis, atopic dermatitis, bathing infants.
1. Historical and Cultural Perspective on Cleansing Practices of personal cleansing varied in history according to the cultural and/or religious context. Ancient Greeks facilitated the mechanical removal of dirt with steam baths and application of oils, whereas ancient Romans found delight in hour-long soaking as a social event that took place in public bathhouses [1]. Regular bathing habits disappeared together with the Roman Empire and gave way to rather filthy conditions in the Middle Ages and beyond in Western civilization. People tended to steer clear of water as it was considered a source of disease and public bathhouses were seen as places of immorality. Personal hygiene was however always strongly emphasized in Islamic and Hindu cultures. The discovery of the existence of microbes and the link to contagious disease (expressed in the “germ theory of disease”) in the 19th century established the importance of hygiene and cleanliness to health. Hand washing with soap is still globally advertised as one of the most effective and most inexpensive ways to curb the spread of infections [2]. The records of soap making date back to as early as 2800 BC in ancient Babylon [3] and it was reportedly used for bathing by ancient Egyptians since 1500 BC [4]. Soap making became an important industry in Mediterranean
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Keeping Infant Skin Healthy through Proper Cleansing
3
towns and soap had the status of a luxury product. Soap was initially made from animal fats boiled in ashes and later also from vegetable oils and natural soda. Technological and scientific progress in the 18th and 19th century marked a leap in soap manufacturing with cheaper and larger scale production and with purer products. Soap thus reached a much larger use for cleansing dishes, clothes, adults, and babies. The 20th century saw the advent of synthetic detergents, based on petroleum-derived products and used in the manufacturing of laundry and personal care products. With the new chemistries made available, the first baby specific cleansers arrived in 1953 and no longer induced the eye stinging effect that soaps cause. This was discussed vividly in the first article to appear on baby cleansing in 1961: “Especially in the case of babies and children, murder most foul could not evoke louder screams. Probably the fondest wish of any mother faced with hair wash hysterics was for a baby shampoo that could not burn when it got into the eyes” [5]. Today, personal hygiene practices are limited by the access to clean water and sanitation in developing countries, which poses a concern for the control of infectious diseases and other illnesses. Neonatal sepsis in developing countries is often due to exposure to environmental pathogens during unsanitary delivery and postnatal care [6]. For example, umbilical cord infections are relatively frequent in developing countries [7]. Clean cord care practice is effective in the prevention of cord infections, however not always practicable in developing countries where many deliveries take place at home under unsanitary conditions. Improvement of hygiene during delivery, umbilical cord care and newborn care should be part of the strategy to prevent infection. In fact, the fourth Millennium Development Goal of the United Nations (MDG4), that concerns reducing childhood mortality, involves promotion of hygiene as a central factor [8]. From a hygienic point of view, cleansing of the diaper area should occur with each diaper change and wiping of the face and hands should occur as needed on a daily basis. Additionally, special attention should be given to the skin folds, where dribbled milk, sweat and moisture are often found. Transition from exclusive milk consumption to a more varied diet, coupled with learning to self-feed, exposes the skin to food residues which can be irritating and which require more thorough, but still gentle cleansing. As infants develop, become more mobile, and begin to explore their world, environmental exposure to unwanted substances, including dirt and bacteria, increases and thus the need for more thorough cleansing. Personal hygiene in infants serves a functional purpose of removing dead skin cells and unwanted
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
4
Georgios N. Stamatas, Russel M. Walters and Lorena S. Telofski
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
substances from the skin surface, including irritants from sources such as saliva, nasal secretions, sweat, urine, and feces, as well as allergens, dirt, and bacteria. Moreover, maintaining the integrity of the skin barrier through proper hygiene is essential for overall health. In addition to supporting good hygiene, bathing can be a pleasurable moment for infants and an occasion to encourage parent-infant interaction [9]. Moreover, cleansing practices often serve a cultural function. Certain ritual procedures that accompany bathing are meant to ensure the spiritual well being and to encourage the physical development of the infant, as seen in the practice of ritual massages with plant oils in Muslim, Indian, and African cultural traditions [10]. Similar to other childrearing practices, such as discipline or toilet training, the timing of the first bath as well as the frequency of bathing infants may vary from one culture to another. Whether driven by biomedical understanding of healthcare needs or adherence to cultural practices and beliefs, maternal intentions to support the well-being and encourage thriving of their infants is considered to be universal.
2. Infant Skin Development and Implications for Proper Skin Care Routines 2.1. Infant Skin Structure, Composition, and Function Continue to Evolve over the First Years of Life Skin plays multiple roles, including acting as a sensory organ and as a protective physical barrier to keep water and nutrients in and external aggressors (such as heat, microbes, UV-irradiation, etc.) out. The barrier function is primarily located in the SC [11] and is defined by its physical and biochemical properties. Even full-term infants have skin properties that differ from adult skin. Due to the structural particularities and the distinct composition of infant skin, its barrier maturity is not yet attained at that young age. Compared to adult skin, these factors contribute to the higher vulnerability of infant skin to environmental aggressors. A gradual skin maturation process occurs over the first few years of life [12]. Structurally, corneocytes and keratinocytes are smaller and the suprapapillary epidermis and the stratum corneum (SC) are on average 20 and 30%, respectively, thinner in infants than in adults [13]. The microrelief network is
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Keeping Infant Skin Healthy through Proper Cleansing
5
more densely knitted, surface glyphics are smaller, underlying dermal papillae are distributed more homogenously and are of more even size and density, and glyphics and dermal papillae are matched one-to-one which is not the case in adults [13]. Furthermore, collagen fibers in the dermis are less densely packed [13-14]. These structural particularities have implications on skin barrier function and water handling properties. Smaller cell size together with thinner SC and epidermis suggest a weaker SC barrier [15]. Denser microrelief structures and the resulting larger surface area may contribute to differences in water absorption and desorption [16]. The composition of infant skin also has distinct features. Newborn SC is relatively dry, but becomes significantly more hydrated during the neonatal phase (i.e. the first four weeks of life) [17-18] and reaches water content levels above those measured in adults [16, 19]. Seemingly contradictory to the high skin hydration, infant skin has a lower concentration of natural moisturizing factors (NMF) [16], which are humectants thought to contribute to skin hydration by binding to water molecules [20]. It may also seem surprising that total lipids and sebaceous lipids are less abundant on the surface of infant skin (authors’ unpublished results) possibly due to lower sebum secretion [21]. This suggests that infant skin maintains its high hydration level by yet unidentified means, different from those in adults and possibly related the thin SC, the high cell turn-over rate [12] and/or its distinct surface structure. Facultative production of melanin, a photo-protective pigment [22], is found at lower concentrations in infant skin compared to their parents [23]. Low melanin concentration and shorter path through the thin SC, together with light scattering that appears reduced in infants [16] may put infants at higher risk for UV-induced damage and help explain the correlation between sun damage in childhood and malignant skin disease later in life [24-25]. The composition of the diverse microbial flora that inhabits adult skin (skin microbiome) has recently been mapped [26], but to date there exists no comprehensive knowledge of the commensal and symbiotic microbes that are hosted by infant skin and that are acquired in a gradual process starting at birth and continuing through subsequent interactions with the post-natal environment [27]. It is clearly desirable to characterize the infant skin microbiome to help understand microbial involvement in both non-infectious and infectious skin diseases. The skin barrier function is influenced among other factors by skin structure, lipid organization, SC hydration, and pH [20, 28] A transversal section through skin resembles roughly a brick wall, in which the bricks are
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
6
Georgios N. Stamatas, Russel M. Walters and Lorena S. Telofski
represented by corneocytes and the mortar by an intercellular lipid matrix [28]. With this image in mind, it can be envisaged why the small cell size and low abundance of lipids may contribute to an incomplete SC barrier. Skin barrier function is commonly indirectly assessed by the rate of trans-epidermal water loss (TEWL), which represents vapor loss that is not related to sweating [29]. It has been shown that young infants have higher TEWL rates than adults [16, 30] together with a higher inter-person variability [16], which is indicative of immature water-handling mechanisms. This notion is further supported by the water absorption and desorption properties, which are different in infants. In an experimental set up, larger amounts of water are absorbed through the skin, which are subsequently lost more quickly than in adults [16]. One may speculate that the more dense microrelief structure and the resulting larger surface area, as well as the lower abundance of NMF, may contribute to differences in water absorption and desorption [16]. The “acid mantle” of the human skin surface is the result of progressive acidification that takes place after a few days to weeks following birth [31]. At birth, the skin pH is close to neutral and varies between pH 6.6-7.5 as a function of the body site [30]. The skin pH then rapidly turns more acidic [17, 30] but still remains higher in infants than in adults [19]. Bacterial proliferation on the skin [32-33], as well as certain biochemical processes within the skin, including processing of the intercellular lipid matrix [34-35] and the desquamation process [35-36], are pH-sensitive. It is thus likely that these processes will be influenced by the differences in infant skin.
2.2. Infant Skin Properties as Risk Factors for Skin Disease and Implications of Proper Cleansing The functional immaturity of the skin barrier puts infants at risk for cutaneous disease. Two commonly observed skin afflictions in infancy that are associated with the breakdown of the skin barrier function are irritant contact dermatitis (ICD), in particular diaper dermatitis (DD) [18, 37] and atopic dermatitis (AD) [38]. 2.2.1. Irritant Contact Dermatitis More than others, the diapered area and the perioral region are repeatedly exposed to irritants that provoke skin inflammation through chemical or mechanical damage to the skin. Affected skin appears to be red and dry (scaling) and may be itchy, swollen, and even blistering [39].
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Keeping Infant Skin Healthy through Proper Cleansing
7
More than half of all infants experience DD, with an incidence peak around 9 to 12 months [40]. The physical characteristics of the diapered area explain why this region is particularly sensitive to skin irritation as manifested by redness and scaling of the buttocks, perianal region, inner thighs, and abdomen [41]. Foremost, the diaper creates a relatively occlusive environment enabling accumulation of excessive moisture, which causes structural changes in the SC, skin barrier breakdown and also creates increased friction [42-43]. Furthermore, and due to a combination of factors, including urine exposure [44-45], high SC hydration and resulting decrease in filaggrin breakdown [42], diapered skin has a more alkaline pH than other areas of the body [18, 37]. Exposure to feces in combination with an elevated pH increases the enzymatic activity of fecal proteases and lipases [42] which is detrimental to normal skin barrier function [46]. Thus this combination of occlusion, skin hydration, high pH, and fecal enzyme exposure damages the skin barrier and renders the diapered area particularly vulnerable to frictional damage and fecal enzyme exposure. Increased exposure to fecal enzymes enables microbial infection [42, 44, 47-48]. Severe and chronic forms of diaper dermatitis involve opportunistic infections predominantly with Candida spp. and Staphylococcus aureus [49]. Prevention and control of irritations in the diaper area should involve gentle cleansing with warm water, however water alone is not effective in removing oil-soluble substances such as feces, which may contain up to 4% fat [50]. Substances such as fecal enzymes, which can cause irritation if not removed, are better removed with a cleanser [51]. Harsh products or rubbing should generally be avoided and use of a gentle cleanser can help solubilize fatty substances and remove skin irritants without aggressive cleansing. There appears to be no association between the occurrence of DD and the use of wet wipes [52]. The use of the latter is recommend particularly when water is not available [53]. There was also no difference in frequency of DD in a recent study that compared bathing to cloth washing in newborns [54]. A recent study in a neonatal intensive care setting suggests that wipes with emollient cleansers that lack alcohol and fragrance and have an acidic pH provide better protection of the barrier function than the water and cloth approach [55]. Frequent diaper changes, together with drying and aeration of the skin should also be part of the routine [56-57]. For prevention and treatment of uncomplicated cases the use of protective barrier ointments or creams and zinc oxide containing preparations are usually sufficient. Severe cases, in particular
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
8
Georgios N. Stamatas, Russel M. Walters and Lorena S. Telofski
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
those with secondary infection, require medical attention and the use of an antimicrobial agent [58]. Even otherwise innocuous substances, such as saliva or breast milk, can be the source of skin irritations and induce ICD. Exposure to oral secretions, often trapped underneath a pacifier, may cause maceration and inflammation of the exposed skin in the perioral region. Even thumb sucking has been associated with perioral dermatitis due to the trapping of saliva against the lips and adjacent skin [59]. Common substances such as spit-up formula or breast milk (pH 7.2 [60]) and breast milk proteases, saliva (pH 7.2-7.3 [61]) and salivary enzymes, nasal secretions, and food soils have been associated with skin irritation which can be further exacerbated by frequent wiping. Steps should be taken to protect infant’s delicate facial skin, particularly the perioral region, including gentle cleansing and efforts to keep the face dry at all times. 2.2.2. Atopic Dermatitis AD is a chronic, inflammatory skin disease which is presented with itching erythematous papules and vesicles that often first appear on the infant’s face. Almost 20% of children develop AD [62-63]. The etiology of AD is a complex interaction between both environmental and genetic factors [64]. The functional hallmark of AD is a defective skin barrier as evidenced by increased water loss (TEWL) and higher pH [38]. This is associated with mutations in structural and other proteins of the epidermis, which are integral to skin barrier function [65]. It was hypothesized that barrier dysfunction is the initial event in the disease development which then allows penetration of allergens and irritants through the skin [65]. This is supported by the observation that barrier function is also impaired in areas of non-involved skin in children with AD compared to healthy children [38]. Even clinically uninvolved perioral and cheek areas may turn dermatitic through mechanical or chemical stress from oral secretions and rubbing against the skin [66]. Barrier dysfunction is also likely related to the risk of microbial infection in children with AD (64). AD may have a decisive role in the future development of allergic airway disease: there is evidence that it is often associated with subsequent development of asthma and allergic rhinitis. Early sensitization and greater severity of AD correlate with the highest risk [67]. It was proposed that the link between AD and other allergic disorders is allergen penetration through the skin and immune sensitization that can affect the airways, a process termed the “atopic march” [67]. This suggests that preservation or restoration of a functional epidermal barrier may diminish the risk, or possibly the severity, of these specific immune diseases.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Keeping Infant Skin Healthy through Proper Cleansing
9
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
In AD, skin barrier dysfunction should not be exacerbated by environmental factors including soap and harsh detergents. Although still remaining somewhat controversial, recent publications suggest regular bathing to help prevent infection and stimulate skin debridement [68]. Recommendations generally include warm versus hot water, bathing of short duration, preferably with a moisturizing cleanser that does not compromise skin barrier integrity, followed by gentle dry patting and immediate application of a moisturizer [64, 69-70]. The use of emollients during and after bathing is recommended in babies at risk for AD [51]. 2.2.3. Cradle Cap (Pityriasis Capitis) Although infants produce less sebum than adults, sebum production is high around birth and during the first weeks of life [21]. Cradle cap is a frequently observed form of infantile seborrhoeic dermatitis (ISD) with onset typically within the first 2-3 months of life. ISD manifests as scaling or crusting and typically involves the scalp, but face, ears, neck, trunk, and the diaper area may also be affected [71-72]. While most cases of ISD self resolve in a matter of weeks, some persist until the age of 8-12 months [73-75]. ISD is an inflammatory disorder related to a dysfunction of the sebaceous glands which are influenced by maternal hormones [76]. Literature has reported association with Pityrosporum ovale in infants with ISD as greater than in healthy infants with no ISD [77]. This condition is generally managed with application of mineral oil, to help release greasy scales from the scalp and hair, followed by cleansing with a mild baby shampoo [78]. Infant eyes continue to develop and mature structurally over the first year of life [79-81] and care should be taken to avoid use of harsh cleansers. Infants blink less often and their eyes are open for a longer time [82-83]; tearing is less robust [79]; defensive eye closure is not fully developed [84] and eye rubbing is common. There is thus greater potential for exposure to unintended substances and for them to be rubbed into the eyes. For these reasons, recommendations are made to use a specially formulated shampoo that has been tested and shown to be safe in case of incidental contact with the eyes of the infant. 2.2.4. Intertrigo Particular attention in infants should be paid to skin folds such as neck fold, axillae, inguinal region, gluteal folds, back of knees, and inside of elbows. Friction of opposing skin surfaces in these areas can be exacerbated by trapped moisture and heat and cause skin inflammation (intertrigo) that may lead to secondary bacterial or fungal infection involving Staphylococcus
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
10
Georgios N. Stamatas, Russel M. Walters and Lorena S. Telofski
aureus, Candida albicans and other microorganisms [85]. This concerns in particular young infants with deep skin fold due to chubbiness and flexed posture. Keeping these areas dry and clean is essential in prevention and treatment of intertrigo [86].
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
3. Cleansing Technology A cleanser is expected to remove unwanted material from the skin, such as dirt, oils, sebum, sweat, and microbes, without causing an unwanted sensation of after-wash tightness or inducing dryness, irritation, erythema, itch, and barrier damage [87]. An ideal cleanser for infants must provide appropriate cleansing action and yet be mild enough to avoid irritation of skin and eyes. Recently, over 90 volatile organic compounds (VOCs) were identified on human skin [88]. These are largely hydrophobic substances that likely originate from multiple sources, both endogenous and exogenous, such as degradation products of microbes. Without any ability to emulsify hydrophobic compounds, water alone cannot remove all these impurities that accumulate on skin. Oil-soluble dirt needs to be emulsified into droplets that can be rinsed off the skin. This is achieved by surfactants (“surface acting agents”) that reduce the interfacial tension between oil and water after absorption to the interface [89]. Physically, surfactants are amphiphilic molecules that feature a hydrophobic tail and a hydrophilic head. At the water/oil interface, the hydrophobic head groups orient towards the aqueous environment, while the hydrophobic tail groups extend towards the oil phase. Reduction of the surface tension allows for emulsification of oily droplets which include the lipid-soluble parts of dirt. In aqueous solutions surfactants exist both as individual monomers and as micelles. Micelles are composed of roughly 80-100 self-assembled surfactant monomers with their hydrophobic tails inside the micelle, excluded from the water. Two types of solid cleanser bars can be distinguished: soaps and syndets (contraction of synthetic detergents). Soaps are detergents derived from saponification, which is the action of a strongly alkaline solution on oils or animal fat, mostly vegetable oils and tallow [90] and have an alkaline pH. Syndets are derived from oils, fat, or petroleum products and with a lower pH they are more compatible with skin than soaps. A third type of cleansers is liquid surfactant systems. Water, pH-adjusters, preservatives, and surfactants make up the core components of liquid cleansers [91]. Added to this mix are stabilizers, moisturizers, conditioners (such as glycerin), and fragrance.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Keeping Infant Skin Healthy through Proper Cleansing
11
Both the foaming action and the mildness of a surfactant are influenced by the charge of their hydrophilic head groups. Anionic surfactants foam well and amphoteric ones (i.e. with both an anionic and a cationic group) moderately well. Non-ionic surfactants have the least foaming action. On the other hand, non-ionic surfactants are the mildest, followed by amphoteric surfactants, while anionic detergents are at the other end of the spectrum [89, 92]. The mildness of surfactants can be experimentally defined by assessing trans-epidermal penetration, protein solubilization, or collagen-swelling potential [93-95]. Potent surfactants not only remove dirt, but also risk damage to the skin barrier by denaturing SC proteins and both removing and disrupting skin lipids. Alkaline soaps can also change skin pH. Removal of NMF from the SC by surfactants can reduce the hydration level of the skin [87]. Denaturation of SC proteins is possibly mediated through the formation of micelle-like surfactant aggregates on the proteins [93]. Likewise, it was proposed that lipid depletion occurs through solubilization of lipids in surfactant micelles [96]. Besides the nature of surfactants that make up a cleanser, the pH value and the pH buffering capacity of the cleanser also play important roles in the alterations of the physical properties of SC. Swelling and denaturation of SC proteins as well as disruption of the lipid organization escalate with increasing pH [97]. The surfactant ability to disrupt barrier function has a self-propagating effect that allows their own penetration into the living epidermis, where they trigger skin irritation through disruption of epidermal cells and a subsequent inflammatory response [96, 98]. As a consequence, surfactants that interact strongly with proteins cause significant skin irritation [87]. Anionic surfactants have a higher tendency to interact with proteins than amphoteric surfactants, while non-ionic ones have the least, thus explaining the difference in their harshness/mildness: the order of surfactant irritation potential is anionic surfactants > amphoteric surfactants > non-ionic surfactants [87]. Disruption of skin barrier function is related to the type of surfactants used in the formulation, as well as to the pH of the cleanser. Due to their alkaline nature (pH 10) [87], soaps may alter the acidic pH of the skin (90). Syndets are considered milder and less irritant than soap due to their pH, which is neutral or acidic (pH ≤ 7) [87] and thus closer to the pH of newborn (pH 6.6-7.5) [30] and adult (pH 4.5-6.7) [30, 99-100] skin. Compared to alkaline soaps, they minimally alter the skin pH and cause less lipid depletion [101], induce significantly less erythema [102], and result in a lower TEWL rate [103]. Typical cleansers contain primarily anionic surfactants because of their foaming characteristics [87]. Adult shampoos for example commonly contain
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
12
Georgios N. Stamatas, Russel M. Walters and Lorena S. Telofski
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
sodium lauryl sulfate (SLS) and sodium laureth sulfate (SLES), strong anionic surfactants that provide rich foam and good cleansing [92, 104]. To increase mildness, liquid body cleansers are often blends of anions and amphoteric surfactants [94]. The surfactants used in body wash products contain milder surfactants than those in bar soaps [105].
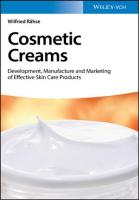
Figure 1. Large micelles are less irritating to the skin. Blended surfactant systems for different cleansing products result in micelles of different sizes. For example, adult shampoo may be composed of anionic surfactants, while adult body cleanser may combine amphoteric and anionic surfactants to make it less harsh on the skin. Baby cleansers contain the mildest blend of surfactants required for the sensitive baby skin and eyes and may include ethoxylated anionic, amphoteric, and nonionic surfactants.
Compared with adult cleansers, infant cleansers contain lower concentrations of surfactants and these are predominantly comprised of a blend of amphoteric, non-ionic, and anionic surfactants [106]. An important characteristic of amphoteric surfactants is their lack of eye irritancy which provides mildness in baby shampoos [92]. Anything more than the associated mild cleansing action is not needed considering that sebum production in infants is limited [21]. When multiple surfactants are present in a formulation, mixed micelles are formed that comprise blends of all the surfactants and whose properties are the results of the interaction between all the surfactants present. Foaming action, mildness, and cleansing activity are determined by micelle size and micelle surface charge (small size and high charge micelles tend to be more irritating). Anionic surfactants create smaller micelles, while amphoteric surfactants in
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Keeping Infant Skin Healthy through Proper Cleansing
13
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
body cleansers and even more so non-ionic surfactants in baby cleansers increase bulkiness and reduce the surface charge (Figure 1). As a consequence, baby cleansers are least aggressive to tissues as indicated by their comparably low ability to disrupt tight junctions that hold together epithelial cells [106]. They also have the lowest foaming ability, while adult shampoos have the highest. Blending surfactant systems with certain non-ionic ethoxylated surfactants such as PEG-80 sorbitan laurate renders such systems milder. Previous related research suggests how the PEG-80 sorbitan laurate interacts with micelles, as depicted in Figure 1, and how polyethylene oxides (PEOs) stabilize micelles through PEGylation. Maltesh and Somasundaran showed that PEG chains interact with the anionic surfactant sodium dodecyl sulfate by forming a pearl necklace structure around the micelles and thereby covering the surface of the micelle [107]. Also Discher and Ahmed used PEG chains to create biocompatible “stealth vesicles” that have long circulation times in the body and are highly biocompatible [108]. Finally, it was shown that PEO chains reduce the amount of sodium dodecyl sulfate that penetrated into the epidermis [109].
4. The Need for Evidence-Based Practice 4.1. Current Knowledge Given the physiological and functional differences between infant and adult skin, it is of primary importance to obtain clinical data in infants of the effect of cleansing methods and cleansing products and to transform this scientific knowledge into guidelines that help parents and caregivers to make informed choices. Bathing is routinely performed after the birth process to wash off amniotic fluid and blood and has been recommended to reduce the risk of exposure to blood borne pathogens for health care professionals [110]. A concern over bathing newborns after delivery is that, when it is not done properly, it may cause hypothermia [111]. However, bathing with warm water is not harmful as early as one hour after birth when practiced on thermostable newborns [112]. Immersion bathing helps prevent heath loss and maintain body temperature better than sponge washing [9, 113]. Garcia Bartels et al. compared the effects of bathing on newborn skin barrier function to those of washing in a randomized study involving 57 newborns [54]. Starting at one week after birth, infants were either bathed
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
14
Georgios N. Stamatas, Russel M. Walters and Lorena S. Telofski
twice weekly in tap water without additives or cloth washed with tap water only. Both regimens were conducted at the same frequency until four weeks of life. TEWL, SC hydration, pH, and sebum content were assessed at different body sites. No significant difference in pH or sebum levels was observed between the two skin care regimens after four weeks. TEWL levels were also similar, with the exception of lower TEWL rates on the buttocks in the bathing group. SC hydration was higher in the bathing group on the abdomen and forehead. Based on clinical evaluations, the authors concluded that no obvious harm was done with either approach. In a similar approach, a randomized, prospective study evaluated the effect of twice weekly bathing on barrier function caused by bathing with a commercial pH 5.5 wash gel or bathing with water alone starting after seven days of life until the age of two months in 64 newborns [114]. None of these regimens shifted the assessed parameters (TEWL, SC hydration, pH and sebum content) to non-physiological values in four different anatomic regions at two months. Bathing with and without washgel resulted in comparable TEWL and SC hydration, however pH was significantly lower (more acidic) in babies cleansed with washgel. Addition of cream after bathing with or without washgel lowered TEWL and enhanced SC hydration in some areas compared to bathing with water alone. Sebum levels were not affected by either of the regimens, and fungal and bacterial colonization of the umbilical region was similar. Importantly, these assessments were carried out at least 12 hours after the last bath, in order to avoid transient effects. Another comparative, randomized study in 180 infants aged 1 day to < 1 year found that two commercial liquid cleansers and water did not significantly change skin properties such as moisture content, pH and TEWL, nor did they induce any visible irritation such as erythema, dryness or flaking after two weeks of testing [115]. One of the two cleansers however caused an increase in TEWL. This finding suggests the need for care, based on data, in selecting a mild cleanser appropriate for infants. As observed in a non-comparative study on 3-6 month old infants bathed with a liquid cleanser, TEWL and moisture accumulation rate were significantly higher immediately after the bath, but this effect disappeared fifteen minutes later on non-diapered skin [116]. After 15 minutes, the moisture accumulation rate was significantly lower compared to before bathing indicating better barrier quality. Since this was a non-comparative study, it is not clear whether this transient effect is attributable to the contact with water alone, or in relation to the liquid cleanser. This was addressed in a randomized study on 40 infants 2 weeks to 16 months old, which were bathed
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Keeping Infant Skin Healthy through Proper Cleansing
15
either with water alone, liquid cleanser (pH 5.5), compact cleanser (pH 5.5), or with alkaline soap (pH 9.5) [101]. All of these cleansing agents, including water, significantly raised the skin pH as measured 10 minutes after the bath compared to pre-bath values. The lowest increase was observed with water, the highest with alkaline soap. A similar effect was observed for the lipid content, which significantly decreased after bathing regardless of the cleansing agent used. No significant effect was observed on skin hydration. This study however did not address longer-term effects of the cleansing procedures used. A factor which was not controlled in these studies and which may contribute to skin irritation or dryness of sensitive skin is the water hardness (relating to calcium ion content) [117]. Acquisition of normal microbial skin flora in newborns was shown not to be affected by the choice of bathing regimen. In a randomized study, the use of mild (pH neutral) soap in bathing newborns after birth or bathing in water alone did not result in differences in the microbe classes, nor in the quantity of microbes acquired during the first 24 hours of life [118]. Garcia-Bartels et al. showed that colonization of the umbilical region with Candida or bacteria does not differ in newborns washed with a cleanser or water alone during the first two months of their life [114]. Taken together, evidence from randomized clinical trials suggests that while bathing with or without cleansers may affect skin conditions in the short term, either approach is safe in the long-term, without any major differences in barrier function, irritation or microbial colonization.
