Pediatric Neurosurgery (Neurosurgery by Example) [1st ed.] 0190617071, 9780190617073, 0190617098, 9780190617097, 019061708X, 9780190617080
Covers a wide range of pediatric neurosurgery topics and authored by a group of the field's leading experts Each ch
574 107 31MB
English Pages 313 Year 2019
Polecaj historie
![Pediatric Vascular Neurosurgery: Technical Nuances in Contemporary Pediatric Neurosurgery (Part 2) [1st ed. 2021]
3030747484, 9783030747480](https://dokumen.pub/img/200x200/pediatric-vascular-neurosurgery-technical-nuances-in-contemporary-pediatric-neurosurgery-part-2-1st-ed-2021-3030747484-9783030747480.jpg)
![Textbook of Pediatric Neurosurgery [1st ed.]
9783319721675, 9783319721682](https://dokumen.pub/img/200x200/textbook-of-pediatric-neurosurgery-1st-ed-9783319721675-9783319721682.jpg)

![Handbook of Neurosurgery [9th Edition]
9781684201389](https://dokumen.pub/img/200x200/handbook-of-neurosurgery-9th-edition-9781684201389.jpg)
![Cerebrovascular Neurosurgery [1st ed.]
9780190887742](https://dokumen.pub/img/200x200/cerebrovascular-neurosurgery-1stnbsped-9780190887742.jpg)
![Pineal Neurosurgery [1st ed.]
9783030531904, 9783030531911](https://dokumen.pub/img/200x200/pineal-neurosurgery-1st-ed-9783030531904-9783030531911.jpg)
![Pediatric Neurosurgery (Neurosurgery by Example) [1st ed.]
0190617071, 9780190617073, 0190617098, 9780190617097, 019061708X, 9780190617080](https://dokumen.pub/img/200x200/pediatric-neurosurgery-neurosurgery-by-example-1stnbsped-0190617071-9780190617073-0190617098-9780190617097-019061708x-9780190617080.jpg)
Table of contents :
Cover......Page 1
Series......Page 3
Pediatric Neurosurgery......Page 4
Copyright......Page 5
Contents......Page 6
Preface......Page 8
Contributors......Page 10
1. Communicating Hydrocephalus......Page 14
2. Obstructive Hydrocephalus......Page 24
3. Prematurity and Intraventricular Hemorrhage......Page 32
4. Spinal Cord Tethering......Page 44
5. Lipomyelomeningocele......Page 54
6. Spinal Dermal Sinus Tract......Page 60
7. Chiari Malformation with Syringomyelia......Page 70
8. Myelomeningocele......Page 78
9. Sagittal Synostosis......Page 86
10. Unicoronal Synostosis......Page 96
11. Inflicted Traumatic Brain Injury......Page 106
12. Traumatic Atlanto-Axial Dislocation......Page 114
13. Spastic Quadriplegia......Page 122
14. Extratemporal Refractory Epilepsy......Page 130
15. Hemispheric Refractory Epilepsy......Page 140
16. Ruptured Arteriovenous Malformation......Page 154
17. Moyamoya Disease......Page 162
18. Vein of Galen Malformation......Page 170
19. Pineal Tumor......Page 178
20. Medulloblastoma......Page 190
21. Hypothalamic-Chiasmatic Glioma......Page 200
22. Mesial Temporal Glioma......Page 212
23. Craniopharyngioma......Page 220
24. Diffuse Brainstem Glioma......Page 230
25. Posterior Fossa Ependymoma......Page 236
26. Middle Fossa Arachnoid Cyst......Page 244
27. Posterior Fossa Cyst and Hydrocephalus......Page 252
28. Occipital Encephalocele......Page 260
29. Nasal Dermoid......Page 270
30. Sinusitus with Subdural Empyema......Page 280
31. Ventricular Shunt Infection......Page 288
Index......Page 294
Citation preview
Pediatric Neurosurgery
ii
NEUROSURGERY BY EXAMPLE Key Cases and Fundamental Principles Series edited by: Nathan R. Selden, MD, PhD Volume 1: Peripheral Nerve Surgery, Wilson & Yang Volume 2: Surgical Neuro-Oncology, Lonser & Elder Volume 3: Spinal Neurosurgery, Harrop & Maulucci Volume 4: Pediatric Neurosurgery, Selden & Baird
Pediatric Neurosurgery Edited by
Nathan R. Selden, MD, PhD Campagna Professor and Chair Department of Neurological Surgery Oregon Health & Science University Portland, OR
Lissa C. Baird, MD Associate Professor and Head Division of Pediatric Neurosurgery Department of Neurological Surgery Oregon Health & Science University Portland, OR
1
iv
1 Oxford University Press is a department of the University of Oxford. It furthers the University’s objective of excellence in research, scholarship, and education by publishing worldwide. Oxford is a registered trade mark of Oxford University Press in the UK and certain other countries. Published in the United States of America by Oxford University Press 198 Madison Avenue, New York, NY 10016, United States of America. © Oxford University Press 2019 All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, without the prior permission in writing of Oxford University Press, or as expressly permitted by law, by license, or under terms agreed with the appropriate reproduction rights organization. Inquiries concerning reproduction outside the scope of the above should be sent to the Rights Department, Oxford University Press, at the address above. You must not circulate this work in any other form and you must impose this same condition on any acquirer. Library of Congress Cataloging-in-Publication Data Names: Selden, Nathan R., editor. | Baird, Lissa C., editor. Title: Pediatric neurosurgery /edited by Nathan R. Selden, Lissa C. Baird. Other titles: Pediatric neurosurgery (Selden) Description: New York, NY : Oxford University Press, [2019] | Includes bibliographical references. Identifiers: LCCN 2018040447 | ISBN 9780190617073 (paperback) Subjects: | MESH: Central Nervous System Diseases—surgery | Child | Infant | Neurosurgical Procedures | Nervous System Malformations—surgery | Glioma—surgery | Case Reports Classification: LCC RD593 | NLM WS 340.5 | DDC 617.4/80083—dc23 LC record available at https://lccn.loc.gov/2018040447 This material is not intended to be, and should not be considered, a substitute for medical or other professional advice. Treatment for the conditions described in this material is highly dependent on the individual circumstances. And, while this material is designed to offer accurate information with respect to the subject matter covered and to be current as of the time it was written, research and knowledge about medical and health issues is constantly evolving and dose schedules for medications are being revised continually, with new side effects recognized and accounted for regularly. Readers must therefore always check the product information and clinical procedures with the most up-to-date published product information and data sheets provided by the manufacturers and the most recent codes of conduct and safety regulation. The publisher and the authors make no representations or warranties to readers, express or implied, as to the accuracy or completeness of this material. Without limiting the foregoing, the publisher and the authors make no representations or warranties as to the accuracy or efficacy of the drug dosages mentioned in the material. The authors and the publisher do not accept, and expressly disclaim, any responsibility for any liability, loss or risk that may be claimed or incurred as a consequence of the use and/or application of any of the contents of this material. 9 8 7 6 5 4 3 2 1 Printed by Sheridan Books, Inc., United States of America
Contents
Preface vii Contributors ix 1. Communicating Hydrocephalus 1 Rowland Han and David D. Limbrick, Jr. 2. Obstructive Hydrocephalus 11 Lissa C. Baird 3. Prematurity and Intraventricular Hemorrhage 19 Catherine A. Mazzola and Tatiana Huk Sikorskyj 4. Spinal Cord Tethering 31 Nathan R. Selden 5. Lipomyelomeningocele 41 Christina Sayama 6. Spinal Dermal Sinus Tract 47 Nathan R. Selden 7. Chiari Malformation with Syringomyelia 57 Yiping Li and Bermans J. Iskandar 8. Myelomeningocele 65 Lissa C. Baird 9. Sagittal Synostosis 73 Mark Proctor and Ali Hazama 10. Unicoronal Synostosis 83 Amy Lee and Richard G. Ellenbogen 11. Inflicted Traumatic Brain Injury 93 Beth A. Costine-Bartell and Ann-Christine Duhaime 12. Traumatic Atlanto-Axial Dislocation 101 Douglas Brockmeyer 13. Spastic Quadriplegia 109 David Harter 14. Extratemporal Refractory Epilepsy 117 Vamsidhar Chavakula, Eun-Hyoung Park, and Joseph R. Madsen
v
vi
Contents
15. Hemispheric Refractory Epilepsy 127 Brian J. Dlouhy and Matthew D. Smyth 16. Ruptured Arteriovenous Malformation 141 Edward Smith 17. Moyamoya Disease 149 Edward Smith 18. Vein of Galen Malformation 157 Lissa C. Baird 19. Pineal Tumor 165 Tadanori Tomita 20. Medulloblastoma 177 Amy K. Bruzek, Shawn L. Hervey-Jumper, and Karin M. Muraszko 21. Hypothalamic-Chiasmatic Glioma 187 James Rutka and Angela Coppola 22. Mesial Temporal Glioma 199 Gerry Grant 23. Craniopharyngioma 207 Lissa C. Baird 24. Diffuse Brainstem Glioma 217 Nalin Gupta 25. Posterior Fossa Ependymoma 223 Frederick A. Boop and Jimmy Ming-Jung Chuang 26. Middle Fossa Arachnoid Cyst 231 Amy K. Bruzek and Cormac O. Maher 27. Posterior Fossa Cyst and Hydrocephalus 239 Peter J. Morone and John C. Wellons, III 28. Occipital Encephalocele 247 Molly Hubbard and Daniel Guillaume 29. Nasal Dermoid 257 Hugh J. L. Garton 30. Sinusitus with Subdural Empyema 267 Christina Sayama 31. Ventricular Shunt Infection 275 Christina Sayama Index 281
vi
Preface
Dear Reader, I am delighted to introduce this volume of Neurosurgery by Example: Key Cases and Fundamental Principles. Neurosurgical training and practice are based on managing a wide range of complex clinical cases with expert knowledge, sound judgment, and skilled technical execution. Our goal in this series is to present exemplary cases in the manner they are actually encountered in the neurosurgical clinic, hospital emergency department, and operating room. For this volume, Dr. Lissa C. Baird and I invited a broad range of expert contributors to share their extensive wisdom and experience in all major areas of pediatric neurosurgery. Each chapter contains a classic presentation of an important clinical entity and guidesreadersthroughtheprocessesofassessmentandplanning,decisionmaking,surgical procedure, aftercare, and complication management.“Pivot points”illuminate the changes required to manage patients in alternate or atypical situations. Each chapter also presents lists of“pearls”for the accurate diagnosis, successful treatment, and effective complication management of each clinical problem. These 3 focus areas will be especially helpful to neurosurgeons preparing to sit for the American Board of Neurological Surgery oral examination, which bases scoring on these 3 topics. Finally, each chapter contains focused reviews of medical evidence and expected outcomes, helpful for counseling patients and setting accurate expectations. Rather than exhaustive reference lists, chapter authors provide lists of high-priority additional reading recommended to deepen understanding. The resulting volume should provide you with a dynamic tour through the practice of pediatric neurosurgery, guided by some of the leading experts in North America. Additional volumes cover each subspecialty area of neurosurgery, using the same case- based approach and board review features. Nathan R. Selden, MD, PhD Campagna Professor and Chair Department of Neurological Surgery Oregon Health & Science University
vii
vi
Contributors
Frederick A. Boop, MD Department of Neurological Surgery University of Tennessee St. Jude Children’s Research Hospital Memphis, TN
Beth A. Costine-Bartell, PhD Department of Neurosurgery Massachusetts General Hospital and Harvard Medical School Boston, MA
Douglas Brockmeyer, MD Department of Neurological Surgery University of Utah, Primary Children’s Hospital Salt Lake City, Utah
Brian J. Dlouhy, MD Department of Neurosurgery University of Iowa Hospitals and Clinics Iowa City, Iowa
Amy K. Bruzek, MD, MS Department of Neurosurgery University of Michigan Ann Arbor, Michigan Vamsidhar Chavakula, MD Clinical Fellow in Surgery Department of Neurosurgery Brigham and Women’s Hospital Boston, MA Jimmy Ming-Jung Chuang, MD Department of Neurological Surgery University of Tennessee St. Jude Children’s Research Hospital Memphis, TN Angela Coppola, MD Division of Neurosurgery The Hospital for Sick Children Toronto, Ontario, Canada
Ann-Christine Duhaime, MD Department of Neurosurgery Massachusetts General Hospital and Harvard Medical School Boston, MA Richard G. Ellenbogen, MD, FCAS Department of Neurological Surgery University of Washington Seattle, Washington Hugh J. L. Garton, MD Department of Neurosurgery University of Michigan Ann Arbor, Michigan Gerry Grant, MD Department of Neurosurgery Stanford University Palo Alto, CA
ix
x
Contributors
Daniel Guillaume, MD Department of Neurosurgery University of Minnesota Minneapolis, MA
Yiping Li, MD Department of Neurological Surgery University of Wisconsin Madison, Wisconsin
Nalin Gupta, MD, PhD Department of Neurological Surgery University of California San Francisco UCSF Benioff Children’s Hospital San Francisco, CA
David D. Limbrick, Jr., MD, PhD Department of Neurosurgery Washington University School of Medicine St. Louis Children’s Hospital St. Louis, Missouri
Rowland Han, MD, MSCI Washington University School of Medicine St. Louis, Missouri
Joseph R. Madsen, MD Department of Neurosurgery Boston Children’s Hospital and Harvard Medical School Boston, MA
David Harter, MD Department of Neurosurgery New York University, New York New York, NY Ali Hazama, MD Department of Neurosurgery Boston Children’s Hospital and Harvard Medical School Boston, Massachusetts Shawn L. Hervey-Jumper, MD Department of Neurosurgery University of Michigan Ann Arbor, Michigan Molly Hubbard, MD Department of Neurosurgery University of Minnesota Minneapolis, MA Bermans J. Iskandar, MD Department of Neurological Surgery University of Wisconsin Madison, Wisconsin Amy Lee, MD Department of Neurological Surgery University of Washington Seattle, WA
x
Cormac O. Maher, MD Department of Neurosurgery University of Michigan Ann Arbor, Michigan Catherine A. Mazzola, MD Division of Pediatric Neurological Surgery Goryeb Children’s Hospital of Atlantic Health Systems Morristown, NJ Peter J. Morone, MD Department of Neurological Surgery Vanderbilt University Medical Center Monroe Carell Jr. Children’s Hospital Nashville, TN Karin M. Muraszko, MD Department of Neurosurgery University of Michigan Ann Arbor, Michigan Eun-Hyoung Park, MD Department of Neurosurgery Boston Children’s Hospital and Harvard Medical School Boston, MA
Contributors
Mark Proctor, MD Department of Neurosurgery Boston Children’s Hospital and Harvard Medical School Boston, MA
Matthew D. Smyth, MD Department of Neurosurgery, Washington University St. Louis Children’s Hospital St. Louis, Missouri
James Rutka, MD, PhD Division of Neurosurgery The Hospital for Sick Children, Toronto Ontario, Canada
Tadanori Tomita, MD Department of Neurosurgery Northwestern University Feinberg School of Medicine Ann & Robert H. Lurie Children’s Hospital of Chicago Chicago, Illinois
Christina Sayama, MD Department of Neurological Surgery Oregon Health & Science University Doernbecher Children’s Hospital Portland, Oregon Tatiana Huk Sikorskyj, R-NP Division of Pediatric Neurological Surgery at Goryeb Children’s Hospital of Atlantic Health Systems Morristown, NJ
John C. Wellons, III, MD, MSPH Department of Neurological Surgery Vanderbilt University Medical Center Monroe Carell Jr. Children’s Hospital Nashville, TN
Edward Smith, MD Department of Neurosurgery Boston Children’s Hospital and Harvard Medical School Boston, MA
xi
xi
Communicating Hydrocephalus Rowland Han and David D. Limbrick, Jr.
1
Case Presentation
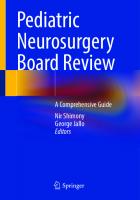
A boy is born at 37 weeks estimated gestational age to a 21-year-old G1P0 mother after a pregnancy complicated by oligohydramnios, intrauterine growth restriction, and pregnancy-induced hypertension. He is delivered by cesarean section for fetal decelerations and weighs 1490 grams with initial orbitofrontal circumference (OFC) of 30 cm. Apgar scores are 8 and 8 at 1 and 5 minutes, respectively. On exam, he is noted to have dysmorphic features including micrognathia, low set ears, and hypospadias. He requires oxygen on the first day of life but is quickly weaned to room air. Head ultrasound on day of life 6 reveals moderate ventriculomegaly involving the bilateral lateral ventricles, third ventricle, fourth ventricle, and prominence of the cisterna magna. Head MRI 2 days later yields similar findings with patency of the foramina of Monro, cerebral aqueduct of Sylvius, and fourth ventricle outlets (Figure 1.1). Over the following weeks, the patient’s OFC progressively increases, his fontanel becomes full, his cranial sutures begin to splay, and he is scheduled for ventriculoperitoneal (VP) shunt placement at 2 months of age. Questions
1. What is the likely diagnosis? 2. What are signs and symptoms of acute and chronic hydrocephalus? 3. What clinical and radiological parameters prompt diagnosis of hydrocephalus and of communicating versus non-communicating (obstructive) hydrocephalus?
Assessment and Planning
The diagnosis is congenital communicating hydrocephalus (CHC), suggested by apparent dilation of the entire ventricular system with progressive macrocephaly. Infants suspected of developing hydrocephalus should be monitored closely with daily physical examination and serial neuro-imaging (typically head ultrasound or magnetic resonance imaging [MRI]). Signs and symptoms of progressive hydrocephalus in young children include a full and bulging fontanel, splaying of the cranial sutures, OFC crossing growth curves, irritability, nausea/vomiting, and, in severe cases, upgaze paresis, irregular respirations with apneic spells, or bradycardia. OFC increasing at >2 cm/week or crossing the 97th percentile should prompt consideration of hydrocephalus treatment.
1
2
Pediatric Neurosurgery
Figure 1.1. MRI scans for the presented patient with communicating hydrocephalus, showing (A) sagittal T1, (B) sagittal T2, axial T1 through the (C) lateral ventricles, and (D) fourth ventricle, prior to any shunting procedures. Note the dilation of the entire ventricular system, the patency of the foramina of Monro, cerebral aqueduct of Sylvius, and fourth ventricle outlets, and the flow jet observed in the cerebral aqueduct on sagittal T2.
Radiological findings suggestive of hydrocephalus include ventriculomegaly, with ballooning of the ventricular system, thinning or upward bowing of the corpus callosum, and effacement of the cerebral sulci and Sylvian or interhemispheric fissures. Plain skull radiographs or CT might reveal splaying of the cranial sutures.
Oral Boards Review—Diagnostic Pearls
1. Hydrocephalus results from an imbalance between cerebrospinal fluid (CSF) production and reabsorption. It can be classified as communicating or non-communicating (obstructive), although individual cases generally have components of both.
2
Communicating Hydrocephalus
a. Traditionally,communicatinghydrocephalushasbeenattributedtoimpaired absorption of CSF through arachnoid villi (e.g., from inflammation) or elevation of cranial venous sinus pressure. Rarely, communicating hydrocephalus may result from excessive CSF production such as with a functional choroid plexus papilloma. Radiologically, communicating hydrocephalus is characterized by dilation of the entire ventricular system, including the fourth ventricle, and patency of the foramina of Monro, cerebral aqueduct of Sylvius, and fourth ventricle outlets (foramina of Lushka and Magendie). b. Non-communicating hydrocephalus occurs as a result of anatomic or functional obstruction to CSF flow. Obstruction can be present at the foramen of Monro, cerebral aqueduct, or fourth ventricle or its outlets. In non-communicating hydrocephalus, the ventricular system is often dilated proximal to the obstruction, while the ventricles distal to the obstruction remain relatively normal in size. 2. Possible symptoms of progressive hydrocephalus include headache, vomiting, lethargy, or irritability. Clinical signs may include a full and bulging fontanel, splayed sutures, papilledema, upgaze paresis/palsy, OFC greater than the 97th percentile, or frontal-occipital horn ratio (FOR) greater than 0.4–0.45. 3. Distinction between communicating hydrocephalus and hydrocephalus ex- vacuo may be difficult in some cases. The latter describes ventriculomegaly resulting from cerebral atrophy, rather than an imbalance in CSF physiology. Radiological characteristics suggesting true hydrocephalus rather than cerebral atrophy may include third ventricular enlargement, periventricular tissue interstitial edema on T2-weighted or FLAIR MRI, and cortical sulci effacement. Clinically, patients with hydrocephalus ex-vacuo typically lack the signs and symptoms of progressive hydrocephalus listed in item 2. The distinction between these 2 entities is important, as CSF diversion surgery is unnecessary for, and perhaps dangerous in, hydrocephalus ex vacuo. 4. Hydrocephalus may follow varying temporal and clinical courses, including rapid progression (acute hydrocephalus), slow progression (chronic hydrocephalus), or spontaneous arrest without intervention. Close monitoring is needed to identify patients requiring surgical intervention, particularly in cases of rapid progression with signs of increased intracranial pressure (ICP).
Questions
1. What are the goals of surgical treatment for CHC? 2. What are the surgical options for treatment, and when should definitive treatment occur? 3. What are the rationale and indications for different shunt designs and constructs?
3
4
Pediatric Neurosurgery
Decision Making
The primary goals of neurosurgical treatment of CHC should be to optimize neurologic function and neurodevelopment, avoid neurological deficits associated with CHC, and provide symptomatic relief from headaches, nausea, emesis, and other signs and symptoms of increased ICP. Surgical treatment for CHC requires CSF diversion to decompress the ventricles and normalize ICP. Most commonly, shunts divert CSF to the peritoneal cavity (ventriculoperitoneal, orVP, shunt), though alternate sites such as the right atrium of the heart (VA shunt) or the pleural cavity (V-pleural shunt) may be used in the setting of peritoneal scarring/infection or high central venous pressure, respectively. Infrequently used distal sites include the bone marrow, gall bladder, or other locations. Valve designs that may be used in CSF shunts include differential pressure, flow- control, or programmable valves, each with or without an antisiphon device. Factors that may influence choice of design include the patient’s propensity for under-or over- drainage, the surgeon’s preference or experience, and the perceived need for valve settingadjustments.Currentdata,however,suggestthatvalvedesigndoesnotsignificantly impact shunt survival. While shunts effectively reduce ICP and ventriculomegaly, they are associated with short-and long-term risks (refer to the section“Complications and Management”), and although CSF shunting is the most commonly employed treatment for CHC and the focus of this chapter, endoscopic third ventriculostomy (ETV) without or with choroid plexus cauterization (CPC) may be offered as an alternative to shunting in select cases. ETV and ETV-CPC will be discussed elsewhere in this volume. Questions
1. What steps should be taken in preparation and patient positioning for insertion of a VP shunt? 2. What technical adjuncts are available for assisting with optimal proximal shunt catheter placement, and what is the evidence for their use? 3. What complications are associated with CSF shunting?
Surgical Procedure
Insertion of a VP shunt is a major procedure performed under general anesthesia. The desired implants, including ventricular and distal catheters (with or without antibiotic impregnation) and valve type should be specified ahead of time.The surgeon also selects the side for the shunt depending on the patient’s intracranial anatomy and other cranial or extracranial factors (other recent surgical procedures, skin abrasions, etc.). Barring the presence of more specific factors, the right side is generally chosen for primary shunt insertion in infants given that the right cerebral hemisphere is likely to be non-language dominant, and given that distal shunt tubing in the right abdomen will not interfere with a later gastrostomy placement if indicated. The choice of anterior (coronal) or posterior (occipital or parieto-occipital) entry site may be based on factors such as intracranial anatomy, recent surgical procedures, skull shape, or surgeon experience or
4
Communicating Hydrocephalus
preference; however, the superiority of one or the other remains controversial and is a topic of continued investigation. For the surgery itself, the patient is positioned supine with a shoulder roll and the neck gently extended to assist in tunneling the distal catheter. If image-guidance is to be used, the device is assembled and registered to the patient’s head, and a trajectory for cannulating the ventricle is planned. The skin is then prepared using an antiseptic solution; many surgeons follow a standard QI protocol for skin preparation and other basic techniques (e.g., the Hydrocephalus Clinical Research Network protocol). The operation begins by making a curvilinear incision at the chosen cranial access site (anterior or posterior), making a burr hole, and placing a ventricular catheter into the lateral ventricle, typically positioning the tip of the catheter near the foramen of Monro. The surgeon may elect to use a free-hand technique or one of several technical adjuncts to assist in optimal catheter placement (ultrasound, endoscope, image-guidance, etc.); although none has been shown to definitively improve shunt survival, there are data to suggest that electromagnetic image–guidance may reduce malfunction rates. After placement of the ventricular catheter, CSF may be sent for culture at the time of catheter insertion to detect any preexisting infection if there is a clinical concern. The distal catheter is passed from the cranial incision to a ~1 cm incision made in the abdomen at a site chosen by the surgeon, based on patient anatomy or other factors (presence of gastrostomy tube or surgical scars). A parietal passing incision may be required to deliver the distal catheter from an anterior entry point to the abdominal incision. Peritoneal access may be achieved through mini-laparotomy, laparoscopy, minimally invasive port or trocar, or other method. After peritoneal access is established, the shunt is fully assembled, securing both the ventricular and distal catheters to the valve.Variability in implant construct (i.e., unitized shunt versus individual components) and surgical technique dictate the sequence of final shunt assembly. The valve itself fits within a subgaleal pocket fashioned for this purpose, and after verification of shunt patency and function the distal catheter is fed into the peritoneum. In general, ~30 cm of intraperitoneal tubing is implanted in small children to allow for continued growth. All incisions are then irrigated and closed.
Oral Boards Review—Management Pearls
1. Although definitive CSF diversion for CHC is typically accomplished using a VP shunt, other locations for distal catheter placement may be chosen for specific indications or if the peritoneum cannot be used. 2. Use of an anterior versus posterior entry site for the ventricular catheter remains a topic of investigation. 3. Propensity for under-or over-drainage, surgeon preference/experience, and the perceived need for valve setting adjustments often inform valve choice. Current data suggest that valve design does not significantly impact shunt survival. 4. The use of ETV and ETV-CPC as an alternative to CSF shunting will be discussed elsewhere in this volume.
5
6
Pediatric Neurosurgery
Pivot Points
1. Programmable valves, high-pressure differential pressure valves, or flow- control valves may aid in the prevention of CSF over-drainage, especially when used in conjunction with an anti-siphon device, particularly in infants presenting for primary VP shunt insertion in the setting of massive congenital ventriculomegaly. 2. The relationship between CSF shunting or ETV/ETV-CPC, ventricular size, and long-term neurodevelopment and quality of life is complex and likely multifactorial. Children with predominantly obstructive hydrocephalus (such as aquaductal stenosis) are excellent candidates for ETV-CPC and may never need ventricular shunting, particularly if they follow a good developmental course after ETV. 3. Children with concomitant congenital malformations of the abdomen can undergo primary ventricular shunt placement with an alternate distal catheter location, often the pleural space for children who are over 2 kg in weight and do not have pulmonary insufficiency.
Aftercare
Sterile dressings may be placed after shunt insertion, which can be removed 24 to 48 hours post-operatively. One to 2 doses of post-operative intravenous (IV) antibiotic may be used to prevent CSF infection. A shunt X-ray series, including skull, chest, and abdominal radiographs, may be obtained as baseline imaging and to determine whether immediate revision is required (Figure 1.2). Initial follow-up after shunt placement is usually within 1 month, at which time neuro-imaging may be ordered to confirm shunt functionandprovideabaselineforsubsequentevaluationofanysuspectedshunt failure episode, although clinical assessment is often sufficient to confirm function. Imaging may show ventricular size continuing to decrease over the course of the first year or
Figure 1.2. VP shunt X-ray series for the presented patient shows the VP shunt assembly. (A and B) AP and lateral skull X-rays, respectively. (C) AP chest and abdomen X-ray.
6
Communicating Hydrocephalus
Figure 1.3. MRI scan for the presented patient two years after implantation of the VP shunt. Sagittal T1 (A), axial T1 through the lateral ventricles (B), and axial T1 through the fourth ventricle (C) images show a dramatic reduction and near-normalization in ventricular size.
longer. Additional regular appointments are often scheduled on a several monthly or annual basis. While long-term imaging may detect subclinical shunt failure, there are concerns about radiation exposure in young children receiving serial CT scans. Thus, monitoring with MRI (Figure 1.3), and in particular rapid brain MRI, is advised. However, the effect of MRI on programmable valve settings must be anticipated, and such valves need to be verified after each MRI. Complications and Management
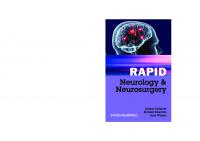
Shunt malfunction is common, occurring in 31.3% of children within the first year and 4.5% per year thereafter. The most common cause of shunt malfunction is proximal obstruction of the ventricular catheter, likely from reduced ventricular size and/or ingrowth of the choroid plexus. Other causes of failure include valve malfunction, kinking, fracturedtubing,shuntmigration,anddistalobstructionormalabsorption.Exceptinrare cases, shunt malfunction requires urgent surgical revision of the shunt. If the ventricles are of sufficient size and the anatomy is favorable, ETV/ETV-CPC can be considered in the setting of shunt malfunction, although success rates in this scenario are lower. Infection is an unfortunate complication of shunt surgery and occurs in up to 6.0% of cases. Shunt infection may be associated with ventriculitis, scarring and loculation of the ventricles, neurological morbidity, and, rarely, death. Risk factors for shunt infection include young age ( 2.5cm from anus, large size), hairy patches, hemangiomas, tails, and masses. Lumbar spine magnetic resonance imaging (MRI) without contrast is the diagnostic study of choice; however, contrasted imaging may be performed for any suspicion of tumor, infection, or vascular anomaly. T1 weighted imaging will demonstrate any associated fatty components, as well as fat associated with the filum or conus. T2 weighted imaging is important for delineation of the conus, nerve roots, and filum. High-quality axial T1 and T2 imaging may be helpful for evaluating any fatty tract traveling through dysraphic elements and the anatomical relationship to the conus. It is important to image the entire spine as dysraphism can be present at multiple levels, although this is uncommon. Spinal dysraphism is also associated with other findings, such as syringomyelia or Chiari malformation. This patient's MRI demonstrated a tethered spinal cord terminating in a spinal lipomatous malformation at L5–S1 with a syrinx in the distal cord extending from L1–2 to L5–S1. The lipomatous malformation expanded the sacral canal and extended through an enlarged left S5 neural foramen into the posterior pelvis, displacing the rectum anteriorly (Figure 5.1).
Figure 5.1. Sagittal T1 and T2 lumbar MR images showing a large lipomyelomeningocele filling the sacral canal and exiting it distally, with a small distal syrinx.
42
Lipomyelomeningocele
Questions
1. How do these clinical and radiological findings influence surgical planning? 2. What is the most appropriate timing for intervention in this patient?
Decision Making
There are three types of LMMC based on the relative anatomy of the lipoma and neural elements: (1) dorsal, (2) transitional, and (3) caudal or terminal. Because of obvious cutaneousabnormalities,infantsareoftendiagnosedbeforetheyaresymptomatic.Timing of surgical intervention is still controversial; however, many neurosurgeons advocate for surgery prior to deterioration as extrapolation studies on the natural history of LMMC patients suggest that a majority of patients will deteriorate over time. One of the highest morbidities of LMMC is bladder and bowel dysfunction, therefore presentation with these symptoms warrants surgery.The goal of surgery is to arrest progressive deterioration,and40–60%withprogressivedeficitshavebeenfoundtoimproveslightly,although those with fixed deficits almost never improve. Urinary continence is more likely to be preserved in children if operated on prior to 1 year of age (80% versus 50%). Surgical intervention for LMMC involves removal of lipomatous tissue with preservation of neural elements and function, identification of the defect in the lumbosacral fascia for release of lipomatous tethering, possible release of the filum terminale, and prevention of retethering of the spinal cord. Pre-operative planning using MRI is important to establish the extent of exposure needed to accomplish surgical goals. Also, defining the type of LMMC can help with surgical planning. If the patient presents with progressive deficits, surgery should be scheduled expeditiously but is rarely urgent or emergent. Pre-surgical neurophysiological testing may be used pre-operatively to assess urological and neurological functions; modalities include urodynamics (in patients old enough to participate), electromyography (EMG), somatosensory evoked potentials (SSEPs), and/or motor evoked potentials (MEPs). Questions
1. How much of the lipoma should be resected? 2. What are some ways to reconstruct the dura and obtain a watertight dural closure?
Surgical Procedure
Resection of a LMMC is a major procedure carried out under a general anesthetic with a Foley catheter in place and duplicate IV access. Neurophysiologic monitoring including EMG monitoring of the lower extremities and anal sphincter, as well as SSEPs and MEPs in older children or adults is essential in these complex cases. Patientsarepositionedproneonastandardoperatingroomtableongelrolls.Pressure pointsarepaddedappropriately.Neuromonitoringelectrodesareplacedaftergeneralanesthesia has been induced. Monitoring typically includes SSEPs (tibial nerve frequently
43
4
Pediatric Neurosurgery
used), MEPs (for the quadriceps, anterior tibial, gastrocnemius, and bilateral external anal sphincters), and both stimulated and free-run electromyograms.Younger children havemoreimmatureunmyelinatedfibersandthusmayrequiredouble-trainstimulation to obtain useful MEP amplitudes.The surgeon and anesthesiologist must communicate that neurophysiologic monitoring is being performed and ensure that no paralytics are given and the appropriate anesthetic is utilized. Thegoalofsurgeryismulti-facetedandincludesremovaloflipomatousmasswithpreservation of neural elements and function, identification of the defect in the lumbosacral fascia for release of lipomatous tethering, possible release of the filum terminale, and prevention of retethering of the spinal cord. The skin incision should be long enough to incorporate the craniocaudal dimensions of the lipomatous malformation. Laminoplasty or laminectomy can be performed for adequate dural exposure. The high-powered microscope is used during all microdissection of the lipoma from the placode and intradural detethering. An understanding of the morphology of LMMC is critical for identification and separation of the interface between the lipoma and the dura, as well as the lipoma from the spinal cord. Stimulated EMG allows for identification of functional nerve roots and delineation of nervous tissue from filum, scar, and fat elements. Resectionofthelipomacanbeaccomplishedusingelectrocautery,laser,orultrasonic aspiration. Identification of the lipoma-placode interface is easier in symmetric lesions than in asymmetric lesions. Once safe removal and detethering are accomplished, attention is then turned to dural closure. If the dural opening is large and primary repair is not possible, duraplasty is performed to ensure a watertight closure for prevention of future cerebral spinal fluid (CSF) leakage. Non-absorbable suture such as neurolon or Gortex are used to close the dura.Valsalva maneuver should be performed to ensure there is no obvious CSF egress from the closure. Some surgeons favor dural sealant as an additional bolster to a watertight closure. Laminoplasty is performed with small plates and screws in the older child whereas in the younger patient, the surgeon may prefer to use permanent suture. After copious irrigation with antibiotic impregnated solution, the lumbodorsal fascia is closed in a watertightfashion.Buriedinterruptedabsorbablesuturesareplacedinthedermisfollowed by skin suture of choice. In young children or those patient's with incontinence, a plastic barrier drape is placed between the incision and the anus to prevent contamination of the incision with stool.
Oral Boards Review—Management Pearls
1. LMMC patients carry high risk for deterioration of urologic and neurologic function. Prompt recognition of cutaneous markers followed by spinal MR imaging and timely intervention is important for optimal outcome. 2. Neurophysiologic monitoring is critical in all LMMC and complex spinal cord untethering cases. 3. Bladder and bowel dysfunction remain the primary morbidity in this patient population and intervention at or before first symptom onset is recommended.
44
Lipomyelomeningocele
Pivot Points
1. If a patient presents with progressive urologic or neurologic function and findings of a LMMC with tethered cord, early surgical intervention is warranted 2. If a patient presents with an ulcerated and draining hemangioma, the presence of a dermal sinus tract (although unlikely) should be ruled out as it can occur with LMMC. Any superficial infection should be appropriately managed prior to surgical intervention if there is no intradural infection.
Aftercare
Many surgeons prefer patients to lay horizontal for a period of 1–3 days post-operatively in order to decrease pressure in the lower thecal sac and decrease the risk of CSF leak. The indwelling Foley catheter is often kept in place while the patient remains flat in bed. Post-operativeantibioticsareadministeredforseveralpost-operativedoses,butusually no longer than 24 hours. After the Foley catheter is removed, it is important to ensure the patient can urinate and check post-void residuals. After the patient is allowed to ambulate, one should inspect for any sign of pseudomeningocele. Some patients experiencelow-pressureheadachesfromoverdrainagesymptoms,whichcanbetreatedwith hydration, lying flat as needed, and caffeine. A lumbar MRI is frequently obtained at least 3 months post-operatively to ensure that post-surgical changes have subsided. This can be used to serve as a new baseline. Some studies have shown that partial resection of the LMMC s is associated with higher incidence of symptomatic retethering compared to total resection. Complications and Management
Urinary dysfunction and constipation are common, generally transient, complications of this intervention. Urinary dysfunction may present as incontinence or retention. Retention is probably multi-factorial, resulting from the surgical procedure, the use of opioid pain medication, recumbency, and trauma from the Foley catheter. Urological consultation and replacement of the Foley catheter may be necessary in rare cases of severe retention. An aggressive bowel regimen can help with post-operative constipation, which is also likely to be multifactorial in nature. Wound infection and flap necrosis may be a higher risk in these patients because of large defects created with subcutaneous lipoma resection. To prevent this, many neurosurgeons will opt to avoid aggressive removal of the subcutaneous lipoma in order to avoid creation of a large dead space. Incision complication of any type has been reported to range anywhere from 2.5 to 56%, with an average of 25%. CSF leak is a major complication in this type of surgery, with reported rates between 2 and 47%. This is attributed to frequent inability to achieve primary closure of dura and necessaryuseofduralgrafts.Also,lipomatousmalformationsthattraversethefasciaoften lead to large muscle and fascial defects, thus the fascia cannot be primarily approximated in a watertight fashion.
45
64
Pediatric Neurosurgery
Oral Boards Review—Complications Pearls
1. Never remove the large subcutaneous lipoma at the time of intraspinal surgery due to higher likelihood of post-operative incision complication. 2. In cases with large defects of the lumbodorsal fascia, the paramedian lumbodorsal fascia may be incised to create relaxing incisions and facilitate a sliding midline closure. 3. CSF leakage through the skin warrants immediate surgical attention with exploration and closure revision.
Evidence and Outcomes
Prospective randomized controlled trials regarding the treatment of LMMC are lacking, though outcomes from several large case series have been reported. Many studies suggest that earlier treatment prior to symptom development yields better prognosis. Retethering rates are relatively high, and maximal safe resection of the lipomatous malformation should be the goal to minimize the risk of retethering. References and Further Reading
Muthukumar N. Congenital spinal lipomatous malformations Part I—Classification. Acta Neurochir. 2009; 151:179–188. Muthukumar N. Congenital spinal lipomatous malformations Part II—Clinical presentation, operative findings, and outcome. Acta Neurochir. 2009; 151:189–197. Pang D. Total resection of complex spinal cord lipomas: how, why, and when to operate? Neurol Med Chir (Tokyo). 2015; 55: 695–721. Sarris CE, Tomei KL, Carmel PW, Ghandi CD. Lipomyelomeningocele: pathology, treatment and outcomes A review. Neurosurg Focus. 2012; 33(4):E3. Tseng JH, Kuo MF, Tu YK, Tseng MY. Outcome of untethering for symomatic spina bifida occulta with lumbosacral spinal cord tethering in 31 patients: analysis of preoperative prognostic factors. The Spine Journal. 2008; 630–638. Byrne RW, Hayes EA, George TM, McLone DG. Operative resection of 100 spinal lipomas in infants less than 1 year of age. Pediatr Neurosurg. 1995; 23(4): 182–186. Herman JM, McLone DG, Storrs BB, Dauser RC. Analysis of 153 patients with myelomeningocele or spinal lipoma reoperated upon for a tethered cord. Presentation, management, and outcome. Pediatr Neurosurg. 1993; 19(5): 243–249.
46
Spinal Dermal Sinus Tract Nathan R. Selden
6
Case Presentation
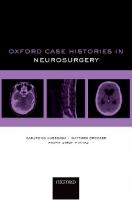
A 9-month-old female and her mother present to the child’s primary care pediatrician, complaining of a punctate skin opening at the midline lumbar spine (Figure 6.1). She states that the opening has been present since birth and has not changed in appearance, drained, or exhibited signs of inflammation. The child is well. She was born at full term via a normal delivery, after routine pre-natal care and an unremarkable pregnancy. Development has been normal, including rolling front to back and back to front, head elevation while prone, feeding, and social engagement. There is no family history of dysraphism or congenital abnormality. Mother took pre-natal vitamins from the 6th week of pregnancy. Referral is made to the pediatric neurosurgeon. Detailed neurological examination by the neurosurgeon is unremarkable, with normal tickle response, reflexes, muscle bulk and tone, and symmetric spontaneous movements in both lower extremities.The palate is visibly and palpably normal as is the external examination of the midline from the nasal tip to the coccyx, with the exception of the noted lumbar opening. Cranial shape is normal with a small flat fontanelle and no sutural splaying. Questions
1. What is the likely diagnosis? 2. What is the most appropriate imaging modality? 3. What are the most appropriate anatomical areas to image, and why? 4. What is the appropriate timing of the diagnostic work-up?
Assessment and Planning
The pediatric neurosurgeon suspects the presence of a dermal sinus tract. The differential diagnosis includes a benign sacral dimple, or a dysraphic sacral dimple suggestive of underlying closed dysraphism (typically a thickened filum terminale or other fatty malformation of the distal cord and/or filum). Although the exact incidences of these entities are not well defined, in general benign dimples are extremely common, dysraphic dimples rare, and dermal sinus tracts extremely rare.
47
84
Pediatric Neurosurgery
Figure 6.1. Photograph of the lumbar integument. A punctate opening is seen a few millimeters left of midline, just above the top of the gluteal fold, representing the superficial presentation of a dermal sinus tract.
Despite their rarity, concern about the presence of a dermal sinus tract drives referral for imaging and pediatric neurosurgery evaluation in many cases.This is because, in addition to the gradual and subtler loss of function typically encountered with minor closed dysraphism (often a fatty and thickened filum terminale causing tethered spinal cord), children with dermal sinus tracts (extremely rarely) present with fulminant pyogenic infection of the conus medullaris or cauda equina resulting in permanent, serious loss of function, including paralysis.
Oral Boards Review—Diagnostic Pearls
1. Physical examination is crucial to the accurate diagnosis of lumbosacral pits and dimples. a. Benign coccygeal dimple. True coccygeal dimples are generally round and smooth edged, 3 to 4 mm in diameter, and are positioned over the sharp tip of the coccyx on palpation. Although there is an intact skin plane at the bottom of a true sacrococcygeal dimple, it can be hard to see. b. Lumbosacral dimple. Dimples over the back of the sacrum may be associated with a thickened and fatty filum terminale or other closed dysraphism. These dimples are also round and smooth edged, and 3 to 4 mm or so in diameter. They may also be associated with a deviation or Y-shape of the upper gluteal fold. c. Pit or tract. Pits are much more focal and punctate than dimples, often having a “punched out” appearance. A true pit may contain one or two dark or dysplastic hairs and may have a small surrounding or satellite
48
Spinal Dermal Sinus Tract
hemangioma. Palpation may reveal underlying areas of firm or rubbery dermoid material and there may rarely be inflammatory signs. 2. Dermal tracts and other dysraphic lesions may occasionally be multiple. It is critical to inspect the entire midline integument, from the nasal tip to the distal sacrum. 3. Children presenting with repeated bouts of confirmed bacterial meningitis, often with variable skin flora, should undergo a meticulous examination of the dorsal midline, oropharynx, and nasal palate, looking for potential dermal sinus tracts or basal encephaloceles as a point of entry. 4. Contrary to standard teaching, dermal sinus tracts may occasionally occur within the upper midline gluteal fold (over the proximal sacrum but not the coccyx). Conversely, the majority of dimples appearing cranial to the fold do not represent dermal sinus tracts, but may be associated with closed dysraphism, such as a thickened filum terminale. 5. Spinal MR imaging is the only imaging modality sensitive and specific enough for diagnosis and surgical planning of lumbar dermal sinus tracts. MRimagingremainsthemostclinicallyuseful,sensitive,specific,anddefinitivediagnostic modality for dermalsinustractandotherdysraphicdefects.T1weightedimagesshowthe neural elements,dura,andothersupportingstructuresinexcellentdetail, andcommonly reveal the dermal sinus tract itself. Nevertheless, it is not uncommon for even experiencedneuroradiologiststomissthepresenceofthindermalsinustractsextendingintothe intradural space on MR imaging. It is extremely important to correlate the physical examination, including the exact dorsal level of the pit or tract, with the imaging (ideally with a superficial vitamin E skin marker). A tract in the superficial soft tissues over the spine in most cases can be tracked on sagittal images all the way to insertion on the dorsal aspect of the conus medullaris just cranial to insertion of the filum terminale. There is often a “beads on a chain”appearance of focal areas of thickening in the dermal sinus tract where accumulation of dermoid material in the tract is more prominent. Occasionally, enough material may focally accumulate to produce a clinically significant mass lesion.There may occasionallybeafocaldermoidmasswithintheconusmedullaris,itself.High-qualityaxial T2 images may allow the clinician to distinguish between the dermal sinus tract and the filum terminale (as well as the surrounding nerve roots of the cauda equina). Because complex dysraphic defects are not uncommonly multiple, may appear at different spinal levels, and may be associated with syringomyelia and/or a Chiari malformation, imaging the entire spine is indicated. Also, because of the potential for infection associated with dermal sinus tract, post-gadolinium images may be helpful. In the present case, MR imaging of the spine demonstrated a dermal sinus tract without any complicating features (Figure 6.2). Questions
1. How do these clinical and radiological findings influence surgical planning? 2. What is the most appropriate timing for intervention in this patient? 3. How should surgery be approached in a patient where intradural extension of the dermal sinus tract is not clearly demonstrated on MRI?
49
05
Pediatric Neurosurgery
(a)
(b)
Figure 6.2. (A) Sagittal T2-weighted MRI in the lumbar midline demonstrates the dermal sinus tract extending from the skin, passing underneath the L5 lamina, coursing through the lumbar subarachnoid space, and attaching to the dorsal conus medullaris just cranial to the insertion of the filum terminale. (B) Axial T2-weighted lumbar MRI demonstrates the dermal sinus tract in cross-section just dorsal to the tip of the conus medullaris.
Decision Making
A history of drainage of fluid, purulence, or cheesy “dermoid” material is virtually diagnostic of a dermal sinus tract, but in practice rarely observed. The presence of inflammatory changes or clinical findings of spinal infection mandate urgent to emergent antibiotics and surgical intervention. Since it is not uncommon for patients with lumbar dermal sinus tracts to present initially during late childhood with no history of infection, in the absence of infection, many practitioners plan surgery routinely. Surgical treatment for a lumbar dermal sinus tract requires total excision to untether the spinal cord and prevent any risk of future intrathecal mass or infection. In the present case, the tract was seen to extend to the conus medullaris, which is true in a substantial majority of cases. Even if intradural extension is not seen definitively on MR imaging, its presence must be suspected and surgery prepared to account for this occurrence. In infants and younger children, laminoplasty from the level of the tract at the integument cranially to the level of the conus medullaris is indicated, to preserve and restore the dorsal spinal bony elements. Parents should be consented for infection, neurological injury, CSF leak and meningitis, bony deformity, pain, and rarely the need for additional surgery. Questions
1. What is the significance of finding post-inflammatory arachnoiditis during the primary resection of a dermal sinus tract? 2. How should extension of dermoid material below the surface of the pia of the conus medullaris be managed surgically?
50
Spinal Dermal Sinus Tract
Surgical Procedure
Resection of a dermal sinus tract is a major procedure carried out under general anesthesia with a Foley catheter in place and duplicate IV access. EMG monitoring of the lower extremities and anal sphincter may be helpful, as well as somatosensory and motor evoked potentials in older children or adults, particularly where extension of the tract into the conus medullaris or a mass in the conus is suspected. Patients are positioned prone, generally in younger children on a standard table with gel rolls for the chest and hips. A slight amount of bed flexion at the level of the hips and lumbar spine may be added to encourage opening of the dorsal interspinous elements. It is important to prepare the skin and drape widely in order to assure access to the entire sinus tract, which most often extends to the conus medullaris. The goal of dermal sinus tract surgery is total resection of both the extra-and intradural components of the malformation, in order to prevent late recurrence and neurological morbidity. It is therefore important to dissect free and follow the dermal sinus tract in a single piece, extending from the pit on the skin. This begins by ellipsing out the skin containing the pit, and bluntly dissecting the soft tissue planes around the tract at each level, leaving its tubular walls intact and dermoid contents contained. At each anatomic level (fascial, bony and dural), there will be an oval ring transmitting the tract, which must be carefully removed or ellipsed circumferentially. Typically removal of half a lamina just cranial to the tract is adequate to release it from the bony dysraphic ring and to access the dorsal epidural space. If entry of the tract into the dural sac is then confirmed visually, it is necessary to expose the dural sac from the entry point to and over the level of the conus medullaris. The number of levels of exposure required can be observed on the sagittal MR imaging. In younger children, a laminoplasty of these levels may be performed using a small craniotome, or“footplate” drill, or alternatively with small Kerrison punches. Leaving the interspinous ligaments intact allows the entire dorsal bony complex in the area of exposure to be rotated out of the way as a piece, and considerably simplifies the reconstruction at the end of the procedure. The dural opening may be linear, except where it should ellipse out the dural ring transmitting the dermal sinus tract, and should extend from just caudal to the tract cranially to expose the conus medullaris. In virtually all cases, the dermal sinus tract will attach to the dorsal conus medullaris just cranially to its tip, and thus cranial to the attachment of the filum terminale (Figure 6.3). To prevent future recurrence and/or growth of an intraparenchymal mass in the conusmedullaris,theentiretractshouldberesected.Generally,thisisaccomplishedwith high-power microscopic dissection of the tract from the dorsal conus, flush with the pial surface. Extensions of obvious dermoid material below the pial surface, separated from cord parenchyma by a reliable plane of dissection, may also be removed, particularly with intact motor monitoring in place. The risk of this maneuver is probably justified by the avoidance of more serious morbidity related to the late recurrence of more difficult to resect intraparenchymal dermoid in a scarred field. Nevertheless, obvious injury to neural tissue in this delicate area should be strenuously avoided. In some cases, diffuse post-inflammatory changes and metastatic deposits of dermoid material may indicate prior infection and or dermoid rupture. If possible without neural injury, all dermoid material should be removed to avoid later recurrences. 51
25
Pediatric Neurosurgery
Figure 6.3. Operative photomicrograph, cranial to the right and caudal to the left. A red vessel loop has been placed under the filum terminale, just distal to the tip of the conus medullaris. The dermal sinus tract attaches to the dorsal aspect of the distal conus medullaris, just cranial to the attachment of the filum terminale, and extends to the skin (dissected free along its entire length). In general, the filum terminale in such cases will appear normal, and the cord may end at a normal level. Nevertheless, in the absence of any known negative consequence of cutting thefilum(otherthanrelatedtothesurgicalapproach),thefilumisgenerallytransectedwhile it is exposed for tract removal. Meticulous intradural hemostasis should be obtained. If any portion of the dermal sinus tract has been violated, with leakage of its inflammatory dermal contents, the thecal space should also be thoroughly flushed with irrigation fluid prior to linearprimaryclosure.Theintegrityoftheclosureshouldbetestedwithaventilator-induced valsalva.A thincontinuouslayerofduralsealantisoftenusedtosupplementtheduralclosure. Depending on the age of the patient, the laminoplasty bone may be replaced with suture or with a small laminar plating system. Meticulous fascial closure with tightly spaced interrupted sutures adds additional protection against CSF leak after surgery. In younger children, it is important to dress the incision in watertight fashion and separate it from the gluteal region with a post-operative adhesive drape, in order to avoid early contamination with gram-negative organisms from stool.
Oral Boards Review—Management Pearls
1. Total excision of all dermoid and tract material is necessary to prevent recurrence. 2. Intradural extension may be present even in cases where it is not clearly seen on MR imaging. A pit that is classical in appearance and location for dermal sinus tract should be explored at least to the lumbodorsal fascia and excised in
52
Spinal Dermal Sinus Tract
its entire extent, as verified at surgery. Only 10 to 20% of true lumbar dermal sinus tracts terminate superficially. 3. In younger children, multi-level lumbar laminoplasty is a standard approach to expose and resect the entire dermal sinus tract.
Pivot Points
1. If a patient presents with physical findings suggestive of a dermal sinus tract plus local inflammatory changes, fever and/or neurological or urological deficit, urgent broad-spectrum antibiotics and surgical exploration are indicated. 2. Imaging or surgical confirmation of intradural extension mandates surgical exploration and resection extending to the conus medullaris. 3. The presence of extensive post-inflammatory arachnoiditis indicates a history of past rupture or infection of the dermal sinus tract. If possible, all “metastatic” deposits of dermoid material should be removed to prevent recurrence.
Aftercare
Althoughnotsupportedbydefinitiveclinicalevidence,mostsurgeonsrequirethatthese patients be nursed in a horizontal position for the first 1 to 3 days, in order to discourage lumbar CSF leak or pseudomeningocele formation. During this time, the Foley catheter is generally left in place. On the day of mobilization, the Foley catheter is removed and serial inspection of the incision is made to rule out pseudomeningocele formation. The patient should be definitively confirmed to have returned to their pre-operative functional and gait status. Adequate bladder emptying should be confirmed by ultrasound prior to discharge. Routine peri-operative antibiotics are generally given, but not continued more than 24 hours post-operatively. Steroids are generally not necessary or indicated. Narcotic painmedicinemaybesupplementedwithnon-steroidalanti-inflammatorymedications on the first post-operative day. A single remote (1 to 2 years) follow up lumbar MRI, with and without contrast, is useful to rule out a rare intra-parenchymal (conus medullaris) dermoid reccurrence. Complications and Management
Urinary retention and constipation are common, generally transient, complications of this intervention. Urinary retention is likely to result from a combination of recumbency, pain, and narcotic medication. However, manipulation of the conus medullaris may contribute to temporary, or very rarely, permanent dysfunction. Avoidance of complicating factors, such as bladder distension, is important. In rare circumstances, discharge with a Foley catheter in placed combined with planned and supervised Foley catheter discontinuation as an outpatient may be useful.
53
45
Pediatric Neurosurgery
Lumbar pseudomeningocele with headache, or more rarely with minor neurological compromise from entrapped nerve roots or frank spinal fluid leak, occur in a very tiny fraction of patients. Patients should be carefully warned about leak, and treated emergentlyifitoccurs,topreventinfection.Eitherleakorpersistentpseudomeningocele should be treated with incision re-exploration under general anesthetic. If the dural closure was insufficient, re-do primary repair is reasonable, otherwise reinforced closure with a course of lumbar drainage and recumbency, is advisable. Neurological injury to the cauda equina or conus medullaris is rare following this procedure,andwouldrequirecarefuldiagnosis,inpatientmanagementandthenreferral to rehabilitation medicine. Any concern with urinary bladder function should prompt urology referral and potential ongoing follow-up to assure that a high-pressure bladder does not result in renal damage. Multilevel lumbar laminoplasty in infants and young children has rarely been associated with the late occurrence of spinal instability or hyperlordosis, the latter due to a “crank-shaft”phenomenon involving relatively diminished local growth potential in the lumbar dorsal elements. Very rarely, additional spinal surgery for alignment correction and/or fusion might be indicated.
Oral Boards Review—Complications Pearls
1. Careful peri-operative assessment and long-term follow-up of voiding will protect both bladder and renal function. 2. The presence of a persistent pseudo-meningocele at the operative site requires elective revision of the surgical closure, while CSF leak requires emergency repair to prevent contamination and bacterial meningitis.
Evidence and Outcomes
Prospectivecontrolledevidenceregardingthetreatmentoflumbardermalsinus tracts is lacking, in large part because of the very uncommon occurrence of this disorder, pres entation largely in children, and the rarity of the devastating variant presentation with intradural infection or mass and serious permanent neurological deficit. Case series have documented experience with various approaches to surgical management of these lesions, generally with excellent outcomes, very low recurrence rates, and minimal major or permanent surgical morbidity. References and Further Reading
Dermal sinus tract of the spine. Radmanesh F, Nejat F, El Khashab M. Childs Nerv Syst. 2010 Mar;26(3):349–357. doi: 10.1007/s00381-009-0962-z. Epub 2009 Aug 7. http://www.ncbi. nlm.nih.gov/pubmed/19662426 Spinal congenital dermal sinuses: a 30-year experience. Ackerman LL, Menezes AH. Pediatrics. 2003 Sep;112(3 Pt 1):641–647. http://www.ncbi.nlm.nih.gov/pubmed/12949296 Tethered cord syndrome in children: a single-center experience with 162 patients. Geyik M, Alptekin M, Erkutlu I, Geyik S, Erbas C, Pusat S, Kural C. Childs Nerv Syst. 2015 May 22. [Epub ahead of print] http://www.ncbi.nlm.nih.gov/pubmed/25997405
54
Spinal Dermal Sinus Tract
Congenital dermal sinus tract of the spine: experience of 16 patients. Mete M, Umur AS2, Duransoy YK, Barutçuoğlu M, Umur N, Gurgen SG, Selçuki M. J Child Neurol. 2014 Oct;29(10):1277–1282. doi: 10.1177/0883073813520501. Epub 2014 Feb 20. http://www. ncbi.nlm.nih.gov/pubmed/24563472 Diagnostic approach to recurrent bacterial meningitis in children. Wang HS, Kuo MF, Huang SC. Chang Gung Med J. 2005 Jul;28(7):441–452. http://www.ncbi.nlm.nih.gov/pubmed/ 16231527
55
65
Chiari Malformation with Syringomyelia Yiping Li and Bermans J. Iskandar
7
Case Presentation
A 16-year-old female presents with a 3-year history of occipital headaches, tingling sensations in the left arm, unsteadiness, and loss of temperature sensation in the finger tips. Her headaches are exacerbated by neck extension and Valsalva maneuvers such as coughing, sneezing, and bearing down during a bowel movement. She recently presented to the emergency room with painless burns on her hands, which she sustained while cooking. The headache is her most consistent symptom. There is no history of trauma or other congenital problems. There is no family history of neurological illness. On examination, the patient is fully alert and oriented, with normal speech and mentation. Extraocular eye movements are full without nystagmus, funduscopic examination does not reveal papilledema, the face is symmetric, the tongue is midline without fasciculations or atrophy, shoulder shrug is symmetric. Her motor strength is 5/5 in all 4 extremities. She exhibits reduced sensation to pain and temperature in both hands up to the wrist, worse on the left, with normal proprioception and light touch sensation, but asymmetric dysmetria. She has Lhermitte’s sign, hyperactive lower extremity reflexes, equivocal Babinski reflexes, and gait unsteadiness. Questions
1. What is the likely diagnosis? 2. What is the differential diagnosis? 3. What additional studies are appropriate?
Assessment and Planning
The pediatric neurosurgeon suspects the presence of a Chiari I malformation (CIM) withcervicalsyringomyelia.Thedifferentialdiagnosisincludescervicalspondylosis,overt or glacial occipito-cervical instability, occipital migraines or tension headaches, spinal vascular anomalies, and spinal cord tumor. The presence of Valsalva-induced (“tussive”) occipital headaches is highly suggestive of CIM, distinguishing it from other etiologies ofoccipitalheadaches,suchastensionheadacheormigraine.Associatedsyringomyeliais strongly suspected based on the presence of sensory loss in the hands, indicating central cordimpairment.Patientageandtheprotractednatureofthesymptomssuggestaslowly developing spinal pathology such as tumor and syringomyelia, compared to the sudden central cord deficits incurred, for example, by older individuals with cervical spondylosis.
57
85
Pediatric Neurosurgery
The constellation of symptoms requires additional imaging evaluation, with MRI being the diagnostic test of choice. If syringomyelia is present without sufficient explanation (such as the presence of an obvious CIM), then images with and without Gadolinium contrast may also be indicated. Imaging of the brain and entire spinal cord is indicated to rule out other etiologies of syringomyelia, such as tumor and arachnoiditis, andassociatedabnormalitiessuchashydrocephalusandspinalcordtethering.SinceCIM and syringomyelia rarely lead to life-threatening or sudden neurological complications, imaging is considered non-urgent and is carried out within weeks or months of diagnosis. However, urgent consideration should be given to syringes that extend into the brainstem (syringobulbia). Characteristic findings of Chiari I on MRI include tonsillar descent into the foramen magnum of 5 mm or more. Special attention is given to imaging evidence of craniocervical instability (e.g., basilar invagination, platybasia, and/or ventral brainstem compression). A syrinx consists of tubular cystic cavitation with associated expansion of the spinal cord. Syrinx fluid is T1 hypointense and T2 hyperintense without uptake of gadolinium. Occasionally, a pre-syrinx state exists, in which cord edema precedes cyst formation. However, when a pre-syrinx state is suspected, a spinal cord tumor and transverse myelitis should be ruled out. The utility of CSF flow studies and computational flow dynamics remains uncertain. Dynamic craniocervical imaging, to rule out underlying or additional craniocervical instability, should be considered in patients with dynamic neck pain or neurological symptoms.Typically, flexion-extension cervical radiographs are sufficient, although in some cases flexion-extension MRI also demonstrates neural compression associated with different anatomical positions. The prevalence of CIM on imaging (often defined by cerebellar tonsillar herniation of 5 mm or more below the foramen magnum) is estimated to be between 0.24 and 3.6%. The natural history of CIM remains uncertain, and less than a third of CIM cases diagnosed by imaging studies are considered symptomatic at the time of imaging.While surgeons uniformly avoid operative intervention on an asymptomatic CIM patient, most agree that the presence of an associated syrinx is an indication for Chiari decompression, as untreated syringomyelia may progress over months to years to produce progressive neurologic deficits. Depending on the study, up to a quarter of patients with radiographic evidence of CIM are found to have concomitant syringomyelia on screening spinal imaging, and the majority of syringes are cervical.
Oral Boards Review—Diagnostic Pearls
1. Chiari and syringomyelia symptoms share a long differential diagnosis list, and symptoms can often be non-specific and confusing. Accordingly, surgical success is determined in large part by patient selection. 2. A complete brain and spine MRI is indicated to rule out associated abnormalitiessuchashydrocephalus,tumor,arachnoiditis,aswellasadditional craniocervical junction anomalies. The utility of CSF flow studies and computational flow dynamics remains uncertain. 3. Syringomyelia can be preceded by a pre-syrinx state, in which only edema is present on the spinal MRI. This should to be distinguished from spinal cord tumors and transverse myelitis.
58
Chiari Malformation with Syringomyelia
Although the concomitant presence of CIM and syringomyelia almost always signifies that the CIM is the cause of the syrinx, this cannot be assumed, and other etiologies should be ruled out. Causes of syringomyelia can be congenital or acquired. Congenital causes include craniocervical abnormalities such as CIM, arachnoid cysts and other posterior fossa anomalies, basilar invagination and other subtle craniocervical instability conditions, spina bifida and Chiari II malformation, as well as spina bifida occulta and associated spinal cord tethering. Acquired or secondary causes include cervical canal stenosis, postoperative spinal cord tethering, post- operative or post-infectious arachnoiditis, hemorrhage, vascular malformations, and spinal cord tumors. Proposed mechanisms of syringomyelia formation in CIM include so called water- hammer, perivascular CSF dissection, pulse pressure, or suck effect alterations to CSF dynamics. Although there is no widely accepted consensus, each theory suggests a dynamic process related to pressure differentials between the CSF or microvasculature within different compartments of the neuroaxis (formed by adhesions, arachnoiditis, or obstructionsattheforamenmagnum),therebyresultinginsupraphysiologicforcesupon the posterior fossa and spine. Questions
1. What is the most appropriate timing of intervention? 2. What types of surgical procedures are indicated?
Preoperative Decision Making
Indications for surgery: There are 3 major and separate indications for surgery on CIM: debilitating symptoms referable to the CIM, neurological deficits referable to the CIM, and/or the presence of syringomyelia. Notably, the syrinx should be of sufficient size to be convincing. Often, simple dilation of the central canal can be misconstrued as a syrinx and is not a surgical indication. Furthermore, CIM patients, especially adults, may present with a complex of non-specific symptoms that have no localizing value and may complicate the decision to operate (e.g., chronic fatigue, whole body aches and pains, memory problems, “brain fog”, or frontal headaches). Surprisingly, some of these symptoms improve after Chiari decompression, but usually in the younger age group and when they are associated with other, typical CIM symptoms. Otherwise, the presence of such symptoms will increase the chance of Chiari surgery failure. Choice of type of surgery: Surgical treatment of CIMs consists of a suboccipital craniectomy and C1 laminectomy. A growing number of surgeons is now limiting the intervention to bony decompression, with or without stripping of the outer leaf of dura, as this minimizes the risk of complications such as CSF leak and aseptic meningitis. However, the majority still proceeds to a duraplasty, and approximately half of the surgeons who perform duraplasty also shrink 1 or both tonsils. Treating the syrinx independently,suchasusingsyringo-subarachnoid,syringo-peritonealorsyringo-pleural shunting is rare. Considering that the majority of Chiari-related syringes improve or resolve after CIM decompression, the added syrinx procedure is not considered necessary.
