Dealing with Depression : Five Pastoral Interventions 9781317763970, 9781560249337
This important book explores strategies to enable clergy and lay persons to identify and help individuals suffering from
226 112 2MB
English Pages 194 Year 1995
Polecaj historie










Citation preview
Dealing with Depression Five Pastoral Interventions
This page intentionally left blank
Dealing with Depression Five Pastoral Interventions
Richard Dayringer, ThD with Byron Eicher, MA Myron C. Madden, PhD John J. O'Heame, MD H. Darby Trotter, PhD Morton Jacobs, MD Robert M. Mathews, MD
~ ~~o~~~~n~f{~up New York London
© 1995 by The Haworth Press, Inc. All rights reserved. No part of this work may be reproduced or utilized in any form or by any means, electronic or mechanical, including photocopying, microfilm and recording, or by any information storage and retrieval system, without permission in writing from the publisher.
First published by
The Haworth Pastoral Press, an imprint of The Haworth Press, Inc., 10 Alice Street, Binghamton, NY 13904-1580 This edition published 2012 by Routledge Routledge Taylor & Francis Group 711 Third Avenue New York, NY 10017
Routledge Taylor & Francis Group 27 Church Road, Hove East Sussex BN3 2FA
Dayringer, Richard Dealing with depression five pastoral interventions / Richard Dayringer,with Byron Eicher .. [et al.]. p. em. Includes bibliographical references and index. ISBN 1-56024-967-6 (ISBN-1-56024-933-1 (alk. paper) 1. Depression, Mental-Treatment. 2. Psychotherapy. 3. Depressed persons-Pastoral counseling of. I. Eicher, Byron. II. Title. RC537.D39 1995 616.85'270651--dc20
94-33088 CIP
DEDICATED TO TWO INSTITUTIONS (typical and symbolic of many others) that were interested enough in the topic herein considered and in the professional group to whom the book is addressed to provide time, money, and space for the completion of this endeavor BAPTIST MEDICAL CENTER Kansas City, Missouri and SOUTHERN ILLINOIS UNIVERSITY SCHOOL OF MEDICINE Springfield, Illinois
This page intentionally left blank
CONTENTS Foreword
xiii Robert M. Mathews
Preface
xv
Chapter 1: Recognizing Those Who Are Depressed
1
Richard Dayringer
Chapter 2: Transactional Analysis Dealing with Depression 13 John J. O'Hearn.e Richard Dayringer
Chapter 3: Pastoral Counseling Dealing with Depression Myron C. Madden
27
Richard Dayringer
Chapter 4: Gestalt Therapy Dealing with Depression
41
Byron Eicher Richard Dayringer
Chapter 5: Behavior Therapy in Dealing with Depression
51
H Darby Trotter Richard Dayringer
Chapter 6: Cognitive Therapy Dealing with Depression
71
Richard Dayringer
Chapter 7: Medical-Religious Case Conference
85
Moderator: Robert M. Mathews Presenter: Richard Dayringer
Chapter 8: Clergy Dealing with Depression Richard Dayringer
107
Appendix I: Mood Disorders
127
Appendix II: ManiaIHypomania
145
Appendix III: Pleasant Events Schedule
157
Index
171
ABOUT THE AUTHOR
Richard Dayringer, ThD, is Professor and Director of Psychosocial Care in the Department of Medical Humanities and Professor and Chief of Behavioral Science in the Department of Family and Community Medicine at Southern Illinois University. A pastoral psychotherapist for 30 years, he has worked extensively with more than 100 depressed counselees. Dr. Dayringer has also served as a pastor in Missouri, Kansas, and Louisiana. He is a member of the American Academy of Religion, the American Association for Marriage and Family Therapy, and the American Association of Pastoral Counselors. Other books by Dr. Dayringer include Pastor and Patient (editor) God Cares for You, and The Heart ofPastoral Counseling.
This page intentionally left blank
CONTRffiUTORS Byron Eicher, MA, began private practice as a clinical psychologist in Kansas City in 1970, after receiving his undergraduate and graduate degrees from Memphis State University. Mr. Eicher's internship was completed at Gaylor Psychiatry Hospital at the University of Tennessee School of Medicine. He then received a five-year grant from the National Institute of Mental Health to study psychotherapeutic methods under such leaders as J. L. Moreno, Frederick Perls, Carl Rogers, George Bach, Abraham Maslow, and Albert Ellis. Byron is one of 37 therapists from the Moreno Institute to have been certified at the level of director. He often conducts weekend workshops and has founded the Kansas Institute of Gestalt Therapy and Psychodrama. Morton Jacobs, MD, received his MD from the University of Kansas School of Medicine and was certified as a psychiatrist by the American Board of Psychiatry and Neurology. He is a member of the American Psychiatric Association and for a number of years has been practicing psychiatry from the viewpoint of transactional analysis. Myron C. Madden, PhD, has retired after serving as the Director of the Department of Pastoral Care at Southern Baptist Hospital in New Orleans, Louisiana from 1960 to 1983. He was pastor of St. Charles Avenue Baptist Church in New Orleans prior to that time. A graduate of Louisiana State University, Madden also holds ThM and PhD degrees from Southern Baptist Theological Seminary in Louisville, Kentucky. He is a Chaplain Supervisor in the Association for Clinical Pastoral Education and a Diplomate in the American Association of Pastoral Counselors. Dr. Madden has written five books. Robert M. Mathews, MD, received his MD from the University of Kansas School of Medicine. He has practiced as a general surgeon and is a member of both the American and the International Colleges of Surgeons. He has also served as Director of Education at Baptist Medical Center and is a member of the faculty at the University of Missouri (Kansas City) School of Medicine. Dr. Mathews has been interested in writing for a number of years and has served as the Associate Editor of the International Surgery Journal.
John J. O'Hearne, MD, is in the private practice of psychiatry in Kansas City with his wife, who is also a psychiatrist. He is a graduate of Southwestern University at Memphis and received his MD from the University of Tennessee. Dr. O'Heame is a Fellow of the American Psychiatric Association and the American Orthopsychiatric Association, and in 1974 served as the President of the American Group Psychotherapy Association. He is a certified teaching member of the International Transactional Analysis Association. He is listed in both Who~ Who in America and Who~ Who in the World. In 1992 he also became an Episcopal priest.
H. Darby Trotter, PhD, is a clinical and consulting psychologist in private practice at the Psychological Treatment and Consultation Center' Incorporated, Kansas City. He is a graduate of the University of Houston and has a PhD degree from Texas Technological College. Dr. Trotter has been certified as a psychologist in Kansas and Missouri since 1972. He is a member of the American Psychology Association. He has taught at the University of Kansas and the University of Missouri. He has been quite active with the Boys' Club and the Youth Service System.
Foreword The pervasive problem of depression touches everyone. Some people experience only a mood change, transient and superficial. Others may be totally incapacitated by an oppressive, paralyzing sense of futility and unworthiness. No one is immune from the ravages of depression. The therapist is as much a potential victim as the patient receiving therapy. Therefore, we must approach this problem personally and aggressively wherever we meet it. When we are down and depressed, we must look up if we are to improve. When people are saddled with low moods, it has been my observation that the person with the ability to laugh or smile has a greater recovery potential than the person who for some reason cannot smile at his own frailty or predicament. A sense of humor and the ability to laugh at oneself may, indeed, be a neglected secret weapon in our constant struggle against the universal tendency toward mental depression. It certainly is one way to look up. But maybe it is too simple, too easy a solution. A very depressed and sad person sought the services of a Scottish physician. After evaluating his patient the doctor felt that the depression was not serious. He suggested to his patient, "Go see the clown Gremboli, and let him make you laugh. That should cure you." The patient looked at him with large, tear-filled, sad eyes and whispered, "Doctor, I am Gremboli." Another slap at this simplistic approach to depression therapy comes from Will Rogers, Jr., who stated that too many American humorists become bitter, cynical, or negative in their attempts to cheer people up. They are caught up in the technique of "cutting people down." Nevertheless, the observation that humor helps holds true. It is valid when constructive and shared with others. It works. Such a devastating malady could be met with a simplistic and cheerful sermon: "How to Keep Depression Away." Certainly the XlU
xiv
DEAUNG WITH DEPRESSION
concept of prevention is valid-but is it realistic amid today's frightfully tumultuous events so personally and overtly ominous? The impersonal environment and the threats and frustrations of a complex, industrialized society may certainly result in a high incidence of depression. But does this depression differ from that experienced by the starving masses in Africa and the subcontinent of India? I think not. Therefore, the problem is not just local or provincial, or determined by economic or social class. It is all pervasive; worldwide. Ministers, physicians, and also psychologists and counselors simply cannot avoid dealing with depression. It affects all busy clinical practitioners. I project a thought that seems pertinent and relevant in the context of this book's dynamic approach to dealing with depression. It is personal and unencumbered with ponderous theory. My own minister gave it to me to think about and live by. It is in three parts. 1. If you believe in God, go all the way. Let Him run the show. 2. Keep God's Law. Do right and you will feel right. 3. Remember that if God accepts you as you are, why not accept yourself as being worthy after all. The contributors to this book have met depression head-on. You will not find easy answers to place in your hip pocket for ready use. You will, however, experience some incisive probing and candid analyses of specific problems with depression. You will be exposed to the various techniques of therapy-some unique, some shocking, all interesting and cogent. You will find guideposts that will allow you to deal with depression as you encounter it. You may understand yourself better.
Robert M Mathews, MD
Preface
When I was a young pastor, a man who was a leader in the church asked to talk to me. He described a lot of thoughts of aimlessness, dissatisfaction, and lack of confidence along with feelings of sadness, hopelessness, and unworthiness. He said he wished he were dead! I tried to refer him to a psychiatrist I had heard about in a nearby city, but he refused, saying that he preferred to talk to me. I saw him a few more times. Then after he returned from a weekend trip with his family to his hometown, he asked to see me again. As he told me about his failed plan to kill himself, I was so frightened that the small hairs on the back of my neck stood out. He had taken his gun, telling his family that he planned to do some hunting. His secret plan was to shoot himself while crawling through a fence to make it look like an accident. He had parked on the town square to let his family out to do some shopping. When he tried to back his car out to go "hunting," he was blocked by a relative in a truck who insisted that he go on a delivery with him. Hearing this suicide plan, I insisted that he consult with the psychiatrist, and he is still living today.' There are an estimated 35 million depressed people in this country according to a U.S. News and World Report article dealing with depression (1983,1993). Statistics from the National Institute of Mental Health indicate that one in ten persons is afflicted seriously enough to require treatment (Regier, 1993, p. 88). Even though suicide is grossly underreported and many attempts at suicide are unsuccessful, the National Center for Health Statistics reports almost 30,000 suicides in the United States annually (U.S. Public Health Service, 1988, p. 312). This figure accounts for one percent 1. The case histories used in this book are for illustrative purposes. Some represent actual people whose identity is disguised, some are composites of several people, some are drawn from historical literature, and some are fictitious.
xv
xvi
DEAUNG WITH DEPRESSION
of the yearly deaths and places suicide among the twelve leading causes of death. This all means that one U.S. citizen commits suicide about every 30 minutes. Sometimes called "the common cold of mental illnesses," the term depression is used to describe a variety of conditions ranging from mild sadness to extreme psychosis. The Merriam-Webster Dictionary (1974) defines depression as "an emotional disorder marked by sadness, inactivity, difficulty in thinking and concentrating, and feelings of defection" (p. 199). Mild to extreme forms of depression are discussed in this book. I do not believe there is any sharp distinction between so-called normal and abnormal depression. Sadness or mourning is a normal reaction to loss imposed by outside circumstances. Depression of more than a mild degree usually comes from within and is associated with hostility turned on oneself, low self-esteem, and feelings of helplessness and hopelessness. It is also associated with a mosaic or composite of symptoms, including affective, bodily, and cognitive disturbances. Depression has also been called "a family affair." Some forms of depression seem to run in families. It also occurs during a wide age range. The peak years for major depression disorders are between the ages of 25 and 44. Depression is also a worldwide disease. A study which included subjects from North America, Puerto Rico, Western Europe, the Middle East, Asia, and the Pacific Rein found that the incidence of depression is actually increasing (Cross-National Collaborative Group, 1992).2 This book is addressed to clergy and all those in the helping professions who are concerned about people with the above-mentioned symptoms. The backgrounds, study disciplines, theoretical orientations, social roles, and philosophies obviously are different among those in the fields of medicine, sociology, theology, psychology, and allied health. Yet from our individual perspectives, we all come with the equipment unique to our profession to fish in the same pool of 2. Cross-National Collaborative Group, "The Changing Rate of Major Depression," Journal of the American Medical Association, 268(21):3098-3105, Dec. 2, 1992.
Preface
xvii
knowledge and catch those ideas that we can use in helping those who come to us and depend on us. Since the number of persons experiencing depression in more than its mild form has reached almost epidemic proportions, the subject of how to treat depression is arousing increasing professional intrest.' The number of entries in the bibliographies at the end of each chapter of this book is good evidence of this interest. A bimonthly journal entitled Depression was launched in 1993.4 Faced with the preponderance of depressed people, one would expect that a well-integrated theory supported by a large body of research is available on the subject. Such is not the case, however, and religious professionals find themselves reviewing one esoteric analysis of depression after another with little progress in understanding how to treat depression successfully. In this book we have presented five approaches to understanding and assisting those who suffer from depression. Recognized experts in each of the systematic viewpoints of transactional analysis, pastoral counseling, Gestalt therapy, behavioral therapy, and cognitive therapy have contributed chapters that set forth their understanding of depression and their methods of treatment. The techniques that each of these contributors use in their work with depressives are discussed in practical and understandable ways. I doubt that any individuals in the helping professions can read this book and not improve their ability to help those who are depressed. A careful reading of the different chapters will reveal that the authors variously place credence on reason, experience, ideas, or some selection or combination of all of these. In Chapter 7, I present my work with a young woman who came to me thinking that she was demon-possessed. My pastoral diagnosis was that she was depressed. Her case is discussed by the authors of the various chapters from their respective viewpoints and then the counselee herself is interviewed. Since my own theoretical orientation to pastoral psychotherapy is eclectic, I used techinques from each of these systems in working with her. Thus, Chapter 7 serves as an example 3. In 1993 the National Mental Health Association organized a National Public Education Campaign on Clinical Depression. 4. Charles B. Nemeroff, editor, Depression, New York: Wiley-Liss,
xviii
DEAUNG WITH DEPRESSION
of how ideas from throughout the book can be unified in the treatment process. These topics were first addressed orally by the authors at a conference at the Baptist Medical Center in Kansas City, Missouri, while I was the Director of the Department of Pastoral Care and Counseling. I have utilized the substantive concepts presented in this book in pastoral counseling with more than 100 counselees who were depressed. I have used these materials in teaching each class of Family Practice residents at Southern Illinois University, School of Medicine, (SIU-SM), and more recently in a course on depression I taught at Sangamon State University. They have been further researched and greatly revised for publication, to suit the eye rather than the ear. I wish to express my appreciation to the Baptist Medical Center for making possible the conference that spawned this present study. My thanks also go to my colleagues in the Department of Medical Humanities at SIU-SM: Dr. Glen W. Davidson, Nancy Pistorious, and Linda Keldermans for their invaluable editorial suggestions; and Margaret "Peg" Moehle, Charlene Meents, and Jean Zoelzer for typing the manuscript. Richard Dayringer
Chapter 1
Recognizing Those Who Are Depressed Richard Dayringer
Depression is not entirely uncommon among the great saints of the church. William Cowper, who wrote poems and hymns, was depressed. He was a parishioner and close friend of John Newton, the eighteenth-century sea captain who became a preacher and wrote the words of the hymn "Amazing Grace." Well-educated, cultured, and affluent, Cowper became involved in lay ministry but was devastated by bouts of despair. One time Newton was called to Cowper's home only to find that he had made an unsuccessful suicide attempt by cutting his throat. He was utterly convinced that God had rejected him. At another time when Cowper was suicidal, Newton brought him to his home and kept him under surveillance. For months Cowper insisted that God had marked him for eternal damnation. Newton formed prayer groups to pray for Cowper's mental health. Finally, the gloom lifted and he became his normal self (Deal, 1974). Surveys indicate that 20 million people-15 percent of all adults between the ages of 17 and 74-may suffer serious depression from time to time, and few of them receive help (Bielski and Friedel, 1977). This means that during any six-month period, as many as 10 million Americans find themselves sliding into the black hole of depression, powerless to stop their descent. Or, to put it another way, "The chance of someone who lives to age 70 contracting depression during his lifetime is now seven and eight-tenths percent for males and twenty percent for females" (Callan, 1979). An international study found that depression is on the rise the world over. Researchers questioned over 39,000 people in nine 1
2
DEALING WITH DEPRESSION
countries. They found that in each successive generation, major depression began at an earlier age and affected a greater number of people. Several explanations were offered for rising depression: a doubling of the divorce rate, a decrease in the time available for parents to spend with their children, industrial substances released into the air, and the decline of religious faith (Weissman, 1992). It has been estimated that the average physician, during a lifetime of practice, will have 14 patients who commit suicide. Perhaps as many as 10 percent see their physicians on the day of or just prior to their suicide. Ancient people also had to deal with depression. The Bible charts the depressive symptoms of such men as Job, Moses, Elijah, David, and Jeremiah. Elijah, for example, (First Kings, Chapter 19) withdrew into hiding after the triumph over the 400 priests of Baal. He expressed low self-esteem, lost his appetite, slept a lot, and asked to die. Jesus may have suffered depression during the time of the temptation. He fasted, slept little, and was tempted to jump off the pinnacle of the Temple. Shakespeare put a description of Hamlet's depression into the mouth of Polonius: He . . . a short tale to make, Fell into sadness, then into a fast, Thence to a watch, thence into a weakness, Thence to a lightness, and by this declension, Into the madness wherein he now raves And all we mourn for." (Hamlet, Act 2, Scene 2) Numerous studies have shown that, at any time, between 9 and 20 percent of the U.S. population have depressive symptoms. The figures are higher among women (11 to 24 percent) than men (6 to 16 percent) (Office of Disease Prevention and Health Promotion, 1988). When mental health professionals speak of "clinical depression," they are referring to the clinical depressive syndromes. This means that the person is so depressed as to have physiological symptoms. The following terms are also generally used synonymously: autonomous, endogenous, endogenomorphic, melancholia, or vital depression. These terms refer to a group of increasingly identifiable subtypes of depression based on specific sets of symptoms and
Recognizing Those Who Are Depressed
3
associated factors. The benchmark for clinical depression, compared to normal sadness, depends on the intensity, severity, and duration of symptoms. Generally (except in the case of bereavement over the death of a loved one), if the depressed mood and associated symptoms last for more than two weeks, and if they are of sufficient intensity to interfere with ordinary daily activities, this is considered a clinical depressive syndrome. Depressive disorders occur most often between the ages of 25 and 44, although it has been documented in children as young as age five. For depression to first appear after age 60 is less common. Most studies indicate that it strikes women almost twice as frequently as men. In recent years, remarkable progress has been made in the classification, diagnosis, and treatment of depression. But paradoxically, even in light of these clinical advances, depression often goes unrecognized. So, undertreatment is a significant problem. Some specialists believe that fewer than one-third of those who have serious depressive disorders receive adequate treatment. Despite the distressing nature of this illness, there is good news: even in its most serious forms, depression usually responds well to modem treatment methods, and symptoms often can be relieved quickly-sometimes within weeks. Depression affects people in different ways. However, there are two consistent symptoms that can be relied upon to diagnose depression: a loss of interest or pleasure in all or almost all usual activities (anhedonia), and a relatively persistent disturbance of mood (dysphoria). The Diagnostic and Statistical Manual ofMental Disorders, fourth edition, (DSM-IV), published by the American Psychiatric Association, is the system most widely used in this country by mental health professionals to diagnose and classify mental and emotional disorders. According to DSM-IV (see Appendix I), five of the following nine symptoms must be present most of the day, nearly every day, during a two-week period for a diagnosis of major depression to be made: 1. Depressed mood, or irritable mood in children and adolescents; 2. Loss of interest or pleasure in usual activities;
4
DEALING WITH DEPRESSION
3. Significant weight loss or gain (more than 5 percent of normal body weight) when not dieting; 4. Disturbances in sleep patterns, whether insomnia (difficulty falling asleep, early morning awakening, or waking in the middle of the night) or hypersomnia (excessive sleepiness); 5. Agitation or a generalized slowing of intentional bodily activity, known as psychomotor retardation; 6. Fatigue or loss of energy; 7. Feelings of worthlessness, or excessive or inappropriate guilt; 8. Diminished ability to think or concentrate; 9. Recurrent thoughts of death or suicide, or a suicide attempt. NOTE: One of the five required symptoms must be either depressed mood or loss of interest in or failure to derive pleasure from usual daily activities. The many characteristics of depression fall into four main categories: mood disturbances, behavioral disturbances, cognitive (thought) impairment, and physiological changes or bodily complaints. Depressed church members may express their mood with statements such as: "I feel down in the dumps," or some other colloquial equivalent. They may worry about their sinfulness and magnify past failings or feel that they have not been forgiven for wrongs. They may complain, "I am unable to feel any emotion," or "Nothing interests me or satisfies me," or "I just don't care about anything anymore." They may feel worthless, guilty, and negative about the world and the future. They may become irritable, easily annoyed, and openly display anger in church meetings. Depressed persons demonstrate various behavioral disturbances. Facial features may reveal the most important clues, such as appearing unhappy or sad, looking older than their actual age, having a furrowed forehead and downcast eyes, maintaining a blank expression, and allowing the comers of the mouth often to be turned downward. In addition, they may frequently withdraw from others, including not attending worship services. They may neglect their personal hygiene or appearance. Crying episodes often accompany depression, particularly in its early stages. But as depression becomes more protracted or severe, many individuals become incapable of weeping, even though they say they want to do so. Their
Recognizing Those Who Are Depressed
5
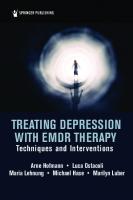
FIGURE 1.1 Agitated
Manic
Neurotic Normal
Bipolar
Moods Depress on MOOD SADNESS ( Exogenous Grief Post-Partum Reactive
Normal Moods Dysthymic Unipolar ) PSYCHOSIS Neurotic Melancholia Endogenous Dysthymic Autonomous Seasonal Cyclothamic
posture may become stooped, the pitch of their voice monotonous, and they may delay noticeably in responding to questions. As a result of impaired cognitive functioning, depressed persons often fmd it difficult to concentrate. Thoughts are slowed and confused, and decision making becomes exceedingly difficult. Thoughts often are centered on the self with prominent themes of helplessness and hopelessness. When posed questions, a depressed individual typically responds, "I don't know." Thoughts of death (not just fear of dying) are common. Often such persons believe that they would be better off dead. There may be suicidal thoughts, with or without a specific plan, or suicide threats and attempts. Various physical symptoms frequently accompany bouts of depression. Most clinicians regard insomnia, especially early morning awakening, as the hallmark symptom of depression. Other bodily signs of depression include: gastrointestinal disturbances (such as indigestion, constipation, or diarrhea), weight loss or gain, menstrual cycle disturbances, loss of sexual interest, itching, dry mouth, blurred vision, and excessive sweating. However, not all depressed people initially admit to symptoms typically associated with depression. Rather, they may complain of more vague ailments, such as headaches, backaches, or chronic pain. Depression with atypical features has been labeled "masked depression" (Lesse, 1974) and even "smiling depression." Depressive disorders come in different forms (see Figure 1.1). Some are episodic in nature, occurring just once or twice during a
6
DEALING WITH DEPRESSION
lifetime. Others are chronic, and they require some form of ongoing treatment to assist with disabling symptoms. Although different depressive disorders have many similar features, they often can be differentiated by certain characteristics, such as the type, severity, and duration of symptoms. Four of the most common types of depressive disorders are discussed below.