4.2. Current Guidelines Infant skin care practices are very much driven by cultural context and traditions. Even within developed countries there is a divergence in approaches, such as the timing of the first bath [51], removal or preservation of the vernix caseosa [119] or choice of washing over bathing [120]. This, together with the emerging understanding of the physiology of infant skin calls for infant skin care recommendations to be based on clinical evidence. A recent conference held in 2007 by European dermatologists and pediatricians reached consensus on guidelines for infant bathing and cleansing based on a comprehensive literature review [51]. Additionally, a US evidence-based practice guideline on neonatal skin care, based on a 3-year research project, was published in 2001 by the Association of Women’s Health, Obstetric and Neonatal Nurses (AWHONN) and the National Association of Neonatal
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
16
Georgios N. Stamatas, Russel M. Walters and Lorena S. Telofski
Nurses (NANN) [121-122]. The second edition, published in 2007, was updated based on review of quantitative literature, published in the interim between the first and second editions, that was then evaluated using recognized analysis and assessment methods [53]. Both guidelines address newborn care, i.e. from birth to four weeks of age. The European guideline is tailored to full-term newborns (i.e. at least 37 weeks gestational age), whereas the AWHONN guideline also addresses care in babies born at an earlier gestational time. Overlaps between the two guidelines are prevalent. There are however some noteworthy differences, such as the water temperature recommended for newborn bathing and the specific recommendations for the care of the vernix and the circumcised penis, which are absent in the European guideline (Table 1).
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Table 1. Comparison of guidelines set forth by the European round table meeting and by the AWHONN. European consensus panel recommendations (51)
AWHONN guidelines (53)
First bath
Performed in thermally stable babies Wiping or washing with water Potential benefit of delay after umbilical cord has fallen
Performed in thermally stable babies (after 2-4 hours) Minimal amount of pH-neutral cleanser if desired Duration as short as possible
Routine bathing
2-3 times per week 5-10 minutes 37.0-37.5°C Mild liquid cleansers preferable to water alone
No more often than every other day 38-40°C pH-neutral cleansers Leave on, allow to wear off with normal care and handling Neutral pH cleansers or water, no antimicrobial topical agents.
Vernix care Umbilical cord care Circumcised penis care
Cleansing with water
Atopic dermatitis
Use of moisturizing liquid cleansers and emollients during and after bathing in babies at risk for AD
Diaper dermatitis
Treatment with a protective ointment or emollient
Washing with water or detergent- and alcohol-free wipes Use of barrier creams
The European guideline stipulates that the first cleansing immediately after birth may involve wiping or washing with water and that the first bath Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Keeping Infant Skin Healthy through Proper Cleansing
17
should be performed on thermally stable babies. Studies found no difference in body temperature in newborns bathed one to 6 hours after birth [112, 123124]. The European guideline leaves the timing of the first bath thus to local culture. Importantly, bathing for newborns was found to be safe, as shown by studies that evaluated the effect on temperature stability, umbilical cord healing, and risk of infections and the effect on skin barrier function [9, 54, 125-126]. The European guideline does however concede possible advantages associated with postponing bathing until after the umbilical cord has fallen, as one study found higher incidence of umbilical cord infections in tub-bathed babies [127]. Routine baths should be given no more than 2-3 times a week and for no longer than 5-10 minutes. The recommended water temperature is 37.0-37.5°C. Bathing is considered better than cloth washing, as it better protects thermal stability [9, 125], leaves newborns calmer and quieter [9, 125] and causes less TEWL and higher SC hydration [54]. The European consensus calls for liquid cleansers which have undergone thorough safety testing. Addition of vegetable oils or cosmetic bath oils to bath water should be avoided; the use of fragrances should be limited or avoided and appropriate preservation should be used. It is expected that a liquid cleanser does not change the pH of the skin nor causes irritation to skin or eyes. No recommendation on the timing of the first addition of liquid soap to bath water was given in the European recommendation, as the consulted sources were not consistent and appeared to represent opinions. In routine bathing, use of a mild liquid cleanser is recommended over water alone, as data suggests that water alone may have a more drying effect on skin and induce erythema more readily than a liquid cleanser [128]. Liquid cleansers with emollients are considered to better protect skin than water alone. The lack of sufficient clinical data regarding the benefits of liquid cleaners is however underscored and the lack of an effect on skin barrier development by bathing either with a wash gel and use of topical lotion or bathing with water alone in a recent study [114] is noted. Care of AD skin includes the uses of moisturizing liquid cleansers and the use of emollients during and after bathing in babies at risk for AD. DD should be treated with a protective ointment or emollient. The AWHONN guideline suggests that the first bath should be performed on thermally stable babies which may take 2-4 hours after birth. For the purpose of removing blood and amniotic fluid, a mild pH-neutral cleanser might be added to the first bath. Routine baths should be given no more than every other day at a water temperature of 38-40°C. The AWHONN guideline gives particular consideration to the vernix caseosa. The vernix develops during the last trimester in utero and is made of water, proteins, and lipids,
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
18
Georgios N. Stamatas, Russel M. Walters and Lorena S. Telofski
with cell ghosts embedded in a lipid matrix and is presumed to facilitate SC barrier development [129]. It is recommended to leave the vernix on the skin after birth and to allow it to wear off with normal care and handling due to the potential beneficial properties, which among others include protection against infection [130-133], decreased TEWL [134], skin moisturization [133, 135], temperature regulation [131, 135], and positive effect on pH development [136]. According to the AWHONN guideline, the umbilical cord stumps should be cleansed with a neutral pH cleanser or water and the use of antimicrobial topical agents is discouraged. It is however noted that in developing countries the use of topical agents may be indicated to reduce the risk of neonatal tetanus and sepsis, when standard hygiene practices in childbirth and neonatal care are not met. The circumcised penis should be cleansed with water only. Cleansers should be used sparingly and have a pH of 5.5-7.0. Care for DD includes washing with water or detergent- and alcoholfree wipes and use of barrier creams. Preservative-free products or preservatives with proven safety/tolerance profile are recommended.
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Summary – Outlook Keeping the skin clean is essential to the overall health of an individual and this statement is even more relevant for infants. Infant skin needs to be kept clean, with particular attention given to frequently soiled body parts, such as the diaper area, hands and face, but also skin folds and creases. More than providing the means to rid the body of dirt and debris and to maintain good hygiene, cleansing and in particular bathing is an opportunity for caregivers and infants to connect and to provide a pleasurable moment for the infant. Immersion bathing is considered a safe method even for newborns. The immature barrier function and the related propensity for disease and damage explain why particular considerations should guide appropriate formulation and use of infant cleansers. Adequately formulated cleansers are needed that respect the immature skin barrier and do not interfere with its natural maturation process. Basic principles of infant cleansing thus involve adequate hydration, preservation of the acid mantle, avoidance of excessive friction, and protection from irritants. Although the need for and benefits of good skin hygiene are clear, there is certainly a gap in useful (randomized, controlled) clinical trial data on optimum skin care in infants, such as the effect of frequency of bathing and the use of skin care products on the barrier function in older infants. Cleansing
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Keeping Infant Skin Healthy through Proper Cleansing
19
needs evolve as infants develop, change feeding habits and encounter more dirt during increasing exploration of their environment. Our understanding of infant skin is evolving, such as the notion that infant skin maturation is a process that is not complete at birth or shortly thereafter as previously assumed [137], but that continues throughout the first years of life [16]. This new knowledge has to be considered when designing studies on the effect of cleansing on infant skin and should stimulate the evolution/adaptation of evidence-based practice guidelines accordingly.
Acknowledgments The authors would like to thank Dr Beate Gerstbrein of Ascopharm for editorial assistance.
References Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
[1] [2]
[3] [4]
[5] [6]
[7]
[8]
Ashenburg K. Clean: An Unsanitised History of Washing: Profile Books Ltd; 2008. Global Handwashing Day 2008. [Accessed on 30/09/2010]; Available from: http://www.who.int/gpsc/events/2008/Global_Handwashing_Day_ Planners_Guide.pdf. Willcox M. Soap. In: Butler H, editor. Poucher's Perfumes, Cosmetics and Soaps. 10th edition ed. Dordrecht: Academic Publishers; 2000. Eng RW. The Discovery and Prehistory of Soap. [Accessed on 30/09/2010]; Available from: http://www.butser.org.uk/iafsoap_ hcc. html. Mannheimer HS. Baby shampoo. American Perfumer. 1961;76:36-7. Zaidi AK, Thaver D, Ali SA, Khan TA. Pathogens associated with sepsis in newborns and young infants in developing countries. Pediatr. Infect. Dis. J. 2009;28(1 Suppl):S10-8. World Health Organization DoRHaR. Care of the umbilical cord: A review of the evidence. 1998 [Accessed on 30/09/2010]; Available from: http://whqlibdoc.who.int/hq/1998/WHO_RHT_MSM_98.4.pdf. United Nation Millennium Development Goals. [Accessed on 30/09/ 2010]; Available from: http://www.un.org/millenniumgoals/.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
20 [9]
[10] [11] [12]
[13]
[14]
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
[15] [16]
[17]
[18]
[19]
[20] [21] [22]
Georgios N. Stamatas, Russel M. Walters and Lorena S. Telofski Bryanton J, Walsh D, Barrett M, Gaudet D. Tub bathing versus traditional sponge bathing for the newborn. J. Obstet. Gynecol. Neonatal. Nurs. 2004;33(6):704-12. Lévy I. Mères et enfants d'ailleurs. Médecine and enfance. 2000:533-47. Lee SH, Jeong SK, Ahn SK. An update of the defensive barrier function of skin. Yonsei Med. J. 2006;47(3):293-306. Stamatas GN, Nikolovski J, Mack MC, Kollias N. Infant skin physiology and development during the first years of life: a review of recent findings based on in vivo studies. Int. J. Cosmet. Sci. 2010 [Epublished ahead of print]. Stamatas GN, Nikolovski J, Luedtke MA, Kollias N, Wiegand BC. Infant skin microstructure assessed in vivo differs from adult skin in organization and at the cellular level. Pediatr. Dermatol. 2010;27 (2):125-31. Vitellaro-Zuccarello L, Cappelletti S, Dal Pozzo Rossi V, Sari-Gorla M. Stereological analysis of collagen and elastic fibers in the normal human dermis: variability with age, sex, and body region. Anat. Rec. 1994;238(2):153-62. Marks R, Nicholls S, King CS. Studies on isolated corneocytes. Int. J. Cosmet. Sci. 1981;3(6):251-9. Nikolovski J, Stamatas GN, Kollias N, Wiegand BC. Barrier function and water-holding and transport properties of infant stratum corneum are different from adult and continue to develop through the first year of life. J. Invest. Dermatol. 2008;128(7):1728-36. Hoeger PH, Enzmann CC. Skin physiology of the neonate and young infant: a prospective study of functional skin parameters during early infancy. Pediatr. Dermatol. 2002;19(3):256-62. Visscher MO, Chatterjee R, Munson KA, Pickens WL, Hoath SB. Changes in diapered and nondiapered infant skin over the first month of life. Pediatr. Dermatol. 2000;17(1):45-51. Giusti F, Martella A, Bertoni L, Seidenari S. Skin barrier, hydration, and pH of the skin of infants under 2 years of age. Pediatr. Dermatol. 2001;18(2):93-6. Rawlings AV, Harding CR. Moisturization and skin barrier function. Dermatol. Ther. 2004;17 Suppl 1:43-8. Agache P, Blanc D, Barrand C, Laurent R. Sebum levels during the first year of life. Br. J. Dermatol. 1980 Dec;103(6):643-9. Brenner M, Hearing VJ. The protective role of melanin against UV damage in human skin. Photochem. Photobiol. 2008;84(3):539-49.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Keeping Infant Skin Healthy through Proper Cleansing
21
[23] Mack MC, Tierney NK, Ruvolo E, Jr., Stamatas GN, Martin KM, Kollias N. Development of solar UVR-related pigmentation begins as early as the first summer of life. J. Invest. Dermatol. 2010;130(9):23358. [24] Gallagher RP, Hill GB, Bajdik CD, Fincham S, Coldman AJ, McLean DI, et al. Sunlight exposure, pigmentary factors, and risk of nonmelanocytic skin cancer. I. Basal cell carcinoma. Arch. Dermatol. 1995;131(2):157-63. [25] Mills O, Messina JL. Pediatric melanoma: a review. Cancer Control. 2009;16(3):225-33. [26] Grice EA, Kong HH, Renaud G, Young AC, Bouffard GG, Blakesley RW, et al. A diversity profile of the human skin microbiota. Genome Res. 2008;18(7):1043-50. [27] Capone K, Dowd SE, Stamatas GN, Nikolovski J. Survey of bacterial diversity on infant skin over the first year of life. J. Invest. Dermatol. 2010;130(S1):S124. [28] Elias PM. Epidermal lipids, barrier function, and desquamation. J. Invest. Dermatol. 1983;80 Suppl:44s-9s. [29] Levin J, Maibach H. The correlation between transepidermal water loss and percutaneous absorption: an overview. J. Control Release. 2005;103(2):291-9. [30] Yosipovitch G, Maayan-Metzger A, Merlob P, Sirota L. Skin barrier properties in different body areas in neonates. Pediatrics. 2000 Jul;106(1 Pt 1):105-8. [31] Behrendt H, Green M. Skin pH pattern in the newborn infant. AMA J. Dis. Child. 1958;95(1, Part 1):35-41. [32] Matousek JL, Campbell KL. A comparative review of cutaneous pH. Vet. Dermatol. 2002;13(6):293-300. [33] Korting HC, Hubner K, Greiner K, Hamm G, Braun-Falco O. Differences in the skin surface pH and bacterial microflora due to the long-term application of synthetic detergent preparations of pH 5.5 and pH 7.0. Results of a crossover trial in healthy volunteers. Acta Derm. Venereol. 1990;70(5):429-31. [34] Mauro T, Holleran WM, Grayson S, Gao WN, Man MQ, Kriehuber E, et al. Barrier recovery is impeded at neutral pH, independent of ionic effects: implications for extracellular lipid processing. Arch. Dermatol. Res. 1998;290(4):215-22. [35] Hachem JP, Man MQ, Crumrine D, Uchida Y, Brown BE, Rogiers V, et al. Sustained serine proteases activity by prolonged increase in pH leads
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
22
[36]
[37]
[38]
[39]
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
[40]
[41]
[42] [43] [44] [45] [46] [47] [48]
Georgios N. Stamatas, Russel M. Walters and Lorena S. Telofski to degradation of lipid processing enzymes and profound alterations of barrier function and stratum corneum integrity. J. Invest. Dermatol. 2005;125(3):510-20. Deraison C, Bonnart C, Lopez F, Besson C, Robinson R, Jayakumar A, et al. LEKTI fragments specifically inhibit KLK5, KLK7, and KLK14 and control desquamation through a pH-dependent interaction. Mol. Biol. Cell. 2007;18(9):3607-19. Stamatas GN, Zerweck C, Grove G, Martin K. Documentation of Impaired Epidermal Barrier in Mild and Moderate Diaper Dermatitis In Vivo Using Non-Invasive Methods. Ped. Dermatol. 2010 (in print). Seidenari S, Giusti G. Objective assessment of the skin of children affected by atopic dermatitis: a study of pH, capacitance and TEWL in eczematous and clinically uninvolved skin. Acta DermVenereol. 1995;75(6):429-33. Lisby S, Baadsgaard O. Mechanisms of irritant contact dermatitis. In: Rycroft RJG, Menné T, Frosch PJ, Lepoittevin JP, editors. Textbook of contact dermatitis. 3rd ed. Berlin, Heidelberg, New York: Springer; 2001. p. 91-110. Jordan WE, Lawson KD, Berg RW, Franxman JJ, Marrer AM. Diaper dermatitis: frequency and severity among a general infant population. Pediatr. Dermatol. 1986;3(3):198-207. Visscher MO, Chatterjee R, Munson KA, Bare DE, Hoath SB. Development of diaper rash in the newborn. Pediatr. Dermatol. 2000; 17(1):52-7. Visscher MO, Hoath SB. Diaper Dermatitis. In: Chew A-L, Maibach HI, editors. Irritant dermatitis. Berlin, New York: Springer; 2006. p. 37-51. Atherton DJ. The aetiology and management of irritant diaper dermatitis. J. Eur. Acad. Dermatol. Venereol. 2001;15 Suppl 1:1-4. Berg RW, Buckingham KW, Stewart RL. Etiologic factors in diaper dermatitis: the role of urine. Pediatr. Dermatol. 1986;3(2):102-6. Berg RW, Milligan MC, Sarbaugh FC. Association of skin wetness and pH with diaper dermatitis. Pediatr. Dermatol. 1994;11(1):18-20. Buckingham KW, Berg RW. Etiologic factors in diaper dermatitis: the role of feces. Pediatr. Dermatol. 1986;3(2):107-12. Zimmerer RE, Lawson KD, Calvert CJ. The effects of wearing diapers on skin. Pediatr. Dermatol. 1986;3(2):95-101. Wolf R, Wolf D, Tuzun B, Tuzun Y. Diaper dermatitis. Clin. Dermatol. 2000;18(6):657-60.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Keeping Infant Skin Healthy through Proper Cleansing
23
[49] Brook I. Microbiology of secondarily infected diaper dermatitis. Int. J. Dermatol. 1992;31(10):700-2. [50] Geigy Scientific Tables: Units of Measurement, Body Fluids, Composition of the Body, Nutrition v. 1. 8th ed: Novartis (formerly Ciba Geigy); 1981. [51] Blume-Peytavi U, Cork MJ, Faergemann J, Szczapa J, Vanaclocha F, Gelmetti C. Bathing and cleansing in newborns from day 1 to first year of life: recommendations from a European round table meeting. J. Eur. Acad Dermatol. Venereol. 2009;23(7):751-9. [52] Adalat S, Wall D, Goodyear H. Diaper dermatitis-frequency and contributory factors in hospital attending children. Pediatr. Dermatol. 2007;24(5):483-8. [53] Lund CH, Kuller J, Raines DA, Ecklund S, Archambault ME, O'Flaherty P. Neonatal skin care - Evidence-based clinical practice guideline. Second ed. Washington: Association of Women's Health, Obstetric and Neonatal Nurses and the National Association of Neonatal Nurses; 2007. [54] Garcia Bartels N, Mleczko A, Schink T, Proquitte H, Wauer RR, BlumePeytavi U. Influence of bathing or washing on skin barrier function in newborns during the first four weeks of life. Skin Pharmacol. Physiol. 2009;22(5):248-57. [55] Visscher M, Odio M, Taylor T, White T, Sargent S, Sluder L, et al. Skin care in the NICU patient: effects of wipes versus cloth and water on stratum corneum integrity. Neonatology. 2009;96(4):226-34. [56] Shin HT. Diaper dermatitis that does not quit. Dermatol. Ther. 2005;18(2):124-35. [57] Atherton D, Mills K. What can be done to keep babies' skin healthy? RCM Midwives. 2004;7(7):288-90. [58] Gupta AK, Skinner AR. Management of diaper dermatitis. Int. J. Dermatol. 2004;43(11):830-4. [59] Fisher AA. Contact Dermatitis. 3rd ed. Philadelphia: Lea and Febiger; 1986. [60] Begg EJ, Duffull SB, Hackett LP, Ilett KF. Studying drugs in human milk: time to unify the approach. J. Hum. Lact. 2002;18(4):323-32. [61] Parvinen T, Larmas M. Age dependency of stimulated salivary flow rate, pH, and lactobacillus and yeast concentrations. J. Dent. Res. 1982 Sep;61(9):1052-5. [62] Laughter D, Istvan JA, Tofte SJ, Hanifin JM. The prevalence of atopic dermatitis in Oregon schoolchildren. J. Am. Acad. Dermatol. 2000;43(4):649-55.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
24
Georgios N. Stamatas, Russel M. Walters and Lorena S. Telofski
[63] Schultz Larsen F, Diepgen T, Svensson A. The occurrence of atopic dermatitis in north Europe: an international questionnaire study. J. Am. Acad. Dermatol. 1996;34(5 Pt 1):760-4. [64] Krakowski AC, Eichenfield LF, Dohil MA. Management of atopic dermatitis in the pediatric population. Pediatrics. 2008;122(4):812-24. [65] Cork MJ, Danby SG, Vasilopoulos Y, Hadgraft J, Lane ME, Moustafa M, et al. Epidermal barrier dysfunction in atopic dermatitis. J. Invest. Dermatol. 2009;129(8):1892-908. [66] Sugarman JL. The epidermal barrier in atopic dermatitis. Semin. Cutan. Med. Surg. 2008;27(2):108-14. [67] Spergel JM, Paller AS. Atopic dermatitis and the atopic march. J. Allergy Clin. Immunol. 2003;112(6 Suppl):S118-27. [68] Eichenfield LF, Hanifin JM, Luger TA, Stevens SR, Pride HB. Consensus conference on pediatric atopic dermatitis. J. Am. Acad. Dermatol. 2003;49(6):1088-95. [69] Dohil MA, Eichenfield LF. A treatment approach for atopic dermatitis. Pediatr. Ann. 2005;34(3):201-10. [70] Cheong WK. Gentle Cleansing and Moisturizing for Patients with Atopic Dermatitis and Sensitive Skin. American Journal of Clinical Dermatology. 2009;10(5):13-7. [71] Steigleder GK, Maibach HI. Pocket atlas of dermatology. 2nd ed. Stuttgart: Thieme; 1993. [72] Janniger CK. Infantile seborrheic dermatitis: an approach to cradle cap. Cutis. 1993;51(4):233-5. [73] Cohen BA. Pediatric Dermatology. 2nd ed. London, Philadelphia, St Louis, Sydney, Tokyo: Mosby; 1999. [74] Schachner LA, Hansen RC, editors. Pediatric Dermatology. 2nd ed. New York: Churchill Livingstone; 1995. [75] Hurwitz S. Clinical Pediatric Dermatology - A textbook of Skin Disorders of Childhood and Adolescence. 2nd ed. Philadelphia: Saunders; 1993. [76] Henderson C, Taylor J, Cunliffe W. Sebum excretion rates in mothers and neonates. British Journal of Dermatology. 2000;142(1):110-1. [77] Ruiz-Maldonado R, Lopez-Matinez R, Perez Chavarria EL, Rocio Castanon L, Tamayo L. Pityrosporum ovale in infantile seborrheic dermatitis. Pediatr. Dermatol. 1989 Mar;6(1):16-20. [78] Sarkar R, Basu S, Agrawal RK, Gupta P. Skin care for the newborn. Indian Pediatr. 2010;47(7):593-8.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Keeping Infant Skin Healthy through Proper Cleansing
25
[79] Toker E, Yenice O, Ogut MS, Akman I, Ozek E. Tear production during the neonatal period. Am. J. Ophthalmol. 2002;133(6):746-9. [80] Isenberg SJ, Del Signore M, Chen A, Wei J, Guillon JP. The lipid layer and stability of the preocular tear film in newborns and infants. Ophthalmology. 2003;110(7):1408-11. [81] Dahl H, Dahl C. Hydrogen ion concentration of tear fluid in newborn infants. Acta Ophthalmol. (Copenh). 1985;63(6):692-4. [82] Lavezzo MM, Schellini SA, Padovani CR, Hirai FE. Eye blink in newborn and preschool-age children. Acta Ophthalmol. 2008;86(3):2758. [83] Lawrenson JG, Birhah R, Murphy PJ. Tear-film lipid layer morphology and corneal sensation in the development of blinking in neonates and infants. J. Anat. 2005;206(3):265-70. [84] Kayed NS, Farstad H, van der Meer AL. Preterm infants' timing strategies to optical collisions. Early Hum. Dev. 2008;84(6):381-8. [85] Janniger CK, Schwartz RA, Szepietowski JC, Reich A. Intertrigo and common secondary skin infections. Am. Fam. Physician. 2005; 72 (5): 833-8. [86] Neville JA, Yosipovitch G. Intertrigo. In: Arndt KA, Hsu JTS, editors. Manual of dermatologic therapeutics. 7th ed. Philadelphia: Lipponcott Williams and Wilkins; 2007. p. 137-8. [87] Ananthapadmanabhan KP, Moore DJ, Subramanyan K, Misra M, Meyer F. Cleansing without compromise: the impact of cleansers on the skin barrier and the technology of mild cleansing. Dermatol. Ther. 2004;17 Suppl 1:16-25. [88] Gallagher M, Wysocki CJ, Leyden JJ, Spielman AI, Sun X, Preti G. Analyses of volatile organic compounds from human skin. Br. J. Dermatol. 2008;159(4):780-91. [89] Hasenoehrl E. Facial Cleansers and Cleansing Cloths: Wiley-Blackwell; 2010. [90] Gelmetti C. Skin cleansing in children. J. Eur. Acad. Dermatol. Venereol. 2001;15 Suppl 1:12-5. [91] Kuehl BL, Fyfe KS, Shear NH. Cutaneous cleansers. Skin Therapy Lett. 2003;8(3):1-4. [92] Draelos ZD. Skin and hair cleansers. 2009 [Accessed on 22/09/2010]; Available from: http://emedicine.medscape.com. [93] Vincent C, Yang L, Hua X, Ananthapadmanabhan K, Lips A, Deo N, et al. Role of Surfactant Micelle Charge in Protein Denaturation and
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
26
Georgios N. Stamatas, Russel M. Walters and Lorena S. Telofski
Surfactant-Induced Skin Irritation. Surfactants in Personal Care Products and Decorative Cosmetics, Third Edition: CRC Press; 2006. p. 177-87. [94] Walters RM, Fevola MJ, Librizzi JJ, Martin K. Designing cleansers for the unique needs of baby skin. Cosm. toil. 2008;123(12):53-60. [95] Blake-Haskins JC, Scala D, Rhein LD, Robbins CR. Predicting surfactant irritation from the swelling response of a collagen film. Journal of the Society of Cosmetic Chemists. 1986;37(4):199-210. [96] Imokawa G. Surfactant mildness. In: Rieger MM, Rhein LD, editors. Surfactants in Cosmetics; Surfactant Science Series. New York: Marcel Dekker; 1997. p. 427-71. [97] Ananthapadmanabhan KP, Lips A, Vincent C, Meyer F, Caso S, Johnson A, et al. pH-induced alterations in stratum corneum properties. Int. J. Cosmet. Sci. 2003;25(3):103-12. [98] Rhein LD. In vitro interactions. Biochemical and biophysical efects of surfactants on skin. In: Rieger MM, Rhein LD, editors. Surfactants in Cosmetics; Surfactant Science Series. New York: Marcel Dekker; 1997. p. 397-426. [99] Braun-Falco O, Korting HC. [Normal pH value of human skin]. Hautarzt. 1986;37(3):126-9. [100] Fluhr JW, Pfisterer S, Gloor M. Direct comparison of skin physiology in children and adults with bioengineering methods. Pediatr. Dermatol. 2000;17(6):436-9. [101] Gfatter R, Hackl P, Braun F. Effects of soap and detergents on skin surface pH, stratum corneum hydration and fat content in infants. Dermatology. 1997;195(3):258-62. [102] Strube DD, Koontz SW, Murahata RI, Theiler RF. The flex wash test: a method for evaluating the mildness of personal washing products. J. Soc. Cosmet. Chem. 1989;40:297-306. [103] Lukacovic MF, Dunlap FE, Michaels SE, Visscher MO, Watson DD. Forearm wash test to evaluate the clinical mildness of cleansing products. J. Soc. Cosmet. Chem. 1988;39:355-66. [104] Visscher MO. Update on the Use of Topical Agents in Neonates. 2009;9(1):31-47. [105] Abbas S, Goldberg JW, Massaro M. Personal cleanser technology and clinical performance. Dermatologic Therapy. 2004;17:35-42. [106] Walters RM, Fevola MJ, Librizzi JJ, Martin K. Designing cleansers for the unique needs of baby skin. Anglais. 2008;123(12):53-60.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Keeping Infant Skin Healthy through Proper Cleansing