59
06
Pediatric Neurosurgery
Other disadvantages of syrinx shunts include (1) they do not address the underlying pathology, (2) they are prone to frequent obstructions long-term, and (3) they may result in arachnoiditis and, in turn, spinal cord tethering. Surgicalrisks:Patientsshouldbeinformedoftherisksofbleeding,infection,neurologic injury,CSFleak,meningitis,hydrocephalus,craniocervicalinstability,postoperativepain, andthepossiblefutureneedforadditionalsurgery(potentiallyincludingcranio-cervical fusion or the placement of a ventriculoperitoneal shunt), among others. Surgical Procedure
Type of procedure: The authors’ standard surgical technique for the treatment of CIM comprises a suboccipital craniectomy, C1 laminectomy, and harvest of nuchal ligament for expansive duraplasty. The arachnoid is usually left intact. Positioning: Once the patient is under general anesthesia and an airway is established, the head is fixed in a 3 pin (Mayfield) head holder. The patient is turned prone onto a standard table with gel rolls to support the chest and pelvis and to allow the abdomen to hang freely thus minimizing venous obstruction and intraoperative bleeding.The head is then positioned in capital flexion to expose the foramen magnum. In children under 2, in whom head fixation is not recommended, the neck is flexed gently allowing the head to be immobilized on a foam pad or gel and foam-padded horseshoe head holder. The arms are tucked and the shoulders can be taped caudally in patients with broad shouldersorshortnecks.Thepatientreceivesstandardperioperativeantibioticsandmechanical DVT prophylaxis. Corticosteroids and osmolar therapy are used by some, but not all, surgeons. Technical details: An incision is planned from the inion to the C2 spinous process. The incision is carried down through the skin and subcutaneous tissues to expose the posterior cervical fascia. The tissue is undermined laterally to aid in skin retraction. A “T” incision is made 0.5–1cm inferior to the inion through the posterior cervical fascia down to the occiput to expose the muscle fibers while providing a fascial cuff on the superior nuchal line for watertight closure. Some surgeons simply open the midline intermuscular plane. As the avascular midline raphe is developed, part of the nuchal ligament is harvested for duraplasty. The muscle attachments are released from the occipital bone and the posterior arch of C1. The exposure is carried out laterally to visualize the medial aspect of the occipital condyle, with care taken to avoid entering the sulcus arteriosus where the vertebral artery resides. A curette or Penfield 1 elevator is used to strip the attachments of the posterior atlanto-occipital membrane off the inferior edge of the occipital bone.The height of the craniectomy is estimated on the preoperative MRI scan by measuring the distance between the edge of the foramen magnum and the cerebellar hemisphere just superior to the tonsils.The width of the craniectomy corresponds to the width of the spinal canal. Two small burr holes are first created on both sides of the midline at the most cephalad portion of the intended craniectomy flap. This helps identify the midline keel, which is then drilled down carefully while connecting the 2 burr holes. The craniectomy flap is then turned inferolaterally in a crescent shape toward the foramen magnum ending just
60
Chiari Malformation with Syringomyelia
medial to the occipital condyles.The thickness of the occipital bone varies and thus must be taken into account during any drilling to prevent injury to the underlying dura. The dura is separated from the bone with a blunt instrument and the bone flap removed. C1 is then removed in similar fashion. If the tonsils extend even further into the spinal canal, additional more caudal laminectomy may be necessary to decompress them (although this is preferably avoided in order to reduce the risk of late post-operative upper cervical deformity). All bone edges are waxed to reduce bleeding, and all sharp edges reduced with the rongeur or drill. The posterior atlanto-occipital membrane is then resected.The dura is opened sharply just caudal to the foramen magnum, taking care not to violate the underlying arachnoid. The durotomy is extended rostrally in a “Y” shape fashion branching just past the level of the foramen magnum. Especially in children, preparation should be undertaken in case a large occipital sinus is encountered during the dural opening. Silver surgical clips or 4–0 suture material can be used to control sinus bleeding. Atourcenter,wedonotroutinelyopenthearachnoid,exploretheforamenMagendie, or coagulate the cerebellar tonsils, although these techniques have been well described in the literature. We keep the arachnoid intact and perform an expansile duraplasty by suturing the previously harvested nuchal ligament to the dura using a running 5–0 absorbable monofilament suture. Pericranium or dural substitutes may also be used for duraplasty. Some surgeons use a liquid sealant, such as fibrin glue, to reinforce the dural closure. The muscle and fascia are closed in multiple layers in a watertight fashion to avoid a postoperative pseudomeningocele and/or CSF leak. The skin is often closed using buried absorbable suture.
Oral Boards Review—Management Pearls
1. The CIM and syringomyelia association, if left untreated, can cause progressive neurological injury. However, the deterioration is slow and incremental, and rarely life-threatening. The only exception is when the syrinx extends into the brainstem (syringobulbia), to which urgent consideration is advised. 2. There continues to be controversy regarding the type of posterior fossa decompression best suited for the management of CIM with syringomyelia, including bone-only decompression, bony decompression followed by duraplasty, and bony decompression followed by duraplasty and tonsillar shrinkage.
Aftercare
Our patients are admitted to the hospital for a length of stay ranging between 2–4 days based on patient’s mobility, appetite, and pain control. Antibiotics are only administered immediately preoperatively.We schedule alternating doses of acetaminophen and ibuprofen to reduce the request for opiates, as described in Chiari decompression surgery literature. Muscle relaxants such as valium are also frequently used to improve muscle spasm-related pain. Patients are typically monitored in the intensive care unit during the first postoperative day and transferred to the general ward for mobilization on
61
26
Pediatric Neurosurgery
postoperative day 2, at which point the bladder catheter is discontinued. After discharge, the patient follows up in the neurosurgery clinic for routine incision check at 1–2 weeks. Definitive follow-up with repeat MR imaging, to assess the decompression and re-evaluate syrinx size, is done around 3 months after surgery. In the majority of patients, the syrinx will have noticeably diminished in size by this point. Complications and Management
Pain: Neck pain is a predictable occurrence in all patients and the primary reason for prolonged hospitalization following posterior fossa decompression. It is likely to be related to muscle spasm and occasionally aseptic meningitis, especially if the arachnoid is entered. Scheduled muscle relaxants, acetaminophen, and NSAIDs reduce the rates of opiate use and allow for earlier mobilization and discharge. CSF leak: Cervical pseudomeningocele, often accompanied by headache, CSF leak from the skin incision, and neurologic symptoms occur with less frequency. Although pseudomeningoceles alone can be managed conservatively, CSF leaks require immediate medical attention to prevent incision infection and meningitis. Persistent headaches and pain from a pseudomeningocele requires wound re-exploration with primary dural repair when applicable. In such cases, a period of perioperative lumbar CSF drainage may facilitate incision healing. Persistent CSF leak or pseudomeningocele formation may be indicative of hydrocephalus or pseudotumor cerebri, and may require CSF diversion. Neurological injury and craniocervical instability: Injury to the cerebellum, brainstem, spinal cord, or posterior inferior cerebellar arteries is extremely uncommon. These complications would require prolonged inpatient management and rehabilitation. Vascular injury may require additional diagnostic or surgical interventions. Iatrogenic instability of the craniocervical junction can arise, especially if bone drilling involves removing greater than 1/3 of the occipital condyles, which is not indicated in standard cases.
Oral Boards Review—Complications Pearls
1. Postoperativepseudomeningocelecanoftenbemanagedconservatively,while CSF leaks require urgent revision and surgical closure to prevent infection and meningitis. 2. The most common reasons for early or late surgical failures or symptom recurrence are inadequate decompression, subtle chronic craniocervical instability, undiagnosedpseudotumorcerebri,andhydrocephalus.Accordingly,athorough clinical and imaging evaluation is imperative prior to the decision to operate. Chiari surgery failure: Posterior fossa decompression may fail to alleviate symptoms or syringomyelia in the early postoperative period. Late failures or symptom/syrinx recurrence may also occur months to years after surgery.
62
Chiari Malformation with Syringomyelia
Causes of immediate postoperative failures:
1. Inadequatesurgicaldecompression:Thisincludesinadequateboneremoval,needtoopen the dura if a bone-only decompression was done, and presence of outlet foraminal obstructions (e.g., obstructive congenital veil in the foramen of Magendie). 2. Inaccurate diagnosis: Patients whose symptoms may not be related to the CIM or syringomyelia would obviously not improve after posterior fossa decompression.This highlights the importance of thorough history taking that would include the type and location of the headaches and association with other symptoms. 3. AssociatedCSFhydrodynamicproblems:Rarely,hydrocephalusorpseudotumorcerebri may be present preoperatively or develop postoperatively, which would require CSF diversion.
Causes of subacute or late recurrences (months to years):
1. Subtlecraniocervicalinstability,whichmightrequirecraniocervicalfusion:Thishighlights theimportanceofthoroughpreoperativeassessmentofmechanicalsymptoms(with neck movement), but more importantly, abnormalities in bone formation and morphometrics at the craniocervical junction (platybasia, basilar invagination, ventral compression, etc.). 2. Bone formation:Ininfantsandtoddlers,restenosisoftheforamenmagnummayoccasionally occur via new bone formation at the operative site. 3. Intradural adhesions: Arachnoiditis and scarring of the tonsils, brainstem and spinal cord tissues may occur in the late postoperative period, and is possibly more likely in the setting of direct tonsillar manipulation, intraoperative bleeding, and other unexpected intradural complications. 4. Unknown: Rarely, CIM decompression does not relieve syrinx symptoms or reduce syrinx size for an unknown reason, in which case a syrinx shunt can be considered. Evidence and Outcomes
Although most pediatric neurosurgeons tend to treat CIM and associated syringomyelia with posterior fossa decompression, most of the evidence published to date relies solely on retrospective single center series. Furthermore, although the literature almost uniformly suggests that the vast majority (up to 80%) of CIM/syringomyelia patients treated surgically show long-term clinical and radiographic benefit, including Karnofsky scores and quality of life and satisfaction measures, the choice of surgical technique remains controversial. Strong collaborations between the neurosurgical community and patient advocacy groups (the American Syringomyelia and Chiari Alliance Project, the Chiari and Syringomyelia Foundation, Conquer Chiari, and others) has led to the initiation of various multi-center studies and registries designed to study outcome measures in relation to type of surgical intervention, imaging diagnostics, and pathophysiology. We hope that these efforts will lead to answers to the most important questions and controversies in the near future.
63
46
Pediatric Neurosurgery
Pivot Points
1. Mild dilatation of the central canal is a normal variant and should not be confused with syringomyelia or be an independent indication for surgery. 2. Attention should be given to craniocervical junction anomalies that indicate chronic instability (basilar invagination, etc.), which depending on severity, may result in surgical failure and necessitate a craniocervical fusion as a part of the primary treatment plan. 3. Attention should be given to ventricular size and symptoms and signs of hydrocephalus prior to deciding on a posterior fossa decompression. Posterior fossa decompression in the setting of frank, untreated hydrocephalus is considered by some to be hazardous, suggesting that CIM is a secondary phenomenon. In some situations, surgeons observe hydrocephalus with obstructive features secondary to the CIM, and accordingly perform a CIM decompression first. 4. In patients with symptomatic CIM, in the absence of syrinx, some surgeons will incise the outer leaf of the dura in the midline, peel it back, and resect it, without opening the inner leaf or exposing the arachnoid. So-called “extradural Chiari decompression” has a lower primary complication rate but also higher recurrence and re-operation rate.
References and Further Reading
Kahn EN, Muraszko KM, Maher CO. Prevalence of Chiari I malformation and syringomyelia. Neurosurg Clin N Am. 2015 Oct;26(4):501–507. doi: 10.1016/j.nec.2015.06.006. Review. PubMed PMID: 26408058. https://www.ncbi.nlm.nih.gov/pubmed/26408058 Tubbs RS, Beckman J, Naftel RP, Chern JJ, Wellons JC 3rd, Rozzelle CJ, Blount JP, Oakes WJ. Institutional experience with 500 cases of surgically treated pediatric Chiari malformation Type I. J Neurosurg Pediatr. 2011 Mar;7(3):248–256. doi: 10.3171/2010.12.PEDS10379. PubMed PMID: 21361762. https://www.ncbi.nlm.nih.gov/pubmed/21361762 Rocque BG, George TM, Kestle J, Iskandar BJ. Treatment practices for Chiari malformation type I with syringomyelia: results of a survey of the American Society of Pediatric Neurosurgeons. J Neurosurg Pediatr. 2011 Nov;8(5):430–437. doi: 10.3171/ 2011.8.PEDS10427. PubMed PMID: 22044364. https://www.ncbi.nlm.nih.gov/ pubmed/16734077 Litvack, Z.N., Lindsay, R., Selden, N.R. (2013). Dural splitting craniocervical decompression for Chiari I malformation in pediatric patients: Clinical outcomes, healthcare costs and resource utilization. Neurosurgery, doi: 10.1227/NEU.0b013e31828ca1ed.
64
Myelomeningocele Lissa C. Baird
8
Case Presentation
A neurosurgical consultation is placed for a female newborn infant with a prior fetal diagnosis of lumbar myelomeningocele. She was born at 38 weeks gestation via uneventful cesarean section. During prenatal consultation, her mother had given a history of unplanned pregnancy and initiation of prenatal vitamins approximately 3 weeks after conception. Fetal ultrasound and MRI had demonstrated lumbar myelomeningocele, Chiari II malformation, and mild ventriculomegaly.The pregnancy was otherwise complicated by mild hypertension in the third trimester. Upon delivery, the myelomeningocele is immediately covered with a moist, non- adhesive dressing and a non-permeable covering.The baby is placed prone to avoid mechanical trauma to the exposed neural tissue and transported to the neonatal intensive care unit. Detailed neurologic examination reveals an open lumbar myelomeningocele with a visible placode and intact membranes. No cerebrospinal fluid leakage is noted. The anterior fontanel is flat and soft, and the coronal sutures are not splayed. Sensorimotor functionisassessed,andthebilaterallowerextremitiesdemonstratesymmetricandgood movement through the knees, with no movement noted at the ankles. The baby does not withdraw to pinprick stimulation at the feet, ankle reflexes are absent, and club foot deformity is noted. Questions
1. What further work-up should be completed prior to treatment of the myelomeningocele? 2. What is the appropriate timing of the surgical repair? 3. What therapeutic interventions should be instituted immediately after birth?
Assessment and Planning
An accurate initial neurologic assessment is critical in order to monitor for any future progressive deficit. The approximate spinal level of the defect is noted, and spontaneous movement, response to stimulation, and reflex testing are undertaken. The neurological level for this patient corresponds to approximately L3. Assessment of the myelomeningoceledeterminesextentoftheskindefect,circumferenceandshapeofthe
65
6
Pediatric Neurosurgery
(A)
(B)
Figure 8.1. Lumbar myelomeningocele in a newborn infant. lesion, and leakage of any cerebrospinal fluid. Any gross deformities of the spine, hips, or lower extremities are identified (Figure 8.1). Hydrocephalus may be present at birth or may develop in the postnatal period. A baseline head circumference and head ultrasound are performed on the first day of life, and any symptoms or signs of elevated intracranial pressure are noted. It is uncommon for these patients to require urgent intervention for hydrocephalus. Surgical treatment, when indicated, should be delayed until after the myelomeningocele repair whenever possible (Figure 8.2). An open neural tube defect carries an immediate risk for infection to the central nervous system, as well as risk of mechanical or toxic exposure to the neural placode. The myelomeningocele should therefore be protected and maintained in a moist, covered environment using non-adhesive dressings with warmed Ringer’s lactate solution continuously irrigating the dressing at a low rate through open-ended IV tubing. Broad spectrum intravenous antibiotics are initiated at birth and continued until surgical closure has been completed. A thorough pediatric evaluation is performed to assess the cardiovascular, respiratory, gastro-intestinal, and genitourinary systems. This is important for both complete baseline assessment and to ensure that the infant will tolerate general anesthesia and a surgical procedure. Echocardiogram should be performed prior to surgery, as well as ultrasound of the kidneys, ureters, bladder, and urethra. If necessary, intermittent bladder
(A)
(B)
Figure 8.2. Baseline head ultrasound is obtained on the first day of life.
66
Myelomeningocele
catheterization may be initiated, or a Foley catheter temporarily placed during the perioperative period. Questions
1. What preoperative findings may require modification of the surgical plan in order to ensure success of the myelomeningocele closure? 2. What are the considerations for determining optimal timing of definitive hydrocephalus intervention?
Oral Boards Review—Diagnostic Pearls
1. Establishing an accurate baseline neurologic function in the setting of open neural tube defect is critical. This will be referenced for future progressive deficits, which can occur in the setting of symptomatic Chiari II, syringomyelia, tethering, and progression of hydrocephalus. 2. A complete pediatric evaluation is necessary prior to proceeding with surgical repair of the myelomeningocele. Associated congenital anomalies involving thecardiovascular,respiratory,gastrointestinal,andgenitourinarysystemsmay be present. 3. Hydrocephalus may manifest at birth or develop postnatally in 85 to 90% of patients with open myelomeningocele. Baseline head circumference and head ultrasound should be established on the first day of life, and close observation continued in the post-operative period. Decision Making
Surgical repair is recommended in all cases that do not have an associated fatal birth defect.Ifthe completepediatricevaluationdoesnotelucidateacontraindicationtogeneral anesthesia, the timing of surgery should optimally be within 48 hours. Surgery may be delayed in the setting of compromised pulmonary status, or if more extensive cardiac work-up is indicated after initial echocardiogram. Rarely, associated skeletal anomalies, such as a severe kyphosis, may be present at birth and impact the ability to successfully close the myelomeningocele. Such a lesion may require correction at the same time as the myelomeningocele repair and indicate more detailed spinal work-up in the preoperative period. Severe kyphoscoliosis and asymmetry of the legs may suggest presence of a split cord malformation, and require an alteration of the original surgical plan. Defects with a wide diameter or with minimal redundant cutaneous tissue may result in challenging and complex closures, even with lateral tissue mobilization. In some circumstances, a plastic surgery consultation should be considered for a more extensive repair that may include skin grafts, rotational flaps, or rarely microvascular free flaps. Determining the optimal timing for definitive treatment of hydrocephalus requires consideration of multiple variables including the presence of elevated intracranial
67
86
Pediatric Neurosurgery
pressure, severity of ventriculomegaly on initial head imaging, and progression of macrocrania. If the infant is clinically stable, definitive intervention should be deferred in order to minimize the risk of shunt infection, determine if progressive hydrocephalus is indeed present, and whenever possible allow the infant to reach an older age in order to optimize the success of the initial treatment. Both CSF shunt placement and ETV/ CPC have higher success rates when performed later in infancy. Questions
1. What are the intraoperative steps that will minimize the risk of late complications such as inclusion dermoid cysts and tethered spinal cord? 2. Which anatomic structures need to be meticulously protected in order to avoid a compromise to neurologic function? 3. How can the risk of CSF leak in the postoperative period be minimized?
Surgical Procedure
Once the infant is cleared to undergo general anesthesia, she is brought into the operating room and positioned with the assistance of the neurosurgical team. Care is taken to keep pressure and shearing tension off of the spinal placode. Foam rings and bolsters can be modified for utilization during supine positioning in a manner that avoids any mechanical pressure to the myelomeningocele. After induction of anesthesia, the patient is placed in the prone position with all pressure points padded.The skin surrounding the defect is widely prepared using providone- iodine solution, and the myelomeningocele is gently prepped with diluted solution prior to draping the patient in sterile fashion. Care is taken to avoid placing surgical drapes directly over the placode. Either loupe or operative microscope magnification should be used to begin the procedure. The placode is dissected from the junction to the epithelium, taking care to avoid any retained epithelial fragments on the neural tissue in order to avoid future development of an inclusion dermoid cyst. This dissection is continued around the entire circumference of the placode, while avoiding injury to the dorsal roots and vasculature which may be entering the neural placode just lateral and anterior to the epithelial attachments. Once the placode and nerve roots are freed, the placode is closed in a tubular fashion by approximating pia to pia with absorbable sutures.This technique allows for reconstruction of the distal central canal and conus, and minimizes the risk of future tethering. Leaving the placode open is not advisable as this will allow the parenchymal neural tissue to become densely adherent to the overlying dura, both increasing the risk of tethering adhesions and leading to more complex and tedious dissections should future untethering procedures occur. The dura mater is typically fused laterally to the lumbodorsal fascia. Reconstruction of the thecal sac requires careful elevation of the dural edges at the most lateral extent in order to ensure adequate dural tissue for closure. Care should be taken to avoid any tears to the dura in order to obtain a watertight closure when reconstructing the thecal sac. Once free, the dural edges are brought together and closed in the midline in watertight fashion.
68
Myelomeningocele
If possible, the paraspinal musculofascial layer is mobilized and closed in the midline. This may require partial elevation from posterior bony elements, or relaxing incisions in the lateral aspect of the fascia. Mobilizing the lumbodorsal fascia is more difficult at the sacral level, and may not always be possible. Rotational fascial flaps from superior regions ofthesurgicalexposurehavebeendescribed;however,noevidenceexiststosuggestthis minimizes the risk of postoperative wound complications or long-term morbidities.The subcutaneous tissue and skin may be undermined directly over the lumbodorsal fascia in order to avoid any vascular compromise. This layer is then mobilized to the midline, redundant skin is trimmed, and subcutaneous and skin closure is carried out using absorbable sutures.
Oral Boards Review—Management Pearls
1. Meticulous care should be taken when dissecting the placode from the epidermal attachments in order to minimize risk for future inclusion dermoid cysts and avoid injury to nearby neurovascular structures. Magnification using the operative microscope or loupes is recommended for this step. 2. The placode is closed in tubular fashion, pia to pia, to minimize formation of tethering adhesions and to protect the parenchyma of the neural placode from injury during any future spinal cord untethering procedures. 3. Reconstruction of the thecal sac using elevated dura should be carried out in a watertight fashion. Any defects in the dura that are noted after elevation from the lumbodorsal fascia should be primarily repaired.
Pivot Points
1. If large skin defects are anticipated preoperatively, a plastic surgery consultation for assistance in the closure may be considered. Myelomeningoceles with large diameters may require rotational or myocutaneous flaps, or other complex repair techniques in order to ensure adequate soft tissue coverage of the distal spine. 2. The presence of a severe kyphosis or kyphoscoliosis with asymmetric lower extremities may indicate further spinal anomalies. More extensive preoperative imaging may be undertaken to determine the necessary modifications to the surgical plan in order to ensure safe and complete repair of the neural tube defect.
Aftercare
Following surgery, the infant is positioned prone for several days to minimize pressure and mechanical strain to the reconstructed tissues. The prophylactic broad-spectrum antibiotics may be discontinued following surgical closure. The repair is monitored closely for any sign of infection, dehiscence, or cerebrospinal fluid leakage.
69
07
Pediatric Neurosurgery
(A)
(B)
Figure 8.3. Hydrocephalus is present in 85–90% of patients born with open myelomeningocele.
The urology service evaluates bladder function and provide education to the parents during the postoperative period for any necessary intermittent catheterization and home care. Up to 85–90% of infants with open spinal dysraphism will develop progressive hydrocephalus. Monitoring for the signs and symptoms of hydrocephalus is critical in the postoperative period. Interval assessment of head growth, fontanel, cranial sutures, ocular position, developmental status, and ventricular volumes on serial imaging needs to be continued until either stability is ensured or surgical intervention is warranted (Figure 8.3). A baseline MRI of the brain and spinal cord is performed once the postoperative positioning of the patient is liberalized. The craniocervical junction is assessed along with the extent of the Chiari II malformation and the spine is evaluated for any presence of associated anomalies, compression, or syringomyelia. The ventricular and cisternal anatomy of the brain are imaged in order to evaluate for progressive ventriculomegaly, as well as to determine whether endoscopic treatment options may be anatomically feasible should surgical intervention for hydrocephalus be indicated. In the setting of a symptomatic Chiari II malformation, the patient may demonstrate lower brainstem symptoms such as difficulty swallowing, central apnea, stridor, weak cry, or sustained arching of the head. Should these occur, the first recommended step is placement of a CSF shunt (Figure 8.4). Complications and Management
The neural placode and surrounding nerve roots carry functional tissue, and any mechanical or surgical injury to these structures could result in loss of neurologic function. Protection of the placode as described earlier from birth to closure will avoid preoperative injury. Surgical injury to the placode or nerve roots can be avoided by using meticulous technique, operative magnification, and exercising extreme care during the initiation of the placode dissection. If the nerve roots cannot be visualized when beginning the
70
Myelomeningocele
(A)
(B)
Figure 8.4. Postoperative MRI is obtained to assess for spinal cord syringomyelia and severity of Chiari II malformation at the craniocervical junction. dissection, a more lateral opening in the adjacent epithelial tissue may be made initially in order to allow for visualization and protection of the lateral nerve roots. As the circumferential dissection progresses, the visibility of the nervous structures will improve. Meticulous separation of dermal and neural elements will avoid a late complication of inclusion dermoid cyst. Once the placode is free, the edges should be further explored, and any residual cutaneous fragments removed using microdissection techniques. Wound complications may arise in the postoperative period, including dehiscence of skin edges, cerebrospinal fluid leakage, and wound infection. Ensuring an intraoperative watertight closure of dura, flat positioning for several days postoperatively, and careful monitoring for rapid progression of hydrocephalus in the postoperative period will minimize the risk of CSF leakage. Routine external ventricular drainage has been described as a method for preventing CSF leakage; however, this should not be necessary if good closure techniques are utilized. Wound dehiscence can usually be avoided by ensuring an appropriate degree of tissue mobilization during the intraoperative closure in order to prevent significant tension on the tissue layers in the midline. Risk of postoperative infection is low.
Oral Boards Review—Complications Pearls
1. Careful preoperative care and intraoperative dissection of the neural placode and adjacent nerve roots will minimize risk to intrinsic neurologic function. 2. Meticulous closure of the reconstructed layers—including watertight dural closure and mobilization of soft tissue layers—will minimize postoperative wound healing complications.
71
27
Pediatric Neurosurgery
Evidence and Outcomes
The primary determinant of neurologic outcome is the spinal level at which the open defect is located and the neurological function present at birth. A myelomeningocele occurring at the L1 level, for instance, would associate with motor function through hip flexion, but not below. A patient with myelomeningocele at S1 may have motor function through plantar flexion. Good antenatal care and expedited closure of the myelomeningocele will prevent life-threatening central nervous system infections. Almost all children survive the neonatal period with appropriate treatment. Mortality associated with myelomeningocele has been reported between 15 and 34% in the first 5 years of life and between 9 and 26% thereafter. Deaths in infancy are most commonly associated with complications of the Chairi II malformation or intrinsic brainstem dysfunction, while mortality in older children is most commonly due to shunt malfunction. Treatment outcomes have continuously improved over the last 50 years, with most children now reaching normal levels of intellectual ability. Normal IQ is attained in 70– 75% of children with spina bifida, and 82% of adults are independent with their activities of daily living. Significant improvements have been made in the initial and chronic care received by these patients, leading to an overall improvement in their quality of life. References and Further Reading
Spina bifida outcome: a 25-year prospective. Bowman R, McLone D, Grant J, Tomita T, Ito J. Pediatr Neurosurg. 2001 Mar;34:114–120 Expectation of life and unexpected death in open spina bifida: a 40-year complete, non-selective, longitudinal cohort study. Oakeshott P, Hunt G, Poulton A, Reid F. Dev Med Child Neurol. 2010 Aug;52:749–753. Myelomeningocele: prenatal diagnosis, pathophysiology and management. Adzick N, Walsh D. Semin Pediatr Surg. 2003 Aug;12(3):168–174. Surgical complications of open spinal dysraphism. Pang D. Neurosurg Clin N Am. 1995 Apr;6(2):243–257. Myelomengocele repair: surgical management based on a 30-year experience. Mattogno P, Massimi L, Tamburrini G, Frassanito P, Di Rocco C, Caldarelli M. Acta Neurochir Suppl. 2017;124:143–148.
72
Sagittal Synostosis Mark Proctor and Ali Hazama
9
Case Presentation
An 11-week-old otherwise healthy male was referred for evaluation regarding an elongated head since birth. His parents state that his head was elongated at birth, and has slightlyworsened.Thechildwasseenregularlybyhispediatricianandwasingeneralgood health with no other concerns, except for a slightly enlarged head. He was born full term by C-section secondary to a prior maternal C-section. He was meeting developmental milestonesappropriately,includingfeeding,smiling,cooing,fixingandfocusingonfaces, and head elevation while prone. Detailed neurologic examination by the neurosurgeon wasunremarkable,withnormalspontaneousmovementsinallextremities,normalreflexes, muscles tone and bulk. His head was elongated with prominent frontal bossing and occipitalbathrocephaly,referringtoitspointyandprominentappearance.Headexamination revealed a soft and flat anterior fontanel that was slightly smaller and more anteriorly displacedthananticipated,withapalpableridgealongthesagittalsuture.Hisheadcircumferencewas43 cm,justabovethe98thpercentile.Headanthropometrywasperformedusing a sliding cranial caliper to calculate the cranial (or cephalic) index (CI), yielding a width of 103 mm, length of 148 mm, and CI of 0.696 (significantly lower than normal). Questions
1. What is the likely diagnosis? 2. Are imaging studies required to arrive at this diagnosis? 3. What normal variant of occipital bone development can be mistaken for this condition?
Assessment and Planning
The pediatric neurosurgeon suspects the presence of sagittal suture synostosis.This is a classic presentation, with the combination of frontal bossing, ridging along the sagittal suture, and a narrow and prominent occiput. In normal skull development, the biparietal region should be the widest part of the cranium. Sagittal synostosis results in the frontal region being the widest portion of the skull, with gradual tapering towards a narrow occiput (see Figure 9.1). The differential diagnosis for an elongated and narrow head includes 2 other conditions. One condition is a postnatally persistent mendosal suture. The mendosal suture is an accessory suture of the occipital bone, which divides the bone transversely into superior and inferior portions, and is the embryological separation
73
47
Pediatric Neurosurgery
(A)
(B)
Figure 9.1. (A) Lateral view of 3D CT in sagittal craniosynostosis. (B) Bird’s eye view of 3D CT in sagittal craniosyntosis.
betweenmembranousskullformationaboveandendochondrialboneformationbelow. It normally closes in utero or during the first few days of life. Rarely, this suture persists after birth, resulting in a posterior calvarial morphology similar to that seen with a fused sagittal suture, and referred to as bathrocephaly (see Figure 9.2). A second condition that can mimic some features of sagittal synostosis is prematurity. Children born
Figure 9.2. Persistent Mendosal suture resulting in bathrocephaly. 74
Sagittal Synostosis
prematurely are susceptible to elongated and narrow skulls from lying in the lateral position on the very soft premature infant skull. Positional scaphocephaly should not have frontal bossing or a prominent occiput, there should be no prominent sagittal ridge, and if examined early enough the parietal bones tend to be quite mobile across the patent sagittal suture on physical exam. Sagittal craniosynostosis is the most common type of craniosynostosis, accounting for approximately 50% of all cases. Presentation is usually isolated but may also occur as a part of a genetic syndrome with other concomitant anomalies. There are numerous congenitalsyndromesthathavecraniosynstosisasacomponent,suchasApert,Crouzon, and Pfeiffer syndrome as common examples. Although some are sporadic, most of these syndromes have autosomal dominant inheritance and a genetic work-up is appropriate in suspected cases. The diagnosis of sagittal craniosynostosis is established clinically by history and physical examination in the vast majority of cases. Because it prevents normal lateral growth of the parietal portion of the skull, premature fusion of the sagittal suture leads to narrowing of the posterior skull, with elongation in the anterior-posterior direction. Scaphocephaly (from Greek, skaphe meaning“boat,”and kephale meaning “head”), is a term that is commonly used to describe the elongated, narrow head shape that develops as a result of the prematurely fused sagittal suture. On clinical examination, there is commonly a palpable ridge of bone along the fused suture and immobility of the parietal bones with palpation. Another useful tool is cranial anthropometry and measurement of the CI, which represents the ratio of the maximal cranial width to the maximal cranial length. The CI in children with sagittal craniosynostosis generally ranges from 0.6–0.7, whereas the normal range is approximately 0.75–0.85. After surgical intervention, the CI can be used to follow the improvement in scaphocephaly and the success of surgery, which generally should result in a CI increase of 0.1. Clinical presentation and examination are usually sufficient for diagnosis and treatment planning in the majority of cases of sagittal craniosynostosis. Imaging studies in the form of plain radiographs or computed topography scans may confirm sagittal suture closure in cases where the clinical presentation is unclear, and may be additionally useful in cases where synostosis of other sutures and/or other intracranial anomalies are suspected. Not infrequently imaging studies are performed by the referring primary care physician prior to evaluation by a neurosurgeon, but it is rare that the specialist needs to initiate these films to establish the diagnosis or institute treatment. Questions
1. What is the next step in management in a patient with sagittal craniosynostosis? 2. What is the most appropriate timing for intervention?
Decision Making
Once the diagnosis is established, the next decision is whether or not treatment is required, and if so, what surgical option is best. The rationales for surgical intervention are
75
67
Pediatric Neurosurgery
twofold: (1) to allow for normal brain growth by eliminating the limitation on lateral skull expansion and (2) for aesthetic concerns. Surgery for correction of sagittal synostosis is definitely the standard of care, although mitigating factors can include major medical co-morbidities, very mild cosmetic deformity, or late presentation in a minimally symptomatic child. Surgery for this condition can be performed via minimally invasive or open surgical techniques.Minimallyinvasivesurgerythroughendoscopicallyassistedstripcraniectomy restores normal anatomy, and relies subsequently on the exponential increase in brain growth in the first few months of life. Hence, surgery is ideally performed by 3 to 4 months of age to allow for the normal brain growth to assist with restoring skull expansion after thesutureisreleased,althoughthetimeframecanbeextendedto6 monthsformildcases where less correction is needed to obtain a normal cephalometric outcome. After the procedure, cranial orthotic therapy is used to direct skull growth, although implantation ofspringstointernallydirectgrowthispreferredbysomeauthors.Helmettherapygenerallycontinuesfor6–9 months,dependingontherapidityandcompletenessofcorrection. In contrast, open techniques, are generally performed between 6 and 12 months of age, with reconstruction of the skull shape at the time of surgery.These techniques can also be used for older patients who present with increased intracranial pressure.
Oral Boards Review—Diagnostic Pearls
1. History and physical examination should be adequate to establish the diagnosis of sagittal synostosis. a. Sagittal craniosynostosis. A fused sagittal suture limits the biparietal expansion of the head leading to an abnormally low CI, scaphocephalic head shape with narrow and prominent occiput and frontal bossing, and a sagittal ridge. b. Persistent mendosal suture. This is an occipital bone anomaly which results in bathrocephaly: a prominence of the occipital bone which resembles the occipital findings seen in sagittal craniosynostosis. There is usually a lack of frontal bossing and no associated sagittal ridge. This deformity tends to correct overtime and is not managed surgically. c. Dolichocephaly of prematurity. This is a condition that develops in low-birth-weight infants with very soft skulls. Because of the relatively large head to body ratio and poor neck muscle tone, the head is kept turned to the side while resting. This results in a narrow, elongated head shape. The sagittal suture is not fused, however, and the deformity can correct on its own in the first few months of life. The parietal bones should be mobile. 2. While commonly obtained, imaging is typically not necessary to establish the accurate diagnosis of sagittal craniosynostosis. In rare cases where the diagnosis is not clear, or other associated suture fusions are suspected, plain radiographs or computed topography may be useful. Many recent studies in the literature have demonstrated endoscopic surgery with release of the fused suture and subsequent use of a helmet is an excellent alternative to
76
Sagittal Synostosis
open surgery.The endoscopic procedure has significantly less blood loss, less anesthesia time, and is well tolerated by the baby when compared to the open technique. Since transfusions rates for this surgery are higher in infants less than 5 kilograms, surgery is generally delayed until this threshold is reached, which is often by 8–10 weeks of age. For children less than 4–6 months of age, both open and minimally invasive procedures are discussed with families at the time of initial consultation. The generally discussedadvantagesforendoscopicsurgeryaretheshortersurgicalandanesthetictime with lower need for transfusion, as well as the much smaller surgical scars. The disadvantage is the need for adjuvant therapy with a helmet post-operatively (or occasionally internal placement of springs, a decision that is surgeon and family specific) when the endoscopically assisted surgery is used.The general risks of infection, hemorrhage, and the rare need for re-operation with both endoscopic and open surgery are also discussed at that time. Questions
1. What is the goal of the surgery? 2. What is the most optimal position for this procedure?
Surgical Procedure
There are 2 types of procedures that have been described for treatment of sagittal synostosis. The first type is a calvarial reconstruction which is an extensive procedure that involves making multiple craniectomies to recontour the shape of the skull. There are literally dozens of variations on this procedure, all of which should restore immediate shape correction, and involve a large bicoronal skin incision. The second type is strip craniectomy which is performed by either an open or a minimally invasive technique. Sagittal craniosynostosis is particularly amenable to the latter technique, and therefore the endoscopically assisted strip craniectomy will be discussed in detail. As with any surgery for an infant, sagittal suture release is carried out under general endotracheal anesthesia. The patient is positioned in the “Sphinx” position, which is a modified-prone position using chest rolls and cervical extension to assist with exposing the top of the head. A deflatable bean bag can be used for this, although we prefer a multipurpose head-rest system that uses U-shaped gel supports to cup the ears.Two parallel gel pads support the chin and allow for the passage of the endotracheal tube (see Figure 9.3).The entire top of the scalp is prepped and draped and the intended incision areas are anesthetizedusingalocalanestheticwithepinephrinetolessenbloodloss.Twoincisions are used, both of which are about 2 cm in length. The first incision is placed behind the posterior border of the anterior fontanel and the second is placed at the junction of the lambdoid sutures and sagittal suture. The incisions are made with a needle-tip cautery and deepened to the level of the periosteum with cautery. Burr holes are made at the midline of each incision using a high-speed drill and locally enlarged using Kerrison rongeurs. The goal is to obtain a 1–2 centimeter-wide strip craniectomy along the fused suture. Weconsidersuturereleaseanendoscopically-assistedprocedurebecausethecraniectomy
77
87
Pediatric Neurosurgery
(A)
(B)
Figure 9.3. Intraoperative positioning for endoscopic release of sagittal craniosynostosis. is started from the burr holes under direct visualization prior to endoscope use, and as much bony work as possible is performed under direct visualization. Subperiosteal dissection is then performed between the lambda and the anterior fontanel. An endoscope is then inserted parallel to a suction tip to improve visibility of emissary veins and dural attachments to ensure complete epidural dissection prior to proceeding with bone scissor use. Close attention should be paid to emissary vessels in order to avoid bleeding.Bipolarcauteryshouldbeusedtocoagulateveinswheneverencounteredprior to dissecting them. After complete dissection, with the endoscope, bone scissors are used to incise a strip of bone 1–2 centimeters wide along the sagittal ridge. Bone bleeding can be controlled with bone wax and thrombin-soaked Gelfoam as needed. The field is then irrigated with bacitracin irrigation and Gelfoam is placed over the craniectomy site. Finally, the incisions are closed with inverted 4–0 Vicryl suture followed by running 4–0 Vicryl Rapide suture over the skin.
Oral Boards Review—Management Pearls
1. The strip craniotomy should extend from the posterior edge of the anterior fontanel to the lambdoid suture to restore mobility in the parietal bones, and the surgeon should be certain the bones are mobile at the completion of surgery. 2. As little as a 1–2 centimeter-wide strip craniotomy should allow for adequate skull shape correction prior to the closure of the gap over time.
Pivot Points
1. Endoscopic surgery should be performed prior to 6 months of age as this technique relies on the rapid brain growth in this time frame; older patients
78
Sagittal Synostosis
generally require open primary reconstruction through a larger, bicoronal incision. 2. Post-operative adjuvant therapy, generally using a cranial orthosis, is essential to redirect skull growth and prevent early re-fusion of the craniotomy. 3. Endoscopic surgery does not lead to immediate correction. Close follow-up over the next 6–9 months is essential to ensure appropriate head growth and correction of the skull shape.
Aftercare
Near the conclusion of the procedure, blood is drawn and sent for hemoglobin and hematocrit levels to determine the degree of blood loss, which is notoriously hard to estimate surgically. Transfusion rates should be low, and they are 15 mmHg) in 8–13% of patients with single suture synostosis. Additional patients may be affected by local compressive forces on the cerebral hemisphere, without diffusely raised ICP. Since there is no reliable way to determine which patients will develop problems from craniosynostosis, early intervention is advocated. Surgicaltreatmentsforcraniosynostosishaveevolvedovertimeandthetreatmentmodality largely depends on the age of the patient, the suture that is fused, and the severity of the deformity. Most craniofacial centers of excellence offer both open cranial vault remodeling and endoscopic techniques. The endoscopic procedure utilizes the rapidly growing brain to reshape the skull, requiring post-operative helmet therapy until 1 year of age, but has the advantage of less blood loss and shorter operative time. At our center, this technique is typically performed before 4 months of age. The open technique, specifically fronto-orbital advancement (FOA) for unicoronal sysnostosis or other frontal craniofacial deformities, is typically performed between 9 and 12 months of age. FOA is delayed until the infant is older for 2 reasons: (1) the strength of the bone increases with age, allowing a morestablereconstructionandlesschanceofrelapse,therefore,optimizinglong-termsurgical outcomes. Many surgeons have experienced higher revision rates for this procedure whenperformedbefore6 monthsofage;(2) thesurgerycanbeassociatedwithsignificant bloodlossandlongeroperativetimes,bothofwhicharebettertoleratedbyanolderinfant. In the present case, the family chose the open technique for treatment. Questions
1. What is the goal of your surgical correction? 2. What method can be used to maintain long-term symmetry and anticipate irregular growth?
Surgical Procedure
Fronto-orbital advancement is a major operation carried out under general anesthesia with duplicate IV access, arterial line placement, precordial Doppler monitoring, and 86
Unicoronal Synostosis
(A)
(B)
(C)
Figure 10.3. (A) Skull after scalp reflection, vertex view; (B) skull after scalp reflection, lateral view; (C) orbital bar after removal. Foley placement. Since blood loss is the most frequently encountered complication, type-specific and cross-matched blood should be available in the operating room prior to starting the procedure.The importance of a skilled anesthesiologist and team are paramount given the complexity of these cases. 87
8
Pediatric Neurosurgery
The patient is placed supine with the head stabilized in a padded horseshoe headrest. A zigzag bicoronal incision is used to minimize the visibility of scalp alopecia. The bicoronal incision also allows access to both the anterior and posterior parts of the skull (Figure 10.3). The scalp flaps are elevated in the subperiosteal plane, bringing the temporalis muscle up with the scalp flap. The dissection is continued down to the superior orbital rims. The supraorbital neurovascular bundles must be identified and an osteotome is used to release the foramina so the nerves can be protected. The dissection is carried down into the temporal fossa on either side. On the involved side, the dissection is carried down to the infraorbital rim, while on the uninvolved side the dissection is carried down to the frontozygomatic suture. A bifrontal craniotomy is performed. Multiple barrel stave osteotomies are made in the parietal bone on the synostotic side, outwardly fractured at the base and reshaped with the Tessier bone bender to create more space and to align with the expanded frontal reconstruction on that side. The epidural dissection is carried out along the floor of the anterior fossa and into the middle fossa on both sides, and cotton patties are placed to protect the dura along this interface.Temporal extensions are cut beneath and behind the sphenoid wing in preparation for the cuts to remove the orbital bandeau. Orbital osteotomies are made by making cuts across the orbital roof on either side using a reciprocating saw then making a cut across the nasal glabellar region. On the involved side, the osteotomy goes through the infraorbital rim at the junction with the zygoma, and through the lateral orbital wall to meet the cuts from above. On the unaffected side, the osteotomy is made through the frontozygomatic suture line. The entire orbital bandeau can be removed in 1 piece where it can be untwisted to move the affected side anteriorly and the unaffected side posteriorly, followed by rigid fixation with resorbable plates. Both orbits are contoured to reduce the asymmetry. A closing osteotomy of the sphenoid bone of the orbital roof is created to correct the harlequin eye deformity. Once the correct shape of the bandeau is obtained, it is rigidly fixated with absorbable plates and screws. Some surgeons additionally fix the bandeau in place using up to 3 wires: 1 at the zygomatic intraorbital rim on the affected side, 1 in the nasal glabellar region, and 1 at the frontozygomatic suture line. A wedge osteotomy can be removed from the unaffected side to pull the orbit and frontal region posteriorly, thus reducing frontal bossing. Once this is done, the frontal bone flap can be shaped and placed back as 1 large piece. Bone graft is often harvested from the inner table of the flap so that it can be used to fill in the gaps. At the end of the procedure, the affected side is somewhat overcorrected since there will be further skull growth on the unaffected side and it is the best way to maintain long-termsymmetry.Foreheadcorrectionandorbitalnormalizationshouldbeachieved (Figure 10.4). The scalp is re-approximated and the canthal tendon is re-suspended to ensure normal eye appearance. Some surgeons use a subgaleal drain for 1 to a few days to reduce swelling. Antibiotic ointment is liberally placed on the incision line as a dressing.
88
Unicoronal Synostosis
Figure 10.4. Immediate post-operative 3D CT reconstruction showing fronto-orbital advancement (a surgical drain remains in place).
Oral Boards Review—Management Pearls
1. Once the diagnosis of unicoronal synostosis is made, surgical correction is necessary to make adequate space for normal brain growth and to alleviate any future psychosocial impact. 2. Both open and endoscopic techniques are effective treatments for unicoronal synostosis.The chosen method depends on the age of the patient at presentation, severity of the deformity, surgeon preference, and family preference. 3. There is an increased prevalence of strabismus in unicoronal synostosis. Patients should be evaluated both pre-operatively and post-operatively since ophthalmologic surgery is frequently necessary to address this problem.
Pivot Points
1. For patients presenting at less than 4 months of age, endoscopic repair may be considered to take advantage of soft bone and rapidly growing brain to shape the skull, along with the use of helmet therapy. The open technique of fronto- orbital advancement provides the best results when performed closer to a year of age to optimize long-term surgical outcomes and prevent recurrence. 2. Patients presenting with syndromic craniofacial anomalies including coronal synostosis and midface hypoplasia need careful monitoring of ophthalmological condition, dental occlusion, and airway sufficiency. Many need staged surgical repairs, with fronto-orbital advancement during infancy, and midface advancement later in childhood.
89
09
Pediatric Neurosurgery
Aftercare
Although the surgery is safe, these patients require care in the intensive care unit after surgery for a minimum of 1 night of observation, given the possibility of meaningful blood loss and resulting transfusion received in the operating room in some patients. Patients typically move to the ward on post-operative day 1, and electrolytes and complete blood count should be monitored if indicated. Routine peri-operative antibiotics are given for 24 hours, but no longer. The subgaleal drain remains in place until the output decreases. Narcotic pain medication may be supplemented with scheduled acetaminophen. The incision is managed with twice daily application of antibiotic ointment for 7 days. Typical follow-up at our institution includes an incision check at 2 weeks, routine follow-up at 1 year, then a follow-up low-dose CT scan at 2 years post-operatively (Figure 10.5). These patients should be followed yearly in this manner until 6 to 7 years of age, when brain growth is complete. The follow-up period may be extended as deemed necessary. Complications and Management
The overall morbidity and mortality rates for craniosynostois surgery are low and generally the surgery itself is quite safe. However, because the infants’circulating blood volume is relatively small, and blood loss can be significant, it is of utmost importance to maintain euvolemia. Untreated or inadequately treated hypovolemia can have devastating consequences for the patient.To combat anemia and hypovolemia from blood loss, crystalloid, colloid, and blood transfusion are often necessary. A dilutional coagulopathy can occur if platelets and/or fresh frozen plasma are not given with packed red blood cells during the volume resuscitation. If injury to the venous sinuses occurs, the result can be
Figure 10.5. Late post-operative 3D CT showing result of fronto-orbital advancement.
90
Unicoronal Synostosis
catastrophic if not recognized and appropriately treated in a timely fashion.Venous sinus injury can be treated with gelfoam and patty occlusion followed by repair with a muscle plug. Preparation for blood loss and avoidance of disruption of the venous sinuses and dura are 2 of the more important surgical issues in craniofacial surgery. The extensive bony work involved in an FOA, may lead to incorporation of air into the vascular system causing an air embolism.This is a serious complication that requires monitoring with a precordial Doppler. Identifying and occluding the site of entry, flooding the field with saline, and lowering the head of the bed are early maneuvers that are employed when an air embolism is recognized. Other complications that may be encountered in this procedure include dural injury leading to a CSF leak requiring dural repair, injury to the underlying brain parenchyma, transfusion reactions, seizures, and surgical site infections. Patients may present years later with post-reconstruction calvarial defects that may require additional surgery to fill. Because titanium plates migrate intracranially with infant skull growth, in recent yearsresorbableplateshavealmostalwaysbeenused.Theseabsorbableplatesbreakdown approximatelyayearpost-operatively,occasionallycausingswellingunderthescalpover the area where the plates were placed and causing alarm for some families. Preemptive counseling about this possibility is useful.
Oral Boards Review—Complications Pearls
1. Monitoring for blood loss and adequate volume and blood product resuscitation are the critical to surgery for the treatment of craniosynostosis. 2. Routine pre-cordial Doppler monitoring for air embolism and avoidance of this complication with proper positioning should be used for early recognition and avoidance of this complication.
Evidence and Outcomes
Presently, good outcome measures for the different procedures used and neurodevelopmentaloutcomesarelackinggiventhewidevariabilityinthemanagement of craniosynostois. However, children with nonsyndromic synostosis often live normal lives with good long-term outcomes after surgery. It is important to recognize they require multidisciplinary care provided by pediatric neurosurgeons, craniofacial plastic surgeons,pediatricians,geneticists,pediatricnurses,andophthalmologists.Becauseofthe complexity of their care, referral to craniofacial centers of excellence is recommended. References and Further Reading
Warren SM, Proctor MR, Bartlett SP et al. Parameters of care for craniosynostosis: craniofacial and neurologic surgery perspectives. Plast Reconstr Surg 2012; 129: 731–737. https://www. ncbi.nlm.nih.gov/pubmed/19569905?dopt=Abstract Mehta VA, Bettegowda C, Jallo GI, Ahn ES. The evolution of surgical management for craniosynostosis. Neurosurg Focus 2010; 29: E5 https://www.ncbi.nlm.nih.gov/pubmed/ 21121719?dopt=Abstract
91
29
Pediatric Neurosurgery
MacKinnon S, Rogers GF, Gregas M, Proctor MR, Mulliken JB, Dagi LR. Treatment of unilateral coronal synostosis by endoscopic strip craniectomy or fronto-orbital advancement: Ophthalmologic findings. J AAPOS 2009; 13: 155–160 https://www.ncbi.nlm.nih. gov/pubmed/19393513?dopt=Abstract Breugem CC, van R Zeeman BJ. Retrospective study of nonsyndromic craniosynostosis treated over a 10-year period. J Craniofac Surg 1999; 10: 140–143 https://www.ncbi.nlm.nih.gov/ pubmed/10388415?dopt=Abstract
92
Inflicted Traumatic Brain Injury Beth A. Costine-Bartell and Ann-Christine Duhaime
11
Case Presentation
A 6-week-old girl was brought to a local emergency department in the morning about 1 hour after a seizure at home that lasted 2 minutes. The patient’s father reported that the patient arched her back and then stiffened her body, had bilateral arm jerking, her eyes were rolled back, and she was unresponsive during the seizure and for 5–7 minutes thereafter.Herfatherthoughtshemayhavestoppedbreathingandgaveherafewbreaths and chest compressions but did not observe cyanosis.The seizure occurred 3 hours after a feeding. When the mother returned she noted that the infant was pale and called 911; emergency responders reported that the infant looked normal at arrival. At the emergency department (ED), the infant was mostly sleeping on the mother’s lap while being examined and did not cry when awakened by the exam. The abdomen was soft and non-tender, the limbs were moving bilaterally and equally, no twitching or other signs of seizure were observed, the head was of normal circumference, and there were no signs of trauma or bruising. The neurological exam was normal by report. Her lungs were clear.The cardiac exam and electrocardiogram revealed no concerns. Her capillary refill was normal. Her blood chemistry, electrolytes, white blood cells, toxicity screen, and urinalysis were normal. A bedside electroencephalogram (EEG) was interpreted as normal with no epileptiform features. A head ultrasound was performed in the ED and was interpreted as normal. During observation in the ED, there was no difficulty with feeding, no seizures, and no apneic episodes. Because the infant was acting normally, and there were no signs of trauma, infection, or metabolic acidosis, the medical team concluded that the episode was probably due to laryngotracheomalacia because of the patient’s history of difficulty with feeding. Stool cultures (for possible rotavirus), urine cultures, and blood cultures for other infections were ordered. After 24 hours of observation in the ED, the infant was discharged. Studies for larygotracheomalacia were scheduled. The parents were given a continuous video recording unit and were instructed to report any shaking indicative of a seizure. At a follow-up visit with their regular pediatrician, the mother reported no additional episodes.The stool, urine, and blood cultures were all determined to be negative. Ten days later (1.7 months of age), the parents brought the infant to their pediatrician for “twitching” of arms and legs and looking “out of it” over the past several hours the night before. The previous evening, the father reported that he left the infant in her crib for 1 minute and came back to find her seizing with rhythmic motor activity involving her left side, which resolved. Both parents observed the infant intermittently crying and inconsolable with the twitching movements occurring intermittently through the
93
49
Pediatric Neurosurgery
night. They did not bring her back to the ED, as they were told that these movements probably reflected discomfort due to reflux disease. In the morning, the parents brought the infant to their pediatrician, who then immediately sent them to the ED. In the ED, the left arm was fixed at 45° and was rhythmically circling. The right arm was flexed at less than 45° and rhythmically moving left to right. She had increased tone during episodes and an EEG confirmed status epilepticus. She was treated with lorazepam without effect, followed by a loading dose of fosphenytoin, and then phenobarbital. She then developed respiratory depression requiring intubation, thought likely to be related to anticonvulsant medication administration. Hypotension was treated with dopamine infusion. A non-contrast head CT revealed an acute right sided parafalcine subdural hemorrhage over the right convexity, with a possible small, isodense SDH that was 6 mm thick over the left hemisphere (Figure 11.1). Lack of white and gray matter differentiation was noted diffusely.There was no skull fracture, no intraparenchymal blood, and no midline shift. The infant was then transported to a tertiary referral center where a pediatric neurosurgeon was consulted. The patient was hypotensive and tachycardic. She showed intermittent eye opening and twitching of the extremities, but did not cry or show change in facial expression to trapezius pinch; Infant Face Scale score was 9 (eyes: 4 of 4, motor: 3 of 6, verbal/face: 1 of 5). Pupils were reactive bilaterally, did not blink to threat, the face was grossly symmetric, withdrew from painful stimuli in all 4 extremities, and deep tendon reflexes were normal bilaterally; there was no ankle clonus, and no response to plantar stimulation was noted.The fontanelle was moderately full with prominentpulsations.Theinfanthadrepeatedepisodesofdesaturationthatwereameliorated with suctioning and positive end expiratory pressure. On careful questioning there was no history of trauma provided by either parent. There was no evidence of bruising or swelling on the head or body. With respect to past medical history, the baby was born at term via cesarean section. She was the first child of this couple. The mother had two other children with a different father.Thepatientdevelopedgastroesophagealrefluxdisease(similartoherhalfsiblings) that was treated with ranitidine, but was otherwise healthy.The mother reported that the infant screamed for hours during feedings, which was reported to the infant’s physician on multiple previous occasions. She had been developing well with normal weight gain and with no other major medical issues. There was no family history of seizures except for the father, who reported that he may have had seizures as a child. The parents were the only caretakers. Questions
1. What is the differential diagnosis? 2. What immediate interventions are most important? 3. What additional testing and imaging would be helpful? 4. What is the role for surgical intervention?
94
Figure 11.1. Diagnostic imaging of a 1.7 month old female. Axial (A) and coronal (B) computed tomography demonstrates loss of white mater and gray matter differentiation and bilateral subdural hematoma (black arrows). Venous drainage is intact as demonstrated by MRV (C). Increased intensity of the cortical ribbon and major white matter tracts predominantly in the periphery of the bilateral frontal, parietal, occipital, and posterior lobes indicated damage via T2 weighted MR (D). There was an abnormal decreased signal in the bilateral thalami, which may have related to the seizure activity (D). Extra axial collections are observed on the MPRAGE (E). Diffusion weighted imaging reveals symmetrical, bilateral diminished diffusion in the frontal and occipital lobes (areas of hyperintensity; F). The skeletal survey reveals a periosteal reaction indicating healing from an injury one week before on the left posteriorlateral rib (black arrow; G). There are callus formations at the right third, fifth, and sixth posterior costovertebral junction suggestive of healing fractures (white arrows; G). The left femur has a periosteal reaction along the antererolateral aspect suggestive of a healing non-displaced fracture (white arrow; H). The left tibia has a periosteal reaction suggestive of subperiosteal new bone formation in response to a non-displaced healing fracture (white arrow; I). A small tibial spur is located on the left tibia but is equivocal for injury vs. a normal variant (vertical white arrow; I).
69
Pediatric Neurosurgery
Assessment and Planning
Despite the prolonged course and the infant superficially appearing “awake,” this presenting exam is consistent with status epilepticus and unresponsiveness.The patient needs to be stabilized in an intensive care unit, and surgical decisions made. The“ABCs” of airway, breathing, and circulation come first. An infant with this presentation usually requires intubation, careful fluid management to maintain perfusion without large free water loads, and critical care monitoring. Continuous EEG monitoring and treatment of seizures by the child neurology and/or neuro-critical care team is essential to minimize exacerbation of brain injury. Consideration is given to minimizing sedation when possible in order to follow clinical exam. The presence of a subdural hematoma and lack of history of trauma is relevant to the differential diagnosis. There are no clinical indications for infection, but for very young infants with unexplained status and neurologic compromise, obtaining CSF is a consideration that must be weighed against the danger of lumbar puncture or other method of CSFinterrogationinthesettingofpotentialelevatedintracranialpressure.Fontanelletap for withdrawal of CSF from the subdural/subarachnoid space can be useful in this setting for culture and to transiently relieve pressure. Coagulation is assessed to determine the risk of continued bleeding of the subdural hematoma and risk of bleeding from intervention. Vitamin K is given if it was not administered at birth. Because sedation is needed for comfort during intubation, the goal is to follow the exam carefully and, if possible, to extubate the infant as soon as seizures are under control and mental status improves, in order to use the clinical exam to recognize effects of interventions and/or need for additional treatment. The differential diagnosis includes coagulopathy, infection, venous thrombosis, head trauma due to accidental injury, abusive head trauma, or a metabolic disorder. The abusive head trauma diagnosis is further interrogated with skeletal survey and retinal examination once the patient is stable. For further reading, please refer to Campbell et al. for the current guidelines for history, laboratory, and imaging (specific for the age of the child) required for medical evaluation for suspected abuse in children 0–60 months of age that present with a skull fracture or long bone fracture or intracranial hemorrhage. Questions
1. What is the role for surgical intervention in this setting? 2. What are the goals of overall management? 3. What adjuncts help in diagnosis and in prognostication for the family? In this case, initial coagulation work-up showed no evidence of coagulopathy, so the neurosurgeon tapped the fontanelle to lower intracranial pressure and obtain CSF for culture to rule out an infection. The CSF contained bloody CSF but no evidence to support infection.The fontanelle remained soft, so an intracranial pressure monitor was not placed at that time. Once the patient is stabilized, MRI can be extremely useful to 1.) follow the subdural hematoma 2.) to determine whether there are contusions or other intraparenchymal
96
Inflicted Traumatic Brain Injury
lesions, such as venous thrombosis, 3.) to assess the status of the basilar cisterns and any evidence of focal or diffuse brain swelling, and 4.) use diffusion-weighted imaging to assess for ischemic or excitotoxic injury. In the absence of any other etiology, inflicted trauma was suspected.The majority of severe head trauma in children under the age of 2 is due to inflicted injuries. The hospital Child Protection Services team was consulted promptly after explanation to the family about the protocol for children who appear to have potential injuries or other problems as evaluation is ongoing. Social workers supported the family and attempted to keep communication open. Families respond best when Child Protection Services is involved from the start and can react more negatively if this new team is introduced days into the hospital stay. The neurosurgeon should be one of the many clinicians talking to the family. The mother disclosed to social workers the acute financial stress the family has been experiencing and noted that the father’s history was changing in the details described.The lack of trauma history and changing history along with a subdural hematoma are highly suspicious for inflicted injury.
Oral Boards Review—Diagnostic Pearls
1. Infants with subdural hematoma, subarachnoid hemorrhage, or parenchymal lesions related to trauma, particularly non-accidental trauma, may present with otherwise unexplained seizures. 2. Status epilepticus in infants may be difficult to recognize, and a high level of suspicion is required. 3. Very young infants with head trauma may appear superficially less neurologically impaired than is the case, and examination techniques should look for cortical response to stimulation such as crying to pain along with other aspects of standard infant examination. 4. Evaluation must assess for other causes requiring prompt intervention, such as infection and thrombosis. 5. In the absence of explanation, evaluation for coagulopathy and metabolic disorders is undertaken for completeness. Pediatricians expert in child protection usually can advise on which tests are most valuable in this setting. 6. Complete skeletal survey and retinal examination are essential parts of the evaluation of suspected inflicted injury. Other exams, such as bone scans, delayed skeletal surveys, and evaluation for other disorders can be obtained in collaboration with child protection experts.
Decision Making
On day 2 of hospital admission at the tertiary hospital, the infant received packed blood cells for ongoing tachycardia, low blood pressure, and low hematocrit. The fontanelle was soft, flat to almost sunken, and therefore no pressure monitor was placed. Seizures canincreasethepressure,andanalmostsunkenfontanellewasprobablyduetoincreasing seizure control. She continued to have intermittent brief seizures throughout the day. Continuous EEG monitoring revealed a total of 8 seizures over 24 hours lasting 10–67
97
89
Pediatric Neurosurgery
minutes each. Seizures were repeatedly treated with doses of levetiracetam, lorazepam, phenobarbital, midazolam, fosphenytoin, and then with a constant midazolam infusion. Seizures ceased on the evening of day 2 of admission. From the time the parents observed status epilepticus to the last seizure observed on EEG in the hospital was approximately 48 hours. Hematology reported that her platelet level was normal and coagulation was normal at admission. Diagnostic tests for metabolic disorders were sent.The infant’s fontanelle remained flat to slightly sunken. Her pupils remained small and she had some responsive movement to stimuli but had no facial expression to neurological exam, which was thought in part to reflect the continued sedative effect of medications to control the seizures. Eventually, the father tearfully confessed to an intensive care resident that he was roughly bouncing her on his knee without supporting her head, grabbed her quickly, and then slammed her head into his shoulder to a degree that it caused him pain at which point she temporarily stopped crying and then her limbs began twitching. The fatherwasarrestedlaterthatday.Laterinterviewsrevealedadditionalepisodesofinflicted trauma. MRI was performed on day 2 of admission. The T2 sequence revealed increased intensity of the cortical ribbon and major white matter tracts. These changes were predominantly peripheral and partly followed a watershed pattern that involved the cortex, subcortical, and deep white matter in the bilateral frontal, parietal, occipital, and posterior lobes. There was an abnormal decreased signal in the bilateral thalami. The subdural hematoma had grown to 9 mm thick on the right frontal and parietal parafalcine and interhemispheric descending into the posterior fossa of the tentorium, and scant subarachnoid and intraventricular hemorrhage were noted. The MR venography was negative for venous thrombosis. Over the bilateral frontal lobes and basal ganglia lactate/creatine was elevated with preservation of NAA/creatine as determined by MR spectroscopy.There was symmetrical, bilateral diminished diffusion on diffusion weighted imaging in the frontal and occipital lobes (Figure 11.1). There was sparing of the perirolandic gyri (sensoriomotor cortex), corticospinal tracts, and brain stem. There was no other focal intraparenchymal lesion or intraparenchymal hemorrhage. On day 4 after injury, the infant displayed surface evidence of trauma with the development of a large subgalael hematoma posteriorly which resolved completely by day 6. On day 6, the infant was extubated, and responded to stimuli during neurological exams but did not change facial expression. A skeletal survey revealed multiple periosteal reactions indicative of non-displaced fractures (Figure 11.1). There was a healing fracture on the left sixth posterior lateral rib and callous formations on the right third, fifth, and sixth posterior ribs at the costovertebral junction suggestive of healing fractures.There were periosteal reactions of non-displaced fractures along the left femoral diaphysis and left tibial diaphysis. Rib fractures and tibia/fibia fractures are 14.4 and 6.3 times more likely to occur from inflicted injures versus accidental injury. An ophthalmology exam revealed extensive pre-retinal and intraretinal hemorrhage in the macula and periphery bilaterally. A follow-up MRI on day 11 revealed evolution of injury including both the white and gray matter in the occipital cortex and extending into white matter in the frontal
98
Inflicted Traumatic Brain Injury
lobes, but sparing portions of both hemispheres.The infant was more active overall, able to drink from a bottle after passing the bedside swallowing test, and was prepared for discharge. It was determined that no additional surgical interventions were needed and a rapid MRI was scheduled 3–4 weeks post-discharge to follow the subdural collections, which most often resolve spontaneously. The infant was discharged on day 19 after admission. She tracked light and passed hearing tests.