Manic Episode. The essential feature of a manic episode is a distinct period during which the predominant mood is either elevated, expansive, or irritable. These symptoms usually appear suddenly, with a rapid escalation over a few days. Associated symptoms include inflated self-esteem or grandiosity which may be delusional, decreased need for sleep, pressure of speech (speaking rapidly or hurriedly), flight of ideas, distractibility, psychomotor agitation, and excessive involvement in pleasurable activities. Manic speech is typically loud, rapid, and difficultto interrupt, The euphoric mood is usually so cheerful as to be infectious for the uninvolved observer, but is recognized as excessive by those who know the person well. However, the predominant mood may be irritability, which may become most apparent when the person's desires are thwarted. Grandiosity is the over-estimation of one's importance. Persons in a manic phase may give advice on matters about which they have no special knowledge, such as how to run a church or denomination. Despite lack of any particular talent, such a person may compose an anthem and insist that it be sung by the choir. Flight of ideas is a nearly continuous flow of accelerated speech, with abrupt changes from topic to topic. Any external stimuli, even though irrelevant, may add to the person's distractibility and tendency to jump from one subject to another. People in a manic state have boundless energy, enthusiasm, and increased sociability. They may volunteer for numerous tasks at church and attempt to phone or visit prospects at all hours of the night. They usually do not recognize the intrusive, domineering, and demanding nature of these activities. They may contribute outrageously large gifts, drive recklessly, fight, or engage in unusual sexual behavior. Often these activities have a flamboyant quality,
Recognizing Those 'Who Are Depressed
7
such as wearing strange garments or poorly applied makeup, or distributing money. Bipolar Disorder. The most widely accepted subdivision of affective disorders is the distinction between bipolar and unipolar disorders, first proposed by Leonhard, Kerff, and Shulz in 1962. Some people experience recurrent cycles of both depression and mania. Because this condition involves emotions at different poles or extremes, it is termed "bipolar" disorder. It is frequently referred to as manic-depressive disorder and accounts for less than one-quarter of major depressive illnesses. In the depressive phase of a bipolar disorder, an individual may suffer from any of the symptoms typically associated with major depression. The manic phase of the disorder is characterized by symptoms of a manic episode. The cycles of bipolar disorders are not necessarily predictable or regular during the course of the illness. This disorder is equally common in both males and females, unlike major depression, which is more common in females. It has also been shown by research to occur at much higher rates in biologic relatives. Cyclothymia is a milder form of this. Dysthymic (dis-thy'mik) Disorder. This condition, also referred to as dysthymia or depressive neurosis, is similar in many ways to major depression, but symptoms tend to be less severe. It usually begins in childhood, adolescence, or early adulthood. The symptoms are not always disabling, but keep the person from feeling well and functioning effectively. For a diagnosis to be made, one must have depressive symptoms for most of the day, more days than not, for at least two years (one year for children and adolescents). It is important to note that some individuals with dysthymic disorder also may experience episodes of major depression. This is called "double depression." Seasonal Affective Disorder (SAD). During the winter months, when days are short and nights are long, some people begin to feel lethargic and depressed, and may crave carbohydrate-rich foods. SAD is an extreme form of the winter "blahs" or "cabin fever." Those who are afflicted by this disorder experience a seasonal pattern of their depressive symptoms.
8
DEALING WITH DEPRESSION
No one knows exactly what causes SAD. But many experts believe the condition may result from prolonged secretion or increased levels of melatonin, a hormone that the brain produces during darkness. In recent years, many SAD patients have benefited from phototherapy: early morning exposure to special full-spectrum lights. A popular query along this line is the question, "Is the ChristmasHanukkah season hazardous to your health?" Is there such a thing as a "holiday depression"? Since the 1950s, the lay press and medical publications have offered various opinions on the subject. By 1985, the Reader's Guide to Periodical Literature began a separate heading for the numerous articles on this popular topic. However, the professional literature generally fails to support the notion that the holidays are a time of increased depression (David, 1983; Hillard and Buckman, 1982). Nevertheless, it is a time when some individuals become depressed. Reactive Depression. Depression is sometimes brought about by factors external to the self. This type of depression is referred to by such terms as "reactive, secondary, environmental, or exogenous." The symptoms for reactive depression may be similar to major depression or dysthymia, but they are more temporary in nature. Grief over the death of a loved one is the most common type of reactive depression. One difficulty in distinguishing grief from other types of depression is that normal grief lasts from 18 to 24 months, and morbid grief may last even longer (Davidson, 1984). Grief is the dominant emotion following divorce or the loss of a job, goal, pet, etc., although these forms of grief may not last as long as grief related to the death of a loved one. One distinguishing difference between grief and depression is that grief does not cause low selfesteem as does depression. Severe illness may produce a secondary depression, recognizable in and of itself, but which clears up as the patient recovers from the illness. Some diseases, such as hypothyroidism (underactive thyroid gland), arthritis, heart attack, or stroke can bring on a secondary depressive reaction. Also depression can be secondary (an undesirable side effect) of certain prescription medications, especially steroids, some high blood pressure medicine, and antiparkinsonian agents. A postpartum depression may follow the birth of a baby for some mothers as the attention shifts from mother to baby and as mother
Recognizing Those 'Who Are Depressed
9
begins to face the 20-year responsibility of rearing the baby. Women may also experience depressive symptoms with varying levels of severity preceding their menstrual periods, or during menopause. There are now available a number of brief paper and pencil tests that can be quite helpful to clergy in diagnosing depression. These tests have been standardized and validated on large populations and can help to confirm or dispute a pastor's clinical judgement. The Beck Depression Inventory is probably the best-known, best-researched, and most widely used of the tests available Multiple causes for depression have been offered by psychological theoreticians. These depress 0 genic factors will be summarized here and many of them greatly expanded in the ensuing chapters of the book. Psychoanalytic. The oldest and perhaps most widely held theory for the cause of depression came out of Sigmund Freud's psychoanalytic school and maintains that depression is caused by anger for others that is unconsciously turned on oneself. Neo-Freudians have suggested that depression is caused by the loss of self-esteem or other object losses that are never resolved. Heredity. Studies have shown that some depressive disorders are hereditary (Cohen, 1994). For example, manic-depression has been linked, in some cases, to a genetic defect. For some reason, this theory has been taken more seriously in Europe than in the United States. Depression does sometimes run in families, and pastors, who usually have good access to families, should check for this in forming a diagnosis. Biochemical. Some types of depression may result from abnormal chemical activity within the brain. These chemicals playa role in the transmission of electrical impulses from one nerve cell (neuron) to another. These chemical "messengers," called "neurotransmitters," set in motion the complex interactions that control moods, feelings, and behaviors. They also regulate pain, learning, and memory, as well as the desire to eat, drink, and sleep. Three neurotransmitters-dopamine, norepinephrine, and serotonin-have been associated with depressive illnesses. Research suggests that episodes of depression or mania may be related to an improper balance of neurotransmitters. No one yet knows with certainty whether
10
DEALING WITH DEPRESSION
biochemical factors cause depression, or depression causes the biochemical disturbance. Nevertheless, pastors who counsel are wise to regularly advise their depressed counselees to consult a physician who can evaluate the biochemical factor. Behavioral. Behavior therapists theorize that depression is caused by feelings of helplessness and hopelessness. They believe, on the basis of much research, that these feelings are the result of a loss of positive rewards in life. Cognitive. Cognitive therapists contend that people become depressed because of a preponderance of negative thinking about themselves. They criticize themselves, call themselves bad names, and undermine their self-esteem. Gestalt. Gestalt therapists maintain that depression is due to one's perceived failure to live up to the expectations of others. The depressed look to others for directions and strength rather than within themselves. Existential. Existentialphilosophy and theology is a quest for meaning in life. Existential therapists believe that depression is caused by not finding meaning or by a loss of meaning in living. We all struggle with questions such as: "Why am I here?" "What should I do with my life?" "What have I accomplished?" Not finding adequate answers to these and similar questions can be devastating. Family Systems. Family systems theorists have observed that often an individual member of a family will feel and act out the emotions of the whole family. This person may unknowingly become the "designated patient" and may be subtly rewarded with extra attention by family members for depressive behavior. Religious. Depression may be caused by a religious value crisis (Oates, 1978). Nostalgia and rumination over one's self-consistency, competence, guilt, or lack of courage may take on crisis proportions during times of self-evaluation. People may also become greatly discouraged when observing injustice in society and their powerlessness to do anything about it. Unfortunately, people with depression often hesitate to seek help. This is ironic. Millions of people who suffer from depressive disorders, which can respond to treatment, do not obtain professional
Recognizing Those Who Are Depressed
11
care and thus suffer needlessly during their lifetime. Pastors are given free access to people in our society. They can do case-finding and enable such people to be helped. That is what this book is about. BIBLIOGRAPHY American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, revised (DSM-IV). Washington, DC: American Psychiatric Association, 1994. Anthony, James, (ed.). Depression and Human Existence. Boston: Little, Brown, 1975. Arieti, Silvano and Jules Bemporad. Severe and Mild Depression. New York: Basic Books, 1978. Ayd, Frank Jr. Recognizing the Depressed Patient. New York: Greene and Stratton, 1961. Beck, Aaron T. The Diagnosis and Management of Depression. Philadelphia: University of Pennsylvania Press, 1973. Becker, Joseph. Depression: Theory and Research. New York: John Wiley and Sons, 1974. Bielski, Roleng and Robert D. Friedel. "Subtypes of Depression-Diagnosis and Medical Management," Western Journal of Medicine, 126(5):347-352, May 1977. Callan, John. "Affective Illness on the Increase," Journal of the American Medical Association, 241(6):545, Feb. 1979. Cohen, David B. Out of the Blue: Depression and Human Nature. New York: W.W. Norton, 1994. David, Daniel J. "Christmas and Depression," Journal of Family Practice, 17(6):1083, 1086, 1983. Davidson, Glen W "Understanding Mourning: A Guide for Those Who Grieve." Minneapolis: Augsburg, 1984. Deal, William. John Newton. Westchester, IL: Good News, 1974, pp. 61-66. Feighner, J.P. and W.F. Boyer. Diagnosis of Depression. Somerset, NJ: John Wiley & Sons, 1991. Freden, Arthur J. Four Therapies Integrated: A Behavioral Analysis of Gestalt, TA. and Ego Psychology. Englewood Cliffs, NJ: Prentice-Hall, Inc., 1984. Freden, Lars. Psychological Aspects of Depression. New York: John Wiley and Sons, 1982. Friedman, Raymond J. and Martin M. Kate (ed.). The Psychology of Depression. Washington, DC: H.Y. Winston and Sons. 1974. Hillard, James R. and John Buckman. "Christmas Depression," Journal of the American Medical Association, 248(23):3175-3176, 1982. Jacobson, Edith. Depression: Comparative Studies of Normal, Neurotic, and Psychotic Conditions. New York: International Universities Press, 1971. Kline, Nathan S. (ed.). Factors in Depression. New York: Raven Press, 1974.
12
DEALING WITH DEPRESSION
Leonhard, K., I. Kerff, and H. Shulz. "Die Temperamente in den Familien der Monopolaren und Bipolaren Phasischen Psychosen," Psychiatric Neurolosy, 143:416-434, 1962. Lesse, Stanley. Masked Depression. New York: Jason Aronson, 1974. Mann, 1. John. (ed.). Phenomenology of Depressive Illness. New York: Human Science Press, 1988. Press, Marsella, Anthony J., Robert M.A. Hirschfeld, and Martin M. Katz (eds.). The Measurement ofDepression. New York: Guilford Press, 1987. Oates, Wayne. The Religious Case of the Psychiatric Patient, Philadelphia: Westminster Press, 1978, pp. 124-140. Office of Disease Prevention and Health Promotion, U.S. Public Health Service. Disease Prevention/Health Promotion: The Facts. Palo Alto, CA: Bull Publishing, 1988, p. 310. Rosenthal, Norman E. Winter Blues: Seasonal Affective Disorder. New York: Guilford Press, 1993. Rush, A. John and Kenneth Z. Altshuler. Depression: Basic Mechanisms, Diagnosis and Treatment. New York: Guilford Press, 1986. Schuyler, Dean. The Depressive Spectrum New York: Jason Aronson, 1974. Usdin, Gene. (ed.). Depression: Clinical, Biological and Psychological Perspectives. New York: BrunnerlMazel, 1977. Watts, Cuthbert A.H. Depression: The Blue Plaque. London: Priory Press, 1973. Weissman, Mryna and Cross-National Collaborative Group. Dec. 2, "The Changing Rate of Major Depression," Journal of the American Medical Association, 268(21):3098-3104, 1992. Willner, Paul. Depression: A Psychobiological Synthesis. Somerset, NJ: Wiley and Sons, 1985. Winokur, G., D. Glayton, and T. Reich. Manic Depressive Illness. St. Louis: C. V. Mosby, 1969. Winokur, G., D. Glayton, and T. Reich. Depression: The Facts. New York: Oxford University Press, 1981.
Chapter 2
Transactional Analysis Dealing with Depression John J. O'Hearne Richard Dayringer
According to the dictionary, the root of the word depression is "to press down" and the verb to depress means "(1) to lower in spirits, deject, dispirit, make sad, or gloomy; (2) to lower in force, vigor, activity; (3) to lower in amount or value; (4) to put into a lower position." The noun depression is much more pallid: "a condition of general emotional dejection and withdrawal" (Webster's, 1984, p. 364). This is exactly what happens in the human condition. Depression causes feelings of dejection, dispirit, and a lowering of self-worth. The second definition of the noun, "Sadness greater and more prolonged than that warranted by an objective reason," is not accurate according to the psychiatrist's viewpoint of depression. There is a vast difference between sadness, which is a normal reaction to loss, and depression. Babies cry when they lose the nipple; children cry when they lose favorite toys; adults cry when they lose someone they love. These reactions are ones of sadness, as contrasted with depression. From the classical viewpoint, depression has two causes. The first is a loss, usually of some idea: "I should have been a good boy and I goofed" ; "I should have led the class"; "I should have won the race"; or "I should have studied harder for that exam." Sometimes people even get like the old fellow who in his earlier days was converted to Christianity and became very humble. But his conceit came through because on his tombstone was written, "Here lies the world's greatest sinner." Most people who feel depressed 13
14
DEALING WITH DEPRESSION
dub themselves with distinctive titles such as "world's greatest sinner," the "greatest 'goof' artist," the "greatest mistake," etc. This tendency is a natural part of depression. Now what is depression? As indicated earlier, one component of depression is loss and the other one is apparent when people "get down" on themselves. Depressed individuals exhibit a cycle. The phenomena of this cycle include the feeling that there is no future; "I have run out of future; I may as well die because there is no future." If there is no future, there is no hope. In treating depressed patients in the hospital environment, it is particularly important to prove to them that there is a tomorrow-that the future is important. Counselors often give these patients tasks which may be boring, monotonous, and menial. There is a method in this. First, patients need to realize that there is time for them to finish their tasks. Second, menial types of activities take some of the pressure off. Instead of their consciences berating them, people are now saying: "You didn't clean up behind the toilet. You didn't get those ash trays clean enough." Taking over part of the punitive aspects depressed people ordinarily ascribe to themselves can sometimes lighten the load. A patient is turning the comer toward recovery when the menial, monotonous things become annoying. The following example illustrates the power of this method of treatment. I saw a woman who was not sick enough to go into the hospital. She had been awakening every morning about 4:00 a.m. feeling terrible. This waking up early is common in cases of depression of any severity. Most people feel hopeless at that hour and usually feel better by bedtime in the evening. I asked this poor woman, "What would you really hate to do most of all at that hour of the day? What is the job around the house that you despise?" She replied, "I despise mopping floors." Even though she thought I was crazy, she agreed to my suggestion that the next day when she woke up at 4:00 a.m., she would mop the floors. The first morning she did just that. The second morning she got up, put the warm water in the bucket, and went back to bed, and the third morning she slept. This is perhaps a rather tricky way to begin treating depression, but the patient began to overcome her depression in three days. Modem drugs can work no faster. I do not intend here to oversimplify this
Transactional Analysis Dealingwith Depression
15
treatment because depressed patients constitute psychotherapist's emergencies and are just about their only opportunity to actually help save lives. Psychoanalysts used to say that depressives are love addicts. I disagree with this statement. Most people who have tried to help someone who is depressed have already found that tender loving care will not work. Remonstrations of "I love you; you are great," are not helpful. Comfort in this sense usually is to no avail. Why? Well, the feelings of one person are not felt by another. Who gets depression? Only good people, only nice people, only proper people. Those who do not care one way or the other do not suffer from depression. Their consciences are not as restricting. Only people with strict consciences and high standards get depression. This includes people with compulsive-type personalities who suffer many headaches, rheumatoid arthritis, etc. These personality types usually are meticulous individuals who may not know much about playing, and who seldom find themselves comfortable asking for help. There is an old saying that physicians make terrible patients. Why? Because they are used to doing the caretaking, rather than having others do it for them. To be confronted suddenly with their own dependent needs often is more than their professional standards will allow. On the medical side, what causes depression? European practitioners pay much more attention to heredity than do their counterparts in the United States. Europeans look for the person who is short and stocky with short stubby fingers and check to see if the grandparents had severe depression. Americans do not stress the importance of heredity as much. There are some biochemical changes in depression. Psychiatrists still hope that someday there will be a perfect drug cure for depression, but so far there is not. The drugs used often are helpful, sometimes lifesaving, but do not necessarily cure depression. So there must be some psychological factor in addition to biochemical changes. Transactional analysts emphasize the importance of communication. Dr. Eric Berne, author of Games People Play (1964), used to say that "professional people-helpers" spend their professional lives reacquiring 50 percent of the diagnostic abilities of small children. One of the reasons is that adults have been taught to listen
16
DEALING WITH DEPRESSION
primarily for words. They deal so much in words and abstractions in teaching and learning. Words were not the first language, however. Let's take a look now at some of the basic concepts of transactional analysis. Dr. Berne, a brilliant, highly verbal, pedantic psychiatrist, loved words-they were his playthings. Although many people have looked at Games People Play, how many have read it cover-tocover? It is a difficult book to read. Berne covered every loophole. In fact, Eric was such a precise man that I am surprised he did not suffer from depression himself. Berne started this whole business of transactional analysis when he was talking with a lawyer and the lawyer told him in effect, "But, Dr. Berne, I'm not a lawyer right now; I am a little boy," and then told Eric about an incident in his childhood when he was on vacation. His family went to a dude ranch, and there he helped a real cowboy with the chores that had to be done. The cowboy said, "I'm not really a cowpoke; I'mjust a little boy." In his listening, Berne noted that when this lawyer said, "But, Dr. Berne, I'm not a lawyer right now; I'm a little boy," he sounded like, looked like, thought like, and felt like a little boy. He was in a different state of being than when he was functioning as an attorney. Transactional analysts often prepare their new patients by asking them to think about the last big moment of joy in their lives and to contrast it with the way they are feeling at present. There is usually a big difference. The moment of genuine joy is what transactional analysts call "the Child ego state." Most of the time people are in their Adult ego states: learning something, thinking about something. The difference is that the Child ego state represents all that each adult was as a child: scared, weak, curious, devilish, unprincipled. A child has the ability to shift quickly from love to hate, to curiosity, to joy. By contrast, the Adult ego state can be thought of as a data processor, a computer, a thermostat. The Adult gets information, makes decisions, and orders action. Notice the "dry," feelingless quality I have used in describing the Adult. What I am talking about is the Adult with a capital "N.' in this particular system. Adults are loaded with feelings. Because of these feelings people have three states of being. The Adult ego state is easiest to think of as feelingless.
Transactional Analysis Dealingwith Depression
17
Transactional analysts also add the Parent figure into the picture. Eric and the lawyer began to look into this phenomenon, too. They found that at times he neither seemed like a child nor did he seem like a lawyer. Instead, he sounded, looked, acted, and thought like his parents, or other important people in his early life. As a Parent now, this lawyer has feelings. He has recorded, as if on videotape in a recessed part of his brain, certain shoulds, should nots, and value judgements. How did he learn that bowel movements smell bad? Little babies do not think that they smell bad. By the time children have watched a number of people hold diapers out in the air with their noses turned up, they begin to get an idea that the smell is bad. Later on, they learn other shoulds and should nots. The lawyer does not need children of his own to have a Parent ego state. Neither does he have to be a grown-up, 21-year-old to have an Adult ego state. I have seen depressed four-year-olds. I do not think depression could exist before the age of four in the sense I am using it here, however. It does not seem possible for very young children to begin to put a Parent into their own minds-although this does not take long. Young children will reach out for cookies, slap their own hands, and say, "No, no" when they see a parent. A four-year-old boy says to his six-year-old brother, "Mom's gone next door. She just made some cookies. Let's get them." The Child in the six-year-old would say, "Great, I love cookies." The Adult would say, "No, she will catch us. Well, maybe she won't catch us if we just take one each." The Parent might say, "No, you are not supposed to steal cookies." So you don't have to be of a certain age to have these three ego states. Transactional analysts think that the Parent state should be externalized. One elderly lady whom I treated almost died during one electric shock treatment. Every time she got sick with depression after that, I could make her get well without shock treatments by using TA. TA makes the process simple so that people, including the Child in each individual, can understand. To exemplify the Parent ego state, think for a moment of something your parents taught that you still regard as valuable, positive, good, helpful. Just think about it. Flip it over and think of something that you got from them that didn't feel so good. You felt bad when you heard it. See if that perception is not still alive. In fact, you may
18
DEALING WITH DEPRESSION
be passing it on to your own children. If you want to teach prejudice, make generalized statements when your children are around. "All Baptists have big buildings and lots of money." "All Irishmen are drunk Roman Catholics." "All Arabs have oil." When parents teach prejudices like these, they are telling things that they consider to be facts. Even though they are not facts, children learn them as such. Until they are adults, and reexamine those "facts" and theories, they never know whether they are looking through their own eyes or the glasses their parents put on their noses. Any prejudice is a contamination of the Adult ego state by the Parent ego state. It is not a fact. To rid the self of prejudice necessitates addressing attention to facts. This procedure is used with depressed patients. If a man says "I am totally worthless," a good analyst will ask, "What is the evidence?" When does the Bible say anyone is totally worthless? Anyone who claims to have committed the unpardonable sin needs to let others know what it is. Only those people who are suffering from extreme depression seem to feel they cannot forgive themselves. Counselors sometimes can heal that breach by asking, "Have you forgiven yourself for falling short of the mark?" Like Paul, people can only press toward the mark for the prize of the high calling. God doesn't expect us actually to reach it. Although a religious background can be very helpful at times like these, there are many people with religious backgrounds who get terrible depressions. It is the Child who loses: "I lost the beauty contest"; "I lost the race"; or "I didn't do enough preparation for the exam." It is the Child who sustains the loss and has the same reaction to loss that any other child would. I have been asked why a nurturing parent and the analyst cannot join forces to counteract the power of the depressed person's punishing Parent. It is difficult. The material that is recorded in the brain near the core of the videotape has more influence and has been practiced longer than the material that comes later. If the person says, "I am no good," and is told, "Yes, you are," it will be to no avail. That person cannot hear the caring because depressed people do not have love available to them. No minister has ever cured anyone's grief by going to the funeral of the person's father and saying, "Don't feel bad."
Transactional Analysis Dealingwith Depression
19
In ego states people are not playing roles-rather, they are shifting from one state of being to another. When the child shifts from feeling hurt back to feeling loved, he shifts his entire state of being. Most adults have disciplined children, feeling at the same time, "Oh, I wish I hadn't cracked down so hard." So, I am not talking about roles here, but rather about the shift of the state of being and the phenomena that differ in the various ego states. A six-year-old child hears that his mother is going to die of cancer. The family tries to shield him. He knows that something is going wrong because the adults are all acting differently. They give him less attention. He will ask why, and maybe they will tell him the truth. Finally, he feels total despair. "My mother is going to die. Who will love me? Who will feed me?" That is easy enough to understand about a six-year-old. What he has done is to hear a fact from the outside world from which there is no escape. He will feel despair when she dies. He will feel sadness. That is not enough to create depression. What is needed in addition to despair is for the inner Parent to crack down on the child and figuratively blame him, producing guilt. "You dirty little rat, you should have studied. You caused your mother to get cancer by worrying her so much." The fury that the Child experiences from the Parent is clear. If he puts that together with his loss, the Child will have everything needed to create depression. And when that happens, he will feel that all hope is lost. He will unplug his Adult facade just like pulling the electric cord out of the wall. When that big Parent on top is beating down on the little Child on the bottom, it is very easy to predict the outcome. At best, such a child will feel bad; at worst, he will have such fears as a child commonly has between three and six years of age. One such fear is that his father will hurt him physically if he gets angry with him. Another fear is that his father may get so angry or disappointed with him that he will leave him. These are the fears that a young child may have, and these are the fears that he has when he begins to go into a deep depression. The Adult with a capital "P:' does not experience loss. A man may register the fact, for example, that his mother is dead, and within him is a Child who cries. Maybe the nurturing Parent says, "Poor Mom, she wasn't having any fun in the nursing home and
20
DEALING WITH DEPRESSION
wasn't able to walk, anyway. Though the Child in me hates to lose her, I am glad she is gone." The Adult only registers the fact that his mother is dead. The Parent and the Child ego states do the feeling. Now it becomes more apparent why putting an arm around a depressed person and offering tender loving care does not work. That person is so busy listening to the Parent in his head telling him what a worthless, hopeless thing he is that he cannot hear words of support or comfort. With his Adult virtually unplugged, all he will feel and believe is that he is a big, bad guy. He will not even understand that people can die and that it is only a matter of time before he will recover from his depression. Sometimes the depression is so severe and the Adult so unplugged that the psychiatrist has to take over and hospitalize the patient, prescribe medicines, and in certain cases, even use electroconvulsive treatment. In spite of the disadvantages, there are some cases of depression that still need electroconvulsive therapy. It can be lifesaving for severe depression. It is also useful for the sudden onset of other types of psychosis. In this situation, though, the treatment seems to help in ways not fully understood. There are many theories about it. The electrical theory maintains that the situation is similar to when a radio is not working and it is jolted by a slap and then begins to work. Maybe the connections fall into place better. The chemical theory, which maintains that the electrical induced convulsion changes brain chemistry significantly, is gaining acceptance today. The chief psychological theory is that depressed patients regard this treatment as punishment-putting them to death and letting them come back to life, though this theory sounds farfetched. Regardless of what happened, the technique is still sometimes used as a treatment for severe depressions. There are other ways in which to help most depressed patients get well. These methods may take a little bit longer and there may be a risk of suicide during the early part of the treatment. Many years ago I was asked to see in consultation an elderly woman who has since become one of my favorite people. When she was not depressed, she was writing critical letters to congressmen. She was a delight. However, when I first saw her, she was a picture of severe depression. While she was talking to me about her depression, I sized her up with my Child and then with my Adult. I decided to take a therapeutic risk and called her by her first name, in spite of
Transactional Analysis Dealing with Depression
21
the difference in our years. I said, "You are a greedy, selfish bitch." She turned to me with surprise and then she said, "Thank you, doctor; you are right. Will you be my doctor?" Now, this woman was not crazy. What I did was to take over for the Parent in her head that was beating on her. I externalized it in a way that she could feel. A great many counselors were trained not to be directive. There is an old joke about the non-directive therapist on the fourteenth floor of an office building, sticking his head out the window and saying to the patient who has just thrown himself out, "You feel like killing yourself?" That is neither good medicine nor good loving. In the transactional analysis (TA) treatment of depression, the first thing to do with a mild, moderate depression (or sometimes even a severe one) is to get a contract with the depressed person for his own life. The analyst attempts to get the Adult part of the patient to agree to this. The treatment dialogue goes something like this: "No matter what happens, no matter how bad I feel, I will not kill myself, either accidentally or on purpose." If he does not have a defective brain function from drugs or old age, the patient is asked how long he will abide by this statement. If the analyst can get the contract with the patient's Adult ego state, even though the patient may feel like killing himself, he will honor the contract. This is one of the most fantastic things to me about transactional analysis: to get a contract from somebody that he will not kill himself. I think many psychiatrists have had some of their patients surprise them by committing suicide. The contract for life is something that should not be done lightly. I frankly do not think that TA can be learned from simply reading about it in a book. Second, the analyst asks the patient's Adult ego state, "Do you want to feel differently? And, if so, how?" Then, if the analyst feels it is possible to help, he can enter into a contract with the patient and emphasize building the relationship. First the patient needs to know that there is a future; there is some help. In this kind of situation a member of the clergy could be of particular value. If a pastor tries to come in and administer tender, loving care to a depressed patient and talks about how God loves the patient and gave His only begotten son for him, I would tell him it was not the best way.