27
[107] Maltesh C, Somasundaran P. Effect of binding of cations to polyethylene glycol on its interactions with sodium dodecyl sulfate. Langmuir. 1992;8(8):1926-30. [108] Discher DE, Ahmed F. Polymersomes. Annu. Rev. Biomed. Eng. 2006;8:323-41. [109] Moore PN, Puvvada S, Blankschtein D. Challenging the surfactant monomer skin penetration model: penetration of sodium dodecyl sulfate micelles into the epidermis. J. Cosmet. Sci. 2003;54(1):29-46. [110] Hudson CN. HIV infection in pregnancy; the position in the United Kingdom and Europe. Aust. N. Z. J. Obstet. Gynaecol. 1992;32(2):91-4. [111] Darmstadt GL, Dinulos JG. Neonatal skin care. Pediatric Clinics of North America. 2000;47(4):757-82. [112] Varda KE, Behnke RS. The effect of timing of initial bath on newborn's temperature. J. Obstet. Gynecol. Neonatal. Nurs. 2000;29(1):27-32. [113] Hylen AM, Karlsson E, Svanberg L, Walder M. Hygiene for the newborn--to bath or to wash? J. Hyg. (Lond). 1983;91(3):529-34. [114] Garcia Bartels N, Scheufele R, Prosch F, Schink T, Proquitte H, Wauer RR, et al. Effect of standardized skin care regimens on neonatal skin barrier function in different body areas. Pediatr. Dermatol. 2010;27 (1):1-8. [115] Dizon MV, Galzote C, Estanislao R, Mathew N, Sarkar R. Tolerance of Baby Cleansers in Infants: A Randomized Controlled Trial. Indian Pediatr. 2010 [Epublished ahead of print]. [116] Visscher MO, Chatterjee R, Ebel JP, LaRuffa AA, Hoath SB. Biomedical assessment and instrumental evaluation of healthy infant skin. Pediatr. Dermatol. 2002;19(6):473-81. [117] Warren R, Ertel KD, Bartolo RG, Levine MJ, Bryant PB, Wong LF. The influence of hard water (calcium) and surfactants on irritant contact dermatitis. Contact Dermatitis. 1996;35(6):337-43. [118] Medves JM, O'Brien B. Does bathing newborns remove potentially harmful pathogens from the skin? Birth. 2001;28(3):161-5. [119] Yoshio H, Tollin M, Gudmundsson GH, Lagercrantz H, Jornvall H, Marchini G, et al. Antimicrobial polypeptides of human vernix caseosa and amniotic fluid: implications for newborn innate defense. Pediatr. Res. 2003;53(2):211-6. [120] Lund C, Kuller J, Lane A, Lott JW, Raines DA. Neonatal skin care: the scientific basis for practice. J. Obstet. Gynecol. Neonatal. Nurs. 1999;28(3):241-54.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
28
Georgios N. Stamatas, Russel M. Walters and Lorena S. Telofski
[121] Lund CH, Kuller J, Lane AT, Lott JW, Raines DA, Thomas KK. Neonatal skin care: evaluation of the AWHONN/NANN research-based practice project on knowledge and skin care practices. Association of Women's Health, Obstetric and Neonatal Nurses/National Association of Neonatal Nurses. J. Obstet. Gynecol. Neonatal. Nurs. 2001;30(1):30-40. [122] Lund CH, Osborne JW, Kuller J, Lane AT, Lott JW, Raines DA. Neonatal skin care: clinical outcomes of the AWHONN/NANN evidence-based clinical practice guideline. Association of Women's Health, Obstetric and Neonatal Nurses and the National Association of Neonatal Nurses. J. Obstet. Gynecol. Neonatal. Nurs. 2001;30(1):41-51. [123] Behring A, Vezeau TM, Fink R. Timing of the newborn first bath: a replication. Neonatal. Netw. 2003;22(1):39-46. [124] Penny-MacGillivray T. A newborn's first bath: when? J. Obstet. Gynecol. Neonatal. Nurs. 1996;25(6):481-7. [125] Henningsson A, Nystrom B, Tunnell R. Bathing or washing babies after birth? Lancet. 1981;2(8260-61):1401-3. [126] Anderson GC, Lane AE, Chang HP. Axillary temperature in transitional newborn infants before and after tub bath. Appl. Nurs. Res. 1995;8(3):123-8. [127] Shoaeib FM, All SA, El-Barrawy MA. Alcohol or traditional methods versus natural drying for newborn's cord care. J. Egypt Public Health Assoc. 2005;80(1-2):169-201. [128] Galzote C, Dizon MV, Estanislao R, Mathew N. Opportunities for mild and effective infant cleansing beyond water alone. J. Am. Acad. Dermatol. 2007;56(2):AB158. [129] Hoath SB, Pickens WL, Visscher MO. The biology of vernix caseosa. Int. J. Cosmet Sci. 2006;28(5):319-33. [130] Larson AA, Dinulos JG. Cutaneous bacterial infections in the newborn. Curr. Opin. Pediatr. 2005;17(4):481-5. [131] Tollin M, Bergsson G, Kai-Larsen Y, Lengqvist J, Sjovall J, Griffiths W, et al. Vernix caseosa as a multi-component defence system based on polypeptides, lipids and their interactions. Cell Mol. Life Sci. 2005;62(19-20):2390-9. [132] Akinbi HT, Narendran V, Pass AK, Markart P, Hoath SB. Host defense proteins in vernix caseosa and amniotic fluid. Am. J. Obstet. Gynecol. 2004;191(6):2090-6. [133] Haubrich KA. Role of Vernix caseosa in the neonate: potential application in the adult population. AACN Clin Issues. 2003 Nov;14(4): 457-64.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Keeping Infant Skin Healthy through Proper Cleansing
29
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
[134] Bautista MI, Wickett RR, Visscher MO, Pickens WL, Hoath SB. Characterization of vernix caseosa as a natural biofilm: comparison to standard oil-based ointments. Pediatr. Dermatol. 2000;17(4):253-60. [135] Youssef W, Wickett RR, Hoath SB. Surface free energy characterization of vernix caseosa. Potential role in waterproofing the newborn infant. Skin Res. Technol. 2001;7(1):10-7. [136] Visscher MO, Narendran V, Pickens WL, LaRuffa AA, Meinzen-Derr J, Allen K, et al. Vernix caseosa in neonatal adaptation. J. Perinatol. 2005;25(7):440-6. [137] Hoath SB, Maibach H, editors. Neonatal Skin - Structure and Function. New York: Marcel Dekker; 2003.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved. Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
In: Skin Care Editor: Sandra M. Hayes, pp. 31-58
ISBN 978-1-61209-568-4 © 2011 Nova Science Publishers, Inc.
Chapter II
Novel Approaches for Wound Repair Therapies Gerd G. Gauglitz1 and Marc G. Jeschke∗2
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Sunnybrook Health Sciences Centre, Department of Surgery, Division of Plastic Surgery, University of Toronto, Canada, and others
Abstract Treatment of non-healing wounds has remained difficult, in spite of better understanding of pathophysiologic principles. Gene therapy, initially developed for treatment of congenital defects, represents a novel option for enhancing wound repair. In order to accelerate wound closure, genes encoding for growth factors or cytokines have showed most potential. The majority of gene delivery systems are based on viral transfection, naked DNA application, high pressure injection, and liposomal vectors. Besides advances stemming from breakthroughs in recombinant growth factors and bioengineered skin, early data suggest the use of multipotent stem cells in order to accelerate wound healing. ∗
1 2
Corresponding author: Marc G Jeschke, MD PhD. Sunnybrook Health Sciences Centre, Department of Surgery, Division of Plastic Surgery University of Toronto. Rm D704, 2075 Bayview Ave. Toronto, ON CANADA M4N 3M5. Tel: 416-480-6703. Fax: 416-480-6763. Email: [email protected]. Sunnybrook Health Sciences Centre, Department of Surgery, Division of Plastic Surgery University of Toronto, Canada Department of Dermatology and Allergology, Ludwig Maximilians University, Munich, Germany
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
32
Gerd G. Gauglitz and Marc G. Jeschke Cutaneous wound healing requires a well-orchestrated integration of the complex biological and molecular events of cell migration and proliferation, as well as extracellular matrix deposition, angiogenesis, and remodeling. Stem cells, due to their ability to differentiate into various tissue types by asymmetric replication thus represent a promising tissue repair strategy. A variety of sources, such as bone marrow, peripheral blood, umbilical cord blood, adipose tissue and skin/ hair follicles, have been utilized to isolate stem cells to modulate the healing response of acute and chronic wounds. Recent data have demonstrated the feasibility of autologous ASC therapy in cutaneous repair and regeneration. Very recently, the combination of gene and stem cell therapy has emerged and could provide a promising approach for future treatment of chronic and acute wounds. The aim of this review is to discuss the use and the potential of these novel technologies in order to improve wound healing capacities.
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Keywords: stem cells, adult, embryonic, wound healing, umbilical cord, gene therapy.
Abbreviations ADSCs HSCs ES cells AS cells MSC BM MEFs IPS FGF VEGF HDF PDGF IGF KGF TGF HFs CXCL5
adipose-derived stem cells hematopoietic stem cell Embryonic stem cells Adult stem cells mesenchymal stem cells bone marrow mouse embryonic fibroblasts induced pluripotent state Fibroblast Growth Factor Vascular Endothelial Growth Factor human dermal fibroblasts Platelet Derived Growth Factor Insulin-like Growth Factor Keratinocyte Growth Factor Transforming Growth Factor Hair Follicles C-X-C motif chemokine 5
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Novel Approaches for Wound Repair Therapies
33
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Introduction World-wide millions of patients suffer from acute and chronic wounds due to infections, trauma, or underlying medical conditions thus cutaneous wounds represent a major health care issue and socioeconomic problem. Appropriate wound care is critical, and various treatment modalities have been used to improve the wound bed. The overall therapy for non-healing wounds has largely focused on the identification and correction of the precipitating and perpetuating factors. This approach includes antibiotic use for accompanying cellulitis, revascularization of ischemic limbs, rigorous off-loading for decubitus (pressure) ulcers and compression devices for venous ulcers. Besides well known components of wound care including debridement of the necrotic tissue, removal of edema fluid, decreasing the bacterial burden, and providing the right balance of moisture to the wound bed, more advanced therapeutic approaches, such as topically applied growth factors and cell-based therapies have been developed in recent years. Some of these treatment modalities are either in the development phase, available as off-label use or actually approved by the Food and Drug Administration for specific indications (Table 1). Table 1. Skin Substitutes [41]. Biobrane Epicel AlloDerm Integra Artificial Skin Oasis TranCyte Dermagraft
Orcel Apligraf
Bertek Pharmaceuticals; Morgantown, WV Genzyme; Cambridge, MA LifeCell Corporation in Palo Alto, CA Integra Lifesciences; Plainsboro, NJ Cook Biotech, Inc. West Lafayette, IN Advanced Tissue Sciences; La Jolla, CA Smith and Nephew, La Jolla, CA Ortec International, Inc. New York, NY Novartis; East Hanover, NJ
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
acellular dressing, collagen bound to nylon fabric autologous epidermal graft accellular, allogeneic dermal graft bovine collagen and chondroitin-6-sulfate pig intestinal mucosa devitalized fibroblasts on nylon mesh Human fibroblasts in an absorbable matrix (approved in UnitedStates for diabetic ulcers) Human fibroblasts and keratinocytes in a bovine collagen sponge human fibroblasts and keratinocytes in a bovine collagen matrix (approved in United States for venous and diabetic ulcers)
34
Gerd G. Gauglitz and Marc G. Jeschke
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Figure 1. Summary of current skin substitutes available for wound coverage.
Platelet-derived growth factor–BB has been approved for the treatment of diabetic neuropathic ulcers of the foot. As for bioengineered skin, a bilayered living skin construct has been approved for venous and diabetic ulcers. A living dermal skin equivalent was also approved for diabetic neuropathic ulcers. Thus, in the last 10 years or so, tremendous progress has been made in chronic wounds, where the mainstay of treatment has largely relied on improvements in dressings and compression bandages. In addition to standard and more advanced treatments, other less commonly used and unusual therapeutic products, not necessarily new, are being used by some clinicians. For example, cadaver skin, serves frequently as skin substitute in severely burned patients. While this approach is still commonly used in burn centers throughout the world, it bears considerable risks, including antigenicity, crossinfection as well as limited availability [1]. Xenografts have been used for hundreds of years as temporary replacement for skin loss. Even though these grafts provide a biologically active dermal matrix, the immunologic disparities prevent engraftment and predetermine rejection over time [2]. However, both xenografts and allografts are only a mean of temporary burn wound cover. True closure can only be achieved with living autografts or isografts. Autologous epithelial cells grown from a single full-thickness skin biopsy have been available for nearly two decades. These cultured epithelial autografts (CEA) have shown to decrease mortality in massively burned patients in a prospective, controlled trial [3]. Our institution found CEA utilized in combination with wide mesh autograft and allograft overlay in a pediatric patient population with burns of ≥ 90% TBSA to be associated with
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Novel Approaches for Wound Repair Therapies
35
improved cosmetic results [4]. However, widespread use of cultured autografts has been primarily hampered by poor long term clinical results, exorbitant costs and fragility and difficult handling of these grafts, that have been consistently reported by different burn units treating deep burns, even when cells were applied on properly prepared wound beds [2, 5, 6]. Alternatively, dermal analogs have been made available for clinical use in recent years. Integra™ was approved by the United States Food and Drug administration for use in life-threatening burns and has been successfully utilized in immediate and delayed closure of full-thickness burns, leading to reduction in length of hospital stay, favorable cosmetics, and improved functional outcome in a prospective and controlled clinical study [7-10]. Our group recently conducted a randomized clinical trial utilizing IntegraTM in the management of severe full-thickness burns of ≥ 50% TBSA in a pediatric patient population comparing it to standard autograft-allograft technique, and found Integra™ to be associated with attenuated hepatic dysfunction, improved resting energy expenditure and improved aesthetic outcome post-burn [11]. AllodermTM, an acellular human dermal allograft, has been advocated for the management of acute burns. Small clinical series and case reports suggest that AllodermTM may be useful in the treatment of acute burns [12-15]. Tissue engineering technology is advancing rapidly. Fetal constructs have recently been successfully trialed by Hohlfeld and colleagues [16] and the bilaminar skin substitute of Boyce [17] is now routine in clinical use and promise spectacular results [18]. However, all currently available examples of artificial dermis lack a vascular plexus for the nourishment of the epidermis and require host vasculogenesis into the dermis graft to supply nourishment to the grafted epidermis. Recent artificial dermal substitutes are structurally optimized to incorporate the surrounding tissue and to allow cell invasion by fibroblasts and capillaries for subsequent dermal remodeling [19]. Although topically applied platelet-derived growth factor– BB remains the only recombinant growth factor approved for wound healing in the United States, there are several reports that other cytokines or growth factors are critical to wound healing [20, 21]. These growth factors play major roles in local inflammation, reepithelialization, granulation tissue formation, neovascularization, and extracellular matrix production from various cell sources and through diverse mechanisms [21]. There have been extensive investigations into wound healing by the exogenous application of various growth factors [22]. Transient gene therapy is of particular interest in this context delivering the respective growth factor. Presently, several technologies are under active development to
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
36
Gerd G. Gauglitz and Marc G. Jeschke
aid cutaneous wound repair [23] since it is becoming increasingly clear, that more radical steps need to be taken to enhance and accelerate the treatment of chronic and burn wounds in a direction that allows greater effectiveness.
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Gene Therapy Gene therapy, defined as the insertion of a gene into recipient cells, was initially considered only as a treatment option for patients with a congenital defect of a metabolic function or a late-stage malignancy [24]. More recently, skin has become an important target of gene therapy research, based on the ease of fibroblast and keratinocyte harvest and in vitro cultivation, allowing for gene transfer testing in vitro and for the use of skin cells as vehicles in gene transfer [25]. Skin is also easily accessible and the effects of therapy can be repeatedly monitored. Two basic strategies for introduction and expression of foreign DNA into host cells are 1) gene therapy, which is based on the permanent insertion of DNA, and 2) gene medicine, which is used for transient transformation and short-term expression of a gene product [25]. Furthermore, genes can be delivered by either in vivo and ex vivo or approaches. In vivo techniques are based upon the direct introduction of genes to the target tissue. Ex vivo techniques rely upon the isolation and cultivation of selected cells with their transfection in vitro and a subsequent transplantation to a host. In both approaches, the selection of an appropriate vector for the introduction of genes is paramount for success [26]. Gene transfer with viral vectors relies on the ability of viruses to carry and express their genes into host cells. Viral vectors are the original and most established technology for gene delivery. A wide range of applications has been developed and many virus-mediated gene transfer models work successfully. However, the production of viral vectors is time and cost consuming, transfection efficacy is very variable, and the risk of local or systemic infections, leading to fatal outcomes, remains a large concern. Nonviral gene therapy in contrast has the advantage that gene transfer is performed without a viral vector, which eliminates the risk of infection and cost of vector production [27]. The transient nature of gene expression is of advantage in wound healing applications. Especially the use of CL appears to be safe, efficacious, and clinically applicable. On the negative side, some non-viral gene transfer methods tend to be non-specific, and a high variability in the level of gene expression has been reported.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Novel Approaches for Wound Repair Therapies
37
A potential problem of single growth factor gene therapy is that increasing the concentration of a single growth factor may not promote all phases of wound healing. A single growth factor cannot counteract all the deficiencies of a burn wound, nor can it control the complexities of chronic wound healing. Lynch et al. [28] demonstrated that the combination of PDGF and IGF-I was more effective than either growth factor alone in a partial thickness wound healing model created with the use of a dermatome. Sprugel et al. [26] found that a combination of PDGF and FGF-2 increased the DNA content of wounds in the rat better than any single growth factor. Our group subsequently investigated the feasibility of multiple cDNA constructs, using multiple genes (KGF and IGF-I cDNA) and compared it to the administration of the same genes individually [29]. Accelerated re-epithelization, increased proliferation, and decreased skin cell apoptosis were noted. The re-epithelialization in the burn model was over twice that of the untreated control with a significant improvement in cell survival [29]. Transfection of multiple growth factor genes at strategic time points of wound healing (known as sequential growth factor therapy) is therefore the next logical step in augmenting wound healing. Other delivery routes such as biomaterials [30], calcium phosphate transfection [31], diethylaminoethyl-dextran [32], and microbubble-enhanced ultrasound [33] have been investigated. Slow-release matrices [34] and genedelivering gel/matrix products [35] allow for prolonged transgenic expression. The concept of a genetic switch is another exciting development, where transgenic expression in target cells can be switched ‘on’ or ‘off’, depending on the presence of or absence of a stimulator such as tetracycline [36]. Biotechnological refinements, such as wound chamber technique [37], may also improve the efficacy of gene delivery to wounds. These new techniques show promise, but need further studies to define the efficacy and clinical applicability. More studies are also needed to define growth factor levels in different phases of wound healing and to elucidate the precise timing of gene expression or down-regulation required to better augment wound healing and control of scar formation.
Stem Cells Stem cells, defined based on the findings of Ernest A. McCulloch and James E. Till [38, 39], are characterized by 1) a prolonged self renewal capacity and 2) the ability to differentiate into mature stages and different tissue types by asymmetric replication [40, 41]. These properties have led to
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
38
Gerd G. Gauglitz and Marc G. Jeschke
the expectation that human embryonic stem cells can be useful in understanding disease mechanisms, the development of effective drugs, and the treatment of patients with various diseases and injuries [42, 43]. Despite their unique potential, the use of embryonic stem cells has remained controversial. Ethical concerns regarding the use of human embryos for the purpose of obtaining their cells have been raised by both the scientific community and public media. Even though there are new studies suggesting that embryonic stem cells may be obtained without destroying the embryo [44], it remains unclear whether this approach would eliminate the ethical concerns. To circumvent these issues, Yamanaka et al. [45] produced pluripotent somatic cells by direct reprogramming, and generated pluripotent stem cells from adult human dermal fibroblasts and other human somatic cells, which were comparable to the differentiation potential of human embryonic stem cells [46]. In addition, differentiated adult tissues have been shown to harbor pluripotent stem cells with unexpected plasticity [42]. Thus, stem cells derived from adult sources may have the same clinical and experimental potential as embryonic stem cells. The opportunity to repair and regenerate tissues injured by disease and trauma is opening the way to new optimistic treatments that need to be carefully evaluated in early clinical trials. These developments are building on the successes of bone marrow hematopoietic stem cell (HSCs) transplants that have more than 30 years of patient applications in blood diseases and cancer. This chapter is focusing on presently discussed sources of stem cells, their possible mechanism of action and their clinical applicability particularly for the healing of acute and chronic cutaneous wounds.
Embryonic Stem (ES) Cells ES cells are pluripotent stem cells that are harvested from the inner cell mass of the pre-implantation blastocyst (3–5-days-old embryo), and have been obtained from mice, non-human primates, and humans [47, 48]. ES cells have had an enormous impact on biology and medicine. ES cells can be maintained in culture as undifferentiated cell lines or induced to differentiate into many different lineages, including blood cells, neural cells, adipocytes, muscle cells, and chondrocytes, among others [42, 49]. The ability of researchers to efficiently manipulate ES cells to differentiate into specifically directed cells will provide means of an unlimited supply of cells that may be used, not only for the growth of implantable tissues, but also for testing new drugs to cure
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Novel Approaches for Wound Repair Therapies
39
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
diseases, and in the identification of potentially problematic genes [48, 50-52]. Thus, ES cells have had and will have an enormous impact on biology and medicine. However, in spite of their tremendous potential, ES cells are the subject of considerable controversy. Opponents of ES cell use most often question the morality of using cells obtained from destroyed embryos, an act they consider equivalent to destroying human life [53]. They fear the possibility that the use of human ES cells could lead to the almost industrial production of human embryos for the sole purpose of obtaining their cells. Current research has been directed towards developing methods that will permit the use of ES cells while eliminating the ethical concerns surrounding their use. Methods to produce human ES cells without destroying embryos were proposed in the President’s Council on Bioethics report in 2004 [54]. Two of these methods were further investigated in individual proof of concept studies [44, 55] which gleaned promising results. Questions, however, still point to the ethical use of these methods for many involved in these debates [56]. The use of stem cells derived from adult tissues, and not those derived from embryonic tissues, avoids many of the ethical concerns that may arise from the use of stem cells in research applications.