Oral Boards Review—Management Pearls
1. In infants in status epilepticus, initial management revolves around airway, breathing, and resuscitation. Both seizures and sedating anticonvulsants may lead to respiratory depression. Young infants in prolonged status or with trauma may require fluid resuscitation to avoid hypotension and inadequate cerebral perfusion. 2. Early MRI, including diffusion weighted imaging, may be very helpful for prognosis. Infants with diffuse bilateral damage, including deep gray matter or brainstem, have a poor prognosis. Infants with damage confined to 1 hemisphereorpatchydamagehavevariableprognoses,andaggressivemanagement may help limit progression.
Evidence and Outcomes
At her 1 month follow-up appointment the patient showed increased tone and had no visual response on exam. Her head circumference was in the 90th percentile. A rapid T2 and susceptibility-weighted MRI revealed atrophy in the frontal and parieto-occipital periventricular regions. The extra-axial subdural collections remained stable without mass effect. Coagulation and metabolic evaluations disclosed no other diagnoses. At 1 year of age, the child’s head circumference dropped into the 15th percentile and she had marked developmental delays. Rapid T2-weighted MRI revealed atrophy of the occipital lobes bilaterally, and some thinning of the temporal and parietal cortices bilaterally.The frontal lobes were relatively spared.The extra axial fluid collections were resolved. She had started displaying some stereotypy. At 18 months of age, her head circumference was in the 25th percentile and she exhibited some visual ability to fix upon and follow objects. At 2.5 years of age the patient started walking, was social, and had a head circumference in the 25th percentile. She remained seizure-free after weaning anticonvulsants. At 4 years of age she was attending preschool and receiving intensive occupational, physical, speech, and vision therapy. She walked, ran, and jumped, but exhibited some dyspraxia and sensitivity to sounds and food textures. She was pleasant and social although she had a short attention span and exhibited occasional aggressive behavior and irritability. She had amblyopia and intermittent exotropia but not complete blindness. Her recovery and development were thought to be at the better end of the typical recovery spectrum.
99
01
Pediatric Neurosurgery
Oral Boards Review—Management Pearls
1. Infants with an acute subdural hematoma with midline shift may require urgent craniotomy for decompression. Many young infants with no evidence of incipient herniation can be managed with fontanelle tap initially and followed closely for evidence of increased intracranial pressure or brain swelling that may require decompression. 2. The role of intracranial pressure monitoring in infants remains individualized. In very young infants in whom there is a low index of suspicion for dangerous tissue shift and who have a clinical exam that can be followed serially and a reliably palpable fontanelle, close observation is utilized by some clinicians. If there is any doubt about the ability to follow the patient’s status with these measures, intracranial pressure monitoring should be considered.
References and Further Reading
Campbell, K.A., Olson, L.M., and Keenan, H.T. (2015). Critical Elements in the Medical Evaluation of Suspected Child Physical Abuse. Pediatrics 136(1), 35–43. doi: 10.1542/ peds.2014-4192. Duhaime, A.C., Alario, A.J., Lewander, W.J., Schut, L., Sutton, L.N., Seidl, T.S., et al. (1992). Head injury in very young children: mechanisms, injury types, and ophthalmologic findings in 100 hospitalized patients younger than 2 years of age. Pediatrics 90(2 Pt 1), 179–185. Duhaime, A.C., Christian, C., Moss, E., and Seidl, T. (1996). Long-term outcome in children with the shaking-impact syndrome. Pediatric Neurosurgery 24, 292–298. Duhaime, A.C., Christian, C.W., Rorke, L.B., and Zimmerman, R.A. (1998). Nonaccidental head injury in infants--the “shaken-baby syndrome.” N Engl J Med 338(25), 1822–1829. doi: 10.1056/nejm199806183382507. Durham, S.R., Clancy, R.R., Leuthardt, E., Sun, P., Kamerling, S., Dominguez, T., et al. (2000). CHOP Infant Coma Scale (“Infant Face Scale”): a novel coma scale for children less than two years of age. J Neurotrauma 17(9), 729–737. Hasbani, D.M., Topjian, A.A., Friess, S.H., Kilbaugh, T.J., Berg, R.A., Christian, C.W., et al. (2013). Nonconvulsive electrographic seizures are common in children with abusive head trauma. Pediatr Crit Care Med 14(7), 709–715. doi: 10.1097/PCC.0b013e3182917b83. Keenan, H.T., Runyan, D.K., Marshall, S.W., Nocera, M.A., Merten, D.F., and Sinal, S.H. (2003). A population-based study of inflicted traumatic brain injury in young children. JAMA 290, 621–626. Kleinman, P.K., and Newton, A.W. (2015). Diagnostic Imaging in Child Abuse. Cambridge, United Kingdom: Cambridge University Press. Pandya, N.K., Baldwin, K., Wolfgruber, H., Christian, C.W., Drummond, D.S., and Hosalkar, H.S. (2009). Child abuse and orthopaedic injury patterns: analysis at a level I pediatric trauma center. J Pediatr Orthop 29(6), 618–625. doi: 10.1097/BPO.0b013e3181b2b3ee. Young, J.Y., Duhaime, A.C., Caruso, P.A., and Rincon, S.P. (2016). Comparison of non-sedated brain MRI and CT for the detection of acute traumatic injury in children 6 years of age or less. Emerg Radiol. doi: 10.1007/s10140-016-1392-3.
100
Traumatic Atlanto-Axial Dislocation Douglas Brockmeyer
12
Case Presentation
A 3-year-old boy was a backseat passenger in a car involved in a high-speed motor vehicle accident. The driver, his mother, was killed at the scene. He was seated in a forward-facing car seat. Upon extrication, the EMS providers documented that he was moving all of his extremities weakly and had a GCS of 15. He did not require intubation and was placed in a hard cervical spine collar. He was placed in full spine precautions and transported to a Level I trauma facility. Upon arrival, he is awake and crying. Cranial nerve examination is normal.The motor examination reveals diffuse arm and leg weakness, graded 3 out of 5, with diminished sensation to pinch at feet and hands. The reflexes are 1+ and symmetric, with bilateral upgoing toes on plantar stimulation. Questions
1. What is the most likely diagnosis for this patient? 2. What is the most appropriate imaging at this stage? 3. How would you manage this patient’s spinal cord injury?
Assessment and Planning
A full trauma assessment is performed, including a CT scan of the head and cervical spine.The head CT demonstrates a small amount of subarachnoid blood at the foramen magnum and is otherwise normal. The cervical spine CT (Figure 12.1) reveals increased distance between the occipital condyle and C1, with a condylar-C1 interval (CCI) of over 4 mm in both sagittal and coronal measurements. Because of his extremity weakness, an emergent cervical spine MRI is obtained (Figure 12.2). The STIR (Short-TI Inversion Recovery) sequence of MR images show high signal intensity in the upper cervical spinal cord, with high signal in the bilateral occipital-C1 joint capsules and the posterior ligamentous structures. The pediatric neurosurgeon suspects there is atlanto-Axial dislocation (AOD). The combination of the mechanism of injury, motor weakness, and imaging findings all support the diagnosis. The diagnosis is confirmed by the radiographic demonstration of a CCI greater than 4 mm on sagittal and coronal CT and the abnormal STIR signal in the O-C1 joint and posterior ligaments. Other radiographic measures used to diagnose AOD, including Power’s ratio and the basion-dens interval, have demonstrated low positive and negative predictive value (Pang et al., 2007). Additionally, whereas
101
2 0 1
Pediatric Neurosurgery
Figure 12.1. Parasagittal CT reconstruction showing a widened atlanto-occipital joint. plain lateral cervical spine films are appropriate during the trauma work-up, flexion- extension x-ray are contraindicated given the patient’s neurological deficit and the clear demonstration of occipitocervical instability on imaging. In fact, attempts to obtain dynamic imaging or to place a large cervical collar with distracting force on the mandible and subocciput in a patient with AOD are occasionally associated with acute
Figure 12.2. Sagittal STIR MR images of the cervical spine, showing both articular and ligamentous craniocervical injury.
102
Traumatic Atlanto-Axial Dislocation
cardiorespiratory instability and/or cranial nerve deficits (such as 6th nerve palsies) because of mechanical brainstem traction. This patient’s spinal cord injury is best initially managed with careful immobilization and by increasing the patient’s blood pressure to improve spinal cord perfusion. In a pediatric patient this can be challenging and is best done in conjunction with a pediatric intensivist. An arterial line is necessary, and careful management of the patient’s fluid status is required. A reasonable way to manage the fluid requirements is to start the patient’s IV at a rate 1.5 times normal maintenance and to use fluid boluses as necessary to hit a target mean arterial pressure (MAP). A reasonable target MAP for a young patient with a spinal cord injury such as this one is 90 mmHg. Because of the high ratio of head to body size and mass, as well as the relatively flat atlantal and occipital articular surfaces, young children are particularly prone to AOD compared with older children, adolescents, and adults. In addition, the large head size of young children predisposes them to a relatively flexed position when lying flat. It is often important to very carefully place padding under the shoulders of young children with AOD to maintain a neutral position for their neck and craniocervical junction while lying supine.
Oral Boards Review—Diagnostic Pearls
1. For all pediatric patients involved in a high-energy traumatic injury, the presence of AOD must be ruled out. A flexion-distraction mechanism is most common. A high level of suspicion is necessary at all times. The most efficient way to determine the presence or absence of AOD is cervical spine CT with sagittal and coronal reconstructions. A CCI greater than 4 mm is consistent with AOD, but the injury must be confirmed with MRI. A CCI less than 3mm is normal in all age groups. 2. Unilateral AOD can occur and must be evaluated carefully for instability. 3. Special attention must be paid to the O-C1 joints on MRI. The presence of abnormal signal intensity in the joint may indicate AOD. 4. Occasionally, flexion-extension cervical CT is necessary to rule out AOD in cases where the CCI is indeterminate. When indicated, dynamic imaging in borderline cases should be carried out under direct neurological supervision by a member of the neurosurgical team. 5. Combination O-C1–C2 injuries can occur and are usually accompanied by extensive MR STIR signal abnormality in the posterior ligamentous structures from the occiput to C2.
Questions
1. What is the role of a flexion-extension cervical spine x-ray in a patient with a confirmed AOD on CT and MRI? 2. How does the presence of a combination O-C1 and C1–2 injury influence surgical planning and decision making? 3. How often can an O-C1 injury be managed conservatively?
103
4 0 1
Pediatric Neurosurgery
Decision Making
Once the diagnosis of AOD is confirmed on imaging, the decision to move forward with occipitocervical fusion is straightforward. A flexion/extension cervical spine x-ray is not necessary if the CT and MRI are diagnostic; in fact, it is potentially dangerous. Although not emergent, the operative procedure should be performed in a timely manner. If a moderate or severe head injury is also present, the procedure should wait until any significant intracranial pressure (ICP) issues have been resolved. If elevated ICP is present and the patient is paralyzed and sedated because of a head injury, the cervical collar may be removed and padding used to immobilize the head in midline position without any distraction. Occasionally, severely unstable patients will show deterioration with minimal amounts of distraction and may need to be provided a mild compression force until stabilized by placement of a halo ring and vest, prior to definitive surgery. When sedating and paralyzing medicines are weaned, a collar is replaced and kept on for the duration of management. For patients with CCIs of indeterminate distance, such as 3.0 to 3.8 mm, it is necessary to determine whether a stabilization procedure is necessary, based on a combination of clinical factors, including presence of a neurological deficit and/or neck pain. Combined with careful review of the competency of the craniocervical ligaments on imaging, these clinical factors are generally sufficient to guide further decision making. In rare borderline cases, a 1- to 3-month trial of collar immobilization along with serial cervical spine flexion/extension x-rays, is reasonable prior to a final decision to proceed with fusion. Children whose neck pain resolves over a few weeks and who have normal x-rays do not need surgical stabilization. A combination O-C1–C2 injury and O-C1 injury are, for all intents and purposes, treated the same. Both types of injuries require O-C2 fusion. Questions
1. What potential complications can occur during patient positioning and how can one safeguard against them? 2. What are key anatomical landmarks and danger areas to avoid during the procedure?
Surgical Procedure
The patient is brought to the operating room and maintained in a hard cervical collar or halo ring and vest while being placed under general anesthesia. Motor and sensory evoked potentials are recommended, and a pre-flip baseline evaluation is performed. The head is placed in a Mayfield pin head holder, which can also be attached to a halo ringusingapurpose-designedadaptor.Thepatientispositionedproneandpaddedadequately. If relevant, the posterior half of the halo vest and rear posts can then be removed to provide access for performing the craniocervical fusion and any associated bone graft harvest. Intraoperative fluoroscopy should be used to confirm neutral position immediately after turning the patient prone, and stability of the baseline motor and sensory evoked potentials should be reconfirmed. A vertical midline suboccipital and upper cervical incision is planned, along with a posterior rib incision on the chest if rib autograft 104
Traumatic Atlanto-Axial Dislocation
is being used.The patient is prepped and draped, and the suboccipital exposure is done in the usual manner, exposing the occiput to C3. ThefirststepistoplaceanchorscrewsintoC2.EitherC2parsscrews,C1–2transarticular screws,C2pediclescrews,orC2translaminarscrewsmayalsobeplacedusingfluoroscopy according to the surgeon’s training and patient’s anatomy. Our preferred method is to use C2 pars screws, usually 12 to 20 mm in length depending on patient age. The next step is to place the occipitocervical (OC) hardware. Several OC instrumentation systems are available, including rod–plate and occipital plate–rod configurations. Again, the choice of hardware is up to the surgeon, as there are no data to suggest that one system is better than another.Thin occipital bone may be managed by placing short (6-mm) screws into the occiput or by using an occipital plate with the anchor screws engaged in the midline occipital keel. If autograft is used, either rib or iliac crest may be harvested, but rib is preferred because of its high natural content of bone morphogenetic protein (BMP) and natural contour generally matching the curvature of the dorsal craniocervical junction. Full-thickness ribs, cut to the appropriate length, are harvested and decorticated at the contact points. The suboccipital bone and posterior elements of C2 are decorticated as well to receive the graft. We prefer to hold the ribs solidly down against the occiput and C2 using a small maxillofacial screw through the rib into the occiput and a titanium cable wrapped around the rods. If allograft is used, then the chips are packed into the O-C2 space as appropriate. Some surgeons choose to use recombinant human BMP (rhBMP) or a graft adjunct, although these biological agents are generally off label in the pediatric age group. If an intraoperative CT is available, a spin after hardware placement is very useful, as it documents the position of the hardware and the craniocervical alignment prior to softtissue closure,allowingforanyrarelyneededadjustmentsandobviatingtheneedfor immediate post-operative imaging.
Oral Boards Review—Management Pearls
1. Proper set-up of the operating room is important so that reconstructed CT images and fluoroscopy can be easily seen and referenced. 2. Careful attention to the vertebral canal at C2 is important to avoid arterial injury. For a surgeon inexperienced with the placement of C2 pars screws, or in the presence of unfavorable patient anatomy, it is best to use an alternative approach, such as a translaminar screw placement, rather than risk injury to the vertebral artery. 3. If a vertebral artery injury occurs during screw placement, the screw placement should be completed to control bleeding. If the injury occurs on the first side, a screw should not be placed contralaterally, which would put the remaining vertebral artery at risk. An immediate post-operative angiogram is required to detect the presence of a pseudoaneurysm or other complication. Ideally, the angiogram will demonstrate vertebral artery occlusion on the side of injury all the way from its origin, greatly lessening the risk of embolization-related ischemia. Any additional complications from this injury can typically be managed endovascularly.
105
6 0 1
Pediatric Neurosurgery
Aftercare
The patient is maintained in a hard cervical collar, with a custom collar usually necessary for patient comfort. The collar is worn 24/7. If intraoperative CT imaging was obtained, then no x-rays are needed. Otherwise, a plain lateral cervical spine film is obtained. Plain lateral cervical spine films are taken at 1 and 2 months postoperatively to document hardware integrity. At 2 months, if the hardware is intact and the surgeon knows the placement is solid, collar restrictions may begin to be lifted. A thin-cut cervical CT with 2-dimensional reconstructions is obtained 4 months after surgery to document fusion. If fusion is present, the collar is removed. If fusion is not present, a repeat CT is done in 2–3 months depending on the clinical circumstance. Patients who have failed to achieve fusion by 1 year after surgery or who demonstrate hardware movement or bony lucencies around the hardware require reoperation. Complications and Management
Aside from intraoperative events, the most common complications of craniocervical fusion are wound issues and fusion failure. Small stitch abscesses may be managed with local wound care and oral antibiotics. Deeper wound infections require operative debridement. For infections involving and surrounding the bone graft, the bone graft must be removed, but the instrumentation may generally be kept in place. Appropriate, culture-directed intravenous antibiotics should be administered for 6 to 8 weeks duration, followed by re-do of bony fusion at a later date. Fusion failure, defined as hardware shifting or a failure to achieve a solid bony arthrodesis, must be managed with reoperation. Surgical strategies in these cases revolve aroundachievingadequatebonepurchaseforhardwarerevisionoraugmentationofthe arthrodesis. The use of rhBMP, if not previously used, can be helpful here.
Oral Boards Review—Complications Pearls
1. In pediatric OC fusions, careful attention to intraoperative technique and screw placement will give the construct enough strength to result in successful arthrodesis. Postoperative imaging is mandatory to ensure that hardware integrity is present and ultimately, that the fusion is successful. 2. Proper fitting of the cervical orthosis is important to avoid skin breakdown and pressure sores. A custom collar is frequently necessary.
Evidence and Outcomes
Many modern studies of pediatric patients with AOD have shown that the success rates of surgical fusion using internal fixation are extremely high, usually in the 95–99% range (Mazur et al., 2014; Vedantam et al., 2017). Previous studies using bone–wire–halo strategies are less successful and fraught with all the complications that come with halo usage. Intuitively this makes sense, as AOD patients are almost always previously healthy and have normal anatomy. High rates of success should be expected.
106
Traumatic Atlanto-Axial Dislocation
Pivot Points
1. Patients presenting with severe craniocervical instability may also have intermittent profound neurological and cardiorespiratory instability in the field, emergency department, and even pediatric ICU, resulting from what would normally be seemingly trivial changes in position. Rare patients, for example, exhibit instability any time vertex pressure (manual or from padding) is removed. In such cases, emergent halo ring and vest placement, generally with introduction of a mild compressive force, may be needed to temporize until surgery. 2. Instrumentation of the pediatric craniocervical junction may be problematic depending on age and anatomy. Ideally, a solid construct incorporating suboccipital keel screws and C2 pars screws can be used. In very young children or those with suboptimal bony or vertebral artery anatomy, however, other techniques such as translaminar C2 screws, or even cable- immobilized rib fusion graft and halo placement, may be necessary.
References and Further Reading
Pang D, Nemzek WR, Zovickian J. Atlanto-occipital dislocation: part 1—normal occipital condyle-C1 interval in 89 children. Neurosurgery. 2007 Sep;61(3):514–521 Pang D, Nemzek WR, Zovickian J. Atlanto-occipital dislocation—part 2: The clinical use of (occipital) condyle-C1 interval, comparison with other diagnostic methods, and the manifestation, management, and outcome of atlanto-occipital dislocation in children. Neurosurgery. 2007 Nov;61(5):995–1015. Bertozzi JC, Rojas CA, Martinez CR. Evaluation of the pediatric craniocervical junction on MDCT. AJR Am J Roentgenol 2009; 192:26–31 Mazur MD, Sivakumar W, Riva-Cambrin J, Jones J, Brockmeyer DL. Avoiding early complications and reoperation during occipitocervical fusion in pediatric patients. J Neurosurg Pediatr. 2014 Nov;14(5):465–475. Hankinson TC, Avellino AM, Harter D, Jea A, Lew S, Pincus D, Proctor MR, Rodriguez L, Sacco D, Spinks T, Brockmeyer DL, Anderson RC. Equivalence of fusion rates after rigid internal fixation of the occiput to C-2 with or without C-1 instrumentation. J Neurosurg Pediatr. 2010 Apr;5(4):380–384. Anderson RC, Ragel BT, Mocco J, Bohman LE, Brockmeyer DL. Selection of a rigid internal fixation construct for stabilization at the craniovertebral junction in pediatric patients. J Neurosurg. 2007 Jul;107(1 Suppl):36–42. Vedantam A, Hansen D, Briceño V, Brayton A, Jea A. Patient-reported outcomes of occipito cervical and atlantoaxial fusions in children. J Neurosurg Pediatr. 2017; 19(1):85–90.
107
8 0 1
Spastic Quadriplegia David Harter
13
Case Presentation
A 14-year-old male and his mother present to the neurosurgeon’s office complaining of excess muscle tone. She notes that he was born at 32 weeks gestation and suffered intraventricular hemorrhage. Hydrocephalus did not develop and shunt placement was not required. Metabolic screening was negative at birth. She notes that he had failure to thrive, and development has been impaired, particularly of motor skills. She adds that his motor tone makes activities of daily life, transfers, and transport difficult. He has had multiple tendon-release operations of the lower extremities and has also required surgery for spontaneous hip dislocation. He has not undergone any spinal procedures, but he does have mild scoliosis. Oral feeding has been challenging; however, gastrostomy placement has not been required. Medical management has included extensive physical and occupational therapy and oral baclofen. His mother notes that oral baclofen therapyhasresultedinexcessdaytimesomnolence.Physicalexaminationdemonstrates a wheelchair-bound, thin-appearing adolescent boy in no acute distress. There is strabismus, and papilledema is absent. Speech is dysarthric, and excessive oral secretions are noted. There are flexion contractures, and clasped knife spasticity in the upper and lower extremities. Dystonic movements are noted in the neck and upper extremities, less so in the lower extremities. There are no fixed contractures noted. Hoffmann sign is absent; however, there are 5 beats of clonus bilaterally in the lower extremities. He is normocephalic. There is a 22° thoracolumbar dextroscoliosis without signs of spinal dysraphism. Questions
1. What is the most likely diagnosis? 2. Is imaging indicated? 3. Is consultation with other disciplines indicated?
Assessment and Planning
The diagnosis of spastic quadriplegia with dystonia due to cerebral palsy is made by the pediatric neurosurgeon.The differential diagnosis is narrow, given the clear clinical historyofprematurityandintraventricularhemorrhage.Also,thedevelopmentalhistory and clinical findings support the diagnosis. Alternative diagnoses are considerably less likely.Hydrocephalusisunlikely,giventheabsenceofmacrocephalyandofpapilledema,
109
0 1
Pediatric Neurosurgery
as well as the static nature of the neurological findings. Occult dysraphism is unlikely, given the involvement of the upper and lower extremities, as well as the absence of cutaneous markers. The patient presents with a predominant picture of spasticity with a component of dystonia. Oral baclofen and other medications have been trialed, with some efficacy but with excessive side effects. Given that his spasticity interferes with daily activities and function, spasms interfere with positioning, and he suffers from excess somnolence from oral baclofen, without hypersensitivity, he is a good candidate for a trial of intrathecal baclofen (ITB). The generalized nature of his dystonia is not a contraindication to ITB therapy. Consultation with a pediatric neurologist, geneticist or physiatrist may aid in decision making, and allow for the elimination of other possible diagnoses or confounding factors. Patients with atypical historical, physical findings or an unusual response to oral medications are good candidates for additional subspecialty input. Imaging, preferably magnetic resonance imaging (MRI), is recommended for the evaluationofsuspectedcerebralpalsy.Mostpatientshaveundergonediagnosticimaging either at birth or during development prior to referral for neurosurgical evaluation. For patients without prior imaging, MRI of the brain and spine is useful to exclude underlyinganatomicabnormalitiesthatmayaffectpumpplacementorsuggestalternative diagnoses. The diagnosis of cerebral palsy is supported by findings of periventricular leukomalacia, porencephaly, subcortical leukomalacia, or lesions of the basal ganglia or thalami.
Oral Boards Review—Diagnostic Pearls
1. The patient’s history is essential to proper diagnosis of spastic quadriparesis due to cerebral palsy. a. Prematurity b. Intraventricular hemorrhage c. Staticencephalopathy,followingacharacteristicdevelopmentalprogression of neurological findings 2. The evaluation of patients with cerebral palsy typically includes cranial imaging (preferably MRI), with the addition of metabolic and/or genetic testing for atypical cases (particularly in the setting of progressive encephalopathy). 3. The physical finding of generalized dystonia is not a contraindication to ITB therapy; in this setting dystonia is likely to improve in conjunction with spasticity.
Questions
1. What neurosurgical options are available? 2. What presurgical tests are required?
110
Spastic Quadriplegia
Decision Making
The patient has historical and physical findings to support the diagnosis of spastic quadriparesiswithdystoniaduetocerebralpalsy.Hehasundergonemedicaltherapywith oral baclofen, resulting in excess somnolence. No hypersensitivity reaction was noted. No alternative diagnoses are suspected. Neurosurgical procedures for spasticity include dorsal rhizotomy and ITB therapy. The nature of this patient’s condition, quadriparetic spasticity with generalized dystonia, makes ITB therapy the treatment of choice. For patients with focal dystonia, ITB therapy is unlikely to be effective. Some focal dystonias may be treated with botulinum toxin injection and physical therapy. Most groups recommend a trial of ITB prior to pump implantation, although this is not uniformly applied for patients with typical history and physical findings (particularly in the setting of thoracolumbar spinal fusion). The trial administration of baclofen is completed by lumbar puncture and injection into the subarachnoid space.The patient is usually sedated, and local anesthetic is given at the site of injection, usually the L4/5 interspace; 50–100 µg of baclofen for intrathecal injection is administered by barbatage technique.The patient is evaluated by caretakers or family and a physical therapist and/ or physiatrist for therapeutic response and is monitored for possible side effects, including respiratory suppression, somnolence, hypotonia, or hypersensitivity reaction. A positive result is documented by improved motor tone and the absence of side effects. Maximal response is usually noted within 2–4 hours of administration. After a positive trial, pump implantation is scheduled. Our practice is to keep the patient admitted and perform implantation the following day. Surgical Procedure
Patients and their caregivers considering pump placement for the long-term administration of ITB must be carefully counseled regarding the need for ongoing careful follow-up,aswellasthepotentialcomplications.Arrangementsforpost-proceduralcare, including dose titration and pump refills, is considered. Careful counseling regarding the potentialforoverdosingandunderdosing,includingthepotentiallylife-threateningsyndrome of baclofen-withdrawal, must be completed. Placement of an intrathecal pump is carried out on an elective basis under general anesthesia.Routinepreoperativeclearanceisobtainedincludingconfirmationofnormal coagulation.Pumpimplantlocationisconsidered;factorsincludingpatientanatomyand BMI,thepresenceofventriculoperitonealshunt,tracheostomy,gastrostomy,fusionmass, and instrumentation from prior scoliosis repair are weighed. Factors that may confound pump placement include low or high BMI, and particularly extensive fusion masses in patients who have undergone prior surgery for scoliosis or other spinal deformity. In patients with prior lumbar fusion consideration of catheter placement above the fusion mass, via laminotomy, or drilling through the fusion mass at a lower level are options. Both of these approaches add significant time and potential morbidity to the procedure. The patient is placed in the lateral decubitus position, with flexion of the hips and knees to the maximum extent possible considering the need for concurrent abdominal exposure. The L4/5 interspace is marked out by palpation, and a corridor extending to the paraumbilical region is prepared. A template of the pump may be useful for incision planning.Typically a transverse paramedian incision at the level of the umbilicus is used.
111
2 1
Pediatric Neurosurgery
We preferentially use the right side based on surgeon comfort; however, severe scoliosis or the presence of a ventriculoperitoneal shunt may favor placement on the left. The proposed field is sterilely prepared with chlorhexidine solution and intravenous antibiotics are administered. We do not routinely employ fluoroscopy; however, many groups recommend this adjunct to validate the precise location of the catheter tip in the intra-thecal space. The optimal terminus of the intrathecal catheter is debated, but for spastic quadriparesis with dystonia, the mid cervical level is chosen. A marker for palpation is placed on the skin prior to final draping allowing for estimation of catheter length, or as a landmark for easy identification on fluoroscopy if necessary.The proposed incision sites are infiltrated with local anesthetic with epinephrine. A small midline incision is made (approximately 2cm) in the midline over the L4/5 interspace. A small area of fascia is exposed in the paraspinal region, a small, (approximately 5mm) incision is made in the sagittal plane, then using a cephalad and slightly medial trajectory with the bevel of the needle oriented parallel to the sagittal plane, aTuohy needle is used to access the lumbar cistern. Upon egress of spinal fluid, the bevel is turned cephalad. Opening pressure may be obtained at the discretion of the surgeon. Intrathecal catheter length is then estimated based on the distance from the needle to the previously placed marker andthecatheterisadvancedcephalad.Resistanceshouldbeminimal,withtheguidewire in place. If significant resistance is obtained or difficulty with advancement is noted, the catheter should be withdrawn and the needle rotated.The catheter is then reintroduced and advanced. Fluoroscopy is employed on an as-needed basis or when difficulty with CSF access or catheter advancement is encountered. When the desired catheter length has been advanced, the guidewire is removed, and spontaneous CSF flow is confirmed. The abdominal incision is then opened sharply, and depending upon the desired pump position, suprafascial or subfascial, dissection is carried out. For placement in the suprafascialcompartment,thepumppocketisdissectedeitherwithinthesubcutaneous fatorbetweenthesubcutaneousfatandsheathoftherectusabdominis.Securingsutures are placed. For subfascial placement, which is recommended in smaller and/or thinner patients with spastic quadraparesis, the rectus sheath is sharply opened just off of the midline extendinglaterally.AnAllisclampisusedtoelevatethefascialedge.Therectusabdominis muscle is dissected from fascia, using blunt dissection and Bovie cautery. The use of a sponge stick, may facilitate displacement of the rectus abdominis away from the fascia. The tendinous inscription of the rectus muscle requires dissection to expand the pump pocket. The lateral boarder of the rectus sheath fuses with the aponeurosis of the transverse and oblique abdominal muscles, requiring connection of the compartments by division of fascial bands. Care is taken to avoid intraperitoneal exposure—the transversalis fascia is the final layer superficial to the peritoneum. Using a catheter or shunt passer, the intrathecal catheter is tunneled to the abdominal pocket and connected to the pump, which is filled and primed off the field. For initial pump placement, the lower commercially available concentration (500 µg per mL) of baclofen is used for pump filling because of the ability to give a lower minimal daily dose. For subfascial location of the intrathecal catheter, the passer is placed under at the lumbar fascia, and no connector or securing suture is used. A single suture is used to close the fascial opening. For suprafascial placement of the lumbar catheter, a securing right angle or straight connector is tacked to the fascia. A purse-string suture is placed around
112
Spastic Quadriplegia
the site of catheter exit from the fascia. Our preference is for placement of the catheter subfascially.This obviates the need for a connector and also allows for an additional layer of tissue over the entrance site of the catheter, as well as avoidance of a prominence over the connector in patients with low BMI. Confirmation of secure connection using the sutureless connector of the Medtronic SynchroMed II pump is made by an audible or palpable click, as well as the ability to easily rotate the connector on the pump. Previouslyplacedstaysuturesarethenplacedthroughthesutureloop.Properorientation of the pump, with the reservoir filling port facing externally, is confirmed.The sutures are tied. Hemostasis is confirmed. Our practice is to apply vancomycin, or bacitracin antibiotic powder in the pump pocket and at the site of the lumbar catheter prior to final closure. Incisions are closed in layers, with absorbable suture for the deep layers, and finally a subcuticularsuturefollowedbycyanoacrylatefortheskin.Thepumpisthenprogrammed with the desired initial settings based on response to test dose and provider experience. For patients with prior fusion in the lumbar region, positioning for placement of the intrathecal catheter is initially prone.The approach for patients with prior fusion involves an incision in the midline, at the previously used incision, or alternatively a paramedian incision. Subperiosteal dissection is used to expose the fusion mass, a high-speed drill is used to make a small laminotomy. Identification of the normal anatomic landmarks can be difficult given the irregular nature of the fusion mass. Operating loupes may be used or a microscope. When the ligamentum flavum or dura is identified, the Tuohy needle is used to access the lumbar cistern and the catheter is placed as usual. If dural exposure is adequate, a purse-string suture is placed. The entry site is then reinforced with tissue sealant and Gelfoam to prevent the potential for CSF leak. For patients in whom an approach above the fusion mass is planned, a midline incision is made, and the periosteum is reflected, typically in the mid to upper thoracic region over 1 level. Given normal anatomic landmarks, a small laminotomy is made, a small durotomy is made in the lateral aspect of the thecal sac, and the catheter was fed in with or without the Tuohy needle, with care being taken to avoid contact with the spinal cord. Depending on the desired catheter location, the catheter is either advanced cephalad or caudally. A purse-string suture is placed if feasible, and tissue sealant is placed at the entry site. In both cases, the catheter is tunneled to a lateral intermediate position after CSF egress is confirmed.The incisions are then closed in multiple layers, and the patient is placed supine for creation of the pump pocket, and connection of the intrathecal catheter, after tunneling to the pocket from the lateral intermediate incision. For patients with severe dystonia, intraventricular catheter placement for long-term administrationofbaclofentherapyhasbeendescribed,withgoodfollow-upandacceptable complications.
Oral Boards Review—Management Pearls
1. Proper patient selection for ITB placement can be confirmed by preoperative evaluation and a trial of ITB by lumbar puncture. 2. Patient and caregiver counseling is critical to ensure identify and treat potential perioperative complications, underdosage, and overdosage. 3. The presence of lumbar fusion may make catheter placement difficult.
113
4 1
Pediatric Neurosurgery
Pivot Points
1. Patients without access to adequate after care and follow-up support are poor candidates for ITB therapy. 2. Pediatric patients, particularly those with low BMI and medical comorbidities, are at elevated risk of pump-related complications. Indications should be carefully considered and subfascial pump implantation technique used when proceeding. 3. Severe spasticity in conjunction with generalized dystonia is a solid indication for ITB trial, although higher chronic dosing is generally required to effectively treat the dystonic symptoms. Focal dystonias and other movement disorders are relative contraindications.
Aftercare
Following pump placement, patients are nursed flat overnight, and monitored for signs of overdose. Some groups advocate longer periods of immobilization, and others placement of an abdominal binder in the perioperative period to prevent formation of a seroma around the pump. Seroma formation is probably more common in patients with subcutaneous rather than subfascial pump placement. Seromas are usually self-limited, and no intervention is undertaken. Conversely, CSF collections around the pump are usuallyprogressivelyenlarged,andmaybeaccompaniedbysignsofintracranialhypotension such as prolonged nausea, headache or neck pain. Routine perioperative antibiotics are continued for no more than 24 hours. The incision sites are clean and dry, the use of cyanoacrylate on the skin may ensure the presence of a physiologic barrier. In the immediate perioperative period, spasticity may be worse than baseline due to stress or pain. The pump dosage may be titrated as tolerated during the perioperative period, with appropriate monitoring. Upon discharge, the patient or caregiver is provided with a printout of the current pump settings including dosage, and estimated date for refill. Signs of overdose, under dose and withdrawal, as well as other complications are reviewed. Routine follow-up is scheduled for approximately 2 weeks after surgery. Problems encountered in the immediate perioperative period may include infection, CSF leak, wound breakdown, under-or overdosage. After the immediate perioperative period, CSF leak may occur in the presence of a catheter fracture or perforation, disconnection of the catheter or in some cases simply around the catheter. Cutaneous CSF leaks from the lumbar incision may initially be managed by oversewing of the incision. Persistent leakage usually requires operative exploration; radiographs of the pump and catheter may demonstrate a disconnection or migration. Exposure of the catheter site may demonstrate a leak through the fascia, and may be amenable to local repair and/or small local fascial transposition flaps, with reinforcement by tissue sealant. In all cases, CSF leak may be associated with subsequent occurrence of a pocket or other surgical site infection, and suspicion of such must be maintained. Fracture or dislodgment of the intrathecal catheter mandates
114
Spastic Quadriplegia
revision and replacement. CSF leaks at the site of the pump may be due to catheter fracture, inadvertent puncture of the catheter during refill, or disconnection. Alternatively, CSF may occasionally leak around the catheter from the lumbar site to the pump pocket. Catheter fractures are repaired by replacement. Disconnections are reconnected. It is important to consider the underlying CSF pressures in the development of CSF leak. Patients with a history of intraventricular hemorrhage may have compensated hydrocephalus, with moderately elevated ICP, which results in increased risk of cutaneous CSF leak or contained pseudomeningocele. Other causes of elevated CSF pressure can include venous hypertension, and pseudotumor cerebri. The treatment of choice for persistent leaks in the setting is shunt placement or revision of an existing shunt if present. Rapid return of spasticity usually relates to an underlying medical condition such as orthopedic or urologic disorders; however, it may also herald a mechanical complication or obstruction. After elimination of other likely confounding factors, if pump malfunction is suspected, a stepwise evaluation of pump function and catheter patency is recommended. Programming of a bolus and observation for therapeutic effect may be diagnostic and allow for treatment with simple dose escalation. The requirement for rapid dose escalation may also indicate pump malfunction. Should bolus administration be unsuccessful, aspiration at the catheter access port may be used to evaluate for catheter patency. Obstruction is indicated by lack of return of CSF or inability to flush forward; however, flushing forward may inadvertently result in the administration of the full catheter volume, which may lead to overdose. Emptying of the pump reservoir, and comparing the actual versus expected volume may allow for the diagnosis of improper refilling of the pump. In such cases, the aspirated volume is expected to be much less than the volume indicated on pump interrogation. Refilling of the pump reservoir in this case may solve the problem. Mechanical malfunction of the pump is uncommon. Baclofen withdrawal syndrome may occur secondary to pump malfunction. This life-threatening syndrome usually occurs due to the abrupt disruption of therapy and includes return of spasticity, formication, diaphoresis, hyperthermia, autonomic instability, and potentially seizure. The development of 1 or more of these symptoms requires evaluation on an emergent basis by experienced practitioners in a critical care setting. Management of ITB withdrawal has included intravenous or oral benzodiazepines, Cyproheptadine, oral baclofen, and intrathecal administration of baclofen via lumbar puncture, intrathecal catheter, or through the pump catheter access port.This acute syndrome is potentially life-threatening. Early recognition and management is critical to avoid prolonged hospitalization and morbidity. After the initial perioperative period, ITB dosage is titrated based on therapeutic effects and side effects. Generally, dose adjustments of no more than 10% are recommended in the ambulatory setting. Inpatient rehabilitation may allow more rapid and significant adjustments. Goals of treatment include increased comfort, pain control, facility of daily care, and decreased need for orthopedic procedures.
115
6 1
Pediatric Neurosurgery
Oral Boards Review—Complications Pearls
1. Acute baclofen withdrawal is a life-threatening medical emergency requiring prompt diagnosis and management including restoration of ITB administration and other supportive measures. 2. Persistent CSF leak without catheter fracture or other etiology may represent elevated CSF pressures and responds best to CSF diversionary procedures, and also poses a significant risk for infection. 3. Rapid dose escalation to maintain therapeutic effect may represent impending catheter occlusion, pump malfunction or error during refill.
References and Further Reading
Long-term intrathecal baclofen therapy for severe spasticity of cerebral origin. Albright AL, Gilmartin R, Swift D, Krach LE, Ivanhoe CB, McLaughlin JF. Journal of neurosurgery 2003;98:291–295. http://www.ncbi.nlm.nih.gov/pubmed/12593613 Practice parameter: diagnostic assessment of the child with cerebral palsy: report of the Quality Standards Subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society.Ashwal S, Russman BS, Blasco PA, et al. Neurology 2004;62:851–863. http://www.ncbi.nlm.nih.gov/pubmed/15037681 Intrathecal baclofen therapy: complication avoidance and management. Haranhalli N, Anand D, Wisoff JH, et al. Child’s nervous system: ChNS: official journal of the International Society for Pediatric Neurosurgery 2011;27:421– 427. http://www.ncbi.nlm.nih.gov/pubmed/ 20853002 Subfascial implantation of intrathecal baclofen pumps in children: technical note. Kopell BH, Sala D, Doyle WK, Feldman DS, Wisoff JH, Weiner HL. Neurosurgery 2001;49:753–756; discussion 6–7. http://www.ncbi.nlm.nih.gov/pubmed/11523691 Acute intrathecal baclofen withdrawal: a brief review of treatment options. Ross JC, Cook AM, Stewart GL, Fahy BG. Neurocritical Care 2011;14:103–108. http://www.ncbi.nlm.nih.gov/ pubmed/20717751 Long-term follow-up for lumbar intrathecal baclofen catheters placed using the paraspinal subfascial technique. Thakur SK, Rubin BA, Harter DH. Journal of neurosurgery Pediatrics 2015:1–4. http://www.ncbi.nlm.nih.gov/pubmed/26588457
116
Extratemporal Refractory Epilepsy Vamsidhar Chavakula, Eun-Hyoung Park, and Joseph R. Madsen
14
Case Presentation
The patient is a 10-year-old girl with no significant past medical history who developed seizures at the age of 5. Her seizure semiology was characterized by an aura of blurry vision,followedbyleft-armnumbness,progressingtoweaknessandeventuallyfalls.She was initially started on levetiracetam; however, this medication was ineffective at controlling seizures, and after a 6-month trial, she was started on carbamazepine as a second agent. She had partial response to the dual agent therapy and over the course of the next year only experienced 5 seizures. However, over the course of the next 2 years, her seizure frequency increased to 6 to 10 seizures per month. At this point a third agent was started, lacosamide. She had minimal response to the addition of the third agent, and at this point she was deemed to have medically refractory epilepsy given the poor response to a multi-agent regimen. Her seizure frequency progressed to at least 5 focal seizures per day with at least 2 generalized atonic seizures resulting in falls per day, and requiring constant use of a wheelchair. She was referred to a pediatric epilepsy surgeon for consideration of surgical options for treatment of her epilepsy. At the time of initial neurosurgical evaluation, she was 9 years old. Developmentally, she was at an age appropriate level with appropriate function on neuropsychological testing and was performing well at school. Her physical exam was notable for dysdiadochokinesia and impaired sensation of the left hand, and diminished fine motor skills. EEG recordings had demonstrated onset of seizure activity in the right medial parietal region. Magnetic resonance imaging (MRI) of brain performed at 1.5T showed evidence of gyral thickening and blurring along the intraparietal sulcus (Figure 14.1). Questions
1. What is the most likely diagnosis? 2. What further imaging is appropriate?
Assessment and Planning
In this child with a diagnosis of medically refractory epilepsy, defined as the persistence of seizures after appropriate treatment with 2 different medications, the seizure onset zone is outside of the temporal lobes, deeming this a case of extra-temporal lobe epilepsy. The finding of gyral thickening and blurriness is consistent with a diagnosis of focal cortical dysplasia. In this case, the primary goal of the epilepsy surgeon is to identify
117
8 1
Pediatric Neurosurgery
Figure 14.1. Axial T2-weighted MRI image demonstrating the area of focal cortical dysplasia, with abnormal gyral pattern.
a cortical lesion responsible for the seizure activity, and to maximally resect that lesion suchthatseizurefreedomisachievedwithoutthedevelopmentofpermanentneurologicaldeficits.Aninitialassessmentofthepatientinvolvesathoroughunderstanding of the clinical history and seizure semiology in order to develop a hypothesis for the functional localization of seizure onset. Comprehensive video EEG monitoring demonstrating electrographic localization of the seizures is also necessary. Finally, an anatomic basis for the seizures must be determined via imaging. The highest rates of success for resective epilepsy surgery are found when all data streams are concordant, that is, an anatomic lesion is found to be at the ictal onset zone, with semiology consistent with seizures arising from that location. Multiple imaging modalities exist for the evaluation of extra-temporal lobe epilepsy. MRI remains the most useful imaging modality for lesion evaluation. Although 1.5T MRI can detect presence of most lesions, the superior spatial resolution and clarity of 3T imaging allows for the detection of more subtle lesions. T1 and T2 weighted images are standard in any study to detect the presence of tumor, evaluate gray-white matter borders, and understand the fluid space anatomy. FLAIR (fluid-attenuated inversion recovery) sequences are useful in identifying edema, subcortical sclerosis, and atrophy. GRE (gradient-recalled echo) or SWI (susceptibility weighted imaging) sequences can demonstrate the presence of hemosiderin, which serves as a proxy for the presence of either a vascular lesion or hemorrhagic cortex. In cases of lesion near eloquent cortex,
118
Extratemporal Refractory Epilepsy
functional MRI (fMRI) may also be performed to better understand the location of the lesion with respect to functional areas. Other modalities that may be performed include ictal or inter-ictal PET (positron emission tomography) and SPECT (single photon emission coherent tomography), which are nuclear medicine studies that seek toidentifyvariablecerebralmetabolismandperfusionrespectivelyattheepilepticonset zones. Magnetoencephalography (MEG) is another testing modality, which relies on the presence of magnetic dipoles as a proxy for electrographic activity in order to localize seizure activity. The types of lesions that may cause extra-temporal epilepsy are quite varied, with pathology including tumor, infection, infarcted or post-hemorrhagic cortex, vascular malformation (arteriovenous malformation or cavernous malformation), focal cortical dysplasia, cortical heterotopia, and so on.
Oral Boards Review—Diagnostic Pearls
1. The most important part of pre-surgical epilepsy evaluation is understanding the clinical history and semiology of the seizures. A patient in whom seizures always present in the exact same fashion is most suggestive of focal onset of seizures. Multiple seizure semiologies raises concern for multi-focal epilepsy, which may not be amenable to resective epilepsy surgery. 2. Imaging—The goal of imaging is to identify a focal lesion which is the source ofictalonset.Anatomical,functional,andmetabolicimagingsequences may assist in detecting a lesion. 3. EEG provides a functional localization of seizure onset. If non-invasive scalp EEG does not provide clear localization of seizure focus then either short- term or long-term electrocorticography (ECoG) via implanted electrodes may be implemented to better identify the ictal onset zone.
Questions
1. What additional studies may be performed if seizure onset zone is ambiguous? 2. How does localization of seizures to eloquent cortex affect surgical planning?
Decision Making
Oncetheappropriateimagingstudiesandnon-invasiveelectrographicmonitoringhave beenperformed,thesurgeonmustdeterminewhetherenoughinformationispresentto safely proceed with surgical resection. If there is discordance between the anatomic and functional studies, consideration must be given to intracranial EEG via either placement of grids and strip electrodes or placement of stereotactic EEG (sEEG) electrodes. If initial electrode recordings are unequivocal for seizure activity, the surgeon may proceed with resection. If there remains uncertainty about seizure onset, electrodes can remain in place for up to 2 weeks, and anti-epileptic drugs (AEDs) may be weaned in order
119
0 2 1
Pediatric Neurosurgery
to induce seizure activity and promote accurate localization of seizure focus so that the most targeted resection may be performed. It is vital to understand the relationship of the potential resection zone to any neighboring areas of eloquent cortex so that maximal seizure reduction occurs with minimal neurological deficit. Question
1. What tools may be used to achieve maximal lesion resection?
Surgical Procedure
The exact procedure must be tailored to the location of the lesion. Typically, surgery is performed under general anesthesia. Choice of anesthetic agents is important if ECoG or neuromonitoring are to be performed. Consideration may be given to performing awake surgery if the lesion is adjacent to eloquent cortex. Intraoperative neuronavigation and ultrasound may be utilized during surgery to identify lesion boundaries. Intraoperative MRI, although not necessary, may also be a useful tool to determine whether the entire region of abnormality has been resected, especially in the case of subtle lesions. In this case, seizures were localized to an area of focal cortical dysplasia in the right parietal lobe.The patient was positioned supine with 3-point fixation in a Mayfield head clamp with the head turned such that right side was superior and parallel to the floor. Neuronavigation was then registered and utilized to design the incision. A curvilinear skin incision was performed, followed by craniotomy. A 32 contact grid electrode was placed over the exposed fronto-parietal cortex and ECoG was performed to elucidate the seizure onset zone. This case illustrates the potential to combine reconstructed images with the intraoperative view and ECoG. Prior to surgery we generated a 3-dimensional representation of the surface of the brain using the 3D Slicer (open source medical image computing platform). Direct inspection of the sulcal pattern suggested the location of the central sulcus well in front of the evident cortical dysplasia. We were able to align our intraoperative photo of the brain surface with the gyral pattern on the reconstructed brain surface (Figure 14.2). Cortical dysplasia was found deep to the contacts shown in Figure 14.3 (upper panel) which corresponded to the highest spike frequencies and the area encompassing those electrodes was removed (Figure 14.3, lower panel). Additional discretionary methods may be used to help refine resection planning. For example, a recently reported computational method called Granger causality may be used to generate a network map of related cortical circuits, which in this case corresponded to the area involved in epileptic spike generation (Figure 14.4). Theinvolvedcortexwasresectedwithneuronavigationandultrasoundassistance,as the lesion was noted to be echogenic. Post resection corticography showed no evidence of abnormal activity. Intraoperative MRI was then performed to ensure gross total resection of the area of cortical abnormality. The dura was then closed in watertight fashion, and the bone flap was replaced with titanium screws and plates, followed by galeal
120
Extratemporal Refractory Epilepsy
Figure 14.2. Merged image of two intraoperative photos showing dural opening and placement of electrocorticography grid over the region of focal cortical dysplasia overlaid onto 3D reconstructed brain surface. Central sulcus is marked by the blue circles.
closurewithinterruptedabsorbablesuturesandrunningabsorbablesutureclosureofthe skin. The patient has been seizure-free since the surgery. Aftercare
Patients are often monitored in the Intensive Care Unit (ICU) for at least 1 day. They are kept on their home epilepsy drug regimen, and weaning of these agents is not
121
21
Pediatric Neurosurgery
Figure 14.3. Map of electrodes identified as frequent spikes and resected area displayed on 3D reconstructed brain surface with post resection photo taken in the operating room. Central sulcus is marked by the blue circles.
performed until months after the resection has been performed. Patients should continue close follow-up with their neurologist, and further EEG monitoring and imaging, although not routinely necessary, may be performed depending on postoperative seizure frequency. Further care rests on the specific pathology of the lesion. For example, a tumor will require referral to oncologist for further workup and treatment. Dysplasia doesnotrequireanyadditionaloradjunctivetherapy,althoughresidualdysplastictissue
122
Extratemporal Refractory Epilepsy
Figure 14.4. Granger causality map (causal connectivity map and causal nodes map) produced using intraoperative ECoG data obtained from the patient (the details of the causality map have been published in Park and Madsen, 2018).
may be responsible for persistent seizures or failure to improve after respective epilepsy surgery.Thespecificdysplasiasubtyperevealedonpathologyhassomeprognosticsignificance for long term seizure control. For example, cortical dysplasia type IIb (“balloon cell dysplasia”) tends to be relatively anatomically focal and carries a good prognosis compared to other types.
123
4 2 1
Pediatric Neurosurgery
Oral Boards Review—Management Pearls
1. Patients should remain on their home AED regimen postoperatively, and a slow wean may be performed under the careful supervision of an experienced epileptologist. 2. Lesion pathology should be followed closely and specific postoperative management should be dictated by the natural history of the noted pathology.
Pivot Points
In patients with medically refractory epilepsy, adequate presurgical workup must be performed to ensure that lesional epilepsy from a single focus is present. 1. Discordant information in clinical history, semiology, and functional and anatomic studies may suggest the need for extended intracranial EEG recording as opposed to single stage resection. 2. The presence of multifocal seizure onset may also steer away from a respective procedure and towards a neuromodulatory strategy, such as vagal nerve stimulation.
Complications and Management
Specific complications depend on the exact location of the lesion. In the case of lesions adjacent to eloquent cortex, patients must be counseled regarding neurological deficits related to the region of interest. For lesions adjacent to motor or sensory regions, deficits in strength or sensation should be explained to the patient. For motor deficits, intensive physical therapy may significantly improve any postoperative weakness. Language deficits need be considered in lesions near dominant language areas, and if deficits do arise, speech therapy may be initiated.
Oral Boards Review—Complication Pearls
A thorough peri-operative assessment is necessary to understand the relationship of the lesion with respect to adjacent eloquent cortex. The surgeon must make an informed decision on the maximal amount of lesion that may be resected while not incurring neurological deficits. Evidence and Outcomes
In most studies, success of epilepsy surgery is defined using the Engel classification score. Class I reflects complete seizure freedom or presence of few non-disabling seizures, Class II refers to rare presence of disabling seizures, Class III is worthwhile improvement in seizure frequency, and Class IV means no significant improvement. Given the heterogeneouspathologyresponsibleforextra-temporalepilepsy,outcomesarevariable.
124
Extratemporal Refractory Epilepsy
In general, seizure freedom following extra-temporal epilepsy are lower than cases of temporal lobe epilepsy. Long-term seizure freedom rates in cases of extra-temporal epilepsy have been reported between 27–46%, with occipital and parietal resections more favorable than frontal resections. References and Further Reading
Baltuch GH, Villemure J-G, Kandula P, Placantonakis DG, Schwartz TH: Operative techniques in epilepsy surgery. New York: Thieme, 2009. Park E.-H., Madsen JR: Granger Causality Analysis of Interictal iEEG Predicts Seizure Focus and Ultimate Resection. Neurosurgery 82:99–109, 2018. Elsharkawy AE, Behne F, Oppel F, Pannek H, Schulz R, Hoppe M, et al: Long-term outcome of extratemporal epilepsy surgery among 154 adult patients. J Neurosurg 108:676–686, 2008. Rasmussen T: Surgery for central, parietal and occipital epilepsy. Can J Neurol Sci 18:611–616, 1991. Tellez-Zenteno JF, Dhar R, Wiebe S: Long-term seizure outcomes following epilepsy surgery: a systematic review and meta-analysis. Brain 128:1188–1198, 2005.
125
6 2 1
Hemispheric Refractory Epilepsy Brian J. Dlouhy and Matthew D. Smyth
15
Case Presentation
A 4-year-old boy presents with right hemiplegic cerebral palsy and seizures. His seizures consist of right eye deviation, jaw clenching, choking sound, emesis and a loss of consciousness. Per his mother, many of his seizures last longer than 5 minutes. He typically has 1 seizure per month but can have them more frequently. He was born full term via cesarean section due to failure to progress.The pregnancy was uncomplicated, and at birth APGAR scores were fine. He began having apneic events associated with eye deviation and nystagmus on day 1 of life. EEG confirmed neonatal seizures. There is no family history of seizures. He has had some developmental delay, most notably with speech and motor development. Despite multiple antiepileptic drugs (AEDs), he continues to have seizures. Referral was made to a multidisciplinary epilepsy team for further evaluation. On neurological exam, he makes poor eye contact, speaks in single words, and moves all 4 extremities, the left side more than the right. He holds his right hand close to the body with a clenched fist. He wears a brace on his right lower extremity. Questions
1. What is the diagnosis? 2. What studies should be considered next? 3. What imaging should be done next? 4. What is the appropriate timing of the diagnostic work-up?
Assessment and Planning
This child has medically refractory epilepsy and his seizures are characteristic of complex partial epilepsy. With right-sided hemiplegia on exam and ictal right eye deviation, one would suspect left sided seizure onset. According to the International League Against Epilepsy (ILAE), drug resistant epilepsy occurs when a person has failed to become (and stay) seizure free with adequate trials of 2 AEDs. To determine if this child would be a possible surgical candidate, video encephalography (VEEG) monitoring is conducted. VEEG reveals bilateral slowing, left more than right, and very frequent interictal discharges, left more than right. A total of 4 clinical and electrographic seizures are captured, the first with apparent onset in the left hemisphere.The remaining seizures
127
8 2 1
Pediatric Neurosurgery
Figure 15.1. Preoperative MRI in (A) axial and (B) coronal views of a 4-year-old boy with a left perinatal MCA infarct resulting in left hemispheric refractory epilepsy. are remarkable for indeterminate but likely left hemisphere onset with early transfer to the right temporal lobe. To assess brain abnormalities present that may cause seizures, magnetic resonance imaging (MRI) of the brain is conducted (Figure 15.1). This reveals a partial left MCA infarct, which probably occurred in the perinatal period. No masses, tumors, or hydrocephalus is found. No abnormal gyri or evidence of cortical dysplasia or mesial temporal sclerosis is identified. To further assess the brain anatomy and evaluate for dysfunctional regions and better establish seizure foci, a positron emission tomography (PET) is conducted (Figure 15.2). This reveals a hypometabolic left hemisphere, most prominent in the region of the perinatal infarct. No other abnormalities identified, specifically, none seen in the right hemisphere.
Figure 15.2. Preoperative PET scan of a 4-year-old boy with a left perinatal MCA infarct resulting in left hemispheric refractory epilepsy.
128
Hemispheric Refractory Epilepsy
Oral Boards Review—Diagnostic Pearls
1. All patients are evaluated by the multidisciplinary epilepsy team. This entails a history and physical examination and analysis of the semiology of the seizures, plus any additional indicated imaging and functional brain studies. 2. Other diagnoses that can mimic epileptic seizures includes a. syncope and anoxic seizures b. behavioral, psychiatric, and psychological disorders c. sleep related conditions d. paroxysmal movement disorders e. migraine associated disorders f. other miscellaneous events. 3. Further work-up includes VEEG monitoring of seizures, MRI, PET, and neuropsychological evaluation. 4. Additional diagnostic tests occasionally used include SPECT (single positron emission computed tomography) and MEG (magnetoencephalography). 5. In cases of hemispheric epilepsy, many patients will have deficits localized to that hemisphere. Therefore, the hemisphere contralateral to the hemiplegia should be demonstrated by radiological (MRI/CT) and/or functional (VEEG, PET) evaluation to have a diffuse abnormality. 6. More importantly the remaining hemisphere should be normal to have a good result following surgery. Spread of epileptiform discharges to the normal hemisphere on EEG or even rare independent discharges on the normal side however does not necessarily predict a poor response to surgery.
Questions
1. How do these clinical and physical exam findings, radiological findings, and EEG findings influence surgical planning? 2. What is the most appropriate intervention in this patient? 3. What is the most appropriate timing for intervention in this patient?
Decision Making/Patient Selection
The structural and metabolic imaging, history and EEG findings are consistent with predominant effects and epileptic onset diffusely throughout the left hemisphere. In general, hemispherectomy or hemispherotomy is indicated for the treatment of refractory hemispheric epilepsy. The indication is the same; independent of whether a hemispherectomy or hemispherotomy is utilized. As described byVillemure, the surgical decision to proceed to hemispherotomy is based on the critical evaluation of the following6parametersinepilepsypatients: seizures,etiologies,neurologicalstatus,electroencephalography, imaging, and neuropsychology. Medicalintractabilityisarequirement.However,long,exhaustivetrialsofanti-seizure medications may not be necessary in hemispheric epilepsy as the seizure frequency is
129
0 3 1
Pediatric Neurosurgery
often very high. Determining the etiology of the epilepsy will help predict the effectiveness of anti-seizure medications. Rasmussen’s encephalitis, SturgeWeber syndrome and cortical dysplasia almost always result in intractable epilepsy. In an ideal patient, the brain insult is unilateral and widespread throughout the hemisphere.Thepathologiesknowntobenefitfromhemispherotomyhavealreadybeenwell identified.Acquiredconditionsincludetrauma,infection,andRasmussen’sencephalitis. Congenital conditions include perinatal vascular infarct resulting from carotid or middle cerebral artery occlusion, hemimegalencephaly, diffuse hemispheric cortical dysplasia, non-hypertrophic diffuse hemispheric migrational disorder, and extensive Sturge– Weber syndrome. Classically,thepatienthasacompleteandstablehemisphericsyndromecharacterized by hemiplegia and hemianopsia. However, this varies depending on the etiology. In certain cases, such as in perinatal infarct, plasticity may have resulted in varying degrees of preservation of motor function bilaterally. In some conditions at an early stage, such as Rasmussen’s encephalitis or extensive Sturge–Weber, there may be debilitating seizures and minimal neurological deficits at the time of presentation. However, in all of these cases, either the disease itself (e.g., Rasmussen’s encephalitis) or ongoing seizures will lead to worsening neurological decline. The electroencephalographic abnormalities of the affected hemisphere are usually multifocal, diffuse and independent, reflecting the extent of the hemispheric involvement and the severe epileptogenicity. Epileptic abnormalities from the good hemisphere are often seen. From a prognostic view, it is important to evaluate these to determine if they are secondary or independent.Their presence is not a contraindication tohemispherotomy,astheymayrepresentdependentorintermediateepileptogenicity, in which case, the ultimate seizure outcome should be excellent; nevertheless, their presence remains slightly unfavorable. However, the abnormalities in the “good hemisphere” raise concern about possible etiologies that could affect the brain bilaterally, bringing into question the nature of the anatomical substrate and the presence of secondary epileptogenesis. Such findings explain some cases in which seizures persist after hemispherectomy. The ideal hemispherotomy candidate has ipsilateral ictal and interictal epileptiform activity, unilateral MR imaging abnormalities, contralateral hemiplegia, and a normal contralateral hemisphere. However, certain patients present with a mixed picture of bilateralelectroencephalography(EEG)findingsandsevereintractableepilepsy,prompting considerationofamoreaggressivetreatmentapproach.Cilbertoet al.foundthat7patients with bilateral seizure onset noted on routine or video-EEG monitoring benefited from hemipsherotomy with improvement in seizure control and overall quality of life, thus introducing the possibility of surgery for patients who normally would not meet criteria for hemispherotomy. Typically, thorough structural and functional brain imaging, as well as neuropsychologicalevaluation,isneededestablishbaselinedataandtodocumentthepathologic hemisphere and demonstrate integrity of the “good” hemisphere is essential prior to surgery.
130
Hemispheric Refractory Epilepsy
Questions
1. What are the different surgical approaches to treating hemispheric epilepsy? 2. What is the difference between a hemispherectomy and hemispherotomy 3. Which areas are most commonly observed to have incomplete disconnection with a hemispherotomy?
Surgical Procedure
The first anatomic hemispherectomy (AH) for the treatment of epilepsy was performed in 1938 by McKenzie. In 1950, Krynauw reported on the first major series of AH for intractable seizures. In these 12 patients, seizure control was excellent and AH subsequentlygainedwidespreadpopularity.ComplicationsofAH,namelysuperficialcerebral siderosis, encouraged modifications to the original technique.Therefore, the procedure evolved and technical variations were established based on the realization that parts of the hemisphere could be left in situ but disconnected. Hemispherotomy techniques consist of variable amount of cortical removal associated with hemispheric disconnection. All the techniques share callosotomy and disconnection of the frontal, temporal, parietal and occipital lobes and can be summarized into 3 groups: (1) the lateral approach through the frontal and/or temporal opercula and Sylvian fissure; otherwise known as the peri-insular hemispherotomy (PIH) and first reported by Villemure; (2) the vertical approach using a technique that reaches the lateral ventricle and then corpus callosum from the brain vertex, otherwise known as the vertical paramedian hemispherotomy and first described by Delalande; and (3) the lateral approach through the Sylvian fissure; otherwise known as the transylvian hemispherotomy and first reported by Schramm. As described by Morino et al., specifically, all hemispherotomy techniques consist of disconnection of the following projection and commissural fibers: internal disruption of the internal capsule and corona radiata,resectionofthemedialtemporalstructures,transventricularcorpuscallosotomy, and disruption of the frontal horizontal fibers. Here, we will discuss the operative steps associated with the peri- insular hemispherotomy (PIH)—our modification of the approach described byVillemure and Mascott and Shimizu and Maehara (Figure 15.3). Positioning
Patients are positioned supine on the operating table with the head positioned laterally. A gel roll or rolled towel may be placed under the shoulder to facilitate positioning the head in a completely lateral position. All pressure points are padded and multiple straps placed across the patient. The head can be placed in a Mayfield 3 pin skull clamp or placed on a padded horseshoe headrest depending on the age of the patient. Frameless stereotacticnavigationisregisteredtothepatientandtheproposedcraniotomyandskin incision is planned and marked.
131
2 3 1
Pediatric Neurosurgery
Coronal
Axial
Figure 15.3. Hemispheric “cuts” required for disconnection in a peri-insular hemispherotomy. Incision, Craniotomy, and Dural Opening
A standard C-shaped incision is used to allow for a frontotemporal craniotomy that spans the Sylvian fissure (Figure 15.4). Frameless stereotactic navigation can be helpful in planning the incision and performing the craniotomy. The craniotomy is performed with burr holes and fashioned with a footplate. Rongeurs can be used to further remove the sphenoid wing anteriorly. After removal of the bone flap, the dura is opened in a C-shaped fashiontowardthesphenoidwingandstaysuturesareplacedalongtheedgesofthedura to keep tension on the dural flap and dural edges to allow for a clean operative field.
Figure 15.4. Operative head positioning and skin incision for peri-insular hemispherotomy. The head is positioned directly lateral on a horseshoe headrest or in a Mayfield 3-pin skull clamp. The incision is made in a C-shaped fashion to allow for a craniotomy centered over the sphenoid wing and extending to the posterior aspect of the Sylvian fissure.
132
Hemispheric Refractory Epilepsy
Surgical Approach—The 7 Steps
After the dura is opened, the Sylvian fissure, temporal lobe, and inferior frontal gyrus should be visualized. We breakdown our technique for peri-insular hemispherotomy into 7 steps. All resections and disconnections are performed using a combination of bipolar cautery, micro-scissors, suction, and an ultrasonic aspirator. Step 1. The Sylvian fissure is widely dissected from the sphenoid wing to the posterior aspect of the fissure and medially to expose the entire insula. The extent of the circular sulcus is then defined and dissected (Figure 15.5).