22
DEALING WITH DEPRESSION
There can be a danger, in fact, in clergy and physicians enjoying TA if they have had only a minimal exposure to the method themselves. Most ministers are not going to know how to treat a psychotic depression. They might know how to help a person whose depression is mild. Maybe ministers could cure mild depressions and refer severely depressed people to trained psychotherapists. The essence of transactional analysis can be taught in about one year, providing students get supervision following that introduction. My own pastor has instructions from me, that, if I get sick and I am seriously ill, to please come and read the Twenty-Second Psalm. When I feel bad, I can understand how that psalmist felt. After getting a contract with the depressed patient, the analyst should seal the leaks (contaminations) of the patient's Adult ego state, possibly by giving a command. To many psychiatrists who have been trained to think that in order to help a person get well you must help them understand, this command may seem surprising. I hope I help them to change. When a person is depressed, change is the necessity; understanding, the luxury. I ask depressed people what they want to change. I make contracts with them that they can fulfill. Along the way I may have to give a particular patient permission to live. The first part of this permission is the command, "Don't kill yourself." I gave this command in a mild form to a woman who had gotten in trouble before. She was beginning not to talk in the group she was in and was beginning to look "down in the mouth." I asked her about it for two weeks in a row. I knew something was brewing and she hesitated to ask, which was a sign of regression for her. She said, "I have had a dream that keeps coming that I am jumping off a building." I stopped her right there and ordered, "Don't jump off any building! Will you agree not to jump off any buildings this week no matter where you are or no matter how you feel?" "Yes," she replied. The group asked me, "What caused you to say that?" I replied, "Because it is recurring in her dreams and I want to make very sure she doesn't jump off any buildings." At first, my command was: "Don't jump off any buildings," then from my Adult I asked, "Will you agree not to jump off any buildings?" I followed up with one more statement for the Adult, "If you do, you would kill yourself or get severely hurt and then you couldn't get well."
Transactional AnalysisDealingwith Depression
23
It is difficult to motivate someone who doesn't want to change, but transactional analysts do try. The easiest way to do this is to contract with the Adult. A man came into my office with "chips" on both shoulders. I asked him what he wanted to change about himself. He replied, "Change? My doctors just told me to come to see you." I said, "Well, you have seen me already; is there anything else you want?" At that point, I was talking to his Adult and we were not playing games. The man answered, "No, I just came down here to get my doctors and my wife off my back." I said, "Well, if it doesn't work, and you want to go further, let me know." We decided not to waste our time and his money. Transactional analysts use three P's: permission, potency, and protection. I had to be potent enough with this woman and have enough of a relationship with her that from my Parent ego state I could say, "Don't kill yourself!" That command was from my Parent state to her Child state. Then I had to tell her why and get an agreement with her Adult not to do it. I not only tried to help that person to stay alive, but in addition, I had an even tougher job. Her Parent state was still beating on her Child state when she wanted something, when she wanted to be taken care of instead of giving all the time to other people. That was not a way to get strokes or recognition for the Child state in her. My job with her was to make my Parent state stronger than hers so she would hear: "Don't kill yourself!" My next job was to get her to see what the facts were. "Did your mother truly want you never to need anything for yourself?" The answer was "No." Unfortunately, this woman was overtrained. Most people have been overtrained, not to the extent that they just regulate their behavior, but that they have overregulated so much that they do not even know what they feel. Parents only want children to regulate their behavior when they are little. I wish clergy would emphasize the humanity of Jesus more, because a lot of my patients have never heard about it. They never even knew he got thirsty like other people, or that he was lonely and wanted somebody to be with him. Instead, they think that a good Christian is somebody who never has needs and who always gives to and loves his neighbors instead of himself. This is a Parent precept. It is not a fact; it is not a safe way to live. If there is a Child
24
DEALING WITH DEPRESSION
in a person who never gets loved, or taken care of, then that person in all probability will suffer depression.
BIBLIOGRAPHY Babcock, Dorothy and Terry Keepers. Raising Kids O.K. New York: Avon, 1976. Barnes, G. (ed.). TA After Berne: Teaching of These TASchools. New York: Harper's College Press, 1977. Berne, Eric. A Layman's Guide to Psychiatry and Psychoanalysis. New York: Simon & Schuster, 1957 (also Grove Press, 1962). Berne, Eric. Transactional Analysis in Psychotherapy. New York: Grove Press, Inc., 1961. Berne, Eric. The Structure and Dynamics of Organizations and Groups. New York: Grove Press, Inc., 1963. Berne, Eric. Games People Play. New York: Grove Press, Inc., 1964. Berne, Eric. Principles ofGroup Treatment. New York: Grove Press, Inc., 1966. Berne, Eric. Sex in Human Loving. New York: Pocket Books, Inc., 1970a. Berne, Eric. The Mind in Action. New York: Pocket Books, Inc., 1970b. Berne, Eric. What Do You Say After You Say Hello. New York: Random House, 1972. Blakeney, Roger N. Current Issues in Transactional Analysis. New York: BrunnerlMazel, 1977. Bontrager, John. Free the Child in You. Philadelphia: Pilgrim Press, 1974. Brown, M. and S. Woolams. TA: The Total Handbook of Transactional Analysis. Englewood Cliffs, NJ: Prentice-Hall, 1979. Bry, Adelaide. The TA Primer. New York: Harper & Row, 1973. Gold, Mark S. The Good News About Depression. New York: Villard Books, 1987. Goulding, R.L. and M.M. Goulding. Power is in the Patient. San Francisco: TA Press, 1970. Harris, Thomas A. I'm O.K.-You're O.K. New York: Harper & Row, 1967. Harris, Amy and Thomas A. Harris. Staying O.K.: How to Maximize Good Feelings and Minimize Bad Ones. New York: Harper & Row, 1985. Hartogs, Renatus. Four-Letter Woni Games. New York: Dell Publishing Co., 1968. Horewitz, James S. Family Therapy and Transactional Analysis. New York: Aronson, 1982. James, Mureil and Dorothy Jongeward. Born to Win. Reading, MA: AddisonWesley Publishing Co., 1971. James, Mureil. Born to Love: Transactional Therapy in the Church. Reading, MA: Addison-Wesley Publishing Co., 1973. James, Mureil. Transactional Analysis for Moms and Dads. Reading, MA: Addison-Wesley Publishing Co., 1974. James, Mureil. (ed.). Techniques in Transactional Analysis. Reading, MA: Addison-Wesley Publishing Co., 1977.
Transactional Analysis Dealing with Depression
25
James, Mureil. Marriage is for Loving. Reading, MA: Addison-Wesley Publishing Co., 1979. James, Mureil and Louis Savary. The Power at the Bottom of the Well. New York: Harper & Row, 1974. Jorgensen, Elizabeth W. and Henry I. Jorgensen. Eric Berne-Master Gamesman: A Transactional Biography. New York: Grove Press, 1984. Meninger, J. Success Through Transactional Analysis. New York: Grosset & Dunlap, 1973. Morrison, James H. and John o 'Hearne. Practical Transactional Analysis in Management. 1977. Murphree, Jon Tal. When God Says You're O.K. Chicago: Inter Varsity Press, 1975. Oden, Thomas. Game Free. New York: Dell Publishing Co., 1974. Reuter, Alan. Who Says I'm O.K.? A Christian Use of Transactional Analysis. St. Louis: Concordia Publishing Co., 1974. Rowe, Dorothy. Depression: The Way Out of Your Prison. Boston: Routledge and Kegan Paul, 1983. Schiff, Jacqui Lee with Beth Day. All My Children. New York: J.B. Lippincott Company, 1972. Shepherd, Martin and Marjorie Lee Shepherd. Games Analysts Play. New York: Berkley Medallion Books, 1970. Spiegel, John. Transactions: The Interplay Between Individual, Family and Society. New York: Jason Aronson Publishers, 1972. Steers, D.A. Bodily Expressions in Psychotherapy. New York: BrunnerlMazel, 1983. Steiner, Claude M. Games Alcoholics Play. New York: Grove Press, Inc., 1971. Steiner, Claude M. Scripts People Live. New York: Bantam Books, 1974. Websters II New Riverside University Dictionary, Boston: Houghton Mifflin, 1984, p. 364. White, John. The Masks ofMelancholy: A Christian Physician Looks at Depression and Suicide. Downers Grove, IL: Inter Varsity Press, 1982.
This page intentionally left blank
Chapter 3
Pastoral Counseling Dealing with Depression Myron C. Madden Richard Dayringer
Let's start by breaking down the words transactional analysis: the analysis of human transactions. What is a human transaction? Did you ever go down the hall in the morning and say "hello" to someone, just about the time that person vanished up the other corridor and missed your greeting? The transaction did not happen because to have a transaction necessitates at least two people communicating in some way. The human brain keeps a record of how many transactions a person owes and is owed with the weight a bit heavier on how much is owed rather than the other way round. In commerce, it is easy to say that so many dollars and cents are owed, but in human transactions such precise measurements are impossible. Market transactions usually are clean; emotional transactions are more often murky. A very depressed woman came to see me once, complaining about her sister who lived in Denver. Ostensibly, my patient, whom I will call Anne, was concerned because her sister Sophie weighed about 250 pounds and because she could not get any help for her. Anne had sent Sophie three or four books to read and the names of several good counselors. It came out in Anne's narrative that their father had died about six months before, and so she was concerned about losing her sister, too, if she did not improve her health. Anne asked if I had any suggestions. 1 asked, "What would you give to get your sister well?" She replied immediately, "I would give my inheritance." (I asked Anne this question because 1 wanted to 27
28
DEALING WITH DEPRESSION
reduce this situation to a "cash" transaction.) We continued talking about how Sophie had not taken any of the advice she had given. As she talked, Anne began thinking a bit more. She said, "Well, really, I would not give Sophie all of my inheritance. I guess I would give her half of it." Later I said, "Well, what do you think you have to do to help your sister?" At this point, Anne charged, "Really, I think that I have done all I can do-I have done it all." When she got ready to go I stopped her. "Well, let's put it back in cash terms, what would you give to help your sister?" Anne concluded, "I wouldn't give her a dime. I don't owe her anything." What do people really owe each other? For example, husbands and wives cannot communicate in the real sense of the word unless they know what they owe each other. What does a husband owe his wife for having been rude to her in front of their company? What does he owe her for letting his brother come to live with them and eat their food while he goes to college? What does she owe him for three trips over to her folks' house and none to his parents' home? People build up obligations and those obligations are important. Depression is often the result of being frustrated by what people owe and are not paying.
DEALING WITH DEPLETION AND EMPTINESS Depletion and emptiness are important to pastoral counselors. Dr. George W. Truett's daughter told me several years ago when I was a pastor in her neighborhood that her father used to come through the house tearing his hair out on Saturday nights saying that he just could not deliver another sermon. Then on Sunday night, he would repeat the scene saying, "But I don't think that I can do it again." There is a problem of depletion and emptiness because people agree to accept the responsibility to inflate others' egos and keep them pumped up. This responsibility includes loving them, supporting them, making them happy. Given the fragility of human nature, though, it is difficult to find people who are secure enough in their own needs to take on such an awesome responsibility continually. Among physicians and clergy, this can become a problem. As professionals, both groups like to appear independent, to appear as if they do not need love. This is just a false front. They do need their
Pastoral Counseling Dealingwith Depression
29
patients' and parishioners' strokes. Because people cannot work independently of each other, strokes are an everyday necessity. People who run out of strokes are prime candidates for depression. Now, let me deal with this from the standpoint of losing meaning. People get depleted and empty when meaning is lost-when it is out of joint. In Shakespeare's The Merchant of venice, Antonio complained, "I do not know why I am so sad; it wearies me. You say, it wearies you, but where I found it, came by it, where it is born, I am yet to learn." At such times, a feeling of sadness predominates. Then, in the middle of this situation where meaning is lost, desire becomes a threat. Pain and pleasure are mixed together to the point that every time there is a movement toward desire, pain comes. This is not true in the animal world; animals get pain and pleasure in separate places. Human desire, though, reaches out and wants to be fulfilled, but runs into the edges of pain. For the baby, there is no anxiety over food, but for the adult weighing 300 pounds, there is. Even the pure pleasure of sexual feeling to the child is soon met with the parental message, "Don't touch it, lest you die." That message goes all the way back to the Garden of Eden. People have the feeling that if their desires are fulfilled, they will run into the edges of pain; they will suffer disapproval and rejection. Love cannot even be pure, free-flowing, and single-hearted. There is always a problem concerning whether someone is being too loving or not loving enough. Jealousy is a factor for the person not receiving enough love. It is very human to make one particular individual the number one person in your life. But it is not possible to make two people number one, is it? On the other hand, it is possible to be number one to more than one person. I know a man who is number one to about fifteen people. He lets them make him number one, but if they ever call for the contracts, he is in trouble. I know of no ministers or physicians who can avoid these pitfalls all the time. A parent may be number one to several children, but that will pass because they will later make someone else their number one. Even God is associated not only with love, but with pain. Meaning comes from understanding what God is really like. Sometimes a psychological approach helps in understanding what God is like. I counseled another very depressed person several years ago. She
30
DEALING WITH DEPRESSION
discussed religion a bit and I asked, "What is God like to you?" She said, "I am sort of embarrassed to tell you, but God, to me, is a gray blob." I asked, "Can you draw it?" I put a piece of paper out and she drew an oblong circle on the paper and said, " Now it is all gray inside. When I am happy, it tends to have a little pink trim around the edge, but otherwise it is always gray. That is God; that is what I see when I pray." When she came the next week, I asked, "How are you and God in terms of the gray blob?" She said, "You know, that gray blob is not God. That is me! Can't you tell that?" I asked, "How could I know that?" She answered, "By the way I dress." I said, "Well, come to think about it, you never wear anything but gray or dull colors." She replied, "But I am going to put some color into my life." This ambition cost her husband the price of a new wardrobe because she got this image of God as being gray, dull, and unhappy out of her system. The God who had been revealed to her through traditional religion was not the one who is the God of the Bible. The Jesus of the Bible is the one who, as Karl Olsson says, is "at the party" (Olsson, 1972). He wrote the book Come to the Party, dealing with happiness, relationships and just "being with it!" Depletion and emptiness emerge when choice becomes tedious and difficult, and when choice absorbs all energy. There was a mentally ill patient in Kentucky who was trying to stop smoking. He would smoke a cigarette down about halfway and then look at that cigarette and finally throw it down on the floor. He then proceeded to walk around the room, go back and pick it up, and take one more draw. Then he would throw it down again. He continued until he would almost bum his lips. Another patient watching this, said, "There is nothing wrong with him; he ain't crazy, he just can't trust his judgement." He just could not make a decision. Every time he sucked up the pleasure, he ran into the pain. Life is full of paradoxes, and choices become extremely difficult because people are not able to invest. Instead, they enter into what I call the "dialectic of despair." This is the inner dialogue that keeps running into the "opposites." It is human nature to look one way and tum the other-going back and forth in an endless cycle between two positions. It is the despair that is the literal breathing out. One way to recognize depression in people is to note the way they sit down and sigh or exhale. To be inspired is to breath in-to take air
Pastoral Counseling Dealingwith Depression
31
into the body. The "dialectic of despair," however, is more of a breathing out and emptying, and not being able to be filled. I call this the dialectic between the past and the future. In other words, despairing individuals try to change bad fortune, or whatever mistakes that were made in the past. They are attempting to go back and unlock the past so as to get it straightened out and make everything come out right in the future. This is impossible. In World War II, I was a chaplain overseas in Europe, and a lot of soldiers came to me and confessed that they had stolen things during combat, and would like to be forgiven. I requested that they give the stolen objects to me. They replied, "You never could get them back to the right persons." I told them, "We'll get them into the hands of people who are closer, next of kin or something. These things don't belong to me or you." They wanted to settle scores to quiet their consciences, but not at the cost of giving up what they had stolen. Attempts to open the past imply that there are choices yet to be made in the past. Depressed people may go to palm readers or fortune tellers to get the future opened up. When they feel the future is sealed, they become more depressed. If the future does not have any possibilities, then life seems to be over. Pastoral counselors, then, must deal with a future that has possibilities. Some people fear a fate that makes all things necessary, as if everything had already been written down at creation and must occur according to a timetable. To seal down the past and open the future is how people can make honest choices. They need to accept the past. The past is there. People cannot change what they are or the choices they have made. Yet there are opportunities and choices to make for tomorrow. Having those choices can get depressed individuals moving again-out of the past and into the future. People can also become depressed when they forget the "party" that I mentioned earlier. My wife said that the church took away the party for her, that it became the judge. She said that we never really had parties; we had "socials." Some people do not believe in parties. There are others who believe, but have decided they never will be invited. Some go but not unless they can wash the dishes to earn it! And then there is that group that can go and stay and celebrate, God bless them! That is what it is all about: being at the party and
32
DEALING WITH DEPRESSION
celebrating. Once I met with some clergy and asked, "If you gave the party of your life, who would be the first ten people that you would invite?" They sat there for a long time, talking to one another. One asked another, "Would you have the Bishop?" There was no reply. And one guy asked, "Would you have your wife?" His friend replied, "I couldn't have a party if my wife was there." One man didn't have anybody on his list when the time was up and he said, "I can't give a party." The kingdom of God is a feast and a party. It is the prodigal son who returns and rejoices, and his father throws the feast of his life for the prodigal. What type of action can be taken to deal with depletion? First, a sensitive counselor moves into the emptiness. I found that I was moving into the emptiness when I counseled the lady with the gray blob, and she found some color. It is important not to just camp at the edge of people's wilderness. If they will invite you, walk to the center of it. I believe that the wilderness in people's lives has a gift in it, and that it can be shared. When that gift is shared, the givers are blessed if they authorize the sharing. The telling must not be some kind of spiritual burglary or theft whereby one person breaks in and steals the property of another person. It must be by invitation. At some points all human beings have something that seems to be unsharable. For example, a lady told me once, "I've got something to share with you that you have never heard." I asked, "How do you know that I can hear it?" She replied, "You have a reputation of being able to hear things." I said, "But I am not sure that I can." (I was speaking to her feelings.) "Oh, I know that you can hear it," she answered. I answered, "It might be too big for me." (You see, that is the way she felt.) The woman replied, "Well it is big. I have carried it for over eighteen years, but I just cannot carry it any longer." I told her, "But I might have to run out into the hall and shout or scream, 'Somebody help me, I've heard too much.'" She insisted, "You wouldn't do that!" I said, "You don't know." Then she pulled her chair up and said, "I'm going to tell you, anyway." Now, wouldn't you like to know what it was she told me? The story stops there! Moses had something that was tough to share. He had to come back and tell those Israelite people that he had been out in the
Pastoral CounselingDealingwith Depression
33
wilderness and had seen a talking bush that was burning and it did not even bum up. I would hate to bring that story into camp. It's beautiful, though, because he shared it, and it makes me feel as though I am not so crazy! Sometimes people who are mutually depressed can sit together, but they are not going to help each other much. I have little ability to help anyone else when I am depressed. If a person comes to me for treatment of a depression, and I am depressed myself that day, I know that I am not going to be able to help. In such a situation, I would set up an appointment for the two of us to meet later when I was feeling better. This person does not have to be told that I am also depressed; it probably is obvious. It is not necessary to share my depression; however, at some point in the future, it might be good for that person to know that I suffer from depressions, too. Sometimes laughter is used to overcome feelings of depression. My mother was laughing all the time, even though we lived in first-class poverty. But we were happy. I remember one of the early depressions that I had. It was when my mother told me that we were poor. With her good laughter and the parties that she had going all the time, I thought we were rich. People help others when they agree to share. Religious people feel the need to give their crazy stuff to the clergy so the clergy can take it and bring some affirmation. Clergy do not help people by serving as perfect examples; they help other people by being human. Good counselors lead with their weaknesses and strengthen others by allowing them to see it as such. I was at a party one night with a group of doctors and their wives. On meeting one woman, I was surprised to hear her say, "Oh, yes, Myron Madden. I know you. You live next door to my best friend. I know everything about you." She had heard that there was not always peace in my house and she was greatly consoled by that. Therefore, this woman could afford the courage to relate to me that she knew I was not perfect. She felt I was a human being because I fought with my wife and children as she fought with her family. It is okay to be human and it is humanity that affirms other people. Yet people do not share their heavy loads. Their reticence causes tension and depression. Sometimes it takes other people to help me understand myself. I can only understand my problems in the terms of other people.