Adult Stem (AS) Cells Ethical concerns regarding human ES cells and the human embryos involved together with the scientific as well as public discussion about efficiency and abuse of cloning technology in humans caused an intensive search for practical alternatives. In addition, recent studies challenged the belief that stem cells, which persist after early embryonic stages, are restricted in potential to form only the cell types characteristic of the tissue they belong to, and opened up the investigations on adult stem cells (AS) cells. AS cells, also referred to as somatic stem cells or mesenchymal stem cells (MSC), are those mature, adult cells that are undifferentiated and found in a specific tissue or organ [57]. These cells are self-renewing, and are able to differentiate into major specialized cell types that serve to maintain the integrity of and repair the tissues in which they are found [47, 57]. For example, only a very small proportion (1 in 15,000 cells) in the bone marrow are haematopoietic stem cells (HSCs), which are constantly generated in adult individuals, but when dispersed in tissues they differentiate into the various mature blood cell types depending on the local environment [40]. In addition to the capability of self-renewal throughout the entire lifetime of an organism, AS cells are
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
40
Gerd G. Gauglitz and Marc G. Jeschke
characterized by being clonogenic (a single adult stem cell should be able to generate a line of genetically identical cells) and being able to differentiate into cells with a mature phenotype regarding morphology, specific cell surface markers, and characteristic behavior [58]. Unlike ES cells, which are defined by their origin from the ICM of blastocysts, AS cells do not have such a definitive basis and are likely characterized by being set aside during fetal development and restrained from differentiation. AS stem cells are often determined by labeling and tracking in vivo after re-transplantation or, when grown in vitro, they can be manipulated by adding growth factors or introducing genes to determine what differentiated cell types they will yield. It is often difficult to distinguish adult, tissue specific stem cells from progenitor cells, which are found in fetal and adult tissues and are partly differentiated to give rise to certain cell types of a tissue [58]. Besides the bone marrow (BM), other adult tissues such as peripheral blood, brain, spinal cord, skeletal muscle, epithelia of the skin and digestive system, and pancreas contain stem cells. However, because of the ease with which they are obtained, human mesenchymal stem cells (hMSCs) derived from bone marrow have received considerable attention. Human umbilical cord blood has also been explored as an alternative source of stem cells to repopulate the bone marrow in the treatment of diseases in children and adults [59]. In addition, adipose tissue has been identified as a source of multipotent cells that have the capacity to differentiate to cells of adipogenic, chondrogenic, myogenic, and osteogenic lineages when cultured with the appropriate lineage specific stimuli [57, 60]. However, research on adult stem cells has been slow, largely because great difficulty has been encountered in maintaining adult non-mesenchymal stem cells in culture. There are challenges involved in maintaining and expanding long term cultures of adult stem cells in large numbers. Isolation has also proven to be quite problematic as these cells are present in extremely low numbers in the adult tissue. While current use of adult stem cells is still limited, there is great potential in future utilization of such cells for the use of tissue specific regenerative therapies. The advantage of adult stem cells is that they can be used in autologous therapies, thus avoiding any immune rejection complications. Recently, it became evident that stem cells from a particular tissue can also generate specialized cell types of another tissue, either derived from the same or from a different embryonic germ layer. This so-called plasticity [61] describes the ability of stem cells from one adult tissue to generate the differentiated cell types of another tissue and is also referred to as ‘transdifferentiation’ [62, 63]. Most experiments demonstrating somatic stem
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Novel Approaches for Wound Repair Therapies
41
cell plasticity involve cells derived from bone marrow, which may differentiate into another mesodermderived tissue such as skeletal muscle [64, 65], cardiac muscle [64, 65], or liver [66, 67]. While bone marrow-derived mesodermal stem cells were reported to generate ectoderm-originated neural tissue [68], neural stem cells from adult brain tissue were found to form haematopoietic cells [69]. Another area of current study is the production of pluripotent somatic cells by direct reprogramming. Reprogramming is a technique that involves dedifferentiation of adult somatic cells to produce patient-specific pluripotent stem cells without the use of embryos. Cells generated by reprogramming would be genetically identical to the somatic cells and would not be rejected by the donor. This method also avoids the technical limitations of nuclear transfer into oocytes. Takahashi and Yamanaka were the first to discover that mouse embryonic fibroblasts (MEFs) and adult mouse fibroblasts can be reprogrammed into an induced pluripotent state (IPS) [70]. In recent studies the authors demonstrated that reprogramming can be done with human cells [46].
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Bone Marrow Derived Stem Cells Bone marrow contains hematopoietic stem cells and it is also the most recognized source of mesenchymal stem cells. Stem cells obtained from bone marrow are found in the stroma of the marrow. These cells are multipotent, and are therefore able to differentiate into lineages of cells such as adipocytes, osteocytes, myocytes, tenocytes, and neural cells [57, 61, 71]. The ability of bone marrow–derived stem cells to contribute to a number of different tissues has been demonstrated in vitro and in vivo in animal models and, more recently, in human transplantation chimeras [72]. These cells are typically obtained from bone marrow aspirates from marrow transplant donors. When cultured in vitro, bone marrow stem cells exhibit a fibroblast-like morphology. Marrow stromal cells have been studied and, to date, certain cell surface markers have been identified that are useful in cell selection and determination of preparation of marrow stem cell populations [73]. In addition to their ability to differentiate into multiple cell lineages, the use of marrow stem cells is advantageous because they offer a source of cells that is isolated and expanded in vitro with relative ease. The number of cells may be significantly increased by subculturing a small sample of donor tissue [51, 73].
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
42
Gerd G. Gauglitz and Marc G. Jeschke
Bone marrow-derived cells, used to help heal chronic wounds, have been of particular interest. Fathke et al. [74] showed in the chimeric mouse model that distant bone marrow-derived cells may contribute to the reconstitution of the dermal fibroblast population in cutaneous wounds. Bone marrow stroma cells were further found to synthesize higher amounts of collagen, FGF, and VEGF, when compared to native dermal fibroblasts, indicating a potential use for accelerating wound healing [75]. Ichoka et al. [76] investigated the effect of a bone marrow impregnated collagen matrix on wound healing in a microcirculatory mouse model and observed significant increases in angiogenesis. Furthermore, patients with chronic leg ulcera treated with this method demonstrated successful wound closure. Falaga et al. [77] successfully utilized a fibrin polymer spray to apply cultured autologous mesenchymal stem cells obtained from bone marrow aspirates to wounds. The technique accelerated the rate of healing of acute and non-healing cutaneous wounds in both humans and mice. This approach may represent a feasible method for introducing cells into wounds. There are, however, some difficulties related to these techniques. Stem cells must be cultured in sufficient numbers for topical application and grow in the wound for a therapeutic response. Another limitation in severe burn trauma is that bone marrow suppression has been observed either as a result of silver sulphadiazine toxicity [78] or sepsis [79, 80]. Ultimately, the number of bone marrow mesenchymal stem cells significantly decrease with age [81].
Umbilical Cord Derived Stem Cells Human umbilical cord blood is a rich source of hemopoietic stem cells for clinical application [82, 83]. McGuckin et al. [84] proposed umbilical cord blood to be one of the largest untouched sources of stem cells with characteristic features such as naive immune status. However, the presence of mesenchymal stem cells in umbilical cord blood remains controversial. Studies by Erices et al. [85] showed that mesenchymal stem cells together with hematopoietic precursors are circulating in the blood of preterm fetuses, while Mareschi et al. [86] failed to isolate these cells in preterm umbilical cord blood. In contrast, Romanov et al. [87] found that cord vasculature contains a large amount of mesenchymal stem cell-like elements. These elements form colonies of fibroblastoid cells that were successfully expanded in culture.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Novel Approaches for Wound Repair Therapies
43
Figure 2. A shows the tissues used for SC isolation. Freshly isolated tissues were cut and cultured as described above, and approximately 10 to 14 days after starting the culture, we observed significant numbers of cells migrating from the explants. Figure 5B shows representative phase contrast images of the two types of cells isolated from the umbilical cord and amnion. The majority of cells are mesenchymal (fibroblastic, left), but we also observed small populations of epithelial-like cells (right). With permission from Kita et al. [44].
They suggested that the umbilical cord stroma could thus be utilized as an alternative source of mesenchymal stem cells for experimental and clinical investigation. A study by Kamolz et al. [88] indicated that stem cells from umbilical cord blood are able to differentiate into epithelial cells under in vitro conditions and suggested their use as a starting material for isolation and expansion of cells in large skin defects. It should be pointed out that umbilical cord blood–derived stem cells are usually obtained from allogenic sources, potentially leading to immunological rejection upon transplant or transfusion.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
44
Gerd G. Gauglitz and Marc G. Jeschke
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Phan and colleagues recently found the amniotic membrane of the umbilical cord to be an extremely rich source of stem cells for burns resurfacing (unpublished data). The isolated cells, termed “Cord Lining Stem Cells”, can be divided into subpopulations of epithelial cells (Cord Lining Epithelial Cells) [89] and mesenchymal cells (Cord Lining Mesenchymal Cells) (Figure 2). They express stem cell markers, such as Oct-4 and Nanog, and have been shown to form healthy colonies in culture. Our group has recently shown that the amniotic membrane is a source of mesenchymal stem cells that can differentiate into bone, cartilage, and fat (Figure 3, [44]).
Figure 3. Characteristics of mesenchymal stem cells. (A) Expression of CD73 (green) and CD105 (purple) analyzed by flow cytometry. (B) Differentiation of mesenchymal stem cells into osteogenic, adipogenic, and chondrogenic lineages. Undifferentiated cells or differentiated cells were stained with Alizarin Red S (osteogenic), Oil-Red O (adipogenic), or Safranin O (chondrogenic). Cell pellet after chondrogenic differentiation is shown in the red circle. Scale bars=100 µm (adipogenic and chondrogenic) and 200 µm (chondrogenic), respectively. (C) CFU-F assay. Left: no cells, Middle and right, dish #1 and 2. With permission from Kita et al. [44].
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Novel Approaches for Wound Repair Therapies
45
Both have been successfully utilized to treat partial thickness and full thickness burns as well as chronic diabetic wounds in an ongoing clinical case series (unpublished data). Growing these cells on specific scaffolds creates an accessible way of applying these cells to the wound. Immunological rejection of these cells has not been observed in ongoing trials.
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Adipose-Derived Stem Cells (ADSCs) In addition to bone marrow, adipose tissue has been identified as a source of multipotent cells which have characteristics similar to BM-MSCs [90] and have the capacity to differentiate to cells of adipogenic, chondrogenic, myogenic, and osteogenic lineages when cultured with the appropriate lineage specific stimuli [60, 91, 92]. ADSCs can be obtained from the processing of either liposuctioned or excised fat. Adipose tissue contains 100 to 1000 times more pluripotent cells on a percubic centimeter basis than bone marrow [93, 94]. ADSCs have surface markers and gene profiling similar to BM-MSCs [90]. Given their convenient isolation compared with BM-MSCs and extensive proliferative capacities ex vivo, ADSCs hold great promise for use in wound repair and regeneration. Kim et al. recently investigated the effect of ADSCs on human dermal fibroblasts (HDF), which play a well known key role in skin biology such as wound healing, scar and photoaging. Co-culture of ADSCs and HDFs increased collagen and fibronectin synthesis and proliferation and migration activity of HDFs. ADSCs produced various growth factors such as PDGF, insulin-like growth factor (IGF) and KGF in addition to the previously reported growth factors, such as bFGF, TGF-β, HGF, and VEGF. In an animal model, ADSCs significantly reduced the wound size and accelerated the reepithelialization from the edge, suggesting that ADSCs may be used for the treatment of photoaging and wound healing. Theoretically, the abundance of isolated stem and therapeutically active cells from adipose eliminates the requirement of cell expansion in tissue culture facilities as is required with bone marrow derived cells and makes these cells readily available to the clinician, at the bedside. Human liposuction aspirates was used by Huang et al. [95] to culture adipo-derived mesodermal stem cells and differentiate them into chondrogenic cells. A study by Kim et al. [90] indicated that adiposederived stem cells promoted human dermal fibroblast proliferation by direct cell-to-cell contact and by secretory induced paracrine activation which significantly accelerated the re-epithelialization of cutaneous wounds. ADSCs are limited, however, by several factors. First, ADSCs have not been classified
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
46
Gerd G. Gauglitz and Marc G. Jeschke
as immortal. ADSCs display obvious signs of ‘‘old age’’, thus limiting their capacity for subculturing. Additionally, adipose tissue is known to vary in metabolic activity and in its capacity for proliferation and differentiation, depending on the location of the tissue depot and the age and gender of the patient [96, 97].
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Cutaneous Stem Cells In mammals, the epidermis is a multilayered epithelium that is composed of hair follicles (HFs), sebaceous glands and interfollicular epidermis. The interfollicular epidermis, defined as the portion of the epidermis located between the orifices of hair follicles, regenerates throughout adult life in order to replace terminally differentiated cells that are continuously shed from the surface of the skin and also to renew the hair follicle [98]. The regeneration of the epidermis and the hair follicle is sustained by many different types of epidermal stem cell, which also participate in the repair of the skin after injuries. In addition to their self-renewing capacity and multipotency, these cells are quiescent with a low tendency to divide, but upon injury are characterized by an extensive and sustained self-renewal capacity [98]. Recent advances in methods in isolating cutaneous stem cells have lead to a greater understanding of the potential use for these cells. Hair follicles with their ability for self-renewal represent currently the most promising source of multipotent stem cells [99]. Using transplantation of the murine bulge region, Oshima et al. (100) demonstrated that bulge cells could repopulate the epidermis, sebaceous glands, and the epithelial layers of the hair follicle. Roh et al. [99] showed that stem cells extracted from the human bulge region can be induced to exhibit hair follicle differentiation and form epidermal and sebaceous cells in vitro as well as form an epidermis and sebaceous cells in vitro, and this supports the multi-potential capacity of human cutaneous stem cells. In addition, cells from the hair follicle are currently used clinically to generate epithelium used for chronic wound coverage. The above evidence has overwhelmingly demonstrated that the cells located in the hair follicle bulge region represent multi-potent, tissue-specific epithelial stem cells. Most authors agree that these stem cells will become an important source for therapeutic applications, which is based on their accessibility and the easy access to skin.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Novel Approaches for Wound Repair Therapies
47
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Clinical Applications of Stem Cells to Wound Healing One of the first clinical uses of adult stem cells was the treatment of blood cancers such as leukaemia, which results from the uncontrolled proliferation of white blood cells using HSCs. In these applications, cancerous haematopoietic cells destroyed via radiation are replaced by a bone marrow transplant or a HSC transplant collected from the peripheral circulation of a matched donor. Autologous stem cell transplants collected from the peripheral blood of the patient are also used to replace haematopoietic cells destroyed by chemotherapy. As excellently summarized in a recent review by Lau and colleagues [101], encouraging results from stem cell-based treatment strategies in post-infarction myocardial repair [102] have led to application of similar strategies in order to treat skin wounds, where positive effects on all phases of wound healing have been reported with various types of MSC [90, 103-108]. In addition, the implantation of HFs in IntegraTM skin equivalent templates for transplantation onto a human patient’s burn wound accelerated reepithelialization, minimized skin graft failure by reconstituting the epithelial stem cell pool, and was felt to produce cosmetically satisfactory results [108]. Other than transplantation, recruiting endogenous stem cells to the site of injury presents an alternative for the treatment of cutaneous wounds. For example, intradermal injection of cutaneous T-cell attracting chemokines and chemokine (C-C motif) ligand-17 and ligand-21 resulted in a significant acceleration of skin regeneration via recruiting BM-derived keratinocyte precursors and BM-MSC, respectively [109, 110]. Increased MSC migratory rate has been shown to be induced by HGF [111], basic fibroblast growth factor (bFGF) [112, 113] and CXCL5 [113] in vitro. Thus, HGF, bFGF and CXCL5 may be exploited as BM-MSC chemoattractants. To enable a sustained, long-term and localized delivery of these diffusible factors, various forms of ECM-like material have been developed and examined as carriers [111, 114]. However, application of stem cells seems advantageous over administering single biological diffusible factors because stem cells can interact with their environment and release multiple wound healing factors. As shown by Krause et al. enriched populations of hematopoietic stem cells homing to bone marrow within 48 hours could incorporate and function in a variety of tissues, including stomach, kidney, lung, and skin [61]. In a human study of chronic non-healing wounds, the group of Badiavas et al. showed that directly applied bone marrow–derived cells can lead to wound closure and
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
48
Gerd G. Gauglitz and Marc G. Jeschke
possible rebuilding of tissues [104]. The lack of an efficient delivery system for these autologous bone marrow–derived cultured cells this study was encountered in a recent study the same group where hMSC were successfully applied to non-healing and acute wounds, using a specialized fibrin spray system [115]. However, despite the above mentioned improvement in wound healing using various stem cell lines, several issues need to be considered before administering stem cells to wound patients. As with all areas of research, there are specific areas of scientific concern to consider for furthering the development of methodologies. With the use of stem cells for tissueengineering applications, there will be numerous concerns to address, including standardization of methods for tissue procurement, cell isolation, and cell culture. Also, functionality of stem cells decreases with age, thus older patients may not present the perfect population as donors [116-118]. Using a mouse model, Schatteman et al. demonstrated that BM-MSC from old mice inhibit rather than promote wound healing when applied to wounds in diabetic mice [118]. Also, the risk of immunological rejection upon transplant or transfusion must be considered if using stem cells from allogenic sources. The mode of stem cells delivery is another frequently discussed current issue. Ideally, stem cells should retain their stemness until delivered and should maintain localized at the wound site in order to enhance engraftment. For such purposes, an acellular dermal matrix was employed by Altman and colleagues as a carrier for delivering ADSC to the wounds locally [106]. This method successfully prevented systemic distribution of the ADCS and may thus be superior to simply injecting stem cells in the wound site [106]. Other concerns of BM-MSC-based wound healing therapy include the increased risk keloid scaring since BM-MSC release VEGF which has been linked to excessive scar formation [107].
Stem Cells and Gene Transfection An ex vivo technique has been described by Mathor et al. [119] using clonogenic keratinocytes with the characteristics of cutaneous stem cells. The authors were able to induce interleukin-6 (IL-6) cDNA using a retroviral construct to achieve a stable transgene expression in vitro. Epidermal sheets from these transfected keratinocytes grafted on to athymic animals showed IL6 production for up to seven days after grafting. In vivo approaches include a recent study by Hachiya et al. [120] in which different lentiviral vectors were
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Novel Approaches for Wound Repair Therapies
.
49
used to transfect human skin grafted onto severe combined immunodeficient mice. These mice showed an effective targeting of epidermal stem cells which underwent terminal differentiation resulting in transgene expression. Stem cells of the follicular outer root sheath and matrix can also be transfected using by non-viral method. Our group has shown that cationic liposomes carrying genes encoding for β-galactosidase were able to transfect hair follicle cells at the edge of the wound [121]. This was confirmed by positive immunohistochemical staining in epithelial stem cells both on the outer root sheath and the matrix of hair follicles. Taking into account the main qualities of the therapeutic options discussed, the transfection of cutaneous stem cells with an optimized gene therapy vehicle could provide a future approach.
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Conclusion Chronic wounds remain a formidable challenge. In spite of recent advances from breakthroughs in recombinant growth factors, gene therapy and bioengineered skin, up to 50% of chronic wounds that have been present for more than a year remain resistant to treatment. Cutaneous wound healing requires a well-orchestrated integration of the complex biological and molecular events of cell migration and proliferation, as well as extracellular matrix deposition, angiogenesis, and remodeling. Gene therapy has evolved from a purely experimental scientific endeavor in a clinically applicable method with countless target organ systems. In wound healing, there still remain challenges such as the identification of optimal target cells, development of sequential therapy methods, and identification of factors detrimental to the introduction of genes into the wound. Stem cells, due to their ability to differentiate into various tissue types by asymmetric replication thus represent a promising tissue repair strategy. A variety of sources, such as bone marrow, peripheral blood, umbilical cord blood, adipose tissue and skin/ hair follicles, have been utilized to isolate stem cells to modulate the healing response of acute and chronic wounds. Recent data have demonstrated the feasibility of autologous ASC therapy in cutaneous repair and regeneration. However, further research in order to solve the many questions on experimental and clinical application of stem cells in wound healing is necessary. Nevertheless, proper wound care and adherence to basic principles cannot be bypassed, even by the most sophisticated approaches.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
50
Gerd G. Gauglitz and Marc G. Jeschke
Ackowledgment The authors would like thank Dr. Katsu Kita, PhD for his support and help.