Figure 15.5. Intraoperative photographs: craniotomy, dural opening and steps 1–2: Sylvian fissure dissection, and frontal and temporal opercula resection. (A) Using stereotactic navigation, a frontotemporal craniotomy is fashioned and centered over the Sylvian fissure. (B) The dura is opened in a C shaped fashion and reflected anteriorly toward the sphenoid wing and held in place with stay sutures. (C) The Sylvian fissure is dissected open widely to the level of the insula. The circular sulcus underlying the frontal and temporal opercula is dissected as well. (D) The frontal and temporal opercula are resected, exposing the insula with overlying middle cerebral artery branches. TL: temporal lobe; FL: frontal lobe; STG: superior temporal gyrus; IFG: inferior frontal gyrus.
133
4 3 1
Pediatric Neurosurgery
Step 2. The frontal and temporal opercula are resected and sent for pathological evaluation (Figure 15.5). Step 3. The frontal horn of the lateral ventricle is entered using guidance and trajectory gained from stereotactic navigation. The ventricular opening is continued posteriorly to the atrium of the lateral ventricle and followed to the anterior extent of the temporal horn (Figure 15.6). Step 4. Once the temporal horn has been opened, a selective amygdalohippocampectomy is performed and sent for pathological evaluation.The tail of the hippocampus is resected posteriorly and medially, providing the mesial occipital disconnection (Figure 15.6). Step 5. From the frontal horn of the lateral ventricle, image guidance and/or Doppler ultrasonography is used to localize the pericallosal arteries through the corpus callosum. A transventricular corpus callosotomy is performed and extended from the frontal horn to the mesial occipital disconnection (Figure 15.7). Step 6. A frontal basal disconnection is performed using the anterior cerebral arteries to follow the anterior aspect of the corpus callosotomy from the frontal horn of the lateral ventricle through the basal frontal cortex to the arachnoid of the Sylvian fissure and pia/arachnoid of the sphenoid wing and anterior cranial fossa floor through the gyrus rectus (Figure 15.7). Step 7. Finally, the insula is decorticated, leaving the white matter and underlying basal ganglia intact (Figure 15.7). Hemostasis is achieved with bipolar cautery and thrombin soaked or diluted hydrogen-peroxide soaked cotton balls. An external ventricular drain is placed in the frontal horn of the lateral ventricle to clear blood and degradation products. The bone flap is replaced and the temporalis muscle, fascia, galea, and skin are closed in layers. The areas most commonly observed to have incomplete disconnection include the mesial occipital tissue and the basal frontal tissue with residual occipital and inferior frontal cortex remaining respectively.Therefore, these areas need more attention to ensure a complete disconnection. In certain cases, abnormal anatomy can make aspects of the hemispherotomy more challenging. The larger volume of tissue to disconnect in hemimegalencephaly can provide a challenge and usually requires more surgical time and potentially more blood loss. Following the anterior cerebral arteries can be difficult and if the anatomy is prohibitive, the midline falx can be a guide and good landmark to follow.
134
Figure 15.6. Intraoperative photographs: steps 3–4: ventricular opening from anterior frontal horn to anterior temporal horn, amygdalohippocampectomy, and mesial occipital disconnection. (A) Stereotactic navigation is used to choose the most appropriate entry point to the lateral ventricle through the white matter adjacent to the insula. The entire ventricle is opened from the anterior frontal horn to the anterior temporal horn following the C-shape of the ventricle. (B) The frontal horn of the lateral ventricle is exposed. (C) The head and body of the hippocampus (*) is observed in the anterior temporal horn of the lateral ventricle. (D) The tail of the hippocampus (*) is seen as well. (D) The amygdala and head/body of the hippocampus (*) is resected. (E) The tail of the hippocampus (*) is resected posteriorly and medially to the midline and splenium of the corpus callosum. This provides part of the mesial occipital disconnection. TL- MTG: temporal lobe—middle temporal gyrus; MFG: middle frontal gyrus; FH: frontal horn; CF: choroidal fissure.
6 3 1
Figure 15.7. Intraoperative photographs: steps 5–7: transventricular corpus callosotomy, frontal basal disconnection, and insula decortication. (A–B) Doppler ultrasonography is used to locate the pericallosal artery just above the interface between the septum pellucidum and the corpus callosum. (C) Once the artery is located, bipolar cautery and suction is used to dissect through the corpus callosum (CC) via subpial aspiration down to the level of the vessel. (D) The transventricular corpus callosotomy continues posteriorly, following the course of the pericallosal artery. The corpus callosotomy is continued to the area of the previous hippocampal tail resection to complete the mesial occipital disconnection. (E) A frontal basal disconnection is performed using the anterior cerebral arteries to follow the anterior aspect of the corpus callosotomy from the frontal horn of the lateral ventricle through the basal frontal cortex to the arachnoid of the Sylvian fissure and pia/arachnoid of the sphenoid wing and anterior cranial fossa floor. (F) The lateral ventricles are filled with diluted hydrogen peroxide soaked cotton balls to assist in hemostasis. The insula is then decorticated. FH: frontal horn; MFG: middle frontal gyrus; CC: corpus callosum; TL- MTG: temporal lobe—middle temporal gyrus; SW: sphenoid wing; CBs: cotton balls.
Hemispheric Refractory Epilepsy
Oral Boards Review—Management Pearls
1. Remember the 7 steps in a hemispherotomy. 2. The larger volume of tissue to disconnect in hemimegalencephaly can provide a challenge and usually requires more surgical time and potentially more blood loss. 3. The areas most commonly observed to have incomplete disconnection include the mesial occipital tissue and the basal frontal tissue with residual occipital and inferior frontal cortex remaining respectively.Therefore, these areas need more attention to ensure a complete disconnection. 4. Following the anterior cerebral arteries can be difficult and if the anatomy is prohibitive, the midline falx can be a guide and good landmark to follow.
Pivot Points
1. The individual anatomy of the patient will affect the 7 steps of a peri-insular hemispherotomy. For example, in challenging cases, a wider temporal lobectomy will facilitate the safe removal of mesial structures. 2. If anatomy is abnormal because of infarct, excessive tissue as in hemimegalencephaly, then use common anatomic landmarks to guide disconnection.
Aftercare
An MRI of the brain is obtained on postoperative day #1 to demonstrate disconnection (Figure 15.8). If a postoperative MRI is done weeks after surgery, the tissues may become more opposed and demonstrating disconnection on imaging may be difficult. The external ventricular drain is leveled to ensure continuous drainage for 5 days postoperatively. Usually by postoperative day #5, the cerebrospinal fluid (CSF)
Figure 15.8. Postoperative MRI demonstrating the complete disconnection in (A) axial and (B) coronal views. 137
8 3 1
Pediatric Neurosurgery
is xanthrochromic and the ventricular drain can be removed. In some cases when more tissue needs disconnection, such as in hemimegalencepahly, the ventricular drain needs to remain in place for longer than 5 days. Fevers are common after hemispherotomy, likely due to blood products within the ventricular system and not from infection. The use of external ventriculostomy can reduce the incidence of postoperative fevers. Complications and Management
During disconnection, large draining veins should be preserved to prevent cerebral edema, as well as increased bleeding, throughout the procedure.When decortication of the insula is performed, care should be taken to not enter the basal ganglia. The basal ganglia is friable tissue and once entered, often bleeds. Hemostasis of the basal ganglia can be difficult with bipolar cautery and usually requires hemostatic agents to stop bleeding. Hydrocephalus can also occur postoperatively. The incidence of this varies in the literature and appears to depend on surgical approach, technique, and etiology of the hemispheric refractory epilepsy and therefore patient anatomy.
Oral Boards Review—Complications Pearls
1. Fevers are common are hemispherotomy. Aggressive infectious work-up post- hemispherotomy should only be conducted in cases where there is serious concern over infection with signs/symptoms on exam and laboratory values. 2. Hydrocephalus post-hemispherotomy may present early but can present even years after surgery. Patients need to be observed and have good long-term follow up to ensure they won’t need CSF shunting.
Evidence and Outcomes
Hemisphericdisconnectionhaslongbeenusedtotreatpatientswithintractableepilepsy secondary to unilateral hemispheric syndromes such as extensive unilateral cortical dysplasia,hemimegalencephaly,Sturge-Weberdisease,Rasmussen’sencephalitis,perinatal hemisphericinfarctandotherunilateralrefractoryepilepsy.Multiplestudieshaveshown hemispheric disconnection to result in a seizure freedom rate of 43–90%. Long-term, these patients are characterized by hemiparesis, hemianopia, language deficits, and cognitive impairment. The degree of all of these depends on the epilepsy syndrome,involvedhemisphere,andageoftreatmentaswellasanyotherassociatedmedical problems. The hemiparesis is spastic, patients can walk, and frequently arm movement is more impaired than leg movement. In many cases the fine pincer movements of index finger and thumb are not possible but handgrip is maintained. Patients will require rehabilitation, both physical and occupational therapy. Patients with maximal or near maximal hemiplegia with intractable epilepsy with radiological and functional imaging demonstrating unilateral hemispheric abnormality should be considered as candidates for hemispherotomy. Hemispherotomy
138
Hemispheric Refractory Epilepsy
irrespective of the actual variant performed gives total or almost seizure free status in 43–90% of cases. References and Further Reading
Villemure JG, Daniel RT. Peri-insular hemispherotomy in paediatric epilepsy. Childs Nerv Syst. 2006;22(8):967–981. Smith SJ, Andermann F, Villemure JG, Rasmussen TB, Quesney LF. Functional hemispherectomy: EEG findings, spiking from isolated brain postoperatively, and prediction of outcome. Neurology. 1991;41(11):1790–1794. McKenzie KG. The present status of a patient who had the right cerebral hemisphere removed. JAMA. 1938;111:168–183. Krynauw RA. Infantile hemiplegia treated by removing one cerebral hemisphere. J Neurol Neurosurg Psychiatry. 1950;13(4):243–267. RasmussenT.Postoperativesuperficialhemosiderosisofthebrain,itsdiagnosis,treatmentandprevention. Trans Am Neurol Assoc. 1973;98:133–137. Daniel RT, Villemure JG. Peri-insular hemispherotomy: potential pitfalls and avoidance of complications. Stereotact Funct Neurosurg. 2003;80(1-4):22–27. Danielpour M, von Koch CS, Ojemann SG, Peacock WJ. Disconnective hemispherectomy. Pediatr Neurosurg. 2001;35(4):169–172. Delalande O, Bulteau C, Dellatolas G, et al. Vertical parasagittal hemispherotomy: surgical procedures and clinical long-term outcomes in a population of 83 children. Neurosurgery. 2007;60(2 Suppl 1):ONS19-–32; discussion ONS32. Delalande O, Pinard JM, Basevant C, Gauthe M, Plouin P, Dulac O. Hemispherotomy: A new procedure for central disconnection. Epilepsia. 1992;33(Suppl 3):99–100. Rasmussen T. Hemispherectomy for seizures revisited. Can J Neurol Sci. 1983;10(2):71–78. Schramm J, Behrens E, Entzian W. Hemispherical deafferentation: an alternative to functional hemispherectomy. Neurosurgery. 1995;36(3):509–515; discussion 515–516. Schramm J, KralT, Clusmann H.Transsylvian keyhole functional hemispherectomy. Neurosurgery. 2001;49(4):891–900; discussion 900–901. Shimizu H, Maehara T. Modification of peri-insular hemispherotomy and surgical results. Neurosurgery. 2000;47(2):367–372; discussion 372–373. Villemure JG, Mascott CR. Peri-insular hemispherotomy: surgical principles and anatomy. Neurosurgery. 1995;37(5):975–981. De Almeida AN, Marino R, Jr., Aguiar PH, Jacobsen Teixeira M. Hemispherectomy: a schematic review of the current techniques. Neurosurg Rev. 2006;29(2):97–102; discussion 102. Morino M, Shimizu H, Ohata K, Tanaka K, Hara M. Anatomical analysis of different hemispherotomy procedures based on dissection of cadaveric brains. J Neurosurg. 2002;97(2):423–431. Kamath AA, Limbrick DL, Smyth MD. Characterization of postoperative fevers after hemispherotomy. Childs Nerv Syst. 2015;31(2):291–296. Sood S, Asano E, Chugani HT. Role of external ventriculostomy in the management of fever after hemispherectomy. J Neurosurg Pediatr. 2008;2(6):427–429. Limbrick DD, Narayan P, Powers AK, et al. Hemispherotomy: efficacy and analysis of seizure recurrence. J Neurosurg Pediatr. 2009;4(4):323–332.
139
0 4 1
Ruptured Arteriovenous Malformation Edward Smith
16
Case Presentation
A 12-year-old girl with no known past medical history or antecedent trauma presents to her local hospital with the sudden onset of the worst headache of her life and mild right-sided weakness. Over the course of an hour, she experiences worsening headache and exhibits progression of her weakness to right-sided hemiplegia. An emergent computerized tomographic (CT) study is obtained, ultimately followed by a digital subtraction angiogram (DSA; Figure 16.1). Questions
1. What is the likely diagnosis? 2. What additional imaging modality would be critical in the emergent setting? 3. What vessels are the likely sources of arterial supply to this lesion? 4. If the clinical examination continued to deteriorate rapidly, with somnolence andevidenceofherniation,whataresomeimmediatemanagementstrategies?
Assessment and Planning
The initial diagnosis is intracranial intraparenchymal hemorrhage, as documented by CT. Absent a history of trauma or known bleeding diathesis, the differential diagnosis should favor a vascular lesion, such as an arteriovenous malformation (AVM), followed by other structural causes of hemorrhage, including cavernous malformation, tumor or aneurysm. Typically, a CT angiogram (CTA) is performed immediately subsequent to the CT. CTA affords rapid identification of vascular lesions in most cases and affords the surgeon an understanding of the critical anatomy should emergent operation be deemed necessary. Decisionsonfurtherdiagnosticstudiesaredictatedbytheclinicalstatusofthepatient. If the child is clinically well, with a small hemorrhage and normal neurological examination, it may be possible to obtain detailed anatomical imaging, including multiplanar magnetic resonance imaging/angiography (MRI/A), in addition to a DSA. Ideally, a DSA will include injection of the internal carotids, external carotids and vertebrobasilar supply. In contrast, if the child is critically ill, there may be a need to operate prior to obtaining other studies.
141
2 4 1
Pediatric Neurosurgery
Figure 16.1. On the left is a non-contrast axial computerized tomography image demonstrating a large left frontal intraparenchymal hemorrhage (*) with associated mass effect and midline shift. On the right is an anterior-posterior (A-P) arterial phase image from the injection of the left internal carotid artery in a digital subtraction angiogram (DSA). Note a large, cone-shaped AVM nidus (arrow), fed from hypertrophied branches of the middle and anterior cerebral arteries.
Oral Boards Review—Diagnostic Pearls
1. Emergent assessment of a pediatric patient with a non-traumatic intraparenchymal brain hemorrhage should include AVM as a leading diagnostic possibility. 2. During initial radiographic evaluation of children with non-traumatic intraparenchymal brain hemorrhage, consider including CTA. 3. More detailed assessment with DSA should look for early draining veins, asymmetrically enlarged arterial feeding vessels and include external carotid, internal carotid and vertebrobasilar injections. Understanding the anatomy of arterial supply is critical to planning surgical treatment, as is knowledge of venous drainage. 4. Familial history of intracranial vascular disease, stroke and hemorrhage is important, looking for the rare genetic conditions associated with multiple AVMs, most notably hereditary hemorrhagic telangiectasia (HHT).
Summary of Initial Evaluation: • CT: If a child presents with an intraparenchymal hemorrhage (IPH) without a clear etiology on initial evaluation, AVM should be considered and a CT angiogram (CTA) maybehelpfulin the acute settingto identify the presence of dilatedvesselsor nidus.
142
Ruptured Arteriovenous Malformation
• If no clear lesion is found, repeat imaging with MRI in 4–6 weeks should be performed to evaluate the hemorrhage cavity after the clot has cleared. • Further testing is dependent on the stability of the patient. In general, MRI is helpful for 3-dimensional visualization of lesional anatomy, in particular for delineating the relationship between the malformation and underlying brain structures. Digital subtraction angiography (DSA) is critical for defining angioarchitecture. • Standard preoperative laboratory studies include a complete blood count (CBC), clotting times (PT/PTT), type and cross (T&C) for blood bank, and chemistry panel. Decision Making
Initial therapeutic maneuvers are dependent on the presentation of the child. For a child who is healthy or has chronic symptoms (such as seizure or developmental delay), there are often no immediate interventions necessary (with the exception of anti-epileptic medication if seizures are present). The following steps are warranted for the child who presents with an intracranial hemorrhage. It is important to note that severity of presentation can vary greatly and thus treatment must be individually tailored. For the child that presents with hemorrhage, as illustrated here, a number of immediate interventions should be considered prior to definitive management. These include • Access and stabilization: placement of large bore intravenous (IV) lines (at least 2), arterial line, bladder catheter, and intubation if needed for airway protection as well as a nasogastric tube if intubated. • Blood pressure control: labetolol or nipride with goal of normotension for age. • ICP control: elevation of the head of the bed and external ventricular drain placement if hydrocephalus is present. To prevent re-ruprture, it is important to avoid overdrainage of cerebrospinal fluid (CSF). • Seizure avoidance: Anti-epileptic medication if seizures suspected. Intraventricular hemorrhage with hydrocephalus may require urgent placement of an external ventricular drain, with care taken to plan a trajectory for drain placement that does not pose risk of causing additional hemorrhage by further damaging an underlying causative lesion. Large intraparenchymal hemorrhages—such as in the case illustratedhere—mayneedemergentevacuationofclottodecompressthebrainandreduce intracranial pressure (ICP). In these cases, it may sometimes be prudent to simply evacuate clot and not attempt AVM resection if the lesion is formidable or poorly visualized. Availability of a CTA can be invaluable in formulating an operative approach that avoids dangerous areas of the AVM while allowing clot resection. In contrast, for a child that presents in good clinical condition, the need for intervention is typically less urgent. Non-emergent management varies greatly depending onpresentation.Inelectivecases,preoperativelabsandimagingareneeded.Forpatients with a hemorrhage but minimal deficits, admission to the intensive care unit for blood pressure control and preoperative imaging studies is appropriate.
143
41
Pediatric Neurosurgery
In any case of AVM, there are certain key anatomical factors that should be considered during the evaluation. These features are generally best visualized on DSA and include:
• • • • •
High-flow versus low-flow lesions. Outflow stenoses. Varices in subarachnoid or ventricular spaces. Number and location of feeding vessels. Aneurysms: In approximately 7–25% of cases of cerebral AVM, there is an associated arterialaneurysmonafeedingpedicle.Oftentheseflowrelatedaneurysmsspontaneously regress following reduction in blood flow after treatment of the AVM.
Once the anatomy of the AVM and the clinical status of the patient has been determined, a treatment plan can be prepared. The goal of treatment is to remove or reduce the risk of bleeding or AVM growth. There are no currently accepted medical therapies for the primary treatment of AVM. While adjuvant medical therapy may be helpful (antiepilepticmedicationforseizure,painmedicationforheadache,etc.),theobliteration of an AVM is currently achieved either by surgical resection or treatment with radiation. The treatment goal is complete removal/obliteration of the lesion. Two major modalities are used—surgery or radiation. (The use of embolization as a standalone therapy for AVM remains controversial, with little data supporting long-term efficacy except in very simple, small lesions.) The decision to operate on an AVM is based on several factors: (1) eloquence of cortical location (including speech, motor function, and sensation), (2) pattern of venous drainage, (3) size, (4) associated aneurysms, (5) recent hemorrhage, (6) clinical deterioration, and (7) risk of complication from other modalities of therapy (such as radiation injury to the developing brain). Several of these factors are combined in the Spetzler-Martin grade that incorporates eloquence of location, pattern of venous drainage, and size and is considered predictive of outcome from surgical management (several modifications of this grading scale have been published, but the original remains best known and easiest to use). The Spetzler-Martin grade helps to predict surgical risk. If a low-grade lesion (1–3) is present, surgery should be considered. Higher-grade lesions (4 and 5) often benefit from multidisciplinary approach and might be considered for radiation therapy. Spetzler-Martin AVM grading scale: Size 0–3 centimeters >3–6 centimeters >6 centimeters
1 2 3
Non-eloquent Eloquent
0 1
Not present Present
0 1
Location
Deep venous drainage
144
Ruptured Arteriovenous Malformation
Questions
1. What is the importance of the pattern of hemorrhage relative to the location of the AVM? 2. What are some measures that can be employed preoperatively to reduce the risk of intraoperative hemorrhage and postoperative hyper-perfusion syndrome?
Surgical Procedure
Timing: If a child presents with symptoms of increased ICP then urgent operation may be necessary. If there are worrisome findings on angiography (high-flow lesion with intraventricular varices or aneurysms) then surgery may be planned within the same hospital stay. If not, then a delay of several weeks may help, with delayed reimaging offering better understanding of the anatomy for surgical or radiosurgical planning, as well as an easier surgical approach once the clot has resorbed. • A key element of AVM surgery is careful exposure of the AVM. If the lesion is on the surface (or any draining veins are superficial), then the craniotomy and dural opening need to be executed with care. Often, adhesions between the dura and AVM may occur, making it easy to tear AVM vessels during the opening. This can oftenbeavoidedwithslow,meticulousduralopening,and—occasionally—leaving areas of dura attached to the AVM and cutting around them. • A primary surgical principle for AVM resection is the obliteration of feeding arteries before occlusion of draining veins, as premature closure of outflow can lead to AVM rupture with uncontrolled bleeding. • AVMs are often wedge or cone shaped, and resection can be performed in a circumferential pattern, staying close to—but not entering—the nidus. It is helpful to try to maintain an even depth of resection around the lesion to avoid getting in a “hole” and caution must be taken to minimize retraction on draining vessels during dissection. • Repeated inspection of the surrounding brain for swelling or bleeding can aid the surgeon in preventing complications by early identification of poorly placed retractors or clips. • AVM vessels may coagulate poorly and consideration should be given to clip application or gentle tamponade (if the bleeding is of small volume) if bipolar electrocautery is not working. Every attempt should be made to avoid operating within the nidus itself. Embolization: Althoughnottraditionallyusedasastand-alonetreatmentforAVMsother than in rare cases with a small nidus and a small number of feeding pedicles, there is a growing literature on the use of newer embolization agents (including Onyx) for definitive treatment of brain AVM in adults. However, the situation in children is more complex and embolization is rarely used as a stand-alone modality, as the recurrence rate
145
6 4 1
Pediatric Neurosurgery
is higher, and lesion immaturity may preclude complete visualization angiographically. Regardless, embolization is a significant aid in the treatment of AVMs, reducing their blood supply and facilitating operative approaches (usually < 72 hours before surgery to prevent recanalization). Embolization also has a role in targeted treatment of non- operative lesions, by occluding areas at risk of hemorrhage such as aneurysms or high-risk (intraventricular) varices.
Oral Boards Review—Management Pearls
1. Total excision of an AVM is important to reduce the risk of rebleeding. 2. Sequential attack on AVM vasculature, starting with feeding arterial vessels and leaving venous drainage until the end of the case is critical. 3. Younger children can have significant blood loss relative to their total blood volume,soestablishinggoodintravenousaccessandhavingbloodavailablefor transfusion is important.
Pivot Points
1. If the patient presents in extremis with a hemorrhage, it may be necessary to decompress the clot emergently. If the AVM is large, complex or poorly visualized, it may sometimes be wiser to leave the AVM alone and only perform interventions necessary to control ICP, such as an external ventricular drain or partial clot removal. It can be important to leave a margin of clot behind deliberately in order to minimize the risk of rebleeding in the operating room. 2. Some of the most important AVM surgical decision making is performed well before ever entering the operating room. Whether an operation is warranted at all, deciding on perioperative adjuncts (such as embolization) and rehearsing a well-defined surgical plan of attack, with potential bailout strategies, are all steps crucial for success.
Aftercare
The management of AVM patients varies widely depending on the initial presentation, the clinical state of the patient and the anatomy of the AVM. A patient treated electively for a small frontal AVM will receive very different postoperative care than a critically ill child who has had a large, hemodynamically significant AVM emergently removed. However, most children will typically be monitored in the intensive care unit, with perioperative antibiotics, blood pressure control (varying based on age and AVM presentation) and frequent neurological examinations. Most of the immediate management steps for complex AVM postoperative care are reviewed in the“Complications and Management” section next. Once out of the hospital, much of the care becomes more uniform.
146
Ruptured Arteriovenous Malformation
Frequency of office visits: • Postoperative care will frequently consist of an office visit approximately 1 month postoperatively, then annually thereafter. Radiation therapy also involves annual visits post-treatment. Frequency of imaging: • In addition to a perioperative angiogram to confirm obliteration of the AVM, a MRI/A at 6 months may be helpful as a baseline study, to then be compared to subsequent annual MRI/A studies. The duration of repeated imaging varies by institution, but a common practice is to perform a MRI annually for 5 years, if feasible. • An angiogram (DSA) is often performed at 1 year postoperatively to confirm durable cure and exclude any residual lesion. Complications and Management
Some of the most devastating complications from AVM treatment occur in the immediate postoperative period, especially with larger or higher-flow lesions. As such, in addition to intraoperative management, meticulous attention to postoperative care in the ICU is crucially important. Neurologic deficit can occur following AVM resection, although the specific incidence of deficits is hard to specify, given the wide variability in AVM size and location. Overall, there is low postoperative morbidity in low-grade (1–3) Spetzler-Martin lesions (ranging from 0–12%), along with a high rate of complete obliteration (up to 100%), suggesting that surgical resection of these lesions is warranted, especially when performed in experienced centers.
Oral Boards Review—Complications Pearls
1. Bleeding is the most immediate complication of surgery and risks are magnified in smaller children, who have little reserve. The loss of 1/4 of blood volume can induce shock and there may be rapid decompensation in children, which mandates careful monitoring and replacement of blood products by the operative team. 2. Normal perfusion pressure breakthrough is a phenomenon that is thought to occur after resection of high-flow AVMs in which the blood previously transmitted through the AVM is redirected to smaller, normal vasculature after the AVM has been removed, with subsequent inability of the vessels to handle the increased flow.This can result in brain swelling, increased intracranial pressure, seizure, neurologic dysfunction, or hemorrhage. The problem may be minimized by staged preoperative embolization and rigorous blood pressure control postoperatively.
147
8 4 1
Pediatric Neurosurgery
Evidence and Outcomes
Outcome after surgery • In pediatric patients with grade I–III Spetzler-Martin AVMs treated by resection, good recovery was achieved in 90% and deaths occurred at a rate of 5%. Radiographic obliteration rates were 89%. • Although class I or II data is lacking, the combined class III data strongly supports resection as a primary treatment for patients with Spetzler-Martin grade 1 or 2 AVMs. The relatively low postoperative morbidity in these lesions (ranging from 0–12%), along with a high rate of complete obliteration (up to 100%) suggests that delayed control, inherent to radiosurgery, might not be warranted. Outcome after multimodal therapies: • Multimodality therapy of AVMs has been advocated by several investigators. Neurointerventionalists,radiationoncologists,andneurosurgeonswork together to determine the best strategy for a particular patient. Using a multimodality approach, angiographic obliteration rates of > 90% have been reported. • The efficacy of multimodality treatment of large, complex lesions is supported by findings from a group of 53 children at 3-year follow-up in whom a 58% cure rate was noted for AVMs greater than 6 cm in diameter. • In summary, the high likelihood of obliteration, coupled with low complication rates, make a convincing argument in favor of multimodality treatment of pediatric AVMs. Although no class I or II data directly support this recommendation, the class III data are compelling and there is wisdom in pooling the skills of the concerned specialists. References and Further Reading
Spetzler, R. F. & Martin, N. A. A proposed grading system for arteriovenous malformations. J Neurosurg 65, 476–483 (1986). Gross, B. A., Storey, A., Orbach, D. B., Scott, R. M. & Smith, E. R. Microsurgical treatment of arteriovenous malformations in pediatric patients: the Boston Children’s Hospital experience. J Neurosurg Pediatr 15, 71–77, doi:10.3171/2014.9.PEDS146 (2015). Ellis, M. J. et al. Angioarchitectural features associated with hemorrhagic presentation in pediatric cerebral arteriovenous malformations. J Neurointerv Surg 5, 191–195, doi:10.1136/ neurintsurg-2011-010198 (2013). Rangel-Castilla, L. et al. Molecular and cellular biology of cerebral arteriovenous malformations: a reviewofcurrentconceptsandfuturetrendsintreatment.NeurosurgFocus37,E1,doi:10.3171/ 2014.7.FOCUS14214 (2014). Nair, A. P. et al. Clinical, radiological profile and outcome in pediatric Spetzler-Martin grades I-III arteriovenous malformations. Childs Nerv Syst 28, 593–598, doi:10.1007/s00381-011- 1668-6 (2012).
148
Moyamoya Disease Edward Smith
17
Case Presentation
An 8-year-old child of Asian ancestry presents with a 6 month history of increasingly frequent headaches and spells of transient weakness of the right face, arm, and leg.These spells are worse after exertion and particularly after swimming or running around outside when it is hot. Speech arrest then occurred, with an expressive aphasia. This new finding prompted imaging (Figure 17.1). Questions
1. What is the likely diagnosis? 2. What imaging studies are helpful in this scenario? 3. What are some initial management strategies?
Assessment and Planning
This child presented with symptoms suggestive of intermittent interruptions of blood supply to the left frontal lobe.The diagnosis of ischemia is substantiated by MRI showing slow flow (the so-called “ivy sign” on axial FLAIR imaging) as well as old watershed infarctions. A digital subtraction angiogram (DSA) anterior-posterior (AP) view of the left internal carotid artery (ICA) injection reveals marked tapering of the ICA as it enters the brain, coupled with collateral formation in the region of the basal ganglia. Together, this clinical history and radiographic data supports the diagnosis of transient ischemic attacks (TIA) secondary to moyamoya syndrome. The diagnosis of moyamoya is defined by 3 angiographic criteria, based on the Japanese Ministry of Health and Welfare guidelines. First, there must be stenosis of the distal (intracranial) ICAs, up to and including the bifurcation, along with segments of the proximal ACA and MCA. Second, dilated basal collateral vessels must be present (to varying degrees, depending on stage). Third, the findings must be bilateral. However, there are many situations in which the diagnosis of moyamoya is very likely, yet these strict criteria are not fully met. Once the diagnosis of moyamoya is suspected, a series of evaluations should be undertaken. Computerized tomography (CT), sometimes with dedicated arterial imaging (CTA) may be performed as an initial study in an emergent setting for patients who present with acute neurologic deficits or headache suggestive of intracranial
149
0 5 1
Pediatric Neurosurgery
Figure 17.1. Left two images are axial FLAIR MRI studies showing slow blood flow (as evidenced by “ivy sign”—bright sulcal signal, white arrows) and watershed infarction between the ACA and MCA territories (red arrow). The right image is an anterior-posterior (A-P) view of a DSA injection of the left internal carotid artery, demonstrating marked attenuation of the apex of the ICA, with prominent collateral vessels in the region of the basal ganglia (white arrow). hemorrhage, although MRI is rapidly supplanting CT as the first-line study for suspected brain ischemia. Most moyamoya patients will undergo magnetic resonance imaging with magnetic resonance angiography (MRI/MRA). The MRA can reveal affected arterial branches, along with the severity of stenosis. Axial MRI is useful for identifying strokes (acute ischemia is best seen on diffusion weighted imaging—DWI—and chronic ischemia is best seen on FLAIR or T2 weighted imaging). Digital subtraction catheter-based angiography (DSA) is the original standard used todiagnosemoyamoya.Studiesshouldincludeall6cranialvessels(bothinternalcarotids, externalcarotidsandvertebrals).TheseverityofarteriopathyisassessedusingtheSuzuki grade, a staging system from I to VI. Important features to note include the presence of any spontaneous transdural collateral vessels, particularly those arising from vessels contained within the surgical field such as the superficial temporal artery (STA) and the middle meningeal artery (MMA). DSA is also useful in order to identify the course of any potential surgically placed, direct or indirect, collaterals. Other functional diagnostic tests (such as single photon emission CT—SPECT— with acetazolamide challenge) are used to varying degrees depending on institutional preference and practice. It may also be helpful to consider a number of laboratory studies, such as genetic tests (RNF213 in patients of Asian ancestry) and tests of inflammatory markers (for patients with a differential diagnosis inclusive of vasculitis).
Oral Boards Review—Diagnostic Pearls
1. Ischemic stroke in children has a broad differential, but several clinical findings may point to moyamoya. These include a chronic history (months to years) of TIAs, evidence of ischemia with dehydration or hyperventilation (crying, sports related activity, fever) or links to known at-risk populations
150
Moyamoya Disease
associated with moyamoya (East Asian ancestry, sickle cell disease, Down syndrome, neurofibromatosis type I). 2. Recently, several genetic mutations have been linked to moyamoya, including RNF 213 (common in patients with Asian ancestry), ACTA2 (associated with a characteristic angiographic appearance typified by patulous proximal ICAs and radial, narrow, and straight intracranial vasculature) and GUCY (often found in conjunction with esophageal or intestinal motility problems). 3. More detailed assessment with DSA should look at disease severity (with Suzuki stage) and careful investigation for spontaneous transdural collateral vessels from branches of the ECA, as this can affect surgical planning.
Decision Making
Initial therapeutic maneuvers are dependent on the presentation of the child. For a healthy child or for a child who presents with chronic symptoms (seizure, rare TIA, or headache), there are often no immediate interventions necessary, with the exception of typically starting children on low-dose aspirin (81 mg for most children, but lower in infants if they weigh 20 kg or less). Patients with acute symptoms should be assessed with MRI to look for a new stroke. The management of large, hemispheric infarction is beyond the scope of this chapter, but smaller, non-life threatening infarctions are often initially treated in the hospital (for blood pressure management, intravenous fluids and—if needed—seizure control), then followed at home with physical or occupational therapy if warranted. Indications for surgery include children with radiographic evidence of moyamoya, including ongoing ischemic symptoms and/or evidence of compromised blood flow or cerebralperfusionreserve,barringothermedicalcontraindicationstosurgery.Specifically, children who are clinically asymptomatic but who demonstrate radiographic or functional evidence of impaired cerebral perfusion in the setting of moyamoya arteriopathy should be considered as surgical candidates. In general, if the diagnosis of moyamoya is unclear—or asymptomatic with no evidence of impaired flow (such as Suzuki stage 1)—it may be appropriate to adopt a policy of careful monitoring without operation. No recommendations can be made on specific timing for surgery, although the general principle of minimizing the time between diagnosis and revascularization is supported.Delaysmaybereasonable—orrequired—toallowschedulingofexperienced anesthetic and ICU staff to maximize the safety of the procedure. There may also be medicalcontraindicationstosurgerythatmandatedelayspriortorevascularization(such as recent infarction, infection, or hemorrhage). Questions
1. What are the risk factors that predict a higher likelihood of contralateral progression in cases of unilateral moyamoya? 2. What are some measures that can be employed perioperatively to reduce the risk of stroke?
151
2 5 1
Pediatric Neurosurgery
Surgical Procedure
The goal of surgery is to establish a new vascular supply to the areas of brain at risk of stroke, typically by utilizing vessels from the external carotid circulation. Approaches can generally be categorized into 2 groups; direct bypasses (in which a vessel from the external circulation is divided and the open end is anastomosed into a recipient cortical artery) or indirect bypasses (in which vascularized tissue—an artery, muscle, dura, and so forth—is put into contact with the cortex and a new vascular network is then established by ingrowth of vessels from the donor tissue over time). Direct and indirect approaches each have distinct advantages and disadvantages. Direct bypass: • Pro—Immediate perfusion • Con—Technically challenging (may have small vessel size in children and proximal stenoses may limit distribution of the donor vessel) • Con—Requires clamping time which can cause focal ischemia Indirect bypass: • Con—Delayed perfusion • Pro—Simpler surgery which is not limited by vessel size and any proximal stenoses are not an issue, as the graft can span multiple areas • Pro—No clamping time • Pro—Potentially broader area of revascularization The surgical technique of encephaloduroarteriosynangiosis (EDAS) is unique in its focus on creating a direct connection between the recipient brain and donor tissue.This principle is best exemplified by the most common subtype of EDAS used in the United States for children, pial synagiosis. In this procedure, an indirect anastamosis of the parietal branch of the superficial temporal artery is made to the cerebral cortex. It differs from other EDAS procedures by the use of pial sutures and the aggressive approach of a wide arachnoidal opening. The principle of the pial sutures rests on the concept that the normal pulsatile nature of the brain and donor vessel might inhibit growth of new vasculature, but suturing them together reduces relative motion and facilitates better growth. The wide arachnoidal opening is perhaps the biologically most important aspect of the surgery, as recent data has revealed the significant role of angiogenic growth factors in the spinal fluid and embedded in the extracellular matrix of the pia as contributors to new vessel growth. Opening the arachnoid offers the double benefit of removing a mechanicalbarriertoingrowthwhilealsofacilitatingimprovedcontactbetweennascent vasculature and growth factors. The technical aspects of the surgery include several unique steps. Preoperatively, the patient is admitted the day before surgery for overnight intravenous hydration and aspirin therapy is continued right up to—and including—the day before surgery. On the day of surgery, intraoperative electroencephalographic (EEG) monitoring may be used to help identify real-time changes in cerebral blood flow, as indicated by EEG slowing, allowing anesthesia to adjust blood pressure, CO2 levels and medications.
152
Moyamoya Disease
Figure 17.2. Left image reveals dissection of the parietal branch of the STA, overlying the temporalis muscle, with a cuff of tissue around the artery to aid in synangiosis. The right image shows the cortical surface, with the arachnoid widely opened and the placement of a 10–0 nylon suture to affix the donor vessel to the pia.
Positioning is important, keeping the neck as neutral as possible with the use of a shoulder roll and bed turning, in order to prevent kinking of vessels in the neck and concomitant reductions in cerebral blood flow. Keeping the STA course flat relative to the floor and seating on opposite sides of the vessel with the microscope will aid an easy dissection for both the surgeon and assistant. Before the incision is made, the course of the STA may be identified non- invasively using a small“pencil”Doppler ultrasound probe. Scalp injection with local anesthetic and epinephrine should not be used, to avoid injury to or vasospasm of the intended bypass vessel. During the initial dissection of the STA, the risk of vessel injury can be minimized by exposing the vessel in small segments (Figure 17.2). Arachnoidal opening is critical and spending time to widely open as much area as possible is important. Use of an arachnoid knife, linear openings along cortical vessels and sharp dissection with microscissors are helpful techniques. At closure, the risk of cerebrospinal fluid (CSF) leak can occur if there is inadequate galeal closure. Careful inspection of the incision prior to skin suture placement can reveal areas that may need additional sutures. Patient Position with Skin Incision and Key Surgical Steps
• The patient is placed supine in the Mayfield head holder or on a headrest with a roll placed under the ipsilateral shoulder. The head is turned to the contralateral side. • The STA is marked by Doppler ultrasonography, and a linear incision is made over it. The artery is skeletonized with perivascular tissue using the microscope. • The temporalis muscle is incised in a cruciate fashion and the craniotomy performed based on burr holes placed at either end of the arterial segment. The dura is incised along the artery and in flaps so as to allow retraction of the dura. • The arachnoid is incised widely under the microscope. The superficial temporal artery is then placed on the pial surface and sutured to the pia using 10–0 monofilament sutures (Figure 17.2).
153
4 5 1
Pediatric Neurosurgery
• Several sutures are placed to encourage tight approximation of the artery to the brain surface. • When replacing the bone flap, care must be taken to prevent stretching the artery. The artery must enter and exit the burr holes in a gentle curve without tension. • The temporalis muscle is loosely approximated so as not to kink or occlude the artery.The galea and skin are closed in the standard fashion, taking care not to injure the artery.
Oral Boards Review—Management Pearls
1. Avoidance of hyperventilation (in contrast to its use in many other types of craniotomies) is critical to minimize vasoconstriction. 2. Perioperative blood pressure control—specifically avoiding hypotension—is key to minimizing stroke risk. 3. Indirect bypasses can sometimes be combined with direct procedures (although committing donor vessels to direct bypass necessarily limits distal revascularization).
Pivot Points
1. There are general problems that can occur at any time during a moyamoya procedure. a. EEG slowing can herald reduced cerebral blood flow (possibly from spasm or blood pressure changes) and bolus administration of propofol may serve to reduce metabolic demand of the brain and thereby provide a neuroprotective effect. b. Bleeding is particularly troublesome and may be more pronounced if aspirin is used. Meticulous hemostasis is crucial, although“over-cautery”will only serve to deprive the brain from potential additional sources of blood supply. c. Brain swelling (unrelated to direct bypass) can create a cycle of reduced venous outflow—feeding more swelling. Elevation of the head of the bed, opening of arachnoid to drain CSF and increased sedation are all tools to help. Hyperventilation and driving down pCO2 should be avoided in moyamoya patients, as this may precipitate vasoconstriction and stroke in a brain with a tenuous blood supply. d. Significant areas of ischemia toward the frontal and/or occipital poles of the hemisphere can be mitigated by creating additional isolated burr holes, with dural and arachnoid opening, in these areas, which encourage spontaneous ingrowth of collaterals from unnamed scalp and dural vessels. 2. A child presenting with isolated or nearly isolated, unilateral, moyamoya-like disease should be treated with unilateral surgical revascularization and carefully watched for the occurrence of contralateral disease.
154
Moyamoya Disease
Aftercare
Immediate postoperative care should be administered in the intensive care unit, with the goals of avoiding hypotension and hypocarbia. Generally patients are extubated, awake and have an arterial line (for blood pressure management) and a bladder catheter (for monitoring volume status). Antibiotics are used for 24 hours. Aspirin is administered on the day immediately after surgery. Antiepileptics are not routinely prescribed. Intravenous fluids are run at 1–1.5 times maintenance and slowly decreased as the ability to take oral fluids recovers. Pain control is important and frequent neurological examination is critical to detect any changes in exam. The patient is encouraged to ambulate as soon as possible and children are managed to minimize pain and anxiety (as crying can cause vasoconstriction and potentially increase the risk of stroke). Frequency of office visits: • Postoperative care will frequently consist of an office visit approximately 1 month postoperatively, then annually thereafter. Frequency of imaging: • A MRI/A at 6 months may be helpful as a baseline study, to then be compared to subsequent annual MRI/A. The duration of repeated imaging varies by institution, but a common practice is to perform a MRI annually for 5 years, if feasible. • An angiogram (DSA) is often performed at 1 year postoperatively to confirm Matsushima grade of the vascular bypass. Complications and Management
The major risk of this surgery is perioperative stroke. The overall perioperative stroke rate is reported at about 4.5% per hemisphere (during the operation and subsequent 30 days postoperatively). This rate varies in different populations, with higher risk associated with younger age (under 3 years of age), syndromic cases (Down syndrome and sickle cell disease in particular), and history of recent stroke (within 1 month prior to surgery). Another known risk factor for perioperative stroke is the presence of transdural collateral vessels. It is particularly important to consider a full, 5-vessel catheter angiogram to fully detail the extracranial circulation. This allows identification of any pre-existing, spontaneoustransduralcollateralvesselsthatmaybesupplyingthecortex—andthereby reduce the risk of inadvertently interrupting these vessels during surgery. This is particularly important in children who have already undergone any cranial operations (for ventricular shunt placement, tumor removal, etc.).
155
6 5 1
Pediatric Neurosurgery
Oral Boards Review—Complications Pearls
Steps to mitigate the risk of peri-operative stroke include: 1. Preoperative hydration (admitting patients 1 day before surgery for intravenous fluids) 2. Ongoing use of aspirin, including the day before and the day after surgery 3. Good pain control to minimize crying/hyperventilation (in order to avoid hypocarbic-related vasoconstriction)
Evidence and Outcomes
Independentofcause,evidencesuggeststhatchildrenwithmoyamoyaareatriskforischemic damagefromprogressivearteriopathy.Theconditionworsensinnearlyallindividuals,and morethan2/3ofpatientswillhaveclearsymptomaticprogressionwithin5 years,resulting in permanent neurological deficits or death without treatment. Recent reports also supportthestanceoftreatingasymptomaticpatientswithadvancedradiographicdisease,asup to 50% of patients will experience a stroke within 5 years of diagnosis. Data indicate that a patient’s neurological status at the time of treatment is the most important predictor of long-term outcome.The inconsistent results of attempted medical therapy do not match themarkedsuccessofsurgicaltreatment,whichreducessymptomaticprogressionfrom> 66% down to < 4% over a 5-year window. These data, incorporated into the American HeartAssociationGuidelinesandanevidence-basedreviewofmoyamoyaliterature,support the use of surgical revascularization in children with moyamoya. Unilateral disease will progress to involve the contralateral hemisphere in about 1/3 of children within 5 years. Children can also develop arteriopathy of the posterior circulationand—takentogether—thesefindingssupporttheneedforlong-termmonitoring to provide the best possible outcome for children with moyamoya. Overall, the data stronglysupportstheuseofsurgicalrevascularizationasadurable,effectivetreatmentto improve the long-term outcome by reducing stroke risk in children with moyamoya. References and Further Reading
Suzuki J.T. A. Cerebrovascular“moyamoya”disease: Disease showing abnormal net-like vessels in base of brain. Arch Neurol 20, 288–299 (1969). Fukui, M. Guidelines for the diagnosis and treatment of spontaneous occlusion of the circle of Willis (‘moyamoya’ disease). Research Committee on Spontaneous Occlusion of the Circle of Willis (Moyamoya Disease) of the Ministry of Health and Welfare, Japan. Clin Neurol Neurosurg 99 Suppl 2, S238–240 (1997). Scott, R. M. & Smith, E. R. Moyamoya disease and moyamoya syndrome. N Engl J Med 360, 1226–1237, doi:10.1056/NEJMra0804622 (2009). Roach, E. S. et al. Management of stroke in infants and children: a scientific statement from a Special Writing Group of the American Heart Association Stroke Council and the Council onCardiovascular Diseasein theYoung.Stroke;ajournalofcerebralcirculation39, 2644–2 691, doi:10.1161/STROKEAHA.108.189696 (2008). Lin, N. et al. Discovery of asymptomatic moyamoya arteriopathy in pediatric syndromic populations: radiographic and clinical progression. Neurosurg Focus 31, E6, doi:10.3171/ 2011.10.FOCUS11228 (2011). 156
Vein of Galen Malformation Lissa C. Baird
18
Case Presentation
A preterm twin boy is born at 36 weeks gestation due to maternal preterm labor. He carries an antenatal diagnosis of vein of Galen malformation (VOGM). The infant transitions well to the neonatal intensive care unit without additional respiratory support. Consultations are placed to the pediatric cardiology, neuroendovascular, and pediatric neurosurgery services. A detailed pediatric, cardiac, and neurologic evaluation is undertaken. The infant weighs 2.5 kg and is well-appearing with a good cry. He is in no respiratory distress. The head is normocephalic with a sunken fontanel.There is no evidence of dilated scalp veins. A cranial bruit is auscultated. The eyes are midline and he moves his extremities symmetrically and with good strength. Questions
1. What additional diagnoses are associated with VOGM? 2. Which imaging studies should be obtained? 3. What is the appropriate timing for intervention?
Assessment and Planning
VOGMs consist of multiple arteriovenous fistulas shunting arterial blood into the median prosencephalic vein of Markowski—a persistent embryonic vein—which then develops aneurysmal-like dilation.These malformations can be classified into 2 primary categories: mural type and choroidal type. Mural type malformations consist of high- flow shunts that drain directly into the wall of the dilated vein. Feeding arteries arise from collicular and posterior choroidal arteries. Choroidal types are more complex, with an extensive arterial network between the feeding vessels that drain directly into the venous dilation. Feeding arteries for choroidal-type VGMs may arise from the choroidal, pericallosal, or thalamoperforator arteries. This subtype of VGM associates with more severe clinical presentations. Mixed forms can occur. If the diagnosis of VGM is made in the antenatal period, as in this case, the infant will be taken to the neonatal intensive care unit for a full pediatric, neurologic, and cardiac evaluation. High-volume cardiac failure may be present as early as fetal age, and cardiopulmonary support may be necessary immediately after delivery. Cardiac sequelae from VGM may range from mild volume overload to severe cardiogenic shock. Medical
157
8 5 1
Pediatric Neurosurgery
managementisinitiatedifindicated,andmayincludediuretics,pressors,inotropicagents, and mechanical ventilation. A head ultrasound is obtained to evaluate the size of the ventricles and assess for any undiagnosedparenchymalpathology.Hydrodynamicdisordersmaybepresent at birth, and can manifest anytime between fetal age and treatment of the VGM during infancy. The arteriovenous shunting through the malformation leads to elevated intravenous pressure,impairedcerebrospinalfluidresorption,andelevatedintracranialpressure.This canresultinhydrocephalus,macrocrania,seizures,subduralhematoma,cerebraledema, developmental delay, and neurocognitive deficits. Obstructive hydrocephalus may also be caused by direct mechanical compression on the cerebral aqueduct. Extremely high flow malformations may be associated with severe vascular steal phenomenon due to diversion of the majority of the oxygenated blood. This may lead to ischemic damage and cerebral atrophy. MRI, MRA, and MRV (magnetic resonance imaging, magnetic resonance angiography, and magnetic resonance venography) are obtained for initial non-invasive evaluation of the vascular anatomy. Ventricular size and brain parenchyma are found to be normal (Figure 18.1). The MRA demonstrates a small choroidal component to the VGM. Diagnostic angiography provides greater detail and dynamic information; however, this is not obtained during this early phase and is deferred until the time of planned endovasculartreatment.Itispreferabletodelayendovasculartreatmentuntiltheinfantis 5–6 months of age when possible, and angiography in the neonatal period should only occur when urgent embolization is necessary and being considered in the same setting. If medical management proves insufficient to maintain cardiopulmonary stability, or if mechanical ventilation cannot be weaned, endovascular intervention will need to be performed at an earlier age. Cardiomegaly and hypercontractility on echocardiogram, pulmonary hypertension, and systemic hypertension are all findings that may lead to earlier endovascular intervention.
(A)
(B)
Figure 18.1. Anterior flow voids demonstrate a choroidal component to the vein of Galen malformation.
158
Vein of Galen Malformation
Questions
1. What is the appropriate timing for endovascular intervention in this patient? 2. How might the subtype of VGM impact management of the patient? 3. How is the development of hydrocephalus optimally managed in patients with VGM?
Oral Boards Review—Diagnostic Pearls
1. Mural type VOGMs are characterized by fewer fistulas, are easier to treat, and more commonly present with progressive hydrocephalus. 2. Choroidal type VOGMs have more complex and numerous fistulas with higher flow. They are more difficult to treat and commonly present with severe high-output cardiac failure. 3. Infants with VGM require close monitoring for adequate control of heart failure and for development of hydrocephalus. Urgent endovascular treatment is required should non-surgical measures fail to stabilize cardiac status or should hydrocephalus progress.
Decision Making
The natural history of untreated VOGM is poor, as spontaneous resolution of the arteriovenous shunting rarely occurs. If left untreated, hydrocephalus, cerebral venous hypertension,cerebralcalcifications,seizures,developmentaldelay,anddeathwilloccur.Open surgical treatment has resulted in universally poor outcomes and is not recommended. The development of endovascular embolization techniques has allowed for safer and more effective management of these children, and this has become the gold standard of treatment. Transarterial embolization of the feeding arteries in order to obliterate the arteriovenous shunt is the optimal choice when vascular anatomy allows.Transvenous embolization has limited indications, as this method exposes the patient to an increased risk of intracranialhemorrhage,canacutelyexacerbatethevenoushypertension,andisusually contraindicated in the choroidal subtype of VGM. Stereotactic radiotherapy may be effective for a small residual shunt in an older child, but it is not indicated for primary treatment in infancy. The long-term goal of treatment is complete obliteration of the arteriovenous shunting in order to optimize normal neurodevelopment of the patient. The more immediate goal of treatment is the control of congestive heart failure and hydrocephalus. Appropriatetimingofinterventionisasignificantconsiderationascerebralangiography is easier, safer, and carries less risk to the femoral artery in an older infant. If cardiac failure can be successfully managed with medical treatment, endovascular intervention should be delayed until the infant is 5–6 months old. This child was monitored in an outpatient setting by cardiology and neurosurgery over the first 2 months of life. His cardiac function remained stable. His head
159
0 6 1
Pediatric Neurosurgery
(A)
(B)
Figure 18.2. Progression of hydrocephalus over a 2-month interval. circumference was noted to be crossing percentiles at 4 weeks of age, and ventricular volumes were enlarged. He was clinically well-appearing and asymptomatic at this time, and observation was continued. At 3 months of age, the patient’s hydrocephalus was continuing to progress, and he demonstrated macrocrania, poor feeding, and increased irritability. Recommendation was made to proceed with endovascular embolization at this time (Figure 18.2, Figure 18.3). Questions
1. What are the vascular access options available for transarterial embolization? 2. When would a transvenous approach be indicated for treatment of VGM?
Figure 18.3. The dramatic volume of arteriovenous shunting is demonstrated on a sagittal T2-weighted MR image obtained just prior to endovascular treatment.
160
Vein of Galen Malformation
Surgical Procedure
The infant is placed under general anesthesia and intravenous access is established. He is brought to the angiography suite and a 4F sheath is placed in the femoral artery under ultrasound guidance. If treatment is carried out in the neonatal stage due to medically refractory cardiac failure, access can also be achieved through the umbilical artery. Low-osmolarity nonionic contrast material is injected for pre-therapeutic angiography (Figure 18.4). A flow-guided microcatheter is placed through the 4F sheath. Liquid embolic material is used to target the fistula sites of the malformation. It is important to obliterate the arteriovenous shunting at the fistula site in order to avoid collateralization and recurrence. N-butyl-cyanoacrylate is most commonly used as the embolic glue. Onyx is increasingly used as well. Detachable microcoils may be used, although their application takes a longer amount of time and they are likely to carry an increased risk for vessel rupture. If medical therapy fails to manage cardiac failure, treatment is carried out in the neonatal stage.The goal of embolization in a neonate is to sufficiently reduce the amount of arteriovenous shunting to permit control of congestive heart failure. A limited amount of liquid and contrast material must be used efficiently and multiple sessions may be needed to achieve the treatment goal. Once severe heart failure is resolved, further endovascular treatments may be delayed until 5–6 months of age. Following total or near total occlusion of the fistulas, progressive thrombosis and shrinkage of the dilated and ectatic vein are observed on serial MR imaging. Mural-type lesions may typically be occluded in a single session, while choroidal VGMs may need to be staged. Transvenous approaches, while suboptimal due to the increased risk of intracranial hemorrhageandvenousinfarction,maybeconsideredwhentransarterialembolizations are not feasible due to the vascular anatomy.
(A)
(B)
RT VERT
RT VERT
Figure 18.4. (A) Pre-treatment angiography demonstrating arteriovenous shunting and (B) a dilated median prosencephalic vein of Markowski.
161
2 6 1
Pediatric Neurosurgery
Oral Boards Review—Management Pearls
1. Transfemoral transarterial embolization at the fistula sites of the malformation for complete obliteration of the arteriovenous shunting is the optimal intervention for VGM. 2. An interdisciplinary approach is critical from the time of diagnosis through the post-treatment follow-up and improves prognosis. Management by a high-risk obstetric team and pediatric cardiologist is critical. 3. Early intervention may be necessary if cardiac failure is severe and uncontrolled with medical management. 4. Slowly developing hydrocephalus and macrocephaly may not require urgent intervention as it is likely to stabilize or reverse upon endovascular obliteration of the VGM. Symptomatic or rapidly developing hydrocephalus is indication to expedite endovascular intervention and avoid ventricular shunting. 5. Transvenous approaches are associated with an increased risk of intracranial hemorrhage and venous infarction. They are considered only when transarterial approaches are not anatomically feasible, and the dilated vein is not communicating with normal cerebral venous drainage.
Pivot Points
1. If medical management fails to control high-output cardiac failure, early endovascular intervention is indicated, even in the neonatal stages. The goal of treatment as this age is to reduce the arteriovenous shunting until the heart failure is controlled. 2. Should hydrocephalus progress rapidly or become symptomatic, early endovascular treatment should be considered to avoid ventricular shunting. 3. Should transarterial approaches fail to completely obliterate the arteriovenous shunting, transvenous approaches may be required. Stereotactic radiosurgery may be considered for a small residual fistula in an older child.
Aftercare
Following the endovascular procedure, the infant is monitored closely in the neonatal or pediatricintensivecareunit,withfrequentneurologicassessments.Iffemoralaccess was obtained, the leg is maintained in a neutral position for 6 hours. Lower-extremity pulses are monitored at regular intervals. Routine quick MR imaging or head ultrasound is obtained in the post-operative periodtoassessforanyintracranialcomplication.Emergentimagingshouldbeobtained with any concern for neurologic deterioration. The cardiac status is monitored closely by the intensive care physicians and pediatric cardiology. There is not an indication for routine antibiotics or steroids during the recovery period. Feeding should resume after the procedure has been completed.
162
Vein of Galen Malformation
Complications and Management
Complications related to the treatment ofVGM may include cerebral hemorrhage, cerebral ischemia, catheter perforation, and intractable congestive heart failure due to failed embolization. Intraprocedural arterial perforation or microcatheter rupture can result in intracranial hemorrhage, stroke, and permanent neurologic injury. Immediate embolization should be performed in this setting. Perforation of the venous wall can be managed with reversalofanticoagulationandcompletionofembolization.A hematomacreatingsymptomatic mass effect will require surgical evacuation, and intraventricular hemorrhage may mandate placement of a ventricular drain. Leg ischemia secondary to femoral artery occlusion may occur, especially with repeated femoral artery puncture. Care should be taken with compression and hemostasis following completion of the procedure in order to maintain long-term patency of the vessel. Lower-extremity pulses should be monitored carefully, and any loss of pulses should be emergently reported to the endovascular team. Pulmonary embolization with embolic agents may occur given the high flow arteriovenous shunting across the malformation.This can be managed with anticoagulation and supportive care.
Oral Boards Review—Complications Pearls
1. Treatment related complication rates have dramatically improved with the development of endovascular techniques; however, these remain complicated and challenging lesions. Treatment by an experienced and proficient endovascular team will minimize procedural morbidity. 2. Close monitoring in an intensive care setting is critical. Perfusion of the lower extremity after femoral artery access should be ensured. Frequent neurologic assessments and imaging when indicated will allow for early diagnosis and treatment of complications. 3. Sequelae of cardiac failure and end-organ damage may be minimized with early endovascular intervention when indicated and complete embolization when feasible.
Evidence and Outcomes
VGMs are rare, and no level I evidence is available. Multiple case series have been reported,whichclearlydemonstrateanimprovementinoutcomewithendovascularmanagement. Microsurgical treatment has been associated with mortality rates as high as 100%, and it is no longer indicated for this diagnosis. Mortality rates without treatment range from 95–100%. Reported mortality with endovasculartreatmentishighlyvariable,butoverallrateshavedecreasedfromabout17 to 11% over the past 15 years with improvements in technology and technique. Normal neurologic outcome is achieved in about 75% of children with VGM, with mild delay in about 10%.
163
4 6 1
Pediatric Neurosurgery
References and Further Reading
Vein of Galen malformation. Hoang S, Choudhri O, Edwards M, Guzman R. Neurosurg Focus. 2009 Nov;27(5):E8. Outcome and complications of endovascular embolization for vein of Galen malformations: a systematic review and meta-analysis. Yan J, Wen J, Gopaul R, Zhang C, Xiao S. J Neurosurg. 2015 Oct;123(4):872–890. Presentation, course, and outcome of postneonatal presentations of vein of Galen malformations: a large, single-institution case series. Gopalan V, Rennie A. Robertson F, Kanagarajah L, Toolis C, Bhate S, Ganesan V. Dev Med Child Neurol. 2018 Apr;60(4):424–429. Vein of Galen malformations: epidemiology, clinical presentations, management. Recinos PF, Rahmathulla G, Pearl M, Recinos V, Jallo G, Gailloud P, Ahn E. Neurosurg Clin N Am. 2012 Jan;23(1):165–177. Endovascular treatment of vein of Galen aneurysmal malformations: management strategy and 21-year experience in Toronto. Li A, Armstrong D, terBrugge K. J Neurosurg Pediatr. 2011 Jan;7(1)Z:3–10.
164
Pineal Tumor Tadanori Tomita
19
Case Presentation
A 3-year-10-month-old boy presented with 1 week of on-off headaches that became constant over the preceding 3 days. His parents also reported morning emesis for the past two mornings. He had a computed tomography (CT) scan on the day of transfer, which showed hydrocephalus. On admission, he was awake and playful with normal speech for his age, without macrocephaly. Neurological examination was normal except for early papilledema. Pupils were equal and showed normal light responses with normal ocular movements. He had normal motor strength and cerebellar function. CT showed trilateral hydrocephalus with a small calcification in the pineal region (Figure 19.1). Following admission, MRI without contrast was obtained (Figure 19.2). Sagittal images demonstrated dilatation of the proximal cerebral aqueduct with a smaller, more normal caliber distal aqueduct. There was focal, mild circumferential narrowing of the mid portion of the aqueduct (Figure 19.2, left). MR showed a moderate lateral and third ventricle dilatation with diffuse sulcal effacement (Figure 19.2, center). The fourth ventricle was normal in size. At this level, there was suggestion of a faint curvilinear lesion traversing inferiorly, raising the possibility of a thin congenital web in the aqueduct. There was a 0.3 × 0.4 cm round T2 signal structure in the region of the pineal gland best seen on sagittal 3-D T2-weighted images (Figure 19.2, right), suggestive of a small pineal cyst. Overnight, the patient was noted to have occasional bradycardia with heart rates dropping into the 50s. Questions
1. What is the likely diagnosis? 2. Is the calcification of the pineal gland normal at this age? 3. What is the most appropriate next action? On the following day, the patient underwent an endoscopic third ventriculostomy (ETV). The ventricular CSF was crystal clear but under high pressure. A narrow neuroendoscope within a slotted ventricular catheter was used for the procedure.There are no abnormalities in the anterior third ventricle on endoscopic inspection. Attempt to visualize the posterior third ventricle failed because of the angulation, trajectory and relatively small ventricle size. The floor of the third ventricle was punctured with the tip of NeuroPen endoscope within a slotted catheter (Shen et al., 2018), followed by widening of the ostomy. The ventricular CSF showed glucose 63 mg/ml, protein 6 mg/
165
61
Pediatric Neurosurgery
Figure 19.1. CT imaging shows trilateral hydrocephalus with a small calcification in the pineal region. ml, rbc 10/cu.mm, and wbc < 1/cu.mm. The CSF culture was negative for infection. Cytology of the CSF was not sent. The slotted catheter was left in the lateral ventricle and connected to a subgaleal Ommaya reservoir. Following the ETV, his symptoms were resolved and he was discharged on the following day. He returned for 6-month follow-up with his parents after scheduled MRI. The parents reported that the patient was doing well and had not had any complaint of headaches or emesis since the ETV. He did not have any neurological concerns and his developmental milestones were normal. However, his parents noted over 3 months’time that he developed deeper voice, increasing penile size, pubic hair, body odor, and acne together with a growth spurt. His genitals showed Tanner Stage 2 for pubic hair and testicular volume. His serum testosterone was markedly elevated (953.6 ng/dl) and bone age radiograph showed advancement by 1 year.
Figure 19.2. MRI imaging without contrast shows moderate lateral and third ventricle dilatation with diffuse sulcal effacement and a normal fourth ventricle. Mild periventricular FLAIR hyper-intensity suggests the presence of transependymal CSF flow. Sagittal images demonstrate dilatation of the proximal cerebral aqueduct. T2 weighted images also demonstrate what appears to be a small pineal cyst.
166
Pineal Tumor
Assessment and Planning
Questions
1. What is the likely cause of precocious puberty during young childhood? 2. What is the appropriate diagnostic work-up? MR of the brain with and without contrast showed resolution of his hydrocephalus. There was a multilobulated hyperintense cystic lesion in the posterior third ventricle on non-enhancing T1-weighted MR (Figure 19.3A). Cystic components of the lesion demonstrated intrinsicT1 signal which may represent proteinaceous content.The only enhancing portion was a small solid pineal gland lesion (figure 19.3B).
(A)
(B)
Figure 19.3. MR imaging with and without contrast shows resolution of the presenting hydrocephalus and a multilobulated, T1-hyperintense, cystic lesion in the posterior third ventricle (A). Cystic components of the lesion demonstrated intrinsic T1 signal which may represent proteinaceous content. The only enhancing portion is a small solid pineal gland lesion (B).
167
8 6 1
Pediatric Neurosurgery
Questions
1. What is the likely diagnosis? 2. What is the next step of diagnostic or therapeutic procedure? 3. If biopsy is needed for posterior third ventricle tumor, how do you approach it: neuroendoscopic or stereotaxic? Tumor markers were tested: Beta-HCG was positive: serum 182 IU/L, ventricular CSF from Ommaya tap 70 IU/L and CSF from lumbar puncture 42 IU/L. Alpha fetoprotein was negative in both serum and CSF. Based on positive tumor markers, malignant germ cell tumor was strongly suspected. For that reasons, he was treated with neoadjuvant chemotherapy with Children’s Oncology Group Study ACNS0122. He received 6 cycles of Induction chemotherapy consisting of carboplatin and etoposide (Cycles 1, 3, and 5) alternating with ifosfamide and etoposide (Cycles 2, 4, and 6). Following the chemotherapy, his posterior third ventricle mass was reduced in size by about half (Figure 19.4). Also noted was a normalization of the beta HCG level to less than 0.5. His pubic hair but he continued to have deep voice.
Oral Boards Review—Diagnostic Pearls
1. History and physical examination, neuroimaging, and tumor markers are crucial to the diagnosis of pineal region tumors. 2. In children, germ cell tumors are a more common tumor pathology than pineal parenchymal tumors.