34
DEALING WITH DEPRESSION
People often feel that they are the only ones who have ever had certain feelings. Such a statement can never be true. However, feelings of an unusual burden, or an unusual problem that no other human has ever had, or ever will have, illustrate the necessity of some public rituals of atonement. If people can only take the story of the cross as the good news that God is communicating his message that they are accepted no matter what the circumstances, then the story of the cross is effective. If they are not able to understand or accept this message, then these individuals must atone in some other way. People develop private rituals of suffering, work, or striving. FINDING AND GIVING AFFIRMATION
One of the real problems of depression is a fear of looking at death. Once defenses are stripped, death seems all-pervasive. Someone once said, "Men cannot look either at death or the sun for too long." A part of depression is the fact that people cannot get their eyes off their mortality, and they cannot be consoled. They go around like Hamlet, trying to release themselves from the fear, but they just don't know how. Death is the ultimate curse! Still, it is not really a curse. Where would the world be without it? Yet people spend a lot of time trying to get above it. Death is the curse at the gut level. Children feel death as something personal. It is a force that gets up and walks and stalks and searches out people and catches them. When it gets hold of them, they have had it. A child perceives of death as a catcher, and a stalking force. I visited the roommate of a man who had died in the hospital and asked him how he was. He said, "Well, it could be worse, death came in here today, and it missed me." He made death a personal visitor who passed him by. Now that is not what death is, but that feeling is understandable. It is a feeling that carries over from childhood, and that is the curse. It is a psychological distortion of a very natural process. Picked up from the old wives' tales, this perception gets reinforced with late night horror shows on television and in movies. So how can a child escape feeling that there is such a powerful dread force? The strength of the book and movie, The Exorcist (Blatty, 1971), is evident when people start believing that
Pastoral CounselingDealingwith Depression
35
death is mobile and preparatory. They assign its actions to demons. Death is not mobile and preparatory though. It is still, noncommunicative, helpless, powerless, motionless, silent. It is a nothing. It is not a person; it is not a power; it is a nothing. Unless death is viewed in this way, a person is split and the death demons are given energies for pursuit. Demon power is more possible for those who have strong belief or strong fear. Now, it is helpful to discuss the subject of blessing. Let me state it a little differently. A counselor cannot affirm an individual without that person's consent. In the same way, a minister cannot bless unless the person assigns the right to bless. I believe that the task of clergy, physicians, and others in the helping professions is to learn to get the authorization from patients to bless and affirm them. All the authority acquired from hindsight, theology, and science is useless without that right. Until a particular patient says, "Okay, put it on me," it is useless and worthless. Every patient has the right to say "No" to anyone in the health professions. That is a tough lesson for some healers to learn, but patients do have that right. One of my students came to me weeping. A patient had told him to "Get lost; I didn't send for a chaplain, and I don't want to see one now or any time." I asked my student if he had talked to the nurses on that floor about this man. He said he had not. Inspired, the student told the nurses what his patient had said. They felt so good because the same patient had been telling them to "get lost," too. If he had said it to the chaplain, then, fine, everybody felt better. My student got blessed in ways he did not expect-by sharing his hurt with people who needed to hear it. A blessing is a very potent force. What is it? The biblical character named Abraham believed himself to be the friend of God and to be blessed by God. He understood blessing to be something that he was to pass down to his seed (his children). Abraham did not perceive of a blessing as something that could be given at peer level, but something that went from the parent to the child, from the authority position to the dependent one. So the concept of blessing was passed down through the generations-authority blessings. What was Abraham's blessing? It was the giving of the father. When Abraham got old and was about to die, he called his son, Isaac, and he blessed him with his castle, his land, and all that he
36
DEALING WITH DEPRESSION
possessed. He poured it on him, he unloaded; he emptied himself. Abraham's blessing symbolized the fact that he was giving Isaac his potency, his sexual strength, his capacity to be a father, giving him all that he had-everything. He blessed him! That was blessing; that was affirmation. The first step of creation, the birthright, is bringing a person into being. That is a kind of blessing, isn't it? The second blessing in the Abrahamic tradition is to bestow all that one is. The blessing is an emptying: I reserve nothing, I give it all to you. Other people mayor may not pass on the blessing, but that is the risk. They may keep it. They may not respond. The work of blessing is giving what one has received to another. It must have been a very difficult task when Jesus started his program with 12 laymen: fishermen and tax collectors, instead of a group of seminary graduates. The people of Israel wanted Jesus to put them first-make them number one. Jesus said in effect, "No, no special treatment for Israel, no special treatment for anybody." What does it take to be able to affirm people? This is a very important part in the process of helping-affirming people, giving out information and blessings. Defining blessing is difficult; it is like trying to define life. Abraham has to have a son to bless. Jesus had no son, so he could put blessing at the peer level, which is the mature level of blessing. The family picture of blessing is still related to childhood growth, though. Children grow in patterns of blessing in families. I had a man whom I was counseling once, the oldest of two sons in a family with no daughters. I find that the eldest son is hardly ever the most blessed by the father. The eldest daughter is seldom ever the most blessed by the mother. The second son is usually the father's most blessed child, and the second daughter is the mother's most blessed child. The first son is most often the mother's specially blessed child. I asked my patient, "Did you get your father's blessing?" He replied, "Oh yes, I got it." Later, he called me and said, "You asked if I got my father's blessing; what did you mean by that?" I asked, "Well, why are you calling?" He said, "My brother, who was younger, got married first, and he had three children. When each of his children was born, my father gave them forty acres of land and one hundred shares of oil stock. Now I have had
Pastoral CounselingDealingwith Depression
37
two children and have received no land or oil stock. Is that what you are talking about?" I said, "It could be; it just could be." Esau said, "Bless me also my father!" But Isaac had to tell Esau, when he came crying for a blessing, that he had already cut it all off the bone for Jacob. Think in terms of heirlooms that come down through the family. There is a blessing in heirlooms because affection was invested in these things. Families become divided over them. They are not really divided over the heirlooms but they are divided over the blessing-over the love. I saw two daughters really fighting in the room when their father died. One said, "I always loved him a little more than anyone else." The sister shouted, "How dare you say that!" (This was said over the man's dead body.) They started arguing. Partiality is a very painful thing, and it often happens. One child is preferred over another. Partiality is always good for the recipient; it is painful when it goes the other way. I am sure Cain felt jealous of Abel because Cain saw the sparkle in his father's eye going to Abel. Most people are all too familiar with this feeling. It is a human trait to search out the partiality of favoritism. But this arouses feelings that are very painful. So, some siblings try not to recognize this favoritism or to deny it. It is still there, though. This explanation is not meant to cause despair; it is not my intent at all. I have worked at understanding the concept of blessing for many years and I still do not understand it fully. I do understand that this is what motivates people. They want blessing. People want affirmation. They need affirmation; they need love, they need acceptance. Also important is the energy of blessing that implies "I am okay forever; I am an okay person. I don't have to base it on what I do, and I don't have to base it on what I have done. I don't have to base it on how I was born, my race, my nation, or my background. It is a gift." A powerful affirmation permits me to affirm other people, if they allow it. It is a high, holy privilege to give the affirmation to others and to help them feel that it is all right to be themselves. People not only need to accept themselves as they are, but they also need to accept the process of choosing the self. Another time I was counseling a woman with severe depression. As she told me her story, I got the picture of a person who had never been herself. I
38
DEALING WITH DEPRESSION
asked her if she had ever been herself. She replied that she had acted and played games all her life! I asked, "Why haven't you been yourself?" "Well, I didn't think I could ever get any acceptance for myself," she said. I asked, "Who is 'myself'?" She replied, "Myself is a formless child way back in the past." I said, "Your task is to go back and get that child." She sat there and screamed, "No, I can't; I won't; I am going to go on playing this game until I die." I told her, "That is your choice then." She said, "Don't let me do that; I can't do that." I said, "You can either go back and get that child that you have put on somebody's doorstep a long time ago, and raise it, and make it yourself or you can go on acting. It's your choice. I am not going to be the boss." With that she started going back to get that child. It was tough raising a child that had been left out in the cold that long. But she could never have been blessed as somebody else. She had to be blessed as herself. She would have been very contemptuous of me if I had blessed her in a false position. Depression nearly always serves a purpose. If we can help people get in touch with the need being met by the depression, they will be in a position to decide if their "game" is worth the effort. I think much depression is the suffering we do to avoid some painful encounter or responsibility. The woman who had lost her sister later went through much grief because she had never grieved for her sister. Instead, she had taken her sister's place. Since she was living for her sister, grief would have been out of place-no tears were shed. When she was in her 30s, she had to go back and rescue herself at age 14 and start over. That was not easy. She told me that if she had known how difficult going back was going to be, she might not have attempted it. People acquire the energy to choose themselves when they eliminate all other possibilities. We can't be any of these other selves. We can't be any of these other persons. We can't get rid of ourselves and become another-as delightful as that might feel. The only choice is whether to choose the self or to evade it. There are about as many choices for people to become something different from what they are as Adam had about whom he was going to marry. The question of blessing is a very powerful thing in the family, in the church, and in society. To bring blessing is to open the window to the sunshine.
Pastoral CounselingDealingwith Depression
39
BIBLIOGRAPHY
Abbott, Joe B. "Depressive Reactions and Pastoral Care," in Pastor and Patient, Richard Dayringer (00.). New York: Jason Aronson, Inc., 1982, pp. 29-38. Anderson, Margaret J. Help for Families of a Depressed Person. St. Louis, MO: Concordia Publishing House, 1983. Anthony, E. James (ed.). Depression and Human Existence. Boston: Little, Brown, 1975. Arieti, Silvano and Jules Bemporad. Severe and Mild Depression: The Psychotherapeutic Approach, New York: Basic Books, 1978. Badal, Daniel. Treatment of Depression and Related Moods. Northvale, NJ: Aronson Press, 1988. Benson, George A. What to Do When You're Depressed: A Christian Psychoanalyst Helps You Understand and Overcome Your Depression. Minneapolis, MN: Augsburg, 1975. Blatty, WilliamP. The Exorcist. New York: Harper & Row, 1971. Crammer, L. Up from Depression. New York: Simon and Schuster, 1969. Fairchild, Roy W. Finding Hope Again: A Pastors Guide to Counseling Depressed Persons. New York: Harper & Row, 1980. Gaylin, Willard. The Meaning of Despair: Psychoanalytic Contributions to the Understanding ofDepression. New York: Science House, 1968. Gaylin, Willard. Psychodynamic Understanding of Depression. New York: Jason Aronson, 1984. Geddies, Jim. The Bright Side ofDepression. Nashville: Broadman, 1985. Hart, Archibald. Coping with Depression in the Ministry. Arcadia, CA: Cope Publications, 1980. Hart, Archibald. Counseling the Depressed. Waco: WordBooks, 1987. Hauk, Paul A. Overcoming Depression. Philadelphia: Westminster Press, 1983. Klein, Donald and Paul Wender, Understanding Depression: A Complete Guide to Its Diagnosis, Course, and Treatment. New York: Oxford, 1992. Kraines, Samuel H. and Eloise S. Thetford. Help for the Depressed. Springfield, IL: Charles C Thomas, 1982. LaHaye, Tim. How to Win Over Depression. New York: Bantam, 1976. Madden, Myron L. Claim Your Heritage. Philadelphia: Westminster Press, 1984. Madden, Myron L. Blessing: Giving the Gift of Power, Nashville: Broadman Press, 1988. Madden, Myron L. and Mary Bea Madden. The Power to Bless. Nashville: Abingdon Press, 1970. Madden, Myron L. and Mary Bea Madden. Raise the Dead. Waco: Word Books, 1975. Madden, Myron L. and Mary Bea Madden. For Grandparents: Wonders and Worries. Philadelphia: Westminster Press, 1980. Mendelson, Myer. Psychoanalytic Concepts of Depression. New York: Spectrum Publishers, 1974.
40
DEALING WITH DEPRESSION
Minirth, Frank B. and Paul D. Meier. Happiness Is a Choice: Overcoming Depression. Grand Rapids: Baker Book House, 1978. Olsson, Karl. Come to the Party. Waco: Word Books, 1972. Sparks, James A. Living the Bad Days: Why They Come and How to Survive. Nashville: Abingdon, 1982. Volkan, Yamik (00.). Depressive States and Their Treatment. New York: Aronson, 1985.
Chapter 4
Gestalt Therapy Dealing with Depression Byron Eicher Richard Dayringer
"Gestalt" is a word that simply means "whole" and Gestalt therapy is a process of psychotherapy developed by Frederick Perls (Shephard, 1980). When he died in 1970, Perls left the legacy of a very practical kind of psychotherapy that seems to lessen the years sometimes necessary to complete a psychoanalysis on a particular patient. The part of Gestalt theory that relates specifically to depression is called introjection. Considered one of the primary psychological defenses, introjection is one of the primary ways in which people become neurotic. Gestalt therapists encountering depression distinguish it from sadness because the latter is considered an active, alive state. When a woman is feeling sad, for instance, she is doing something. In fact, she may be crying and although she may be hurting, she is active, moving, and feels alive. Depression is a very different kind of state. It is a state where people feel immobilized, and have feelings of nothingness. For example, a young man experiencing depression feels that nothing is going to happen, that nothing works. There is no way out. There is no hope and consequently he enters what Gestaltists call an "impasse"-the state of being stuck, not being able to act, not being able to relate. The following diagram shows a continuum ranging from joy to sadness. A person can be anywhere within that range at any time. JOY - - - - -X - - - - - SADNESS STUCK POINT (Depression) 41
42
DEALING WITH DEPRESSION
Depression is brought about by what analysts typically describe as denial. According to Gestaltists, sadness and joy are both very alive states that are similar to each other. Since they are such different emotions, it seems hard to believe that they would be close together. Most people have had the experience of being totally sad and crying, and then laughing at the same time, feeling a peculiar kind of exhilaration. Hidden somewhere within each individual, and away from the surface games and roles people typically play, is both sadness and joy. People who do not want to get in touch with sadness, who refuse to hurt, deny that there is sadness in them. They argue, "Oh, no, I don't really feel so bad; it didn't really bother me; in fact, when he died I didn't even have any tears." It is these same people who deny sadness-and thereby deny access to another layer of themselves-who also deny the joy. Denial of both sadness and joy leaves only the mid-point of the continuum-depression. Depressed individuals suffer from nothingness and dearth of hope. This is the construct with which Gestalt therapists work. They strive to get at a person's sadness, or if they can, at that person's joy. Either may work just as well. Getting at feelings is a very practical kind of thing to do in psychotherapy. People having the neurotic personality (only part of the personality is affected and reality is not changed but may be re-evaluated), fail to discriminate between self and others. They do not know where they end or others begin. This situation is intensified because with depressed individuals, the boundary line is deep inside. In fact, that boundary between self and others is so far inside that depressed people have very little of themselves within the boundary of self. Along with denial, introjection causes depression. An example of the truth of this statement is shown to point out how people eat. Physical food is the food that nourishes the body. Psychological "foods" are handled in much the same way (Perls, 1947). People's eating habits will often provide a good idea of whether they are introjectors. The need for nourishment is a primary reason for eating. It is important to bite cleanly through a piece of meat. Some people kind of gum it, tearing the meat and mauling it around in their mouths. They are not able to act aggressively, that is, to bite cleanly. Instead, they almost swallow food whole, making it difficult
Gestalt Therapy Dealingwith Depression
43
to digest. If food rots in the digestive tract, they become sick. It could even poison them so that they throw up. In the process of treatment of neurosis, therapists attempt to get these people to throw up some of the undigested food they swallowed, some of those things they have taken wholesale without chewing and mixing and swallowing. If they would bite cleanly and chew and digest thoroughly, they could assimilate something. They could make that piece of meat a part of every cell in their bodies. Some people go around with their mouths open and great tubes down their throats. They take in anything anybody has to offer be it theories, ideas, philosophies, ethics, or morality. They take in ideas and people wholesale, buying people on faith. These individuals never learn to discriminate-to take something apart, chew it up, digest it, and really assimilate. Introjectors gulp food without chewing and without testing. In doing so, they lose much of the enjoyment of learning as they lose much of the enjoyment of eating. Introjectors end up stuffed full of everything that everyone else has put into them. Introjectors are people who use primary methods. They treat the world as though it were a giant breast. All they have to do is find the nipple, attach teeth and lips, and continue sucking. They will not have to chew and the food can be taken in a form that is readily digestible. This mechanism is usually in evidence with patients suffering from neurotic or psychotic depression. There are four general things Gestalt therapists can teach introjectors. First is discrimination, differentiating between self and others. One of the ways to tell when someone is not discriminating is to just listen to him. For example, he may use the pronoun "you" instead of "I." He'll say, "Well, you know how it is, and everybody has said that and all of us agree." Introjectors prefer to speak in collective tenus and not individual ones. A good therapist may respond to these generalizations by asking, "Who told you that? Where did you get that idea?" Introjectors often use tenus such as "should," "ought," "must," and "have to." The second thing to teach an introjector is resistance. Teach people how to resist the demands of the group. There are ways to teach resistance that do not approach rebellion. I rather like the idea of resistance in the way that Rollo May talks in his book Love and Will. May differentiates between the revolutionary and the rebel.
44
DEALING WITH DEPRESSION
(The revolutionary is the slave who rises up and slays the masterthere really are two slaves.) May advocates the rebel position rather than the revolutionary. Rebels do not support either the masters or the slaves, but instead act as agents to get the two to talk. People should be taught to be rebels and not revolutionaries. They should be taught to resist the demands of the group when the demands of the group become destructive to the self. Third, therapists need to teach that to assert dominance of individual choices is okay, even when these choices do not meet the needs of the larger group. To make choices based on individual value systems and individualities is all right. Fourth, introjectors need to be taught that they have the ability to rearrange their own experiences. They can take a group of experiences they have had, select from those experiences, and design a way to choose new behaviors. The primary task for Gestalt therapists in undoing the introjector role is to focus on establishing within their patients a sense of available choices and help them gain the power to discriminate between self and others. What do Gestalt therapists mean by power? They rely on a statement: "Take back your power." Introjectors are people who systematically throughout their lives have given away their power. In effect, these individuals have given away their power to say who they are. They have given to other people the power to tell them how to be, what to do, and when to do it. They have given away their power to live their lives from an internal frame of reference. Introjectors are always asking questions such as, "Would you tell me who I am? What do I do now? How do you think I should handle that? When would be a good time for me to start on that?" Gestalt therapists are opposed to answering such questions. They believe that people should be able to do things for themselves as much as possible. The essence of Gestalt therapy is to allow patients, by frustrating their attempts to manipulate, to learn that they can find their own answers. It is important to remember never to do for people what they are capable of doing for themselves. True support is something different. For example, if a therapist with a patient who cannot do something for himself is convinced that the patient is as incompetent and as worthless as he acts, then that therapist should go right ahead and help him. Of course, in the
Gestalt Therapy Dealingwith Depression
45
extreme case of a person who has broken a leg and is lying helplessly along the road, it is perfectly okay in the Gestalt philosophy to stop and give a hand. But in helping, it is important to get the sick person to jump along beside, keeping one leg off the ground. A therapist can be the other leg, but not for too long, and not to the point that any assistance has so fatigued him that he loses power to take care of himself. A good Gestalt therapist will suggest that the doctor aid the patient by putting on a walking cast or at least providing crutches. This way the patient can be an active participant in the healing process. The therapist can offer sympathy, but only if the end result is bolstering a sense of confidence and independence for the patient. In fact, the most healing dialogue for an introjector might go like this: "I can't walk." "Use your crutches." "The crutches hurt my arms." "Your arms will get tough after awhile." This attitude on the part of the therapist may appear cavalier, but it actually is the most considerate and responsible thing to do. Human nature being what it is, more harm is done both to the sick person and to his healer when the latter takes the whole burden from his shoulders. Let me put it this way: if you lift up a man and insist on carrying him, pretty soon you get tired and weak and collapse. By that time, the man's own muscles will have atrophied and he will not be able to walk by himself after you have fallen on your face. Probably he will blame you for having carried him for so long that he became unable to walk. He may even blame you for having interfered with his right to learn how to use his crutches. From this example, it is clear how therapists begin to feel sorry for themselves and decide that nobody appreciates them. They may feel all the more unappreciated if a particular patient threatens to commit suicide. However, here there is a positive approach. Perls said suicide is emotional blackmail, so you refuse to be blackmailed by anyone who has threatened suicide. If a young man who happens to be one of Perls' patients threatened to kill himself, Fritz probably would say, "That is your choice. Please let 45
46
DEALING WITH DEPRESSION
me know whether you are fully intending to kill yourself so I can fill your appointment next week. I see no reason to lose my fee because you want to kill yourself." Of course, he was working mostly with professionals who were interested in learning Gestalt therapy. I feel that his approach is a bit extreme. Even though, as a therapist, I would recognize this behavior as emotional blackmail, I would attempt to maintain some contact. Such a patient needs (and wants) human contact-in fact, the statement would not have been made if there had been no one to interact with. What do therapists do for people to get them to give up their introjection and start taking responsibility for themselves? There are a number of useful techniques. One is called "behavior rehearsal." This is a relatively simple technique that is more effective when tried in a small therapy group, but it can be done individually. (It is better in a group because there are more people to give feedback.) A lot of people are unable to act aggressively because they have never been allowed to do so, or because they were taught that to be aggressive is bad. Aggression is goal-directed. It has nothing to do with violence and killing. To be aggressive implies that individuals can say what their needs are and do what they need to do to meet those needs. In behavior rehearsal, patients rehearse new ways to be aggressive. Role playing is close to behavior rehearsal except it is more spontaneous. In behavior rehearsal, therapists actually show their patients how to play a role or have someone else demonstrate for them while they go through the process of trying out the role. In behavior rehearsal, patients are given a script to act. In role playing, patients are asked to play the aggressive part of their natures. Role playing can also be done individually or in a group. Another thing therapists constantly watch for is the introjectors' facility for the using the pronouns "we," "you," and "they" when they mean "I," and "it" when they mean "I." Listen to the persons' speech patterns and you will frequently hear "it" being used when they are talking about themselves. It is helpful sometimes in this endeavor to ask introjectors to make up some statements beginning with the word "I," after which they should clarify whether each statement is their own or is "borrowed" from someplace else. Introjectors get their identity from how the world identifies them: how their family, teachers, ministers, or doctors have told them to
Gestalt Therapy Dealing with Depression
47
behave. Any time introjectors make a statementthat they obviously got from someone else, good therapists will have them tum that statement around and make it applicable to the introjectors themselves. One example that is particularly illustrative of the way therapists can help introjectors identify with themselves rather than just with others is a case I had while still in training. The patient was an eight-year-old boy who was in an agitated state of depression and who had a discipline problem as well. My supervisor and I were thoroughly ready when the family came into the waiting room with the boy. There were a lot of people waiting, and I got down on one knee so that I would not appear too big for the boy. I said "hello" to him and his family. I attempted to establish some rapport by telling my new patient about the beautiful playroom we were going to see, a playroom with all kinds of toys. Getting up off my knee, I offered my hand and asked him to come with me. He answered me screaming curses that I had never heard from a child before. I was really taken aback. I realized that establishing rapport was essential. So, back on one knee I went, and we went through the whole routine again. The same thing happened, and I literally went through it a third time. At that point, I became painfully aware that everyone in the waiting room was quiet, eager to see what this expert was about to do. I could feel my supervisor's eyes boring into my back. In desperation, I reached out and grabbed the boy, put him on my hip, and disappeared down the hall to the playroom, saying firmly, "We are going." As I sat the boy down, I was really in a panic. I said, "Listen, we have three rules around here. One, you can do whatever you want as long as you don't hurt me. Two, you can't leave until the hour is over because I have the door locked (and I did). Three, if you cuss me anymore or try to hurt me, I am going to beat the hell out of you." I have since learned to be a therapist. I must admit that it got to the point that I really cared about that boy. In spite of my mistakes, he became okay, and even the parents improved. Oddly enough, I wasn't even a Gestalt therapist at the time. There are three powerful ingredients involved in introjection. These ingredients are the behaviors that maintain the introjectionthat is, they keep the introjection inside the individual. The first ingredient is patience. Gestalt therapists help their introjectors to
48
DEALING WITH DEPRESSION
become more aware of impatience. There are other choices for behavior than patience. Laziness is another power ingredient for maintaining the introjection. Patients should be encouraged to do anything that tends to activate them. Group methods involving some action are very helpful in combating laziness. Most of the time, this kind of laziness is evident in the absence of physical movement. Once introjectors sit down, they often do not move much. They have been taught too well not to wiggle, because wiggling is evidence of discomfort. Introjectors have been known to just sit there not moving even though they may be incredibly uncomfortable. They desperately need therapy centered on movement, some kind of action. Some kind of therapies utilize such things as movement and dance. Greed is the other powerful ingredient in maintaining the introjection. Patients need some kind of encouragement to share something-to share their thoughts, ideas, anything. Spoon-feeding, as I explained earlier, is detrimental rather than helpful. Even introjectors on the road to recovery may try to manipulate with all kinds of behaviors to get people to do something about their problems. Pleading, begging, and even playing "crazy" are all too common. Gestalt therapists frustrate this kind of manipulation by not doing what introjectors want. Actually, to get well, they need to do their own dirty work. So much of psychotherapy is tied up making patients realize they must initiate their own healing. BlliLIOGRAPHY Clarkson, Petruska and Jennifer Mackewn, Fritz Perls. London: Sage, 1993. Fagan, Joan and Irma Lee Shepherd (eds.). Gestalt Therapy Now. Palo Alto, CA: Science and Behavior Books, 1970. Hatcher, C. and P. Himelstein (eds.). The Handbook of Gestalt Therapy. New York: Jason Aronson, 1976. Kempler, W. Principles of Gestalt Family Therapy. Salt Lake City: Desert Press, 1974. Kohler, Wolfgang. The Task of Gestalt Psychiatry. Princeton: Princeton University Press, 1969. Latner, Joel. The Gestalt Therapy Book. New York: Bantam Books, 1974. Lederman, 1. Anger and the Rocking Chair: Gestalt Awareness with Children. New York: McGraw-Hill, 1969. May, Rollo. Love and Will. New York: Dell, 1989.