References
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
[1]
Blome-Eberwein S, Jester A, Kuentscher M, Raff T, Germann G, Pelzer M. (2002) Clinical practice of glycerol preserved allograft skin coverage. Burns 28 Suppl 1: S10-12. [2] Garfein ES, Orgill DP, Pribaz JJ. (2003) Clinical applications of tissue engineered constructs. Clin. Plast. Surg. 30: 485-498. [3] Munster AM. (1996) Cultured skin for massive burns. A prospective, controlled trial. Ann. Surg. 224: 372-375; discussion 375-377. [4] Barret JP, Wolf SE, Desai MH, Herndon DN. (2000) Cost-efficacy of cultured epidermal autografts in massive pediatric burns. Ann. Surg. 231: 869-876. [5] Bannasch H, Fohn M, Unterberg T, Bach AD, Weyand B, Stark GB. (2003) Skin tissue engineering. Clin. Plast. Surg. 30: 573-579. [6] Pellegrini G, Ranno R, Stracuzzi G, et al. (1999) The control of epidermal stem cells (holoclones) in the treatment of massive fullthickness burns with autologous keratinocytes cultured on fibrin. Transplantation 68: 868-879. [7] Tompkins RG, Burke JF. (1990) Progress in burn treatment and the use of artificial skin. World J. Surg. 14: 819-824. [8] Burke JF, Yannas IV, Quinby WC, Jr., Bondoc CC, Jung WK. (1981) Successful use of a physiologically acceptable artificial skin in the treatment of extensive burn injury. Ann. Surg. 194: 413-428. [9] Yannas IV, Burke JF, Orgill DP, Skrabut EM. (1982) Wound tissue can utilize a polymeric template to synthesize a functional extension of skin. Science 215: 174-176. [10] Yannas IV, Burke JF, Warpehoski M, et al. (1981) Prompt, long-term functional replacement of skin. Trans. Am. Soc. Artif. Intern. Organs 27: 19-23. [11] Branski LK, Herndon DN, Pereira C, et al. (2007) Longitudinal assessment of Integra in primary burn management: a randomized pediatric clinical trial. Crit. Care Med. 35: 2615-2623.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Novel Approaches for Wound Repair Therapies
51
[12] Tsai CC, Lin SD, Lai CS, Lin TM. (1999) The use of composite acellular allodermis-ultrathin autograft on joint area in major burn patients--one year follow-up. Kaohsiung J. Med. Sci. 15: 651-658. [13] .Lattari V, Jones LM, Varcelotti JR, Latenser BA, Sherman HF, Barrette RR. (1997) The use of a permanent dermal allograft in full-thickness burns of the hand and foot: a report of three cases. J. Burn Care Rehabil. 18: 147-155. [14] Wainwright D, Madden M, Luterman A, et al. (1996) Clinical evaluation of an acellular allograft dermal matrix in full-thickness burns. J. Burn Care Rehabil. 17: 124-136. [15] Sheridan R, Choucair R, Donelan M, Lydon M, Petras L, Tompkins R. (1998) Acellular allodermis in burns surgery: 1-year results of a pilot trial. J. Burn Care Rehabil. 19: 528-530. [16] .Hohlfeld J, de Buys Roessingh A, Hirt-Burri N, et al. (2005) Tissue engineered fetal skin constructs for paediatric burns. Lancet 366: 840842. [17] Supp DM, Boyce ST. (2005) Engineered skin substitutes: practices and potentials. Clin. Dermatol. 23: 403-412. [18] Muller M, Gahankari, D. and Herndon, D.N. (2007) Operative Wound Management. In: Herndon DN (ed.) Total Burn Care. Saunders, New York City, pp. 177-195. [19] Suzuki S, Matsuda K, Isshiki N, Tamada Y, Ikada Y. (1990) Experimental study of a newly developed bilayer artificial skin. Biomaterials 11: 356-360. [20] Gharaee-Kermani M, Phan SH. (2001) Role of cytokines and cytokine therapy in wound healing and fibrotic diseases. Curr. Pharm. Des 7: 1083-1103. [21] Singer AJ, Clark RA. (1999) Cutaneous wound healing. N. Engl. J. Med. 341: 738-746. [22] Steed DL. (1998) Modifying the wound healing response with exogenous growth factors. Clin. Plast. Surg. 25: 397-405. [23] Kamolz LP, Luegmair M, Wick N, et al. (2005) The Viennese culture method: cultured human epithelium obtained on a dermal matrix based on fibroblast containing fibrin glue gels. Burns 31: 25-29. [24] Hernandez A, Evers BM. (1999) Functional genomics: clinical effect and the evolving role of the surgeon. Arch. Surg. 134: 1209-1215. [25] Khavari PA, Rollman O, Vahlquist A. (2002) Cutaneous gene transfer for skin and systemic diseases. J. Intern. Med. 252: 1-10.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
52
Gerd G. Gauglitz and Marc G. Jeschke
[26] Sprugel KH, McPherson JM, Clowes AW, Ross R. (1987) Effects of growth factors in vivo. I. Cell ingrowth into porous subcutaneous chambers. Am. J. Pathol. 129: 601-613. [27] Vogel JC. (2000) Nonviral skin gene therapy. Hum. Gene. Ther. 11: 2253-2259. [28] Lynch SE, Nixon JC, Colvin RB, Antoniades HN. (1987) Role of platelet-derived growth factor in wound healing: synergistic effects with other growth factors. Proc. Natl. Acad. Sci. U S A 84: 7696-7700. [29] Jeschke MG, Klein D. (2004) Liposomal gene transfer of multiple genes is more effective than gene transfer of a single gene. Gene Ther. 11: 847-855. [30] Shea LD, Smiley E, Bonadio J, Mooney DJ. (1999) DNA delivery from polymer matrices for tissue engineering. Nat. Biotechnol. 17: 551-554. [31] .Fu H, Hu Y, McNelis T, Hollinger JO. (2005) A calcium phosphatebased gene delivery system. J. Biomed. Mater. Res. A 74: 40-48. [32] Eriksson E. (2000) Gene transfer in wound healing. Adv. Skin Wound Care 13: 20-22. [33] Lawrie A, Brisken AF, Francis SE, Cumberland DC, Crossman DC, Newman CM. (2000) Microbubble-enhanced ultrasound for vascular gene delivery. Gene Ther. 7: 2023-2027. [34] Chandler LA, Gu DL, Ma C, et al. (2000) Matrix-enabled gene transfer for cutaneous wound repair. Wound Repair Regen. 8: 473-479. [35] Voigt M, Schauer M, Schaefer DJ, Andree C, Horch R, Stark GB. (1999) Cultured epidermal keratinocytes on a microspherical transport system are feasible to reconstitute the epidermis in full-thickness wounds. Tissue Eng. 5: 563-572. [36] .Gossen M, Bujard H. (1992) Tight control of gene expression in mammalian cells by tetracycline-responsive promoters. Proc. Natl. Acad. Sci. U S A 89: 5547-5551. [37] .Breuing K, Eriksson E, Liu P, Miller DR. (1992) Healing of partial thickness porcine skin wounds in a liquid environment. J. Surg. Res. 52: 50-58. [38] Becker AJ, Mc CE, Till JE. (1963) Cytological demonstration of the clonal nature of spleen colonies derived from transplanted mouse marrow cells. Nature 197: 452-454. [39] Siminovitch L, McCulloch EA, Till JE. (1963) The Distribution of Colony-Forming Cells among Spleen Colonies. J. Cell Physiol. 62: 327336.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Novel Approaches for Wound Repair Therapies
53
[40] Weissman IL. (2000) Stem cells: units of development, units of regeneration, and units in evolution. Cell 100: 157-168. [41] Cha J, Falanga V. (2007) Stem cells in cutaneous wound healing. Clin. Dermatol. 25: 73-78. [42] Hadjantonakis A, Papaioannou V. (2001) The stem cells of early embryos. Differentiation 68: 159-166. [43] Thomson JA, Itskovitz-Eldor J, Shapiro SS, et al. (1998) Embryonic stem cell lines derived from human blastocysts. Science 282: 1145-1147. [44] Klimanskaya I, Chung Y, Becker S, Lu SJ, Lanza R. (2006) Human embryonic stem cell lines derived from single blastomeres. Nature 444: 481-485. [45] Yamanaka S. (2007) Strategies and new developments in the generation of patients-specific pluripotent stem cells. Cell Stem. Cell 1: 39-49. [46] Takahashi K, Tanabe K, Ohnuki M, et al. (2007) Induction of pluripotent stem cells from adult human fibroblasts by defined factors. Cell 131: 861-872. [47] Vats A, Tolley NS, Polak JM, Buttery LD. (2002) Stem cells: sources and applications. Clin. Otolaryngol. Allied. Sci. 27: 227-232. [48] Bishop AE, Buttery LD, Polak JM. (2002) Embryonic stem cells. J. Pathol. 197: 424-429. [49] Murray P, Edgar D. (2001) The regulation of embryonic stem cell differentiation by leukaemia inhibitory factor (LIF). Differentiation 68: 227-234. [50] Zandstra PW, Nagy A. (2001) Stem cell bioengineering. Annu. Rev. Biomed. Eng. 3: 275-305. [51] Minguell JJ, Erices A, Conget P. (2001) Mesenchymal stem cells. Exp. Biol. Med. (Maywood) 226: 507-520. [52] Cortesini R. (2005) Stem cells, tissue engineering and organogenesis in transplantation. Transpl. Immunol. 15: 81-89. [53] Young FE. (2000) A time for restraint. Science 287: 1424. [54] Prentice DA. (2004) Adult stem cells. Issues Law Med. 19: 265-294. [55] Chung Y, Klimanskaya I, Becker S, et al. (2006) Embryonic and extraembryonic stem cell lines derived from single mouse blastomeres. Nature 439: 216-219. [56] Grompe M. (2005) Embryonic stem cells without embryos? Nat. Biotechnol. 23: 1496-1497. [57] Gomillion CT, Burg KJ. (2006) Stem cells and adipose tissue engineering. Biomaterials 27: 6052-6063.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
54
Gerd G. Gauglitz and Marc G. Jeschke
[58] Prelle K, Zink N, Wolf E. (2002) Pluripotent stem cells--model of embryonic development, tool for gene targeting, and basis of cell therapy. Anat. Histol. Embryol. 31: 169-186. [59] Rocha V, Sanz G, Gluckman E. (2004) Umbilical cord blood transplantation. Curr. Opin. Hematol. 11: 375-385. [60] Zuk PA, Zhu M, Ashjian P, et al. (2002) Human adipose tissue is a source of multipotent stem cells. Mol. Biol. Cell. 13: 4279-4295. [61] Krause DS, Theise ND, Collector MI, et al. (2001) Multi-organ, multilineage engraftment by a single bone marrow-derived stem cell. Cell 105: 369-377. [62] Anderson DJ, Gage FH, Weissman IL. (2001) Can stem cells cross lineage boundaries? Nat. Med. 7: 393-395. [63] Lagasse E, Connors H, Al-Dhalimy M, et al. (2000) Purified hematopoietic stem cells can differentiate into hepatocytes in vivo. Nat. Med. 6: 1229-1234. [64] Ferrari G, Cusella-De Angelis G, Coletta M, et al. (1998) Muscle regeneration by bone marrow-derived myogenic progenitors. Science 279: 1528-1530. [65] Gussoni E, Soneoka Y, Strickland CD, et al. (1999) Dystrophin expression in the mdx mouse restored by stem cell transplantation. Nature 401: 390-394. [66] Alison MR, Poulsom R, Jeffery R, et al. (2000) Hepatocytes from nonhepatic adult stem cells. Nature 406: 257. [67] Theise ND, Nimmakayalu M, Gardner R, et al. (2000) Liver from bone marrow in humans. Hepatology 32: 11-16. [68] Mezey E, Chandross KJ, Harta G, Maki RA, McKercher SR. (2000) Turning blood into brain: cells bearing neuronal antigens generated in vivo from bone marrow. Science 290: 1779-1782. [69] Bjornson CR, Rietze RL, Reynolds BA, Magli MC, Vescovi AL. (1999) Turning brain into blood: a hematopoietic fate adopted by adult neural stem cells in vivo. Science 283: 534-537. [70] Takahashi K, Yamanaka S. (2006) Induction of pluripotent stem cells from mouse embryonic and adult fibroblast cultures by defined factors. Cell 126: 663-676. [71] Nakagawa H, Akita S, Fukui M, Fujii T, Akino K. (2005) Human mesenchymal stem cells successfully improve skin-substitute wound healing. Br. J. Dermatol. 153: 29-36. [72] Hematti P, Sloand EM, Carvallo CA, et al. (2002) Absence of donorderived keratinocyte stem cells in skin tissues cultured from patients
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Novel Approaches for Wound Repair Therapies
[73]
[74]
[75]
[76]
[77]
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
[78] [79]
[80]
[81] [82]
[83] [84]
55
after mobilized peripheral blood hematopoietic stem cell transplantation. Exp. Hematol. 30: 943-949. Barry FP, Murphy JM. (2004) Mesenchymal stem cells: clinical applications and biological characterization. Int. J. Biochem. Cell Biol. 36: 568-584. Fathke C, Wilson L, Hutter J, et al. (2004) Contribution of bone marrowderived cells to skin: collagen deposition and wound repair. Stem Cells 22: 812-822. Han SK, Yoon TH, Lee DG, Lee MA, Kim WK. (2005) Potential of human bone marrow stromal cells to accelerate wound healing in vitro. Ann. Plast. Surg. 55: 414-419. Ichioka S, Kouraba S, Sekiya N, Ohura N, Nakatsuka T. (2005) Bone marrow-impregnated collagen matrix for wound healing: experimental evaluation in a microcirculatory model of angiogenesis, and clinical experience. Br. J. Plast. Surg. 58: 1124-1130. Falanga V, Iwamoto S, Chartier M, et al. (2007) Autologous bone marrow-derived cultured mesenchymal stem cells delivered in a fibrin spray accelerate healing in murine and human cutaneous wounds. Tissue Eng. 13: 1299-1312. Gamelli RL, Paxton TP, O'Reilly M. (1993) Bone marrow toxicity by silver sulfadiazine. Surg. Gynecol. Obstet. 177: 115-120. Gamelli RL, He LK, Liu H. (1995) Recombinant human granulocyte colony-stimulating factor treatment improves macrophage suppression of granulocyte and macrophage growth after burn and burn wound infection. J. Trauma. 39: 1141-1146; discussion 1146-1147. Shoup M, Weisenberger JM, Wang JL, Pyle JM, Gamelli RL, Shankar R. (1998) Mechanisms of neutropenia involving myeloid maturation arrest in burn sepsis. Ann. Surg. 228: 112-122. Rao MS, Mattson MP. (2001) Stem cells and aging: expanding the possibilities. Mech. Ageing Dev. 122: 713-734. Huss R. (2000) Isolation of primary and immortalized CD34hematopoietic and mesenchymal stem cells from various sources. Stem Cells 18: 1-9. Hows JM. (2001) Status of umbilical cord blood transplantation in the year 2001. J. Clin. Pathol. 54: 428-434. McGuckin CP, Forraz N, Baradez MO, et al. (2005) Production of stem cells with embryonic characteristics from human umbilical cord blood. Cell Prolif. 38: 245-255.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
56
Gerd G. Gauglitz and Marc G. Jeschke
[85] Erices A, Conget P, Minguell JJ. (2000) Mesenchymal progenitor cells in human umbilical cord blood. Br. J. Haematol. 109: 235-242. [86] Mareschi K, Biasin E, Piacibello W, Aglietta M, Madon E, Fagioli F. (2001) Isolation of human mesenchymal stem cells: bone marrow versus umbilical cord blood. Haematologica 86: 1099-1100. [87] Romanov YA, Svintsitskaya VA, Smirnov VN. (2003) Searching for alternative sources of postnatal human mesenchymal stem cells: candidate MSC-like cells from umbilical cord. Stem Cells 21: 105-110. [88] Kamolz LP, Kolbus A, Wick N, et al. (2006) Cultured human epithelium: human umbilical cord blood stem cells differentiate into keratinocytes under in vitro conditions. Burns 32: 16-19. [89] Kita K, Gauglitz GG, Phan TT, Herndon DN, Jeschke MG. (2009) Isolation and characterization of mesenchymal stem cells from the subamniotic human umbilical cord lining membrane. Stem Cells Dev. [90] Kim WS, Park BS, Sung JH, et al. (2007) Wound healing effect of adipose-derived stem cells: a critical role of secretory factors on human dermal fibroblasts. J. Dermatol. Sci. 48: 15-24. [91] Zuk PA, Zhu M, Mizuno H, et al. (2001) Multilineage cells from human adipose tissue: implications for cell-based therapies. Tissue Eng. 7: 211228. [92] Kim CG, Lee JJ, Jung DY, et al. (2006) Profiling of differentially expressed genes in human stem cells by cDNA microarray. Mol. Cells 21: 343-355. [93] Strem BM, Hicok KC, Zhu M, et al. (2005) Multipotential differentiation of adipose tissue-derived stem cells. Keio J. Med. 54: 132-141. [94] Aust L, Devlin B, Foster SJ, et al. (2004) Yield of human adiposederived adult stem cells from liposuction aspirates. Cytotherapy 6: 7-14. [95] Huang JI, Hedrick MH, Lorenz P. (2000) Chondrogenesis of human adipo-derived mesodermal stem cells. Surg. Forum 583-585. [96] Tholpady SS, Llull R, Ogle RC, Rubin JP, Futrell JW, Katz AJ. (2006) Adipose tissue: stem cells and beyond. Clin. Plast. Surg. 33: 55-62, vi. [97] Giorgino F, Laviola L, Eriksson JW. (2005) Regional differences of insulin action in adipose tissue: insights from in vivo and in vitro studies. Acta Physiol. Scand. 183: 13-30. [98] Tiede S, Kloepper JE, Bodo E, Tiwari S, Kruse C, Paus R. (2007) Hair follicle stem cells: walking the maze. Eur. J. Cell Biol. 86: 355-376. [99] Roh C, Lyle S. (2006) Cutaneous stem cells and wound healing. Pediatr. Res. 59: 100R-103R.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Novel Approaches for Wound Repair Therapies
57
[100] Oshima H, Rochat A, Kedzia C, Kobayashi K, Barrandon Y. (2001) Morphogenesis and renewal of hair follicles from adult multipotent stem cells. Cell 104: 233-245. [101] Lau K, Paus R, Tiede S, Day P, Bayat A. (2009) Exploring the role of stem cells in cutaneous wound healing. Exp. Dermatol. 18: 921-933. [102] Amado LC, Saliaris AP, Schuleri KH, et al. (2005) Cardiac repair with intramyocardial injection of allogeneic mesenchymal stem cells after myocardial infarction. Proc. Natl. Acad. Sci. U S A 102: 11474-11479. [103] Francois S, Mouiseddine M, Mathieu N, et al. (2007) Human mesenchymal stem cells favour healing of the cutaneous radiation syndrome in a xenogenic transplant model. Ann. Hematol. 86: 1-8. [104] Badiavas EV, Falanga V. (2003) Treatment of chronic wounds with bone marrow-derived cells. Arch. Dermatol. 139: 510-516. [105] Falanga V, Saap LJ, Ozonoff A. (2006) Wound bed score and its correlation with healing of chronic wounds. Dermatol. Ther. 19: 383390. [106] Altman AM, Matthias N, Yan Y, et al. (2008) Dermal matrix as a carrier for in vivo delivery of human adipose-derived stem cells. Biomaterials 29: 1431-1442. [107] Wu Y, Chen L, Scott PG, Tredget EE. (2007) Mesenchymal stem cells enhance wound healing through differentiation and angiogenesis. Stem Cells 25: 2648-2659. [108] Navsaria HA, Ojeh NO, Moiemen N, Griffiths MA, Frame JD. (2004) Reepithelialization of a full-thickness burn from stem cells of hair follicles micrografted into a tissue-engineered dermal template (Integra). Plast. Reconstr. Surg. 113: 978-981. [109] Inokuma D, Abe R, Fujita Y, et al. (2006) CTACK/CCL27 accelerates skin regeneration via accumulation of bone marrow-derived keratinocytes. Stem Cells 24: 2810-2816. [110] Sasaki M, Abe R, Fujita Y, Ando S, Inokuma D, Shimizu H. (2008) Mesenchymal stem cells are recruited into wounded skin and contribute to wound repair by transdifferentiation into multiple skin cell type. J. Immunol. 180: 2581-2587. [111] Zhao J, Zhang N, Prestwich GD, Wen X. (2008) Recruitment of endogenous stem cells for tissue repair. Macromol. Biosci. 8: 836-842. [112] Schmidt A, Ladage D, Schinkothe T, et al. (2006) Basic fibroblast growth factor controls migration in human mesenchymal stem cells. Stem Cells 24: 1750-1758.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
58
Gerd G. Gauglitz and Marc G. Jeschke
[113] Nedeau AE, Bauer RJ, Gallagher K, Chen H, Liu ZJ, Velazquez OC. (2008) A CXCL5- and bFGF-dependent effect of PDGF-B-activated fibroblasts in promoting trafficking and differentiation of bone marrowderived mesenchymal stem cells. Exp. Cell Res. 314: 2176-2186. [114] Liu Y, Cai S, Shu XZ, Shelby J, Prestwich GD. (2007) Release of basic fibroblast growth factor from a crosslinked glycosaminoglycan hydrogel promotes wound healing. Wound Repair Regen. 15: 245-251. [115] Falanga V. (2005) Wound healing and its impairment in the diabetic foot. Lancet 366: 1736-1743. [116] Chambers SM, Goodell MA. (2007) Hematopoietic stem cell aging: wrinkles in stem cell potential. Stem Cell Rev. 3: 201-211. [117] Van Zant G, Liang Y. (2003) The role of stem cells in aging. Exp. Hematol. 31: 659-672. [118] Schatteman GC, Ma N. (2006) Old bone marrow cells inhibit skin wound vascularization. Stem Cells 24: 717-721. [119] Mathor MB, Ferrari G, Dellambra E, et al. (1996) Clonal analysis of stably transduced human epidermal stem cells in culture. Proc. Natl. Acad. Sci. U S A 93: 10371-10376. [120] Hachiya A, Sriwiriyanont P, Patel A, et al. (2007) Gene transfer in human skin with different pseudotyped HIV-based vectors. Gene Ther. 14: 648-656. [121] Pereira CT, Herndon DN, Perez-Polo JR, Burke AS, Jeschke MG. (2007) Scar trek: follicular frontiers in skin replacement therapy Genet Mol. Res. 6: 243-249.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
In: Skin Care Editor: Sandra M. Hayes, pp. 59-77
ISBN 978-1-61209-568-4 © 2011 Nova Science Publishers, Inc.
Chapter III
Skin Care: Chronic Ulcer Management P. C. Leung
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Dept. Orthopaedics and Traumatology, The Chinese University of Hong Kong, China
Abstract Chronic ulcers are related to vascular, neurological or metabolic problems that either initiate the formation of the ulcers themselves or prevent the usual healing processes. With the aging population, chronic ulcers occur in larger numbers of population in the first place, and give the elderlies disabling disturbances in a lot of circumstances. Chronic ulcers are treated with standard procedures which include basic wound care and surgery, ranging from skin grafting, flap closure and reconstructive measures. Unfortunately, the chronicity is resistant to conservative treatment and either the age or the co-existing morbid conditions are unfavorable for special surgical measures. In recent years, with the development of molecular biology, growth factors are included into the treatment options. Stem cell research has also brought a new area of application to chronic ulcers. These new measures, however, remain in their experimental stage short of general application. On the other hand, traditional herbal medicine might have something special to offer in chronic situations resistant to treatment.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
60
P. C. Leung
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Introduction Human skin has a wonderful ability of healing after injuries like abrasions and cut wounds. The extremely rich supply of vasculature allows an ever copious provision of nutrients and a perfect environment for the interchange of molecular activities related to inflammation thence active cellular replications and healing. Apart from the biologically active histomorphometry that provides the dynamic basis of tissue repair, the physical property of the skin further supports its healing after injuries, whether minor or major. For the minor injuries, the ever shadding cutaneous layers of epithelial cells are providing shielding and replacement effects. For the more major injuries where significant tissue losses occur, the deeper corium layer of the skin plays a significant role. While the layer of damaged collagen fibres of the skin undergoes inflammatory changes, the deeper collagen fibres start to contract, so that any defective gap resulting from the injury would be quickly approximated. It has been found in experimental animals, that as long as the skin gap does not exceed a certain width, the facing edges pulls naturally on a centripedal direction and would thus narrow down the gap and lead to healing. Basing on this observation, large ulcers on the skin may heal by skin grafting (providing normal collagen fibres), not requiring full coverage, but as long as the central part of the ulcer is covered, such surgical manoevre would narrow down the width between the facing edges, thus inducing an effective centripedal pull of the edges to produce a favourable spontaneous closure. With these properties, skin ulcers always heal, given time. The observations that all burnt wounds, no matter how extensive, would heal with scaring, are solid proofs. However, we do have chronic non-healing ulcers under special circumstances. Chronic unhealing ulcers occur when there are unfavourable local or systemic conditions. This chapter deals with the commonly occurring chronic ulcers.
Causes of Chronic Skin Ulcers Causes of chronic skin ulcers could be local or systemic Local causes included: Infection resistant to treatment
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Skin Care: Chronic Ulcer Management
61
⎯ Ischemia, which could be due to local pressure or peripheral vascular ischemia ⎯ Poor circulation in venous stasis of the legs ⎯ Neuropathy which fails to offer protection while at the same time disturbs the vascular integrity Systemic causes included: Malnutrition including anaemia and debilitation ⎯ State of Diabetes where ischaemia, neuropathy and proneness to infection co-exist. ⎯ Aging: the slowing down of physiological activities would be unfavourable for the normal healing.
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Infected Chronic Ulcers Infection is usually the consequence rather than the cause of chronic foot ulcers. Infected chronic ulcers may be classified as mild to moderate or severe, when osteomyelitis is involved [1,2]. Appropriate tissue or bone cultures are useful to guide the use of antibiotic therapy. Gram-positive organisms account for the majority of infections, while the prevalence of methicellin resistant staphylococcus aureus has become common in recent years [3,4]. In the deep categories of chronic ulcers, the prevalent organism of infection is still staphylococcus. Comparing superficial swabs and bone biopsy cultures in the identification of organisms, the latter is much more reliable [5,6]. Although gram-positive organisms are overwhelming in chronic ulcers, including the diabetic variety, the polymicrobial nature of bacterial growth should not be ignored in the management planning, especially in developing countries [7].
Ischaemia Chronic Ulcers Ischaemia leads to tissue necrosis presented as skin dryness, thinning down and proneness to ulceration. The local manifestations of cutaneous microangiopathy could be considered the result of the general circulatory state, which obviously affects skin perfusion [8].
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
62
P. C. Leung
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
It is important to recognise that diabetic patients with co-existing neuropathy, when ischaemia may remain asymptomatic. The clinician, therefore, should check the peripheral pulses carefully, including the femoral, popliteal, posterior tibial, peroneal and dorsalis pedis. The presence of a femoral artery or popliteal artery bruit strongly indicates the presence of treatable peripheral vascular disease. The absence of a bruit, which is more common, indicates generalised vascular occlusion [9]. The Doppler device is a helpful tool at this stage. If there is no clinical indication of vascular compromise, no further investigations are usually required. In contrast, those with suggestions of peripheral vascular disease should be investigated with standard angiographic studies. Those suffering from dry gangrene, rest pain, and/or deep ulceration with absent peripheral pulses require further vascular work-up. Since not all patients are suitable for vascular reconstruction, (e.g. in late presentations, generalised atherosclerosis, elderly age, co-existing morbidities etc.), other tests like transcutaneous oxygen saturation may help to identify those patients who may have better chances of wound healing. Likewise, if the blood pressure of the unaffected great toe is >30mmHg, it stands a much better chance of ulcer healing [10].
Venous Stasis Chronic Ulcers These ulcers occur in the legs which are provided with two systems of venous return, viz the deep veins and the superficial veins. The superficial veins rely on a system of venous valves to prevent a gravitational stagnation of flow. The deep vein system depends on active muscular activities around the veins to initiate an effective back flow of circulation. When muscular activities are insufficient for the normal pumping effects, venous flow from the superficial veins is blocked and subsequently, the weak venous valves fail to support the stagnant columns of blood. The breakdown of these valves lead to high venous pressure over the distal ends the superficial veins which occur over the ankle and sheen of the leg. The results are manifested as extravasation of venous blood to the subcutaneous spaces, pigmentations, swelling and ulcerations. Unless the venous stasis is corrected, the ulcers do not heal. The chronic nature of the ulcer development, at the same time, has adversely affected the histomorphometry of the skin, so that the scaring together with the local ischaemia and infective foci, would be making normal healing most unfavourable [9].
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Skin Care: Chronic Ulcer Management
63
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Neuropathic Chronic Ulcers Peripheral neuropathy and sensory loss is always considered to be the most prominent risk factor in the development of ulcers. The sensory disturbances on the other hand, are further jeopardised by abnormal pressure points under and around the foot and ankle, as well as deformities at different levels of the foot resulting from ageing and arthritis. The same pathology is responsible for the slow healing, non-healing and recurrence of foot ulcers [11,12]. Assessing the state of neuropathy, therefore, is of vital importance with particular reference to prognosis of healing and prevention of recurrence. While it is vital to point out that treating diabetic ulcers without a proper clinical assessment on the state of sensation is totally unacceptable, the practical means of obtaining objective data for proper clinical judgement needs to be discussed. The two most commonly performed tests are the SemmesWeinstein monofilament test and the biothesiometer test [13,14,15]. Sensation testing of the intact skin using the Semmes-Weinstein monofilament is performed by pressing the monofilament onto the site being tested until it bends. The failure to detect the touch indicates that neuropathy is severe and protective sensation is absent. The standard sites to be tested include the plantar surface of the great toe, the metatarsal heads, the heel and any other site under the threat of pressure because of deformities. More sensation testing is achieved using a biothesiometer, which measures the vibration threshold felt by the patient. The head of the instrument is held perpendicularly to the plantar aspect of the at-risk point, while vibration is gradually increased until detected by the patient. These two simple measuring methods have been validated for reliability by various workers who confirm that highly acceptable intercessional correlations and limited repeatability errors are achieved [16,17]. A podiatry study undertaken in Australia showed that the neuropathy group of diabetics have an annual occurence of ulceration of 4% for those with an abnormal biothesiometer reading, but who still feel the monofilament, 10% for those who cannot feel the monofilament, and 26% for those with previous ulceration or amputations. The same group of investigators have estimated that, with reasonable podiatric care, only one ulcer develops in 367 diabetic subjects without peripheral neuropathy. However, the number increases to 1 in 45 for those with neuropathy, 1 in 18 for those who cannot feel the monofilament and one in seven for those who have already experienced ulceration or toe amputation [18].
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
64
P. C. Leung
There is one other aspect of neuropathy occurring among diabetic patients which is often overlooked. Proprioceptive involvement leading to Charcot arthropathy of the foot and ankle joints often co-exists with chronic foot ulcers [19]. It should be realised that many major amputations are done because of uncontrolled neuropathic arthropathy; early awareness with the provision of effective bracing might succeed in limb preservation. A study of 115 patients and 127 limbs with neuroarthropathy has shown a 2.7% annual rate of amputation, 23% requiring bracing but 49% developing recurrent ulceration [20]. With neglected cases, when Charcot arthropathy has been present for a long time, it might be difficult to differentiate it from pyogenic arthritis or osteomyelitis. While Charcot joint most commonly affects the tarso-metatarsal and tarsal joint and is painless, osteomyelitis is almost exclusively adjacent to skin ulcers and occurs most frequently around the metatarso-phalangeal joints and the calcaneum [21,22].