Figure 19.4. Following the chemotherapy, the posterior third ventricle mass is reduced in size by about half.
168
Pineal Tumor
3. Among germ cell tumors, germinoma is the most common histological type followed by teratoma, embryonal carcinoma, yolk sac tumor, and choriocarcinoma. Mixed germ cell tumors are also common. Only mature teratoma is benign histologically. 4. Assay of serum and CSF tumor markers (oncoproteins) needs to be done if one suspects a diagnosis of germ cell tumor, as well as for monitoring response of germ cell tumors to treatment, including beta-HCG (produced by syncytiotrophoblasts and/or choriocarcinoma), AFP (produced by yolk sac endoderm, fetal hepatocytes and embryonic intestinal epithelium and/or yolk sactumor)andplacentalalkalinephosphatase(producedbysyncytiotrophoblasts and/or germinoma). 5. CT often shows a pineal calcification engulfed by the tumor or displaced peripherally by germ cell tumors, while the pineal calcification may be dispersed within tumor.Teratoma may show heterogeneous appearance due to cysts and occasionally fat or bone formation. Choriocarcinoma may show evidence of hemorrhage into the tumor. 6. MRI of germinomas typically appear as a solid, contrast enhancing lesion in the pineal location. They may present bifocal appearance with a concurrent lesion in the anterior third ventricle. Teratomas tend to show heterogeneous contrast enhancement. 7. Hydrocephalus is very common, and may be the primary cause of symptoms. Some patients may present with Parinaud’s syndrome.
Questions
1. What is the most appropriate intervention, (second look) surgical resection or radiation therapy? 2. What craniotomy-based approaches to the pineal region tumors are preferred?
Figure 19.5. Surgical positioning with Mayfield 3-point head fixation and incision planning.
169
0 7 1
Pediatric Neurosurgery
Surgical Procedure
Resection of residual tumor via a right sided occipital transtentorial approach was planned. The patient had a preoperative MRI scan done for surgical planning and neuronavigationalsystemuse.Followingendotrachealintubationandgeneralanesthesia, he was positioned prone with Mayfield three-pin fixation with a torque pressure of 40 pounds and pediatric pins. He was positioned with the neck neutral for a planned midline and right occipital craniotomy. The head was rotated about 10 degrees to the left side, reducing the need for active right occipital lobe retraction and taking advantage of gravity retraction upon entering the occipital interhemispheric fissure. A skin incision was outlined in a hockey stick incision with a midline incision from inion to the 2 cm above the lambda and then the lateral incision extending to the right posterior temporal location with a length of 3–4 cm (Figure 19.5). Once the scalp flap was turned, the right occipital bone, the right lambdoid suture and parts of posterior sagittal and left lambdoid sutures were included in the surgical view. A burr hole was made 2 cm away from lambda directly over the sagittal suture with meticulous care not causing any trauma to the subjacent superior sagittal sinus. Another burr hole was made above the torcular herophili, as located using the neuronavigational system. A 5 cm wide and 8 cm long craniotomy flap was created using the craniotome, crossing the midline exposing the full width of the superior sagittal sinus within the surgical field. (A)
(C)
(B) (D)
Figure 19.6. Operative photographs. (A) The straight sinus and the tentorium are identified at the depth of the interhemispheric fissure along the falx cerebri. (B) The tentorial edge is sectioned parallel and slightly lateral to the straight sinus. (C) Thick arachnoid over the quadrigeminal cistern is opened, exposing the tectum, vein of Galen and tumor. (D) After tumor removal, the column of fornices and foramen of Monro are visible in the anterior third ventricle.
170
Pineal Tumor
Dural opening was done in C-shape and turned medially over the sagittal sinus. The interhemispheric fissure was entered while protecting the occipital lobe with a wet cottonoid patty.The last most posterior bridging vein is usually present 1–2 cm rostral to the lambda.While advancing deeper into the interhemispheric fissure, CSF was drained from his pre-existing Ommaya reservoir to attain brain relaxation. Oneshouldrememberbrainrelaxationistheessentialforinterhemisphericapproach. If no ventricular access device is available and the brain seems to be tight, one can perform intraoperative ventriculostomy and/or use intravenous Mannitol. Caution should be taken to avoid traumatizing displaced brain against the cut dural edge. A sufficiently large craniotomy and dural opening are needed unless brain relaxation is adequate. Use of a surgical microscope is essential for tumor resection. At the depth of the interhemispheric fissure along the falx cerebri, the straight sinus and the tentorium were identified (Figure 19.6A). The tentorial edge was identified and tentorial section was performed parallel and slightly lateral to the course of the straight sinus (Figure 19.6B). The length of the tentorial section used depends on the individual anatomy in each procedure, but is usually 2.5 cm. Thick arachnoid over the quadrigenminal cistern was opened, exposing the tectum, vein of Galen and the tumor (Figure 19.6C). The vein of Galenwasseparatedfromthedomeofthetumorandprotectedwithcottonoidpledgets. The precentral vein was pushed posteriorly, and usually does not need to be sacrificed. As in this case, germ cell tumors are usually firm and rubbery, and well demarcated from the surrounding neural structures.This contrasts with pineoblastoma which is more vascular and soft and suckable.When a tumor is large, it is first debulked internally and then the tumor capsule is separated away from the surrounding midbrain and posterior thalamus. Care must also be taken to avoid injury to the deep venous structures surrounding the pineal region, which can be difficult to control at depth. Additionally, sacrifice of these veins may lead to relatively morbid venous infarcts in deep eloquent structures including the midbrain and thalamus. Once the third ventricle was entered, the anterior third ventrice was protected by cottonoid pledgets. Once the tumor was removed,
Figure 19.7. Post-operative MR imaging showing a gross total resection.
171
2 7 1
Pediatric Neurosurgery
the column of fornices and foramen of Monro were visible at the anterior end of the third ventricle (Figure 19.6D).The microscope projection angle was frequently changed during the tumor resection in order to accommodate the trajectory to the pineal and third ventricle regions, as well as confirming anatomical relationships with the frameless navigation system. Following tumor resection and confirmation of hemostasis, the dura was closed in a water tight fashion with suture. At the edge of craniotomy site, multiple dural tuck-up sutures were applied to prevent postoperative epidural hematoma. The bone flap was replaced and titanium plates and screws were used to secure the flap.The scalp was closed in layers in standard fashion.
Pivot Points
Pediatric neurosurgeons prefer to access pineal region tumors via two common approaches: occipitaltranstentorialversusinfratentorialsupracerebellar.Each has pros and cons, and the decision is made by the neurosurgeon depending on his or her experience and comfort. 1. The occipital transtentorial approach provides a comfortable position for the surgeon and assistant, with their heads looking down on the surgical field as the patient is in a prone position. For the infratentorial supracerebellar approach, the patient in most cases is in a sitting position, in which extra care should be applied to prevent air embolism. When a patient with hydrocephalus is placed in a sitting position, a sudden loss of the CSF from hydrocephalus may cause pneumocephalus or subdural hematoma. The benefits of the occipital transtentorial approach include gaining a wide range of sagittal trajectory angles by sectioning the tentorium and changing the angle of the microscope from the precentral sulcus to anterior third ventricle and from the roof to the floor of the third ventricle. Also, the occipital approach usually carries lower risk of damage to deep venous structures. Early visualization of the vein of Galen provides protection as the tumor capsule is separated away from it. When the ventricle is enlarged, brain relaxation is attained by using a ventriculostomy. However, in the case of a slit-like ventricle, going through the interhemispheric fissure may be difficult but can be aided using hyperosmotic agents and/or a lumbar drain. One should avoid forcible retraction of the occipital lobe, which results in postoperative hemianopsia. Also the visualization of contralateral side of the tumor occurs towards the end of resection. 2. The benefit of the infratentorial supracerebellar approach is that little brain retraction is needed when the ventricles are small (e.g., slit ventricle after shunt), and one can stay on the midline while approaching midline structures and tumor. A disadvantage is sacrificing the superior vermian and precentral veins, which may result in venous infarct of the cerebellum, as well as difficulty visualizing and accessing the precentral region. The portion of tumor extending laterally above and beyond the tentorial opening is hard to reach.
172
Pineal Tumor
Aftercare
Pathological evaluation of the tumor identified a mature cystic teratoma with ectodermal (skin and adnexal structures), endodermal (respiratory and interstinal) and mesodermal (skeletal muscle) elements with glial tissue, fibrosis and numerous aggregates of hemosiderin laden macrophages. No germ cell component was identified (C-Kit immunostaining was negative). Postoperative MR imaging showed gross total resection (Figure 19.7). Immediate postoperative emesisresolvedbythenextmorning.Hewasalertandhadnormalspeech, without signs of visual field, motor or sensory deficits. However, he had a restriction of up gaze in both eyes with convergence retraction on attempted upgaze. Both pupils were equal at 4 mm in size with brisk but limited reaction to light (3 mm). The patient was discharged 3 days postoperatively. On examination a month after he was discharged, the patient had a normal neurological examination but his voice remained deep. His upward gaze improved with minimum restriction and his pupillary size and light reactions were normal. He received proton radiation therapy to the whole ventricle of 30.67CGE with a pineal boost of 23.50CGE, for a total of 54.17CGE. The Ommaya reservoir was tapped periodically to obtain samples for CSF cytology and tumor marker analysis, which both remained negative. Presently, 5 years after diagnosis, he does not have any abnormalities of developmental or neurological function. Upward gaze has normalized. His serum and CSF tumor markers remain negative. Serial MR surveillance imaging has showed no tumor recurrence. However, he did have acceleration in bone age as a result of his original elevated testosterone levels, with a bone age of 12 years at a chronological age of 8 years and 6 months.
Oral Boards Review—Complications Pearls
1. Some patients may develop delayed hemorrhage from a pineal tumor following ETV and endoscopic tumor biopsy. 2. For an occipital interhemispheric, transtentorial approach, good brain relaxation should be obtained and the craniotomy and dural opening should be sufficiently large to prevent incarceration of herniated brain through the durotomy. 3. During an infratentorial, supracerebellar approach with the patient in a sitting position, surgical preparation should include a precordial doppler and central venous catheter for detection and treatment of air embolism. 4. If the intraoperative frozen section shows pure germinoma, aggressive resection is not necessary. However, teratomas require radical resection. Teratomas are generally firm, rubbery, and often large but well encapsulated. Internal decompression followed by separation of the capsule from surrounding neural structures generally allows safe resection. 5. When hemorrhage occurs from the vein of Galen, hemostasis is often attained by placing a gelform pledget and cottonoid on the bleeding point; coagulation can worsen the venous injury.
173
4 7 1
Pediatric Neurosurgery
Oral Boards Review—Management Pearls
1. Hydrocephalus due to pineal tumor is effectively managed by ETV. 2. If tumor markers are negative, a histological biopsy is carried out. Endoscopic biopsy is less invasive. If ETV and endoscopic biopsy are done under same anesthesia, the ETV is done first because the biopsy may cause hemorrhage in the ventricle, thus hindering subsequent ETV due to hemorrhagic CSF. Following ETV, leaving a ventricular catheter and subgaleal ventricular access device is useful, not only for ICP evaluation/management but also as ready access to the CSF sampling for CSF cytology and tumor markers. 3. For endoscopic biopsy, a single rigid endoscope can gain access to the pineal region tumor with advanced hydrocephalus. When hydrocephalus is minor, one may use a flexible scope through the same entry for ETV. Otherwise, a separate burr hole placed more anteriorly than that used for ETV provides a better trajectory for tumor biopsy. 4. When tumor markers are positive, neoadjuvant chemotherapy is recommended to shrink the tumor, which often resolves hydrocephalus. Following chemotherapy, if residual tumor is present, a surgical resection (second-look surgery) is recommended. When the tumor is a teratoma or tumor histology is not verified, surgical resection is mandatory. 5. For pineal region tumors, valid histological confirmation either by biopsy or tumor markers are needed to choose the appropriate therapeutic modalities. 6. Terataoma and residual tumor after chemotherapy (often teratoma) need to be resected. Gross total resection should be the goal of surgery. 7. Pure germinomas respond extremely well to radiation therapy or chemotherapy. 8. For non-germinomatous malignant germ cell tumors including germinoma, radiation therapy is needed in follow-up to initial chemotherapy and second- look surgery.
References and Further Reading
Zimmerman RA, Bilaniuk LT: Age-related incidence of pineal calcification detected by computed tomography. Radiology 142:659–662, 1982. Kulkarni AV, Riva-Cambrin J, Holubkov R, Browd SR, Cochrane DD, Drake JM, Limbrick DD, Rozzelle CJ, Simon TD, Tamber MS, Wellons JC 3rd, Whitehead WE, Kestle JR, Hydrocephalus Clinical Research Network: Endoscopic third ventriculostomy in children: prospective, multicenter results from the Hydrocephalus Clinical Research Network. J Neurosurg Pediatr 18(4):423–429, 2016. Shen W-J, Syed HR, Gandhoke G, Garcia R, Pundy T, Tomita T: Endoscopic third ventriculostomy in children with a fiber optic neuroendoscopy. Childs Nerv Syst 34:837–844, 2018. Navarro R, Gil- Parra R, Reitman AJ, Olavarria G, Grant JA, Tomita T: Endoscopic third ventriculostomy: early and late complications and their avoidance. Childs Nerv Syst 22:506–513, 2005.
174
Pineal Tumor
Tomita T: Pineal Region Tumors. Principles and Practice of Pediatric Neurosurgery, 3rd ed, Albright AL, Pollack IF, Adelson PD. (eds.). New York: Thieme. 2015; pp. 509–526. Hankinson EV, Lyons CJ, Hukin J, Cochrane DD: Ophthalmological outcomes of patients treated for pineal region tumors. J Neurosurg Pediatr 17(5):558–563, 2016. Goldman S, Bouffet E, Fisher PG, Allen JC, Robertson PL, Chuba PJ, Donahue B, Kretschmar CS, Zhou T, Buxton AB, Pollack IF: Phase II trial assessing the ability of neoadjuvant chemotherapy with or without second-look surgery to eliminate measurable disease for nongerminomatous germ cell tumors: a Children’s Oncology Group study. J Clin Oncol 33(22):2464–2471, 2015.
175
6 7 1
Medulloblastoma Amy K. Bruzek, Shawn L. Hervey-Jumper, and Karin M. Muraszko
20
Case Presentation
A previously healthy 6- year- old male who had been born full- term without complications presented to the emergency department with a 2-week history of lethargy, mild frontal headaches, intermittent vomiting, and blurred vision. He had become increasingly clumsy and uncoordinated. On physical examination he had bilateral papilledema and a slightly unsteady, wide-based gait.The remainder of his examination was normal. Neurosurgery was consulted. Questions
1. What is the differential diagnosis? 2. What initial work-up should be done? 3. What is the most common presentation associated with a lesion in this location? 4. What are common characteristics of the classical form of this diagnosis?
Assessment and Planning
Thedifferentialdiagnosisincludedinfectiousetiology,tumor,hemorrhage,andvascular malformation. Brain MRI, with and without contrast, was ordered, which demonstrated a posterior fossa mass (Figure 20.1). The differential diagnosis was then narrowed to a tumor. Tumors of the fourth ventricle in this age group include medulloblastoma (MB), atypical teratoid/rhabdoid tumor (AT/RT), ependymoma, choroid plexus papilloma, low-or high-grade astrocytoma, Lhermitte-Duclos disease, dermoid or, rarely, other entities. The most common brain tumor in children is astrocytoma, followed by MB, then ependymoma. However, in the posterior fossa, MB is the most common tumor, and MB is the second most common cancer in children. Although most are diagnosed before 10 years of age, MB may present in young adolescents and rarely in adults. MB makes up about 20% of all CNS tumors in children and 40% of posterior fossa tumors. The incidence of MB is 0.48 to 0.75 per 100,000 person-years, with the peak between ages 5 and 7 years. There is a bimodal age distribution with another small peak in MB diagnosis between the ages of 20 and 40 years, with incidence of 0.17 per 100,000 person- years. Ependymoma usually occurs in children prior to the age of 5 years, and AT/RT
177
8 7 1
Pediatric Neurosurgery
Figure 20.1. Preoperative brain MRIs. (A) T1-weighted sagittal MRI showing the fourth ventricular mass compressing brainstem anteriorly. (B) Contrast-enhanced T1- weighted axial MRI demonstrating midline location. (C) T2-weighted FLAIR axial MRI. (D) Diffusion-weighted image.
most often occurs in infants. Dermoid and epidermoid tumors are even rarer. Gliomas, especially low-and high-grade astrocytoma, are also in the differential, with pilocytic astrocytoma being most common in the cerebellum. In patients who have received radiation for MB, recurrent MB as well as secondary malignancies such as glioma and meningioma should be considered.
Oral Boards Review—Diagnostic Pearls
1. Presenting symptoms are the key to making an early, quick diagnosis with subsequent referral to neurosurgery. a. Headaches, nausea, vomiting, and visual complaints indicate possible obstructive hydrocephalus.
178
Medulloblastoma
b. Cranial nerve VI or IV deficits are common, which may manifest as double-vision. c. Ataxia and nystagmus further localize the lesion to the posterior fossa. 2. Dermoid tumors may present with fever or signs of infection and meningitis; such presentation warrants meticulous search for a dermal sinus tract. 3. Although head CT is often done initially given concern for hydrocephalus, MRI should be performed quickly, as an aid to diagnosis and treatment planning. 4. Preoperative relief of hydrocephalus by external ventricular drain (EVD) may be needed for tumors in the posterior fossa. 5. Approximately 20–30% of patients require a shunt following tumor resection. 6. Because MB can metastasize throughout the CSF, MRI of the entire spine is indicated on initial imaging. Additionally, many other posterior fossa tumors, such as astrocytoma and ependymoma, can spread through the CSF.
Imaging Findings
Although a head CT may be performed initially, a contrast-enhanced MRI of both brain and total spine is the most helpful imaging tool. Total spine imaging is recommended due to a high incidence of drop metastasis to the spine, which gives the spine a “sugar coated” appearance. A spine MRI should be done prior to surgery to avoid the confusion that arises secondary to postoperative changes and blood seen in the spinal canal post-surgery. Our patient had spinal metastasis on diagnosis (Figure 20.2). On non-contrast head CT, MB presents as an isodense or moderately hyperdense, relatively well-defined mass in the midline or paramidline floor of the fourth ventricle. MB may infiltrate the dorsal midbrain and extend inferiorly into the cisterna magna. Cysts are present in 40% of cases, and calcification may be seen in approximately 20%. MB is rarely grossly hemorrhagic. On contrast-enhanced CT, MB has strong heterogeneous enhancement.Signsofobstructivehydrocephalusarecommon,includingenlargement of the temporal horns, third ventricle, and lateral ventricles, as well as transependymal flow of CSF. On T1-weighted MRI, MB is hypointense and fills the fourth ventricle. T1 contrast- enhanced MRI frequently shows patchy enhancement, although enhancement is highly variable and much of MB does not enhance. MB may compress the pons anteriorly, causing obstructive hydrocephalus. On T2-weighted MRI, MB is mildly to moderately hyperintense, often with hyperintense cysts. As MB is highly cellular, much of the tumor will restrict diffusion and peritumoral edema is present in about 1/3 of cases. FLAIR maydemonstratetransependymalCSFflowwhenobstructivehydrocephalusispresent. Spine MRI is critical due to the frequency of metastasis. Leptomeningeal spread and spinal cord metastasis are usually contrast-enhancing. Although the only way to definitively diagnosis MB is by pathology, MB and ependymoma typically appear somewhat differently on MRI. Ependymomas usually grow laterally out of the foramen of Luschka toward a cerebellar hemisphere. Certain subtypes of MB (namely, desmoplastic) may grow in the lateral cerebellum, although
179
0 8 1
Pediatric Neurosurgery
Figure 20.2. Preoperative spine MRIs demonstrating drop metastasis. (A) T1- weighted axial MRI of thoracic spine, showing metastasis dorsal and ventral to spinal cord. (B) T1-weighted sagittal MRI demonstrating metastasis, most clearly noted in mid-thoracic region. (C) T2-weighted sagittal MRI showing thoracic metastasis. (D) T2-weighted sagittal MRI demonstrating a nodular metastasis at the level of L5.
this is more common in adults than children. When astrocytomas occur in the posterior fossa, they never show restricted diffusion, unlike ependymomas and MB. Important symptoms to recognize are related to hydrocephalus. Nausea, vomiting, ataxia, and headache are almost universal; morning headaches are a common first symptom. Due to the midline cerebellar location, gait instability, psychomotor deficits, diplopia, restricted up-gaze, or spasticity are common.Young children may present with acute, life-threatening hydrocephalus. In infants, common presentations include lethargy, poor feeding, macrocephaly, bulging fontanel(s), diastasis of cranial sutures, and
180
Medulloblastoma
irritability. CSF dissemination may lead to symptoms related to locality of the metastatic focus and cord involvement, including leg weakness, back pain, or bowel or bladder problems. In our patient, head MRI demonstrated a well-demarcated midline mass fill ing the fourth ventricle. It had heterogeneous enhancement and restricted diffusion. Hydrocephalus and transependymal CSF flow were present due to outflow obstruction. Increased fluid was noted around the optic nerves bilaterally. Additionally, drop metastases were seen around the thoracic cord and a metastatic nodule was clearly seen at the L5 level (Figure 20.2). Questions
1. What is the recommended treatment? 2. What preoperative considerations should be made? 3. What additional work-up should be done to guide adjuvant therapy after surgery? 4. Why is age an important consideration for surgical planning and treatment? 5. What stratifies MB as high risk?
Decision Making
MB is a highly malignant WHO grade IV embryonal tumor. Although commonly referred to as a primitive neuroectodermal tumor (PNET) of the cerebellum, it is now known that MB is distinct from PNET and is no longer considered a type of PNET. While MB and AT/RT appear histologically indistinguishable, they remain biologically distinct. MB commonly has isochromosome 17q abnormalities, while AT/RT is characterized by mutation in or loss of INI1 locus at chromosome 22q11.2. Neither of these mutations are found in PNET. Given the aggressiveness of MB, early surgical resectionisstronglyrecommended.Lumbarpuncturetoruleoutdropmetastasisisusually also performed to assist with staging. Lumbar puncture is performed 10–14 days after surgery to avoid false positives that may occur immediately following surgical resection. Ideally, spine MRI should be performed preoperatively. Postoperative MRI should also be performed to assess extent of resection, and the spine MRI should be performed prior to lumbar puncture, as blood from a traumatic tap may be mistaken for metastasis on MRI. Both histological and molecular subtyping for MB aid in guiding treatment and prognosis. The histological subtypes include classic MB and 3 histological variants— desmoplastic/ nodular, MB with extensive nodularity, and large cell/ anaplastic. Desmoplastic MB carries the best prognosis, while large cell/anaplastic has the worst overall survival. On histology, MB appears as sheet-like areas of small round blue cells with minimal cytoplasm. The tumor is highly cellular and mitotic, with occasional Homer-Wright rosettes, necrosis, or hemorrhage. There are four molecular subgroups of MB—Wingless (Wnt) pathway, Sonic hedgehog (Shh) pathway, group 3, and group 4. The Wnt subgroup has the best response to chemotherapy and best prognosis, although it comprises only 10% of MB in
181
2 8 1
Pediatric Neurosurgery
children. The most frequent mutation found in the Wnt subgroup is CTNNB1, which accelerates proliferation through activation of MYC and MYCN oncogenes. The Shh group comprises approximately 30% of MB in children, and prognosis is usually intermediate and depends on histological classification, with desmoplastic histology having the best prognosis. PTCH1 and SUFU are frequent gene mutations found in the Shh group. Group 3 has the highest rate of metastasis and the worst overall survival. Group 3 comprises 35% of MB in children, namely young children and infants, and rarely occurs in adults. Like the Wnt group, group 3 MB has high levels of MYC expression. Both groups 3 and 4 express high levels of OTX2 and FOXG1B. Four characteristics automatically make a diagnosis of MB high risk—age at diagnosis(1.5 cm2 residual tumor). Radiation and chemotherapy are administered as soon as possible following resection. Radiation is avoided in children under 3 years of age due to radiation toxicity to the developing brain. Rather, an aggressive chemotherapy protocol is employed. Surgical Procedure
If an EVD was not already placed, many surgeons choose to do so at the beginning of the procedure. It is advantageous to relieve hydrocephalus and normalize intracranial pressure prior to opening the posterior fossa dura by using an EVD (most common), ventriculoperitoneal shunt, or third ventriculostomy. These measures reduce the intraoperative risk of cerebellar swelling through the dural opening from elevated intracranial pressure. However, with posterior fossa tumors, one also needs to consider the risk of upward herniation due to over-drainage of CSF. Therefore, controlled drainage through an EVD is often employed. Thepatientisplacedundergeneralanesthesiawithadequateintravenousaccessand placement of a Foley catheter. Because surgical resection takes place near lower cranial nerves, intraoperative neuromonitoring may be helpful. Keeping the operating room temperature at an appropriate level, using warming blankets or a conduction system, andwarmedintravenousfluidsmaybeneeded,aschildrenhavepoorthermoregulation. Hemostasis is extremely important, given the low blood volume in children, and it is recommended to have cross-matched blood on hand, as well as peripheral access for rapid transfusion, if necessary. There are 3 possible approaches for removing a posterior fossa tumor—prone, sitting, or lateral (park-bench) positioning—with prone being the most widely used because it provides access to the cerebellar hemisphere, the fourth ventricle, and the cervicomedullary junction. Neck flexion, especially in prone position, must be adequate enough to provide surgical access and views, but not excessive enough to impair venous drainage and airway patency.The advantage of operating in the sitting position is better access to upper cerebellum and inferior tentorium cerebelli with decreased intraoperative blood loss; however, there is increased risk of hypotension and air embolism. Lateral positioning is used for tumors that are further lateral, such as ependymomas. A midline incision is made along the avascular plane with preservation of muscle layers. A cuff of fascia is recommended in order to create a strong and water-tight fascial
182
Medulloblastoma
closure, which is crucial for preventing CSF leak. Burr holes are placed inferior to the transverse sinus bilaterally, each 1 cm from midline. Craniotomy is then performed. The surgeon must be careful of cranial nerves and proximity to the brainstem in posterior fossa surgery. In infants, due to low circulating blood volume, one must be particularly careful not to rupture persistent midline intradural sinuses, which could cause life-threatening bleeding. Once hemostasis has been obtained and intracranial pressure controlled, the dura is opened bilaterally.The telovelar approach is frequently used for a suboccipital posterior fossa surgery.The inferior aspect of the roof of the fourth ventricle is formed by the tela choroidea and inferior medullary velum, and it is through these 2 membranes that the telovelar approach is performed. It is important to identify these structures, as the cranial part of the roof of the fourth ventricle is composed of neural elements. Opening the tela choroidea cranially from the foramen of Magendie reveals the inferior fourth ventricle, while extending the opening through the inferior medullary velum provides access to the superior part of the fourth ventricle. In some cases, a trans-vermian approach to the tumor can be used. Grosstotalresectionisattemptedusingmicrosurgicaltoolsandultrasonicaspiration. The goal of surgery is total resection, as extent of resection improves overall survival. This is especially critical in children under the age of 3 years, in whom radiation is avoided. If the tumor is invasive of the fourth ventricle floor, small residual tumor may be intentionally left, as chemotherapy and radiation are effective adjuvant therapies. Upon completion of the resection, the dura should be closed in a watertight fashion to avoid pseudomeningocele and CSF leak.
Oral Boards Review—Management Pearls
1. Total resection is the goal, as extent of resection, patient age, ependymal spread, and tumor subtype are important predictors of overall survival. 2. Spine MRI and postoperative lumbar puncture are standard care. 3. Radiation (when indicated) and chemotherapy are used post-surgically, even in patients with apparent gross total resection.
Pivot Points
1. If a patient presents with severe signs of hydrocephalus, immediate head CT and placement of an EVD should be considered; however, the EVD should be set at a high level to prevent upward herniation. 2. Acute, life-threatening hydrocephalus with MB is rare and there is often time for MRI and surgical planning. Dexamethasone may also provide sufficient relief of symptoms to allow time for surgery planning. 3. The need for postoperative shunt placement is rare, as most children can be weaned from their ventriculostomy catheter; an endoscopic third ventriculostomy should be considered.
183
4 8 1
Pediatric Neurosurgery
Aftercare
Following surgery, the patient should be admitted to the pediatric intensive care unit with postoperative contrast brain MRI within 48 hours to assess extent of resection. The EVD can usually be weaned and removed within a few days. Lumbar puncture for staging and risk stratification should be performed 10–14 days after surgery. Given the deleterious effects on the rapidly developing nervous system, radiation is avoided in children under 3 years of age. For standard-risk MB, patients receive reduced dose (23.4 Gy) or full dose (36 Gy) cranio-spinal radiation with 54–56 Gy boost to the posterior fossa. Children under 3 years of age undergo surgical resection followed by aggressive chemotherapy. Regardless of standard-risk or high-risk MB, the usual postoperative course includes intensive chemotherapy. Common agents in varying combination include cisplatin, vincristine,etoposide,cyclophosphamide,ifosfamide,andlomustine.Long-termeffectsfrom radiation and chemotherapy can be debilitating. Even with reduced radiation dosing, a substantial decline in IQ may be noticed. Many patients develop headache disorders and are at risk for secondary malignancies following radiation. The entire neuronal axis is at risk, with a broad range of deficits commonly reported. There is no set regimen for follow-up; however, a brain MRI every 3 months for the first 2 years following therapy is recommended, as potential relapse usually occurs within that time frame. After 2 years, follow-up is still recommended, although the imaging interval may be increased. Complications and Management
Complications related to surgery are multiple and often unavoidable, regardless of surgical expertise. Hydrocephalus may persist after surgery, requiring placement of a ventriculoperitoneal shunt. Postoperative cerebellar mutism, also called posterior fossa mutism, may present as dysmetria, hypotonia, dysphagia, hemiparesis, or speech and language apraxia, occurring in 25–30% of patients in various case series. Such symptoms may take 24–48 hours to manifest postoperatively, and are characterized by an oral-motor apraxia. Cerebellar mutism usually improves over months. Our patient presented with verbal mutism, which completely resolved within a month postoperatively. The exact cause or origin of cerebellar mutism is not known, but appears to be associated with brainstem invasion and subsequent dissection of the brainstem. Otherpossiblecomplicationsincludecranialnervepalsies,bothfromthesurgeryand radiation. Careful surgical resection and awareness of the location of cranial nerves with intraoperative monitoring can help prevent palsies. Despite ensuring water-tight dural closure, postoperative pseudomeningocele or CSF leak may occur. For this reason, meticulous fascial closure is important. Occasionally the pseudomeningocele will resolve on its own or with aspiration, but some cases must be surgically corrected. As with any intraduralsurgery,localinfectionormeningitisareconcernsthatshouldbedetected and managed appropriately.
184
Medulloblastoma
Oral Boards Review—Complications Pearls
1. CSF related complications are not infrequent after posterior fossa surgery for medulloblastoma. Meticulous closure at the time of resection reduces the risk of pseudomeningocele or CSF leak. 2. Cerebellar mutism may result from tumor manipulation and resection in the context of brainstem invasion. Mutism generally but not always improves over a period of days to weeks after surgery.
Evidence and Outcomes
MB has been extensively studied and clinical trials are underway to identify treatment regimens with improved survival and reduced toxicity compareed to those currently available. Despite recent advances, extent of surgical resection still strongly influences outcome and all patients with tumor suspicious for MB should be immediately referred to a pediatric neurosurgeon who is experienced with tumor removal. Leptomeningeal dissemination occurs in 27–43% of MB in children, and survival rates vary based on histological and molecular subtype. Patients with molecular subtype in the Wnt profile have an approximately 95% survival rate with treatment. As stated, the Shh group depends on histological subtype, with the desmoplastic variant having the best outcome with a greater than 80% survival rate. Despite treatment, patients with group 3 or 4 subtype have only an approximate 35% survival rate with treatment. Overall 5-year survival for recurrent or disseminated MB with gross total resection is 60%, and 32% with subtotal resection. High-risk MB tends to recur locally despite maximal resection, chemotherapy, and radiation, usually within 2 years of completing therapy, and with disseminated disease. Treatment for recurrent MB, regardless of age, includes repeat brain and spine MRIs followed by resection, radiation, and intensive chemotherapy. References and Further Reading
Dhall G. Medulloblastoma. J Child Neurol 2009;24(11):1418–1430. Crawford JR, MacDonald TJ, Packer RJ. Medulloblastoma in childhood: new biological advances. Lancet Neurol 2007;6(12):1073–1085. Osborn, Anne G. Chapter 21: Embryonal and Neuroblastic Tumors. Osborn’s Brain: Imaging, Pathology, and Anatomy. Amirsys Publishing, Inc. Manitoba: 2013. Raybaud C, Ramaswamy V, Taylor MD, Laughlin S. Posterior fossa tumors in children: developmental anatomy and diagnostic testing. Childs Nerv Syst 2015;31(10):1661–1676. Spennato P, Nicosia G, Quaglietta L, et al. Posterior fossa tumors in infants and neonates. Childs Nerv Syst 2015;31(10):1751–1772. Hervey-Jumper SL, Altshuler DB, Want AC, et al. The role of CD133+ cells in a recurrent embryonal tumor with abundant neuropil and true rosettes (ETANTR). Brain Pathol 2014;24(1):45–51.
185
6 8 1
Pediatric Neurosurgery
Northcott PA, Korshunov A, Witt H, et al. Medulloblastoma comprises four distinct molecular variants. J Clin Oncol 2011;19(11):1408–1414. Tabori U, Sung L, Hukin J, et al. Distinctive clinical course and pattern of relapse in adolescents with medulloblastoma. Int J Radiat Oncol Biol Phys 2006;64(2):402–407. Beroukhim R, Getz G, Nghiemphu L, et al. Assessing the significance of chromosomal aberrations in cancer: Methodology and application to glioma. Proc Natl Acad Sci USA 2007;104(50):20007–20012. Mussi ACM, Rhoton AL. Telovelar approach to the fourth ventricle: microsurgical anatomy. J Neurosurg 2000;92(5):812–823.
186
Hypothalamic-Chiasmatic Glioma James Rutka and Angela Coppola
21
Case Presentation
An 8-year-old girl is admitted to the Emergency Room with a history of persistent headache over the last 2 weeks, worsened in the last 3 days with episodes of vomiting, double vision, and a decrease in normal activity. She had gone to the optometrist the week before, who noted in-turning of the right eye and assigned a diagnosis of strabismus. Her parents reported a 3 month history of increased weight-gain. Apart from these symptoms and signs, there was no significant past history or recent trauma. On detailed neurological examination, a sixth cranial nerve palsy and papilledema are noted. The rest of the examination is unremarkable; there are no stigmata of neurofibromatosis type 1 (NF-1). Questions
1. What is the most likely clinical diagnosis? 2. What is the most appropriate imaging study to order in the emergency room? 3. How would you proceed to investigate this child completely?
Assessment and Planning
Suspecting raised intracranial pressure (ICP), a CT scan was done showing a mass in the suprasellar region causing obstruction of the foramina of Monro and supratentorial hydrocephalus. In the context of a pediatric suprasellar tumor, the differential diagnosis includes hypothalamic-chiasmatic gliomas (HCGs), craniopharyngiomas, germ cells tumors, and pituitary adenomas. In our case, no calcifications and/or cystic components were noted; endocrine hormonal blood tests were normal; and serum tumor biomarkers were unremarkable. Given these findings and test results, the most likely diagnosis is HCG. HCGs are rare tumors, representing approximately 5% of all childhood brain tumors. Of all patients with this diagnosis, 65% occurs in children younger than 5, 80% in the first decade of life. HCGs are usually low-grade gliomas, and pilocytic astrocytoma is the most common histopathological subtype.
187
81
Pediatric Neurosurgery
Oral Boards Review—Diagnostic Pearls
1. Neuro-ophthalmology: impairmentinvisualacuityisthemostcommonclinical finding at presentation (87.5%), followed by nystagmus and strabismus. A central scotoma and peripheral field defects due to the compression of chiasm and optic tracts are also common. Fundoscopy can reveal variable degrees of optic papilla pallor or papilledema. 2. Neurology: non-specific signs and symptoms of raised ICP such as headache, nausea, vomiting and edema of the optic papilla are reported. Seizures are less common. 3. Neuro-e ndocrine: severalimportantneuro-endocrinesignsandsymptomsmay be present such as precocious puberty, linear growth delay, diabetes insipidus, and other hormone deficiencies. Diencephalic syndrome is seen in 21% of infants with HCGs and is characterized by cachexia, increase in fatigue, emaciation, and nystagmus. 4. The diagnosis can be delayed in younger children who are not able to communicate symptoms such as visual acuity loss, double vision and headache. The diencephalic syndrome may also represent a challenging diagnosis due to the numerous alternative causes of failure of thrive. 5. NF-1: HCGs represent the most common central nervous system tumor in patients with NF-1, affecting 11–30% of patients. The optic nerve is more frequently involved than the chiasm and/or retrochiasmatic structures. MRI remains the gold standard for the diagnosis of suprasellar tumors such as HCG, and it is crucial for the management and the assessment of the disease at presentation and in follow-up. Typical findings are iso-hypointense solid tumor signals on T1-weighted images, hyperintensity on T2-weighted images, and homogeneous enhancement following gadolinium administration. FLAIR sequences can be useful to visualize the infiltrativecomponent.Cysticcomponentsarefrequentlyseen,usuallyasaconsequence of tumor degeneration. Existing classifications for the interpretation of the results on MRI are based on topography (e.g., DOGDE classification and modified DOGDE classification)—specific for OPHGs—and on tumor progression (RANO)—validated for all gliomas. In our case the MRI shows the presence of a large suprasellar mass (32 x 30 x 26 mm) arising adjacent to the optic chiasm and extending superiorly to the hypothalamus and III ventricle with a consequent obstructive hydrocephalus (Figure 21.1). The lesion is isointense onT1-weighted images and hyperintense onT2 sequences; post contrast images demonstrate irregular enhancement within the mass. No cystic component or calcifications are noted (Figure 21.2). Questions
1. How do the clinical and radiological findings influence surgical planning? 2. What treatment options are available? 3. How does the diagnosis of NF-1 influence treatment?
188
Hypothalamic-Chiasmatic Glioma
Figure 21.1. CT scan at diagnosis: suprasellar mass and obstructive hydrocephalus.
Decision Making
A multidisciplinary evaluation is needed to reach the main goal of treatment: to control tumor progression and to preserve neural, visual, and endocrine functions.
Oral Boards Review—Management Pearls
1. Wait/w atch/r escan policy: is used with small tumors confined to the optic nerve or chiasm, no obstructions of CSF pathways and no visual deficits.
(A)
(B)
Figure 21.2. Chiasmatic/hypothalamic glioma: pre-treatment imaging. (A) Axial T2-weighted sequence MRI, demonstrating a hyperintense mass with the obstruction of the foramina of Monro. (B) Sagittal T1-weighted with gadolinium, the lesion is isointense.
189
0 9 1
Pediatric Neurosurgery
2. Chemotherapy: can be given to younger patients with low-rate of associated complications, using a combination of Vincristine and Carboplatinum as first- line treatment. It is the first choice in younger patients (less than 3 years) with evidence of progressive disease or threat to eloquent structures. 3. Biopsy at diagnosis: is taken into consideration when clinical or imaging findings are unusual or unclear. Typical HCGs in NF-1 positive patients do not require biopsy, but biopsy is acceptable after multidisciplinary discussion when the patients are managed in a clinical trial with a relevant biological stratification. Biopsy is often performed whenever surgical management of CSF obstruction is required. 4. Primary tumor resection: is not the recommended standard of care. Subtotal or total resection is considered when the size of the tumor causes mass effect due to the compression of the diencephalum or in case of hydrocephalus. 5. Radiotherapy: due to the risk of late sequelae, especially in children younger than 5 years of age and in patients with NF-1, radiotherapy should be considered only after the failure of chemotherapy and surgical debulking.
Pivot Points
1. A neuro-oncology multidisciplinary team evaluation should be adopted in order to formulate a plan for successful tumor control, dependent on the severity of symptoms, child’s age, tumor location and size, and NF-1 status. 2. Characteristics such as early onset (younger than 1 year) and posterior growth pattern with diencephalic symptoms are associated with a more aggressive disease progression. 3. NF-1 is associated with a less aggressive disease course or, occasionally, spontaneous regression. A biopsy is not needed if the appearance on MRI is typical. Inourcasethetreatmentofchoicewasanendoscopicbiopsywithaseptostomy,followed by VP-shunt placement (Figure 21.3). Three lines of chemotherapy were needed to obtaindiseasestabilityover4 years,whichincludedVincristine,Vinblastine,Carboplatinum, and PPCV (Figures 21.4–21.6). Surgical Procedure
The aim of the surgery is to obtain a histological diagnosis, reduce the tumor mass effect without causing additional neurological deficits, and ensure normal CSF circulation. In order to obtain a tumor biopsy, the neurosurgeon can choose between the endoscopicapproach,thestereotactictechniqueoranopenbiopsy.Theendoscopicapproach is a common and safe choice, the neurosurgeon can also perform a septostomy in order to create a communication between the left and the right ventricles. Then, in case of hydrocephalus, a V-P shunt is required to regulate the CSF circulation.
190
Hypothalamic-Chiasmatic Glioma
Figure 21.3. CT scan showing a ventricular catheter placed in the left frontal horn. Air in the right frontal horn, due to the communication between right and left ventricular system after an endoscopic septostomy. Regardingneurosurgicalresection,aftercarefulconsiderationofthepatient’sclinical andradiological presentation,theneurosurgeoncanchoosefromanumberofoperative approaches: Pterional, transcallosal, anterior interhemispheric translaminar terminalis, subfrontal, and subtemporal. The pterional approach is a common choice and it is preferred in tumors with an prominent lateral component. In this approach, the tumor can
(A)
(B)
Figure 21.4. Radiological findings after first-line chemotherapy. (A) Axial T2- weighted sequence. (B) Sagittal FLAIR sequence after gadolinium. Comparing with the pre-treatment imaging, the tumor is stable.
191
2 9 1
Pediatric Neurosurgery
(A)
(B)
Figure 21.5. After the 2nd cycle of chemotherapy, the MRI shows a tumor progression with a slight increase in the size of the tumor and of the left ventricle (A). An irregular contrast-enhancement is noted (B). be reached via a transcortical route, a subfrontal approach, or opening the Sylvian fissure, ending in the suprachiasmatic space. A midline approach is reasonable and safe in tumors with an important exophytic central component, allowing preservation of hypothalamic function. The anterior interhemispheric approach allows excellent visualization of the anterior part of the circle of Willis, the optic nerves, the olfactory nerve and the pituitary stalk. A partial resection of the posterior component of the tumor using a transcallosal approach, especially with large tumors filling the third ventricle, may relieve a number of symptoms. (A)
(B)
Figure 21.6. Two years after the third and last cycle of chemotherapy. The MRI shows a decrease in tumor and ventricles size (A–B), no contrast-enhancement is noted (B).
192
Hypothalamic-Chiasmatic Glioma
Intra-operative neuro-navigation is a useful tool, facilitating a more precise approach and avoiding injury to critical structures. Post-Operative Management
Post-operativeendocrinologicalandneurologicalevaluationsarefundamentaltoassess the new onset of deficits. For most cases, observation with a serial MRI is recommended, with the frequency of imaging being determined by the growth rate of the tumour.Visual examination is crucial and includes visual fields testing, analysis of ocular movements, and fundus oculi. In many cases, HCG is a chronic disease that involves young patients and their families. In this regard, neuropsychological testing over time is very important to identify any early cognitive alterations. Complications and Management
Gross total resection is challenging due to the eloquent location of these tumors. The possible surgical complications are caused by a direct injury to the visual apparatus, hypothalamus and vascular structures. In addition, there is a high frequency of shunt malfunction, most likely due to the high level of CSF protein which can cause shunt blockage. The endocrine dysfunctions are a significant problem, considering that the percentage of a new onset or a progressive deficit during treatment is 64%, and the most common problem is pituitary hormone deficiencies. Chemotherapy has a low rate of associated complications, such as hematologic toxicity,hypersensitivity,andallergies(particularlywithplatinum-containingformulations), neurotoxicity, renal toxicity, and hepatic toxicity. Radiotherapy is associated with long-term side-effects: Endocrine dysfunction (after about 5 years) and cognitive side-effects are well-known sequelae; malignant transformation and secondary vascular syndromes such as moyamoya disease are reported particularly in patients with NF-1 who have higher vulnerability to the secondary effects of radiation therapy.
Oral Boards Review—Complications Pearls
1. Endocrine dysfunction and visual impairment are frequent treatment-related complications. 2. Radiotherapy is associated with long-term side-effects, particularly with younger children and patients with NF-1. 3. Chemotherapy has well-known drug-related toxicity but can be given to younger patients.
Evidence and Outcomes
Overall survival rate is 83–85% over 10 years. Progression-free survival rate is 77% in NF-1 patients and drops to 36% in non-NF-1 patients. In spite of histologically benign characteristics, the behavior of HCGs is unpredictable: the majority shows a slow growth pattern over years; malignant transformation is rare and usually associated
193
4 9 1
Pediatric Neurosurgery
with irradiation, but is also described in young patients, as well as the ability to disseminate along the neuraxis. Younger age (1 year or less), diencephalic symptoms, NF1-negative status, and location along the posterior pathway have been typically associated with a more aggressive disease course.Younger age is an independent poor prognostic factor. The tumor itself can change in configuration over time. The formation of cystic components with mucinous fluid is due to degeneration of the tumor and can cause raisedICPandvisualimpairment,requiringmultipleresectionsanddrainageprocedures (Ommaya reservoirs may be useful for intermittent drainage). In addition, occurrence of intratumoral hemorrhage is not infrequent. Due to the risk of late sequelae, especially in children younger than 5 years of age and in patients with NF-1, radiotherapy is not used unless chemotherapy is ineffective. Now that emphasis has moved away from radical neurosurgical resection towards minimally invasive surgery and chemotherapy, HCGs are becoming more of a chronic disease and patients are treated over many years. At this time, the achievement of stable disease indicates successful treatment. References and Further Reading
Allen JC. Initial management of children with hypothalamic and thalamic tumors and the modifying role of neurofibromatosis-1. Pediatr Neurosurg 2000; 32:154–162. Binning MJ, Liu JK, Kestle JR, Brockmeyer DL, Walker ML. Optic pathway gliomas: a review. Neurosurg Focus 2007;23(5):E2. Garvey M, Packer RJ. An integrated approach to the treatment of chiasmatic-hypothalamic gliomas. J Neurooncol 1996;28:167–183. Silva MM, Goldman S, Keating G, Marymont MA, Kala-Purakal J, Tomita T. Optic pathway hypothalamic gliomas in children under three years of age: the role of chemotherapy. Pediatr Neurosurg 2000;33:151–158. Jahraus CD, Tarbell NJ. Optic pathway gliomas. Pediatr Blood Cancer 2006;46:586–596. Opocher E, Kremer LCM, Da Dalt L, van de Wetering MD, Viscardi E, Caron HN, et al. Prognostic factors for progression of childhood optic pathway glioma: a systematic review. Eur J Cancer 2006;42:1807–1816. Massimi L, Tufo T, Di Rocco C. Management of optic-hypothalamic gliomas in children: still a challenging problem. Expert Rev Anticancer Ther 2007;7:1591–1610. Goodden J, Pizer B, Pettorini B, Williams D, Blair J, Didi M, Thorp N, Mallucci C. The role of surgery in optic pathway/hypothalamic gliomas in children. J Neurosurg Pediatrics 2014;13:1–12. Lee AG. Neuroophthalmological management of optic pathway gliomas. Neurosurg Focus 2007;23 (5):E1. Chourmouzi D, Papadopoulou E, Konstantinidis M, SyrrisV, Kouskouras K, Haritanti A, Karkavelas G, Drevelegas A. Manifestations of pilocytic astrocytoma: a pictorial review. Insights Imaging 2014, 5:387–402. Kocova M, Kochova E, Sukarova-Angelovska E. Optic glioma and precocious puberty in a girl with neurofibromatosis type 1 carrying an R681X mutation of NF1: case report and review of the literature. BMC Endocrine Disorders 2015;15:82
194
Hypothalamic-Chiasmatic Glioma
Avery RA, Ferner RE, Listernick R, Fisher MJ, Gutmann DH, Liu GT. Visual acuity in children with low grade gliomas of the visual pathway: implications for patient care and clinical research. J Neurooncol 2012;110:1–7. Graff JM, Coombs JM, Pramanik S. Neurofibromatosis Type 1—Optic Nerve Glioma: 8- year-old white female with acute awareness of complete vision loss, OS. EyeRounds. org. May 15, 2005; Available from: http://www.EyeRounds.org/cases/38- NeurofibromatosisOpticNerveGlioma.htm. Fisher MJ, Avery RA, Allen JC, Ardern-Holmes SL, Bilaniuk LT, Ferner RF, et al. Functional outcome measures for NF1 associated optic pathway glioma clinical trials. Neurology 2013;18(21 Suppl1):S15–24. Fisher MJ, Loguidice M, Gutmann DH, Listernick R, Ferner RE, Ullrich NJ, et al. Visual outcomes in children with neurofibromatosis type 1—associated optic pathway glioma following chemotherapy: a multicenter retrospective analysis. Neuro Oncol 2012;14:790–797. Williams VC, Lucas J, Babcock MA, GButmann DH, Koef B, Maria L. Neurofibromatosis Type 1 Revisited. Pediatrics 2009;123:124–133. Upadhyaya M. Neurofibromatisis type 1: diagnosis and recent advances. Expert Opin Med Diagn 2010;4:307–322. Szudek J, Evans DG, Friedman JM. Patterns of associations of clinical features in neurofibromatosis 1 (NF1). Hum Genet 2003;112:289–297. Rutkowski JL, Wu K, Gutmann DH, Boyer PJ, Legius E. Genetic and cellular defects contributing to benign tumor formation in neurofibromatosis type 1. Hum Mol Genet 2000;9:1059–1066. Nicolin G, Parkin P, Mabbot D, Hargrave D, Bartels U, Tabori U, Rutka J, Buncic JR, Bouffet E. Natural history and outcome of optic pathway glioma in children. Pediatr Blood Cancer 2009;53(7):1231–1237. McCrea HJ, George E, Settler A, Schwartz TH, Greenfield JP. Pediatric suprasellar tumor. J Child Neurol 2015;Dec 15. pii: 0883073815620671 Allen J: Perspectives on thalamic and hypothalamic tumors in childhood. Ped Neurosurg 2000;32:154–162. Shofty B, Weizman L, Joskowicz L, Constantini S, Kesler A, Ben-Bashat D, Yalon M, Dvir R, Freedman S, Roth J, Ben-Sira L. MRI internal segmentation of optic pathway gliomas: clinical implementation of a novel algorithm. Childs Nerv Syst 2011;27:1265–1272. Listernick R, Ferner RE, Liu GT, Gutmann DH. Optic pathway gliomas in neurofibromatosis- 1: controversies and recommendations. Ann Neurol 2007;61(3):189–198. Segal L, Darvish-Zargar M, Dilenge ME, Ortenberg J, Polomeno RC. Optic pathway gliomas in patients with neurofibromatosis type 1: Follow-up of 44 patients. J AAPOS 2010;14:155–158. Chateil JF, Sousotte C, Pedespan JM, Brun M, Le Manh D, Diard F. MRI and clinical differences between optic pathway tumours in children with and without neurofibromatosis.The British Journal of Radiology 2001;74, 24–31. Dodge HW Jr, Love JG, Craig WM, Dockerty MB, Kearns TP, Holman CB, Hayles AB. Gliomas of the optic nerves. AMA Arch Neurol Psychiatr 1958;79(6):607–621. Taylor T, Jaspan T, Milano G, Gregson R, Parker T, Ritzmann T, Benson C, Walker D, PLAN Study Group. Radiological classification of optic pathway gliomas: experience of a modified functional classification system. Br J Radiol 2008;81(970):761–766. Wen PY, Macdonald DR, Reardon DA, Cloughesy TF, Sorensen AG, Galanis E, Degroot J, Wick W, Gilbert MR, Lassman AB, Tsien C, Mikkelsen T, Wong ET, Chamberlain MC, Stupp R, Lamborn KR, Vogelbaum MA, van den Bent MJ, Chang SM. Updated response assessment
195
6 9 1
Pediatric Neurosurgery
criteria for high-grade gliomas: response assessment in neuro-oncology working group. J Clin Oncol 2010;28(11):1963–1972. Lambron J, Rakotonjanahary J, Loisel D, Frampas E, De Carli E, Delion M, Rialland X, Toulgoat F. Can we improve accuracy and reliability of MRI interpretation in children with optic pathway glioma? Proposal for a reproducible imaging classification. Neuroradiology 2016 Feb;58(2):197–208. Walker DA, Liu J, Kieran M, Jabado N, Picton S, Packer R, et al: A multi-disciplinary consensus statementconcerningsurgicalapproachestolow-grade,high-gradeastrocytomasanddiffuse intrinsic pontine gliomas in childhood (CPN Paris 2011) using the Delphi method. Neuro Oncol 2013;15:462–468. Dodgshun AJ, Elder JE, Hansford JR, Sullivan MJ. Long-Term visual outcome after chemotherapy for optic pathway glioma in children: site and age are strongly predictive. Cancer 2015;121:4190–196. Lee Chong A, Pole JD, Scheinemann K, Hukin J, Tabori U, Huang A, Bouffet E, and Bartels U. Optic pathway gliomas in adolescence-time to challenge treatment choices? Neuro- Oncology 2013; 15(3):391–400. Laithier V, Grill J, Le Deley MC, et al. Progression-free survival in children with optic pathway tumors: dependence on age and the quality of the response to chemotherapy—results of the first French prospective study for the French Society of Pediatric Oncology. J Clin Oncol. 2003;21(24):4572–4578. Alshail E, Rutka JT, Becker LE, Hoffman HJ: Optic Chiasmatic Hypothalamic Glioma. Brain Pathology 1997;7: 799–806. Shofty B, Ben- Sira L, Kesler A, Constantini S. Optic pathway glioma. In: Albright AL, Pollack IF, Adelson PD eds. Principles and practice of pediatric neurosurgery 3rd edition. New York:Thieme Medical Publisher. Cappelli C, Grill J, Raquin M, Pierre- Kahn A, Lellouch- Tubiana A, Terrier- Lacombe MJ, et al: Long-term follow up of 69 patients treated for optic pathway tumours before the chemotherapy era. Arch Dis Child 79:334–338,1998. Collet-Solberg PF, Sernyak H, Satin-Smith M, Katz LL, Sutton L, Molloy P, et al: Endocrine outcome in long-term survivors of low-grade hypothalamic/chiasmatic glioma. Clin Endocrinol (Oxf ) 1997;47:79–85. Erkal HS, Serin M, Cakmak A: Management of optic pathway and chiasmatic-hypothalamic gliomas in children with radiation therapy. Radiother Oncol 1997; 45:11–15. Fouladi M, Wallace D, Langston JW, Mulhern R, Rose SR, Gajjar A, et al: Survival and functional outcome of children with hypothalamic/chiasmatic tumors. Cancer 2003;97:1084–1092. Massimi L, Tufo T, Di Rocco C: Management of optic-hypothalamic gliomas in children: still a challenging problem. Expert Rev Anticancer Ther 2007;7:1591–1610. Thomas RP, Gibbs IC, Wei Xu L, Recht L. Treatment options for optic pathways gliomas. Curr Treat Options Neurol 2015;17(2):333. Kortmann RD, Timmermann B, Taylor RE et al. Current and future strategies in radiotherapy of childhood low-grade glioma of the brain. Part II: treatment-related late toxicity. Strahlenther Onkol 2003;179:585–597. Beyer RA, Paden P, Sobel DF, Flynn FG. Moyamoya pattern of vascular occlusion after radiotherapy for glioma of the optic chiasm. Neurology 1986;36:1173–1178. Ullrich NJ, Robertson R, Kinnamon DD, Scott RM, Kieran MW, Turner CD, et al. Moyamoya following cranial irradiation for primary brain tumors in children. Neurology 2007;68:932–938.
196
Hypothalamic-Chiasmatic Glioma
Shamji MF, Benoit BG. Syndromic and sporadic pediatric optic pathway gliomas: review of clinical and histopathological differences and treatment implications. Neurosurg Focus 2007;23 (5):E3. Gajjar A, Bhargava R, Jenkins JJ, Heideman R. Sanford RA. Langston JW. Walter AW, Kuttesch JF, Muhlbauer M, Kun LE. Low-grade astrocytoma with neuraxis dissemination at diagnosis. J Neurosurg 1995;83: 67–71. Mamelak AN, Pracos MD, Obana WG. Cogen PH, Edwards MS: Treatment options and prognosis for multicentric, juvenile pilocytic astrocytoma. J Neurosurg 1994; 81(1):24–30. Von Hornstein S, Kortmann R-D, Pietsch T, Emser A, Warmuth-Metz M, Soerensen N, Straeter R, Graf N, Thieme B, Gnekow AK. Impact of chemotherapy on disseminated low-grade glioma in children and adolescents: report from the HIT-LGG 1996 trial. Pediatr Blood Cancer 2011;56:1046–1054. Terashima K, Chow K, Jones J, Ahern C, Jo E, Ellezam B, Paulino AC, Okcu MF, Su J, Adesina A, Mahajan A, Dauser R, Whitehead W, Lau C, Chintagumpala M. Long-Term outcome of centrally located low-grade glioma in children. Cancer 2013;119:2630–2638.
197
8 9 1
Mesial Temporal Glioma Gerry Grant
22
Case Presentation
A 13-year-old, right-handed female with no past medical history began having seizures 1 year prior to presentation. The semiology or clinical manifestation of the seizure was characterizedbystaringspells,slappingherhead,lipsmacking,clenchingherhands,and picking at her clothes. She also describes an aura of burning smell prior to start of her seizures. Despite being placed on 3 anti-epileptic drugs, she has continued have 1–2 episodes per day. Detailed neurological exam is unremarkable. She has 1 older brother who is healthy, and there is no significant family medical history. Assessment and Planning
The differential diagnosis for a 14-year-old with new onset seizures is wide. The first objective is to determine whether the child truly has epilepsy or instead has a periodic movement disorder or pseudoseizures. For the patient in this case presentation, there is a classic semiology that helps us localize the seizures to the temporal lobe, due to the presence of aura and automatisms. We then use video-electroencephalography (EEG) monitoring to identify the“ictal” onset zone at the very start of the seizure. We also would obtain neurophysiological testing, which may further help lateralize the seizures if we are able to identify gaps in cognitive domains. If available, magnetoencephalography (MEG) can be useful to map the EEG dipoles onto the MRI to identify epileptogenic spike sources and help define eloquent areas of language or motor function preoperatively. Continuous video EEG on our patient demonstrated epileptiform discharges from the right temporal lobe with secondary generalization. The next step is to obtain structural imaging. CT is not the first line modality, as it does not offer proper anatomical detail. MRI, the gold standard, should be done with a specific epilepsy protocol that includes fine cut coronal T1-weighted and fluid- attenuated inversion recovery (FLAIR) images of the temporal lobe. If there is a structural lesion, gadolinium is needed to help differentiate tumor from dysplasia as well as MR spectroscopy. This patient’s coronal T2- weighted MRI demonstrates an area of T2 FLAIR hyperintensity in the right temporal lobe involving the parahippocampal gyrus. The area does not enhance with contrast (Figure 22.1). In addition, functional pre-operative modalities include a subtraction single-photon emission computed tomography (SPECT) scan derived from ictal and interictal images
199
02
Pediatric Neurosurgery
Figure 22.1. Coronal T2 FLAIR MR image showing high signal intensity in the parahippocampal gyrus. which can help to localize the ictal onset zone to areas of hyperperfusion. An interictal positron emission tomography (PET) is useful in localizing the lesion to areas of hypometabolism. If the patient is left-handed or the ictal onset and lesion is on the left side, a functional MRI is often performed to determine speech lateralization. If there is a concern about memory a Wada test might be helpful to ensure adequate memory function support from the sole remaining hippocampus.
Oral Boards Review—Diagnostic Pearls
1. Any new focal seizure in a child requires a careful diagnostic work-up, including appropriate neuroimaging. 2. The ILEA 2010 classification system distinguishes localization as focal versus generalized epilepsy, etiology as genetic versus structural/metabolic epilepsy, as well as unknown origin. 3. Temporal lobe semiology is common and includes the following features: aura, which is present in the majority cases of mesial temporal origin, and motor findings including aautomatisms and contralateral dystonic posturing. 4. MRI should be obtained using an epilepsy protocol with either 3 or 1.5 Tesla. a. 3T is superior to 1.5 T MR imaging with better spatial and anatomic resolution and increased contrast-to-noise ratio. b. T2 FLAIR and T1 3D gradient-recalled echo coronal sequence are helpful in identifying cortical dysplasia, cavernous malformations, low-grade tumors, and mesial temporal sclerosis. c. Gadolinium contrast should always be included in the initial evaluation. 5. The differential diagnosis for a non-enhancing mesial temporal lesion in a child with seizures originating from the ipsilateral temporal lobe includes
200
Mesial Temporal Glioma
low-grade glioma, glioneuronal tumor, cortical dysplasia, encephalomalacia, vascular malformation, or a low grade tumor mixed with cortical dysplasia. The differential diagnosis is weighted toward tumor in cases, such as this one, that display a temporal lesion with expansile (as opposed to atrophic) properties.
Questions
1. What is the optimal approach to diagnosis and treatment, resection, biopsy, or imaging follow-up? 2. What should the timing of surgery be? Pre-operative imaging: Depending on patient age, a functional MRI in conjunction with neuropsychological assessment of intellectual, language, and memory abilities in addition to handedness can help with surgical planning and risk assessment for speech and memory function. Wada testing, which classically consists of intracarotid injection of amobarbital has also been used to lateralize language and memory representation. Because of the invasive nature of Wada testing, this may not be a suitable modality for young children. Consideration of language function is also important when planning an awake craniotomy for resection of a dominant temporal lobe if there is a need to resect posteriorly along the superior and middle temporal gyri. Timing of surgery: Early surgery should be considered in pediatric patients not just for seizure control but to minimize adverse effects of anti-epileptic drugs, maximize the child’s developmental potential, and reduce behavioral, cognitive, and psychosocial problems. Early seizure control may also prevent secondary epileptogenesis. Decision Making
The relationship between the location of the lesion and localization of the seizures must bedeterminedpre-operatively.Theremaybeacomponentofsecondaryepileptogenesis without clear structural changes or dual pathology with co-existence of hippocampal sclerosis. Secondary epileptogenesis means that the areas surrounding the tumor are also epileptogenic. The process used to evaluate surrounding lesional tissue, in addition to previously discussed modalities, may include presurgical depth or subdural EEG electrodes,aswellasintraoperativeelectrocorticography(ECoG).Lesionectomy,tailored lesionectomy, or lesionectomy combined with removal of mesial structures and anterior lobectomy are commonly used strategies. Intra-operative MRI, if available, may be helpful in determining extent of resection. Location of the tumor— dominant versus non- dominant hemisphere: Approach to the tumor has to be individualized based on the patient’s age, dominant vs. non- dominant side, results of neuropsychological testing, and results of functional or Wada testing. The primary goal of surgery is to remove the lesion. Non-dominant side lesions should have a lower threshold for removal of additional non-tumoral epileptogenic tissue such as the parahippocampal gyrus and/or hippocampus.