Gestalt Therapy Dealingwith Depression
49
Perls, Frederick S. Ego, Hunger and Aggression. London: Allan and Unwin, 1947. (New York: Random House, 1969.) Perls, Frederick S. Gestalt Therapy Verbatim. Lafayette, CA: Real People Press, 1969. Perls, Frederick S., Ralph F. Hefferline and Paul Goodman. Gestalt Therapy. New York: Julian Press, 1951. (Republished by Dell Books in 1965). Perls, Frederick S. In and Out of the Garbage Pail. New York: Bantam Books, Inc., 1972. Polster, Erving and Miriam. Polster. Gestalt Therapy Integrated. New York: Brunner-Mazel, 1973. Priest, Robert G. Anxiety and Depression: A Practical Guide to Recovery. New York: Arco Publications, 1983. Pursglove, P.D. (ed.). Recognitions in Gestalt Therapy. New York: Funk & Wagnalls, 1968. Schiffman, Muriel. Gestalt: Self Therapy. Menlo Park, CA: Self Therapy Press, 1971. Shephard, Martin. Fritz. Sagaponack, NY: Second Chance Press, 1980. Simkin, J.S. Gestalt Theory Mini-Lectures. Millbrae, CA: Celestial Art Publishing Co., 1976. Smith, E.W.L. (ed.) The Growing Edge of Gestalt Therapy. New York: Brunner/ Mazel, 1976. Stevens, John o. Awareness: Exploring, Experimenting, Exercising. Moab, UT: Real People Press, 1971. Walker, James L. Body and Soul: Gestalt Therapy and Religious Experience. Nashville: Abingdon Press, 1971. Zinker, J. Creative Process in Gestalt Therapy. New York: BrunnerlMazel, 1977.
This page intentionally left blank
Chapter 5
Behavior Therapy in Dealing with Depression H. Darby Trotter Richard Dayringer
BEHAVIOR THERAPY DEFINED Behavior therapy is a treatment form that is an application of certain learning theories, particularly the theories of Ivan Pavlov and B.F. Skinner. Behavior therapy emerged more or less from the laboratory, where the learning process and laws governing it are rigorously explored. Because of its laboratory orientation, more emphasis is placed on observable behavior than on non-quantifiable "intrapsychic processes." Behavior therapists view all behavior as learned, and feel that some learned behavior is maladaptive and not in the best interest of the individual. Individuals are believed to learn on the basis of certain principles; this learning accounts for most behavior changes and individual differences. To behavior therapists, much of what has been variously labeled "emotional disturbance," "mental illness," "neurosis," "psychosis," and so on is viewed as maladaptive learning behavior resulting from unfavorable learning experiences. If behavior is learned, then it can be unlearned; or alternative and competing behavior patterns can be learned that will reduce the frequency of maladaptive responding. The goal of therapy is the systematic unlearning (extinction) of behaviors that bring reduction of anxiety but provide no long-range solution. Behavior therapists emphasize that self-destructive patterns tend to continue because they are reinforced by immediate anxiety reduction. They generally do not accept the premise that repressed 51
52
DEALING WITH DEPRESSION
motives are responsible for symptom formation. Instead, their primary concern is for the alleviation of symptoms. As a group, behavior therapists tend to assume full responsibility for their patients' recovery. Vigorously denying popular charges that their therapy is mechanical and dehumanizing, these psychologists argue that it is the neurosis that simplifies and dehumanizes individuals, reducing their human capacity for spontaneity and creativity, and robbing them of dignity. A grief reaction or reactive depression is explained as the sudden loss of positive reinforcement, resulting from the death of a loved one-a situation that creates depression from reinforcement deprivation. The loss of the loved one is not stressed because nothing can be done to bring the person back. Instead, emphasis is placed on preventing further loss of reinforcement due to social withdrawal of the grieving person and initiating behavior that will replace lost positive reinforcement. Behavior therapists emphasize understanding the behavioral processes, such as analyzing consequences that follow the performance of certain tasks. Depression may begin if demands are especially difficult and the rewards fail to keep pace with the growing performance demands. An example of this would be the unrewarded extra effort required of an ambitious school child with a reading disability trying to keep pace with her peers. The behavior-and-consequence chain is the focal point of analysis of depression. Depressive behavior has its footing theoretically in Thorndike's Law of Effect, which states that there is a direct relationship between strength (frequency) of a behavior and the presence and amount of a positive reinforcer. Strength or frequency of a behavior (for example, depression) is directly related to lowered levels of positive reinforcement. Any change in the reinforcement has a direct effect on and produces predictable changes in the behavior coupled with the reinforcement. A high behavior-to-reinforcer ratio refers to any condition in which behavioral expectancies or demands for productivity increase while reinforcement is held constant, or when behavioral expectancies or productivity are held constant but the amount of reinforcement is reduced. One simple illustration is the relationship of work on a job to amount of pay. If the employer wants more work without
Behavior Therapy in Dealingwith Depression
53
increasing payor demands the same amount of work but cuts the salary, the worker will become dissatisfied. Four factors that apply to the behavior-to-reinforcement ratio are: (1) frequency of rewards; (2) amount of rewards; (3) duration or continuation of reward once started; and (4) amount of effort required to produce expected behavior. If rewards are infrequent, too conservative, and/or prone to stop after initial reinforcement while behavior demands continue, and if simultaneously the effort to perform certain tasks increases, the behavior-to-reinforcement ratio increases, leading to increased probability of depressed behavior. The "depressed wife of the busy young professional syndrome" is an example of a high behavior-to-reinforcement ratio resulting from insufficient frequency of positive reinforcement. The wife, forced to remain at home much of the time because of the demands of young children, becomes expectant of reinforcement from her husband. Unfortunately, the young professional is simultaneously dedicating much of his time and effort to developing his career. The wife at home is isolated from the frequent reinforcement available to her more public spouse. Frequency of positive reinforcement becomes insufficient to maintain her domestic behavior, which increasingly requires greater effort with the growth of the family. If the frequency of positive reinforcement decreases and become insufficient while the cost of domestic behavior increases, a high behavior-to-reinforcement ratio is the result. This is a major factor in many depressions. (You may have heard it explained in the general terms that the "patient is not getting enough strokes.") The syndrome of depression resulting from not being treated as special is illustrative of depressions related to an insufficient amount of positive reinforcement. People who regard themselves as somehow special or in some ways better than other people expect tributes befitting their stations. Unfortunately, the degree of specialness usually is only a personal opinion, to which other people respond either inadequately or not at all. For example, a patient who says, "I don't think I can ever measure up to what others want of me" is often indicating that he feels that there is an insufficient amount of positive reinforcement to maintain his behavior. Consider, for a minute, the young girl who had made considerable effort to improve her grades and thereby her grade average. When she proudly presents
54
DEALING WITH DEPRESSION
her grade cards, her parents respond, "We told you that you could do better. Now let's see if you can raise them even more and get on the honor roll." The effects of insufficient duration of positive reinforcement can be seen in syndromes where the failure to make a genuine commitment is a factor in the patient's history. Because such individuals hesitate to make long-range commitments, they may move fromjob to job, relationship to relationship, task to task-never remaining long enough to collect the long-term positive reinforcement that follows many of these commitments. These people will find it increasingly difficult to maintain behavior without depression because of their reliance upon more immediate, short-term reinforcement. Another example of the negative effects of short-duration reinforcement is the individual who complains of having been "conned" and "used" in a relationship in which all romance has ceased once sexual relations are established. As the reinforcement from the romance is terminated but the desire for sexual behavior continues, the passive partner begins to feel depressed and very much the victim of a persuasive individual little interested in anything outside the sexual encounter. Another condition which, like the high behavior-to-reinforcement ratio, tends to produce depression is the withdrawal of a positive reinforcer. Moss and Boren (1972) point out that there are "two interrelated parameters which govern the withdrawal of a positive reinforcement: time (permanent, prolonged, or brief withdrawal); and contingency (whether or not the withdrawal is contingent on behavior)." The issue of whether the withdrawal is contingent upon behavior is important. If it is contingent upon behavior, then withdrawal is a form of punishment and must be considered under the category of aversive control, a topic that will be addressed later. Considering the time involved in withdrawal of positive reinforcement, permanent withdrawal leads to the extinction of behaviors under control of that reinforcer. The most positive reinforcement is a grief reaction resulting from the death of a loved one. Other examples might include the loss of sight, permanent marital separation, and some aspects of aging. The loss of the person or skill that made positive reinforcement possible often leads to depression. Prolonged withdrawal of positive reinforcement occurs when indi-
Behavior Therapy in Dealingwith Depression
55
viduals are separated by illness, marital problems, military service, business trips, children leaving home for the first time, loss of a valued job, and moving away from friends. This type of withdrawal plays particular havoc with dependent personalities who suffer severe loss in self-esteem, security, and trust when the dependency needs are not being met to suit them. Often the prolonged withdrawal is short, but because of the extreme sensitivity of the dependent personality, the individual may overestimate the period of withdrawal. To make matters worse, individuals with these problems often abandon otherwise sound relationships because of their perception of prolonged withdrawal. Brief withdrawal of positive reinforcement is usually observed in punishment situations where the withdrawal is contingent on some specific behavior-such as a parent withholding affection from a child because that child has misbehaved. On a more subtle level, there may be times when one spouse refuses the other sexually, or may pout and withdraw attention for the purpose of punishment. In addition to a high behavior-to-reinforcement ratio and the withdrawal of a positive reinforcer, a major interruption of a chain ofbehaviors leading to positive reinforcement can cause depression. An example of this would be the sudden onset of depression in an athlete forced to abandon a career due to an injury. This particular athlete had long hoped to achieve professional status, practicing with this goal in mind and winning a series of awards reflecting athletic success. Eventually, the athlete had been able to participate successfully in professional sports and had begun to experience some of the positive reinforcement. Despondency set in when the chain leading to reinforcement was interrupted. Another consideration is the depressing effect of behavioral control through aversive means. Punishment is the application of negative or aversive consequences to control behavior. Depression can occur from overreliance on aversive control because the aversive event involves reduction or elimination of positive reinforcement and suppression of behavior that might otherwise lead to positive reinforcement. A child sent to his room by an angry parent not only suffers the withdrawal of the parent's affection but is isolated from other people, such as peers or siblings, who might provide positive reinforcement. Suppressed behavior resulting from aversive control
56
DEALING WITH DEPRESSION
may return with equal or greater strength because of the difficulty in maintaining a continuing threat when the individual spends time separated from the aversive agent. Related to punishment, another form of aversive control is avoidance. This means that an individual behaves in such a manner as to avoid undesirable aversive consequences. For example, a child may clean her room, not out of a desire for orderliness, cooperation, or cleanliness, but because she wants to prevent unpleasant aversive consequences. This little girl is learning early the avoidance behavior that probably will be with her throughout her life. Later in life, this behavior may take the form of avoiding contact with her parents because she does not feel she has lived up to their expectations and will only suffer criticism from them. Avoidance can take the form of withdrawal, fears, and rigid behavior. In the absence of positive reinforcement, depression may occur. Individuals who tend to carry grudges and project blame onto others and who are sensitive to criticism and anticipate others' actions often are involved in avoidance behavior. Escape behavior is another behavioral reaction to aversive stimuli. It involves both the experience of aversive conditions and an active attempt to terminate these conditions by escaping the situation. An aversive condition can be either an aversive stimulus or a noticeable reduction in positive reinforcement. Escape behavior can be depressing when positive reinforcement is not achieved. An illustration of this kind of depression is the case in which a young female requested therapy for periodic depression. A review of the case indicated an aversive home environment, which she escaped by getting married at an early age to her first suitor. As problems emerged in her relationship with her husband, she began an affair. Eventually she fled the marriage and moved in with the man with whom she was having the affair. As problems emerged in that relationship, she terminated it again and sought to escape any subsequent relationship with a man as soon as a problem would appear. Soon the woman became involved only with men who were married and held out no promise of a future relationship. When these relationships became aversive, she escaped by refusing to date altogether. Each escape was unsuccessful in terminating negative consequences, and positive reinforcement was either absent or of short
Behavior Therapy in Dealingwith Depression
57
duration. Thus, with each escape from conflict she became depressed. In treating her, the focus was on developing her ability to tolerate and manage conflict without resorting to escape. "Learned helplessness" (Seligman, 1975,1980) is a concept that seems to provide some answers to the characterological forms of depression evident when patients have experienced chronic defeat and cannot isolate specific events that make them feel depressed. If an individual has experienced a number of painful events over which she could exert no influence-for instance, the death of a loved one, illness, or financial disaster-she may learn to perceive herself as helpless, ineffectual, and impotent. This latter perception is a self-concept that manifests itself behaviorally in the cluster of symptoms associated with depression: self-neglect, tearfulness, intellectual and psychomotor retardation, a sense of impending doom, and negative propaganda ("I'm a failure"; "What's the use? I can't win. "). At this point, a definition of characterological depression seems in order. A characterological depression is one in which patients' painful symptoms are well-ingrained maladaptive patterns of behavior of long standing. In fact, such patients may use many of the symptoms to describe themselves as lazy, slow, or unenthusiastic. They no longer discriminate between symptoms or depressed feelings and themselves. Characterologically depressed patients not only find it difficult to maintain motivation for therapy but, more frequently than not, consider the challenge of a major personality or attitudinal change quite intimidating. Frequently, these patients comment, "That's just the way I am" or "That's me and I don't know how to react otherwise." Depressive behaviors have been typical or characteristic of these people for a long time. What are the possibilities for the extinction of learned helplessness in characterologically depressed patients? Interpretive or insight-oriented therapy, which is explained below, seems inadequate for characterologically depressed patients, since these patients may fully comprehend the genesis of their despair-that is, conditioned helplessness as the result of repeated and unavoidable disappointment and loss-but remain unable to summon any motor response that might restore their sense of mastery and potency as individuals.
58
DEALING WITH DEPRESSION
Behavior therapy attacks such inhibition directly by: (1) determining whether anxiety is involved and, if so, deconditioning that anxiety (by systematic desensitization, assertiveness training, or whatever other method seems appropriate); and (2) structuring behavior in such a way as to ensure small successes, positive reinforcement of effort, and gradual restoration of a belief in an individual's own potency. The schedule of tasks may begin with activities as seemingly mundane as making a telephone call, returning defective merchandise to a department store, or accepting a compliment, but as each task is successfully completed and adequately rewarded by the therapist, these patients experience less inhibition and an increasing sense of mastery over their environments. Behavior therapists generally are more directive and authoritarian than insight therapists in their approach to therapy. Insight-oriented therapists adhere to the questionable assumption that understanding or insight produces change or cure in their patients. They do have their successes and find support for their therapeutic stance. For instance, treatment outcome is generally favorable through insight therapy for short-duration reactive depressions and grief reactions in cases where catharsis of suppressed feelings relieve the depression. Insight therapy is also effective in cases when the therapists guide patients toward environmental restructuring of positive reinforcement and monitoring of psychologically acceptable levels of stress. This therapy, however, is only advantageous when patients actually act on this advice. Insight therapists find their system wanting when dealing with the characterological depressions, in which insight or understand having little effect on life-long habits. The search among other insight approaches to offer better results is basically begging the question. As concern about treatment success erodes traditional barriers between insight and behavior therapy, many psychotherapists are beginning to search the area of behavior modification for solutions to these treatment problems. There are situations in which insight-oriented therapy can be used in combination with behavior therapy. Proponents of the latter utilize insight and understanding to learn just which habits or symptoms concern patients enough that they want to change them. Psychotherapists now have reached a stage in which they are more willing to select from a variety of systems, methods, and techniques
Behavior Therapy in Dealing with Depression
59
that will be most helpful to their patients, instead of forcing them to fit into the narrow confinement of one systematic viewpoint.
TREATMENT OF DEPRESSION WITH BEHAVIOR MODIFICATION A variety of treatment methods have evolved which are designed to respond to the specific conditions that have produced the depression. The fact that various treatment modalities have emerged emphasizes the behaviorists' appreciation for the variety of conditions that can produce depression and the futility of seeking one form of treatment for all conditions. As stated earlier, behavior therapists play an active role in treatment and usually design a specific treatment program which they recommend to their patients. In SOUle cases, several treatment modalities are used in the course of therapy because of multiple etiological factors. Various treatment methods are described below, including some discussion as to when such methods are appropriate.
Confrontmional Therapy An example of confrontational therapy is seen in the case of a housewife who requested therapy for depression and a feeling that no one appreciated her. It was clear she had very strong perfectionistic obsessive traits and continually placed demands on herself that exceeded those expected by her husband. By her own personal pressure to perform, she increased the behavior-to-reinforcement ratio. If people she encountered reinforced this woman merely at the level of her behavioral output, she felt no one appreciated her and was depressed by the subsequent absence of adequate positive reinforcement. I pointed out this behavior to the woman and we began to work on the reasons she held such expectations for herself. Much of her behavior was learned avoidance behavior from childhood, where she escaped the criticism of her parents by being an ideal child. Her perfectionism was then related to fear of criticism, but the setting no longer required this behavior because her husband was not aversive. I encouraged the patient to "check out" if criticism
60
DEALING WITH DEPRESSION
was forthcoming by gradually easing up on unnecessary behavior. As she did, natural reinforcement occurred and with constant confrontation and reinforcement from me her behavior generally eased to levels that would be reinforced by her environment. She learned to monitor obsessive behavior because it led to depression. Given that a good relationship exists between therapist and patient, the therapist's own approval becomes reinforcing as an agent in the change, particularly during the early part of treatment. There is considerable research indicating that the therapist's reinforcement influences patient behavior. For example, patients whose therapists nodded acceptingly to verbalizations tended to verbalize more. These therapists, aware of the target behavior they are working on, can encourage or extinguish behaviors depending on their responses to their patients. If they are consistent in the use of this procedure, they can produce better results. This fact illustrates one of the main features of behavior therapy-an appreciation of the need for systematic responding.
Habit Extinction Through Frequency-of-Responding Procedure
The goal of frequency-of-responding procedure is to reduce or extinguish a patient's tendency to respond in ways that ultimately result in depression. For example, individuals who procrastinate a great deal usually end up feeling depressed because this form of avoidance behavior really does not resolve the problem or take the task away. Ultimately, it makes completing the task more difficult, postpones or prevents acquisition of positive reinforcement available upon completion of the task, and eventually increases the behavior-to-reinforcement ratio. The goal of therapy, in this example, is to eliminate the tendency for the patient to procrastinate so that response costs will be less and reinforcement will be higher. The frequency-counting procedure has been very effective in interrupting longstanding behavioral patterns. Generally, significant results can be obtained during the first few weeks of treatment. The treatment method is simple and straightforward. Instructions are as follows:
Behavior Therapy in Dealingwith Depression
61
1. Therapists should develop a concrete target behavior for individual patients (procrastination, self-derogatory remarks, failure to express oneself, worry, etc. 2. Ask patients to purchase a counting device (golf counter, grocery counter, or frequency counting device from professional supply stores) and graph paper. 3. Instruct patients to count every time they engage in the target behavior and immediately record it on the frequency counter. Persuade patients not to try to keep track of the frequency in their head or with scratch paper and pencil. This rarely works. 4. On the first day, patients are requested only to count the frequency with which they engage in the target behavior. They do not need to graph this initial day, but should use the results of the first day in developing the appropriate scale for the graph. 5. In developing the graph, place the frequency on the vertical scale and the days on the horizontal scale. It is important that the vertical scale is not too large for the frequency because gains are hidden in a highly compacted graph. In order to gather reinforcement, patients must see their gains. 6. Patients should be requested to record the frequency captured by the recording device on the graph just before retiring and, of course, start with a new count in the morning. (Patients who graph each night do much better than those who simply record the number.) 7. Patients should be requested to bring their graphs to therapy sessions so that therapists can reinforce their progress and be sure that they are proceeding according to instruction. (An example of this procedure is provided in Figure 5.1. This is a case where obsessive behavior was contributing to the social isolation of the patient and subsequent loss and devaluation of any positive reinforcement available.)
The pattern of extinction of behavior through frequency counting methods follows the typical pattern of deconditioning of any behavior-that is, spontaneous recovery (return) of the symptoms is likely to occur for short periods during the treatment program. Thus, the graph will be jagged but progressing in a downward direction.
62
DEALING WITH DEPRESSION FIGURE 5.1
Frequency 20 19 18 17 16 15 14 13 12 11 10 9
8 7 6 5
4 3
2 1 1 2 3 4 5 6 7 8 9 101112131415161718192021222324252627282930
Days of the Month
Behavior therapists view depression as a behavior in and of itself and not always as a mood state. Of course, the general perception of the public and most professionals is that depression is a feeling or state that is always contingent upon antecedent disappointment or loss and is not a stimulus or a behavior itself. Behavior therapists often treat the depressed reaction itself as a bad habit and use the frequency graphing method to treat this form of depression. There are many instances where individuals cannot isolate specific reactions because they are depressed all the time. Even these individuals, however, can identify the number of times they engage in negative mental sets and make self-deprecating comments to themselves or in the company of others. Identifying and recording such behavior motivates patients to fight assumptions about themselves that they previously regarded as facts.
Behavior Therapy in Dealingwith Depression
63
TimeProjection Method The goal of this treatment form is to help patients develop an image of themselves functioning in the future so that they can be more aware of recovery from aversive conditions and the availability of positive reinforcement in the future, and experience the fact that life goes on even after the most tragic circumstances. This treatment method relies on patients' abilities to develop images of themselves behaving in ways that compete with behaviors encouraging depression. Time alone does not always cure, as is so often stated. The passage of time, however, does allow for the development of behavior that competes with and opposes behavior that leads to depression-for example, activity rather than passivity, socialization rather than withdrawal, and acceptance rather than bitterness. Being able to develop an image of functioning in the future allows for the emergence of competing behaviors usually not considered when people are deeply depressed. This treatment method seems particularly suited for the treatment of depression resulting from permanent or prolonged loss of positive reinforcement such as grief reactions. Often behavior therapists employing the time projection method gain insight into what their patients are doing to cause depression, especially when the positive image developed is contrasted with present behavior. To manipulate the time variable and develop images of the future, both hypnosis and self-induced imagery are used. During the period devoted to projection into the future, patients are encouraged to visualize themselves functioning some months in the future when they are engaged in constructive behavior such as work or talking with friends. Under these conditions, patients can contemplate future positive reinforcement. For example, one of my patients was depressed about the loss of his spouse. I asked him to develop an image of what he could be doing some four months in the future. I helped him develop an image by pointing out, "You are now the head of the family. How do you see yourself filling that important and valued function?" I asked another patient to visualize a new business venture after he had become depressed over the loss of a previous business. It is important to note that once imagery has been used and positive behaviors isolated, patients must be helped to
64
DEALING WITH DEPRESSION
actually experience some of the rewarding experiences and behaviors which they have visualized.
Rubber Band-Snapping Method The application of self-administered rubber band snapping is often effective in extinguishing depressive symptoms. In this method, patients wear an elastic band on their wrist at all times. Each time they engage in depressive behavior-such as self-immobilization in anticipation of failure-they are instructed to pull back the rubber band and snap it against the wrist continually until they substitute a constructive alternative behavior. Again, patients are requested to keep a frequency count of depressive symptoms and graph the progress of their extinction. This method has obvious applications in the treatment of low self-esteem, self-neglect, psychosomatic complaints, psychomotor retardation and other behavioral correlates of clinical depression.
"Stop-Thought" Method In grief reactions and situational depression, persistent trains of thought which are illogical, unproductive, and anxiety-arousing are a common clinical problem. Consider, for example, the recently divorced woman who, upon the initiation of a new heterosexual relationship, broods continuously upon the possibility of interpersonal failure and rejection. Eventually, her anxiety becomes so intolerable that she either terminates the relationship or provokes, through a variety of alienating behaviors, the very rejection she fears. A stop-thought regimen is instituted by asking the woman to sit down, close her eyes, and verbalize a typical self-defeating thought sequence. In this case, it might be "I've failed in my marriage; I can neither love, nor be loved; I'm socially inept; as this man comes to know me better, he'll see how bad I am and will reject me ..." At some point during the verbalization, the therapist shouts, "STOP," immediately pointing out to the patient how this verbal command did indeed interrupt the destructive rumination. After repeating the procedure several times, the patient is instructed to initiate the interruption herself by saying, "STOP," either vocally or subvocally, at
Behavior Therapy in DealingwithDepression
65
each time the disturbing thought emerges. The usefulness of the technique is increased by helping her design a hierarchy of alternative pleasant thoughts to which she may immediately attend after aborting a negative thought-sequence. The stop-thought technique is a particularly effective method of inhibiting futile thought sequences in the more intelligent, verbal, and motivated depressed patient. The mechanism underlying the success of the procedure seems to be the reinforcing effect of lessening the anxiety that the patient experiences with each successful attempt at thought inhibition.