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Diabetic Chronic Ulcers The diabetic state affecting the lower limbs, viz, vascular ischaemia, neuropathy and proneness to infection, adversely affect the healing of ulcers. In the situation of infection in diabetic patients, the foot is the crossroad for many pathological processes, in which almost all components of the lower extremity are involved; from skin, subcutaneous tissue, muscles, bones and joints, to blood vessels and nerves. An understanding of these processes is necessary for the development and application of management and preventative strategies [23]. The development pathway towards ulceration is multifactorial. A critical triad of neuropathy, minor foot trauma and foot deformity is responsible for over 50% of diabetic foot ulcers. In addition, other risk factors like uneven plantar pressures, joint rigidities, and impaired wound healing ability are all contributing factors. Clinically, the predisposing risk factors leading to nonhealing ulcers are those outlined in Table 1. Apart from the obvious clinical predisposing risk factors, recent studies have revealed that very complex mechanisms are involved at the tissue-molecular level, which prevent normal healing processes. Many chemo-cytokines are involved, including matrix metalloproteinases, serine proteinases, integrins, chemokines, replicative cell senescence, growth factors and adult stem cells [24,25,26].
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Skin Care: Chronic Ulcer Management
65
Diabetic patients with tissue injury initially display impairment in the immune system response with reduced chemotactic effects to recruit inflammatory cells into the damaged tissues, thus, slowing down healing and increasing the risk of bacterial infection. Following this initial period, when the inflammatory response is eventually established, the process switches to an exacerbation of inflammation and proteolysis [27]. The result of prolonged exposure to hyperglycaemia also generates glycation of proteins and disturbances of cell responses, thus, further hindering the process of fibrosis and tissue repair [28,29]. Recent molecular studies on chronic diabetic ulcers indicated that more specific processes may be involved. For example, it has been found that leucocytes are prevented from ready entry and accumulation in the ulcers, which, therefore, fail to achieve normal healing [30]. Other studies on the specific properties of fibroblasts from patients with chronic diabetic ulcers showed that these cells were different from those taken from patients without chronic ulcers in that the high molecular weight hyaluronic acid in the pericellular matrix was much more concentrated. The unique property of the fibroblasts might predispose these patients to chronic ulcer formation [31]. With regard to the circulatory state, it is not uncommon to find totally absent peripheral pulses in the leg affected with chronic ulcers. Orthopaedic or vascular surgeons who rely totally on peripheral vascular integrity as decisive assessment parameters for treatment choices, which often include vascular reconstruction or limb sacrifice, should realize the extreme chronic nature of the pathology, very often does not allow an optional prediction of outcome. On the other hand, if the extremity remains warm and pink inspite of the absent peripheral pulses, it might well indicate that sufficient distal collateral circulation probably has sufficiently established to allow survival of the limb. Studies have shown that if the blood pressure of one unaffected great toe is more than 30 mmHg, the chance of having the ulcer healed is reasonably good. Other tests like transcutaneous oxygen saturation may help to identify those patients who may have better chances of wound healing [10]. With regard to infection in diabetic chronic ulcer, they are frequently coexisting with fungal infections of the foot and it has been said that bacterial infection could be predisposed by fungal infection. A study of 13,271 patients with diabetes has shown that 78.4% have fungal infection of the feet. Among these infections, 70.8% are of Tinea pedis type. The investigators, therefore, consider fungal infection a risk factor for foot ulcers. Other studies try to delineate the different types of tinea, i.e. different Candida species, but have
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
66
P. C. Leung
not succeeded in identifying species of higher risk [32]. As the link between infection and foot ulcers is so strong in diabetics, the question of whether these patients are immunologically compromised arises. Limited studies have shown that secondary immunodeficiency in both cellular and humoral immune parameters, in patients with chronic bacterial foot infection, is not unexpected [33].
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Types of Ulcers Clinicians have tried to classify diabetic foot ulcers into different categories and grades. Attempts have not been successful because classifications fail to help with clinical judgement and management planning. There is the University of Texas system which grades ulcers by depth and then stages them by the presence of infection and ischaemia, excluding degrees of neuropathy [34]. The International Working Group on the diabetic foot proposes the PEDCS classification grades for the ulcers on the basis of perfusion, extent, depth, infection and sensation. This looks good but is too complicated. The size, area, depth (SAD) classification attempts to simplify the categories. Alternatively the six grade Wagner-Meggitt classification looks at the depth of ulcers and the existence of tissue gangrene. Of these classifications the most practical system to help with the prediction of healing and the possibility of amputation is probably the simpler: the Wagner-Meggitt classification [35,36]. For Grade 2 through 6, the overall chance of local or major amputation is estimated to be around 60%.
Management of Chronic Ulcers Before starting a proper planning for the healing of a chronic ulcer, the general condition of the patient should be well taken care of. This includes the control of infection, correction of the nutritional state including the haemaglobin level, and getting a clinical picture of the circulatory state. For the diabetic patient, full clinical control of the hyperglycaemic state should be assured.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Skin Care: Chronic Ulcer Management
67
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Ulcer Care Although a multitude of factors affect the healing of chronic diabetic foot ulcers, and local care of the ulcer does not guarantee its healing, proper local management is still crucial. Daily or more frequent cleaning and dressing are essential requirements. Regular daily bathing in saline or dilute antiseptic solution offers a better chance of cleaning the ulcers, compared with dressing alone [37]. New dressing methods and new dressing materials are now available to help remove the exudate and to promote a more rapid shrinkage of the ulcers. The use of vacuum-assisted closure or dressing, which is popular in other surgical areas, has started to be used in the foot and ankle areas. Repeated minor surgical debridement followed by vacuum dressing has been shown to be useful in the promotion of ulcer healing [38]. In large ulcers once granulation growth becomes healthy and infection controlled, skin grafting can be considered. Waiting for spontaneous epitheliaisation takes too long. Mesh graft is preferred because entrapment of exudation does not occur and the result of re-surfacing is not inferior. Many artificial dermagrafts are available for temporary granulation coverage. These are not genuine grafts because they basically serve as dressing material, to support ulcer shrinkage, as spontaneous epithelialisation occurs from around the ulcer edges. The dermagrafts are either manufactured from human tissue like amniotic membrance or synthetic material which is bioengineered into a thin covering sheet comprised of dermal fibroblasts [39]. Most chronic foot ulcers occur among elderly diabetics. The poor circulatory state, neuropathy, and co-morbid conditions do not allow sophisticated surgery. However, when chronic ulcers occur in healthy younger patients, surgical closure with special techniques could be considered.
Ulcer Surgery Abundant data show that simple surgery consisting of extensive debridement of ulcer wounds and removal of devitalised tissues is the single most important therapeutic step leading to ulcer healing and limb salvage. Chronic ulcers are the result of prolonged biological hazards. Therefore, good outcomes are measured in weeks and months rather than days. At least six to ten weeks is the expected time for healing of these complicated lesions.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
68
P. C. Leung
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Split skin-grafting for weight bearing plantar defects is often a poor option because of the inadequate recipient bed and defective durability of the skin cover. Breakdown of split skin-grafted areas is common with daily ambulation and footwear pressure. Local random flaps have marginal use, because limited local mobility does not allow the skin adjacent to the chronic ulcer to be mobilised. Pedicled muscle flaps have been used as an alternative approach. However, flap viability is still a problem. Under special circumstances, free skin flap transfer using a microvascular technique is feasible and there are many such reported cases. Enthusiasm for these procedures remains low because of the risk of arterial occlusion and the compromised fitness of diabetic patients [40]. Diabetice ulcers over the heel are common. This weight-bearing area needs an epithelial cover that is durable and upports the body weight. The reverse sural flap may be a good choice. The technique and details of the procedures have been described in many reports and ulcers around the ankle and heel have been adequately resurfaced. It is considered particularly useful when chronic osteomyelitis is underlying the chronic ulcers [41].
Supportive Surgery Chronic diabetic foot ulcers combined with functional problems add further risks to the formation of more ulcers. Such situations can arise when the Achilles tendon becomes tight as a result of prolonged disuse of the ankle. The plantar-flexed ankle imposes more pressure on the metatarsal heads which may be responsible for pressure ulcer development. The tight Achilles tendon can be lengthened, so as to release metatarsal head pressure. After the lengthening, there is an initial weakening of the plantar flexion pull, which returns to normal in approximately eight months time [42]. At the same time as releasing of the metatarsal head pressure, the metatarsal head can be removed, via the plantar ulcer or via separate incisions. Under special circumstances, metatarsal head resection can be combined with Achilles tendon release. Other tendon balancing procedures can also be added when functional problems are observed. Peroneus longus tendon lengthening is another commonly performed adjuvant measure in cavus foot deformity related to plantar ulceration. The diabetic patient with chronic ulceration of the foot often has co-existing deformities which might need to be corrected to prevent ulcer recurrence or new ulcer development. Orthopaedic procedures are then required as the deformities commonly occur in the toes. Correction of
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Skin Care: Chronic Ulcer Management
69
Keller's arthroplasty and metatarso-phalangeal joint fusion are two common procedures to correct deformity of the great toe [43,44]. When diabetic neuropathy results in Charcot joints, surgical intervention often becomes necessary. Surgery may involve joint fusion at the site of the arthropathy or in the most unstable late cases, amputation. Charcot arthropathy commonly occurs at the tarsal joints, which become unstable and initiate various deformities of the foot. Debridement and fusion should be the aim but fusion of the neuropathic joint is usually difficult. In late cases, therefore, amputation at the neuropthic site becomes a secondary option [45].
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Other Support Abnormal pressure points undoubtedly predispose the diabetic foot to ulceration. Protecting the pressure points, therefore, becomes vital for the prevention of ulcer formation. Applying total contact casting as the means of treating early uncomplicated ulcers further supports the need for protecting the pressure points. For the healing of purely neuropathic ulcers, simple pressure relieving casting is effective. However, most diabetic ulcers are complicated by peripheral arterial disease and infection. Therefore, pressure relieving devices are important mostly after treatment interventions and ulcer healing. A number of these devices are commonly used. They include the simple insole shoe, a special shoe, pneumatic walking brace and bivalved total contact cast. In a study comparing the effectiveness of the four modalities, it has been found that forefoot pressure is uniformly reduced with all devices but peak pressure is reduced by the special shoe and bivalved cast. The logic of increasing the underfoot contact area to decrease plantar foot pressure, therefore, is very sound and should be endorsed as an essential component for the treatment of diabetic foot ulcers. Commercially available devices are used for convenience and general effectiveness. Since deformities are unpredictable in diabetic feet, the total contact cast and its derivatives remain the most efficient off-pressure applications [46,47].
Herbal Treatment If a wound has received a wide range of treatments yet has failed to heal, alternative treatment is an option. Different modalities are frequently tried,
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
70
P. C. Leung
from the old traditional herbal treatment (topical or systemic) to more innovative ultrasonic therapy. Many reports are available in Chinese language medical journals, describing the effectiveness of herbal combinations in ulcer healing. However, these reports are not validated by proper clinical trials. In Hong Kong, a comprehensive investigation has been completed in 2008 on a popular herbal formula. In the laboratory, the formula is studied by its effects on fibroblast culture, and wound healing through granulation formation and angiogenesis, and so far the outcome has been very positive. A randomised placebo controlled trial was conducted on 80 patients with nonhealing diabetic ulcers occurring in legs which had been listed for major amputation, using the same herbal formula. 85% of the legs were salvaged and the herbal treatment group revealed better granulation, more rapid healing, better surface oxygen tension and microcirculation [48].
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Discussion Among all the chronic ulcers, those with diabetic origin have been most intensively studied. Despite much efforts towards the treatment of diabetic foot ulcers, the incidence of lower extremity amputation remains about the same. Amputation is a costly outcome and should be prevented as far as possible. Ulcers should be prevented and if they have already occurred, should be treated early. There is little doubt that they'll require special care, since these ulcers heal differently from other ulcers, because of the unique predisposing causes including peripheral neuropathy, vascular insufficiency and hyperglyeaemia in diabetics which invites infection, and the lack of an orderly and predictable healing process, Assessment still relies mainly on clinical judgement. Risk factors should be detected on the first encounter; the vascular state should be carefully assessed through pulse studies and surface circulation, and the neuropathic state tested by performing the 10gm SemmesWeinstein monofilament test. The depth of the chronic ulcer is more important prognostically than other criteria such as size, number and duration. Local care of the ulcer is essential. No 'miraculous' outcome can be expected, even with innovative agents like synthetics, growth factors and stem cells. However, dressings including removal of necrotic tissue and drainage of infected exudates, helps to provide better granulation formation. Control of the diabetic state and timely control of infection is also essential. For hospital admissions, the ulcers are already deep, infection prolonged and vascular reconstruction may be too late to be beneficial. Although one has
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Skin Care: Chronic Ulcer Management
71
to acknowledge that a well-performed amputation and successful rehabilitation can improve a patient's quality of life, an abnormal foot after minor amputations is much more acceptable and useful to the elderly patient than an ulcerated foot. Salvage attempts, therefore, need to be carefully tried before ablative surgery. Since ulceration occurs as a result of repeated minor trauma caused by footwear pressure on the deformed foot, prevention of ulcer formation must start with the protection of the pressure points i.e. off-loading. Total contact casts and their modifications remain the most effective off-loading devices and should always be included in the consideration of foot ulcer treatment and prevention. Consideration of the social and psychological implications are also important in planning strategies for the prevention of ulcer recurrences. Since the diabetic foot ulcer has developed into a public health problem, it deserves a holistic approach including socio-economic planning. For all difficult healing problems, the treatment provided is never limited to conventional modalities. Instead, controversial treatment modalities, frontier research-based attempts and even old traditional alternatives, are used. Hyperbaric oxygen treatment is a more conventional form of therapy for chronic ulcers and diabetic gangrene. Some reports on reasonable sized series give a 70% success rate. The failures are related to poor circulation, as is revealed by low transcutaneous oxygen tensions of below 29mmHg. The relatively high rate of failure, in spite of hyperbaric treatment, casts doubts on the true value of this form of therapy [49].
Molecular Biology and Chronic Ulcer Treatment As the pathophysiology of wound healing is being understood at the molecular level, an increasing number of growth factors and cytokines are documented and their possible mode of action understood, the next natural development is the application of this knowledge to promote healing of chronic ulcers. Animal studies have shown that fibroblast growth factors, used either as solitary impregnated gelatin microspheres or laid on artificial dermis, accelerates fibroblast proliferation and capillary formation.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
72
P. C. Leung
Many clinical trials of various growth factors (e.g. granulocyte colony stimulating factors, and fibroblast growth factor have demonstrated the clinical value of their topical use). Innovative attempts to save ischaemic feet with ulcers by the application of stem cells have also been carried out. Stem cells are implanted into the skeletal muscle proximal to the chronic ulcer in an attempt to initiate angiogenesis [50,51]. In spite of scattered clinical reports, one must realise that growth factors, and stem cell therapy remain, as yet, experimental. If the ischaemic state is really so bad that even the marginal nutritional needs for all tissues is not satisfied, the outcome is still tissue necrosis and gangrene irrespective of any form of topical or regional treatment.
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Conclusion Chronic skin ulcers are difficult to heal. For the victims they give endless frustrations. For the clinician, there is a tendency to give up with active treatment and sacrificing the limb. For some reasons chronic skin ulcers affect mostly the socially deprived and for the affluent regions, this chronic clinical problem has been considered a public health issue demanding excessive medical and health resources. As in all chronic situations, prevention if achievable, would be more important than taking remedial measures. In the situation of diabetic chronic ulcers, perhaps even for venous stasis ulcers, the role of patients; own care will be vital for the prevention. Self care includes local ulcer cleaning and prevention of minor tranma, very much related to foot-ware pressure, will need to be perfectly taken care of. Chronic skin ulcers would be occurring more often in the developing world. While modern forms of ulcer care are not affordable, the traditional wisdom of herbal medicine might deserve more exploration in the developing world. Herbal medicine does not aim at single target cure, but in some way attempts to allow the user to develop a physiological state of higher alert and internal balance so as to allow the ulcer to heal [52]. Our recent experience with some lepers who suffered from 10-20 years’ occurrences of chronic unhealed ulcers in their feet, have given us good insight into their treatment. Nobody wants to treat these chronic ulcers and nobody has confidence to cure thru. Using a simple herbal formula which we have used for chronic diabetic foot ulcers and have obtained good results, we found that starting from 2 month’s of oral intake, there appeared definite
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Skin Care: Chronic Ulcer Management
73
evidence of granulation enrichment and effective epithelialisation from the ulcer edges. This brought about ulcer shrinkage, gradual healing. In other cases the granulations became viable for split skin grafting (Illustration). Perhaps the chronicity of the ulceration reflects a most complex molecular environment of a mixture between fibrosis, ischaemia, inflammation and infection, which requires some unusual dietary supplement to initiate a significant change. Under such circumstances, the standard treatment options which we are familiar with do not work, yet, some other regime, apparently obsolete and unscientific, produces unexpected results.
References [1]
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
[2]
[3]
[4]
[5] [6]
[7]
[8]
Ge Y, MacDonald D, Hait H, Lipsky B, Zarloff M, Holroyd K, et al. Microbiological profile of infected diabetic foot ulcers. Diabet. Med. 2002; 19: 1032-4. Calhoun JH, Overgaard KA, Stevens CM, Dowling JP, Mader JT. Diabetic foot ulcers and infections: Current concepts. Adv. Skin Wound Care 2002; 15: 31-42. Tentolouris N, Jude EB, Smirnof I, Knowles EA, Boulton AJ. Methicillin-resistant staphylococcus aureus: An increasing problem in a diabetic foot clinic. Diabet. Med. 1999; 16: 767-71. Dang CN, Prasad YD, Boulton AJ, Jude EB. Methicillin-resistant staphylococcus aureus in the diabetic foot clinic: A worsening problem. Diabet. Med. 2003; 20: 159-61. Mackowiak PA, Jones SR, Smith JW. Diagnostic value of sinus-tract cultures in chronic osteomyelitis. JAMA 1978; 239: 2772-5. Senneville E, Melliez H, Beltrand E, Legout L, Valette M, Cazaubiel M, Cordonnier M, et al. Culture of percutaneious bone biopsy specimens for diagnosis of diabetic foot osteomyelitis: concordance with ulcer swab cultures. Clin. Infect. Dis. 2006; 42: 57-62. Slater RA, Lazarovitch T, Boldur I, Ramot Y, Buchs A, Weiss, et al. Swab cultures accurately identify bacterial pathogens in diabetic foot wounds not involving bone. Diabet. Med. 2004; 21: 705-09. Ngo BT, Hayes KD, Dimiao DJ, Srinivasan SK, Huerter CJ, Rendell MS. Manifestations of cutaneous diabetic microangiopathy. Am. J. Clin. Dermatol. 2005; 6 (4): 225-37.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
74 [9]
[10]
[11]
[12] [13] [14] [15]
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
[16]
[17]
[18] [19] [20] [21]
[22]
P. C. Leung McGee SR, Boyko EJ. Physical examination and chronic lower extremity ischaemia: a critical review. Arch. Intern. Med. 1998; 158: 1357-64. Kalani M, Brismar K, Fagrell B, Ostergren J, Jorneskog G. Transcutaneious oxygen tension and toe blood pressure as predictor of outcome of diabetic foot ulcers. Diabetes Care 1999; 22: 147-51. Wu SC, Crews RT, Armstrong DG. The pivotal role of off loading in the management of neuropathic foot ulceration. Curr. Diab. Rep. 2005; 5 (6): 423-9. Rathur HM, Boulton AJM. Pathogenesis of foot ulcers and the need for off loading. Horm. Metab. Res. 2005; 37: 61-8. Bohannon RW, Pfaller BA. Documentation of wound surface area from tracings of wound perimeters. Phys. Ther. 1983; 63: 1622-4. Diamond JE, Mueller MJ, Delitto A, Sinacore DR. Reliability of a diabetic foot evaluation. Phys. Ther. 1989; 69: 797-802. Armstrong DG, Hussain SK, Middleton J, Peters EJ, W Underlich RP, Lavery LA, et al. Vibration perception threshold: Are multiple sites of testing superior to single site testing on diabetic foot examination? Ostomy Wound Manage 1998; 44: 70-4. Frenette B, Mergier D, Ferraris J. Measurement precision of a portable instrument to asscess vibrotactile perception threshold. Eur. J. Appl. Physiol. 1990; 61: 386-91. Bloom S, Till S, Sonksen P, Smith S. Use of a biothesiometer to measure individual vibration and their variation in 519 non-diabetic subjects. Br. Med. J. 1984; 288: 1793-5. McGill M, Molyneaux L, Yue DK. Which diabetic patients should receive podiatry care? Intern. Med. J. 2005; 35: 451-6. Schon LC, Easley ME, Weinfeld SB. Charcot neuroarthropathy of the foot and ankle. Clin. Orthop. Relat. Res. 1998; 349: 116-31. Pinzur MS. Benchmark analysis of diabetic patients with neuropathic (Charcot) foot deformity. Foot Ankle Int. 1999; 20: 564-7. Ledermann H, Morrison WB, Schweitzer ME. MR image analysis of pedal osteomyelitis, distribution, patterns of sprend and frequency of associated ulceration and septic arthritis. Radiology 2002; 223: 747-55. Saltzman CL, Hagy ML, Zimmerman B, Estin M, Cooper R, et al. How effective is intensive nonoperative initial treatment of patients with diabetes and charcot arthropathy of the feet. Clin. Orthop. Rel. Res. 2005; 435: 185-90.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Skin Care: Chronic Ulcer Management
75
[23] Schaper NC, Nabuurs-Franssen MH. The diabetic foot: Pathogenesis and clinical evaluation. Semin. Vasc. Med. 2002; 2 (2): 221-8. [24] Medina A, Scott Paul G, Ghahary A, Tredget Edward E. Pathophysiology of chronic nonhealing wounds. Burn. Care Rehabil. 2005; 26 (4): 306-19. [25] Harding KG, Morris HL, Patel GD. Science, medicine and the future:healing chronic wounds. BMJ 2002; 324: 160-3. [26] Lobmann R, Ambrosch A, Schultz G, Waldmann K, Schiweek S, Lehnert H. Expression of matrix-metalloproteinases and their inhibitors in the wounds of diabetic and non-diabetic patients. Diabetologia 2002; 45: 1011-6. [27] Mast B, Schultz G. Interactions of cytokines, growth factors, and proteases in acute and chronic wounds. Wound Repair Regen. 1996; 4: 411-20. [28] Wetzler C, Kampfer H, Stallmeyer B, Pfeilschifter J, Frank S. Large and sustained induction of chemokines during impaired wound healing in the genetically diabetic mouse: prolonged persistence of neutrophils and macrophages during the late phase of repair. J. Invest. Dermatol. 2000; 115: 245-53. [29] Duraisamy Y, Slevin M, Smith N, Bailey J, Zweit J, Smith C, et al. Effect of glycation on basic fibroblast growth factor induced angiogenesis and activation of associated signal transduction pathways in vascular endothelial cells: possible relevance to wound healing in diabetes. Angiogenesis 2001; 4: 277-88. [30] Moore K, Ruge F, Harding KG. T lymphocytes and the lack of activated macrophages in wound margin biopsies from chronic leg ulcers. Br. J. Dermatol. 1997; 137: 188-94. [31] Loots M, Lamme EN, Mekkes JR, Bos JD, Middelkoop E. Cultured fibroblasts from chronic diabetic wounds on the lower extremity (noninsulin-dependent diabetes mellitus) show disturbed proliferation. Arch. Dermatol. Res. 1999; 291: 93-9. [32] Lee KH, Lee JH, Lee JD. Prevalence of fungal infection on foot in diabetic patients and correlation between diabetic ulcer and fungal infection. Korean J. Dermatology 2003; 41 (7): 908-15. [33] Jirkovska A, Fejfarova V, Hosova J. Analysis of the inflammation reactiion and selected indicators of imminity in patients with an infected diabetic ulcer. Cas. Lek. Cesk. 2002; 141 (15): 483-6. [34] Oyibo SO, Jude EB, Tarawneh I, Nguyen HC, Harkless LB, Boulton AJ. A comparison of two diabetic foot ulcer classification systems: the
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
76
[35] [36]
[37]
[38]
[39]
[40]
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
[41] [42]
[43]
[44]
[45]
[46]
P. C. Leung Wagner and the University of Texas wound classification systems. Diabetes Care 2001; 24: 84-88. Cuzzell J. Wound assessment and evaluation and diabetic ulcer protocol. Dermatology Nurs. 2003; 15 (2): 153-5. Treece KA, MacFarlane RM, Pound N, Game FL, Jeffcoate WJ. Validation of a system of foot ulcer classification in diabetes mellitus. Diabet. Med. 2004; 21: 987-91. Ramsey SD, Newton K, Blough D, McCulloch DK, Sandhu N, Reiber GE, Wagner EH. Incidence, outcomes and cost of foot ulcers in patients with diabetes. Diabetes Care 1999; 22: 382-7. Mendonca DA, Cosker T, Makwana NK. Vacuum-assisted closure to aid wound healing in foot and ankle surgery. Foot Ankle Int. 2005; 26 (9): 761-6. Marston WA. Dermagraft, a bioengineered human dermal equivalent for the treatment of chronic nonhealing diabetic foot ulcer. Expert Rev. Med. Devices 2004; 1 (1): 21-31. Oishi SN, Levin LS, Pederson WC. Microsurgical management of extremity wounds in diabetic with peripheral vascular disease. Plast Reconstr Surg 1993; 92: 485-92. Hasegawa M, Torii S, Katoh H, Esaki S. The distal based superficial sural artery flap. Plast. Reconstr. Surg. 1994; 93: 1012-20. Salsich GB, Mueller MJ, Hastings MK, Sinacore DR, Strube MJ, Johnson JE. Effect of Achilles tendon lengthening on ankle muscle performance in people with diabetes and neuropathic plantar ulcer. Phys. Ther. 2005; 85 (1): 34-42. Patel VG, Wieman TJ. Effects of metatarsal head resection for diabetic foot ulcers on the dynamic plantar pressure distribution. Am. J. Surg. 1994; 167: 297-301. Stewart J, Reed JF. An audit for Keller arthroplasty and metatarsophalangeal joint arthrodesis from national data. Int. J. Low Extrem. Wounds 2003; 2 (2): 69-73. Pinzur MS, Sage R, Stuck R, Kaminsky S, Zmuda A. A treatment algorithm for neuropathic (Charcot) midfoot deformity. Foot Ankle 1993; 14: 189-97. Beuker BJ, van Deurseu RW, Price P, Manning EA, van Baal JG, Harding KG. Plantar pressure in off-loading devices used in diabetic ulcer treatment. Wound Repair Regen. 2005; 13 (6): 537-42.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Skin Care: Chronic Ulcer Management
77
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
[47] Lavery LA, Vela SA, Lavery DC, Quebedeaux TL. Reducing dynamic foot pressures in high-risk diabetic subjects with foot ulcerations: A comparison of treatments. Diabetes Care 1996; 19: 818-21. [48] Leung PC, Wong MWN, Wong WC. Limb Salvage in Extensive Diabetic Foot Ulceration: An Extended Study Using a Herbal Supplement. Hong Kong Medical Journal 2008; 14(1):29-33. [49] Kessler L, Bilbault P, Ortega F, Grasso C, Passemard R, Stephan D, et al. Hyperbaric oxygenation accelerates the healing rate of non-ischaemic chronic diabetic foot ulcers: A prospective randomised study. Diabetes Care 2003; 26: 2378-82. [50] Huang P, Li S, Han M, Xiao Z, Yang R, Han ZC. Autologous transplantation of granulocyte colony stimulating factor mobilised peripheral blood mononudear cells improves critical limb ischaemia in diabetes. Diabetes Care 2005; 28 (9): 2155-60. [51] Richard J, Richard C, Daures J, Clouet S, Vannereau D, Bringer J, et al. Effect of topical basic fibroblast growth factor on the healing of chronic diabetic neuropathic ulcer of the foot. Diabetes Care 1995; 18: 64-9. [52] Leung Ping-Chung. Happy Aging. Chinese Journal Integrative Medicine 2009; 15(6): 466-469.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved. Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
In: Skin Care Editor: Sandra M. Hayes, pp.79-98
ISBN 978-1-61209-568-4 © 2011 Nova Science Publishers, Inc.