201
2 0
Pediatric Neurosurgery
Questions
1. What are the options for surgical approach? 2. What are the major intraoperative complications?
Surgical Procedure
A complete preoperative organ system–based evaluation is necessary to reduce surgical morbidity in pediatric epilepsy patients. If intraoperative ECoG is planned, the selection of anesthetic agents that will not interfere with EEG should be used. Pre-operative antibioticsshouldbeadministered,aswellaspatient’susualanti-epilepticmedicationson the morning of surgery. Dexamethasone is usually started before incision and is tapered slowly post-operatively. Intraoperative navigation is recommended to help guide the resection and localize the temporal horn of the lateral ventricle, which is an important landmark. After intubation and placement of 2 large-bore IV lines, arterial line, and Foley catheter, the patient is positioned prone with an ipsilateral shoulder bump. The head is affixed in a Mayfield head clamp or a Sugita head holder. The head is turned toward the contralateral side such that the sagittal suture is parallel to the floor with slight head extension.Allpressurepointsshouldbeinspectedandpaddedappropriately.Afterastereotactic navigation system has been registered, a curvilinear incision is drawn starting from the root of the zygoma to 1 cm behind the pinna of the ear, curving antero-medially just behind the hairline above the insertion of the temporalis muscle. The eyes are covered and a small piece of Xeroform inserted into the external auditory meatus for protection. The surgical area is then cleansed and prepped and injected with 0.25% Marcaine withepinephrineforaddedhemostasis.Thesurgicaldrapesareappliedandaftersurgical time-out and confirming availability of the necessary equipment and accuracy of navigation, the procedure is started. Skin is opened with a 15 blade followed by monopolar cautery. A myocutaneous flap is elevated, exposing the posterior root of the zygoma. A towel should be placed behind the scalp flap to prevent devascularization and the flap retracted back with scalp hooks. Intraoperative navigation can be used to localize the Sylvian fissure and to plan the craniotomy. Craniotomy should be tailored to each specific patient and pathology. We commonly extend the craniotomy about 1 cm above the Sylvian fissure to allow partial exposure of the inferior frontal lobe. Inferiorly the craniotomy should be flush with middle fossa floor. Bony edges should be waxed and major dural bleeders cauterized with bipolar cautery. Dural edges should be tacked up to the craniotomy edges with suture. The dura is opened in a U-shaped manner with a sharp hook and an 11 blade and reflected away with the temporalis muscle. The dura is covered with a moist Telfa and sutured to the temporalis with 4–0 braided nylon suture to allow maximal anterior exposure.Beforeplanningthecortisectomy,additionalintraoperativeECoGrecordingscan be performed. In our patient, the ECoG confirmed that the mesial temporal structures were also quite active interictally (parahippocampus and hippocampus) and should be resected along with the tumor. Depending on the specific case and if dealing with the dominant lobe, a more limited approach may be appropriate. In most if not all cases, the
202
Mesial Temporal Glioma
goal should be total resection of the tumor at minimum, except when the tumor extends above the temporal stem. In our case the next step was to start the antero-lateral temporal lobectomy. This was done by cauterizing the pia with bipolar electrocautery at the superior aspect of the middle temporal gyrus, parallel to Sylvian fissure, all the way from the anterior temporal tip to just short of the vein of Labbé posteriorly. The 15 blade is used to open the pia and the ultrasonic aspirator can be used to resect down to the white matter, making a trough in an L-shaped pattern until a pial plane is reached at the level of the collateral sulcus. At this point it is important to localize the anterior tip of the temporal horn. This is crucial to help localize the medial structures, including the hippocampus, amygdala, and fusiform gyrus. Once the ventricle is identified, a small cottonoid is placed in it to protect the choroid plexus and help prevent potential injury to anterior choroidal artery at the choroidal point. In our patient, abnormal tissue was localized around the fusiform gyrus. This could be visualized well after the removal of anterior part of the temporal lobe. Several pieces were sent for pathology before removal of all the abnormal tissue. Our patient’s pathology was consistent on frozen section with a low-grade glioma. Resection of medial structures: After removal of anterior temporal pole en bloc, the uncus was aspirated, which is the most medial part of the parahippocampal region. Care is taken to stay completely subpial to avoid injury to neurovascular structures below the pia such as the third nerve and posterior cerebral artery. No bipolar cautery is performed medial to the tentorial edge. The hippocampus is located just lateral to choroid plexus withinthe choroidalfissure.Theamygdalaisagrayishstructureaboveandantero-medial to the pes of the hippocampus.The amygdala should be removed first, staying lateral and inferior to an imaginary line between the choroidal point and Sylvian fissure. The hippocampus is removed en bloc from posterior to anterior direction using the ultrasonic aspirator at the lowest settings so as not to disrupt the pia over the brainstem. Extent of tumor removal and adequate removal of epileptogenic tissue can be confirmed with intra-operative MRI in lesional cases if available, and ECoG is repeated after resection by placing electrodes at the margins of the resection bed. After confirming that all abnormal and lesional tissue has been removed, hemostasis should be obtained and the dura closed in a watertight manner. Dural closure may require a graft, such as autologous pericranium. After irrigation, the bone plate should be re-affixed with titanium plates and screws, while paying close attention to be sure the temporalis muscle is suspended behind the orbitozygomatic process for proper cosmesis. Galea and skin are closed with interrupted absorbable sutures and superficial skin with a running absorbable suture. A sterile dressing is applied and removed on post-operative day 2.
Oral Boards Review—Management Pearls
1. Early surgery is recommended for medically intractable epilepsy after the patient has failed adequate trials of at least 2 appropriately chosen anti-epileptic drugs.
203
4 0 2
Pediatric Neurosurgery
2. The goal of surgery should be gross total lesionectomy of low-grade temporal tumors with consideration for additional tailored resection including hippocampus and adjacent cortex. 3. Use intraoperative stereotactic navigation and ECoG to guide resection. 4. Identify the temporal horn of the lateral ventricle early to help identify important medial structures. 5. Protect the choroid plexus to avoid injury to the anterior choroidal artery and its branches. 6. Respect medial pial planes to avoid injury to the brainstem, posterior cerebral artery, or third nerve.
Pivot Points
1. If the patient has dual pathology or evidence of an epileptogenic zone extending to the medial structures consider amygdalohippocampectomy along with mesial tumor resection. 2. Consider invasive electrophysiological monitoring pre-operatively using stereo EEG or subdural grids if the results of non-invasive monitoring are non-congruent or inconclusive or there is neocortical onset in the lateral temporal lobe, adjacent to eloquent language cortex.
Aftercare
The patient is cared for in the pediatric ICU immediately post operatively. Antibiotic administration is continued for 24 hours and dexamethasone is slowly tapered over 5 days. Follow-up is at 1 month, 3 months, 6 months, and 1 year after surgery. Post- operativeneuropsychologicalevaluationisin2 years.Antiepilepticmedications are continued though the immediate postoperative period and then are slowly tapered after 6 months if the patient is seizure free. An EEG is often performed prior to tapering the mediations. An epilepsy protocol MRI with and without gadolinium is obtained at 3 months postoperatively. Post-surgical follow-up by the epilepsy team should last at least 5 years. Complications and Management
The most serious potential complications from the surgery include neurological injury to medial structures, or injury to the anterior choroidal artery if one is too aggressive in coagulating the choroid plexus within the temporal horn of the lateral ventricle. Injury to the anterior choroidal artery can cause contralateral hemiparesis, which nonetheless has a good prognosis for recovery. Injury to eloquent cortex, especially if operating on thedominanthemisphere,cancausetransientorpermanentlanguagedeficits.Removal of medial structures during amygdalohippocampectomy can cause memory deficits most commonly on the dominant side, especially if the hippocampus was normal on
204
Mesial Temporal Glioma
imaging and if memory was normal preoperatively. Injury to the large draining veins on the hemispheric surface, such as the vein of Labbé, can cause a post-operative stroke. Naturally, the possibility exists that seizures do not resolve, requiring consideration for re-resection.This can result from error in pre-operative seizure localization or inadequateextentofresection.Re-resectionshouldbeconsidered,butitalwayshasadditional risks, as anatomy will be distorted and gliosis and scarring will make the operation more difficult.
Oral Boards Review—Complications Pearls
1. Careful pre-operative planning for the correct extent of surgery is key to obtaining the best possible seizure outcome. 2. Post-operative seizures, if they occur, require prompt treatment, as they can lead to significantly increased morbidity.
Evidence and Outcomes
Outcomes for lesional temporal lobe epilepsy are excellent. Achieving Engel I and II outcome is more likely in a patient with tumor-related epilepsy than epilepsy secondary to cortical dysplasia. The main predictor of outcome is the extent of resection. The pathology of the tumor is also important. The best outcomes are from resection of gangliogliomas and DNETs. There is generally no need for adjuvant therapy following surgery once pathology is confirmed. Young children have better potential for recovery and capacity for reorganization of neurological function due to plasticity of their brain. This is why surgery should not be delayed once it has been established that seizures are medically refractory, as the young developing brain is also more vulnerable to injury from continued seizure activity. References and Further Reading
Rosenow, F. and H. Luders, Presurgical evaluation of epilepsy. Brain, 2001. 124(Pt 9): p. 1683–1700. Duncan,J.,Thecurrentstatusofneuroimagingforepilepsy.CurrOpinNeurol,2009.22(2): p.179–184. Berg,A.T.,et al.,Revisedterminologyandconceptsfororganizationofseizuresandepilepsies: reportof the ILAE Commission on Classification andTerminology, 2005-2009. Epilepsia, 2010. 51(4): p. 676–685. Bautista,J.F.andH.O.Luders,Semiologicalseizureclassification: relevancetopediatricepilepsy.Epileptic Disord, 2000. 2(1): p. 65–72; discussion 73. Knake,S.,et al.,3TphasedarrayMRIimprovesthepresurgicalevaluationinfocalepilepsies: aprospective study. Neurology, 2005. 65(7): p. 1026–1031. Depositario-Cabacar,D.T.,J.J.Riviello,andM.Takeoka,Presentstatusofsurgicalinterventionforchildren with intractable seizures. Curr Neurol Neurosci Rep, 2008. 8(2): p. 123–129. Jeong,S.W.,et al.,Prognosticfactorsinanteriortemporalloberesectionsformesialtemporallobeepilepsy: multivariate analysis. Epilepsia, 1999. 40(12): p. 1735–1739. Benifla,M.,et al.,Temporallobesurgeryforintractableepilepsyinchildren: ananalysisofoutcomesin126 children. Neurosurgery, 2006. 59(6): p. 1203–1213; discussion 1213–1214.
205
6 0 2
Pediatric Neurosurgery
Clusmann,H.,et al.,Lesionalmesialtemporallobeepilepsyandlimitedresections: prognosticfactorsand outcome. J Neurol Neurosurg Psychiatry, 2004. 75(11): p. 1589–1596. Cross, J.H., et al., Proposed criteria for referral and evaluation of children for epilepsy surgery: recommendationsoftheSubcommissionforPediatricEpilepsySurgery.Epilepsia,2006. 47(6): p. 952–959.
206
Craniopharyngioma Lissa C. Baird
23
Case Presentation
A 2-year-old girl is referred to pediatric neurosurgery by her ophthalmologist for a new finding of intracranial mass. She initially presented with right amblyopia, intermittent exotropia, and mild ptosis. Her initial ophthalmologic exam demonstrated visual acuity of 20/300 on the right, and 20/40 on the left. After a 6-week trial of eye patching she was re-evaluated and noted to have left visual acuity of 20/400 with persistent amblyopia. She also had a new finding of mild bilateral optic nerve pallor. An MRI (magnetic resonance imaging) was obtained and a suprasellar intracranial mass lesion was discovered. Further discussion with her parents elucidates a recent history of frequent falls, bumping into objects, and occasional emesis. She has had no complaints of headache or history of episodes of unexplained irritability. Her neurologic examination reveals an alert and well-appearing toddler. She has equal and reactive pupillary function, intact extra-ocular movements, and a dysconjugate gaze. Right eye vision is grossly poor. Her cranial nerves are otherwise intact, her strength is normal, and her gait is unremarkable for age. Questions
1. What is the differential diagnosis? 2. What further imaging studies, if any, should be obtained? 3. What is the appropriate timing for further diagnostic work-up and intervention? 4. What further clinical evaluation should occur?
Assessment and Planning
A neoplasm in the suprasellar space with mass effect on the optic apparatus is determined to be the cause of the visual and ocular symptoms in this patient. The differential diagnosis of a suprasellar mass in the pediatric population includes craniopharyngioma, pituitary adenoma, optic pathway glioma, hypothalamic glioma, Rathke’s cleft cyst, germinoma, teratoma, chordoma, hamartoma, meningioma, and dermoid cyst. Further imaging studies may narrow the differential and assist with surgical planning. Considerations may be made for obtaining a CT scan of the head and facial bones, stereotactic navigation sequences, magnetic resonance (MR) spectroscopy, or
207
8 0 2
Pediatric Neurosurgery
Figure 23.1. Head CT demonstrates calcifications along the posterior capsule of the tumor.
MR angiography. In this case, a CT scan is obtained and demonstrates calcifications along the base and posterior capsule of the tumor (Figure 23.1). This finding narrows the differential significantly, as peripheral calcifications are seen in 90% of pediatric craniopharyngiomas, and are far less likely to occur in this pattern in the other described pathologies. Children with suprasellar craniopharyngioma most commonly present with headache, although half will demonstrate visual symptoms. Visual loss is well tolerated at this young age, and profound deficits may be present by the time of presentation, with up to 84% demonstrating abnormal visual function at time of diagnosis. Hormonal insufficiency such as growth failure, delayed sexual maturation, excessive weight gain, or diabetes insipidus (DI) is present in 52–87% of children at time of diagnosis. Other findings may include psychomotor slowing, memory deficits, a decline in academic performance, or signs and symptoms of hydrocephalus. In a patient old enough to cooperate, preoperative visual field testing by neuro-ophthalmology should be obtained. A preoperative endocrine evaluation should also be performed, including assessment of adrenal axis, thyroid function, electrolyte and fluid balance, and growth function. This 2-year-old patient would not cooperate with visual field testing. Endocrine work-up is normal. Detailed imaging review demonstrates a lobulated cystic sellar and suprasellar tumor, with mass effect on the bilateral frontal lobes, optic chiasm, and right greater than left optic nerves. The bilateral A1, A2, and anterior communicating arteries are encased by the tumor capsule. The cystic contents are hyperintense on T1 and T2 MR sequences. The pituitary stalk is not visualized. The ventricles are normal (Figure 23.2). In addition to the calcifications, the CT
208
Craniopharyngioma
(A)
(B)
(C)
Figure 23.2. Preoperative MRI demonstrates a cystic, lobulated, sellar and suprasellar mass.
demonstrates that pneumatization of the sphenoid sinus has not yet occurred (Figure 23.3). Visual symptoms in the setting of mass effect from craniopharyngioma mandate urgent intervention, as rapid deterioration and permanent loss of vision is known to occur. Questions
1. What are the anatomic and clinical factors that need to be considered when determining optimal operative approach? 2. What operative techniques may be used to optimize surgical exposure and limit morbidity from brain retraction? 3. What is the treatment goal for first time surgical intervention in pediatric craniopharyngioma?
Figure 23.3. Sphenoid sinus pneumatization is absent.
209
0 1 2
Pediatric Neurosurgery
Oral Boards Review—Diagnostic Pearls
1. Pediatric craniopharyngiomas have a typical radiographic appearance as a lobulated, sellar, and suprasellar mass. a. Solid tumor components enhance with gadoliunium, and cystic components may be hyperintense or hypointense on MR T1 sequences. b. About 90% of tumors will demonstrate calcifications on CT imaging in a stippled and usually peripheral location on the mass. c. Displacement of optic and vascular structures is common. d. Focal areas of fluid-attenuated inversion recovery (FLAIR) signal hyperintensity in adjacent brain may indicate pial adherence or transgression due to past cyst rupture. Brain or vascular injury during surgical resection is a higher risk in the presence of this finding. 2. Preoperative MR and CT imaging should be performed and studied in detail in order to define the extent and location of tumor anatomy, the presence of cystic and solid components, and the displacement or involvement of normal brain structures including the optic nerves and chiasm, pituitary gland and stalk, hypothalamus, and vasculature. a. Ventricular anatomy and any obstruction to CSF flow should be visualized on preoperative imaging. 3. Visual symptoms are frequently involved in the presenting clinical picture, and a complete neuro-ophthalmological assessment in the preoperative period is critical. a. The presence of visual field deficit mandates urgent timing of surgical intervention. 4. Endocrinopathies may be present but undiagnosed at the time of clinical pres entation. While surgical intervention commonly results in further compromise of baseline endocrine function, a preoperative assessment of the adrenal axis, thyroid function, growth history, and electrolyte and fluid balance should be performed.
Decision Making
Pediatric craniopharyngioma is a histologically benign neoplasm with potential for malignant clinical behavior. Presenting vision and endocrine deficits are common, and the natural history carries unacceptable morbidity, including blindness, complete hypothalamic and pituitary dysfunction, and death. The goal of initial treatment for craniopharyngioma in the pediatric population should be permanent tumor control or cure in order to minimize morbidity from recurrent and progressive disease. Surgical interventions carry high associated morbidity for this diagnosis, especially to the endocrine system. As a result, multiple palliative interventions have been developed as treatment options which may carry lower short-term risk. These options include intracystic therapy, interval cystic aspiration through catheter reservoirs, or minimal surgical resection followed by radiotherapy treatment.While these palliative measures may provide temporary relief and some tumor control, progression is very common.
210
Craniopharyngioma
Management of future recurrent craniopharyngioma carries a significant increase in risk and morbidity due to the tendency of these tumors to become more adherent to surroundingneurovascularstructures.Also,intracystictherapieshaveunpredictableefficacy and can result in severe neurologic compromise in the event of leakage outside of the tumor capsule.The likelihood of permanent control decreases substantially with recurrent disease after palliative treatment. The potential life-years of the pediatric patient should be considered when making treatment decisions in regard to both lifelong impact of treatment complications and tumor recurrence. Complete microsurgical or endonasal resection of the tumor at time of initial diagnosis is advocated by our center. Should prior cyst rupture or tumor invasion into surrounding neurovascular anatomy prohibit complete removal with acceptable morbidity, then maximal safe resection is undertaken followed by adjuvant radiotherapy for control of residual disease. Radiotherapy carries unpredictable delayed neurovascular and oncogenic risk, along with potential for long-term developmental and neuropsychological deficits. It is therefore only utilized in the setting of unresectable residual or recurrent tumor. Surgicalapproachoptionsincludeexpandedendonasalapproach(EEA)forresection throughthesphenoidsinusandskullbase,andopenapproachthroughacraniotomy.For EEA to be considered, the child must have sufficiently pneumatized sinuses to allow for access to the skull base. Considerations of prior tumor cyst rupture with subsequent development of adhesions to vascular structures, as well as the lateral extent of the tumor, may influence the likely outcome of complete resection using an endoscopic approach. This 2-year-old patient has optimal tumor anatomy for EEA; however, her sphenoid sinus has not yet developed, thus making this an unfeasible option. Many variables of craniotomy have been described for open resection of craniopharyngioma. I prefer modifications of the orbitozygomatic approach, with extent of bony removal individualized for each patient and influenced by the posterior, superior, and inferior location of tumor extension. If asymmetric visual compromise is present at the time of surgical resection, the craniotomy should be performed on the side with poorer visual function. For this patient, a right-sided modified orbitozygomatic approach is recommended. Questions
1. Which anatomic, clinical, and radiographic features will influence the decision for surgical approach? 2. What post-operative measures should be implemented in anticipation of surgical compromise to the endocrine system? 3. What intraoperative findings may influence extent of surgical resection and need for adjuvant therapy in the post-operative period?
Surgical Procedure
The patient is brought into the operating room, and general anesthesia is initiated. Intravenous access is obtained, considering the potential need for fluid resuscitation
211
2 1
Pediatric Neurosurgery
should diabetes insipidus manifest intraoperatively. An arterial line is placed, and the patient is given a preoperative dose of dexamethasone 0.1 mg/kg, prophylactic antibiotics, and mannitol 0.5 mg/kg to assist with brain relaxation. Serum electrolytes are monitored throughout the procedure. Positioning of the patient is supine, with the head in extension with lateral turn to the left, and secured in 3-point pin fixation. Frameless stereotaxy is not mandatory given the presence of clear, fixed anatomic landmarks in this surgical approach, but may be utilized as an optional adjunct. A curved coronal incision is planned from the root of the zygoma to the contralateral paramedian region behind the hairline. The skin is prepared and draped in sterile fashion. Scalp is carefully elevated, with interfascial dissection deep to the superficial temporal fat pad in order to protect the frontal branch of the facial nerve.The temporalis muscle is elevated in the subperiosteal plane to prevent atrophy. The orbitozygomatic craniotomy is modifed for this patient’s tumor anatomy, and the zygoma is left intact. A frontotemporal craniotomy with inclusion of the orbital rim from the supraorbital foramen/notch to the frontozygomatic suture is elevated in 1 piece. Although a single-piece craniotomy involves more extensive osteotomies to release the flap from the orbital roof, wall, and sphenoid wing, the postoperative cosmetic outcome is superior to a 2-piece bone flap. Removal of the orbital rim improves exposure of the posterior tumor capsule near the hypothalamus and basilar artery. Care is taken to leave the periorbital dura intact in order to avoid injury to the orbital contents. If the frontal sinus is exposed, it can be superficially occluded with muscle and covered with a vascularized pericranial flap. Extradural bone removal from the skull base is performed using a high-powered drill. The orbital roof is drilled flat and thinned, the medial sphenoid ridge is removed down to the meningo- orbital band. The band is coagulated, divided, and extradural dissection down to the anterior clinoid and optic canal is performed. Removal of the anterior clinoid allows significantly improved visualization into the sella. This is accomplished by using a 3-4 mm diamond burr with continual irrigation. The lateral roof of the optic canal is opened, and the optic strut is detached from the sphenoid bone.The internal wall of the clinoid is then thinned until it can be fractured off with microforceps and removed. The dura is opened and reflected anteriorly. The Sylvian fissure is opened widely and CSF is drained from the subarachnoid and cisternal spaces to augment brain relaxation. These measures, along with the bony removal, will minimize or completely eliminate any need for retraction on the frontal lobe. The middle cerebral artery is identified in the Sylvian fissure and followed to the carotid bifurcation. The vascular anatomy should be identified and protected early on in the procedure. After identification of the tumor capsule, the cyst is aspirated, taking care to avoid spillage of cyst contents into the subarachnoid space, as this will induce a potent inflammatory response. The tumor resection is then carried out using internal debulking of solid and cystic components followed by meticulous extracapsular dissection from surrounding neurovascular structures. If the pituitary stalk can be preserved and carefully dissected from the tumor capsule, it should be left intact. If the stalk cannot be safely dissected, it is preferable to sever the stalk rather than put traction on or manipulate the attached hypothalamus. Optic chiasm and nerves should be carefully decompressed.
212
Craniopharyngioma
An angled mirror and ring curettes may be helpful for resection of tumor within the corners of the sella. Vascular structures of the circle of Willis may have formed significant adhesions to the tumor either from prior leakage of cyst contents, or through embedded calcified capsule into the wall of the artery. A small amount of residual tumor capsule should be left behind in these situations, rather than risk a major vascular injury. The basilar artery is usually protected by the membrane of Liliequist; however, distal tumor manipulation should be minimized until access to the vascular structures has been obtained with ongoingtumorremoval.Vascularadhesionsaresometimesassociatedwithintra-operative bradycardia resulting from traction on the tumor capsule and, secondarily, on the adherent blood vessel’s adventitia.When encountered, this serves as an important warning sign to the surgeon. The tumor is completely removed in this fashion. Strict hemostasis is observed. Any spasm of major cerebral arteries should be managed with papaverine pledgets and irrigation until resolved. The dura is closed in watertight fashion and tack-up sutures are placed to avoid epidural fluid collection.The bone is secured with titanium microplates, ensuring the orbital rim is lined up perfectly.The temporalis muscle is re-suspended to a fascial cuff left on the bone flap. Any large cranial gaps should be filled with bone putty to ensure optimal cosmetic result.The scalp is closed in standard fashion with absorbable sutures.
Oral Boards Review—Management Pearls
1. Every attempt should be made to achieve complete resection of the tumor without unacceptable neurologic compromise. If tumor is severely adherent to the hypothalamus or critical vascular structures, the goal of the surgery should be changed to maximal safe resection. A thin rim of adherent capsule is left attached to the artery in order to protect the patient from significant surgical morbidity. Adjuvant radiotherapy can be effective for long-term control with small amounts or residual tumor. 2. Surgical approach is selected based on presence of pneumatized sinuses, location and lateral extent of tumor, suspicion for vascular adhesions to the tumor capsule, and lateralization of preoperative visual deficit. 3. Removal of the orbital rim and anterior clinoid, along with drilling of bone at the skull base, will allow for optimal visualization of peritumoral anatomy, and avoidance of retraction on the frontal lobe during tumor resection. 4. An excellent cosmetic outcome can be achieved with attention to dissection and reconstruction techniques. The bone flap and orbital rim are ideally removed in 1 piece. The scalp is elevated after interfascial dissection of the superficial fat pad for protection of the frontal branch of the facial nerve. The temporalis muscle is dissected in the subperiosteal plane. Bony defects are filled with bone putty when indicated.
213
4 1 2
Pediatric Neurosurgery
Pivot Points
1. If significant attachments of the tumor capsule to the hypothalamus or vascular structures are encountered, it is appropriate to leave a small amount of residualcapsuleandtreatwithadjuvantpostoperativeradiotherapyratherthan expose the patient to significant risk for vascular injury and stroke, or permanent hypothalamic dysfunction. The function of the hypothalamus should be prioritized over efforts to preserve the pituitary stalk. If the stalk cannot be freed from the tumor capsule without manipulation, it should be severed at a distal point in order to avoid any traction on the hypothalamus. 2. The function of the hypothalamus should be prioritized over efforts to preserve the pituitary stalk. If the stalk cannot be freed from the tumor capsule without manipulation, it should be severed at a distal point in order to avoid any traction on the hypothalamus.
Aftercare
The patient is extubated and recovered in the PACU prior to transfer to the pediatric intensive care unit. Hourly neurologic checks are performed and the volume status is strictly recorded. The Foley catheter should be left in place until the patient’s endocrine status has stabilized. Diabetes insipidus should be anticipated in the majority of patients, and short interval electrolytes, urine osmolality, urine specific gravity, and fluid deficit assessments are initiated. Complete injury to the pituitary stalk will result in a triphasic response, with DI transitioning to SIADH, and back to DI. It is therefore critical to continue ongoing monitoring of labs and volume status even after initial stabilization of postoperative DI. Endocrinology will assess hormonal function in the immediate and ongoing post- operative period, as some deficits may demonstrate late presentation or even resolution. A post-operative dexamethasone taper is completed, followed by initiation of hydrocortisone replacement therapy until the function of the hypothalamic-pituitary-adrenal axis has been established. Long-term endocrine follow-up and care is necessary in the pediatric population to ensure optimal growth and maturation. Adjuvant therapy, when necessary, can be planned after several weeks of wound healing. Surveillance post-operative MR imaging is obtained over long-term follow-up care in the multidisciplinary brain tumor clinic (Figure 23.4). Complications and Management
Post-operative worsening of endocrine status is expected in most cases. The endocrinology service should be involved with the patient’s care from an early stage, and will need to establish long-term follow-up as the patient grows older and hormonal requirements change. Long-term injury to hypothalamic function, especially the satiety centers, should be monitored for as the patient grows. Hypothalamic dysfunction is typically quite morbid and difficult to treat. Significant neurovascular injuries can typically be avoided with careful preoperative planning and good surgical technique. Craniopharynigoma, however, is known to have
214
Craniopharyngioma
Figure 23.4. MRI 2 years after initial complete resection is negative for recurrent disease. a higher risk of arterial injury than most tumors in this region due to the propensity for vascular wall invasion and calcified attachment. Distal tumor manipulation during resection should be avoided, as any avulsion of a vascular wall will be difficult to repair if tumor bulk prevents access to the bleeding vessel. If initial dissection of the tumor reveals significant prior scarring in the suprasellar region, vascular clips should be made available for any potential unexpected injury. Such an injury should be primarily repaired and patency of the vessel verified with Doppler to avoid a catastrophic ischemic event. Hydrocephalus, if present at presentation, can be managed intraoperatively with a temporary ventricular drain. Following resection of the tumor, CSF flow pathways are re- established,anddefinitivesurgicalinterventionforhydrocephalusshouldnotbeneeded. Cerebrospinal fluid leakage and infection are rare with craniotomy approach.
Oral Boards Review—Complications Pearls
1. Treatment-related morbidity is acute with surgical intervention, and requires immediate postoperative management in the intensive care unit. Radiotherapy is associated with delayed treatment morbidity, and may include vasculopathy, secondary malignancy, vision loss, endocrinopathy, or neurocognitive impact. Long-term monitoring of these patients by a multi- disciplinary pediatric brain tumor team, including endocrinology, is important to optimize final outcome and quality of life. 2. Inadequate tumor control after initial treatment will result in inevitable recurrence, with more complex and less effective treatment options, and higher associated treatment morbidity. Every effort should be made to achieve permanent tumor control with the initial intervention. 3. Unexpected intraoperative complications, such as neurovascular injury, can be avoided with careful preoperative planning and good surgical technique. Peritumoral arteries should never be sacrificed in the setting of injury, and microvascular repair will be necessary should this occur.
215
6 1 2
Pediatric Neurosurgery
Evidence and Outcomes
Radiographically confirmed total resection has been reported between 80–100% in large, retrospective case series of pediatric craniopharyngioma. Recurrence rates following complete resection are reported from 0–52%, with an average 10-year recurrence rate of 16%. Tumor recurrence may be distant from the primary site as a result of implantation during the initial surgical procedure. Reoperation should be attempted when feasible, and while technically more difficult in the setting of adhesions from previous surgery, resection of recurrent disease may still be curative. Perioperativemortalityrateshavedecreasedoverthepast15 years,withrecentreports between0–4%.Pediatrictumorcenterswithhighervolumeshavedemonstratedimproved tumor outcomes, as well as lower morbidity and mortality rates. Craniopharyngiomas are challenging and complex tumors, and are optimally treated at high-volume centers. Post-operative visual improvement is described in 30–50% of cases, although visual decline has been seen in up to 13% of patients in some series. New post-operative endocrinopathiesarefrequentlyexpected,andreportedbetween60–93%.Fortunately, progression of endocrinopathies after complete tumor removal is rare. There have been variable reports on the neurocognitive impact of surgical treatment forcraniopharyngioma,andthisareawarrantsfurtherstudy.Overallsurvivalratesamong patients treated with radical resection vs subtotal resection and radiotherapy are comparable; however, long-term data on quality of life as affected by behavioral, emotional, and cognitive sequelae are limited. References and Further Reading
Recurrent craniopharyngioma after conformal radiation in children and the burden of treatment. Klimo P, Venable G, Boop F, Merchant T. J Neurosurg Pediatr. 2015 May;15(5):499–505. Role of radiation therapy and radiosurgery in the management of craniopharyngiomas. Suh J, Gupta N. Neurosurg Clin N Am. 2006 Apr;17(2):143–148. Thetranssphenoidalresection ofpediatriccraniopharyngiomas: acaseseries.JaneJ,PrevedelloD, Alden T, Laws E. J Neurosurg Pediatr. 2010 Jan;5(1):49–60. Efficacy and safety of radical resection of primary and recurrent craniopharyngioma in 86 children. Elliott R, Hsieh K, Hochm T, Belitskaya-Levy I, Wisoff J, Wisoff J. J Neurosurg Pediatr. 2010 Jan;5(1):30–48. Neuropsychological outcome in patients with childhood craniopharyngioma and hypothalamic involvement. Ozyurt J, Thiel C, Lorenzen A, Gebhardt U, Calaminus G, Warmuth-Metz M, Muller H. J Pediatr. 2014 Apr;164(4):876–881.
216
Diffuse Brainstem Glioma Nalin Gupta
24
Case Presentation
An 8-year-old girl presents with a several week history of intermittent double vision that the parents describe as 1 one eye deviating inward when she attempts to visually fixate on objects. They also note some drooling when she is eating. In addition, the parents have noticed that she has been stumbling more frequently when she runs. Prior to these symptoms, the patient was entirely well. She denies any headaches, nausea, or vomiting. On examination, the patient has a partial right 6th nerve palsy and gait dysmetria. Her strength is normal and she does not have papilledema. The sensory examination is normal. The lower-extremity reflexes are brisk but she does not have clonus. Questions
1. Based on the clinical picture, where is the lesion localized? 2. Does the relative paucity of clinical features imply limited CNS involvement? 3. What is the preferred initial diagnostic modality?
Oral Boards Review—Diagnostic Pearls
1. The development of rapidly progressive cranial neuropathies in a child 5– 15 years of age is the most common clinical pattern at presentation of a diffuse brainstem glioma. Ataxia and weakness can occur early but are generally not severe. 2. Despite the extent of involvement that is demonstrated by imaging studies, brainstem glioma patients are usually awake, alert and not in significant distress. 3. Obstructive hydrocephalus is not common at presentation. 4. Brainstem gliomas, unlike primary tumors in other brain locations, tend to demonstrate a pathologic-anatomic correlation. Midbrain (tectal) gliomas are typically low grade and rarely require treatment. Pontine gliomas are usually diffuse, unresectable, and are World Health Organization (WHO) grade IV. Cervicomedullary gliomas are usually WHO grade I and many can be treated successfully with surgery.
217
8 1 2
Pediatric Neurosurgery
Assessment and Planning
The presence of new and persisting cranial neuropathies in a child between the ages of 5 and 15 is concerning and the presence of a brainstem glioma should be considered. These patients typically lack symptoms of raised intracranial pressure, unless there is a coincident hydrocephalus, which is less frequent at diagnosis.The differential diagnosis includes other entities such as demyelinating disorders, ocular masses (if diplopia is the only finding), or rarely infectious causes. The initial imaging study should be a high-quality diagnostic MR scan with and without contrast. Brainstem gliomas can arise in the medulla, pons and midbrain. Although there is some overlap, tumors arising in the medulla and midbrain tend to be lower grade.Well-defined tumors of the medulla are usually pilocytic astrocytomas and, depending on their exact location, can be surgically removed. Common tumors of the midbrain arise in the tectum, are well-defined, and paradoxically can remain indolent for long periods. These tumors do usually present with hydrocephalus related to direct obstruction of the aqueduct of Sylvius, and initial treatment is usually restricted to endoscopic third ventriculostomy (ETV) or placement of a cerebrospinal fluid (CSF) shunt. Unfortunately, 80% of brainstem tumors fall into the category of diffuse intrinsic pontine gliomas (DIPG). These tumors do not displace normal structures but rather infiltrate the normal brainstem causing relatively minor symptoms compared to the volume of tissue involved. The typical appearance on MR imaging is that of a large mass involving usually the entire pons (Figure 24.1). The pons is expanded, often enough to surround the basilar artery. The tumor is usually bright on T2-weighted sequences but can have focal areas of enhancement and necrosis. There can be extension of the imaging abnormality into the cerebellar peduncles and rostrally into the midbrain and diencephalon.
Figure 24.1. A sagittal FLAIR MR image from a child with a typical DIPG. The entire pons between the midbrain and medulla is involved.
218
Diffuse Brainstem Glioma
In the latest WHO classification of brain tumors, DIPGs fall into a larger group of midline gliomas (diencephalon, brainstem and spinal cord), the majority of which have a unique mutation in one of the histone genes. The most common is a methionine-to- lysine alteration in the histone 3.3 gene. Decision Making
For lesions with a typical imaging appearance, surgical biopsy is usually not required and treatment is generally initiated with focal, fractionated, external beam radiotherapy, sometimes in conjunction with adjuvant chemotherapy. Steroids are often used to manage tumor-associated edema, but due to its associated complications, the trend has been to try to wean steroids early in the course, reserving additional use for the time of tumor progression. Despite this approach, treatment outcome remains dismal with less than 5% survival 2 years following diagnosis. For patients who present with hydrocephalus, treatment can begin with ETV, although if the pons is expanded, the basilar artery will be displaced anteriorly increasing the risk complications. In general, placement of a ventriculoperitoneal (VP) shunt is usually favored. Other rare tumors that can arise in the brainstem include primitive neuroectodermal tumor, atypical teratoid-rhabdoid tumor, lymphoma, ganglioglioma, and oligodendroglioma. If the lesion is atypical in appearance, or if another tumor type is suspected, then a tissue diagnosis should be obtained. Usually this can be accomplished with a stereotactic biopsy. Rarely, hemangioblastomas can present in association with von Hippel-Lindau disease. If this diagnosis is suspected, stereotactic biopsy is strongly contra-indicated due to the risk of life-threatening brainstem hemorrhage that could occur. Surgical Procedure
Diffusetumorsoftheponscannotberesectedsurgicallywithoutunacceptablemorbidity. Indicationsforsurgeryincludesuspicionofanalternativediagnosis,anintratumoralcyst, hydrocephalus, or obtaining tissue as a prerequisite to participation in a clinical trial. When the pons the diffusely involved, the goal of stereotactic biopsy is to obtain diagnostic tissue without injury to functional pathways. If the tumor extends posteriorly toward the middle cerebellar peduncle, then access to the posterior boundary is straightforward through a trans-cerebellar route, arising from a burr hole inferior to the transverse sinus. Adjuncts such as diffusion tensor imaging (DTI) and pathway mapping can help select a trajectory that avoids major descending tracts. In general, the ventral half of the pons should be avoided as a surgical target (Figure 24.2). An alternate approachisthroughthefrontallobe,traversingthediencephalonandupperbrainstem.The disadvantage of this route is its length and passage through many functionally eloquent regions. The varied and complex mutation spectrums found in diffuse brainstem gliomas have shown their uniqueness in comparison with other high-grade gliomas. This spectrum of mutations has provided opportunities for therapeutic trials, especially with the advent of new medications targeting receptor kinase domains. The tumorigenesis of DIPG and specific oncogenic mutations are still undergoing detailed study to provide improved therapeutic targets for this highly morbid disease.
219
0 2
Pediatric Neurosurgery
Figure 24.2. A screen capture from a neuronavigation system demonstrating a stereotactic biopsy of a DIPG. The motor pathways (red) were identified using pre-operative diffusion tensor imaging (DTI). In rare cases, there may be a bulky component to the tumor that has an exophytic or accessible component that may be partially resected through an open craniotomy.This option should be carefully considered in terms of the potential morbidity and whether it affects the patient’s outcome favorably. Finally, there are new clinical trials for patients with DIPGs that are evaluating the safety and efficacy of convection-enhanced delivery of therapeutic agents using catheters surgically placed directly into the tumor.
Oral Boards Review—Management Pearls
1. Surgical resection of a true intrinsic glioma that expands the pons is not indicated. 2. Biopsy is indicated for those tumors that are atypical in imaging appearance, or for those tumors where tissue is required for participation in a clinical trial. 3. Infrequently, tumors can be exophytic into the fourth ventricle or cerebello- pontine angle and are amenable to surgical resection.
220
Diffuse Brainstem Glioma
Pivot Points
1. An early decision should be made regarding biopsy, since it will affect the start of standard therapy, which consists of fully fractionated external beam radiotherapy (55–60 Gy total dose). 2. Patients should be monitored during their disease course for the development of hydrocephalus which should be treated promptly.
Aftercare
For the neurosurgeon, the therapeutic options are limited during the disease course. In an experimental setting, stereotactic biopsy allows analysis of tumor tissue. Although a minority of patient present with hydrocephalus, CSF diversion is often required because of disease progression.This can frequently have a positive effect on a patient’s quality of life. Finally, in the rare circumstance when a large tumor-associated cyst is present, surgical drainage can provide symptomatic relief. Complications and Management
The main associated problem that children develop is obstructive hydrocephalus secondary to the posterior fossa mass. Although focal masses obstructing the CSF pathways can be treated with an ETV, the expansile nature of DIPGs results in displacement of the basilar artery forward and obliteration of the pre-pontine cistern. An ETV should be considered carefully since the risks will be higher, and the likelihood of success lower. In general, placement of a standard VP shunt will provide symptomatic relief. For stereotactic biopsy of lesions in the pons, the objective is usually to avoid major long tracts. However, worsening of cranial neuropathies and focal weakness or sensory changes can occur in 10–20% of patients following biopsy. The most serious complication is hemorrhage resulting from the biopsy itself. Small hemorrhages along the biopsy track or at the biopsy site are commonly noted. Larger hemorrhages can cause permanent neurologic deficits or death. The incidence of these more serious consequences is approximately 1–3%.
Oral Boards Review—Complications Pearls
1. Due to constriction of the pre-ponting cistern by tumor, the late occurrence of hydrocephalus may be better treated with placement of a ventriculoperitoneal shunt than by endoscopic third ventriculostomy. 2. Hemorrhage at the time of stereotactic tumor biopsy is rare, but can be devastating or fatal. Careful trajectory planning will reduce but not eliminate this risk.
221
2
Pediatric Neurosurgery
Evidence and Outcomes
Aside from conventional fractionated radiotherapy, which can be considered as a palliative therapy, no other treatment has been shown to affect outcome. It is believed that the distinct genetic features of DIPG have contributed to the lack of success with agents developed first for other tumor types. Furthermore, the blood brain barrier is perceived as an obstacle for drug delivery contributing to the lack of chemotherapeutic effect. As mentioned above, new approaches, such as convection enhanced delivery are being tested in an effort to achieve higher local drug levels while limiting systemic toxicity. References and Further Reading
Barkovich AJ, Krischer J, Kun LE, Packer R, Zimmerman RA, Freeman CR, et al. Brain stem gliomas: a classification system based on magnetic resonance imaging. Pediatric Neurosurg 16:73–83, 1990. Cage TA, Samagh SP, Mueller S, Nicolaides T, Haas-Kogan D, Prados M, et al. Feasibility, safety, and indications for surgical biopsy of intrinsic brainstem tumors in children. Childs Nerv Sys 29:1313–1319, 2013. Fangusaro J. Pediatric high-grade gliomas and diffuse intrinsic pontine gliomas. J Child Neurol 24:1409–1417, 2009. Gupta N, Goumnerova LC, Manley P, et al. Prospective feasibility and safety assessment of surgical biopsy for patients with newly diagnosed diffuse intrinsic pontine glioma. Neuro Oncol 2018 (epub ahead of print) Jones C, Baker SJ. Unique genetic and epigenetic mechanisms driving paediatric diffuse high- grade glioma. Nat Rev Cancer 14, 2014. Kebudi R, Cakir FB. Management of diffuse pontine gliomas in children: recent developments. Pediatric Drugs 15:351–362, 2013. Puget S, Beccaria K, Blauwblomme T, Roujeau T, James S, Grill J, Zerah M, Varlet P, Sainte-Rose C. Biopsy in a series of 130 pediatric diffuse intrinsic Pontine gliomas. Childs Nerv Syst 31: 1773–1780, 2015. Wu G, Diaz AK, Paugh BS, et al. St. Jude Children’s Research Hospital–Washington University Pediatric Cancer Genome Project.The genomic landscape of diffuse intrinsic pontine glioma and pediatric non-brainstem high-grade glioma. Nat Genet 46:444–450, 2014.
222
Posterior Fossa Ependymoma Frederick A. Boop and Jimmy Ming-Jung Chuang
25
Case Presentation
A 9-year-old male patient presented to clinic with complaints including headache, nausea, vomiting, balance disorder, and blurred vision for 1 month. On neurological examination, ataxia, nystagmus, and papilledema were noted. Altered tandem gait and left-sided dysmetria were noted. Romberg’s sign was positive, but there was no facial hypo-or hyperesthesia or hearing impairment. Muscle strength and limb tone were normal. No significant past medical history or family history were noted. Magnetic resonance imaging (MRI) revealed a posterior fossa tumor arising from the 4th ventricular floor and filling the ventricle (Figure 25.1). There was heterogenous enhancement and extension into cervical subarachnoid space via the foramen Magendie. Obstructive hydrocephalus was also noted. Questions
1. What is the likely diagnosis and differential diagnosis? 2. What is the best treatment plan? 3. What is the appropriate timing of surgical intervention?
Assessment and Planning
Only 33% of pediatric brain tumors are diagnosed within the 1st month after the onset of signs and symptoms. The most common initial complaints are headache, nausea/ vomiting,seizures,andbehavioralchanges.Theseearlysignsandsymptomsarenonspecific indications of elevated intracranial pressure (ICP). Most children with headache as the initial symptom of a brain tumor will show additional signs and symptoms within a relatively short period. Malignant tumors grow more rapidly with symptom progression occurring over weeks rather than months and may also cause weight loss and other constitutional symptoms. Benign tumors often exhibit a long history of ataxia and elevated ICP resulting from gradual obstructive hydrocephalus. Only a high degree of suspicion based on detailed clinical history and a targeted neurological examination leads to more accurate and timely diagnosis of brain tumor. Cranial computed tomography (CT) is typically the first-line imaging study obtained for children with symptoms of a brain tumor. A complete workup, however, requires
223
4 2
Pediatric Neurosurgery
Figure 25.1. Sagittal T1 contrast enhanced MRI imaging reveals a posterior fossa mass arising from the 4th ventricular floor with heterogenous enhancement and extension into cervical subarachnoid space via the foramen of Magendie.
high-quality craniospinal MRI. Although MR spectroscopy may suggest the relative probability of a benign or malignant tumor, there is currently no imaging modality that can accurately predict tumor histology. Pediatric infratentorial (posterior fossa) ependymomas are usually well-delineated masses that are hypointense on T1 and hyperintense on T2-weighted imaging, with heterogenous enhancement. They arise from the floor (60%), lateral aspect (30%), or roof (10%) of the 4th ventricle. The “plastic” growth of tumor into the posterior fossa subarachnoid spaces, particularly into cervical subarachnoid space via foramen of Magendie and cerebellopontine angles via the foramen of Luschka, is the radiological hallmark of this tumors. The differential diagnosis includes medulloblastoma, which generally has a more centrally located 4th ventricular mass without subarachnoid extension, and astrocytoma, which is typically an intrinsic cerebellar mass or cystic mural nodule. Although less common, choroid plexus papilloma and carcinoma may also mimic ependymoma, but are less likely to have plastic extension into the subarachnoid space, and are often more uniformly and brightly enhancing. Decision Making
Because this patient presented with obstructive hydrocephalus and symptoms of raised ICP, he was admitted to the intensive care unit and begun on intravenous steroids. With steroid therapy, in most cases surgery can be performed on an urgent but not emergent basis, and few children require emergent ventricular drainage. Because of the risk of upward herniation with ventricular drainage, posterior fossa surgery for tumor removal should follow ventricular drain placement as soon as possible. Thegoalofsurgeryistotalremovaloftheependymoma,whichsignificantly improves prognosis, with resolution of the obstructive hydrocephalus. Most children with posterior fossa tumors do not require permanent ventricular shunting.
224
Posterior Fossa Ependymoma
Oral Boards Review—Diagnostic Pearls
1. Differential diagnosis for a single posterior fossa lesion in a pediatric patient includes a. Medulloblastoma (more common in childhood, usually arise from the vermis and grow rapidly) b. Juvenile pilocytic astrocytoma (majority present as a large cyst with an enhancing mural nodule). c. Hemangioblastoma (occur both sporadically and in patients with von Hippel Lindau). d. Others include atypical teratoid/rhabdoid tumor, papilloma, teratoma, and glioma. 2. Ependymoma typically arise from the floor or walls of fourth ventricle. Nausea and vomiting as a result of irritation of the area postrema near the obex is often an initial symptom.
Questions
1. What is the appropriate surgical approach? 2. What is the appropriate surgical positioning? 3. What are the necessary steps to obtain a complete resection? 4. What are the options for and value of intraoperative monitoring?
Surgical Procedure
For cases with significant ventriculomegaly, many surgeons place a frontal ventricular drain immediately before turning the patient prone, in order to drain CSF and relax the brain prior to posterior fossa dural opening. To prevent uncontrolled pressure shifts or upward herniation, CSF is usually drained during the craniotomy in controlled fashion by the anesthesiologist, on the instructions of the neurosurgical team. The safest and most direct approach to the fourth ventricle is the midline suboccipital approach. The skin incision begins midline and can curve toward the side with the predominant cerebellopontine angle invasion, at the level of the nuchal crest. This allows bony removal in the midline and extending to the sigmoid sinus on the more affected side. The superior and lateral limits of the craniotomy are the transverse and sigmoid sinuses. Inferiorly, the craniotomy should always include the posterior edge of the foramen magnum. C1 laminectomy is helpful for lesions that herniate through the foramen magnum and is almost always necessary. Always keep in mind that extending a laminectomy to or below C2 in pediatric patients will increase the risk of swan neck deformity. Techniques for intradural exposure and tumor resection depend on the location and size of the tumor. The arachnoid is opened over the cisterna magna to allow drainage of CSF. Gentle separation of the cerebellar tonsils will expose the cerebellomedullary fissure through the opened vallecula giving an unimpeded view of the inferior roof of
225
6 2
Pediatric Neurosurgery
the fourth ventricle. It is important to identify each posterior inferior cerebellar artery (PICA) as it often tethered to the tonsils and the walls of the cerebellomedullary fissure. PICA branches give the main blood supply to vermian tumors and can be ligated early as surgeons approach to the tumor, taking care not to damage or cause vasospasm of the parent vessel. Ependymomas, by definition, take origin from the ependymal lining of the ventricle floor. Those arising from the floor of the fourth ventricle derive blood supply from multiple small perforating vessels arising from the brainstem. If the surgeon avulses these vessels it may cause them to retract and bleed in the brainstem, leading to additional damage. They must therefore be meticulously coagulated and cut. A variant of the ependymoma arises from ependymal rests at the lateral margin of the foramen of Luschka and grows out the foramen into the cerebellopontine angle.These tumors often encase the lower cranial nerves as well as the vertebra-basilar complex, and may invade the side of the pons. Sometimes it is necessary to do a secondary retromastoid approach to completely resect these tumors. Intraoperative monitoring may be helpful if there is danger of violating the brain stem or cranial nerves during posterior fossa surgery. The common option for direct monitoring of brainstem function is brainstem auditory-evoked potentials (BAEP).This produces five waves that correspond to the proximal cochlear nerve, distal cochlear nerve, cochlear nucleus, superior olivary complex, and lateral lemniscus/inferior colliculus in response to auditory stimulation. Evidence of pontomesencephalic transmission of the impulses implies that the brain stem has not been compromised. Another monitoringtechnique,somatosensoryevokedpotentials(SSEP),followssensorysignals through the medial lemniscus, tracing a more medial brainstem pathway. Due to its distance from the floor of the fourth ventricle, SSEP is less sensitive to changes associated with ependymoma resection than BAEP. Mapping with direct stimulation of the facial nerve or facial nucleus (at the 4th ventricular floor landmark, the facial colliculus) can be used to confirm the integrity of these cranial nerve fibers or to identify relatively safer entry zones for the brainstem.
Oral Boards Review—Management Pearls
1. There are three possibilities for positioning: prone, lateral decubitus, or sitting. a. Prone position, or concorde position (prone with neck flexed), affords many ergonometric advantages such as better visualization, better exposure, and greater surgeon comfort. The disadvantage of the prone positioning is venous congestion that can lead to more blood loss and soft tissue swelling of the face. This can be improved by elevating the head above the level of the heart. b. The lateral decubitus position allows superior visualization of the lateral recess and cerebellopontine angle.The disadvantage of the lateral position is that the anatomy is not centered, so the surgeon must visualize all anatomical structures as rotated. c. The sitting position offers a clear operative field since blood and cerebrospinal fluid drain out of the operative site. Some studies also showed better
226
Posterior Fossa Ependymoma
lower cranial nerve preservation. However, there are additional risks associated with cardiovascular instability, hypotension and venous air embolism. Because of these risks, this position is rarely used in children. 2. For the children older than 2, a pin head holder is appropriate. For those younger than 2, a horseshoe headrest without pin fixation is preferred. The risk of pressure sores on malar imminence requires careful attention and the use of multiple layers of gel and foam padding. 3. For infratentorial ependymoma, gross total resection (GTR) is sometimes challenging due to tumor adherence to three critical structures: the floor of 4th ventricle, the cerebellar peduncles, and middle to lower cranial nerves. Nevertheless, GTR is extremely important to the ultimate prognosis. It is important to mention that intraoperative monitoring tends to cause the surgeon to leave more tumor behind. Recognizing that the most important predictor of survival in pediatric posterior fossa ependymoma is gross or near total resection, the neurosurgeon must rely on intraoperative monitoring to modulate risk but not preclude an attempt at total resection.
Aftercare
Sub-occipital craniotomy for near-total excision of the tumor was performed. Pathology confirmed ependymoma (WHO grade II). Postoperatively, the patient was awake and followed commands. Over the next few days, she was noted to be irritable, mute, and unable sit up. Postoperative MR imaging showed no evidence of residual tumor. Her mutism improved significantly by 1 month with continuing speech therapy and occupational therapy. Questions
1. What is the prognosis of cerebellar mutism syndrome? 2. What adjuvant therapy is recommended for posterior fossa ependymoma? 3. What is the prognosis of this tumor?
Complications and Management
The most common postoperative complication of 4th ventricular ependymoma resection, seen in approximately one-fourth of patients, is posterior fossa syndrome, also referred to as cerebellar mutism or pseudobulbar palsy.This syndrome is characterized by a delayed onset of mutism, emotional lability, and dystonia that occurs 12 to 72 hours following resection of a posterior fossa tumor. The cause of the syndrome is poorly understood. The outcome of posterior fossa syndrome is variable. Recovery typically occurs at a mean of 8.3 weeks; however, a residual ataxic dysarthria is common. Indeed, speech impairments were present in 95% of patients with moderate or severe mutism 1 year postoperatively.There are no reliable strategies for either the prevention or treatment of posterior fossa syndrome, although care to avoid damage to the 4th ventricular
227
8 2
Pediatric Neurosurgery
floor and/or deep cerebellar nuclei and vermis may lessen the risk of its occurrence. Neuropsychiatric deficits in patients with posterior fossa syndrome suggest that multidisciplinary rehabilitation is required in these patients. The current standard of care for children with ependymoma consists of a gross total resection with subsequent focal radiotherapy. In trial of pediatric ependymoma, gross total resection or near-total resection doubles the 5-year survival compared with lesser resection. After a GTR or NTR in pediatric patient with ependymoma, there is a consensus that radiation may be limited to the local tumor field. But the optimal dose and method of delivery remain controversial. About 5% of patients with ependymoma will present with evidence of leptomeningeal dissemination at the time of diagnosis as determined by a whole spine MRI with contrast and CSF sampling. Craniospinal radiation is generally reserved for these patients with neuraxis dissemination at presentation.
Oral Boards Review—Complications Pearls
1. Hydrocephalus: Only about 10% to 20% of patients with cerebellar and posterior fossa tumors require permanent shunting. 2. Posterior fossa syndrome: Delayed onset of mutism, emotional lability, and dystonia that occurs 12 to 72 hours following resection of a posterior fossa tumor. 3. Vascular injury: The most likely artery to be injured is PICA. Most patients with PICA injury present with postoperative flocculonodular lobe dysfunction causing nausea, vomiting, nystagmus, vertigo, and inability to stand or walk without appendicular dysmetria. 4. Postoperative pseudomeningoceles: Occur in 15% to 28% incidence rate. Normally, these small CSF collections are self-limited. Occasionally they can enlarge putting the closure under tension and may eventually produce a CSF leak, which carries a risk of meningitis. Pseudomeningoceles may be a manifestation of hydrocephalus and in some cases may require a permanent CSF diversion to resolve. 5. Cranial VI and/or VII palsy (“floor of the fourth ventricle syndrome”): Related deficits are usually immediately evident in the recovery room. The most common deficit is cranial VI and VII palsy caused by disruption of the nerve fibers coursing under the fourth ventricular floor at the facial colliculus where intra-pontine facial nerve fibers loop around the abducens nucleus. Damage in this area, often related to tumor invasion, results in ipsilateral facial and abducens palsy with contralateral hemiparesis. 6. Low cranial nerve palsy: Cranial nerve XII palsy can occur from injury to the hypoglossal trigone. Children with cerebellopontine angle ependymomas, in which the tumor invades the inferior floor of the fourth ventricle or involves the lower cranial nerves, should be carefully observed post-operatively for aspiration pneumonitis. This is a very serious complication that can severely limit recovery and occasionally prove life threatening. For those with vocal cord paralysis or insensate pharynges, tracheostomy and gastrostomy are generally indicated on at least a temporary basis.
228
Posterior Fossa Ependymoma
7. Skewed ocular deviation: This usually occurs with damage to the region of the cerebral aqueduct. This condition usually resolves within weeks after surgery and should be followed in cooperation with a pediatric ophthalmologist.
Pivot Points
1. The current standard of care for children with ependymoma consists of a gross total resection with subsequent focal radiotherapy. Chemotherapy, to date, has not been shown to be of particular value. 2. The single most important determinant of outcome in pediatric ependymoma is the extent of resection. 3. Careful perioperative planning and inspection of detailed imaging studies and neurological findings as well as meticulous microsurgical dissection can reduce but not eliminate the risk of neurological complications.
Evidence and Outcomes
The 5-year and 10-year event-free survival (EFS), progression-free survival (PFS), and overall survival (OS) for pediatric posterior fossa ependymoma have steadily increased over the decades. A recent long-term study showed 5-year and 10-year EFS/OS to be 74% /85% and 69% /75%. Recurrent ependymoma, which is most often local and almost always within 5 years of initial diagnosis, carries with it a poor prognosis. The 2-year survival rate for these patient ranges from 20 to 49%. The two most important prognostic factors for ependymoma are the extent of disease at diagnosis and the proportion of tumor resected at the time of initial surgery. Recent evidence suggests that midline ependymomas and cerebellopontine angle ependymomas are two distinctly different tumors. Integrated genomic approaches have clearly shown the existence of the distinct molecular variants of posterior fossa ependymoma as Type A and Type B (Figure 25.2). Type A ependymoma occurs
Taylor Type A Ependymoma
Taylor Type B Ependymoma
Figure 25.2. Taylor type A (left) and B (right) ependymomas. 229
0 3 2
Pediatric Neurosurgery
primarily in infants and young children and frequently follows a lateral distribution. Type A ependymomas carry a poorer prognosis with a higher likelihood of recurrence, metastases, and death compared with midline, or type B, tumors. Survival rates are particularly poor for subtotally resected type A ependymoma, even with adjuvant radiation therapy. Patients with type B ependymoma who undergo gross total resection are at lower risk for relapse. References and Further Reading
Pollack IF, Gerszten PC, Martinez AJ, et al. Intracranial ependymomas of childhood: long-term outcomeandprognosticfactors.Neurosurgery.1995Oct;37(4):655–666;discussion666–667. Figarella-Branger D, Civatte M, Bouvier-Labit C, et al. Prognostic factors in intracranial ependymomas in children. J Neurosurg. 2000 Oct;93(4):605–613. Tihan T, Zhou T, Holmes E, et al. The prognostic value of histological grading of posterior fossa ependymomas in children: a Children’s Oncology Group study and a review of prognostic factors. Mod Pathol. 2008 Feb;21(2):165–177. Epub 2007 Dec 14. Johnson RA, Wright KD, Poppleton H, et al. Cross-species genomics matches driver mutations and cell compartments to model ependymoma. Nature. 2010 Jul 29;466(7306):632–636. Taylor MD, Poppleton H, Fuller C et al. Radial glia cells are candidate stem cells of ependymoma. Cancer Cell. 2005 Oct;8(4):323–335. Merchant TE, Mulhern RK, Krasin MJ, et al. Preliminary results from a phase II trial of conformal radiation therapy and evaluation of radiation-related CNS effects for pediatric patients with localized ependymoma. J Clin Oncol 2004;22: 3156–3162 Merchant TE, Boop FA, Kun LE, Sanford RA. A retrospective study of surgery and reirradiation for recurrent ependymoma. Int J Radiat Oncol Biol Phys. 2008 May 1;71(1):87–97. Siffert J, Poussaint TY, Goumnerova LC et al. Neurological dysfunction associated with postoperative cerebellar mutism. J Neurooncol 2000; 48: 75–81 Rath GP, Bithal PK, Chaturvedi A, et al. Complications related to positioning in posterior fossa craniectomy. J Clin Neurosci. 2007 Jun;14(6):520–525.
230
Middle Fossa Arachnoid Cyst Amy K. Bruzek and Cormac O. Maher
26
Case Presentation
A previously healthy 16-month-old female presented with decline in language function. She previously had been using 2 or 3 words together; however, over the past 3 to 4 months, she had stopped using more than 1 word. Additionally, her head circumference had crossed multiple percentiles and exceeded the 99th percentile at presentation (50.2 cm). Her mother reported that the child occasionally hit her head with her hand as if she was in pain. She was otherwise developing normally. She had no papilledema. Her neurological examination was normal and her behavior was appropriate for her age. There was no past medical history other than a single ear infection, and no relevant family history. The patient lived at home with her mother and an older sibling. Questions
1. What should be included in the differential diagnosis? 2. What is the etiology of arachnoid cysts? 3. How do arachnoid cysts commonly present? 4. What is the most common location for an arachnoid cyst? 5. How are arachnoid cysts classified?
Assessment and Planning
Brain MRI showed a cystic lesion that was homogeneously hypointense onT1-weighted and hyperintense onT2-weighted imaging (Figure 26.1).There were no associated solid or enhancing components. The imaging features of arachnoid cysts are very characteristic and, in general, the diagnosis can be made accurately on the basis of MRI alone. Other cysts that have a lining of non-neural epithelium that secrete material other than CSF include colloid cysts, craniopharyngiomas, Rathke’s cleft cysts, epidermoid cysts, and dermoid cysts. These are usually easy to differentiate from arachnoid cysts on imaging. One must rarely consider other etiologies such as porencephalic cysts under the right clinical setting. When differentiating cysts on imaging, understanding the fluid content of different cysts is helpful. Arachnoid cysts contain CSF and therefore will appear water density on CT, hypointense on T1-weighted MRIs, and hyperintense on T2-weighted MRIs. Arachnoid cysts do not contrast-enhance or restrict diffusion. Cysts with non- neural epithelium will contain fluid composed of mucin, cholesterol crystals, calcium,
231
2 3
Pediatric Neurosurgery
Figure 26.1. Preoperative brain MRI. (A) T1-weighted post-contrast axial MRI showing a right middle fossa cyst compressing the brainstem medially. (B) T1- weighted post-contrast coronal MRI showing a right middle fossa cyst compressing the brain medially. (C) T2-weighted axial MRI demonstrating the arachnoid cyst.
keratin, or lipid. These other cyst types will usually be isodense or hyperdense on CT, and hyperintense on T1-weighted and T2-weighted MRIs. The etiology of arachnoid cysts is not known with certainty. While many are congenital, there are examples of de novo arachnoid cyst formation.These are benign developmental cysts that may occur in any location in the neuraxis adjacent to an arachnoid membrane.Themostlikelypathophysiologicalexplanationforarachnoidcystformation is a small tear in the arachnoid leading to a space within a division of the membrane. Histological studies of arachnoid cysts have revealed that cyst walls contain hyperplastic arachnoid cells and an absence of traversing trabecular processes. The increasing use of diagnostic imaging has led to more frequent diagnosis of arachnoid cysts. In the United States, most arachnoid cysts are found incidentally, although neurological signs and symptoms will occasionally lead to the diagnosis. The prevalence of arachnoid cysts in children is probably in the range of 2–3%. Arachnoid cysts are approximately twice as common in boys compared to girls. The middle fossa is the most common location for arachnoid cysts with approximately 47%–55% of all arachnoid cysts occurring in this location. The second most common location is a posterior fossaorretrocerebellarlocation.Forunknownreasons,left-sidedarachnoidcystsappear to be more common than right-sided or midline cysts, even when considering only asymptomatic cases. In1982,Galassiet al.publishedaclassificationsystemformiddlefossaarachnoid cysts based on cyst size and extent of surrounding brain displacement. Some surgeons continue to classify cysts according to this system, although its clinical usefulness is not clear. GalassitypeI middlefossaarachnoidcystsaresmall,spindle-shapedcyststhatarelimited to the anterior middle fossa posterior to the sphenoid ridge. Type II cysts are larger than type I, triangular or rectangular in shape, and are located superiorly along the anterior and middle parts of the sylvian fissure. Arachnoid cysts that are large, ovoid, or elliptical in shape, and fill the entire middle cranial fossa are classified as type III arachnoid cysts. In infants, type III cysts will cause macrocephaly. The cyst harbored by the patient in our case presentation is an example of a Galassi type III arachnoid cyst.
232
Middle Fossa Arachnoid Cyst
Oral Boards Review—Diagnostic Pearls
1. The differential diagnosis includes CSF-content cysts and non-neuroepithelial cysts. a. CSF-content cysts include arachnoid cysts, leptomeningeal cysts, post- surgical cysts, porencephalic cysts, and neuroepithelial cysts. b. Non-neuroepithelial cysts include colloid cysts, craniopharyngiomas, Rathke’s cleft cysts, epidermoid cysts, and dermoid cysts. 2. The most likely pathophysiological explanation for arachnoid cysts is a developmental anomaly splitting the meningeal membranes. 3. On imaging, arachnoid cyst contents will follow CSF signal on both CT and MRI. 4. Arachnoid cysts are more common in boys than girls.
Questions
1. When should arachnoid cysts be treated? 2. What are some preoperative considerations? 3. What surgical or nonsurgical options are available?
Decision Making
The vast majority of patients with an intracranial arachnoid cyst should be managed without surgery. The natural history of asymptomatic arachnoid cysts is excellent. Clinically significant arachnoid cyst growth is rarely seen after 4 years of age. There is no reason to consider“prophylactic”surgery to repair an asymptomatic arachnoid cyst (Figure 26.2). Headache, which is common in the general population, is also common in
Figure 26.2. T2-weighted axial MRI demonstrating a typical non-operative middle fossa arachnoid cyst. 233
4 3 2
Pediatric Neurosurgery
patients with arachnoid cysts.We believe that clinicians should exercise extreme caution when attempting to attribute non-specific symptoms such as headache to the presence of an arachnoid cyst. Cysts may occasionally compress a narrow CSF pathway such as the cerebral aqueduct or the foramen of Monro. The suprasellar location is especially likely to obstruct CSF pathways, and surgery is indicated when such obstruction occurs. Intracranialarachnoidcystsmayoccasionallycausecranialdeformitiesorincreasedhead size/macrocephaly, especially in infants. Progressive macrocephaly in an infant with a very large middle fossa arachnoid cyst, as seen in the case example, is currently the most frequent indication for surgical treatment of an arachnoid cyst in our practice. Posterior fossa arachnoid cysts are usually non-symptomatic and should almost never be treated. The lining of an arachnoid cyst may occasionally tear following a traumatic injury (Figure 26.3). When the tear communicates the cyst with the subdural space, a subdural hygroma results. Management of subdural hygromas resulting from a tear in a cyst lining is controversial. These patients will often present with symptoms of raised intracranial pressure including headaches and nausea. Third nerve palsies and even papilledema are occasionally seen. In general, all symptoms resolve over the course of a few weeks without surgical treatment. We currently reserve surgical treatment for only the most refractory patients. Occasionally, a traumatic tear of the arachnoid cyst lining will lead
Figure 26.3. (A) T2-weighted MRI of a right-sided middle fossa arachnoid cyst with hygroma. (B) The hygroma resolved several months later; however, the arachnoid cyst persists.