EmotionalProvocation and Expression This particular method consists of assigning to affectless and inert depressed patients monotonous or unpleasant tasks that will provoke anger. After patients begin performing tasks, all attempts are made to prevent them from returning to the previous inert depressed state. This is accomplished by providing recognition, support, and opportunities for personally satisfying activities. Depressed patients most probably will benefit from therapists' requests to discuss and express emotion in therapy, particularly if the emotion is anger. Sometimes anger at therapists can be encouraged; certainly, expression of anger toward other individuals should be encouraged, though acting out of the affect should be controlled. If attacked verbally by a depressed patient, the therapist should learn how to encourage assertive behavior rather than respond defensively and suppress the patient's anger when it is expressed. This form of therapy is contingent on eliciting the patient's feelings. Many patients are habitually inhibited and rarely express their feelings. This is an occasion when the frequency or counting method designed to break habits can be used to help patients become more expressive. Most depressed people can experience a variety of feelings, but so thoroughly censor these feelings that they are never expressed. The frequency method breaks up the undue censoring, allowing expression. Expression, in tum, breaks up the depression. For example, one patient complaining of depression and anxiety found herself unable to express her resentment at being "used" by her husband. She felt that expression of this resentment would only anger him and provoke him to reject her further. As a result, she did
66
DEALING WITH DEPRESSION
not complain about his treatment and became increasingly depressed. As a result of interviews, it became clear that throughout her life this woman had been loath to express her feelings because she anticipated aversive control. Under therapy she began to count the frequency of her period of acquiescence and participated in some assertive training. As she became expressive of her feelings, her husband was more than cooperative and resolved a number of "misunderstandings," her friends reacted to her enthusiasm in a positive way, and she began to experience relieffrom a life of inhibition and depression.
Sensory Deprivation Method This procedure is largely dependent on a highly controlled environment and is designed to break up depressed patients' resistance to responding to various forms of available stimulation. Basically, patients are given bedrest for a five-to-seven-day period in an environment devoid of external stimuli. No forms of entertainment are provided; visitors are prohibited, diet is bland, and all distractions intenupted. At the end of this period, patients' appreciation of stimuli has changed and they usually indicate positive reinforcement in almost any form of external stimuli.
Treatment Based on Premack's DifferentialProbability Hypothesis Premack (1959) developed and tested the hypothesis that for any pair of responses or behaviors, the one most likely to occur will influence and reinforce a paired response that is of less strength initially. Roughly speaking, the weaker response "piggybacks" the stronger and thus is more likely to be an available response. I have used Premack's principle effectively with a patient who was requested to state firmly to himself, "I'm adequate" just before making each telephone call. The patient's depression was reduced significantly with bolstered self-esteem.
Token Economy Treatment Method In patients where the primary affect is depression and where few cheerful or varied affective responses are manifested, a token econ-
Behavior Therapy in Dealingwith Depression
67
omy system has proven an effective treatment mode (Hersen and Eisler, 1973). The procedure is quite simple; patients under this treatment must pay for even the simplest privileges with tokens earned by performing behaviors that compete with depression-for example, showing anger, exhibiting cheerfulness, initiating conversation, etc. Tokens are forfeited by severe withdrawal. Briefly, the only way patients can have any pleasurable experiences is to earn tokens by not being depressed. When patients experience enough deprivation as the consequences of their own actions and see that they cannot beat the system, they usually will get better. It is interesting to note that when most people get depressed, they are given support, reassurance, comfort, pills, and lowered expectations. These measures reinforce depression. In contrast, the token economy method turns the table on the patient.
Desensitization Procedures Desensitization procedures have been effective in the treatment of certain forms of depression, such as agitated depression, grief reactions, depression with significant somatic preoccupation, and certain states or periods of depression precipitated by high anxiety and the threat of psychological injury. These procedures involve teaching autohypnosis or self-relaxation. While patients are relaxed, therapists using these procedures present materials that previously provoked depressive reactions. However, now the emotionally upsetting response is paired with a competing response of deep relaxation. Gradually, patients learn to react to conflict or stress with calm control rather than depression. Painful memories, as in grief reactions, are paired with pleasant relaxing. Tapes of a relaxation session can be made and sent home until patients learn how to relax in the face of stress and to use relaxation to relieve psychosomatic symptoms. Patients are encouraged to learn to relax and to engage in imagery of positive memories to break up the depression response. This procedure gives them considerable encouragement; they now rely on themselves to relax and no longer need protective, limiting, environmental structure.
68
DEALING WITH DEPRESSION
Environmental The broad category of environmental manipulation includes a variety of treatment forms that involve diagnosis of the reinforcement available, the reaction of the individuals involved in the level of available reinforcement, and specific designs to change the environment to better support those involved psychologically. All of these methods may be used to reduce depression, but will not be elaborated on in detail here. Treatment forms include job enrichment and human engineering approaches, educational programs (such as parental guidance and premarital counseling), and vocational guidance.
CONCLUSION In a number of these approaches, the concern is less with an individual state of mind and more with improving the psychological well-being of a large group. Behavior therapists-with their appreciation for such variables as reinforcement, response cost, behaviorto-reinforcement ratios, learned patterns of responding, concrete observable systems, and manipulation of reinforcers and/or development of responsiveness to reinforcers--can and do offer consultation on the level of social planning and also collaborate with other therapists in developing individual treatment programs. BIBLIOGRAPHY Bass, A.A. "An Unusual Behavioral Technique for Treating Obsessive Ruminations." Psychotherapy: Theory, Research and Practice, 1973 (10):191, 192. Davidson, Park o. (ed.). The Behavioral Management ofAnxiety, Depression and Pain. New York: BrunnerlMazel, 1975. Gallant, Donald M. and George M. Simpson. (eds.). Depression: Behavioral, Biochemical, Diagnostic and Treatment Concepts. New York: Spectrum, 1976. Hersen, M. and R.M. Eisler. "Effects of Token Economy on Neurotic Depression: An Experimental Analysis." Behavior Therapy, 1973 (4):392-397. Karasu, T. Byram. Psychotherapy for Depression. Northvale, New Jersey: Aronson Publishers, 1990. Kora, T. "Morita Therapy." International Journal ofPsychiatry, 1965 (1):611-640. Lazarus, A.A. "Learning Theory and the Treatment of Depression." Behavior Research and Therapy, 1968 (6):83-89.
Behavior Therapy in Dealingwith Depression
69
Lowry, Michael R. Major Depression: Prevention and Treatment. St. Louis, MO: W.H. Green, 1983. Morrison, Helen L. (ed.). Children ofDepressed Parents: Risk, Identification and Intervention. New York: Grune and Stratton, 1983. Moss, G.R. and J.H. Boren. "Depression as a Model for Behavioral Analysis." Comprehensive Psychiatry, 1972 (13):581-590. Nezu, Arthur M., Christine Nezu, and Michael G. Perri. Problem-Solving Therapy for Depression. Somerset, New Jersey: Wiley and Sons, 1989. Premack, D. "Toward Empirical Behavior Laws: 1. Positive Reinforcement." Psychological Review, 1959 (66):219-223. Rehm, Lynn P. (ed.). Behavior Therapy for Depression. New York: Academic Press, 1981. Rush, John. Beating Depression. New York: Facts on File. 1983. Seitz, F.C. Behavior Modification on Depression (29th Annual Convention Proceedings). American Psychological Association, 1971. Seligman, Martin P. Helplessness: On Depression, Development and Death. San Francisco: W.H. Freeman, 1975. Seligman, Martin P. Human Helplessness. New York: Academic Press, 1980. Wolpe, Joseph. The Practice of Behavior Therapy. New York: Pergamon Press, 1973.
This page intentionally left blank
Chapter 6
Cognitive Therapy Dealing with Depression Richard Dayringer
Cognitive therapy was defined by Aaron Beck (Beck et al., 1979, p. 3) as an active, directive, time-limited, structured approach used to treat a variety of psychiatric disorders .... It is based on an underlying theoretical rationale that an individual's affect and behavior are largely determined by the way in which he structures the world. Cognitions are inner thoughts or internal dialogue based on one's attitudes or assumptions that have been developed from previous experiences. Albert Ellis called his brand of cognitive therapy "Rational-Emotive Therapy" or "RET" (Ellis and Grieger, 1977). He postulates that people do not directly react emotionally or behaviorally to the events they encounter. Rather, people cause their own reactions by the way they interpret or evaluate the events they experience.
HISTORICAL DEVELOPMENT Ellis and Beck both began developing their theories during the 1950s. They both traced the philosophical origins of their theory to the Stoic philosophers of the fourth century B.e.E. Each credited 71
72
DEALING WITH DEPRESSION
Epictetus with the statement: "Men are disturbed not by things, but by the views which they take of them" (Beck et al., 1979; Ellis and Grieger, 1977). A history of the development of this theory has been traced by Ellis (1962). The personal style of Ellis was rather loud and abrasive (Hauck, 1972), and he claimed that RET was useful for almost every known disorder. On the other hand, Beck and his colleagues, working at the University of Pennsylvania, focused on the disorders of mood, were more tactful in presenting their views, and have apparently earned a greater respectability for cognitive therapy. Beck and Ellis may differ in terminology and tone, but they differ very little in substance. Both Ellis and Beck maintain that they have always used behavioral techniques in their therapy. Since around 1970, a number of behavior therapists have also begun to accept some of the cognitive tenets, thus producing what is now called "cognitive-behavioral therapy" (Kendall and Hollon, 1979).
RATIONAL-EMOTIVE THERAPY Ellis (1962) posited what he named the ABC theory of emotional and behavioral reactions. In this he asserted that we do not react directly to the events we experience; rather, we cause our own responses by the way we think about these events. Thus, we control our own emotional destinies by the way we interpret and choose to respond to the events that occur in our lives. For example, if my son yells at me for not letting him borrow the car, and tells me I am a bad father, he does not make me mad or depressed. I may not have direct control over what he says, but I do have total control over my response. I could react in many ways, and the one I choose depends on how I interpret his behavior and how I choose to respond to my perception. The ABC theory states that at point A (an ACTIVATING experience or event), something occurs: my son yells at me and tells me I am a bad father. At point C (an emotional and/or behavioral CONSEQUENCE), I react to the events of point A, and I feel angry and depressed. Since the consequence (C) immediately and directly follows after the occurrence of the activating experience (A), we frequently, though falsely, assume that A caused C. According to RET,
Cognitive Therapy Dealingwith Depression
73
this conclusion is not logical. If I had allowed my son to use the car and he had an accident, I would not become sad at the moment of the accident, but rather, after I received the news. We become upset only by all the internal cognitions of BELIEFS (B) we have about A. Within seconds of hearing of a problem (A), many internal thoughts and much inner speech occurs. In the case of my son, I might say to myself: "I shouldn't have let him drive the car!" RET maintains that it is not A (son's behavior) that leads to C (anger or depression). Instead, it is all the irrational beliefs (B) about A which leads to my choice of reactions. In our example, had I thought (B): "I was trying to be a considerate father in letting him use the car, and I know he is a good driver. It surely wasn't his fault," then my reactions would be altogether different. Therefore, reactions (C) are never caused by circumstances (A), but by beliefs or internal thoughts (B) about the event (A). Ellis refers to the inner thoughts or internal dialogue as being either Irrational Beliefs or Rational Beliefs. Rational beliefs are based on reason and an accurate assessment of data. Irrational beliefs are distortions and exaggerations which are often filled with such words as should, must, and ought. He called such thinking "MUSTurbation." Another major reason for our negative emotions, he called "awfullizing." He pointed out that most of the unpleasant things that happen to us, which we label as "awful," are actually very common in occurrence. In recent years, RET has lost some of its idenity as a major force in theory and has come to be considered as one form of cognitive therapy.
PREMISES OF COGNITIVE THEORY Humans have a great interest in processing information from their environment. Consequently, we actively search for meaning in our reality by selecting, transforming, encoding, storing, and retrieving information about ourselves and the world around us. This information-processing activity in tum affects our emotional and behavioral responses. In Beck's cognitive theory, the essential features of depression are the negative triad: a negative view of the self, the world, and the future. In other words, depressed persons distort perceptions of self,
74
DEALING WITH DEPRESSION
world, and future in a negative direction. They are prone to conclude incorrectly or prematurely that they are failures or bad persons, or deserve some other pejorative label (bias against the self); that their life situation is intolerably harsh, joyless, unfair, and painful (bias toward the personal world); and that these conditions will never find remediation (bias toward the future). Beck argues that experience is filtered through cognitive schemata. "A schema is a relatively enduring unit of belief from which momentto-moment cognitions are derived. These schemas are the rules that govern how an individual assigns meanings" (Schuyler, 1991). Depressed people engage negative schemata that produce negative distortions of experience. Beck describes specific forms of distortion such as selective abstraction and arbitrary inference. In selective abstraction, people selectively focus on minor negative aspects of situations while excluding some more positive information, In arbitrary inference, people arbitrarily assume that they are to blame for negative events in their lives. Schemata operate without conscious effort and produce what cognitive theorists call "automatic thoughts" (Beck, 1963). Frequent negative automatic thoughts produce depressive affect. Depressive schemata are acquired in childhood, according to Beck and his associates, through the influence of role models, direct feedback, cultural factors, and experience. They may develop because of early experiences of loss. The result is a broad range of negative generalizations about the self. Or, they remain in existence but are latent and come into use when other losses are encountered. Beck et ale (1979) contend that the maintenance of depressive schemas is the consequence of a faulty system of information processing in which the individual draws illogical conclusions from six basic cognitive errors:
1. Arbitrary inference: drawing a specific conclusion in the absence of evidence to support it; 2. Selective abstraction: drawing a conclusion based on a detail taken out of context; 3. Overgeneralization: drawing a broad, global conclusion on the basis of one or more isolated pieces of information;
Cognitive Therapy Dealingwith Depression
75
4. Magnification and minimization: exaggerating the significance of negative events and minimizing the significance of positive events; 5. Personalization: relating external events to oneself when there is no realistic basis for making such a conclusion; 6. Absolutistic, dichotomous thinking: placing all experiences in one of two opposite categories. Cognitive theorists have producedmuch research (Kendalland Watson, 1989)that supports their premises. "Beck's formulation of cognitive theory and therapy resulted from his clinical and experimental fmdings that depressed individuals were prone to idiosyncratic cognitive distortions centering around themes of loss and deprivation" (Wolman and Stricker, 1990, p. 345). They found that when in a sad mood, it is easier for individuals to recall sad events from last week or from childhood. When asked to recall a happy childhood event, it will take longer when in a current sad mood. All their findings are consistent with the notion that emotion is a factor in the storage and retrieval of information, Kendall and Watson(1989, p. 387) report a number of research studies concluding that when comparedto nondepressed controls, depressed patients: (1) underestimate the success of their performance; (2) notice significantly more negative and fewer positiveinterpersonal behaviors when viewing a videotape of their role-play interactions; (3) overestimate the negative and/or underestimate the positive feedback received following performance of a task; and (4) exhibit a negative bias when presented pleasant, unpleasant, and neutral words. Psychiatrist David Bums' book, Feeling Good: The New Mood Therapy, is probably the best single resource on cognitive therapy for both counselor and counselee. He gives three principles of cognitive therapy (1992, p. 12, 13). First, all moods are created by thoughts. People feel the way they do because of their thoughts at that moment. Second, feeling depressed means that thoughts are dominated by pervasive negativity. Such persons come to believe that their lives are really as bad as they imagine them to be. Third, negative thoughts that cause emotional turmoil nearly always contain gross distortions. As people learn to think more objectively, they will begin to feel better.
76
DEALING WITH DEPRESSION
Bums concludes: "Our research reveals the unexpected: Depression is not an emotional disorder at all! ... Every bad feeling you have is the result of your distorted negative thinking" (1992, p. 28). Sadness, he maintains, comes without thought distortion. It involves a flow of feeling and has a time limit. But it never results in a lessening of self-esteem. Depression is frozen and tends to persist or recur indefinitely, and always involves loss of self-esteem (1992, p. 232).
CHARACTERISTICS OF COGNITIVE THERAPY Cognitive therapy is an active, structured, psychoeducational, collaborative dialogue, as opposed to a passive client monologue. Counse1ees are taught the cognitive theory that has been described previously. These activities proceed best when the cognitive therapist exemplifies the basic therapeutic characteristics of warmth, genuineness, and openness, and is adept at empathically listening to and understanding the client's uniqueness. Although cognitive therapists need to be critical thinkers, they do not merely engage clients in arid intellectual debate, nor do they harangue clients into agreeing with the therapists' points of view. Cognitive therapists strive to build a trusting, mutually respectful relationship with their clients as the foundation for the use of cognitive techniques. Prior to beginning treatment, cognitive therapists typically give counse1ees a rather comprehensive diagnostic evaluation. This is to rule out an underlying organic disorder that may be causing the client's dysphoria, such as hypothyroidism, hypoglycemia, diabetes, epilepsy, or postconcussive syndrome. Or, the depressed affect may actually be secondary to an even more primary psychological disorder, such as obsessive-compulsive disorder or borderline personality disorder. Furthermore, the severity of the depression as well as the degree of suicidality is assessed using the Beck Depression Inventory. In serious cases, medication and/or hospitalization may be indicated. Clients are educated into the cognitive approach to therapy beginning with the first session. Client problems and treatment goals are mutually agreed upon with the therapist who maintains flexibility in structuring treatment programs. Therapists establish an important precedent by asking counse1ees to suggest items for the agenda for
Cognitive Therapy Dealingwith Depression
77
each session. The therapist suggests other items, then asks for feedback on the overall plan for each session. An important therapist characteristic is the ability to present information in a clear, concise, and understandable manner. Therapists attempt to strike a balance between being active and directive in providing explanations and rationales for problem solving and conveying a sense of collaboration with clients. Therapists instruct, model the application of various skills, and provide corrective feedback. A spirit of teamwork is encouraged as counselor and counselee act as co-investigators or "investigative reporters" who examine the counselee's dysfunctional beliefs. Therapists utilize a form of questioning like Socratic dialogue to guide clients toward accepting logical conclusions about the unrealistic nature of their erroneous assumptions. This approach leads to clients' guided discovery of maladaptive thinking and errors of logic. A common myth about cognitive therapy is that it ignores the past experiences of clients. To the contrary, assessment of past learning experiences is required because some of clients' most dysfunctional beliefs have their roots in early life or in their family of origin. Although cognitive therapists attempt to deal with such beliefs in the present, a conscious, rational exploration of the past is an important part of the process of cognitive reevaluation. A behavioral technique frequently used with severely depressed counselees who may be suffering from lethargy, inertia, and/or withdrawal is the scheduling of activities with mastery and pleasure ratings. The therapist and client generate a daily schedule for the client to follow. The client is asked to rate each activity on two 1-10 scales: pleasure and mastery. "How much did I enjoy this activity?" and "How well did I perform or cope with this activity?" The pleasure scale may contradict the client's contention that nothing is enjoyable, and the mastery scale focuses on the client's ability to act constructively. Early in therapy, clients are taught to recognize automatic thoughts. These thoughts often go unnoticed because they are habitual and take place very quickly. Clients typically do not realize that these thoughts do not necessarily represent objective reality. Clients are taught to be "healthy skeptics" about these thoughts. They are instructed to use their emotional sadness or hopelessness as a cue to
78
DEALING WITH DEPRESSION
ask themselves: "What am I saying to myself right now that could be causing me to feel so badly?" They are asked to jot down these thoughts on paper and bring them to the sessions. This is only one of many varieties of homework that are included in cognitive therapy. Whenever an affective shift occurs in a session, therapists ask: "What is going through your mind right now?" This is another method for isolating automatic thoughts. If an upsetting event is in the interpersonal realm, therapists role-play the situation with the client to elicit automatic thoughts that occur in the heat of the moment (so-called "hot cognitions"). The six systematic errors in logic that Beck proposed as early as 1967 have been expanded to ten by Bums (1992, pp. 42, 43). Bums' list follows: 1. All-or-Nothing Thinking: Seeing things in black-and-white categories. If performance falls short of perfect, individuals see themselves as total failures. 2. Overgeneralization: Seeing a single negative event as a never-ending pattern of defeat. 3. Mental Filter: Picking out a single negative detail and dwelling on it exclusively so that a person's vision of all reality becomes darkened, like the drop of ink that discolors the entire beaker of water. 4. Disqualifying the Positive: Rejecting positive experiences by insisting they "don't count" for some reason or other. In this way a negative belief is maintained even though contradicted by everyday experiences. 5. Jumping to Conclusions: Making a negative interpretation even though there are no definite facts that convincingly support it. a. Mind Reading. Arbitrarily concluding that someone is reacting negatively to you, without bothering to check this out. b. The Fortune Teller Error. Anticipating that things will turn out badly, and feeling convinced that your prediction is an already established fact. 6. Magnification (Catastrophizing) or Minimization: Exaggerating the importance of things (such as a goof-up or someone else's
Cognitive Therapy Dealingwith Depression
79
achievement), or inappropriately shrinking things until they appear tiny (desirable qualities or the other fellow's imperfections). This is also called the "binocular trick." 7. Emotional Reasoning: Assuming that negative emotions necessarily reflect the way things really are: "I feel it, therefore it must be true." 8. Should Statements: Trying to motivate yourself with shoulds and shouldn'ts, as if you had to be whipped and punished before you could be expected to do anything. "Musts" and "oughts" are also offenders. The emotional consequence is guilt. When you direct should statements toward others, you feel anger, frustation, and resentment. 9. Labeling and Mislabeling: This is an extreme form of overgeneralization. Instead of describing your error, you attach a negative label to yourself: "I'm a loser." When someone else's behavior rubs you the wrong way, you attach a negative label to him: "He's a louse." Mislabeling involves describing an event with language that is highly colored and emotionally loaded. 10. Personalization: Seeing yourself as the cause of some negative external event for which in fact you were not primarily responsible. One particularly useful format of homework for organizing, concretizing, and recording the self-help process is the Daily Record of Dysfunctional Thoughts (Beck et al., 1979). Figure 6.1 gives the format that is given to clients in printed form on which they can record their thoughts. Bums (1992, pp. 62-65) regularly utilizes a shortened version of this. He simply has clients draw two lines down a blank piece of paper, dividing it into thirds, and then labeling the columns automatic thought, cognitive distortion, and rational response (see Figure 6.2). Another method used to reevaluate dysfunctional thinking involves reverse role playing. The therapist plays "devil's advocate," arguing in favor of the client's automatic thoughts, while the client is given the responsibility of countering these arguments with rational responses. Sometimes the therapist accentuates this process
gg
1. Specify sad! anxious/ angry, etc. 2. Rate degree of emotion. 1-1000/0
Briefly describe the actual event leading to the unpleasant emotion. Write the automatic thought(s) that accompany the emotion(s).
Automatic Thought(s) Identify the distortion(s) present in each automatic thought.
Cognitive Distortion (5) Write rational response(s) to the automatic thought(s).
Rational Response(s)
Specify and rate subsequent emotions. 0-100%
Outcome
Explanation: When you experience an unpleasant emotion, note the situation that seemed to stimulate it. Then, note the automatic thought associated with the emotion. In the rating degree of emotion. 1 =a trace; 100 =the most intense possible. *Copyright 1979, Aaron T. Beck
Emotion (5)
Situation
FIGURE 6.1. Daily Record of Dysfunctional Thoughts.
~
2. Overgeneralization
3. Mind reading Overgeneralization All-or-nothing thinking Fortune teller error 4. Labeling 5. Labeling Fortune teller error
2. I'm always late.
3. Everyone will look down on me.
4. This shows what a jerk I am.
5. I'll make a fool of myself.
I (Burns, 1992, p. 63)
1. Overgeneralization
Cognitive Distortion
1. I never do anything right.
(SELF-CRITICISM)
Automatic Thought
5. Ditto. I'm not "a fool" either. I may appear foolish if I come in late, but this doesn't make me a fool. Everyone is late sometimes.
4. Come on, now, I'm not "a jerk."
3. Someone may be disappointed that I'm late but it's not the end of the world. Maybe the meeting won't even start on time.
2. I'm not always late. That's ridiculous. Think of all the times I've been on time. If I'm late more often than I'd like, I'll work on this problem and develop a method for being more punctual.
1. Nonsense! I do a lot of things right.
(SELF-DEFENSE)
Rational Response
FIGURE 6.2. The "triple-column technique" can be used to restructure the way you think about yourself when you have goofed up in some way. The aim is to substitute more objective rational thoughts for the illogical, harsh self-criticisms that automatically flood your mind when a negative event occurs. .
82
DEALING WITH DEPRESSION
by asking the client to imagine that a best friend's automatic thoughts are being challenged. Ideas for homework are abundant in cognitive literature. Bums (1989, pp. 561-563 and 1992, pp. 128-130) gives two different lists summarizing a dozen or more each time. If a client refuses to do any such assignments, the therapist avoids labeling the client as "resistant" or "passive-aggressive." This would mean that the therapist is engaging in dysfunctional thinking. Rather, the therapist can model appropriate problem-solving behavior and work with the client to identify the sources of difficulty. Actually, the homework is designed as a "no-lose" assignment that cannot be failed. Cognitive therapy is known as being a short-term treatment method. Most outcome studies specify an average of 12 to 16 sessions before termination. However, the chronic nature of a diagnosis of dysthymia dictates that treatment will run a longer course, perhaps six months to two years. Cognitive therapists give a good deal of attention to building self-esteem. They stubbornly refuse to agree with their clients' feelings of worthlessness. They agree with other researchers that there is a formal thinking disturbance among the depressed. They urge their counselees to talk back to their "internal critic," mostly by using the Daily Record of Dysfunctional Thoughts. Cognitive therapists also take clients' anger seriously. Bums (1992, pp. 194-197) suggests ten ways to deal with anger. He says you are responsible for your anger by the way you choose to think about the events around you. Anger usually does not help, so energy should be used to find solutions. Correcting distorted thoughts will often reduce anger. Anger is frequently caused by the belief that someone acted unfairly. These actions may not seem so unfair when seen from that other person's point of view. Retaliation is unlikely to achieve anything positive. Pouting and insisting that you have the right to be angry are childish. TilUS, you rarely need your anger. It is seldom to your advantage. The feeling of guilt is often brought on by distorted thinking too. Depressed people have a self-defeating way of irrationally expecting themselves to be perfect, all-knowing, or all-powerful. So, guilt feelings are usually an offshoot of perfectionism.