Chapter IV
The Role of Nonprescription Topical Treatment on the Skin Diana Badiu∗,1, Rafael Luque2 and Dănuţ Dincă3
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Dept. Biochemistry, Faculty of Natural and Agricultural Sciences, Ovidius University of Constanta, Constanta, Romania, and others
Abstract Natural and holistic treatments have been found to be extremely beneficial for maintaining problem-free and healthy skin. Treatments with cosmeceutical products such as herbal and homeopathic remedies are a safe and gentle alternative without the harmful side effects of synthetic chemicals often found in topical prescription medication. Several products are being manufactured today with the use of cosmeceutical ingredients, such as moisturizers and anti-aging treatments. Cosmeceuticals are likely to contain active ingredients like retinoids, hidroxy acids, antioxidants and other important constituents. These ingredients are a great aid in improving the appearance and delivery of essential nutrients to the skin that elp maintaining the skin’s vitality. ∗
E-mail: [email protected]. Department of Biochemistry, Faculty of Natural and Agricultural Sciences, Ovidius University of Constanta, 124, Mamaia Blvd, 900527, Constanta, Romania 2 Departamento de Quimica Organica, Universidad de Cordoba, Campus de Rabanales, Edificio Marie Curie (C- 3) Ctra Nnal IV, Km 396 Cordoba, Spain 3 Department of Otorhinolaryngology, Constanta Clinical Emergency Hospital, 145 Tomis Blvd. 900591, Constanta, Romania 1
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
80
Diana Badiu, Rafael Luque and Dănuţ Dincă This chapter review many interesting topics and ideas with the aim to improve the knowledge of chemists and/or physicians who desire to better understand the meaning of this unusual created word cosmeceutical.
Keywords: cosmeceutical, ingredients, damaged skin, treatment, products
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
List of Abbreviations UV AHAs DNA vitamin E GAGs FDA BHAs ROS ATP DMAE SOD NAC
ultraviolet alpha hydroxy acids deoxyribonucleic acid alpha- tocopherol glycosaminoglycans Food and Drug Administration beta hydroxy acids reactive oxygen species adenosine triphosphate dimethylaminoethanol superoxide dismutase N- acetyl cysteine
1. Cosmetic VS Drugs In contrast to youthful skin, dermal thinning, loss of dermal collagen and decreased lipid production are complicated by the effects of life-long sun exposure. These changes manifest as wrinkling, loss of elasticity, dryness and textural changes (Griffiths, 1999). Sometimes the appearance of the skin is affected by genetics, age, and unhealthy choices such as poor diet, too much alcohol, stress or harsh chemicals which characterize mature skin. One of the biggest culprits responsible for skin damage is long-term exposure to the sun, and most sun damage occurs before the age of twenty. The harmful effects of spending too much time in the sun is due to ultraviolet (UV) radiation, known as photoaging. It speeds up the rate of aging of the skin and in the same time increases the risk for developing skin cancer (Alam and Dover, 2001).
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
The Role of Nonprescription Topical Treatment on the Skin
81
By long-standing status, the world of topicals is divided into two opposed groups, cosmetics versus drugs. Stated simply: a topical product is a drug when it is used to prevent or treat a disease. Cosmetics, on the other hand, are used for beautification and enhancement of appearance. Thus far, the separation is neat and simple (Serri and Iorizzo, 2008). However, there is one further legal stricture which thoroughly confounds the issue, namely, that a cosmetic “not affect the structure and function of skin”. This statutory differentiation of drugs from cosmetics was probably appropriate for the state of knowledge, a half-century ago. Since then, the great increase in knowledge of the physiology of skin has brought the law and biology into conflict. The truth is that all topical substances, whether as simple as water or as complex as multi-ingredient moisturizes, inevitably will affect the structure and function of skin. Further, its action may be helpful in some circumstances and harmful in others. This lead to the oxymoron every topical formulation one can buy in a supermarket is by law, a drug. Taken literally, the consequences for industry are not only formidable, but also intolerable. Clearly, the status should be rewritten. Nonetheless, the term cosmetic has permanently entered our vocabulary. The differences between a drug and a cosmetic is obvious to professionals, based namely on intended usage. Thus, a drug is a medicine for disease and the other is designed for pleasure. These seem to be clearly antithetic. The trouble is that is no sharp dividing line between these two categories. Many maybe most topicals, whether labeled as drugs or cosmetics, are actually hybrids which share properties of both classifications. Between the poles of completely cosmetic and entirely drug products, there lies a wide spectrum of preparations which occupy on intermediate group it is this third domain to which the term “cosmeceuticals” applies (Vermeer and Gilchrest, 1996). In this broad zone, some topicals will be closer to drugs and some more proximate to cosmetics. Usually, it can’t be argued for additional legislation to accommodate by prudent language which stops short of drug claims. As usual, the Japanese are way ahead of the United States in resolving the legal contradictions. The authorities sensibly recognize a category of “quasi-drugs” which are, in fact, what we now call cosmeceuticals (Port et al., 1986). The term cosmeceuticals break down the artificial barrier between physicians and cosmetic scientists. This restores us to the practice of classical times, as when Galen, a Roman physician, served as both a cosmetician and a physician, in functions which complemented each other. He invented cold
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
82
Diana Badiu, Rafael Luque and Dănuţ Dincă
cream, an emulsion of olive oil and beeswax, which he recommended for keeping the skin healthy (Zhang et al., 1999). Cosmeceuticals, which contain no recognized medicaments, may, nonetheless, have medicinal value. The concept of cosmeceuticals has been strengthened by the current requirement to incorporate a vehicle control in double-blind studies of topical drugs. It is surprising how often substantial beneficial effects are obtained by the supposedly inactive control (Pelle et al., 1999).
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
2. Cosmeceutical Trends Cosmeceuticals are now one of the leading segments of natural skin care and the customer base is expanding. This could be that people have realized the difference between standard cosmetic products and non prescription treatment with cosmeceuticals. At the same time, the controversy surrounding the term cosmeceutical, which stands squarely between COSMEtic and pharmaCEUTICAL is still very vibrant. Across the globe, cosmeceuticals are still largely confined to the skin care sector, and within this sector the anti-aging market is the dominant market position. The cosmeceuticals category hosts an extensive and everexpanding range of biologically active ingredients, each promising drug-like benefits and a dramatic, rejuvenating effect on the skin. The category itself can be divided into several major groups based on active ingredients. Antioxidants represent the largest category (Katiyar and Elmets, 2001), followed by peptides (small proteins that stimulate the production of collagen and thicken the skin) (Hipkiss et al., 2001) and growth factors (compounds that act as chemical messengers between cells and play a role in cell division, new cell and blood vessel growth, and the production and distribution of collagen and elastin). The fourth group includes combination products such as multiple antioxidants, retinol plus antioxidants, growth factors plus vitamin C and other unique combinations that are now being mass marketed (Steenvoorden and Van Henegouwen, 1997). Some of today's popular ingredients include retinoids, which speed up the skin renewal process, and alpha hydroxy acids (AHAs), which are used in chemical peels (Stratigos and Katsambas, 2005). The rise of the cosmeceutical is proof that most cosmetics now recognize these "scientific-sounding" terms as beneficial in skin care, even if they were not sure of their exact proposed benefits. More recently, cosmeceuticals have been moving toward transdermal
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
The Role of Nonprescription Topical Treatment on the Skin
83
products containing collagen and even stem cell technology. Cosmeceuticals backed by expensive scientific research are ideally situated in the premium end of the market. There is a common notion or misconception that these ingredients are safer than synthetic ingredients. In actuality, there is no human clinical data to support the idea that natural or organic ingredients-derived from animals or the root, stem, leaves, flowers and fruit of plants are safer or even more effective than their synthetic counterparts. From a product development point of view, most compounds as they exist in their natural state cannot be easily formulated into skin care products. They must be chemically altered in some way before they can be incorporated into cosmetics. For instance, compounds such as retinol, vitamin C and soy are among those that require chemical alteration after which they are referred to as enhanced natural ingredients (Humbert, 2001). Enhanced natural ingredients tend to be more stable and have better bioavailability and more long-lasting effects on the skin compared to unaltered animal or plant products. This is why most cosmeceuticals contain chemically altered ingredients. There are several cosmeceutical ingredients such as collagen-boosting peptides and forms of vitamin A that are completely synthetic. These compounds are among the most potent anti-aging ingredients and have been used extensively by dermatologists. So, it's important for consumers to understand that synthetic ingredients are not necessarily bad. In fact, skin care products containing these ingredients are probably among the most effective in the marketplace.In contrast to the under-substantiation of products, a surplus of scientific claims and proof seems to be off-putting for beauty consumers. Too many scientific buzzwords in the marketing of cosmetics seem to confuse consumers about what works and what doesn't.
3. Cosmeceutical Ingredients Retinoids Retinoids are widely prevalent in the skin care business. Found in most living organisms as carotenoids or preformed vitamin A, retinoids are derivatives of vitamin A. Retinol is an essential ingredient and is the prototype of all existing retinoids. The effects of retinol are that it helps in proper growth and bone development. Retinol also helps strengthen and maintain the integrity of the epithelial surfaces and the mucosal surfaces (Serri and Iorizzo, 2008).
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
84
Diana Badiu, Rafael Luque and Dănuţ Dincă
Early civilizations recognized the benefits of vitamin A in treating and healing night blindness with diets rich in liver. In the 1930s, the clinical manifestations of vitamin A deficiency were recognized, and the idea to use vitamin A in the treatment of skin diseases was initiated. The advent of synthetic analogs of vitamin A in the 1970s brought new interest into their biological activity, especially on the skin. Since then, vitamin A and its derivatives have been useful in the treatment of many skin disorders, including ichthyosis, acne, and psoriasis. Vitamin A and its derivatives have 2 main functions: they act as antioxidants, and they activate specific genes and proteins. As antioxidants, they protect cells from oxidative damage by 3 different mechanisms: (1) scavenging peroxyl radicals, (2) quenching singlet oxygen, and (3) triplet-state sensitizers. Vitamin A also exerts a hormone like effect on the skin, activating specific genes through nuclear receptors (Kligman et al., 1969). The receptors bind to target sequences called hormone response elements on deoxyribonucleic acid (DNA) and activate gene transcription. Retinoic acid receptors bind all-trans retinoic acid, and retinoic X receptors bind 9-cis retinoic acid. Vitamin A and its derivatives inhibit lipid peroxidation, increase levels of alpha-tocopherol (vitamin E) and activate growth factors, oncogenes, keratins, and transglutaminases (Stege et al., 2000). Histologically, vitamin A and its derivatives induce epidermal thickening, increase mitoses, differentiate keratinocytes, and reduce the number of sebocytes. The dermis shows increased amounts of glycosaminoglycans (GAGs) and anchoring fibrils. Structural changes underlying the cosmetic benefits include correction of epidermal atrophy, deposition of new collagen, generation of new vessels, and enhancement of mitogenesis. This enhanced mitogenesis promotes the shedding of melanin-laden keratinocytes, resulting in bleaching and subsequent depigmentation. The ability of topical retinoids to improve the appearance of aged and photo-damaged skin by reducing wrinkles, decreasing laxity, bleaching hyperpigmented spots, and bringing about a smoother surface have been well studied and documented (Goodman, 1984). Importantly, the effectiveness of the non- Food and Drug Administration (FDA) approved cosmetic retinoids has been studied. Clinical and histological evidence suggests structural changes induced by excessive sun exposure can be partially reversed by the use of topical retinoids, such as retinaldehyde. They have been used for the treatment of photoaged skin with demonstrated beneficial clinical and histological effects (Varani et al., 1998). Because clinical correlates of these in vitro findings are not entirely convincing, with most studies being poorly constructed, the utility of these
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
The Role of Nonprescription Topical Treatment on the Skin
85
preparations for their stated uses is regarded by many authorities as marginal at best (Gendler, 1997).
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Hydroxy Acids Hydroxy acids are second to retinoids in being the most sought-after cosmeceutical products. Hydroxy acids are normally formulated in lower concentrations and are widely available in the mass market of cosmesceuticals. Hydroxy acids are organic forms of carboxylic acids and can be classified into two acid categories, AHAs and beta hydroxy acids (BHAs). Commonly known to be fruit acids, they can be derived from natural resources. There are various AHAs including lactic acid, glycolic acid, mandelic acid, citric acid, tartaric acid and malic acid. AHAs are often used for anti-aging treatments. By helping the skin appear more uniform and also maintain smoothness, AHAs have been shows to help the signs of aging to decrease (Draelos, 1997). With such healing properties, the AHAs not only cause the decrease signs of aging, they also enhance epidermal shedding. It has been claimed that AHAs promotes the synthesis of GAGs, while also promoting elastic fiber’s quality and increasing collagen density. However, this supportive evidence reached by scientists is still incomplete and debatable (Van Scott and Yu, 1989). BHAs are aromatic compounds. A reference of salicylic acid showed to have dermolytic properties and aids in several ichthyotic and xerotic disorders. Some other types of BHAs are betalipohydroxyacid, tropic acid and 2-hydroxy-5-octanoyl benzoic acid (Smith, 1994). Despite their popularity, the exact mechanisms of action of hydroxy acids remain unknown and are largely controversial; however, at least one aspect of its biological activities may be attributed to the inherent acid strength of the compounds. Studies show that AHAs may increase sensitivity to UV radiation and that sunscreen application may be advisable when these products are used (Van Scott and Yu, 1974).
Antioxidants The skin is frequently exposed to a constant exogenous damaging agents. Agents such as pollutants, and heat and/or cold are continually character of the skin. In addition to these external
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
assault of endogenous and UV radiation, drugs, air challenging the protective insults, the skin also has to
86
Diana Badiu, Rafael Luque and Dănuţ Dincă
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
cope with endogenous mitogens, most importantly reactive oxygen species (ROS) and other free radicals. These species are continuously produced during physiological cellular metabolism. To counteract the harmful effects of ROS, the skin is equipped with an antioxidant system to maintain equilibrium between the pro-oxidants, or damaging agents, and the antioxidants, or protective agents; these antioxidants intervene at different levels in the protective process. Many of the antioxidants used in the cosmeceutical formulations on the market today are listed below. Vitamin C Vitamin C is a known antioxidant and is a very necessary element for life. Vitamin C, also known as L-ascorbic acid, was discovered in the early 1930s and it has numerous roles. Vitamin C is essential for the hydroxylation of procollagen, lysine and praline. A deficiency in this vitamin can cause keratotic follicles, bleeding gums and purpura. As an antioxidant that is water soluble, vitamin C helps in capturing the free radicals and also regenerates vitamin E. It also regulates the stimulation and promotion of collagen synthesis. A depletion of vitamin C on the skin has been shown through studies to be caused by the irradiation of UV rays. Additionally, the cells altered by photodamage are normalized and improved with vitamin C. By incorporating vitamin C, the results show a reduced effect of photoaging on the skin and can also be used to stimulate collagen repair (Humbert, 2001). Ascorbigen, a skin-permeable form of vitamin C, may have anticarcinogenic effects (Wagner and Rimbach, 2009). However, the underlying mechanisms regarding its potential antiaging and UV-protective properties have not been fully elucidated (Steenvoorden and Van Henegouwen, 1997). Vitamin E The major lipophilic anti-oxidant in plasma, tissues and membranes is vitamin E. Vitamin E is compiled of 8 naturally occurring molecules consisting of 4 tocotrienols and 4 tocopherols (Maguire et al., 1992). These each exhibits vitamin E activities. Vitamin E should be topically applied before the skin is exposed to UV rays in order to diminish edema, erythema, sun burn cells, DNA adduct formation and immunosuppression from sunlight. Palm oil esters-in-water nanoemulsions with vitamin E have been formulated as potential nanocosmeceuticals (Chan, 1993).
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
The Role of Nonprescription Topical Treatment on the Skin
87
Panthenol Panthenol is the alcohol analog of vitamin B5. Panthenol is a water soluble humectant often used in the commercially made products such as skin creams, lotions, lipsticks and hair care preparations (Shuster, 1984). Lipoic Acid Lipoic acid is a unique free radical protector. It is fat and water soluble. Once lipoic acid crosses the cell membrane, it is broken down into dihydrofolic acid, which is also an antioxidant. Alpha lipoic acid also recycles other key antioxidants, such as vitamin C, vitamin E, and glutathione (Yarosh et al., 2001).
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Coenzyme Q Coenzyme Q is a derivative of quinone and is lipid-soluble. It can be found in the mitochondria and used for adenosine triphosphate (ATP) generation, which boosts energy (Thiele et al., 2001). Niacinamide Niacinamide or nicotinamide, is a basic amide that is a member of the vitamin B complex. It is used in the prophylaxis and treatment of pellagra. Niacinamide does not induce the peripheral flush that accompanies therapy with nicotinic acid. It is one of the newest vitamins in the marketplace. In vitro studies have shown anti–tumor activity on keratinocytes and suppression of UVB photocarcinogenesis. The main reason for its surge in popularity is its stability. Niacinamide is stable in the presence of oxygen, acid, and high temperatures, and it is inexpensive to formulate. Most of its known effects are the result of increased epidermal turnover and exfoliation (Chiu et al., 2007). Dimethylaminoethanol Topical preparations containing dimethylaminoethanol (DMAE) have been touted for their ability to improve skin firmness and to lift sagging skin. DMAE has been used as a dietary supplement and is associated with improving mental function and enhancing physical performance due in part to its ability to increase the neurotransmitter responsible for stimulating muscles. DMAE is able to diminish the cross-linking of proteins that occurs during aging, probably acting as a free-radical scavenger (Messager et al., 2001).
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
88
Diana Badiu, Rafael Luque and Dănuţ Dincă
Spin Traps Free radical spin traps are species that react with reactive free radicals to produce fairly stable, unreactive free radicals, thus blocking the free radicals from damaging cellular components. Note the following: 5,5-dimethyl-1pyrroline-N -oxide, 5-diethoxyphosphoryl-5-methyl-1-pyrroline-N-oxide and 1-hydroxy-2,2,6,6-tetramethyl-4-oxo-piperidine (Liao and Hiipakka, 1995). Melatonin Melatonin, a hormone secreted by the pineal gland, is known to have antimutagenic and oncostatic actions. This beneficial action of melatonin has been explained in terms of its ability to scavenge free radicals and to augment the activities of antioxidant enzymes. It has been shown to suppress UV radiation–induced erythema (Matsuda et al., 1996; Bangha et al., 1997; Kumar and Das, 2000).
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Catalase Catalase, an enzyme present in almost all cells of the human body, catalyzes the decomposition of hydrogen peroxide to water and oxygen. High amounts of this enzyme in the skin can impart antioxidative activity (Lin and Chang, 1997). Glutathione Glutathione is a tripeptide of glutamic acid, cysteine, and glycine. It is found in all active animal tissue. It is fundamental as an antioxidant, and significantly decreased amounts of glutathione found after UV exposures (Weber et al., 1999). Superoxide Dismutase Superoxide dismutase (SOD) is an enzyme that destroys superoxide (a highly ROS). SOD is a large molecule and has difficulty penetrating deep into the skin. In theory, once in the lower epidermis and dermis, SOD should decrease UV erythema and damage and act as an excellent antioxidant (Lin and Chang, 1997). Peroxidase Kulkarni and colleagues (1989) have developed a water-soluble fennel extract with measurable peroxidase activity. In vitro studies have shown far better consumption of oxygen than tocopherol, and they have also shown antibacterial activity.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
The Role of Nonprescription Topical Treatment on the Skin
89
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Glucopyranosides Resveratrol and polydatins are glucopyranosides found in many fruits and vegetables, the highest concentrations being found in grape skins, which synthesize these compounds in response to exposure to UVA and UVB and fungal pathogens. Biologic activities of these glucopyranosides include potent free radical scavenging activity, with cardioprotection and neuroprotection and inhibition of lipid peroxidation similar to that seen with vitamins C and E (Pelle et al., 1999). Polyphenols Polyphenolic compounds (e.g. catechins, flavonols, thioflavins, thearubigins), also known as epicatechins, are antioxidant in nature (Wei et al., 1995). These compounds, tested against human keratinocyte cells stressed by UVB irradiation, showed high antioxidative properties (Merfort et al., 1994). Many laboratories have shown that topical treatment or oral consumption of polyphenols inhibits chemical- or UV radiation–induced skin tumorigenesis in different animal models. It also possesses anti-inflammatory activity (Bernstein et al., 1986). One of the major and most chemopreventive constituents responsible for the biochemical or pharmacologic effects is epigallocatechin-3-gallate found in green tea (Nagata et al., 1998). Genistein, the isoflavone found in soybeans, and pycnogenol, an extract of the bark of French maritime pine Pinus pinaster, has been shown to significantly prolong tumor latency and to decrease tumor multiplicity with a potent ability to scavenge free radicals (Prager et al., 2002). Cysteine Several recent studies have shown that cysteine derivatives can protect against the negative effects of UV exposure. In particular, N- acetylcysteine (NAC) is shown to be an effective protector against UVB- induced immunosuppression, to modulate the expression of some oncogenes and tumor suppressor genes, and to increase the amounts of intracellular glutathione. Glutathione is known to be critical in protecting the body's cells against oxidative stress; however, taking glutathione itself does not raise the levels of glutathione in the blood as effectively as taking its precursor NAC. Current research has NAC in the center for measures to combat the aging process (Steenvoorden and Beijersbergen van Henegouwen, 1997).
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
90
Diana Badiu, Rafael Luque and Dănuţ Dincă
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Allantoin Allantoin promotes cell proliferation, aiding in the healing process. Allantoin has long been known to enhance the effectiveness and desirability of cosmetic creams and lotions by its action as a skin protectant. Allantoin has been incorporated into shampoos, lipsticks, shaving creams, suntanning products, bath foams, hair gels, baby powders, and various aerosol preparations. It has also been used in topical pharmaceutical markets (Ghersetich et al., 1994). Most recently, allantoin has been used in various dental preparations, such as toothpaste and mouthwash. Allantoin has been called a cell proliferant, an epithelization stimulant, and a chemical debrider. It is said to clean away necrotic tissue, hastening the growth of new healthy tissue (Moriwaki et al., 1999). Furfuryladenine Furfuryladenine or kinerase, is a natural plant growth factor that retards the aging process in plants. Cut leaves dipped in a solution that contains furfuryladenine remain green, while untreated leaves turn brown. It is marketed as the natural evolution of antiaging treatment with similar effects in vitro on human skin cells as that in plants, helping to slow and reverse alterations that naturally occur in the cell-aging process (Mills and Kligman, 1983). Uric Acid In the past, uric acid was generally looked upon as merely an end product of purine metabolism. More recently, uric acid has become increasingly recognized as an important biological antioxidant. Scientific studies have demonstrated that uric acid is a potent physiological antioxidant, playing a major role in both extra- and intra-cellular defense mechanisms. Although the precise biochemical mechanism is not completely determined, uric acid appears to have a sparing action in plasma ascorbate, probably by complexing transition metals such as iron and copper (Weber et al., 1999). Carnosine Carnosine or beta-alanyl-L-histidine, is a physiological dipeptide that can rejuvenate senescent cultured human fibroblasts. Carnosine has been shown to contain antioxidant, free radical- and metal ion–scavenging activities (Hipkiss et al., 2001).
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
The Role of Nonprescription Topical Treatment on the Skin
91
Essential Oils Extracts from olive oil can scavenge hydroxyl radicals better than other oils. In addition to the direct antioxidant effects of olive oil, extracts are also potent inhibitors of xanthine oxidase activity. Olive oil contains significantly more squalene than seed oils. Squalene is largely transferred to the skin, probably by scavenging singlet oxygen generated by UV light. Virgin olive oil applied to the skin after sunbathing could protect against skin cancer by slowing the growth of tumors (Badiu et al., 2010).