234
Middle Fossa Arachnoid Cyst
Figure 26.4. Additional example of a self-resolving hygroma associated with an arachnoid cyst. (A) Right middle fossa arachnoid cyst with hygroma. (B) Follow-up MRI several months later demonstrates the resolved hygroma and decreased size of arachnoid cyst.
to an “auto-fenestration” phenomenon, where the cyst will be seen to spontaneously resolve over the months following the initial tear (Figure 26.4). Ourpatientpresentedwithenlargingheadcircumferenceanddeclineinneurological function. Because of the large size of the cyst and regression in development possibly related to the cyst, the decision was made to pursue surgery. Due to the minimally invasive nature and possibility of definitive treatment, endoscopic fenestration was performed. Surgical Procedures
There are 3 surgical options for the management of middle fossa arachnoid cysts, each with unique risks and benefits. Craniotomy with fenestration allows the surgeon to clearly see cranial nerves and vessels, which increases safety, especially for those inexperienced with endoscopic techniques. In this approach, a small craniotomy to gain access to the middle fossa is performed, followed by fenestration of the outer cyst membrane andthentheinnercystmembrane,takingcaretopreservecranialnervesandvasculature. Fenestration of the inner membrane into the basal cisterns is very important to maximize the chance for a successful fenestration. The inner membrane fenestration opens
235
6 3 2
Pediatric Neurosurgery
the cyst space into a cisternal space that is more efficacious at draining excess CSF than the lateral space over the convexity. Iatrogenic subdural hygroma, or the accumulation of CSF in the subdural space lateral to the cyst, is a common complication of any fenestrationformiddlefossaarachnoidcyst.Ingeneral,aswithspontaneousorpost-traumatic subdural hygroma formation, most of these iatrogenic postoperative hygromas will resolve over a few weeks. Endoscopic fenestration, like craniotomy for fenestration, offers the opportunity for definitivetreatmentbutusinglessinvasivetechniques.Althoughendoscopiccystfenestration is not technically demanding in most cases, some training and experience with endoscopic techniques is required. As with craniotomy for fenestration, postoperative subduralhygromasmaybeseenbutinmostcasesshouldbemanagedwithoutadditional surgicalprocedures.Endoscopicfenestrationofarachnoidcystsisbeingperformed with increasing frequency for deep locations that are difficult to reach via direct surgery, such as the suprasellar or quadrigeminal cisterns, but may also be used for middle fossa arachnoid cysts. The use of an intraoperative navigation system may be helpful for planning an entry site, trajectory, and site of fenestration. Either a flexible or rigid endoscope may be used according to surgeon expertise and preference. Cystoperitoneal shunting carries the risk of shunt dependence and a lifelong risk of shunt failure or infection. It effectively reduces cyst size in infants who have significant macrocrania. In our own practice, we reserve shunt treatment for infants with massive macrocrania or cysts that have proven to be refractory to fenestration.
Oral Boards Review—Management Pearls
1. Middle fossa and retrocerebellar are the 2 most common arachnoid cyst locations. Most average-sized middle fossa or retrocerebellar arachnoid cysts should not be treated surgically. 2. We recommend surgical treatment for a. Infants with massive cysts and progressive macrocrania. b. Patients with suprasellar arachnoid cysts and obstruction of CSF pathways. c. Unusual cases where substantial cyst growth occurs or specific neurological signs are present. 3. Traumatic tears in the cyst lining may result in subdural hygroma formation. a. Subdural hygroma may be associated with increased intracranial pressure. b. Symptoms usually resolve over weeks with no treatment. c. Surgical treatment for patients with hygroma may be necessary for refractory or very severe elevations in intracranial pressure. 4. Iatrogenic hygroma formation may also be seen following fenestration of an arachnoid cyst.
Pivot Points
There are 3 surgical options for the management of middle fossa arachnoid cysts, each with unique risks and benefits.
236
Middle Fossa Arachnoid Cyst
1. Craniotomy with fenestration allows the surgeon to clearly see cranial nerves and vessels thereby increasing safety, especially for those inexperienced with endoscopic techniques. 2. Endoscopic fenestration is less invasive than craniotomy but requires some experience with endoscopic techniques and offers less ability to manipulate the lining compared with craniotomy. 3. Cystoperitoneal shunting carries the risk of shunt dependence and a lifelong risk of shunt failure. It effectively reduces cyst size in infants with significant macrocrania.
Aftercare
After surgery, patients should be closely monitored in a post-anesthesia care unit prior to being admitted to an intensive care unit (especially for craniotomy) or general care unit under neurosurgical care for close monitoring.Worsening of clinical status should raise concern for hemorrhage, and immediate head CT or MRI should be performed if the patient is clinically stable. Most patients are able to leave the hospital after 1 or 2 days. Complications and Management
Possible complications include subdural hygroma, subdural hematoma, pseudo meningocele, CSF leak, wound complications, subdural empyema, meningitis, cranial nervepalsy,spasticity,hemiparesis,hydrocephalus,seizure,ortheneedforrepeatsurgery. Surgical fenestration of a cyst’s outer lining, either from deliberate fenestration or from shuntplacement,willallowegressofcystfluid,sometimesunderpressure.Thismayresult in subdural hygroma if it is under the dura, or a pseudomeningocele if the dura is not watertight. In the most extreme cases, a CSF leak will occur, placing the patient at risk for further infectious complications. Occasionally the placement of a shunt is necessary forpersistentpressureproblemsfollowingfenestration.Sincemostofthepressure-related complicationswilleventuallyresolvewithoutshuntplacement,weattempttodelayshunt placement until there is clearly no alternative. After surgery, our patient had improvement in language function and overall was doing well neurologically. Follow-up visits withrepeatMRIshowedawell-decompressedarachnoidcystandaneurologicallystable examination.
Oral Boards Review—Complications Pearls
1. CSF complications may ensue after arachnoid cyst treatment, including hydrocephalus, subdural hygroma, or rarely CSF leak. 2. Risk of CSF complications may be reduced by meticulous primary closure. 3. Post-operative CSF hygromas typically resolve but may rarely require placement of a CSF shunt to alleviate persistent and serious symptoms.
237
8 3 2
Pediatric Neurosurgery
References and Further Reading
Go KG, Hew JM, Kamman RL, Molenaar WM, Pruim J, Blaauw EH. Cystic lesions of the brain. A classification based on pathogenesis, with consideration of histological and radiological features. Eur J Radiol 1993;17(2):69–84. Fernandez Molina G. Neuroendoscopic management of middle fossa arachnoid cysts. World Neurosurg 2013;79(2 Suppl):e19–23. Rengachary SS, Watanabe I. Ultrastructure and pathogenesis of intracranial arachnoid cysts. J Neuropathol Exp Neurol 1981;40(1):61–83. Starkman SP, Brown TC, Linell EA. Cerebral arachnoid cysts. J Neuropathol Exp Neurol 1958;17(3):484–500. Al-Holou WN, Yew AY, Boomsaad ZE, Garton HJ, Muraszko KM, Maher CO. Prevalence and natural history of arachnoid cysts in children. J Neurosurg Pediatr 2010;5(6):578–585. Galassi E, Gaist G, Giuliani G, Pozzati E. Arachnoid cysts of the middle cranial fossa: experience with 77 cases treated surgically. Acta Neurochir Suppl 1988;42:201–204. Galassi E, Tognetti F, Gaist G, Fagioli L, Frank F, Frank G. CT scan and metrizamide CT cisternography in arachnoid cysts of the middle cranial fossa: classification and pathophysiological aspects. Surg Neurol 1982;17(5):363–369. Maher CO, Goumnerova L. The effectiveness of ventriculocystocisternostomy for suprasellar arachnoid cysts. J Neurosurg Pediatr 2011;7(1):64–72. Maher CO, Garton HJ, Al-Holou WN, Trobe JD, Muraszko KM, Jackson EM. Management of subduralhygromasassociatedwitharachnoidcysts.JNeurosurgPediatr2013;12(5):434–443. Okano A, Ogiwara H. The effectiveness of microsurgical fenestration for middle fossa arachnoid cysts in children. Childs Nerv Syst 2016;32(1):153–158.
238
Posterior Fossa Cyst and Hydrocephalus Peter J. Morone and John C. Wellons, III
27
Case Presentation
A 3-month-old male was referred by their pediatrician for an abnormally large head. The child was born at full term with a normal delivery. At birth, the child’s occipital- frontal circumference was normal, his fontanel was flat and his sutures were not split. Over the following 3 months, however, his mother noted a rapid increase in the child’s head size and his pediatrician confirmed an increase in head circumference percentile. On neurological evaluation the child was noted to be awake and alert. His head circumference was 39 cm (97 percentile) with a full but soft fontanel, and his cranial sutures were splayed. His cranial nerves II–XII were grossly intact, and his arms and legs moved symmetrically with good strength. Routine magnetic resonance imaging (MRI) of the child’s brain demonstrated an enlarged and largely CSF-filled posterior fossa. Sagittal T2-weighted images demonstrated a posterior fossa cyst with severe hypoplasia of the cerebellar vermis, sparing only the most rostral portion (Figure 27.1). In addition, the lateral ventricles were massively enlarged, consistent with hydrocephalus. Questions
1. What is the differential diagnosis? 2. What is best imaging modality for making the diagnosis? 3. What is the appropriate timing of the diagnostic work-up?
Assessment and Planning
The differential diagnosis of posterior fossa fluid collections includes Dandy-Walker malformation, Blake’s pouch cyst, posterior fossa arachnoid cyst, and mega cisterna magna. A Dandy-Walker malformation is an anatomical triad characterized by a large posterior fossa, agenesis of the cerebellar vermis and dilation of the 4th ventricle. Additionally, 70– 90% of patients with a Dandy-Walker malformation have hydrocephalus secondary to obstruction of 4th ventricular outflow through the foramen of Luschka and Magendie. The presence of a small remnant of vermis would lead many experts to refer to this patient’s malformation as a “Dandy-Walker variant.” However, different references use an inexact threshold for the degree of vermian hypoplasia constituting a true Dandy- Walker Malformation. Even more concerning, in pediatric and even radiological practice, “Dandy-Walker variant” is commonly used to refer to a wide range of anatomical
239
0 4 2
Pediatric Neurosurgery
Figure 27.1. Sagittal T2-weighted MRI demonstrating an enlarged posterior fossa, inferior vermian hypoplasia and cystic dilation of the fourth ventricle. These findings are consistent with a Dandy-Walker malformation (with atypical sparing of a superior remnant of the vermis). Additionally, there is presence of hydrocephalus and corpus callosum agenesis.
findings, from functionally and prognostically true Dandy-Walker malformations (as in this case), to benign entities, such as mega cisterna magna. Unfortunately, pre-natal counseling and other care decisions may be inadvertently and seriously affected by this imprecision. In general, there is probably a reduced risk of other associated brain deformities and hydrocephalus proportional to the amount of vermis remaining. Although also characterized by enlarged posterior fossa CSF spaces, other cystic posteriorfossamalformationshaveverydifferentembryologyandcarrydifferentprognoses. “Mega cisterna magna”refers to a large posterior fossa secondary to an enlarged cisterna magna, with a normal cerebellar vermis and 4th ventricle without mass effect. This is usually a benign or normal variant condition. A Blake’s pouch cyst is a cystic structure originating within the roof of the 4th ventricle that herniates into the cisterna magna, resulting from a persistent Blake’s pouch during embryological development. The cerebellum, 4th ventricle and posterior fossa are normal. Posterior fossa arachnoid cysts generally displace both the cerebellum and 4th ventricle anteriorly or, if located predominantly in the cerebellopontine angle, antero- laterally. Generally, they are asymptomatic, but given their propensity to enlarge, they can occasionally exert mass-effect on surrounding structures and also cause obstructive hydrocephalus. Magnetic resonance imaging (MRI) is the best modality for accurately diagnosing enlarged posterior fossa CSF collections. Since 4th ventricular cysts in Dandy-Walker Malformation are filled with CSF or a fluid of similar density, the cysts mimic CSF on all sequences. They appear hypointense on T1-weighted images, hyperintense on T2- weighted images and do not demonstrate contrast enhancement.
240
Posterior Fossa Cyst and Hydrocephalus
In the current case, given the child’s stable neurologic examination, an MRI was obtained on a routine basis.
Oral Boards Review—Diagnostic Pearls
1. A Dandy-Walker malformation consists of the following triad: a large posterior fossa, agenesis of the cerebellar vermis, and cystic dilation of the 4th ventricle. 2. A Dandy-Walker malformation is associated with hydrocephalus 70–90% of the time. Hydrocephalus should be thought of as a sequelae of Dandy-Walker malformation and typically develops postnatally. 3. Brain MRI is the best diagnostic imaging modality to evaluate Dandy-Walker malformations and posterior fossa anatomy. Like CSF, the cystic 4th ventricle is hypointense on T1-weighted images, hyperintense on T2-weighted images and does not contrast enhance.
Questions
1. What are the surgical approaches used to treat posterior fossa cysts? 2. Which surgical techniques should be employed when hydrocephalus is present? 3. For the described patient, what is the most appropriate timing for operative intervention?
Decision Making
In general, asymptomatic patients with posterior fossa cysts do not require surgical intervention and can be monitored for cyst growth with serial MRI scans. However, if thepatientissymptomaticduetocystassociatedmass-effectorhydrocephalus,operative intervention is required. When hydrocephalus is absent, and symptoms are purely related to mass-effect, the cyst can be directly decompressed or shunted. Decompression can be accomplished via several techniques: stereotactic puncture, fenestration (either open or endoscopic) or cystoperitoneal shunt placement. Fenestration is growing in popularity as it allows the neurosurgeontovisualizeimportantsurroundinganatomywhileavoidingplacementof permanent shunt hardware. When performing cyst fenestration, the goal should be to achieve communication between the cyst, ventricular system and subarachnoid space. In the posterior fossa, this can often be accomplished by fenestrating the cyst into the quadrigeminalcisternorcisternamagna.Evenaftersuccessfulfenestration,however,the cyst may recur. In this setting, many surgeons may elect to place a cystoperitoneal shunt. No systematic, controlled data exist favoring any specific approach. Inthesettingofhydrocephalus,operativeinterventionshouldbeaddressedurgently or emergently if the symptoms warrant. Emergent placement of an external ventricular drain may be warranted if the patient presents with symptoms of high intracranial
241
2 4
Pediatric Neurosurgery
pressure such as drowsiness, bradycardia or respiratory depression and if emergent definitive surgery cannot take place. If the patient is neurologically stable, however, treatmentofhydrocephalusmaybeachievedwithplacementofaventriculoperitonealshunt, cystoperitoneal shunt, or endoscopic third ventriculostomy with or without choroid plexus cauterization (ETV +/– CPC). In the present case, a ventriculoperitoneal shunt was inserted. In general, if the ventricular system is relatively normal other than obstruction at the level of the posterior fossa, primary treatment may be directed at the posterior fossa cyst, with the strategy of secondarily relieving the obstructive hydrocephalus. If the entire ventricular system is dysmorphic (as in this patient), placement of a ventricular shunt, with or without fenestration of the posterior fossa cyst into the ventricular system, may be necessary.Occasionally,persistentclinicalproblemsandexpandingfluidcollections despite attempts at fenestration result in tandem shunting of the posterior fossa cyst and supratentorial ventricles, typically through a singleY-ed shunt valve in order to equalize pressures. This anatomical result, however, is difficult to manage and such children are prone to frequent CSF shunt malfunction and need for revision. Surgical Procedure
Surgical fenestration, shunting, or ETV with or without CPC require the patient to be intubated and placed under general anesthesia. Both ventricular and cyst shunts are placedutilizingstandardanatomicalreferences,withthedistalterminustypically placed in the peritoneal cavity. The step by step details of VP shunt placement and ETV are covered in other chapters. Lateral posterior fossa entry into the cyst should be accomplished using a retromastoid burr hole or midline entry via a suboccipital burr hole. In either case, the goal should be a parallel and not perpendicular trajectory of the proximal shunt catheter relative to the brainstem. For fenestration via a midline approach, the patient is placed in the prone position and pressure points are appropriately padded. For small children, the head can be safely positioned on a Mayfield horseshoe device. Older children may require cranial pin fixation. During head positioning, the chin should be slightly flexed and the head translated upward placing the child in a military tuck position. After positioning, it is important to ensure that the eyes are free of pressure. An incision is made and the suboccipital bone is exposed to the foramen magnum. As dissection is carried down to bone, it is important to stay within the avascular midline raphe and to leave a muscle cuff inferior to the inion to aid in watertight fascial closure. Sufficient tissue dissection has been completed once the suboccipital bone, and posterior aspect of the C1 arch have been exposed. It is important to leave the muscle attachments to the C2 lamina intact in order to maintain upper cervical stability. A more lateral approach into the CP angle utilizes a retromastoid approach. Minimal retraction of the cerebellum is necessary during these procedures. The use of neuronavigation assists with placement of a burr hole or small craniotomy in the suboccipital bone, being mindful of the midline sinuses and circular sinus as well as unexpected venous lacunae. It is critical to choose a trajectory that will allow access to the distal cistern into which the cyst is to be fenestrated. After the dura is coagulated and incised, the retractor blades or endoscope should be advanced into the cyst. Surgical
242
Posterior Fossa Cyst and Hydrocephalus
fenestration is completed when the surgeon feels that the cistern has been breached, therefore communicating cyst, ventricle, and subarachnoid space. In general, it is important to perform a water-tight dural closure. In the setting of a large dural opening we recommend harvesting a pericranial graft from the bone superior to the inion, and suturing this graft to the edges of the of dura. The wound should then be irrigated and closed in a standard fashion.
Oral Boards Review—Management Pearls
1. Not all patients with posterior fossa cysts require treatment. Indications for surgical intervention include symptomatic mass effect and/or hydrocephalus. 2. The goal of surgical treatment includes cyst decompression via shunting, or fenestration, and communication of the intracystic, subarachnoid, and ventricular spaces. 3. Fenestration via open or neuroendoscopic approach or placement of a cystoperitoneal shunt are viable options for treatment. If hydrocephalus is present, then consideration should be given to ETV-CPC or ventricular shunt placement.
Pivot Points
1. Patients with posterior fossa cysts that do not meet indication for surgical intervention may be followed with serial MR imaging to monitor for interval growth. 2. Patients with midline posterior fossa cysts presenting with associated hydrocephalus may be treated with placement of a ventriculoperitoneal or cystoperitoneal shunt, or with ETV +/–CPC. Of note, based upon current data, there is no additional benefit to CPC in children greater than 2 years old. 3. For patients with laterally located posterior fossa cysts presenting with associated hydrocephalus, surgical options include placement of a ventriculoperitoneal or cystoperitoneal shunt, ETV +/–CPC, and neuroendoscopic or open fenestration.
Aftercare
Post-operatively,patientsundergoingshuntplacementareadmittedtoaregularinpatient nursing unit with routine vital sign and neurological checks. Discharge home typically occurs the morning following surgery.Those who undergo craniotomy for fenestration may be admitted to the pediatric intensive care unit (ICU) for approximately 24 hours. Blood and chemistry counts are checked if indicated eight hours after surgery and the morning of post-operative day 1. Routine peri-operative antibiotics are given preoperatively and a single dose postoperatively. While in the ICU, patients are monitored with neurological checks every 1 hour. Upon transfer to the regular nursing unit, care
243
42
Pediatric Neurosurgery
continues as detailed for shunt placement. Once patients are eating and voiding without assistance, and are tolerating age appropriate activity, they can be discharged home. For pain control, patients are discharged with a prescription for acetaminophen and non- steroidal anti-inflammatory medications, but we generally avoid prescribing narcotics. For follow-up, patients are seen in clinic for an incision check within 2 weeks and are scheduled for a routine brain MRI at 6 weeks to evaluate changes in the size and conformation of the cyst and ventricular system. In the present case, the patient was doing well at his 2-month follow-up with a stable head circumference, a sunken fontanelle, and imaging demonstrating a reduction in the ventricles and a stable posterior fossa cyst. Complications and Management
Cystwallsareoftenadherenttoimportantvasculatureandcranialnerves,thereforethese structures may be at risk for damage during surgery. Injury to neurovascular structures can be avoided, however, by obtaining a solid understanding of the patient’s anatomy through meticulous review of the pre-operative images, and by ensuring complete visualization of the cyst wall with the microscope or neuroendoscope intraoperatively. Post-operative pseudomeningocele or CSF leak may occur after craniotomy for cyst fenestration and decompression if the dura is not closed in a water-tight manner. Often, primary closure of dura is difficult, especially after a suboccipital craniotomy. In this instance, we recommend harvesting a pericranial graft from the bone superior to the incision and incorporating this graft into the dural closure. If a patient develops a persistent pseudomeningocele or CSF leak, we believe that re-do repair of the duraplasty closure is indicated prior to CSF diversion. Therearemultiplereportsofmalpositionedproximalcystoperitonealshuntcatheters within the brainstem or cerebellum have been reported. This is most likely secondary to a non-parallel catheter trajectory as well as the cysts’ tendency to obscure normal surrounding anatomy. Thus, when placing a cystoperitoneal shunt it is paramount to directly visualize placement of the proximal catheter with a neuroendoscope or to use stereotactic navigation. The ideal approach orients the catheter parallel to the 4th ventricular floor, either from a lateral approach or via the 4th ventricular outlet. This avoids the tendency of the catheter to enter the brainstem once the cyst collapses.
Oral Boards Review—Complication Pearls
1. As the cyst wall may be adherent to essential vascular structures and cranial nerves, it is necessary to study all pre-operative imaging in detail prior to surgery. 2. If a persistent pseudomeningocele or CSF leak presents post-operatively, the patient should be taken to the operating room for direct repair of the leak as the initial rescue procedure.
244
Posterior Fossa Cyst and Hydrocephalus
Evidence and Outcomes
Posterior fossa cysts are rare, and there is no level I evidence regarding their treatment. Various surgical approaches and treatment modalities have been described by numerous case reports and case series, which are usually classified as level IV evidence. While these articles provide a useful clinical overview, their quantitative results should be interpreted with caution. References and Further Reading
Srinivasan U, Lawrence R. Posterior fossa arachnoid cysts in adults: Surgical strategy: Case series. Asian J Neurosurg. 2015;10:47. Huang J-H, Mei W-Z, Chen Y, Chen J-W, Lin Z-X. Analysis on clinical characteristics of intracranial Arachnoid Cysts in 488 pediatric cases. Int J Clin Exp Med. 2015; 8:18343–18350. Zandian A, Haffner M, Johnson J, Rozzelle CJ, Tubbs RS, Loukas M. Endoscopic third ventriculostomy with/without choroid plexus cauterization for hydrocephalus due to hemorrhage, infection, Dandy-Walker malformation, and neural tube defect: a meta-analysis. Childs Nerv Syst. 2014;30(4):571–578. Martínez-Lage JF, Pérez-Espejo MA, Almagro M-J, López-Guerrero AL. Hydrocephalus and arachnoid cysts. Childs Nerv Syst. 2011;27:1643–1652. Nakagawa Y, Pooh KH, Nishiyama I. [Dandy-Walker syndrome and Dandy-Walker variant]. Ryoikibetsu Shokogun Shirizu. 2000;28 (Pt 3):586–589.
245
6 4 2
Occipital Encephalocele Molly Hubbard and Daniel Guillaume
28
Case Presentation
A 36-year-old woman with 2 previous normal pregnancies presented to her obstetrician for a routine 12-week ultrasound, which revealed a large cystic structure arising from the posterior aspect of the fetus’s head (Figure 28.1A). Fetal magnetic resonance imaging (MRI; Figure 28.1B) confirmed a large occipital encephalocele with scant brain tissue insidethecysticstructure,herniationofcerebellartonsilsthroughtheforamenmagnum, and no hydrocephalus. Amniocentesis at 18 weeks revealed an alpha-fetoprotein (AFP) level of 4.8 multiples of the median (normal 0.5–2 multiples of the median) and an acetylcholinesterase (ACH) level of 9.54 m units/ml (normal < 4.5 m units/ml). At 36 weeks the woman underwent a cesarean section (C-section) due to oligohydramniosandenlargingencephaloceleonserialultrasounds.Apgarscoreswere5 and 9, 1 and 5 minutes after birth, respectively. Physical exam revealed a 6 x 7 cm occipital encephalocele with a small amount of clear fluid leaking of from a translucent area near the middle ofthelesionthatwasotherwiseskin-coveredwithsomeareasappearing more translucent than others. She was microcephalic with an occipital frontal circumference (OFC) of 27.5 cm. Her anterior fontanelle was soft and flat, sutures were not splayed, pupils were equal and reactive, and her face moved symmetrically with crying. She had no evidence of midline facial abnormalities. She had a small low-lying midline sacral dimple with no surrounding hyperpigmentation or tuft of hair. There were no other midline spinal or cranial neurocutaneous manifestations of dysraphism. She had moderate inward rotation of both feet. Both toes were up-going to plantar stimulation and she otherwise had symmetric voluntary movement of both upper and lower extremities. Questions
1. What is an encephalocele? 2. What is a Chiari III malformation? 3. What is the significance of elevated AFP and ACH levels? 4. What are other abnormalities to be aware of during the work-up? 5. Is there benefit to C-section over vaginal delivery? 6. What are the other common locations of encephaloceles? 7. What is the incidence of Chiari III malformation among all Chiari malformations?
247
8 4 2
Pediatric Neurosurgery
Figure 28.1. (A) Prenatal ultrasound demonstrating a large cystic structure arising from the posterior aspect of the head. (B) Fetal MRI confirming large occipital encephalocele with scant brain tissue. (C) Sagittal MRI of the infant’s brain, with brain tissue herniating into the cystic structure. (D) Sagittal MRI demonstrating the herniation of the cerebellum through the foramen magnum.
Assessment and Planning
Inafullphysicalexamitisimportanttonoteanyassociatedeyemovementabnormalities, includingtitubationanddownbeatnystagmus,respiratorycompromise,dysphagia,and risk for aspiration, as well as abnormalities in strength, sensation, or muscle tone. An MRI (Figures 28.1 C and D) was performed confirming the findings of the prenatal MRI and ultrasound, and a magnetic resonance venogram (MRV) showed no involvement of venous sinus structures within the encephalocele sac. Spinal MRI showed no additional abnormalities. Based on imaging characteristics and physical exam, the diagnosis of occipital encephalocele with Chiari III malformation was definitively made. Few other entities are included in this differential diagnosis. Loss of bone in the parietal and occipital region is also consistent with enlarged parietal foramina. Other etiologies of posterior cervical masses include epidermoid and dermoid cysts, cervical hydromyelocele, or
248
Occipital Encephalocele
thickened nuchal fold associated with Down syndrome. Epidermoid and dermoid cysts may also be associated with dermal sinus tracts and meningitis, or recurrent unexplained aseptic meningitis. However, in this case the physical exam and MRI findings are definitive for the diagnosis of encephalocele. An encephalocele, thought to result from a post-neurulation disorder, is an outpouching of meninges, CSF and dysplastic brain tissue through a defect in the skull, typically covered by dysplastic skin. Contents vary from mostly CSF to dysplastic brain tissue or, rarely, functional occipital lobe, brainstem or cerebellum. A Chiari III malformation is an occipito-cervical cleft and encephalocele at the same site, with confirmed cerebellar tissue in the posterior cervical mass. The actual etiology is not well understood, but may relate to failure of induction of endochondral bone by incomplete closure of the neural tube, or from a primary mesodermal defect. Alternatively, Chiari III malformations may develop due to lack of distention of the embryonic ventricular system because of abnormal neurulation leading to a hypoplastic posterior fossa with secondary displacement of the hindbrain. In Caucasians and most other patients in theWestern Hemisphere, posterior or occipitalencephalocelesarethemostcommontype.Characteristically,theyarelocatedbetween the lambda and the foramen magnum and can be further characterized by their relationship to the torcula. Other locations include nasofrontal, nasoethmoidal (sincipital), naso- orbital (more common in Southeast Asia and Latin America), and basal (trans-sphenoidal, spheno-ethmoidal,trans-ethmoidal,spheno-orbital).Mostencephaloceles(75–90%)are occipital. Out of 57 encephaloceles reported by Ivashchuk et al. 23 were high cervical/low occipital, 8 were high cervical, and 17 were low occipital. Occipital encephalocele has a femalepredominance(M:F1:2.4).Encephaloceleshavebeenassociatedwiththeuseduring pregnancy of the BCR-ABL1 targeted tyrosine kinase inhibitor Dasatinib. AFP and ACH are markers on amniocentesis that may be elevated or normal depending on if the defect is covered with skin or not. The elevated markers in this case suggest that there is an open defect. Other abnormalities to be aware of during the work-up include associated hydrocephalus and other dysraphic cranial or spinal defects, including myelomeningocele or tethered cord; dysgenesis of the corpus callosum; septo-optic dysplasia; absent, rudimentary, or inverted cerebellum; a small cyst similar to Dandy-Walker Malformation; and Meckel-Gruber Syndrome (syndromic occipital encephalocele associated with dysplastic kidneys, pulmonary hypoplasia, and polydactyly). In cases of small encephaloceles, there is no increased risk the fetus of vaginal delivery compared to C-section. However, larger encephaloceles require C-section. Most obstetricians prefer C-section for planning the timing and coordination of multiple teams required immediately after birth for all cases of encephalocele. It is important to have pediatric neurosurgery, pediatrics, and genetics teams available and involved prior to and at the time of birth. Questions
1. What are some of the characteristic exam findings? 2. What other studies should be ordered? 3. What are common findings on imaging?
249
0 5 2
Pediatric Neurosurgery
Decision Making
Characteristic exam findings include: micropthalmia, facial clefts, and sloping forehead due to the intracranial contents being posteriorly displaced within the cranial vault.Occipitalencephalocelesmayalsobeassociatedwithmyelomeningocele,cardiac, renal, limb and genital anomalies. Goals of surgery include removal of the protruding encephalocele sac, resection of nonviable or gliotic tissue, reduction of presumed viable tissue into the true intracranial space, watertight dural closure, adequate repair of the cranial defect, and appropriate skin closure. Pre-operative MRI, often including MRV, is required to evaluate presence and degree of herniation of brain contents into the sac, the proximity and involvement of venous sinuses to the lesion, the presence and degree of associated hydrocephalus, and the presence of a Chiari III malformation. The size of occipital encephaloceles varies; some include little or no cerebral contents and some include large amounts of functional cortex, cerebellum, or the brainstem within them. Often with larger lesions the brainstem is kinked and there is associated hydrocephalus. Diffusion tensor imaging can be helpful to evaluate white matter tracts, which may be involved in the encephalocele. MRI of the total spine is useful to evaluate for syringomyelia, which can be present with associated Chiari III malformation or other dysraphic abnormalities such as tethered spinal cord. There is a high rate of syringomyelia, and almost 70% of patients have incomplete fusion of the posterior cervical elements. After a full work-up for associated anomalies involving both a neonatologist and a geneticist, surgical intervention should be planned for repair of the defect. Questions
1. What factors affect timing of surgical intervention? 2. How would your plan change if there were no leaking from encephalocele? 3. What counseling should be given to the parents regarding functional outcome of their child?
Oral Boards Review—Diagnostic Pearls
1. Occipital encephaloceles are typically diagnosed prenatally with ultrasound and are obvious at birth. 2. After ultrasound diagnosis, OB-GYN physicians typically refer mothers for a fetal MRI for better definition of the defect and to evaluate for any associated abnormalities. MRI is safe in pregnancy and superior to ultrasonography. 3. Occipital encephaloceles may be associated with cranial nerve palsies, blindness, seizures, developmental delay, and/or spasticity. 4. It is important to obtain a genetics consultation to evaluate for other associated syndromes. One study reported a 60% rate of multiple associated genetic anomalies.
250
Occipital Encephalocele
5. Hydrocephalus may not be present initially but can develop after repair of the encephalocele because the encephalocele sac can serve as an expandable CSF reservoir. It is important to follow serially with measurement of head circumference and head ultrasound after encephalocele repair to monitor for the development of hydrocephalus.
Surgical Procedure
If there is CSF leaking from the lesion, surgical intervention should be done in a more urgent fashion to lower the rate of infectious complications. If the skin is intact over the lesion and there is no leaking, surgical repair for reconstructive reasons may be done in an elective fashion. However, the infant should be watched closely with daily OFC measurements to ensure that the infant is not developing hydrocephalus, and that additional neural tissue is not herniating progressively into the defect. Informed consent should cover risks of the procedure including infection, pseudomeningocele, CSF leak, hydrocephalus, blood loss requiring transfusion, neurological deficits including vision loss, failure of the cranial defect to close, and need for further surgery. An early discussion regarding prognosis can be important, although long-term prognosis is difficult to predict given the scant literature. Posterior encephaloceles are typically associated with a worse prognosis when compared to anterior or sincipital encephaloceles, probably due to greater association of occipital encephaloceles with hydrocephalus, seizure disorder, and additional morphological brain abnormalities. Roughly 50% of children with an occipital encephalocele are independent in adulthood. Working with an anesthesiology team that is familiar with pediatric neurosurgery is of great importance to ensure that the infant’s body temperature is optimized, and that the blood loss is replaced in a prompt and judicious manner. Intubation can be challenging and, depending on the size of the encephalocele, can be done with the patient supine with the head resting on a donut or horseshoe headrest, in the lateral position, or on the operating room table after decompression of fluid. For posterior encephaloceles, patients are positioned prone on a padded horseshoe headrest. Care should be taken to avoid pressure on the eyes, and other bony points should be padded. A Foley catheter is used to ensure adequate fluid resuscitation and an arterial line is placed to monitor hemodynamic status. Often an external ventricular drain (EVD) or shunt is placed pre-operatively for CSF management. Preoperative antibiotics are given. If there is concern for brainstem herniation into the encephalocele, intra-operative neuromonitoring can be used to assist in identifying normal tissue. If significant ventriculomegaly is already present at the time of surgery, EVD placement can help with fluid drainage and reduction of encephalocele-associated neural tissue. The incision is planned as an ellipse encircling the lesion, and the surgery begins with creation of a plane between the abnormal epithelium covering the lesion and the skin. Lidocaine with epinephrine may be used to help minimize blood loss. While dissecting down to the pericranium, care is taken to avoid early
251
2 5
Pediatric Neurosurgery
dural opening because maintaining a fluid filled sac can sometimes aid in dissection. The bony edge should be carefully defined. When the bone is fully exposed, the brain can be decompressed by releasing CSF either from the cystic structure or with an EVD. Pre-operative MRI provides clues to the degree of neurovascular structures incorporated into the lesion. After careful inspection, any gliotic or non-functional tissues can be removed to debulk the mass. If there is functional tissue within the encephalocele this should be preserved and reduced intracranially. If hydrocephalus is present, CSF drainage can aid in creating space for the brain tissue. However, if hydrocephalus is not present and it is felt that viable brain tissue is present within the sac, one option for management is to close dura and skin around the herniated brain tissue, and to plan a second cranial vault expansion procedure in order to create space to cranialize the encephalocele without increasing intracranial pressure. The dura may be repaired primarily after excision of redundant dura, or with a dural substitute. If the dura is intact and the bony defect is small enough, the defect can be left to close spontaneously. However, with a larger defect, split thickness calvarial or rib grafts can be used to close the defect. In some cases, repair of the cranial defect can occur in a separate procedure when the calvarium has become thick enough to split.
Oral Boards Review—Management Pearls
1. Carefully study a pre-operative MRI/MRA/MRV to evaluate for neurovascular structures or possible functional tissue within the encephalocele. 2. Water-tight closure is important to lower infectious risk. 3. Non-functional tissue can be excised while an attempt to preserve presumed functional tissue should be made. 4. Small bony defects do not need bone graft to cover. Larger areas can be closed using autologous grafts.
Aftercare
If shunting is not performed with the initial repair, it is critical to monitor the patient closely for evidence of enlarging ventricles. In the neonatal ICU postoperatively, the OFC should be measured daily and the incision should be inspected for signs of pseudomeningocele or leakage. Hydrocephalus is associated with 88% of patients with encephalocele and Chiari III malformations. There should be a low threshold for ventriculoperitoneal shunt placement if there are signs of leaking, pseudomeningocele formation, increasing ICP or brainstem dysfunction. Patients should be monitored closely for seizures and treated promptly should they develop. Hemoglobin and coagulation markers should be carefully followed in the post-operative period; especially if there was significant blood loss (i.e., 100 ml in a 5 kg child, or 10% loss) during the procedure.
252
Occipital Encephalocele
Pivot Points
1. If hydrocephalus is present before encephalocele repair, the patient may require placement of a CSF shunt. If not initially shunt, however, the patient should be monitored closely for signs of increasing intracranial pressure. 2. Shunting ideally is performed before there is actual leaking of CSF, as a CSF leak can lead to CSF contamination and subsequent infection of the shunt or encephalocele closure site. 3. Outcome is related to the amount of tissue within the encephalocele (which is generally inversely related to the degree of ultimate microcephaly) and to the associated conditions of hydrocephalus and seizures; thus prompt treatment of any associated conditions improves the likelihood of higher functional status in adulthood.
Complications and Management
This patient underwent surgical resection and had no functional tissue within the encephalocele. Gliotic tissue was amputated and primary closure of the dura obtained. On post-operative day 2 the nurse noted a fluid collection developing beneath the incision, with no fluid leaking from the suture line. She also measured a 2 cm increase in the OFC over a single day. On physical exam, the anterior fontanelle was full but not bulging, and there was a fluctuant collection under the skin at the area of the incision.The patient also suffered from an initial seizure, which resolved without treatment. A ventriculoperitoneal shunt was placed and neurological consultation undertaken for seizuremanagement.Aftertheseinterventions,thechild’sneurologicalstatusimproved.
Oral Boards Review—Complication Pearls
1. Treatment of seizures early on is important to reduce the chance of furthering developmental delay. Integration of care with a pediatric neurologist affords the best management of seizure disorders. 2. Seizures or neurological changes should be managed promptly. After ensuring that the airway is patent and there is no cardiovascular compromise, a head CT or “quick brain” MRI is indicated to evaluate for hydrocephalus and hemorrhage within the resection cavity.
Evidence and Outcomes
Little evidence exists to guide therapy of this relatively rare disorder. An early study by Mealey et. al. reported their experience from 1948 to 1968 with 559 infants with myelomeningocele,60withencephalocele,and4withboth.Intheirstudy,thesechildren accounted for roughly 0.82% of pediatric admissions to the hospital, and one of every six pediatric neurosurgical admission. In a more recent review by Ivashchuk et al. a similar incidence was found, ranging from 0.65 to 4.4%. Furthermore, they also found a higher
253
4 5 2
Pediatric Neurosurgery
rate of occipital encephaloceles compared to anterior skull base malformations. Small encephaloceles may not be diagnosed in the pre-or ante-natal period, and patients may be diagnosed at a later age; especially if the child is otherwise developmentally normal. While surgical techniques have improved greatly since that time, the survival rate remains similar. Primary repair of actively leaking malformations is the optimal treatment. Better understanding of the contents of the encephalocele may lead to improved cognitive outcomes. In a retrospective study, the presence of neural tissue within the defect, size > 2 cm, seizuredisorderandmicrocephalywereeachindependentlyassociatedwithhydrocephalus. Lesion size was previously not seen as a factor in outcome; and it appears that larger lesions are more likely to contain viable brain tissue than smaller encephaloceles. As discussedpreviously,overalloutcomeisassociatedwithseizurecontrolandtreatmentof hydrocephalus.Treatment of the hydrocephalus associated with encephaloceles is typically accomplished by ventriculoperitoneal shunting, although there have been reports of successful treatment with endoscopic third ventriculostomy in select cases. References and Further Reading
Ivashchuk, G., Loukas, M., Blount, J. P., Tubbs, R. S. & Oakes, W. J. Chiari III malformation: a comprehensive review of this enigmatic anomaly. Child’s Nervous System 31, 2035–2040, doi:10.1007/s00381-015-2853-9 (2015). Shahabi,S.&Busine,A.Prenataldiagnosisofanepidermalscalpcystsimulatinganencephalocoele. Prenatal Diagnosis 18, 373–377 (1998). Douvoyiannis, M., Goldman, D. L., Abbott Iii, I. R. & Litman, N. Posterior Fossa Dermoid Cyst With SinusTract and Meningitis in aToddler. Pediatric Neurology 39, 63–66, doi:http://dx.doi. org/10.1016/j.pediatrneurol.2008.03.019 (2008). Cama, A., Tortori-Donati, P., Piatelli, G., Fondelli, M. & Andreussi, L. Chiar complex in children— neuroradiologicaldiagnosis,neurosurgicaltreatmentandproposalofanewclassification(312 cases). European Journal of Pediatric Surgery Supplement 1, 35–38 (1995). Cortes,J.E.et al.Theimpactofdasatinibonpregnancyoutcomes. AmericanJournalofHematology 90, 1111–1115, doi:10.1002/ajh.24186 (2015). Barisic, I. et al. Meckel-Gruber Syndrome: a population-based study on prevalence, prenatal diagnosis,clinicalfeatures,andsurvivalinEurope.EuropeanJournalofHumanGenetics23,746–7 52, doi:10.1038/ejhg.2014.174 (2015). Case, A. P., Colpitts, L. R., Langlois, P. H. & Scheuerle, A. E. Prenatal diagnosis and cesarean section inalarge,population-basedbirthdefectsregistry.JournalofMaternal-Fetal&NeonatalMedicine 25, 395–402, doi:10.3109/14767058.2011.580801 (2012). Winn,H.R.&Youmans,J.R.YoumansNeurologicalSurgery,Volume1.5thed.(Saunders,2004, 2004). Cakirer, S. Chiari III malformation: varieties of MRI appearances in two patients. Clinical Imaging 27, 1–4 (2003). Mangels, K. J., Tulipan, N., Tsao, L. Y., Alarcon, J. & Bruner, J. P. Fetal MRI in the evaluation of intrauterine myelomeningocele. Pediatric Neurosurgery 32, 124–131, doi:28916 (2000). Wininger, S. J. & Donnenfeld, A. E. Syndromes identified in fetuses with prenatally diagnosed cephaloceles. Prenatal Diagnosis 14, 839–843 (1994).
254
Occipital Encephalocele
Zolal, A. et al. Identification of the large descending tracts using diffusion tensor imaging in Chiari III malformation. Child’s Nervous System 26, 867–870, doi:10.1007/s00381-010- 1155-5 (2010). Bui, C. J. et al. Institutional experience with cranial vault encephaloceles. Journal of Neurosurgery 107, 22–25, doi:10.3171/ped-07/07/022 (2007). Mealey,J.,Jr.,Dzenitis,A.J.&Hockey,A.A.Theprognosisofencephaloceles. JournalofNeurosurgery 32, 209–218, doi:10.3171/jns.1970.32.2.0209 (1970). Isik, N., Elmaci, I., Silav, G., Celik, M. & Kalelioglu, M. Chiari malformation type III and results of surgery: a clinical study: report of eight surgically treated cases and review of the literature. Pediatric Neurosurgery 45, 19–28, doi:10.1159/000202620 (2009). Lo, B.W. et al. Clinical predictors of developmental outcome in patients with cephaloceles. Journal of Neurosurgery. Pediatrics 2, 254–257, doi:10.3171/ped.2008.2.10.254 (2008). Da Silva, S. L., Jeelani, Y., Dang, H., Krieger, M. D. & McComb, J. G. Risk factors for hydrocephalus and neurological deficit in children born with an encephalocele.Journal of Neurosurgery. Pediatrics 15, 392–398, doi:10.3171/2014.10.peds14192 (2015). Kiymaz, N., Yilmaz, N., Demir, I. & Keskin, S. Prognostic factors in patients with occipital encephalocele. Pediatric Neurosurgery 46, 6–11, doi:10.1159/000314051 (2010). Ingraham, F. D. & Swan, H. Spina bifida and cranium bifidum. New England Journal of Medicine 228, 559–563, doi:doi:10.1056/NEJM194305062281801 (1943).
255
6 5 2
Nasal Dermoid Hugh J. L. Garton
29
Case Presentation
A 4-month-old boy presented with a small midline pit at the nasal dorsum noted along with a small right-sided forehead hemangioma and left-hand radial syndactyly. There was no history of drainage or expansion of the nasal pit. Exam showed no associated mass, but a small 3mm midline pit was evident, without hair (Figure 29.1). Because of the child’s young age and benign history and exam, MRI was deferred until he reached age 1. Upon return to the clinic at 13 months of age, the child’s parents reported that they had intermittently noted hair, and minimal clear to purulent drainage. While there had been no history of meningitis or repeated febrile illnesses, 1 week prior to presentationthe area hadbecomemoreswollenandappearedtendertotouch,featuresthatwere evident on exam as well (Figure 29.2). He was afebrile. Height, weight, head size and shape, and development were all proceeding appropriately and neurological exam was normal. The spine appeared normal with no sacral pit or other marking concerning for a spinal dysraphism at any level.The previously noted hemangioma on the left forehead had regressed modestly. An MRI obtained 1 month prior to the clinic visit demonstrated a linear lesion extending from the nasal dorsum, through the cranial base, with a cystic intracranial extension. The cystic material was iso to hypointense on T1, hyperintense on T2, and was associated with modest enhancement in the adjacent dura and restricted diffusion on diffusion weighted imaging (Figure 29.3). Diagnostic Questions
1. What is the diagnosis and expected natural history? 2. What diagnostic imaging is indicated, if any? When should it be performed? 3. What are the key diagnostic features to be observed on imaging? The expected lesion from the initial and follow-up examination is a nasal dermoid. Like spinaldermoids,theselesionsaredermal-linedtracts,and/orcysts,presentfrombirth,although not always recognized in infancy. Most will present along the midline anywhere from the columella to the nasofronal suture, but may also present as lateral as the medial canthus of the eye. The history or presence of hair and sebaceous drainage add further weight to the diagnostic suspicion. In most cases, a pit is present without associated swelling. However, more complex masses can be investigated with transillumination, the presence of which would raise suspicion of an encephalocele, or expansion with
257
8 5 2
Pediatric Neurosurgery
(a)
(b)
Figure 29.1. Photographs showing a small midline nasal pit, without hairs. jugular venous compression, indicating in a vascular mass. Occasionally, and sometimes repeatedly, the cyst tract will become blocked, and/or infected, leading to swelling and increased drainage. Extremely rarely, epidural abscesses or meningitis can occur. Lesions can often follow a very benign natural history and adult, or even geriatric, diagnoses occur. As with any other congenital lesion, the presence of 1 anomaly should prompt a careful search for others. Multiple tracts in a single patient, including sacral, lumbar, and nasal dermoid sinus tracts, do occur.The differential diagnosis in infants, broadened to include either the presence of a nasal pit or mass by exam, includes nasofrontal (sincipital) encephaloceles, nasal glioma, hemangiomas, sebaceous cysts, teratoma, other neoplasms, and skin fibromas. Embryologically, nasal dermoid lesions are an artifact of incomplete separation between cutaneous ectoderm and a dural diverticula that is present early in development through what will become foramen cecum in later development. It is thought that when the dura fails to separate, but begins to regress, cutaneous ectodermal tissues are drawn back toward and possibly through foramen cecum. The extent of the dermoid lesion is then determined by the durability of the dural–ectodermal connection. If separation occurs in a modestly delayed fashion, an extracranial lesion is present, whereas a more persistent connection results in the combined intracranial-extracranial lesion. Dermoid cysts can form along this pathway with or without the presence of a continuous tract/
(a)
(b)
Figure 29.2. Photographs showing a small nasal pit with hairs and some surrounding skin edema.
258
Nasal Dermoid
(a)
(b)
(c)
(d)
(e)
Figure 29.3. Nasal dermoid with intracranial extension. (A–B) Precontrast T1 and T2 Sagittal images (C–D) Pre and post contrast T1 axial images (E) Diffusion weighted imaging.
sinus and a cutaneous pit is not always present with a dermoid cyst, although should be diligently sought for on examination and imaging. Pathologically, the cyst or sinus lining of nasal dermoid lesions is similar to dermoid lesions elsewhere in the body, and consists of squamous epithelium with associated adnexal structures such as hair or sebaceous glands. MRI is probably the best diagnostic study to evaluate the lesion, but the timing of the study must be weighed against the potential harm of general anesthesia in very young infants. Generally, patients with skin findings consistent with an uncomplicated nasal dermoid, with no history or exam findings suspicious for infection have MRI imaging deferred until they are 6 to 12 months of age. Multiple sagittal and axial plane sequences including T1-weighted pre and post contrast, T2-weighted, and diffusion- weighted images are all helpful. Adequate imaging should include the entire nose, as the
259
0 6 2
Pediatric Neurosurgery
lesion may be present anywhere along its length, and the nasal tip is often excluded on standard brain MRI imaging. CT images can useful for evaluating bony abnormalities associated with this lesion. In cases where the MRI is equivocal with respect to intracranial involvement, high resolution CT is very useful to demonstrate the presence or absence of a midline bony defect, lack of which argues against intracranial extension. With intracranial extension, an enlarged foramen cecum (> 4mm in an infant) and/ or widened crista galli is generally seen. A split or bifid crista galli strongly suggests the presence of an intracranial dermoid lesion, while an eroded or absent one favors an encephalocele. However, CT carries an accompanying risk of radiation, although in manycasescanbedonewithoutanesthesia.Ultrasound,usefulinevaluatingtheneonatal spine, has been less useful in assessing for the key anatomic features of nasal dermoids. Our practice is to obtain an MRI as the primary study and reserve a thin cut CT for situations in which the anatomy remains unclear. MR demonstrates key features of a nasal dermoid, particularly whether there is intracranial extension. Of clinically diagnosed nasal dermoid lesions, 60 to 80% do not have intracranialextension(Figure29.4).Manysuchpatientsarecaredforbyotolaryngologists or plastic surgeons, often without neurosurgical involvement. As it can be helpful for treatment planning, anatomic classifications tend to separate lesions into those that are superficial and lack any involvement of bone, lesions that appear to be intraosseous but without a significant intracranial component, and those, like the example patient, that have intracranial extension. Intracranial extension can be limited to dural contact or can involve extension into the crista galli or even the falx cerebri. Brain parenchymal involvement is rare but may occur. The second important distinction to be made is between a dermoid sinus tract alone or in association with a dermoid cyst. This helps determine the width of operative exposure needed for resection. Dermoid cyst material, when present, typically restricts diffusion (Figure 29.3C). The radiographic differential diagnosis includes nasofrontal encephalocele, nasal glioma, and sinus pericranii. Nasal dermoid lesions, unlike nasofrontal encephaloceles, are not commonly associated with other midline CNS anomalies such as septo-optic dysplasia. However, intracranial dermoid cysts, in addition to but distinct from the nasal lesion, have been noted.
(a)
(b)
Figure 29.4. Nasal dermoid without intracranial extension (A) T1 pre-contrast, (B) T2.
260
Nasal Dermoid
Oral Boards Review—Diagnostic Pearls
1. While history of drainage and swelling helps confirm the diagnosis, most patients present with simple nasal pit. 2. Any congenital midline lesion should prompt a careful physical examination of the entire midline from coccyx to nasion. 3. Nasal dermoids may be off-midline as far as the medial canthus. 4. Clinical suspicion of a nasal dermoid lesion should be followed by planned imaging to confirm the diagnosis and evaluate for the extent of the lesion. 5. The specific diagnosis of nasal dermoid, as opposed non-dermoid lesion, is important as it dictates the need for complete removal (as opposed to nasal glioma). 6. Key imaging features relate to the presence or absence of intracranial extension of the lesion and whether the lesion is a tract only, or includes a cyst.
Decision Making
Operative intervention is generally indicated for patient with nasal dermoid lesions. However, these are usually elective rather than urgent procedures, and with increasing concerns about general anesthesia in very young children, it may reasonably be argued that in children with without a history of an expanding nasal mass or repeated infections, surgical intervention may be delayed until after a year of age. Certainly, in lesions without intracranial extension the risks of observation would appear to be low. Conversely, current or repeated infections in a child with known intracranial extension is an indication for antibiotics and more urgent surgical intervention. Surgical Technique
The primary goal of surgical treatment is complete excision of the lesion while providinganacceptablecosmeticresult.Operativeplanningisfocusedonensuringsufficient access. For lesions without intracranial extension, both direct and intranasal endoscopic approaches are available. Given that most such lesions are managed without neurosurgical involvement, the reader is referred to the “References and Further Reading” section for a detailed description of these methods. Briefly, when there is significant skin involvement, and a sinus tract with little to no cystic expansion, an open direct approach is often used. In this approach, a vertical elliptical incision is made around the lesion, and the underlying sinus tract is followed to its origin, often through the nasal bones, which may then require reconstruction. In situations where the skin involvement is minimal or not present, endoscopic techniques have been advocated. Endoscopic intranasal (for lesions on the nasal dorsum) or hairline incision endoscopic subgaleal (for lesions at the glabella) approaches are used. For lesions with intracranial extension, a multidisciplinary team is appropriate. Open intracrananial approaches utilize supine position, usually without cranial fixation in young children. Skin preparation should extend from the bicoronal region to the columella, with the face prepped only with povidone- iodine paint (e.g., Betadine paint) to avoid exposing the eyes to any preparatory agent containingdetergentoralcohol.Preoperativeantibioticcoverageshouldaccountforthe
261
2 6
Pediatric Neurosurgery
potential for contamination of the field with nasal flora. We prefer dual agent coverage with clindamycin and cefuroxime which is then continued for 72 hours postoperatively. Depending on the age and size of the child, a detailed plan for minimizing blood loss, and managing intraoperative anemia should be discussed. A bicoronal skin incision and subgaleal dissection expose the frontal periosteum which is then elevated as a separate vascularized layer for potential use as a graft during closure. A bifrontal craniotomy is performed with care taken to avoid injury to the sagittal sinus. In young children, the relatively shallow anterior fossa and lack of frontal sinuses usually allow for an adequate exposure without removal of the orbital bar, although more complex lesions can require this. Alternatively, for lesions with more limited intracranial involvement and no intradural extension, a subcranial bony exposure can be performed with the bony incisions made superiorly just above the orbital bar, laterally through the supraorbital rims.The inferior osteotomy is dictated to some extent by the location of the transosseus tract passage, but typically it is made with an osteotome through the superior aspect of the nasal bones and medial lacrimal bones, with careful attention to the medial canthal tendons to determine the need for resuspension during closure. Endoscopic endonasal approaches to the anterior skull base have also been used, although in small children access can be somewhat challenging. Intracranial dermoid material can then be removed, generally extending into the foramen cecum, where the tract will generally extend transcranially into the nasal subcutaneous tissue. Depending on the nature of the lesion, exposure of the crista galli can be needed. After resection of the dermoid tract/cyst wall in total, closure is performed. If a durotomy has been required or occurred, primary repair can be augmented by pericranium moved either as a vascularized pedicle or as a free transfer, with the former requiring at least a small gap in the bony reconstruction for passage. Insituationswherepreoperativeimagingleavesdoubtasthetothepresenceorextent of intracranial involvement (usually in cases of a long sinus tract without cystic expansion), a direct transnasal approach can be used, with the team prepared for a combined intra-extracranial procedure if frozen sections at the base of the lesion yield dermoid elements. Since dermoid sinus tracts have been described with only intermittent presence of dermal elements along the fibrous tracts, this approach is best used when the pre-test probability of intracranial extension is relatively low by preoperative radiology. The case patient presented here underwent a combined transnasal excision of the pit and nasal portion of the sinus, with bifrontal craniotomy to address the intracranial dermoid cyst. He made an uneventful recovery, with no recurrence evident on follow-up imaging at 2 years post procedure.
Oral Boards Review—Management Pearls
1. The primary goal of surgical management is complete excision of the lesions, including the punctate skin opening, if present. Incomplete resection is associate with up to a 50% recurrence rate. 2. Lesions without trans-osseous involvement are often managed via direct vertical nasal incision alone, although endonasal and subgaleal endoscopic techniques are also used.
262
Nasal Dermoid
3. For resections for which the neurosurgeon provides pre-operative consultation only, the discussion should focus on how inadvertent durotomy is to be avoided, recognized, and managed. 4. For lesions with intracranial extension, a team approach involving both neurosurgery and a nasal surgeon (typically a plastic surgeon or otolaryngologist) yields the best results. 5. Lesions with trans-osseus extension of a dermoid sinus tract with minimal intracranial cystic expansion can often be removed via an open transansal approaches, often using an open rhinoplasty approach. Small osteotomies that preserve the stalk can be used to expose stalk base which can then be separated from the dura without incision. The dural surface at the point of contact with the stalk is curetted and sometimes coagulated to be sure no residual dermal cells are present. 6. Lesions with significant intracranial cystic expansion are often managed best with bifrontal or subcranial craniotomy in combination with transnasal approaches as needed.
Pivot Points
1. Expanding or infected nasal dermoid lesions may require antibiotics and more urgent surgical care. 2. During imaging work-up, once the primary diagnosis has been recognized, the determination of the presence or absence of transcranial extension must be made. Both MRI and CT may be required as complementary modalities to determine this. 3. If intracranial extension is not entirely excluded by radiology, frozen section of the distal stalk of a dermal sinus tract showing no dermal elements can help confirm the completeness of resection.
Aftercare
For patients undergoing intracranial exposure, postoperative admission to the pediatric intensive care unit is typical. We prefer to continue postoperative antibiotics for 72 hours, although evidence supporting this practice is limited. Hyponatremia is not uncommon and at least daily serum sodium assessments are made until the child resumes taking food. Isotonic intravenous fluid is used for maintenance care until this occurs. At least 1 postoperative hematocrit is obtained in younger children undergoing a bicoronal skin incision. Perfusion status, as determined by vital signs including urine output via Foley catheter, is monitored at least overnight following the procedure. Postoperative analgesia is achieved with a combination of low dose intermittent opiates. Intravenous acetaminophen can be helpful in reducing opiate needs in the first 24 hours following the procedure. Careful attention in postoperative assessments for CSF leak and/or meningitis is warranted. Significant periorbital
263
4 6 2
Pediatric Neurosurgery
swelling is common after a bicoronal approach, and warning families about this before it occurs can alleviate worry. Anecdotally, swelling resolution to the point where the child can open her or his eyes again following the procedure has generally correlated well with a low readmission rate. Incomplete tract or cyst excision is likely to lead to recurrence. Postoperative imaging may therefore be indicated to confirm the absence of recurrence. The follow- up imaging plan is tailored to the particulars of the case. More extensive intracranial disease, or a more limited surgical approach to intracranial disease call for early and late post-operative imaging, and recurrence 5 years or more from initial treatment is reported. While evidence is lacking to guide a precise follow-up plan, an initial postoperative MRI at 1 year following complete resection and subsequent image at 5 years following surgery should exclude most recurrences. Concerning postoperative imaging finding for recurrence would justify more frequent and/or lengthier imaging follow-up. Complications and Management
As noted earlier, hyponatremia, CSF leak, and postoperative meningitis are all potential complications. Depending on the size of the patient at the time of surgery and the degree of intraoperative blood loss, postoperative anemia can be present. When possible, minimizing unnecessary blood draws can help, and young, otherwise healthy children generally tolerate anemia down to a hematocrit of 18% without difficulty, allowing for minimization of postoperative transfusions. Hyponatremia is a potentially serious complication and should be managed aggressively. Differentiating the 2 most common causes—the syndrome of inappropriate antidiuretic hormone secretion and cerebral salt wasting—is often difficult in the early postoperative phase. Management with intravenous hypertonic saline minimizes the chance of resultant cerebral edema or hyponatremic seizures. The risk window for postoperative hyponatremia appears to correlate well with disinterest in food in young children, so when eating resumes, generally the serum sodium level regularizes and hypertonic therapy can be discontinued. A postoperative cerebrospinal fluid leak should prompt rapid re-exploration in order to avoid the occurrence of meningitis, with consideration of a lumbar or ventricular drain to augment a periosteal flap or similar repair. In a more delayed fashion, wound infection, especially given the combined nasal-dural exposure, is a concern, but it is fortunately rare.
Oral Boards Review—Complications Pearls
1. Hyponatremina is common following craniofacial procedures in children. Direct treatment with salt infusion to achieve a normal serum sodium should not be delayed pending a laboratory work-up. Fluid restriction may have a role in some instances but is often ineffective by itself, and it can be deleterious if cerebral salt wasting is present. 2. A postoperative CSF leak should generally be aggressively managed by surgical re-exploration, often with temporary CSF diversion.
264
Nasal Dermoid
Evidence and Outcomes
There are no randomized controlled trials comparing different operative strategies for preoperativeevaluation,operativeapproach,orpostoperativecarespecificallyofpatients with nasal dermoid lesions. Multiple case series have been published and several are noted in the “References and Further Reading” section. Recurrence after incomplete resectioniscommon.Afterpresumedcompleteresection,lesionrecurrencerangesfrom 5 to 30%, thus warranting the follow-up described earlier. References and Further Reading
Update on Current Evaluation and Management of Pediatric Nasal Dermoid, Herrington H, Adil E, Moritz E, Robson C, Perez-Atayde A, Proctor M, Rahbar R1. Laryngoscope. 2016 Sep;126(9):2151–2160. doi: 10.1002/lary.25860. Epub 2016 Feb 18. https://www.ncbi.nlm. nih.gov/pubmed/26891409 The management of midline frontonasal dermoids: a review of 55 cases at a tertiary referral center and a protocol for treatment. Moses MA, Green BC, Cugno S, Hayward RD, Jeelani NU, Britto JA, Bulstrode NW, Dunaway DJ. Plast Reconstr Surg. 2015 Jan;135(1):187– 196. doi: 10.1097/PRS.0000000000000833. https://www.ncbi.nlm.nih.gov/pubmed/ 25285685 Nasal dermoids in children: a proposal for a new classification based on 103 cases at Great Ormond Street Hospital. Hartley BE, Eze N, Trozzi M, Toma S, Hewitt R, Jephson C, Cochrane L, Wyatt M, Albert D. .Int J Pediatr Otorhinolaryngol. 2015 Jan;79(1):18–22. doi: 10.1016/j.ijporl.2014.10.020. Epub 2014 Oct 24. https://www.ncbi.nlm.nih.gov/ pubmed/25481331 Midline approach to pediatric nasofrontal dermoid cysts. Ortlip T, Ambro BT, Pereira KD. JAMA Otolaryngol Head Neck Surg. 2015 Feb;141(2):174–177. doi: 10.1001/jamaoto.2014.3185. https://www.ncbi.nlm.nih.gov/pubmed/25521829 Surgical correction of midline nasal dermoid sinus cysts. Winterton RI, Wilks DJ, Chumas PD, Russell JL, Liddington MI. J Craniofac Surg. 2010 Mar;21(2):295–300. doi: 10.1097/ SCS.0b013e3181cf5f44. https://www.ncbi.nlm.nih.gov/pubmed/20186096 Nasal dermoids. Zapata S, Kearns DB. Curr Opin Otolaryngol Head Neck Surg. 2006 Dec;14(6):406–411. https://www.ncbi.nlm.nih.gov/pubmed/17099348
265
62
Sinusitus with Subdural Empyema Christina Sayama
30
Case Presentation
A 13-year-old male was brought by emergency medical services to the emergency department after a new onset generalized tonic clonic seizure at home lasting 3 minutes. He had recently been diagnosed with sinusitis by his pediatrician and had received antibiotic therapy for 5 days. His parents reported that the patient had demonstrated persistentongoingfevers,worseningheadaches,andlistlessnessforthepastseveraldays.The remainder of his medical history was negative. On examination, the patient is mildly confused and post-ictal after his seizure. He moved all extremities equally to stimuli and followed commands with repetitive prompting. Swelling was noted over his left frontal region extending into the left periorbita. His pupils were equal and reactive to light. He was warm to the touch and noted to be febrile to 102.1 °F in the emergency department with tachycardia to 110 and blood pressure of 108/68. Questions
1. What is the likely diagnosis? 2. What laboratory studies should be done? 3. What is the most appropriate imaging modality? 4. What is the appropriate timing of the diagnostic work-up? 5. Are there any immediate treatment steps that should be initiated?
Assessment and Planning
The pediatric neurosurgeon is consulted and suspects the presence of an intracranial infection secondary to spread from his underlying sinusitis. The differential diagnosis includes a subdural empyema, intracranial abscess, or meningitis. Intracranial spread is most often from direct extension of local infection rather than hematogenous spread from bacteremia.
Oral Boards Review—Diagnostic Pearls
1. Lumbar puncture must not be done prior to brain imaging as there is a potential risk of herniation in the setting of mass effect or parenchymal swelling.
267
8 6 2
Pediatric Neurosurgery
2. If an initial CT is negative and there is high clinical suspicion, an MRI should be obtained with and without contrast and with diffusion weighted imaging. 3. In younger children, subdural empyema is more commonly associated with a suppurative meningitis whereas in older children the more likely source is direct spread from sinusitis and otitis. Evaluation should include imaging, such as a head CT with and without contrast or MRI brain with and without contrast. Additionally, lab work such as a complete blood count with differential, comprehensive metabolic panel, erythrocyte sedimintation rate, C-reactive protein, blood cultures, and coagulopathy panel are important baseline studies to obtain. If the patient demonstrates seizure activity, the use of intravenous benzodiazepines and other anti-epileptic medications is appropriate. MRI imaging remains the most sensitive and definitive diagnostic modality for detection of subdural empyema. T1-weighted images typically demonstrate a low signal fluid collection, while T2-weighted images demonstrate a high signal fluid collection. PeripheralenhancementisnotedonT1-weightedcontrast-enhancedimaging.Subdural empyema manifests as hyperintense signal on diffusion weighted imaging (DWI) and hypointense signal on apparent diffusion coefficient (ADC) imaging (Figure 30.1). CT scans with contrast may be helpful, although non-contrast CT image may not show any obvious abnormality (Figure 30.2). Questions
1. How do these clinical and radiological findings influence surgical planning? 2. What is the most appropriate timing for intervention in this patient? 3. Are there different surgical strategies that should be considered?