Cognitive TherapyDealingwith Depression
83
Nezu and Nezu (1989, pp. 133-135) suggested a number of pitfalls that cognitive therapists should avoid. These include: behaving in a mechanistic manner, utilizing techniques not relevant to a particular client, omitting homework, using humor injudiciously, focusing more on techniques than on the client's feelings, giving undue attention to superficial problems, and inadequately assessing suicidal potential. To summarize, there is considerable evidence that cognitive therapy is effective as a short-term treatment for unipolar depression. It is also efficacious in treating dysthymic disorder over a longer period of time, and bipolar disorder when paired with medication. Caution is advised when using this theory with clients who are "intellectualizers." Cognitive therapy has an excellent record of outcome research studies in the treatment of depression. BIBLIOGRAPHY Alloy, Lauren B. (ed.) Cognitive Process in Depression. New York: Guilford Press, 1988. Baldwin, Lannes. "Cognitive Therapy." Chapter 12 in Gilbert, Marvin G. and Raymond T. Brock. The Holy Spirit and Counseling. Atlanta: Hendricks Publishers, 1985, pp. 188-205. Beck, A.T. "Thinking and Depression: 1. Idiosyncratic Content and Cognitive Distortions." Archives of General Psychiatry, 9:324-333, 1963. Beck, A.T. Depression: Clinical, Experimental and Theoretical Aspects. New York: Hoeber, 1967. Republished as Depression: Causes and Treatment. Philadelphia: University of Pennsylvania Press, 1972. Beck, Aaron T. Cognitive Therapy and Emotional Disorders. New York: New American Library, 1979. Beck, Aaron T., A. John Rush, Brian F. Shaw and Gary Emory. Cognitive Therapy of Depression. New York: Guilford Press, 1979; paperback 1987, 14 printings. Bums, David D. The Feeling Good Handbook. New York: William Morrow, 1989. Burns, David D. Feeling Good: The New Mood Therapy. New York: William Morrow, 1980; Revised Edition, New York: Avon Books, 1992. Burns, D.D. and A. T. Beck. "Cognitive Behavior Modification of Mood Disorders," in Foreyt, 1. P. and D. P. Rathjen (eds.), Cognitive Behavior Therapy: Research and Application. New York: Plenum Press, 1978, pp. 109-134. Ellis, Albert. Reason and Emotion in Psychotherapy. New York: Lyle Stuart, 1962. Ellis, Albert and R. Grieger. Handbook ofRational-Emotive Therapy. New York: Springer, 1977.
84
DEALING WITH DEPRESSION
Ellis, Albert and Robert A. Harper. A New Guide to Rational Living. Hollywood: Wilshire Book Company, 1975. Hauck, Paul A. Reason in Pastoral Counseling. Philadelphia: Westminister Press, 1972. Hauck, Paul A. Overcoming Depression. Philadelphia: Westminister Press, 1973. Hauck, Paul A. Brief Counseling with RET. Philadelphia: Westminster Press, 1980. Kendall, Philip C. and S. D. Hollon. Cognitive-Behavioral Interventions: Theory, Research, and Procedures. New York: Academic Press, 1979. Kendall, Philip C. and David Watson. (OOs.) Anxiety and Depression. New York: Academic Press, 1989. McMullin, Rian E. Handbook of Cognitive Therapy Techniques. New York, London: W. W. Norton, 1986. Nezu, Arthur M. and Christine M. Nezu. Problem-Solving Therapy for Depression: Theory, Research and Clinical Guidelines. New York: Wiley-Interscience Publications, 1989. Persons, Jacqueline B. Cognitive Therapy in Practice. New York, London: W. W. Norton, 1989. Schuyler, Dean. A Practical Guide to Cognitive Therapy. New York: W. W. Norton, 1991. Wtlkes, T. C. R., Gayle Belsher, A. John Rush, Ellen Frank and Associates, Cognitive Therapyfor DepressedAdolescents. New York: Guilford Press, 1994. Wolman, Benjamin B. and George Stricker (eds.). Depression Disorders: Facts, Theories, and Treatment Methods. New York: Wiley & Sons, 1990.
Chapter 7
Medical-Religious Case Conference Moderator: Robert M. Mathews Presentor: Richard Dayringer Patient: Pam (pseudonym) Interviewer: Myron C. Madden Consultants: Byron Eicher Morton Jacobs (Representing T.A.) H. Darby Trotter
Dr. Mathews: Through the training program in Clinical Pastoral Education here in the hospital, we have had at least one MedicalReligious Case Conference a week for the last eight or nine years. I have participated in several of these conferences myself. Usually only a few students, along with those in the helping professions who are closely associated with patients, are present. Because of this, we are particularly pleased to be able to share one of these conferences with a larger public now. In the presentation below, Dr. Dayringer explains the case of one of his current counselees. This young woman is interviewed by Dr. Madden, then by consultants Dr. Trotter, Dr. Jacobs, and Byron Eicher.
CASE PRESENTATION
Dr. Dayringer: The counselee, whom we will call Pam*, is 36 years old and married. She has a teen-age son and an ll-year-old girl. Pam has a part-time job, is a housewife, and a high school *"Pam" is, of course, a pseudonym for this counselee whose identity is carefully disguised. She has read this transcript and has given her permission for it to be published.
85
86
DEALING WITH DEPRESSION
graduate. Her religious denomination is Baptist. Her health is good, and she is under the care of a physician, Dr. Abrams, who has been prescribing Elavil for her. In her own family, Pam was the second girl among four children; both of the parents are living. She had previous counseling at another center five years ago. I first saw her four months ago.
Presenting Problem On Labor Day, Pam described to a friend in a telephone conversation how she had been feeling. The friend, who maintained that she was demon-possessed, had responded by saying that she felt just like Pam did. Ever since this conversation, Pam told me she had been "running scared." She felt that God had "dropped" her and turned her over to the devil. Apparently, Pam was convinced that she had hurt her mom in a church split when she left the church with a tongue-speaking group to begin another church. Her guilt was obvious. To this end Pam read books about the devil and she stopped smoking. She said she had talked daily with her pastor, who prayed for her and told her that she was "tom up by the devil." Frightened, Pam attended exorcism meetings and was told that she had too much spiritual pride for her demon to be cast out. "Running scared" for her meant keeping busy, working, and shaking or trembling. She could not read the paper, watch television, or even sit down to eat. She felt that she had to be almost perfect to earn the love of God or others. Pam had been waking up during the night afraid the demons would destroy her, and she usually arose about 5:30 a.m. and began walking, crying, and praying. With a poor appetite, Pam had lost 15 pounds in seven weeks.
Description and BriefHistory The patient is about 5'3", weighs about 130 pounds, has short brown hair, and is attractive. She is tense, agitated, and fearful. Pam has one sister two years older than she is, one sister ten years younger, and a brother who is eleven years younger. She always felt inferior and ugly in comparison to her older sister. After having been the baby in the family for ten years, Pam felt unloved and
Medical-Religious Case Conference
87
neglected when two new siblings came along. She was forced to take on the extra responsibilities of helping around the home thereafter. Her father told her on several occasions that if she did not help more, her mother would die, because she was not well. Pam obviously was afraid of her father. He ridiculed her often and she never could seem to get his approval. On the contrary, Pam felt that her mother loved her. Her happy memories are about junior high cheerleading. She started working at age 15 in order to get out of the house. The money she made pleased her father, and she made it a point to try to please everyone.
Initial Evaluation My initial evaluation of Pam was agitated depression, complicated by a phobia of demon possession. She had most of the clinical symptoms of depression and described her symptoms in religious concepts. Her responses to the Minnesota Multiphase Personality Inventory confirmed my clinical impression. Tonight, while she was waiting, the patient responded to the "Self-Rating Depression Scale" (SDS) developed by William W.K. Zung, M.D. She came out with a raw score of 43 and an SDS score of 54, which put her in the category of "depressed outpatient" according to this scale.
Initial Recommendation I told Pam frankly that I did not believe in demon possession in the same way that she probably did. I explained that in my opinion such a term was used in the first century to explain unexplainable behavior. Similar behavior is now explained as emotional maladjustment. Many psychologists today understand demon possession as the denial of an unacceptable part of the self that is projected onto demons. I told the patient she was suffering from depression. Later, we made a relaxation tape, which I asked her to use daily. This is a technique of behavior therapy whereby the patient tenses and relaxes various muscles in her body and learns to relax by working through the contents of the cassette recording. I also suggested rubber band snapping each time that she thought about being demon-possessed. This technique helped her to associate pain with
88
DEALING WITH DEPRESSION
the obsession. Then I sent Pam to her physician with instructions to say that she was depressed and to ask for antidepressants.
Recapitulation ofthe Counseling Relationship I was Pam's pastor for more than six years and was the one who performed her wedding. She hesitated initially in coming to me because she has since left that church. I saw her 16 times individually and then transferred her to my counseling group. Pam has attended three of six group sessions. (Because of her working schedule, she could not be there for all six.) I talked to Pam's husband several times and to her parents twice about her behavior in order to determine that hospitalization was not necessary. We often talked transaction analysis language (P-A-C) and used concepts and techniques from behavior and Gestalt therapy. Attending church services became a problem, since Pam cringed at any reference to the devil or demons from a Sunday School teacher or her pastor in his sermon or scripture. Later, she developed feelings of anger or disbelief toward her pastor, who seemed to be playing one of Eric Berne's games entitled, "I am only trying to help." In our fourth session, Pam brought in a list of her fears that I had asked her to record. This list contained 25 fears, ranging from the fear of the devil to fear of sex. We worked at desensitizing these fears and by the thirteenth hour, she said that there were only two fears left: the fear of demons and the fear of possible reoccurrence of her back trouble. The fifth session was the first one in which Pam did not cry. I asked her to bring a list of her anger and resentments to our sixth meeting. Much of the young woman's anger was directed toward the church for forcing her to make a choice as to which church division to accept and for not miraculously ending her depression through prayer. By the eighth session, Pam related to me how she had yelled at her husband in an argument and told her mother off for trying to get her to rejoin the original church. Until this break had occurred, Pam wanted her mother with her as much as possible and had spent much of her time either at her mother's home or having her mother in her home. In the ninth session, Pam told me about a dream she had in which I was too busy to see her. I used the Gestalt approach in dealing with the
Medical-Religious Case Conference
89
dream by asking the patient to be the people and things in the dream. I ended the session by telling her that I was not too busy to see her. By the twelfth session, Pam stated that she rarely shook anymore and that her sex life was much better. She was feeling well enough that appointments fourteen through sixteen were two to three weeks apart. After this, she was transferred into the group.
Clinical Pastoral Appraisal The patient had to assume many responsibilities beginning at age ten, responsibilities which stifled a carefree childhood. She probably had thoughts and wishes about her parents that she could not forgive herself for and did not think God could either. Although Pam has since suppressed and disowned these thoughts, they still produce guilt. Disagreeing with her mother in the church dispute revived her guilt and she explained it as a demon presence. I have a number of questions for the panel of consultants and I am eager to begin a case discussion. So, at this point, I would like to know if there are questions from the consultants before we interview the patient. DISCUSSION OF CASE PRESENTATION
Dr. Madden: How much does she know of this? Does she know that we are getting this information? Yes, she does. She agreed to this whole procedure after discussing it with her husband.
Dr. Jacobs: You mentioned that she was with her mother a good deal. Is her father alive? Yes.
Dr. Trotter: What about her relationship with her husband? It seems to be good. He has been very supportive of her during this ordeal. The church decision was hers. He let her make that
90
DEALING WITH DEPRESSION
decision and tried to go with her in the choice. I think he has been very supportive to her in the midst of this depression and in the counseling that she has been receiving.
Dr. Jacobs: How long ago did she make the splitfrom the church? About two years ago; I don't have a date on that precisely. When did her father tell her that she was going to destroy her mother? This was at about age ten and thereafter when her younger siblings were born. She began to do a lot of housework and was called on to do more and more. She felt a lot of responsibility. What can you tell us about her previous counseling? She had counseling five years ago and was hypnotized in that treatment. Later on someone told her that demons often enter people during hypnosis. What was the reason for her treatment at that time? I am not sure, but I think it was depression. Has she had any thoughts about how these strange forces got into her; whether anybody was involved? Was there any denial and projection? No, I think not.
Dr. Trotter: Did you say that you were once her pastor? Yes, I didn't know her very well then. It was during her adolescent years. I performed her wedding the last year I was there as pastor. I knew her family quite well, but mostly I dealt with the total family rather than Pam in particular.
Dr. Madden: What about her back trouble? She has had some back trouble and was in the hospital. It seems to me that she had to have surgery.
Dr. Trotter: Did she have to get married? No. Can you tell me some more about the current family situation? Yes, her son is getting into his teenage years where he is not as easy to control. She had tried to hide a good many things from the
Medical-Religious Case Conference
91
family, like, for instance, her smoking. She hid that for quite awhile and then during counseling went home and smoked in front of the family. Some of the people in her neighborhood thought of her as a "super Christian" until she became a little more relaxed about doing openly some of the things she had been doing in hiding. Does she have sexual problems? Oh, yes. She seems to love her husband and to have good warm feelings for him. But she has been pretty inhibited sexually and quite reluctant to ever approach him and initiate sex. He always seemed to have more interest in sex than she did and she often was reluctant to engage in sexual intercourse. She has been a very serious sort of person all of her life, with a dominating Parent, in the language of transactional analysis. She rarely gave her Child a chance to play and hasn't known much enjoyment.
Dr. Madden: Did the split in the church seem to bring on the more recent disturbance? Yes, I feel that the emotional pull-and-tug between the two factions was significant in the exacerbation of her problem. Does this typify her struggle, that she gets wedged between the two forces? It may: I felt that it almost revived the old guilt feeling about her mother that Pam has had much earlier. Maybe the feeling of being wedged between her mother and father, along with attemptingto be the household savior by doing the housework, reinforced this feeling.
Dr. Jacobs: Were there any events preceding this? Yes, the patient received a phone call from her friend. Then while she was riding to Kansas City to visit her older sister, she began to think about everything that had happened and started to shake and cry. I think the acute onset came during that trip. Why was she going to Kansas City? The occasion was a Labor Day outing with the family to visit her older sister. What did she begin to think about? About demons? Yes, she began to think that God had forsaken her and turned her over to the devil.
92
DEALING WITH DEPRESSION
What was there about going to visit her sister that precipitated that? Maybe some of these feelings that she had about the sister (that she was second place because her sister had met with parental approval and she had not) precipitated the onset of her disturbance. Had she been seeing her sister through the years? Yes. Why would this be coming about now? Well, I think it has to do with all that had been going on with the church and the recent telephone calls from her very close friend who said she was demon-possessed. She got this call on Labor Day and then later that day drove into Kansas City. She was already feeling depressed at that time and I am wondering if it is a continuous state. Perhaps the counseling five years ago was also to deal with depression. What was it that led her to the speaking in tongues movement? Why did she go for this in the split? Her Sunday School teacher was the one who led this particular group from the church to establish a new church. This teacher had been quite influential in her life. What about her relationship with her mother as a child? I think Pam was close to her mother and loved her. Yet she must have felt angry at her mother at times because of having to do so much of what seemed to be her mother's work. Still, I think her mother came across as a loving, accepting person. Had her mother been ill? No, not seriously ill. Her mother had diabetes. Is her mother very possessive? No, but she does seem to be rather controlling of her children's lives.
PATIENT INTERVIEW Pam was then brought into the room. She sat behind a screen so that she could see the panel of consultants and be seen by them. She could not see the audience, but they could see the shadow of her silhouette through the screen. She was introduced to Dr. Madden, who interviewed her.
Medical-Religious Case Conference
93
Dr. Madden: Pam, we are here for two purposes as I understand it. First, we are here to help you. Maybe the rest of us can help Dr. Dayringer as he works with you. Second, the audience can get some better understanding about helping people who have depression. We will all benefit if we understand a little better and if we understand you. Now, Dr. Dayringer has just told us about your case. You understood that he was going to do that, of course. Let me begin by asking you a couple of questions. How do youfeel about demon possession? I don't believe in it anymore. What was your feeling when you did believe it? Can you describe this? Have you seen the movie, The Exorcist? No, I wouldn't go to see it, either. I've had my mind tampered with enough. Do you find that in the past you have gotten wedged between your loyalty between the groups at church? Have you experienced this? Of being pulled by your relationships, friendships? Yes, I didn't know which way to go. I went with the group that I had started with and most of my friends did, too. You stayed with the people you were closer to? Yes, with people who were more my age. Have you ever had this feeling before? Do you remember the feeling you had during the division of the church? I have never had that feeling before. Let me ask you a rather strange question. When were you somebody's number one? Does that make sense? Have you ever been somebody's number one fully? I feel like my husband makes me number one. And this gives you security. Can you take this back to your childhood of being number one? No, I never felt that way in childhood. I was just one of the four and felt like the others were important in their own way, but I wasn't. You weren't special? No, because my older sister was the first, and then I was born. Ten years later another sister was born, and she was sort of like the first over again. Then came my only brother and they babied him, so I felt that they all had their place more than I did.
94
DEALING WITH DEPRESSION
You were feeling overshadowed perhaps? Did you feel special with your father then? Or didn't you? No. And thenfelt no specialness with your mothet; either? Not really. I knew they loved me, but I wasn't specialas an individual. Do you still have to earn your place with your family? I think I still have to work at it. How do you do that? Well, right now, I am not working at it. Earlier, I was trying to do just what everybody wanted me to do and being what people wanted me to be, and trying to live up to their expectations. You say that this demon thing has kind ofgotten out ofyourfeeling, but where is God and what is He like to you? I believe that God is the God of love; I feel it now. When I went through this, I felt that He didn't love me and if He did love me, why did He let this terrible thing happen to me? What terrible thing? This demon stuff. I couldn't understand it because I had always believed that God loved me. Then I felt that He had just dropped me. When did you feel He dropped you? When I started getting nervous and depressed. I didn't know what was happening to me, and then I was told I had a demon. I felt bad. When were you told this? How long ago was it? I started getting depressed in September. I tried not to let anyone know about it. I just thought it would pass. I didn't even tell my husband. Then I got desperate. I had to tell somebody. I had read a lot of books about demons and I think maybe that is what started it off. Then I talked to our pastor, and he told me that I was demonpossessed. How did you get so you didn'tfeel this anymore? Counseling with Dr. Dayringer. In other words, you hadfaith in his faith. Yes, I did. I just leaned on that faith. He told me that I was safe. I remember asking him if I went home, would I be safe, and he said I would. Then when I got frightened I would think, "He said I was safe." I was just leaning on his faith until it became more real to me. Youfelt then that God loved you? Yes, I know God loves me.
Medical-Religious Case Conference
95
In saying that, do you feel like He makes you number one? No, I feel like he loves you also as much as he loves me, so I am not really number one. What I am trying to say is that I don't think He has any number twos. I wanted that to sound good because I believe that. Do youfeel that God's love cast out this demoniac spirit or whatever it is you felt? At that time I tried to figure out what I had done to make God angry with me. Well, what makes Him angry? Now I don't think He was angry. At the time, I startedreading my Bible and praying. I just couldn't imagine what had happened to my relationship with God. I was told I had a demon. So, I thought something must be wrong somewhere, and I knew it wasn't on God's part. Did you ever name that demon? I don't think so. One minister called it a demon of fear. Where are you now in terms ofyour progress? What can you say of yourself, your feelings? I feel that I am beginning to get back together, and I feel that I have really come a long way. I am not back where I would like to be yet emotionally. I am not as peaceful and happy as I was before all this happened. Your husband makes you number one. Are you able to make him number one? In my mind, yes. It is a task and is not easy.
Dr. Jacobs: You said you were peaceful at one time before this happened. When was this? Before I started getting nervous, last September of this year. Youfelt nice and peaceful before? I think it was building up through the religious meetings I had attended. You said your mind was tampered with. I am a little puzzled about that. I guess that was really a poor expression. I was just listening to uneducated ministers who really don't have the right to tamper with
96
DEALING WITH DEPRESSION
our minds. I really feel strongly against ministers who are not educated. You mean the minister told you this? I blame him, yes. I feel pretty bitter toward him, but I also blame the whole mess, this charismatic group. When you were feeling this wa)7, did you feel that anybody or anything was okay? I felt like everyone else was okay, but I felt like I was the victim, and I didn't know why. You were the only one who was not okay and everybody else was all right? I knew a couple of others who were supposed to have had the same problem. Whose victim did you think you were? I don't know, just kind of an example, I guess. Had you felt that you were not okay when you were small? There were times. I gather that your family expected a good deal from you when you were small. Yes. Did you feel that you were able to live up to their expectations? I did live up to their expectations. What did they expect ofyou? They expected me to be perfect, and I don't mean to say I was; I tried. Is that what you were trying to do last fall? Yes, really that is how I got into the whole thing of trying to be better. Has anything else happened to you in the past few years? Outside of my church problems, my life has been fine, but I have been too involved in church problems. My family life has been fine. Youfeel your problems have been centered around the church? They sure have been. I am wondering if there is any part ofyou that is involved in this? I blame myself to an extent because I feel like I should have thought for myself more and reasoned things out more, rather than taking the word of other people. I have learned to think for myself more. I feel bitter toward most preachers. I sure do. Especially those
Medical-Religious Case Conference
97
who try to preach and lead people when they are not educated and they do not know what they are doing. I think I was taught right at home, though. You blame yourself then for believing the things that you were told? Yes, I am beginning to forgive myself since this movie, The Exorcist, has come out. I have seen where so many people have fallen for it, so I really don't feel ridiculous any more. When you went for help, you went to your pastor; so there must have been some problems before you went? That is why I went. What was the problem when you went? I was afraid, and I didn't know what was wrong with me. I had read a lot of books on demons, and I had been to meetings where there was supposed to be deliverance. I think that at the beginning I came because I was afraid. Have you ever thought that the demon might represent some force within yourself? Some part ofyou, not something foreign? No, I don't think so. Do you trust this man, Dayringer? Yes, I do. Does he redeem the preachers for you in some way? Yes, I don't put down all preachers. But you have found out that they are human? Do you accept that they are human? I accept that they are human, but I feel they should be. I feel that they ought to know the truth before they start preaching.
Dr. Trotter: How do youfeel toward psychologists? I have a high regard for psychology. You said you lived up to your parents' expectations? Yes, I did. Did they recognize this? They didn't until my younger brother and sister didn't, then they realized that I had. I always did what I was told, and I never caused them any trouble. I don't think they really realized it until my younger sister and brother gave them problems. Then they recognized it. What about your family now: you have a son and a daughter? They
98
DEALING WITH DEPRESSION
place a lot of expectations on you as a mother Do you continue to try to live up to their expectations? No, I really don't. Had you at one time? Yes, I did. I really began to break over when I started smoking in front of them. I decided that they needed to know that I am human. My husband always told me that I was too involved. He tried to slow you down. Yes, he did. Why did he feel that you were too involved? He felt I was too involved in church and getting too carried away with a bunch of radicals. What about your friends? Were they aware that you were putting forth to meet the expectations ofall the people around you? I really don't know.
Dr. Jacobs: I am wondering what you expected to benefit from fulfilling what your parents expected ofyou? I just wanted approval. Youfelt that you could not have approval unless you did that? Yes. Didyoufeel that they did approve ofyou? I never felt that I had made the mark. Intellectually I know I was loved, but I never felt loved. Did youfeel you could be loved if you were perfect? Yes, but I could never quite be perfect.
Dr. Madden: Did your parents bless you? No. Who do you authorize to bless you? Maybe God. Would you let your parents bless you now? Or would you tell them they were a little too late? No, they would never be too late. They have been my best friends while I've been going through this depression. We have talked a lot, and they have told me how they loved me.
Medical-Religious Case Conference
99
And did you receive it? Yes, I think I have. Dr. Dayringer has helped me to accept myself as I am.
Dr. Trotter: Do you recall being sad before the demon thing? Did you ever recall being depressed in childhood? Yes, I can remember being depressed in childhood. Did youfeel betterfor awhile when you broke away from the church and you were first told you had a demon? I felt sad. Did that sadness leave? Was it replaced by some other kind of feeling? I was mad. I was running scared and trying to find someone to help me. I am going to ask you one more important question that is a serious one, so don't take it lightly. I want you to be very sure of your next answer; okay? Okay. Did you feel more or less depressed when you came to believe you were possessed? I felt less depressed. Thank you. At this point, Pam was thanked for her willingness to be interviewed and for the help that she had given in this conference. She was excused, and she left the room.