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
4. Product Innovation and Target Delivery In the cosmeceuticals area, in the anti-aging category in particular, as well as in the pharmaceutical arena, nanotechnology has played an important role in delivering active ingredients to the skin in both patch delivery and timedrelease application. The latest trend is to combine clinically proven ingredients with patented delivery systems, such as nanoparticles or nanospheres. Silicone elastomers can also absorb, entrap and release bioactives (Lyle, 2001). In addition, they can fill skin imperfections by forming small, soft microparticles. This reduces the visual impact of skin wrinkles. Unique antioxidants, antiinflammatory agents, immunostimulants and enhancers of molecular and cellular detoxification could also enter the panoply of new cosmeceuticals that can help consumers avoid age spots, dark circles, wrinkles and other clinical aspects of skin aging (Urbach, 1995).
5. Promising Anti-Aging Products Cosmeceuticals that carry the "natural" label are creating new opportunities as well as challenges because these products are not regulated by FDA. Due to the lack of regulatory oversight, "natural" skin care products in some cases are not as well tested and scrutinized compared to synthetic products and pharmaceuticals. Moreover, as product ingredients get stronger, with the recent introduction of stem cell technology for example, claims could become more exaggerated. As a result, cosmeceuticals are at risk of finding themselves under greater scrutiny from regulatory bodies.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
92
Diana Badiu, Rafael Luque and Dănuţ Dincă
Despite a favorable consumer outlook, the inevitable emergence of legislation will no doubt shape the industry in the years to come. Global regulators are still uncertain about cosmeceuticals and how to classify them. New European Union legislation proposed in June 2007 on the use of chemicals has called for restrictions on some active cosmetic ingredients, a move that is projected to be anti-innovative for industry. And if future regulations are introduced on a piecemeal regional basis, the lack of any global consistency may prompt companies, particularly multinationals to be wary of investing in the development of new products they can't market globally. Another future challenge is that products found to cause physiological changes to the skin may be placed under the definition of medicine and may eventually be reclassified as drugs. While the regulations regarding cosmetics are largely the same across developed countries worldwide, there are major variations in drug regulation. The reclassification of cosmeceuticals would again impose a tremendous barrier to manufacturers looking to capture a share of the global cosmetics and toiletries market. This change would undoubtedly slow product development and innovation-smaller companies would effectively be phased out by the escalating costs of development and testing, while multinationals might be put off by the possibility of a product they cannot market globally (Vermeer and Gilchrest, 1996). The market is broken down into segments for disease, appearance and fitness. The disease treatment segment currently maintains the largest share of the market. It consists of preventive and reactive healthcare for all the diseases of aging such as joint and bone health, Alzheimer's, sexual dysfunction, metabolic disorders, and eye and cardiovascular diseases. The appearance segment possesses the second largest share of the market. Facial rejuvenation, skin rejuvenation, hair care and body shaping products are the main components of this market. The fitness segment has the third largest market share and consists of bioregenerative, gym, spa and massage services. There is some overlap, however. For example, some products cover more than two segments, such as facial care, skin care, hair care, drugs, supplements, nutraceuticals, complementary and alternative medicine therapies, and cosmetic and fitness equipment (Vermeer and Gilchrest, 1996). In Japan and much of the Asia-Pacific market, cosmeceuticals are making inroads largely in the form of skin whitening and de-pigmentation products and powerful sunscreens. Japan's lead in innovation and product development may suggest the evolving future of cosmeceuticals (Badreshia- Bansal and Draelos, 2007). For example, Japanese consumers have already embraced the
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
The Role of Nonprescription Topical Treatment on the Skin
93
concept of the "skinceutical," where beauty-enhancing products are added to food. Also gaining ground, the Indian cosmeceuticals market is one of the fastest growing due to the increasing wealth among the middleclass. As a result, the Indian cosmetics and toiletries market has witnessed major changes both in terms of user perception and product availability during the past five years (Draelos, 2007).
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Conclusions and Future Research It may seem unimportant to contemplate doing anything about your complexions before reaching your thirties. However it is in our twenties that the effects of aging begin to be visible in our complexion. As we mature, biochemical changes occur in elastin and collagen, the connective tissues that give skin its firmness and elasticity. Genetics also play a part in this, which is why these changes occur at different times in different people. As skin becomes less elastic, it also becomes drier, and the fat padding begins to disappear. This causes the skin to sag and look less supple. Ultimately wrinkles will appear. Then one day, after glancing in the mirror you suddenly notice those crows feet creeping in around the corners of your immaculately decorated eyelids, or you notice that your lip potions have sadly waded into the spider like crevices above the lips. It is normally then, when decisions are made to go out and get a miracle cream or maybe a facial. The use of cosmeceuticals has drastically risen in recent years. This significantly increases the armamentarium of the clinician in improving the treatment of skin conditions. However, at times, claims of effectiveness lack convincing evidence, thus the industry is challenged to provide convincing evidence of the effectiveness of these compounds. More companies continue to invest money in research and product development pertaining to anti-aging and cosmeceuticals. On the innovation side, there are several ingredients seeking to alleviate the signs of skin aging by increasing energy production in cells, which in turn increases cells production rate of essential proteins such as collagen and keratin, and also increases cells rate of repair and protection. One such ingredient is a synthetic tripeptide that is claimed to increase ATP levels in vitro by as much as 150%. Clinical research combined with innovative development of new actives will keep the cosmeceutical segment of the cosmetics market interesting and exciting, while consumer education removes uncertainties and keeps the segment growing. The interactions between cosmeceuticals and skin are
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
94
Diana Badiu, Rafael Luque and Dănuţ Dincă
inevitable and thus careful preclinical or clinical evaluation of efficacy and safety is a prerequisite for the development of a specific product. Lastly, increased regulation does not have to be so ominous. In the end, strengthened regulations for ingredients may serve to reassure consumers of safety, while regulations surrounding advertising may further build the market by reassuring customers of product claims. Finally, remember that while the effectiveness of the non- FDA approved cosmetic retinoids has been studied and clinical and histological evidence suggests structural changes induced by excessive sun exposure can be partially reversed by the use of topical retinoids, clinical correlates of these in vitro findings are not entirely convincing. Most studies are poorly designed, and many authorities regard the utility of these preparations for their stated uses as marginal at best.
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
References Alam, M.; Dover, J.S. (2001). On beauty: evolution, psychosocial considerations, and surgical enhancement. Arch. Dermatol., 137(6),795807. Badiu D., Balu, A.M.; Barbeş, L.; Luque, R.; Niţă, R.; Radu, M.; Tanase, E.; Roşoiu, N. (2008). Physico-chemical characterisation of lipids from Mytilus galloprovincialis (L) and Rapana venosa and their healing properties on skin burns. Lipids, 43(9), 829 – 841. Bangha, E.; Elsner, P.; Kistler, G.S. (1997). Suppression of UV-induced erythema by topical treatment with melatonin (N-acetyl-5methoxytryptamine). Influence of the application time point. Dermatology, 195(3), 248-52. Badreshia-Bansal, S.; Draelos, Z.D. (2007). Insight into skin lightening cosmeceuticals for women of color. J. Drugs Dermatol., 6(1), 32-9. Bernstein, J.E.; Parish, L.C.; Rapaport, M.; Rosenbaum, M.M.; Roenigk, H.H. (1986). Effects of topically applied capsaicin on moderate and severe psoriasis vulgaris. J. Am.Acad.Dermatol.,15(3), 504-507. Chan, A.C. (1993). Partners in defense, vitamin E and vitamin C. Can.J. Physiol. Pharmacol., 71(9), 725-731. Chiu, P.C.; Chan, C.C.; Lin, H.M.; Chiu, H.C. (2007). The clinical anti-aging effects of topical kinetin and niacinamide in Asians: a randomized, double-blind, placebo-controlled, split-face comparative trial. J. Cosmet. Dermatol., 6(4), 243-249.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
The Role of Nonprescription Topical Treatment on the Skin
95
Draelos, Z.D. (2007). Skin lightening preparations and the hydroquinone controversy. Dermatol. Ther., 20(5), 308-13. Draelos, Z.D. (1997). Hydroxy acids for the treatment of aging skin. J. Geriatr. Dermatol., 5, 236-240. Gendler, E.C. (1997). Topical treatment of the aging face. Dermatol. Clin., 15(4), 561-567. Ghersetich, I.; Lotti, T.; Campanile, G.; Grappone, C.; Dini, G. (1994). Hyaluronic acid in cutaneous intrinsic aging. Int. J. Dermatol., 33(2), 119122. Goodman, D.S. (1984). Vitamin A and retinoids in health and disease. N. Engl. J. Med., 310(16), 1023-31. Griffiths, C.E. (1999). Drug treatment of photoaged skin. Drugs Aging,14(4), 289-301. Hipkiss, A.R.; Brownson, C.; Carrier, M.J. (2001). Carnosine, the anti-ageing, anti-oxidant dipeptide, may react with protein carbonyl groups. Mech. Ageing Dev., 122(13), 1431-1445. Humbert P. (2001). Topical vitamin C in the treatment of photoaged skin. Eur J.Dermatol.,11(2), 172-3. Katiyar, SK.; Elmets, C.A. (2001). Green tea polyphenolic antioxidants and skin photoprotection (Review). Int. J. Oncol., 18(6), 1307-1313. Kligman, A.M.; Fulton, J.E.Jr.; Plewig, G. (1969). Topical vitamin A acid in acne vulgaris. Arch. Dermatol., 99(4), 469-476. Kulkarni, A.P.; Chaudhuri, J.; Mitra, A.; Richards, I.S. (1989). Dioxygenase and peroxidase activities of soybean lipoxygenase: synergistic interaction between linoleic acid and hydrogen peroxide. Res. Commun. Chem. Pathol. Pharmacol., 66(2), 287-296. Kumar, C.A.; Das, U.N. (2000). Effect of melatonin on two stage skin carcinogenesis in Swiss mice. Med. Sci. Monit., 6(3), 471-475. Liao, S.; Hiipakka, R.A. (1995). Selective inhibition of steroid 5 alphareductase isozymes by tea epicatechin-3-gallate and epigallocatechin-3gallate. Biochem. Biophys. Res. Commun., 214(3), 833-838. Lin, S.Y.; Chang, H.P. (1997). Induction of superoxide dismutase and catalase activity in different rat tissues and protection from UVB irradiation after topical application of Ginkgo biloba extracts. Methods Find. Exp. Clin. Pharmacol., 19(6), 367-71. Lyle, W.G. (2001). Silicone gel sheeting. Plast. Reconstr. Surg., 107(1), 272275.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
96
Diana Badiu, Rafael Luque and Dănuţ Dincă
Maguire, J.J.; Kagan, V.; Ackrell, BA.; Serbinova, E.; Packer, L. (1992). Succinate-ubiquinone reductase linked recycling of alpha-tocopherol in reconstituted systems and mitochondria: requirement for reduced ubiquinone. Arc. Biochem. Biophys., 292(1), 47-53. Matsuda, H.; Higashino, M.; Nakai, Y.; Iinuma, M.; Kubo, M.; Lang, F.A. (1996). Studies of cuticle drugs from natural sources. IV. Inhibitory effects of some Arctostaphylos plants on melanin biosynthesis. Biol. Pharm. Bull., 19(1), 153-156. Merfort, I.; Heilmann, J.; Hagedorn-Leweke, U.; Lippold, B.C. (1994). In vivo skin penetration studies of camomile flavones. Pharmazie, 49(7), 509-11. Messager, S.; Goddard, P.A.; Dettmar, PW.; Maillard, J.Y. (2001). Determination of the antibacterial efficacy of several antiseptics tested on skin by an 'ex-vivo' test. J. Med. Microbiol., 50(3), 284-292. Mills, O.H.; Kligman, A.M. (1983). Drugs that are ineffective in the treatment of acne vulgaris. Brit. J. Derm., 108, 371-374. Moriwaki, Y.; Yamamoto, T.; Higashino, K. (1999). Enzymes involved in purine metabolism--a review of histochemical localization and functional implications. Histol. Histopathol., 14(4), 1321-1340. Nagata, C.; Kabuto, M.; Shimizu, H. (1998). Association of coffee, green tea, and caffeine intakes with serum concentrations of estradiol and sex hormone-binding globulin in premenopausal Japanese women. Nutr. Cancer., 30(1), 21-4. Pelle, E.; Muizzuddin, N.; Mammone, T.; Marenus, K.; Maes, D. (1999). Protection against endogenous and UVB-induced oxidative damage in stratum corneum lipids by an antioxidant-containing cosmetic formulation. Photodermatol. Photoimmunol. Photomed., 15(3-4), 115119. Port, R.B.; Paige, M.L.; Berstein, J.R.; Alvarez, G.R. (1986). The 'altered states' foreign body. Am. J. Dis. Child., 140(10), 972-973. Prager, N.; Bickett, K.; French, N.; Marcovici, G. (2002). A randomized, double-blind, placebo-controlled trial to determine the effectiveness of botanically derived inhibitors of 5-alpha-reductase in the treatment of androgenetic alopecia. J. Alter. Complement. Med., 8(2), 143-52. Serri, R.; Iorizzo, M. (2008). Cosmeceuticals: focus on topical retinoids in photoaging. Clin. Dermatol., 26(6), 633-5.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
The Role of Nonprescription Topical Treatment on the Skin
97
Shuster, S. (1984). The aetiology of dandruff and the mode of action of therapeutic agents. Br. J. Dermatol., 111(2), 235-42. Smith, W.P. (1994). Hydroxy acids and skin aging. Cosmet. Toilet., 109, 4148. Steenvoorden, D.P.; Beijersbergen van Henegouwen, G.M. (1997). Cysteine derivatives protect against UV-induced reactive intermediates in human keratinocytes: the role of glutathione synthesis. Photochem. Photobiol., 66(5), 665-71. Steenvoorden, D.P.; Van Henegouwen, G.M. (1997). The use of endogenous antioxidants to improve photoprotection. J. Photochem. Photobiol.B., 41(1-2), 1-10. Stege, H.; Roza, L.; Vink, AA.; Grewe, M.; Ruzicka, T.; Grether-Beck, S. et al. (2000). Enzyme plus light therapy to repair DNA damage in ultraviolet-B-irradiated human skin. Proc. Natl. Acad. Sci. (U S A.), 97(4), 1790-1795. Stratigos, A.J.; Katsambas, A.D. (2005). The role of topical retinoids in the treatment of photoaging. Drugs, 65(8), 1061-1072. Thiele, J.J.; Schroeter, C.; Hsieh, S.N. et al. (2001). The antioxidant network of the stratum corneum. Curr. Probl. Dermatol., 29, 26-42. Urbach, W. (1995). Cosmeceuticals.The future of cosmetics?. Cosmet. Toilet., 110, 33. Van Scott, E.J.; Yu R.J. (1989). Alpha hydroxy acids: procedures for use in clinical practice. Cutis., 43(3), 222-228. Van Scott, E.J.; Yu, R.J. (1974). Control of keratinization with alpha-hydroxy acids and related compounds. I. Topical treatment of ichthyotic disorders. Arch. Dermatol., 110(4), 586-90. Varani, J.; Fisher, G.J.; Kang, S.; Voorhees, J.J. (1998). Molecular mechanisms of intrinsic skin aging and retinoid-induced repair and reversal. J. Investig. Dermatol. Symp. Proc., 3(1), 57-60. Vermeer, B.J.; Gilchrest, B.A. (1996). Cosmeceuticals. A proposal for rational definition, evaluation, and regulation. Arch. Dermatol., 132(3), 337-340. Wagner, A.E.; Rimbach, G. (2009). Ascorbigen: chemistry, occurrence, and biologic properties. Clin. Dermatol., 27(2), 217-24. Weber, S.U.; Thiele, J.J.; Cross, C.E.; Packer, L. (1999). Vitamin C, uric acid, and glutathione gradients in murine stratum corneum and their susceptibility to ozone exposure. J. Invest. Dermatol., 113(6), 1128-1132.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
98
Diana Badiu, Rafael Luque and Dănuţ Dincă
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Wei, H.; Bowen, R.; Cai, Q.; Barnes, S.; Wang, Y. (1995). Antioxidant and antipromotional effects of the soybean isoflavone genistein. Proc. Soc. Exp. Biol. Med., 208(1), 124-30. Yarosh, D.; Klein, J.; O'Connor, A.; Hawk, J.; Rafal, E.; Wolf, P. (2001). Effect of topically applied T4 endonuclease V in liposomes on skin cancer in xeroderma pigmentosum: a randomised study. Xeroderma Pigmentosum Study Group. Lancet. 24(357), 926-929. Zhang, L.; Lerner, S.; Rustrum, W.V.; Hofmann, G.A. (1999). Electroporation-mediated topical delivery of vitamin C for cosmetic applications. Bioelectrochem. Bioenerg., 48(2), 453-461.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
In: Skin Care Editor: Sandra M. Hayes, pp. 99-115
ISBN 978-1-61209-568-4 © 2011 Nova Science Publishers, Inc.
Chapter V
Current Preventive Strategies to Reduce Surgical Site Infections by the Endogenous Flora Pascal M. Dohmen∗ Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Department of Cardiac Surgery, Heart Center Leipzig, University of Leipzig, Sachen, Germany
Abstract Surgical site infection is a mean issue in cardiac surgery, leading to prolonged hospitalization, and substantially increased morbidity and mortality. In the literature the incidence to develop sternal surgical site infection varies from 1.3 to 12.8%. One source of pathogens is the endogenous flora of the patient’s skin, which can contaminate the surgical site. A number of preoperative skin care strategies are performed to reduce bacterial contamination like preoperative antiseptic showering, hair removal, disinfection of the skin, adhesive barrier drapes, and antimicrobial prophylaxis. Furthermore we can also support the natural host defense by optimal intra-operative management of oxygen supply, glycemia, and ∗
Address reprint requests Prof. Dr. Pascal M. Dohmen, Department of Cardiac Surgery, Heart Center Leipzig, University of Leipzig, Struempellstrasse 39, D-04289 Leipzig, Germany. Telephone +49 341 865 1422 Fax +49 341 865 1452 E-mail : [email protected].
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
100
Pascal M. Dohmen temperature. This review overviews the recent literature about preventing SSIs in cardiac surgery.
Keywords: skin bacteria, antibiotic prophylaxis, antibiotic resistance, microbial sealant, surgical site infections.
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Introduction Surgical site infections (SSIs) are serious complications among cardiac surgery. The prevalence of SSIs has been reported to range from 1.3 to 12.8% [1,2,3,4], leading to a prolonged hospitalization, and substantially increased morbidity and mortality. The incidence variation is meanly due to the different patient’s population and the relatively risk profile to develop SSI. The most sever SSI in cardiac surgery is the post-sternotomy mediastinitis showing a mortality from 23% within one year of follow-up compared with a matched control patient population in which the mortality was only 5% [5]. In case the post-sternotomy mediastinitis involves a multi-resistant bacteria, such as methicillin-resistant Staphylococcus Aureus (MRSA) the hospital mortality is as high as 40% and the three years survival as low as 26.3% [6]. This of course is a highly selected patient population, showing a high mortality due to mediastinitis and not representative for a normal patient collective, in which the incidence of mediastinitis is as low as 0.7%. Nevertheless the mortality is as high as documented. The additional costs, due to the prolong hospital stay of patients suffering from SSIs, will be as high as 19.0 billion Euro each year to the European health services [7,8] These costs are only including the health costs, however temporary or permanent work incapacity, care costs and years of productive life lost are not calculated. Alfonso et al. [9] showed that these costs are 10 times higher compared with the health cost. Generally during cardiac surgery a sternotomy is needed to expose the heart, which is at risk to be contamination by the endogenous skin flora; usually aerobic gram-positive microbes [10]. Due to the increase complexity of surgical procedures performed nowadays and the increase number of patients with a serious co-morbidity, the risk of SSIs increases.
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Current Preventive Strategies to Reduce Surgical Site Infections … 101
Pathogenesis of Surgical Site Infection
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
For many SSIs, the source of pathogens is the endogenous flora of the patient’s skin [11,12]. As long as the skin is intact, it resist microbial invasion due to relative dryness, cell mediated immunity and antibody production from T-lymphocytes [13]. Therefore, microbial contamination of the surgical site is a necessary precursor to develop SSIs, however not every contaminated will finally result in an infected wound. The risk of SSIs conceptualized according to the following relationship. On the one hand side there is the amount of inoculated and virulence of bacteria. On the other hand side we have the natural host defense due to the innate immune system to eliminate bacteria. A surgical site infection will normally occur when the contamination of pathogens overcome the host defense system. Quantitatively, 105 microorganism per gram of tissue will be needed to increase markedly the probability to develop SSI [14], however in case prosthetic materials (such as heart valves, conduits or graft materials) are implanted only 102 microorganism per gram of tissue [15]. The presence of several bacterial species in wounds also correlates with increase SSI [16,17].
Reduction of Bacterial Contamination of the Surgical Site A number of preoperative skin care strategies can reduce the risk of contamination by endogenous skin flora at the surgical site.
Preoperative Antiseptic Showering A preoperative antiseptic shower or bath decreases skin microbial colony counts. Garibaldi performed a study which included more than 700 patients, using different preoperative antiseptic showers [18]. Chlorhexidine reduces the bacterial colony counts 9.0-fold, while povidine-iodine or tricarban-medicated soap reduced colony counts at the skin only 1.3- and 1.9-fold, respectively. Even these positive results due to preoperative showering, by reducing the skin’s microbial colony counts, there have no definitively correlation been shown to reduce SSIs rates in several studies [19,20,21].
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
102
Pascal M. Dohmen
Earnshaw et al. [22] showed in a randomized study (n=66) no difference in SSI between washing with chlorohexidine and washing with soap, however the follow-up was until hospital discharge and no washing information was provided to participants in the group washing with soap. Furthermore the number of patients was limited. Hayek et al. [23] compared also in a randomized trial with preoperative washing with chlorohexidine or soap (n=2015) and was able to report a significant reduction of SSIs if patients washed with chlorohexidine (RR 0.70, 95% CI 0.51 to 0.96). In another large trial of Wihlborg et al. [24] significant fewer SSIs were reported in the group who preoperative performed Chlorohexidine washing (n=541) compared with the control group without washing (n=437) respectively (9/541;1.7%) and (20/437;4.6%) (RR 0.36, 95% CI 0.17 to 0.79). Further randomized studies from Hayek et al. [25] showed significant difference between full body washing and partial washing (n=1093) in favor for whole body washing, respectively (1.7%) versus (4.1%) (RR 0.40, 95% CI 0.19 to 0.85).
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Hair Removal Body hair has been though to be a potential carrier of pathogens and therefore it should be removed from the surgical site [26]. There are different methods to remove hair such as shaving with a razor, using an electrical clipper; or applying a depilatory cream. A number of clinical trials compared various combinations of these preparatory techniques. In general, depilatory cream usage was most favorable to reduce the risk of SSI [27,28]. Although the use of depilatories has been associated with a lower risk of SSI than shaving or clipping, sometimes patients suffer from hypersensitivity reactions [29]. Furthermore depilatory creams can only be used in patients undergoing elective surgery and patient who are able to be mobilized. Seropian showed in the same study that SSI rates were as high as 5.6% in patients shaved by a razor compared with the use of depilatory creams 0.6%. The reason for this increased SSI risk could be due to the produced microscopic cuts, that later could serve as a foci for bacterial multiplication [30]. Another important issue is the timing to perform hair removal. During an emergency procedure, the razor, ideally by using an electrical clipper, will be performed immediately before surgery. During an elective procedure, however
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
Current Preventive Strategies to Reduce Surgical Site Infections … 103 clipping hair immediately before an operation has been associated with a lower risk for SSIs, rather than clipping the night before the operation, respectively 1.8% versus 4.0% [31]. Other studies however suggested that independent to the shaving method, hair removal was associated with increased SSIs compared to no hair removal [32]. Therefore it is still difficult to make final comments on the topic hair removal, however in case hair are removed care should be taken not to produce microscopic cuts in the skin.
Copyright © 2011. Nova Science Publishers, Incorporated. All rights reserved.
Skin Disinfection Disinfection of the skin is an important issue to reduce the concentrations of bacteria at the operative site. After preoperative use of skin antiseptics, an average of 1 log CFU (i.e. one 10x potency of microorganisms) remains on the skin [33]. This consists of the residual skin flora, mainly S. epidermidis, can easily migrate during surgery into the surgical wound and become causative factor of SSI. Disinfection of the patient’s skin is complicated due to the hair follicles, which is a large part of bacteria housing which mostly can only be reached incompletely by skin antiseptics [34]. Lilly et al. [35] showed a progressive reduction due to the “two-phase” disinfection as an appropriate method for achieving a higher degree of disinfection of operation sites. Due to repeated disinfection of the skin a further mean reduction of 90% or more in the yield of bacteria could be shown. This means that by the use of antiseptic preparations one can reduce in yield of resident flora to a low equilibrium level, however complete sterilization will never occur. Kampf et al. [36] showed that the best antimicrobial efficacy could be achieved with alcohol based antiseptic solutions. Ethanol at higher concentrations, 70%, showed to be the most effective treatment against naked viruses, whereas n-propanol was more effective against the resident bacterial skin flora. The combination of alcohols is suggested to have a synergistic effect. The promotion of alcohol-based disinfection, containing various emollients, is also a strategy to reduce skin damage and irritation. As the duration of cardiac surgical procedures are prolonged compared with surgical procedures of other disciplines, one needs alcohol based antiseptics [37] compared with to aqueous based antiseptic [38] for optimal skin preparation. Interestingly, the dry time is mentioned to be 3 minutes in case the skin preparation was performed on a hairless surface. Segal et al. [39] showed in a study including 209 cardiac patients a significant reduction of the incidence of
Skin Care, Nova Science Publishers, Incorporated, 2011. ProQuest Ebook Central,
104
Pascal M. Dohmen
SSI by using alcohol-iodophor solution compared with aqueous-iodophor solution, respectively 4% and 13% (P