Decision Making
A patient demonstrating significant symptoms of intracranial infection should not have antibiotics withheld prior to obtaining cerebrospinal fluid or lesional culture samples. Broad spectrum antibiotics are initiated and can be narrowed after cultures provide bacterial speciation and sensitivities. Lumbar puncture is not safe in situations with suspected high intracranial pressure (ICP) and supratentorial mass effect due to the risk of brain herniation. Subdural empyema, in particular, predisposes to a risk of herniation. If imaging indicates a subdural empyema is present, this should prompt urgent surgical intervention and drainage. The minority of patients are appropriate for conservative treatment, including those with very small supratentorial collections and without neurological deficit or associated cerebral edema. Craniotomy with evacuation of subdural empyema is the mainstay of treatment. It allows for complete evacuation of the empyema and decompresses the underlying brain parenchyma. Less commonly, burr hole drainage of subdural empyema can be considered but many studies have shown increased risk of recurrence in these patients with need for further procedures. However, in the event of an emergency situation in a
268
(A)
(B)
(C)
(D)
(E)
Figure 30.1. MR images demonstrating a right fronto-parietal subdural empyema: (A) T1 pre-contrast, (B) T2, (C) T1 post-contrast, (D) DWI, (E) ADC.
0 7 2
Pediatric Neurosurgery
(A)
(B)
Figure 30.2. CT images in the same patient also demonstrate the subdural empyema: (A) CT without contrast, (B) CT with contrast.
medically frail patient, the burr hole technique may be preferred. Burr hole drainage is not optimal for a patient with loculated infection. Other forms of lowering intracranial pressure may be necessary, such as ventriculostomy, hypertonic saline, elevation of the head, or further surgical procedures. In the setting of a patient with severe parenchymal swelling, a craniectomy may be indicated and should be considered if pre-operative imaging is concerning for cerebral edema with mass effect. Patient clinical care and decision making should occur in the setting of a multidisciplinary team of pediatric ICU physicians, infectious disease physicians, and neurosurgeons. If the infection has spread from sinusitis or otitis, ENT surgeons are often involved and may concurrently operate on the sinuses (endoscopic sinus surgery) or ears (placement of ear tubes) to drain any other source of infection. Questions
1. How should the care and assessment of a patient presenting with fevers, altered mental status, aphasia, and hemiparesis be prioritized in the setting of a known history of otitis and active antibiotic therapy? 2. A large panhemispheric subdural empyema with cerebral edema and midline shift is found in this patient. What is the appropriate treatment and timing of intervention?
Surgical Procedure
Craniotomy for evacuation of subdural empyema is a major procedure carried out under general anesthetic with a Foley catheter in place and duplicate IV access. The patient
270
Sinusitus with Subdural Empyema
should have a coagulopathy panel drawn pre-operatively and blood products available if necessary. In the setting of suspected cerebral edema, the surgeon should be prepared with a larger incision for possible hemicraniectomy. Consideration of need for external ventricular drainage should be made in the preoperative period. Discussion should be held with the anesthesiologist regarding use of anti-epileptic medications, hypertonic saline, mannitol, and/or steroids. The patient is positioned supine on a horseshoe head holder and a gel roll is placed under the shoulder. Anatomical landmarks are used to plan the craniotomy; however, neuronavigation may be used if necessary if a pre-operative navigation scan has been completed and the patient is not rapidly deteriorating. The craniotomy flap is turned with a craniotome after circumferential burr holes are placed.Duraltackupsareplacedtopreventpost-operativeepiduralbleeding.Hemostasis must be maintained throughout with bipolar and/or Bovie electrocautery. The dura is opened in a U-shaped fashion and cultures should be collected from the subdural space. The subdural empyema may egress under pressure once the dura has been opened. If there is subarachnoid infection, this should be left alone.The subdural space is carefully irrigated to help wash out any remaining infectious material. The dura is closed primarily and the bone flap is replaced with cranial plates and screws (assuming there is not an excessive amount of cerebral edema). Dependingonthepatient’spresentation,post-operativeintubationmaybenecessary, though extubation is preferred in order to closely follow the neurological examination.
Oral Boards Review—Management Pearls
1. Subdural empyema is considered a neurosurgical emergency requiring surgical drainage. Antibiotic penetration into a subdural abscess is poor and progression of infection may lead to cortical venous thrombosis and risk of venous infarction. Because there are no anatomic barriers, the infection may rapidly spread along the subdural space. 2. In a patient with significant systemic signs of infection, broad spectrum IV antibiotics that cross the blood brain barrier should be started immediately. 3. Burr hole evacuation should be reserved for frail/septic patients who are too unstable to undergo craniotomy, as multiple studies have shown this surgical technique to be inferior for infection control.
Pivot Points
1. If elevated ICP is a concern, the management plan should include post-operative ICP monitoring and neurologic stabilization prior to any necessary ENT intervention. 2. Parafalcine empyemas may pose higher risk of bleeding from bridging veins, and thus extreme caution must be taken with their surgical management. 3. Posterior fossa subdural empyemas should always be evacuated, regardless of their size.
271
2 7
Pediatric Neurosurgery
Aftercare
Post-operative care in the PICU is required and patients remain on broad spectrum antibiotics until speciation and sensitivities from intraoperative cultures are established. If operative cultures fail to identify a bacterial diagnosis, the patient should be treated empirically with broad spectrum antibiotics. The duration of antibiotics is typically 4–6 weeks, though may be longer depending on the suspected organism. Anti-epileptic medications are appropriate in patients with subdural empyema and duration is variable depending on manifestation of seizure as a presenting feature. Post-operativeimagingisappropriatetoevaluatefortheextentofsubduralempyema evacuation and to establish a new baseline. Serial scans may be followed and the timing should be based on clinical judgement, patient condition, and response to treatment. Serial sodium should be monitored and hyponatremia fastidiously avoided. Infectious labs such as serum WBC, ESR, and CRP may be followed over the duration of treatment as a measure of treatment responsiveness. The patient will require a peripherally inserted central catheter (PICC) line for long-term IV antibiotic administration. Neurological outcome is often reflective of the initial presentation; presence of cerebral herniation or neurological deficits carry a poorer prognosis. Subdural empyema is a life-threatening infection and early detection and treatment are important for optimal outcome. Complications and Management
Recurrence of subdural empyema and need for repeat craniotomy can occur. Many studies have shown that treatment with burr hole drainage alone carries a higher likelihood of subdural empyema recurrence. Recurrent seizures are also a common complication following subdural empyema. Seizure prophylaxis is often used even in patients who do not present initially with seizure activity. Cortical venous thrombosis is a serious complication of subdural empyema that can result in permanent deficit. Urgent surgical intervention at time of diagnosis will minimize the development of this complication.
Oral Boards Review—Complications Pearls
1. Detection of recurrent subdural empyema is critical to prevent further morbidity and mortality. Close observation for fever, clinical deterioration, and imaging progression is critical. The possibility of multiple operations should be discussed with families at the time of initial surgery. 2. Arm swelling or pain in a patient being treated with long-term antibiotics should always prompt further evaluation with duplex ultrasonography to rule out catheter associated thrombus. Central lines are necessary for administration of long-term IV antibiotics, often in the form of a PICC line. These can have complications such as thrombosis, which requires
272
Sinusitus with Subdural Empyema
attention and possible removal or treatment with anticoagulation depending on the extent of the clot involved. Evidence and Outcomes
Prospectiverandomizedcontrolledstudiesregardingthetreatmentofsubduralempyema are lacking, in large part due to the uncommon occurrence of this disorder and predominance in the pediatric population. Emergent treatment of subdural empyema is indicatedinmostcasesandseveralstudiessupportimprovedoutcomeswithexpeditious timing of surgical intervention. References and Further Reading
Neurosurgical management of extraaxial central nervous system infections in children. Gupta S, Vachhrajani S, Kulkarni AV, Taylor MD, Dirks P, Drake JM, Rutka J T. J Neurosurg Pediatr. 2011;7(5):441–451. https://www.ncbi.nlm.nih.gov/pubmed/21529183 Cranial and spinal subdural empyema. de Bonis P, Anile C, Pompucci A, Labonia M, Lucantoni C, Mangiola A. Br J Neurosurg. 2009;23(3):335–340. https://www.ncbi.nlm.nih.gov/pubmed/ 19533473 Subdural empyema secondary to sinus infection in children. Farah JO, Kandasamy J, May P, Buxton N, Mallucci C. Childs Nerv Syst. 2009;25:199–205. https://www.ncbi.nlm.nih.gov/ pubmed/18575871 The treatment and outcome of postmeningitic subdural empyema in infants. Liu ZH, Chen NY, Tu PH, Lee ST, Wu CT. J Neurosurg Pediatr. 2010 Jul; 6(1):38–42. https://www.ncbi.nlm. nih.gov/pubmed/20593986 Suppurativeintracranial complicationsofsinusitisinadolescence.Singleinstituteexperienceand review of literature. Kombogiorgas D, Seth R, Athwal R, Modha J, Singh J. Br J Neurosurg. 2007 Dec;21(6):603–609. https://www.ncbi.nlm.nih.gov/pubmed/18071989 Neurological Complications of Acute and Chronic Sinusitis. Ziegler A, Patadia M, Stankiewicz J. Curr Neurol Neurosci Rep. 2018 Feb 5;18(2):5. doi: 10.1007/s11910-018-0816-8. https:// www.ncbi.nlm.nih.gov/pubmed/29404826 Subdural empyema in children. Hendaus MA. Glob J Health Sci. 2013 Aug 14;5(6):54–59. doi: 10.5539/gjhs.v5n6p54. https://www.ncbi.nlm.nih.gov/pubmed/24171874 Paediatric intracranial empyema: differences according to age. Legrand M, Roujeau T, Meyer P, Carli P, Orliaguet G, Blanot S. Eur J Pediatr. 2009;168(10):1235–1241. https://www.ncbi. nlm.nih.gov/pubmed/19137324 Posterior fossa subdural empyema in children—management and outcome. MadhugiriV. S, Sastri B. V, Bhagavatula I. D, Sampath S, Chandramouli BA, Pandey P. Childs Nerv Syst. 2011;27:137– 144. https://www.ncbi.nlm.nih.gov/pubmed/20496071 Twosurgicalmethodsusedin90patientswithintracranialsubduralempyema.MatNayanSA,Mohd Haspani MS, Abd Latiff AZ, Abdullah JM, Abdullah S. J Clin Neurosci. 2009;16(12):1567– 1571. https://www.ncbi.nlm.nih.gov/pubmed/19793660 Craniotomy improves outcomes for cranial empyema in computed tomography era experience with 699 patients. Nathoo N, Nadvi SS, Gouws E, van Dellen JR. Neurosurg. 2001;49:872– 878. https://www.ncbi.nlm.nih.gov/pubmed/11564248
273
4 7 2
Ventricular Shunt Infection Christina Sayama
31
Case Presentation
A 12-year-old female presents to the emergency department with tenderness, redness, and swellingontherightsideofherhead.Shehasahistoryofcongenitalhydrocephalusandhasnot hadaventriculoperitonealshuntrevisionforseveralyears.Shereportsitchingatascabbehind her ear caused by her glasses over the past two weeks. She has had no fevers; however, in the emergency department her temperature is 99.9 F. Her heart rate is regular and 85 bpm, blood pressureis100/65.Otherthandiscomfortontherightsideofherheadnearhershunt,shehasno othercomplaints.Shehasnomeningismus.Herextraocularmovementsareintactwithnormal upgaze.Sheisneurologicallyintact.Shehasnoabdominalpain.Sheandhermotherreportthat therednessandwarmthhasstartedtotraveldownherneck.Shehasapalpable,fluctuantfluid collection along her shunt tubing in the neck which is warm to the touch and erythematous. Questions
1. What is the likely diagnosis? 2. What are the most appropriate imaging modalities? 3. What is the appropriate timing of the diagnostic work-up?
Assessment and Planning
Presence of a shunt infection is suspected. The likely etiology is spread from a superficial infection and unlikely to be related to her last surgical intervention given the remote timing.The differential diagnosis also includes meningitis, intracranial infection, abdominal infection travelling retrograde, or superficial rash. Given the findings of erythema and swelling around the shunt tubing and tract, shunt infection is highest on the differential. Shunt infections most commonly occur within 2 weeks of a shunt intervention (operation or tap); however, they can occur at any time. The likelihood of a shunt infection is very low after 6 months have passed from the last shunt intervention.
Oral Boards Review—Diagnostic Pearls
1. Shunt infection should always be on the differential for any patient presenting with erythema, swelling, or tenderness along the shunt tract. 2. Development of fever within the post-operative period after a shunt placement or revision should always raise concern for possible infection.
275
6 7 2
Pediatric Neurosurgery
Brain imaging and shunt x-ray series are the diagnostic imaging studies of choice. As there is concern for intracranial infection, brain imaging should be done with and without contrast. Identification of intracranial enhancement demonstrating abscess or ventriculitis is important as the presence of these findings (although rare) may change surgical management. Consideration for more detailed imaging of the distal portion of the shunt is appropriate in the setting of suspicion for abscess or other infection related complication. For instance, abdominal imaging may be helpful to rule out intra- abdominalinfection,abscessorpseudocyst.Chestcomputedtomography(CT)withand without contrast may be necessary if pulmonary empyema is a concern in a patient with a ventriculo-pleural shunt. It is important to obtain cerebrospinal fluid (CSF) cultures prior to starting antibiotics. A shunt tap for CSF sampling can be performed in a timely manner. For patients with ventriculoatrial shunts, it is also important to obtain blood cultures. Questions
1. What is the surgery of choice for this patient? 2. What is the most appropriate timing for intervention in this patient? 3. How should management be altered if patient presents with signs and symptoms of sepsis? 4. What antibiotics should be initiated after appropriate cultures have been obtained? This patient underwent a brain magnetic resonance imaging (MRI) with and without contrast, which did not demonstrate any intracranial enhancement.The ventricles were unchangedfrompreviouswellbaselinescansandtherewasnoventricularenhancement. A very small area of subgaleal enhancement just superior to the top part of the valve was seen. A shunt x-ray series showed no kinks or discontinuities in the shunt tubing. The distal end of the shunt was located in the peritoneal cavity with the tip in the right lower quadrant, curving gently without restriction, suggesting the absence of a pseudocyst (Figure 31.1). Decision Making
A sample of CSF should be sent prior to starting antibiotics. One should also ensure that other cultures are sent, including cultures of the blood and urine. Other laboratory studies that should be sent include Complete Blood Count (CBC), Basic Metabolic Panel (BMP), Prothromin Time (PT), Partial Thromboplastin Time (PTT), International Normalized Ratio (INR), Erythrocyte Sedimentation Rate (ESR), and C- Reactive Protein (CRP). Surgical planning often includes removal of the shunt with placement of an external ventricular drain in a timely manner. Antibiotics should be started after CSF samples areobtained;however,inapatientwithsepsis,antibioticsshouldbestartedimmediately. The antibiotic regimen should include broad spectrum coverage of gram positive and gram negative bacteria, often including a combination of vancomycin with a cephalosporin that effectively penetrates the CNS such as ceftriaxone or cefipime. If there is a
276
Ventricular Shunt Infection
(A)
(B)
Figure 31.1. MR imaging with and without contrast do not demonstrate any intracranial enhancement. The ventricles are unchanged from previous well baseline scans and there is no ventricular enhancement. A very small area of subgaleal enhancement is present just superior to the top part of the valve.
high suspicion for anaerobic bacteria, flagyl can be added to the regimen for a “triple antibiotic” cocktail. Questions
1. What is the appropriate management for a patient with a ventriculoperitoneal shunt presenting with fever, lethargy, bradycardia, and enlarged ventricles? How would this management change if an operating room was not immediately available? 2. What is the appropriate management for a patient presenting to the emergency department with exposed shunt tubing?
Surgical Procedure
Shuntsurgeryrequiresgeneralanesthesia,andinthesettingofsuspectedorprovenshunt infection, the infected shunt is ideally explanted and an external ventricular drain is placed. While most pediatric neurosurgeons will opt to explant the entire shunt system and place a temporary external ventricular drain, a less frequently used options includes partial shunt explant and externalization, particularly in the setting of a chronic infection with low-grade fever and abdominal pseudocyst as the presenting symptoms. The patient is placed in the supine position on the operating room table and head positioned in a manner to expose the cranial shunt incision with clear access to abdominal and/or posterior auricular incision. If CSF has not been obtained preoperatively, then antibiotics are often withheld until intraoperative CSF sampling is performed. CSF and incision cultures (where applicable) are obtained. The entire shunt is explanted and an external ventricular drain (EVD) is placed. The EVD is tunneled posteriorly and away from the present subcutaneous tract and suspected infection.
277
8 7 2
Pediatric Neurosurgery
Broad-spectrum antibiotics are initiated. If there is retained tubing, benefits and risks must be weighed in deciding whether to make further attempts at removal.
Oral Boards Review—Management Pearls
1. When clinically appropriate, CSF cultures should be obtained prior to initiation of antibiotic therapy when shunt infection is suspected. 2. Explantation of all foreign material and treatment with EVD and broad- spectrum antibiotics is the treatment of choice.
Pivot Points
1. Patients presenting with suspicion of sepsis or neurologic instability should not have antibiotics deferred for CSF cultures. 2. Duration and choice of antibiotic regimen depends on the speciation of the infectious agent. 3. A patient presenting with lethargy, fever and ventriculomegaly with bradycardia should undergo emergent ventriculoperitoneal shunt tap for CSF gram stain and cultures (followed by initiation of antibiotics) and with the goal of emergently decompressing the ventricular system. 4. The presence of exposed tubing, a perforated viscus at the distal shunt implantation site, or an abdominal pseudomeningocele containing the distal shunt tubing should be considered evidence of a shunt infection until proven otherwise.
Aftercare
The external ventricular drain is often placed at a level that appropriately represents the resistance of the shunt valve that was previously in place. Antibiotics are typically administeredforapproximately14 daysafterobtainingthefirstcleanculture,depending on the organism identified.The actual duration of antibiotics is often determined by the type of infectious agent and the extent of infection. During treatment, daily CSF cultures are sent to detect clearing of the infection and response to antibiotics. Patients being treated for a shunt infection are often in the hospital for at least 2 weeks for IV antibiotic therapy and external ventricular drainage. There is insufficient evidence to support the use of intrathecal antibiotics for routine shunt infections. Many neurosurgeons consult infectious disease physicians for recommendations on antibiotic therapy, route of administration, and duration. Once the infection has been cleared, the shunt can be reimplanted. Some neurosurgeons choose to implant a new proximal catheter at a different site to avoid the previously infected region; however, there is no evidence mandating this and many choose to reimplant the ventricular catheter through the same EVD trajectory to avoid creating a new tract through the brain parenchyma.
278
Ventricular Shunt Infection
Complications and Management
Externalized ventricular drain complications may include dislodgement. Drains should be carefully secured at the exit site to avoid unplanned removal and need for urgent operative replacement.The subcutaneous tunnel from the burr hole to the catheter exit site should be at least 5 cm long to minimize the incidence of a new infection. A secondary infection of the CSF is another complication that can result from long- term external ventricular drainage. Meticulous care of the EVD should be maintained; the site should be kept clean and all attachments sterile. Any access to the EVD for obtaining CSF culture should be performed under sterile conditions and by appropriately trained neurosurgery personnel. Prevention of a super-infection is critical to minimize the morbidity of the primary shunt infection treatment plan. Long-term antibiotics may result in unexpected side effects depending on the antibiotic type administered. Regular lab values must be checked to ensure antibiotics being used (i.e., vancomycin) are within appropriate levels and renal function is not being adversely affected. Patients often require placement of peripherally inserted central catheters (PICC lines), which can cause issues such as thrombosis.
Oral Boards Review—Complications Pearls
1. Careful attention to securing external ventricular drains is important as these catheters are in place for the duration of antibiotic therapy and are critical for managing the underlying hydrocephalus. 2. Determination of antibiotic choice, duration, and need for PICC line placement will depend on the individual clinical scenario and should be determined from multidisciplinary discussions with the neurosurgeon, infectious disease specialist, pharmacist, and other clinical care coordinators.
Evidence and Outcomes
Prospective randomized controlled studies regarding the treatment of shunt infections are lacking. Institutional variability in management is substantial, and the optimal treatment for shunt infection has yet to be determined. Guidelines from a systematic literature review which critically appraised 27 studies were published in 2014. The authors described Class II evidence in support of antibiotic treatment with either partial (externalization) or complete shunt removal for treatment of a shunt infection. It was recommended that clinical judgement be utilized to determine whether shunt externalization or complete removal of a shunt was the preferred management strategy in individual cases. References and Further Reading
Tamber MS, Klimo P Jr, Mazzola CA, Flannery AM; Pediatric Hydrocephalus Systematic Review and Evidence-Based Guidelines Task Force: Pediatric hydrocephalus: systematic literature review and evidence-based guidelines. Part 8: management of cerebrospinal
279
0 8 2
Pediatric Neurosurgery
fluid shunt infection. J Neurosurg Pediatr. 2014 Nov; 14(Suppl 1):60–71. doi: 10.3171/ 2014.7.PEDS14328. https://www.ncbi.nlm.nih.gov/pubmed/25988784 Heidari V, Habibi Z, Hojjati Marvasti A, Ebrahim Soltani Z, Naderian N, Tanzifi P, Nejat F: Different behavior and response of staphylococcus epidermidis and streptococcus pneumoniae to a ventriculoperitoneal shunt: an in vitro study. Pediatr Neurosurg. 2017; 52(4):257–260. doi: 10.1159/000477817. Epub 2017 Jul 14. https://www.ncbi.nlm.nih.gov/ pubmed/28704823 Arnell K, Enblad P, Wester T, Sjölin J: Treatment of cerebrospinal fluid shunt infections in children using systemic and intraventricular antibiotic therapy in combination with externalization of the ventricular catheter: efficacy in 34 consecutively treated infections. J Neurosurg. 2007; 107(3 Supp): l213–219. Forrest DM, Tabara ZB, Towu E, Said AJ: Management of the colonised shunt. Z Kinderchir. 1987; 42(Suppl): 121–2 2. http://t hejns.org/s ervlet/l inkout?suffix=b6-6 0-7 1&dbid=8&doi= 10.3171%2F2014.7.PEDS14328&key=3433969 James HE, Walsh JW, Wilson HD, Connor JD: The management of cerebrospinal fluid shunt infections: a clinical experience. Acta Neurochir (Wien). 1981; 59:157–166. http://thejns. org/servlet/linkout?suffix=b11-60-71&dbid=8&doi=10.3171%2F2014.7.PEDS14328& key=7340429 James HE, Bradley JS: Aggressive management of shunt infection: combined intravenous and intraventricular antibiotic therapy for twelve or less days. Pediatr Neurosurg. 2008; 44:104–111. http://thejns.org/servlet/linkout?suffix=b9-60-71&dbid=8&doi=10.3171%2 F2014.7.PEDS14328&key=18230923 Wang KC, Lee HJ, Sung JN, Cho BK: Cerebrospinal fluid shunt infection in children: efficiency of management protocol, rate of persistent shunt colonization, and significance of ‘off- antibiotics’ trial. Childs Nerv Syst. 1999; 15:38– 44. http://thejns.org/servlet/ linkout?suffix=b34-60-71&dbid=8&doi=10.3171%2F2014.7.PEDS14328&key=10066018 Whitehead WE, Kestle JR: The treatment of cerebrospinal fluid shunt infections. Results from a practice survey of the American Society of Pediatric Neurosurgeons. Pediatr Neurosurg. 2001; 35:205–210. http://thejns.org/servlet/linkout?suffix=b35-60-71&dbid=8&doi=10. 3171%2F2014.7.PEDS14328&key=11694798 Ronan A, Hogg GG, Klug GL: Cerebrospinal fluid shunt infections in children. Pediatr Infect Dis J. 1995; 14:782–786. http://thejns.org/servlet/linkout?suffix=b20-60-71&dbid=8&doi =10.3171%2F2014.7.PEDS14328&key=8559628 Whitney NL, and Selden NR. Pullout proofing external ventricular drains: Technical note. J Neurosurg Pediatr. 2012; 10:320–323. 10.3171/2012.7.PEDS1280.
280
Index
ABCs (airway, breathing, circulation), 96 acute (rapid progression) hydrocephalus, 3 amblyopia, inflicted traumatic brain injury and, 96 American Association of Neurological Surgeons (AANS), 22 American Syringomyelia and Chiari Alliance Project, 63 anatomic hemispherectomy (AIH), 131 anoxic seizures, 129 antibiotic therapy for communicating hydrocephalus, 6–8 for intraventricular hemorrhage, 25, 27 for lipomyelomeningocele, 45 for mesial temporal glioma, 204 for moyamoya disease, 155 for myelomeningocele, 66 for nasal dermoid, 263–64 for obstructive hydrocephalus, 14, 16 for ruptured arteriovenous malformation, 146 for sagittal synostosis, 80 for sinusitis with subdural empyema, 268, 270, 271, 272–73 for spastic quadriplegia, 112–13, 114 for spinal dermal sinus tract, 50, 53 for traumatic atlanto-axial dislocation, 106 for unicoronal synostosis, 90 for ventricular shunt infection, 276–78, 279 aphasia, expressive, moyamoya disease and, 149 arachnoid cysts. See middle fossa arachnoid cyst arachnoiditis, 50, 58 arteriovenous malformation (ruptured AVM), 141–48 anatomical features, 144 assessment and planning, 141, 142–43 case history, 141 complications, 147 decision making, 143–44 diagnostic pearls, 142–41 immediate interventions, 143 management, 146, 147 outcomes
after multimodal therapies, 148 postsurgery, 148 pivot points, 146 Spetzler-Martin AVM grading scale, 144, 148 surgical procedure, 145 aftercare, 146–47 embolization, 145–46 timing, 145 treatment goal, 144 astrocytoma, low and high-grade, 177 atlanto-axial dislocation (AOD), 101–7 aftercare, 106 assessment and planning, 101–3 case presentation, 101 complications, 106 decision making, 104 diagnostic pearls, 103 evidence and outcomes, 106 management, 103, 106 pivot points, 107 surgical procedure, 104–5 young children’s susceptibility to, 103 atretic tails (skin tags), 32 attention deficit hyperactivity disorder (ADHD), 11 atypical teratoid/rhabdoid tumor (AT/RT), 177 baclofen withdrawal syndrome, 115, 116 basilar artery craniopharyngioma and, 212, 213 diffuse brainstem glioma and, 218, 219, 221 obstructive hydrocephalus and, 14–15 bathrocephaly, 73–75, 76 benign coccygeal dimple, 48 benign sacral dimple, 47 bFFE (balanced fast field echo), for obstructive hydrocephalus, 12
281
2 8
Index
bicoronal incision in sagittal synostosis, 78–79 in unicoronal synostosis, 88 bifrontal craniotomy in nasal dermoid, 261–62 in unicoronal synostosis, 88 birth defects, fatal, 66–67 bladder dysfunction lipomyelomeningocele and, 42, 45 tethered spinal cord and, 36–37 Blake’s pouch cyst, 239–40 bony spina bifida occulta, 33 bowel dysfunction, 42 brainstem gliomas. See also diffuse brainstem glioma location, 218 mutation spectrums of, 219 pathologic-anatomic correlation, 217 braintumors.Seecraniopharyngioma;diffusebrainstemglioma; medulloblastoma;mesialtemporalglioma;pineal tumor cardiomegaly, 158 central nervous system neoplasm, 188 cerebral palsy (CP). See also spastic quadriplegia with dystonia due to cerebral palsy post-hemorrhagic hydrocephalus and, 21–22 right hemispheric CP, 127 toe walking in, 31–32 cerebrospinal fluid (CSF) communicating hydrocephalus and, 2–3, 4, 5, 6, 7–8 hydrocephalus and, 2 obstructive hydrocephalus and, 13, 14, 16, 17, 190–15 posterior fossa cyst with hydrocephalus and, 240 post-hemorrhagic hydrocephalus and, 23–24 cervical collars (cervical orthosis) in atlanto-axial dislocation, 103–5, 106 cervical hydromyelocele, 248–49 cervical instability in atlanto-axial dislocation, 101–3, 107 in Chiari I malformation, 57–59, 60, 62, 63 cesarean section birth, 94 chemotherapy for hypothalamic-chiasmatic glioma, 190 for medulloblastoma, 181–82, 183, 184, 185 for pineal tumor, 168, 174 Chiari I malformation dermal sinus tract and, 49
282
MRI for, 58, 60–61 spinal dysraphism and, 42, 49 tethered spinal cord and, 32, 33, 37 Chiari and Syringomyelia Foundation, 63 Chiari I malformation with syringomyelia, 57–64 aftercare, 61–62 assessment and planning, 57–59 complications and management, 61, 62 CSF leak, 62 neurological injury, craniocervical instability, 62 pain, 62 diagnostic pearls, 58 differential diagnosis, 58 evidence and outcomes, 63 extradural Chiari decompression and, 64 pivot points, 64 preoperative surgical decisions indications for surgery, 59 risk factors, 60 type of surgery, 59–60 subacute/late recurrences, causes of, 63 bone formation, 63 intradural adhesions, 63 subtle craniocervical instability, 63 surgery failure, causes, 63 associated CSF hydrodynamic problems, 63 inaccurate diagnosis, 63 inadequate surgical decompression, 63 surgery failure, consequences, 62 surgical procedure positioning, 60 technical details, 60–61 type, 60 surgical procedure, preoperative decisions risk factors, 60 type of surgery, 59–60 Chiari II malformation, 65, 67, 70 Chiari III malformation, 248–49 Children’s Oncology Group Study (ACNSO122), 168 chordoma, 207 choriocarcinoma, 169 choroidal vein of Galen malformations, 157, 158, 159, 161 choroid plexus catheterization (CPC), 4 choroid plexus papilloma, 3, 177, 224 chronic (slow progression) hydrocephalus, 3 CIM. See Chiari I malformation
Index
club foot deformity, 65 coagulopathy, 96, 97 colloid cysts, 233 communicating hydrocephalus (CHC), 1–8 antibiotic therapy for, 6–8 assessment and planning, 1 CT scan for, 1–2, 7 decision making, 4 differential diagnosis, 3 endoscopic third ventriculostomy for, 4 evidence and outcomes, 8 MRI for, 1–2, 3, 7 noncommunicating hydrocephalus comparison, 3 pivot points, 6 shunting, 4–5 aftercare, 6 complications and management, 7 intracranial hemorrhage and, 8 malfunctioning of shunts, 7 overdrainage/intracranial hypotension and, 8 VP shunt X-ray series, 6 signs and symptoms, 1–2 surgical procedure, 4–5 computed tomography (CT) scan arachnoid cyst contents, 233 for communicating hydrocephalus, 1–2, 7 for craniopharyngioma, 210 for nasal dermoid, 259–60, 263 for posterior fossa ependymoma, 223–24 for sinusitis with subdural empyema, 268 “cone-shaped” head, 83 Congress of Neurological Surgeons (CNS), 22 Conquer Chiari, 63 conus medullaris dermoid, 53 conus medullaris-proximal filum cyst, 37 conus medullaris termination, 36 coronal synostosis. See unicoronal synostosis cortical dysplasia, 129–30 diffuse hemispheric cortical dysplasia, 130 hemispheric disconnection and, 138 non-enhancing mesial temporal lesion and, 199 cranial nerve VI, VII, XII palsy, 228 cranial orthotic therapy, for sagittal synostosis, 76, 79 craniectomies, for sagittal synostosis, 77, 81 craniocervical injury, in atlanto-axial dislocation, 104 craniocervical junction anomalies, 58
craniopharyngioma, 207–16 aftercare, 214 assessment and planning, 207–9 case presentation, 207 complications, 214–15 CT scan for, 210 cysts, 233 decision making, 210–11 diagnostic pearls, 210 differential diagnosis, 207 evidence and outcomes, 213, 216 intracystic therapy for, 210–11 management, 213, 214–15 MRI for, 207, 208–9 pivot points, 214 risk factors, 214, 215 surgical options, 210–13 approach selection decision, 213 craniotomy open approach, 211 expanded endonasal approach (EEA), 211 craniosynostosis helmet therapy for, 86, 89 incidence data, 84 craniotomy with fenestration, for middle fossa arachnoid cysts, 235–36, 237 CSF cerebrospinal fluid (CSF) CIM with syringomyelia and, 58, 62, 63, 73, 109–60 Dandy-Walker Malformation and, 240 dermal sinus tract and, 50, 53 diffuse brainstem glioma and, 218, 221 hemispherotomy and, 137–38 inflicted traumatic brain injury and, 96 lipomyelomeningocele and, 44, 45 medulloblastoma and, 179, 180–81, 182–83, 184 myelomeningocele and, 65–66 nasal dermoid and, 263–64 occipital encephalocele and, 249, 251–52, 253 spastic quadriplegia and, 112, 113, 114–15, 116 CSF-content cysts, 233 cystic sellar tumor, 208–9 cystoperitoneal shunting, for middle fossa arachnoid cysts, 236, 237 Dandy-Walker Malformation, 240, 241 dermal sinus tract aftercare, 53
283
4 8 2
Index
dermal sinus tract (Cont.) assessment and planning, 47–48, 49 complications and management, 53–54 decision making, 50 differential diagnosis, 47 evidence and outcomes, 54 pivot points, 53 surgical procedure, 50, 51–52 dermoid cyst. See also nasal dermoid craniopharyngioma and, 207 differential diagnosis, 233 myelomeningocele and, 68, 69, 71 desmoplastic medulloblastoma, 179–80 detrusor-sphincter dyssynergia, 36–37 diffuse brainstem glioma, 217–22 aftercare, 221 assessment and planning, 218–19 case presentation, 217 complications, 221 diagnostic pearls, 217 differential diagnosis, 218 diffuse tensor imaging, 219, 220 endoscopic third ventriculostomy for, 218 evidence and outcomes, 222 hydrocephalus with, 219 imaging modalities, 218, 219, 220 management, 220, 221 MRI for, 218 pivot points, 221 surgical procedure, 219–20 diffuse hemispheric cortical dysplasia, 130 diffuse pontine gliomas (DIPG), 218, 219, 220, 222 diffuse tensor imaging (DTI), for diffuse brainstem glioma, 219, 220 dimples benign coccygeal dimple, 48 lumbosacral dimple, 48 disconnective technique, PIH procedure, 131, 133–38 dolichocephaly of prematurity, 76 Down syndrome, 248–49 drug-resistant epilepsy, 127–28 dyspraxia, inflicted traumatic brain injury and, 96 dysraphic sacral dimple, 47 dystonia, spastic quadriplegia and, 109 electroencephalography (EEG) inextratemporalrefractoryepilepsy, 117–18,119–20, 121–23
284
in hemispheric refractory epilepsy, 127, 129, 130 in inflicted brain injury, 93–94, 97–98 in mesial temporal glioma, 199, 201, 202, 204 in moyamoya disease, 152–53, 154 embryonal carcinoma, 169 encephaloduroarteriosynangiosis (EDAS) surgery, for moyamoya disease encephalomalacia, 200–1 endoscopic fenestration, for middle fossa arachnoid cysts, 235, 236, 237 endoscopic techniques. See also endoscopic third ventriculostomy in sagittal synostosis, 76–79, 81 endoscopic third ventriculostomy (ETV) for congenital communicating hydrocephalus, 4 for diffuse brainstem glioma, 218 for obstructive hydrocephalus, 6, 13, 14 for pineal tumor, 165–66, 174 posterior fossa cyst and hydrocephalus and, 241–42 post-hemorrhagic hydrocephalus and, 24, 26 endoscopic third ventriculostomy (ETV), with choroid plexus cauterization (CPC)(ETC-CPC) for congenital communicating hydrocephalus, 4 for obstructive hydrocephalus, 6, 13, 16–17 for post-hemorrhagic hydrocephalus, 24, 26 Endoscopic Third Ventriculostomy Success Score (ETVSS), 22 endovascular embolization, for vein of Galen malformation, 159–60 Enterococcus faecalis (E. Faecalis) sepsis, 19 ependymoma, 177, 221 epidermoid cysts, 233 epilepsy.Seealsoextratemporalrefractoryepilepsy;hemispheric refractory epilepsy drug-resistant epilepsy, 127–28 focal epilepsy, 117, 119 intractable epilepsy, 129–30, 131, 138–39, 163, 203 medically refractory epilepsy, 117–18, 124, 127–28 treatment history, 131 unilateral refractory epilepsy, 138 exotropia, inflicted traumatic brain injury and, 96 extratemporal refractory epilepsy, 117–24 aftercare, 121–23 assessment and planning, 117–19 case presentation, 117 complications, 124 decision making, 119–20
Index
diagnostic pearls, 119 EEG for, 117–18, 119–20, 121–23 evidence and outcomes, 124–25 focal cortical dysplasia and, 117–18, 119, 120, 121–23 magnetoencephalography for, 118–19 management, 124 MRI for, 117, 118–19, 120–21 pivot points, 124 SPECT for, 118–19 surgical procedure, 120 extratemporal seizures, 117–18, 119, 120, 121–23, 124–25 fibroblast growth factor receptor 2 (FGFR2) mutations, 84, 86 FIESTA (fast imaging employing steady-state acquisition) for obstructive hydrocephalus, 12 filum terminale lipoma dermal sinus tract and, 47 tethered spinal cord and, 32, 33, 36 filum terminale transection for tethered spinal cord, 35–36, 38 FLAIR fluid-attenuated inversion recovery (FLAIR) signal craniopharyngioma and, 210 flap necrosis, 45 flexion-distraction mechanism, role in AODs, 103 focal cortical dysplasia, 117–18, 119, 120, 121–23 focal epilepsy, 117, 119 Foley catheter dermal sinus tract and, 51, 53 filum terminale transection and, 35, 37 lipomyelomeningocele and, 43, 45 fronto-orbital advancement (FOA) for unicoronal synostosis, 86–88 forehead hemangioma, 257 gait abnormalities, 34 ganglioglioma, 219 gastroesophageal reflux disease, 93–94 germ cell tumors. See also pineal tumor choriocarcinoma, 169 embryonal carcinoma, 169 germinoma, 169, 173, 174 mixed germ cell tumors, 169 teratoma, 169, 173, 174 yolk sac tumor, 169 germinal matrix hemorrhage, 20, 23
germinoma craniopharyngioma and, 207 pineal gland tumor and, 169, 173, 174 gliomas. See also diffuse brainstem glioma; hypothalamic- chiasmatic glioma; mesial temporal glioma brainstem gliomas, 217, 218–19 cervicomedullary glioma, 217 differential diagnosis, 225 ganglioglioma, 219 high-grade astrocytoma, 12 hydrocephalus and, 12–13 midline gliomas, 219 nasal glioma, 260 oligodendroglioma, 219 optic pathway glioma, 207 pontine glioma, 217 tectal glioma, 12–13, 217 glioneuronal tumor, 199 gluteal clefts, asymmetric, 41 gram-negative bacillus, 7–8 hairy patches, 41 hamartoma, 207 harlequin eye deformity, in unicoronal synostosis, 84, 88 headaches arachnoid cysts and, 233–34 Chiari I malformation with cervical syringomyelia and, 57, 59, 62, 63 communicating hydrocephalus and, 4, 8 craniopharyngioma and, 208 diffuse brainstem glioma and, 217 hypothalamic-chiasmatic glioma and, 187, 188 lipomyelomeningocele and, 41, 45 lumbar pseudomeningocele and, 37 medulloblastoma and, 177, 178, 180–81, 184 migraine-associated disorders, 129 moyamoya disease and, 149–50, 151 obstructive hydrocephalus and, 11 pineal tumor and, 165, 166 posterior fossa ependymoma and, 223 progressive hydrocephalus and, 3 ruptured arteriovenous malformation and, 141, 144 sinusitis with subdural empyema and, 267 slit-ventricle syndrome and, 8 spastic quadriplegia and, 114 VP shunts and, 8
285
6 8 2
Index
head trauma. See inflicted traumatic brain (ITB) injury helmet therapy for craniosynostosis, 86, 89 for sagittal synostosis, 76, 79–80 hemangioblastomas, 219, 225 hemangiomas lipomyelomeningocele and, 41, 42, 45, 48–49 nasal dermoid and, 257 right-sided forehead, 257 spinal cord tethering and, 32–33 hemimegalencephaly, 130, 137, 138 hemiplegia maximal/near maximal, with intractable epilepsy, 138–39 hemispherectomy, 129 hemispheric refractory epilepsy, 127–38 assessment and planning, 127–28 case presentation, 141 complications, 138 decision making, 129–30 diagnostic pearls, 129 differential diagnosis, 129 EEG for, 127, 129, 130 evidence and outcomes, 138 magnetoencephalography for, 129 MRI for, 128, 129, 137–38 patient selection, 130 peri-insular hemispherotomy (PIH) procedure, 131, 133–37 disconnective technique, 131, 133–38 incision, craniotomy, dural opening, 132 postoperative management, 137 7-step surgical approach, 133–36 perinatal conditions, 130 SPECT for, 129 hemispheric syndrome, 130 hemispherotomy. See also peri-insular hemispherotomy peri-insular hemispherotomy, 131 post-hemispherotomy hydrocephalus, 138 for refractory hemispheric epilepsy, 129 technique description, 131 hydrocephalus. See also communicating hydrocephalus; obstructive hydrocephalus; posterior fossa cyst with hydrocephalus acute hydrocephalus, 3 Chiari I malformation and, 58, 60, 62, 63, 64 endoscopic third ventriculostomy option, 22
286
hydrocephalus ex-vacuo, 3 medical management, 19 medulloblastoma and, 104, 178, 179, 181, 182, 183, 184 myelomeningocele and, 66, 67–68, 70, 71 pineal tumor and, 165–66, 169 post-hemispherotomy hydrocephalus, 138 post-hemorrhagic hydrocephalus, 20, 21–22 progressive, and spinal dysraphism, 70 slowly developing, and VOGM, 162 spinal dysraphism and, 70 steps for diagnostic accuracy, 22 tectal glioma and, 12–13 Hydrocephalus Clinical Research Network, 28 hypospadias, 1 hypothalamic-chiasmatic glioma, 187–94 aftercare, 193 assessment and planning, 187 case presentation, 187 complications, 193 decision making, 189 diagnostic pearls, 188 MRI classifications, 188, 189 neuro-endocrine, 188 neurology, 188 neuro-ophthalmology, 188 NF-1, 188 evidence and outcomes, 193–94 management biopsy at diagnosis, 190 chemotherapy, 190, 193 endoscopic biopsy with septostomy, 190 primary tumor resection, 190 radiotherapy, 190, 193 VP-shunt placement, 190, 193 wait/watch/rescan policy, 189 MRI for, 188, 189, 190, 192, 193 pivot points, 190 suprasellar tumors and, 188 surgical procedure, 190–93 hypothalamic glioma, 207 iatrogenic hygroma, 236 infant cardiac failure, in vein of Galen malformations, 157–58, 159, 161, 162, 163 Infant Face Scale scoring, 94 inflicted traumatic brain (ITB) injury, 93–99
Index
assessment and planning, 96 decision making, 96–97 diagnosis, 95, 97 differential diagnosis, 96 EEG for, 93–94, 97–98 evidence and outcomes, 99 management, 99 MRI for, 96–97, 98–99 seizures and, 93–94, 96, 97–98, 99 subdural hematoma and, 95, 96–97, 98, 100 inflicted traumatic brain (ITB) therapy for spastic quadriplegia with dystonia due to cerebral palsy, 110, 111, 113, 114, 115–16 withdrawal management, 115 International League Against Epilepsy (ILAE), 127–28 intracranial dermoid cysts, 260 intracranial hemorrhage (ICH) ruptured arteriovenous malformation and, 143 as shunting placement complication, 8 vein of Galen malformations and, 163 intracranial pressure (ICP) brainstem gliomas and, 218 effectiveness of shunts in reducing, 4 inflicted traumatic brain injury and, 96, 100 myelomeningocele and, 65, 66 obstructive hydrocephalus and, 11, 13 posterior fossa ependymoma and, 223 ruptured arteriovenous malformation and, 143 fromshuntingincongenitalcommunicatinghydrocephalus, 8 sinusitis with subdural empyema and, 270, 271 intractable epilepsy, 129–30, 131, 138–39, 163, 203 intraventricular hemorrhage (IVH), 19 MRI diagnosis, 23 post-hemorrhagic hydrocephalus and, 20, 22 risk factors, 21–22 ischemic stroke, 149, 150–51 Joint Guidelines Committee of the Congress of Neurological Surgeons (CNS), 22 kyphoscoliosis, 69 kyphosis, 67, 69 lambdoid synostosis, 84 laminoplasty dermal sinus tract and, 51, 52, 53, 54
lipomyelomeningocele and, 44, 45 tethered cord syndrome and, 34, 35–36 leptomeningeal cysts, 233 Lhermitte-Duclos disease, 177 limb length discrepancy, 31–32 lipomyelomeningocele (LMMC) aftercare, 45 assessment and planning, 41, 42 complications and management, 45 decision making, 43 differential diagnosis, 41 dorsal/transitional/caudal (terminal), 43 evidence and outcomes, 148 MRI for, 42, 43, 45 pivot points, 45 surgical procedure, 43–44 lumbar hemangiomata, 32–33 lumbar myelomeningocele, 65, 66 lumbar pseudomeningocele, 53, 54 lumbar pseudomeningocele with headache, 37 lumbosacral fat pads, 41 lumbosacral pits and dimples, 32–33, 48 benign coccygeal dimple, 48 lumbosacral dimple, 48 pits or tracts, 48–49 lymphoma, 219 macrocephaly communicating hydrocephalus and, 1–2 obstructive hydrocephalus and, 11 prematurity/intraventricular hemorrhage and, 28 slowly developing hydrocephalus, VOGM, and, 162 spastic quadriplegia and, 109–10 magnetic resonance imaging (MRI) for Chiari I malformation, 58, 60–61 for communicating hydrocephalus, 1–2, 3, 7 for craniopharyngioma, 207, 208–9 for diffuse brainstem glioma, 218 for extratemporal refractory epilepsy, 117, 118–19, 120–21 for hemispheric refractory epilepsy, 128, 129, 137–38 for hypothalamic-chiasmatic glioma, 188, 189, 190, 192, 193 for inflicted traumatic brain injury, 96–97, 98–99 for lipomyelomeningocele, 42, 43, 45 for medulloblastoma, 177, 178, 179–81, 183, 184 for mesial temporal glioma, 160, 199, 200, 201, 203, 204 for moyamoya disease, 149–50, 151, 155
287
82
Index
magnetic resonance imaging (MRI) (Cont.) for myelomeningocele, 65, 70, 71 for nasal dermoid, 257, 259–60, 263, 264 for obstructive hydrocephalus, 12, 13, 16, 103 for occipital encephalocele, 244–52, 253 for pineal tumor, 165, 166, 169, 170 for posterior fossa cyst with hydrocephalus, 239, 240–41, 244 for posterior fossa ependymoma, 223–24 for post-hemorrhagic hydrocephalus, 22, 23 for ruptured arteriovenous malformation, 141, 143, 147 for sinusitis with subdural empyema, 268 for spastic quadriplegia, 110 for spinal dermal sinus tract, 49, 50, 53 for suprasellar tumors, 188, 189 for traumatic atlanto-axial dislocation, 101, 103, 104 for vein of Galen malformation, 158 for ventricular shunt infection, 276 magnetic resonance venogram (MRV) for occipital encephalocele, 248 magnetoencephalography (MEG) for extratemporal refractory epilepsy, 118–19 for hemispheric refractory epilepsy, 129 for mesial temporal glioma, 199 medulloblastoma (MB), 177–85 aftercare, 184 assessment and planning, 177 case presentation, 177 chemotherapy for, 181–82, 183, 184, 185 complications, 184 decision making, 181–82 desmoplastic medulloblastoma, 179–80 diagnostic pearls, 178–79 differential diagnosis, 177, 225 evidence and outcomes, 178, 185 high-risk medulloblastoma, 185 hydrocephalus and, 104, 178, 179, 181, 182, 183, 184 imaging findings, 179–81 leptomeningeal dissemination and, 185 management, 183, 184 molecular subgroups, 181–82 MRI for, 177, 178, 179–81, 183, 184 pivot points, 183 risk factors, 182 surgical procedure, 182–83 WHO grade IV embryonal tumor, 181 mega cisterna magna, 239–40 meningioma, 207 288
meningitis Chiari I surgical failure and, 62 dermal sinus tract and, 49, 50, 54 nasal dermoid and, 257–58 post-hemorrhagic hydrocephalus and, 24, 27 tethered cord syndrome and, 31–32, 38 mesial temporal glioma, 199–205 aftercare, 204 assessment and planning pre-operative imaging, 201 timing of surgery, 201 case presentation, 199 complications, 204–5 decision making, 201 tumor location, dominant vs. nondominant hemisphere, 201 diagnostic pearls, 200 EEG for, 199, 201, 202, 204 evidence and outcomes, 205 magnetoencephalography for, 199 management, 203–5 MRI for, 160, 199, 200, 201, 203, 204 pivot points, 204 SPECT for, 199–200 surgical procedure, 202 medial structures resection, 203 operative management, 203 work-up, 199 metabolic disorders, 96, 97–98 metopic synostosis, 84 micrognathia, 1 middle cerebral artery occlusion, 130 middle fossa arachnoid cyst, 231–37. See also posterior fossa cyst with hydrocephalus assessment and planning, 231–32 case presentation, 231 complications, 237 decision making, 233–35 diagnostic pearls, 233 differential diagnosis, 233 management, 236, 237 pivot points, 236–37 primary locations, 236 surgical procedures, 235–36 aftercare, 237 craniotomy with fenestration option, 235–36, 237 cystoperitoneal shunting, 236, 237
Index
endoscopic fenestration option, 235, 236, 237 recommendations, 236 migraine-associated disorders, 129 minimally invasive procedures in congenital communicating hydrocephalus, 5 in hypothalamic-chiasmatic glioma, 194 in sagittal synostosis, 76–77, 81 motor vehicle accident. See traumatic atlanto-axial dislocation movement disorders, 129 moyamoya disease, 149–56 assessment and planning, 149–53 at-risk populations, 150–51 case presentation, 149 complications, 155 decision making, 151 diagnostic pearls, 150–51 EEG for, 152–53, 154 evidence and outcomes, 156 genetic mutation links, 151 ischemic stroke and, 149, 150–51 management, 154, 155 MRI for, 149–50, 151, 155 perioperative stroke risk factors, 155 pivot points, 154 risk factors arteriopathy of posterior circulation, 156 ischemic damage from progressive arteriopathy, 156 perioperative stroke, 155 SPECT for, 150 surgical procedure, 152 aftercare, 155 direct bypass approach, 152 encephaloduroarteriosynangiosisvs.pialsynangiosis, 152 goal of, 152 incision/surgical steps, 153–54 indirect bypass approach, 152 patient positioning, 153 Muenke syndrome, 84, 86 mural vein of Galen malformations, 157, 159 muscular dystrophy, 31–32 myelomeningocele, 65–7 2.Seealsolumbarmyelomeningocele aftercare, 69–70, 71 assessment and planning, 65–66 complications, 70–71 decision making, 67 diagnostic pearls, 67
evidence and outcomes, 72 management, 69, 70–71 MRI for, 65, 70, 71 neural tube defects and, 66, 67, 69 pivot points, 69 risk factors, 67–69, 71 surgical procedure, 68–69 nasal dermoid, 257–65 aftercare, 263–64 assessment and planning, 257–60 case presentation, 257, 258, 259 complications, 264 CT scan for, 259–60, 263 decision making, 261 diagnosis, 257–61 differential diagnosis, 257–58, 260 evidence and outcomes, 265 management, 264 MRI for, 257, 259–60, 263, 264 pivot points, 263 surgical technique, 261–62 treatment, 262–63 nasal glioma, 260 nasofrontal (sincipital) encephaloceles, 257–58, 260 neural tube defects, 66, 67, 69, 73 neurocognitive decline, 11 neuroepithelial cysts, 233 noncommunicating hydrocephalus, 3 non-hypertrophicdiffusehemisphericmigrationaldisorder, 130 nonsyndromic synostosis, 91 obstructive hydrocephalus, 6, 11–17 aftercare, 16 assessment and planning, 11 complications and management, 16 decision making, 13 diagnostic pearls, 13 differential diagnosis, 11 endoscopic third ventriculostomy for, 6, 13, 14, 16–17 evidence and outcomes, 17 medulloblastoma and, 178, 179 MRI for, 12, 13, 16, 103 pivot points, 16 posterior fossa ependymoma and, 224 surgical procedure, 13, 14–15 occipital encephalocele, 247–54 289
0 9 2
Index
aftercare, 252 assessment and planning, 248–49 complications, 253 decision making, 250 diagnostic pearls, 250–51 evidence and outcomes, 253–54 magnetic resonance venogram for, 248 management, 252, 253 MRI for, 244–52, 253 pivot points, 253 surgical procedure, 251–52 occipitocervical (OC) fusions, 106 occult dysraphism, 110 oligodendroglioma, 219 optic pathway glioma, 207 orbital osteotomies, 88 papilledema, 11 obstructive hydrocephalus and, 11, 13 pineal tumor and, 165 papilloma, 225 parafalcine empyemas, 271 parenchymal lesions, 97 paroxysmal movement disorders, 129 patent ductus arteriosus, 19 peri-insular hemispherotomy (PIH) procedure, 131, 133–37 disconnective technique, 131, 133–38 incision, craniotomy, dural opening, 132 postoperative management, 137 7-step surgical approach, 133–36 perinatal hemispheric infarct, 130, 138 perioperative stroke risk factors in moyamoya disease, 155 periventricular leukomalacia (PVL), 22 persistent mendosal suture, 76 pilocytic astrocytoma, 225 pineal gland, 165, 167. See also pineal tumor pineal parenchymal tumors, 168 pineal tumor, 165–73 aftercare, 171, 173 assessment and planning, 167–69 case presentation, 165, 166 chemotherapy for, 168, 174 complications, 173 diagnostic pearls, 168–69 endoscopic third ventriculostomy for, 165–66, 174
290
hydrocephalus and, 165–66, 169–74 management, 174 MRI for, 165, 166, 169, 170 pivot points, 172 surgical procedure infratentorial supracerebellar approach, 172, 173 occipital transtentorial approach, 172, 173 tumor resection, 169, 170–71 pineoblastoma, 171–72 pituitary adenoma, 207 porencephalic cysts, 233 positron emission tomography (PET) for extratemporal refractory epilepsy, 118–19 for hemispheric refractory epilepsy, 128, 129 for mesial temporal glioma, 199–200 posterior fossa arachnoid cysts, 239–40 posterior fossa cyst with hydrocephalus, 239–45. See also middle fossa arachnoid cyst aftercare, 243–44 assessment and planning, 239–41 Blake’s pouch cyst and, 239–40 case presentation, 239, 240 complications, 244 Dandy-Walker Malformation and, 240, 241 decision making, 241, 242 diagnostic pearls, 241 endoscopic third ventriculostomy for, 241–42 fenestration and, 241, 242, 243, 244 management, 243, 244 mega cisterna magna and, 239–40 MRI for, 239, 240–41, 244 pivot points, 243 surgical procedure, 242–43 posterior fossa ependymoma assessment and planning, 223–24 case presentation, 223 complications, 227–29 CT scan for, 223–24 decision making, 224 differential diagnosis, 225 evidence and outcomes, 229 management, 227–29 MRI for, 223–24 pivot points, 229 surgical procedure, 225 aftercare, 227
Index
positioning/surgery pearls, 226–22 posterior fossa subdural empyemas, 271 posterior fossa syndrome, 228 post-hemispherotomy hydrocephalus, 138 post-hemorrhagic hydrocephalus, 22, 23 post-hemorrhagic hydrocephalus (PHH) cerebrospinal fluid and, 23–24, 268 complications and management, 27–28 diagnosis, 20 endoscopic third ventriculostomy and, 24, 26 evidence and outcomes, 28 evidence-based treatment guidelines, 28 management, 26, 27 MRI for, 22, 23 periventricular leukomalacia and, 22 surgical procedure, 24–26 aftercare, 27 permanent CSF diversion, 24, 26 pre-surgical planning, 24 temporary CSF diversion, 24–26 treatment recommendations, 22 ventricular reservoirs and, 26 ventriculoperitoneal shunt placement and, 26 ventriculo-subgaleal shunts and, 26 prematurity and intraventricular hemorrhage, 19–28. See also post-hemorrhagic hydrocephalus aftercare, 27 assessment and planning, 19–23 case presentation, 19 complications and management, 27–28 decision making, 23–24 evidence and outcomes, 28 surgical procedure, 24–26 permanent CSF diversion, 24, 26 temporary CSF diversion, 24–26 primitive neuroectodermal tumor (PNET), 181, 219 pseudomeningocele, 53, 54, 62, 228 pseudotumor cerebri, 62 pulmonary embolization, for vein of Galen malformation, 163 pulmonary hypertension, 158 radiotherapy for diffuse brainstem glioma, 221 for hypothalamic-chiasmatic glioma, 190 stereotactic radiotherapy, for VOGM, 159 Rasmussen’s encephalitis, 129–30, 138
Rathke’s cleft cyst, 207, 233 refractory epilepsy. See extratemporal refractory epilepsy; hemispheric refractory epilepsy right hemispheric cerebral palsy, 127 ruptured arteriovenous malformation. See arteriovenous malformation (ruptured AVM) Saethre-Chotzen syndrome, 84, 86 sagittal synostosis, 73–81 aftercare, 79–80 assessment and planning, 73–75 bathrocephaly and, 73–75, 76 complications, 80 decision making, 75–76 diagnostic pearls dolichocephaly of prematurity, 76 persistent mendosal suture, 76 sagittal craniosynostosis, 76 evidence and outcomes, 81 helmet therapy for, 76, 79–80 incidence data, 84 management, 78, 80 persistent mendosal suture, 76 pivot points, 78–79 surgical procedure, 76, 77–78 scaphocephaly, 73–75 scoliosis, 109 sebaceous cysts, 257–58 seizures. See also status epilepticus anoxic seizures, 129 differential diagnosis, 129 extratemporal seizures, 117–18, 119, 120, 121–23, 124–25 inflicted traumatic brain injury and, 93–94, 96, 97–98, 99 ipsilateral temporal lobe origin, 199 tonic clonic, 267 seromas, 114 shunts (shunting). See also ventricular shunt infection; ventriculoperitoneal (VP) shunt in concomitant abdominal congenital malformations, 6 in congenital communication hydrocephalus, 4–5 cystoperitoneal, in middle fossa arachnoid cysts, 237 in myelomeningocele, 67–68, 70 in occipital encephalocele, 251, 252–53, 254 surgical procedure, 68–69 single photon emission coherent tomography (SPECT)
291
2 9
Index
for extratemporal refractory epilepsy, 118–19 for hemispheric refractory epilepsy, 129 for mesial temporal glioma, 199–200 for moyamoya disease, 150 single suture synostosis, 84, 86. See also unicoronal synostosis sinusitis with subdural empyema, 267–73 aftercare, 272 assessment and planning, 267 case presentation, 267 complications, 272 CT scan for, 268 decision making, 268–70 diagnostic pearls, 267–68, 269, 270 differential diagnosis, 267 evidence and outcomes, 273 management, 271, 272 MRI for, 268 pivot points, 271 surgical procedure, 270–71 sinus pericranii, 260 slit-ventricle syndrome, 8 Sonic hedgehog (Shh) pathway, medulloblastoma subgroup, 181–82 spasticity. See spastic quadriplegia with dystonia due to cerebral palsy spastic quadriparesis, 110, 111, 112 spasticquadriplegiawithdystoniaduetocerebralpalsy, 109–16 aftercare, 114–15 assessment and planning, 109–10 baclofen withdrawal syndrome and, 115, 116 case presentation, 109 complications, 116 decision making, 111 diagnostic pearls, 110 differential diagnosis, 109–10 ITB therapy for, 110, 111, 113, 114, 115–16 management, 113 pivot points, 114 surgical procedure, 111–13 SPECT. See single photon emission coherent tomography spinal cord tethering, 32, 33, 59–60. See also tethered cord syndrome spinal dysraphism hydrocephalus and, 70 lipomyelomeningocele and, 41, 42 progressive hydrocephalus and, 70
292
spinal cord tethering and, 31, 33, 41, 42 syringomyelia and, 42, 49 spinal hemangiomata, 32 spinal skin tags, 32–33 spondylolisthesis, mild grade 1, 31, 32, 34 Staphylococcus aureus, 7–8 Staphylococcus epidermidis, 7–8 static encephalopathy, 110 status epilepticus, 93–94 ABCs for, 96 management of, 99 recognition difficulties, 97 stereotactic radiotherapy for vein of Galen malformation, 159 stigmata of dysraphism, external, 32 Sturge Weber syndrome, 129–30, 138 subarachnoid hemorrhage, 97 subdural empyema. See sinusitis with subdural empyema subdural hematoma congenital communicating hydrocephalus and, 8 inflicted traumatic brain injury and, 95, 96–97, 98 subgaleal hematoma inflicted traumatic brain injury and, 98 subperiosteal dissection in craniopharyngioma, 213 in craniosynostosis, 88 in sagittal synostosis, 77–78 in spastic quadriplegia, 113 suprasellar tumors, 187, 188, 207, 208–9 See also craniopharyngioma; hypothalamic-chiasmatic glioma MRI for, 188, 189 syncope, 129 synostosis. See also sagittal synostosis; unicoronal synostosis incidence/types of, 84 lambdoid synostosis, 84 metopic synostosis, 84 non-syndromic synostosis, 91 single suture synostosis, 84, 86 syringobulbia, 58, 61 syringomyelia dermal sinus tract and, 49 myelomeningocele and, 67 spinal dysraphism and, 42, 49 systemic hypertension, 158 tectal glioma, 12–13, 217
Index
teratoid-rhabdoid tumor, atypical, 219, 225 teratoma, 169, 173, 174 tethered cord syndrome aftercare, 37 assessment and planning, 31–32, 33 complications and management, 37–38 decision making, 34 diagnosis, 31–32, 33 evidence and outcomes, 38 myelomeningocele and, 67 pivot points, 36–37 surgical procedure, 35–36, 38 types of symptoms, 36 tethered spinal cord. See tethered cord syndrome toe walking, 31–32 tonic clonic seizures, 267 transarterial embolization for vein of Galen malformation, 159, 160, 161–62 traumatic atlanto-axial dislocation MRI for, 101, 103, 104 traumatic brain injury (TBI). See inflicted traumatic brain (ITB) injury unicoronal synostosis, 83–91 aftercare, 90 assessment and planning, 83–84 characteristic features, 83–84, 85, 88 complications, 90–91 decision making, 86 diagnostic pearls, 85 evidence and outcomes, 91 fronto-orbital advancement and, 86–88 management, 89, 90–91 surgical procedure, 86–91 unilateral refractory epilepsy, 138 urinary incontinence, 31–32 urinary retention dermal sinus tract and, 53 post-operative, in tethered spinal cord, 37 vascular infarct, perinatal, 130 vascular malformation, 200–1 vein of Galen malformation (VOGM), 157–63 arteriovenous fistulas and, 157, 159, 161 assessment and planning, 157–58 case presentation, 157
choroidal type VOGMs, 157, 158, 159, 161 complications, 163 decision making, 159, 160 diagnostic pearls, 159 embolization endovascular, 159–60 pulmonary, 163 transarterial embolization, 159, 160, 161–62 evidence and outcomes, 163 infant cardiac failure and, 157–58, 159, 161, 162, 163 malformation categories choroidal, 157, 158, 159, 161 mural, 157, 159 management, 162, 163 MRI for, 158 mural type VOGMs, 157, 159 pivot points, 162 stereotactic radiotherapy for, 159 surgical procedure, 161 transarterial embolization for, 159, 160, 161–62 vein of Markowski, 157 ventricular shunt infection, 275–79 aftercare, 278 assessment and planning, 275–76 case presentation, 275 complications, 279 decision making, 276–77 diagnostic pearls, 275 evidence and outcomes, 279 management, 278, 279 MRI for, 276 pivot points, 278 surgical procedure, 277 ventriculomegaly, 1 communicating hydrocephalus and, 1–2, 3, 4, 6 myelomeningocele and, 65 obstructive hydrocephalus and, 11 post-hemorrhagic hydrocephalus and, 23 prematurity, intraventricular hemorrhage, and, 19, 20–21 ventriculoperitoneal (VP) shunt communicating hydrocephalus and, 1, 4–5, 6, 8 diffuse brainstem glioma and, 219, 221 obstructive hydrocephalus and, 12, 13, 14–15, 17 in occipital encephalocele, 254 posterior fossa cyst and hydrocephalus and, 241–42 posterior fossa cysts and, 225–26
293
4 9 2
Index
ventriculoperitoneal (VP) shunt (Cont.) post-hemorrhagic hydrocephalus and, 21–22, 26 ventriculo-subgaleal shunts (VSGs), 26 video-encephalography for hemispheric refractory epilepsy, 130 for mesial temporal glioma, 199 vision changes craniopharyngioma and, 210 obstructive hydrocephalus and, 11 Von Hippel-Lindau disease, 219
294
wedge osteotomy, 88 Wingless (Wnt) pathway, medulloblastoma subgroup, 181–82 World Health Organization (WHO) brain tumor classification, 219 cervicomedullary glioma classification, 217 ependymoma classification, 227 pontine glioma classification, 217 yolk sac tumor, 169
6 9 2
8 9 2
03