EVALUATION AND SUGGESTIONS BY THE PANEL
Dr. Trotter: This patient serves as an excellent example of severe depression occurring when the behavior-to-reinforcement ratio is too high. Her case also illustrates avoidance behavior contributing to increasing behavior-to-reinforcement ratio, failure to escape from aversive conditions leading to a sense of helplessness, and excitement used as a competing response to depression. Put more simply, the patient referred time and again to the high expectations placed on her, her attempts to meet them, and her
100
DEALING WITH DEPRESSION
failure to achieve the reinforcing sense of approval she so desperately wanted. For example, she stated that she was trying to find a place in the family through "doing just what everybody wanted me to do and being what people wanted me to be, and trying to live up to their expectations." She felt they expected her to be perfect. She stated she just wanted approval. To her, being perfect would gain approval. She wanted to be special and important. In spite of her efforts, she continued to feel victimized and overshadowed. She was the baby of the family for ten years and then was forced to accept the birth of two siblings, which ended her special role (permanent withdrawal of positive reinforcement) and caused her parents to expect her to assume responsibilities. She was not able to feel any sense of approval from her parents but out of deprivation tried harder to win this approval. No doubt she had been trying too hard to please and has had so little reinforcement that her depression is chronic. The patient's compulsion to try harder and harder to please others in the face of low levels of reinforcement can be understood by examining her intense efforts to avoid aversive control. Such control was evidenced in the frequent prediction and experience of withdrawal of affection and predictions of unpleasant consequences, such as being responsible for her mother's death if she did not work hard enough. This aversive control is evident throughout the interview. Examples include her feelings that God had abandoned her to the devil for not being perfect, feeling she had done something wrong to make God angry with her, fearing her father had ridiculed her and never given her approval, feeling she had hurt her mother by changing churches, and expecting some withdrawal of affection because of the decision, hiding smoking and other behaviors less than "super Christian" from her parents, doubting she would have any place in the family if she did not work hard, and striving hard to please everyone so they would not reject her. Because this young woman tried to be perfect so as to avoid aversive consequences, she placed behavioral demands on herself that far outstripped available reinforcement. Even a very supportive husband was not able to provide the reinforcement required to maintain her striving to be perfect in order to prevent or avoid rejection and attain approval. It is not surprising that she often felt victimized. A number of performance fears seemed to spring from her avoid-
Medical-Religious Case Conference
101
ance behavior and she was always very serious. This was the result of overmonitoring her behavior to ensure that it was acceptable. Letting her hair down would have been too risky. Casual behavior may not have been acceptable and could have generated criticism. Overmonitoring her behavior included suppression of feelings, particularly hostile feelings and even self-assertive comments. This patient's striving to be special to avoid or escape aversive consequences was rarely successful. Thus, in spite of her efforts, she could not prevent rejection, ridicule, and a sense of being unimportant. This gradually gave way to marked feelings of helplessness. She felt like a victim with no way to influence the outcome of her life. She became highly suggestible to others' confidences because she had none of her own and in a very dependent way, she let others shape her attitudes and behavior. Her depression reached severe proportions and she became certain she was unacceptable even to God. The notion of being possessed by the devil fit this state. She did feel helpless and bad. Feeling abandoned by almost everyone, this young woman discovered that accepting the notion that she was possessed made her feel less depressed. Treatment of this patient could include the following: confrontation regarding the effects of increasing the behavior-to-reinforcement ratio; desensitization to fears of punishment; reinforcement of risk-taking behavior and playfulness; developing ways to interrupt her obsessions regarding being possessed, such as by using the rubber band or by frequency counting method; assertiveness training and group therapy to encourage self-identity and independence; and habit extinction used to count the number of times she discovers herself suppressing feelings or worrying about aversive control.
Byron Eicher: I think she is blaming others and avoiding responsibility. She blames others for who she is and she is playing "victim." I really did not have any questions to ask because the interviewers brought out what I thought were the kinds of things supporting the Gestalt view of an introjector. This young woman has not learned to discriminate very adequately between self and others. She has not learned much resistance and she has felt pretty vulnerable to the world. There was no indication that she could assert any dominance
102
DEALING WITH DEPRESSION
of her own choice system. She was not able to choose. She took what was given and saw no indication that she was able to arrange any of her personal experiences in any way differently. Whatever she was given, that's what she got. In terms of working with her, I have these comments. If I ran "bastard" sessions on odd months, I would enter her in a "bitch" group on the even months. That is, I think she needs to get in touch with her "dark side" a bit. As I looked at her, I saw someone who smiled continuously, had such a well-modulated voice, was nice and kind, gentle and good and tried to please. I would do anything to work contrary to that perception to teach her to be otherwise. I think if she could get in touch with whatever part of her is a tiger that we might see a very different kind of person. Now her parents might not be too happy with her and it might amaze her husband, but she would probably be a little happier. I would actually try to get her to get in touch with the "demon" in her. When I was in therapy, I had a dream about an albatross. So for five sessions I wrestled with an albatross and actually became the albatross. It may sound ridiculous, but I got a hell of a lot more out of being an albatross even though it was my own, a part of me. So, when someone reports a demon to me, I take that very seriously. It is not so bad to get in touch with a demon (if it is your own) rather than living the split, which is one of the things in which a Gestalt therapist is interested. I would help this patient to become her demon and let it become part of herself. If you help her to get rid of it, it would be like peeling an onion and taking off each layer of skin when you find out that there are some flaws and throwing each layer away. Soon you would have peeled that onion right down to a soft little core that wouldn't make a decent salad. It would just give you bad breath. So, rather than throwing it away and getting rid of a behavior or getting rid of feelings, the whole purpose of Gestalt is taking back feelings and owning them. I do not think that we can throwaway any part of what we are in this world. I did not hear many "I" statements from this patient. I hope she can get more of a sense of "I" rather than being so adaptive and kind. I would give her "bitch" lessons.
Medical-Religious Case Conference
103
Dr. Trotter: The patient has always avoided that angry side of herself, and she needs to let it come out. I would put her on the frequency counting system and ask her to count every time she suppressed an angry statement. I do not think I would mention "demon" to her but rather "anger" instead because I feel that she is extremely suggestible. I would want her to meet with the family and prepare them for this change in her behavior. Otherwise, her family might think she had really gone crazy when she started getting angry.
Dr. Jacobs: I do not see this patient as having made any significant changes in her position since childhood. She seems to have had the same feelings of persecution for a long time. The change is from depression to anger, gradually evolving to the point where she was unable to contain it and it had to be projected. This young woman has very little ego strength, very little sense of self. Threatened by her angry feelings, she can cope with them only by projecting them to others. She has not, in any sense, begun to take responsibility for this side of herself. So one of the things you begin to wonder about if you are going to work with her is, what does she want? What kinds of changes does she want'iRight now she seems to want enough support to pull herself together. I do not think she has any desire at this point to know what she would regard as an evil side of herself. She sees her demon as very evil. I think this revelation could be threatening to her if it is not made skillfully. I am not saying that it cannot be done, but rather that it will have to be done with her cooperation. The patient will have to be the one who is going to recognize her inner evil. She might become quite disturbed as she realizes this side of herself. I think before you go ahead and set such goals for therapy, you want to be pretty sure of your grounds. I think it could be quite dangerous for people without adequate training to attempt to do something like this with someone.
Dr. Madden: As I see it, the precipitating factor of her depression was her entrance into puberty, which brings up her whole sexuality problem again. It is a conflict which she never settled with her parents. So it
104
DEALING WITH DEPRESSION
is an unresolved thing. There is evidence here of unresolved sexuality. She does not know that she is a woman yet, really. I think her demon is a combination of deep shame and a deep pain and Dick has been able to work with her enough to quiet it down. He has not tried to cast it out yet. That pain and that shame may never come out. I think Dick may not be wise to get it out of her. After all, the pain could be centered around a ten-year-old girl having to face the fact that there is somebody else on the nipple who has replaced her. She could go into the biggest rage you have ever seen about the fact that she had been replaced. She could make resolutions and vows of vengeance and hatred and then have to hide these and live with them. Her demon is very powerful and potent. Dick has given her some good affirmation to build on. I think he has to use that affirmation to confront her about working with the pain and the shame.
Dr. Dayringer: As you know, Pam talks about feeling safe more because of what I have suggested to her rather than because of anything within her. My first concern was to deal with her fear and try to replace that fear with a little more calmness. I think within time she can get stronger and face some of these things more squarely as being things within her more than outside of her.
Dr. Trotter: She may not know how to deal with responsibility, and she is going to have to be trained. Insight alone will never give her all the skills she needs. You must teach her to be a competent person. The more you teach her to take care of herself, the better she will feel. She will not be dependent on someone else. The more she can become competent, the more responsibility she can comfortably assume.
Dr. Jacobs: I feel that Dr. Dayringer has done an excellent job with her. He has given her the warmth and support she desperately needed so that she could accept herself. I visualize Pam as being able to benefit very much from a group in which she could acquire a much better feeling about herself and to feel a good deal of strength about herself as a person. Gradually she might be able to accept further goals. I also
Medical-Religious Case Conference
105
think she needs to develop additional skills. I would be a little careful about too much individual work with her and try to move her more into a group. I think she might focus on you too much individually, Dick, and I think therapy should be spread out more into a group as a whole. In my opinion, she is very close to being psychotic.
Dr. Trotter: We have not talked about the family much and I think the family needs to be more involved in treatment. Although individual treatment should continue, I caution Dick to avoid transference and dependency, since the patient might lean on him and then blame him when things do not go right. I suggest bringing in the family, utilizing the group approach, and spending time therapeutically to try and teach her how to be more competent in dealing with things and encourage more responsibility through some of her behavior techniques. Sensitivity is important in dealing with this young woman. I recommend a group oriented toward teaching her to be assertive and express herself.
Dr. Jacobs: There is one other thing about this case that calls for caution. Dick, when you make the switch from individual counseling to getting her more into a group, be sure that she never feels that you have abandoned her. This is obviously important.
Dr. Mathews: My final task as a moderator is to say "thank you" to the panel. I am certain you could continue to discuss this case further, but the salient points seem to have been made. I also want to say "thank you" to all of you in the audience. I hope you have learned as much as I have and that in the future we will all be more sensitive and helpful to those who suffer from depression. BffiLIOGRAPHY Beach, Steven R., Evelyn E. Sandeen, and K. Daniel O'Leary. Depression in Marriage. New York: Guilford Press, 1990. Berger, Diane and Lisa. We Heard the Angels ofMadness: One Family's Struggle with Manic Depression. New York: William Morrow & Company, 1991.
106
DEALING WITH DEPRESSION
Brown, George W. and Tirril Harris. Social Origins of Depression: A Study of Psychiatric Disorder in Women. London: Tavistock, 1978. Davies, Brian (ed.). Depressive Illness: Some Research Studies. Springfield, IL: Charles C Thomas, 1972. DePaolo, J.R. and K.R. Ablow. How to Cope with Depression. New York: McGraw Hill, 1989. Flach, Frederic and Suzanne C. Drashi. The Secret Strength of Depression. Philadelphia: Lippincott, 1974. French, Alfred P. (ed.). Depression in Children and Adolescents. New York: Human Sciences Press, 1979. McGrath, Ellen et al. (eds.). Women and Depression: Risk Factors and Treatment Issues, Washington, DC: American Psychological Association, 1990. McKnew, Donald H., Yahraes Herbert, and Leon Cytryn. Why Isn't Johnny Crying? Coping with Depression in Children. New York: W.W. Norton, 1983. Neuger, Christie Cozad. "Women's Depression: Lives at Risk," Chapter 7 in Maxine Glaz and Jeanne Stevenson Moessner (eds.), Women in Trial and Transition. Minneapolis: Fortress Press, 1991, pp. 146-161. Preston, John. You Can Beat Depression. San Luis Obispo, California: Impact Publishers, 1989. Stark, Kevin D. Childhood Depression. New York: Guilford Press, 1990. Trad, Paul V. Infant and Childhood Depression. Somerset, NJ: Wiley and Sons, 1987. Wetzel, Janice Wood. The Clinical Handbook of Depression. New York: Gardner Press, 1984. Wurtzel, Elizabeth. Prozac Nation: Young and Depressed in America. Boston: Houghton Mifflin, 1994.
Chapter 8
Clergy Dealing with Depression Richard Dayringer
If you are a clergyperson who has read thus far in this book, you obviously have a serious interest in depression and want to help those who are depressed. I commend you because as you know by now, there is much work to do in this area. We pastoral counselors join forces with others in the helping professions such as counselors, marriage and family therapists, physicians, psychiatrists, psychologists, and social workers. The most encouraging fact about our work is that depression is one of the most treatable of mental illnesses, with 80 percent of even serious depressions responding favorably to the ministrations of the caregiver. As clergy, we want to develop a respected position on the treatment team. We are case finders through the open-door policy to homes that society has given us in our communities. Moreover, a study first reported in 1961 and replicated several times since (Joint Commission on Mental Illness and Health, 1961; Ellinson, Padilla, and Perkins, 1967; Veroff, Kulka, and Douvan, 1981), indicated that of all those people who have sought counseling for their problems, about 40 percent consulted a clergyperson first of all, i.e., before seeing a physician, psychiatrist, psychologist, marriage and family therapist, or social worker. This means that we clergy must be keen diagnosticians, skillful counselors, honest about our limitations, and expert at referral. If primary care physicians only recognize 50 to 60 percent of patients with depression (as has been estimated), I wonder what this figure would be for clergy? In the classification of mood disorders, the distinction between bipolar and unipolar disorders is one of the most important. People 107
108
DEALING WITH DEPRESSION
with bipolar disorders have had at least one manic episode, and most have also had major depressive episodes. Unipolar refers to a major or clinical depression without any manic episodes. In cases of unipolar depression, women outnumber men by about two to one (Weissman and Klerman, 1977). Dysthymia is similar to unipolar disorder and cyclothymia is similar to bipolar disorder except that both are a milder and more chronic form of depression. These two types of depression are more common and more appropriate for clergy to treat (see Appendix I). Medication is usually not needed. One of the most useful tools to help you with an accurate estimate of the severity of depression is the Beck Depression Inventory (BDI) (Burns, 1992, pp. 20-23). The long form has only 21 questions and can be administered quickly. It is the best researched of all the depression scales. A short form is available, but is not yet as well researched. The advisability of giving this test at the first interview and at least monthly or more often thereafter cannot be overstated. In addition to scoring and evaluating the total BDI score, be sure to pay attention to question 9, which asks about suicidal tendencies. A score of two or three on this question may indicate a person who is dangerously suicidal (more about this subject later). It is also important to look at question 20, which asks about health problems. A score of one, two, or three is your clue to refer this person to a physician for a checkup. Many treatable illnesses initially masquerade as depression. These must be ruled out by a physician. If depression is the proper diagnosis, the physician can also determine whether medicine will be helpful. A medical laboratory test for depression has been studied and sometimes used since the 1970s. It is called the- Dexamethasone Suppression Test (DST). This test attempts not only to establish a diagnosis for depression, but also to determine whether antidepressant medication will be helpful. However, for every three outpatients with an abnormal DST, only one is likely to have a true depression. The test is helpful only as one piece of evidence among several. It cannot be regarded as a screening test either to clinch the diagnosis of depression or to rule it out. It may be worth mentioning, in the interest of keeping clergy up to date, that some terms regarding depression have fallen into disuse
Clergy Dealingwith Depression
109
(DSM-IY, cf. Appendix I). Bipolar disorder has replaced the term "manic-depression." "Postpartum depression" is no longer viewed as a separate diagnosis. Rather, a diagnosis of major depression or bipolar disorder should specify if with postpartum onset, that is, the onset of the episode occurred within four weeks of the delivery of the baby. "Involutional melancholia" was formerly the proper term for diagnosing a depression with onset in midlife. Nowadays a diagnosis of major depression or bipolar disorder will suffice. Several caveats are in order. The first is in regard to the use of alcohol. Depressed people rarely resort to the uncontrolled use of alcohol, but alcoholics often get depressed (see Appendix I, pp. 140, 141). Second, approximately half of all those diagnosed with depression also meet the criteria for the diagnosis of anxiety disorder, and vice-versa, Family studies indicate that there is a familial relation between panic disorder and major depression. Both disorders share common risk factors, including family history, preponderance of females, lack of a satisfying relationship, marital separation, divorce, catastrophic life events, experiences of loss, inability to control one's environment, or disaster victims and combat veterans. However, in the majority of cases, one or the other syndrome is clearly dominant. Symptoms that distingish persons with depression from those with anxiety are those that describe the core syndromes of depression (loss of interest, suicidal behavior, psychomotorretardation, early-morning wakening, and pessimism) or anxiety (panic attacks, multiple autonomic symptoms, trouble falling asleep, and avoidance behavior) (Kendall and Watson, 1989, pp. 122, 336). Alexander Maclaren, one of the great expository preachers of nineteenth-century England, was one who apparently suffered from both anxiety and depression. "Always before a sermon or lecture in public, he would be overcome with nervous agitation. . . . And frequently after the service, waves of depression would engulf him, and he wanted to be alone" (Fuller, 1961, pp. 383-384). The third caveat is that depression is contagious (Heath, 1991). It is impossible for a caring person to be in the presence of a person who is depressed and not feel some of the sadness and despair. Clergy get depressed too! No less a stalwart figure than Harry Emerson Fosdick suffered from depression which included a period
110
DEALING WITH DEPRESSION
of hospitalization. In his autobiography (Fosdick, 1956, pp. 72-75) he interpreted the experience theologically by writing: "This whole horrid experience was one of the most important factors in my preparation for the ministry. . . . Without that experience I do not think I would have written one of my early books, The Meaning of Prayer." Many professional psychotherapists acknowledge that they are able to work with only a certain number of depressives at once. We clergy who counsel must deal with our tendency toward omnipotence honestly enough to admit that we have such limitations as well. Fourth, remember from the previous chapter, Pam's resentment about "uneducated ministers" who tried to help her. Clergy should recognize their counseling limitations and do only brief counseling of a few sessions (read four to six maximum). These, and especially longer term counseling, should be done under the supervision of a Fellow or Diplomate in the American Association of Pastoral Counselors, or some other professional therapist qualified to do supervision of the counseling of others. There is a God-given sign built into each of us bodily and emotionally: when the small hairs on the back of your neck stand out, it is a physiological warning that you are frightened by the person in your presence or by what is being said and you are too uncomfortable to be of further help. It is time to refer. Actually, I think clergy should usually counsel depressives in tandem with a physician who will look after their medical needs. One reason why it is so important to have depressive counselees evaluated by a physician is that there are as many as 40 physical disorders that are associated with depression (see Table 8.1). Obviously no amount of counseling, no matter how good, can cure these ailments. Another reason for working with a physician is that "more than 200 medications have been implicated in causing depression" (Zimmerman, 1993, p. 53) Some of the more commonly used drugs are listed in Table 8.2. Third, any depression that lasts more than six months may require medication to restore the body's chemical balance. David Bums (1992, pp. 447-448) summarizes the types of depressives most likely to benefit from drug therapy.
Clergy Dealing with Depression
111
TABLE 8.1 Medical Illnesses Associated with Depression"
Endocrine
Neurologic
Addison's disease Cushing's syndrome Hypo- and Hyperadrenocorticism Hypo- and Hyperthyroidism Hypo- and Hyperparathyroidism Carcinoid syndrome Pancreatic carcinoma Premenstrual syndrome Postpartum syndrome Hypoglycemia Hyperaldosteronism
Cerebral syphilis Encephalitis Epilepsy Huntington's disease Hydrocephalus Migraines Multiple sclerosis Cerebral neoplasm Cerebrovascular disease Narcolepsy Parkinson's disease Stroke (especially left-sided)
Withdrawal States Immunologic Rheumatoid arthritis Systemic lupus erythematosis Temporal arteritis Sjogren's syndrome
Alcohol Cocaine
Vitamin Deficiencies
HIV Mononucleosis
Folate Vitamin B Niacin Vitamin C Thiamine
Metabolic
Systemic
Acute intermittent prophyria Pernicious anemia Wilson's disease
Anemia Renal failure Systemic neoplasm
Infection
*MarkZimmerman, Diagnosing DSM-II-R, Psychiatric Disorders in Primary Care Settings. Philadelphia: Psychiatric Press, 1993, p. 55.
1. Functional impairment: being unable to carryon daily activities; 2. Organic symptoms: insomnia, agitation or retardation, worsening of symptoms in the morning, inability to feel cheered up by positive events; 3. Severe depression: lasting longer than six months;
112
DEALING WITH DEPRESSION
4. Identifiable beginning: symptoms substantially different from normal; 5. No long history of another psychiatric disorder; 6. Family history of depression; 7. Beneficial drug response in the past; 8. No tendency to complain and blame others; 9. No history of exaggerated sensitivity to drug side effects; 10. No history of hypochondriacal complaints.
TABLE 8.2 Commonly Used Medications Associated with Depression* Antihypertensives
Anticonvulsants
Clonidine Guanethidine Hydralazine Methyldopa Beta blockers Reserpine Thiazides Spironolactone
Phenytoin Carbemazepine
Sedatives
H2 Blockers
Alcohol Barbitu rates Benzodiazepines Chloral Hydrate
Cimetidine Ranitidine
Analgesics Ibuprofen Indomethacin Opiates
Stimulant Withdrawal
Steroids
Amphetamines Cocaine
Corticosteroids Oral Contraceptives Prednisone
Other Metoclopramide
Dopamine Agonists Amantadine Bromocriptine Levodpa *Mark Zimmerman, Diagnosing DSM-II/, Psychiatric Disorders in Primary Care Settings. Philadelphia: Psychiatric Press, 1993, p. 54.
Clergy Dealingwith Depression
113
Table 8.3 lists the medications most commonly used to treat depression. The tricyclics are called "antidepressants" and are the most widely used class of prescription drugs for depression. The MAO inhibitors are sometimes prescribed for chronically depressed persons who tend to eat or sleep excessively. Lithium carbonate is the medicine of choice for treating bipolar disorder, but since there is a narrow range between the therapeutic and the toxic level, periodic monitoring of the lithium level in the blood is required. With some frequency, bipolar patients will stop or decrease their lithium, either denying their need for it or wanting a boost from the "high" of mania, because the lithium decreases their energetic feelings and grandiosity (Holinger, 1985, p. 30). One recent seven-year follow-up study of formerly hospitalized bipolar patients found that about 40 percent of those receiving lithium, sometimes combined with other treatments, continue to experience marked emotional highs and lows as well as serious problems at work and home (Goldberg, 1991). Electroconvulsive therapy (ECT) has been the subject of controversy for many years. However, great strides have been made in this form of treatment for serious depression. "It is probably safer than treatment with tricyclic agents or lithium.... It also works faster" (Michels and Marzuk, 1993). ECT is sometimes the first choice of treatment for persons who are dangerously suicidal. Psychiatrists also use it frequently with those who cannot tolerate depressive medicines. The well-known writer and professor of pastoral care William E. Hulme recommends the efficacy of ECT out of his personal bout with depression (Hulme, 1994). In current use a general anesthetic and a muscle relaxant mutes the seizure. This is quite contrary to the way this treatment has been portrayed in the movies. Patients usually experience short-term loss of memory. Nevertheless, EeT is often avoided and frequently used only as a last resort. Fifth, in counseling with depressives, clergy should be careful about allowing the patient to ventilate too much. We need to either save the last few minutes of a session to intervene with more positive ideas or intersperse such interventions throughout the session, or both. Silences are appropriate to a degree and convey to·counselees your tolerance for their retarded thinking and speaking speed. However, prolonged silences are usually not helpful and only allow
~
~ ~
(A) 150-300 (M) 75-150
(A) 150-300 (M) 75-150
Cap 25, 50, mg Tab 10, 25, 50, 75, 100, 150 mg.
Cap 10, 25, 50, 75,100,150 mg. Soln 10 mglmL.
(A) 150-300 Tab 10,25, (M) 75-150 50 mg. Inj 12.5 mglmL. Cap (as pamoate) 75, 100, 125, 150 mg.
Desipramine Norpramin® Pertofrane® Various
Doxepin Adapin® Sinequan Various
Imipramine Tofranil® Janimine® Various
100-250d 100-1506
(A) 150-300 (M) 75-150
Cap 25, 50, 75 mg.
Tab 10, 25, 50 75,100,150 mg Inj 10 mg/mL.
TRICYCLICS Amitriptyline Elavil® Endep® Various
Clomipramine Anafranil
Dosage Forms
Drug Class Drug
Usual Daily Adult Dosage Range (Mg) (A) Acute (M) Maintenance
Moderate
High
110-250b
>200 b
Low
High
High
Sedation
100-160
c
125-250 b
Therapeutic Plasma Levels (J!glL)
Moderate
Moderate
Low
High
High
High
High
Moderate
High
High
Relative Frequency Of Side Effects Orthostatic AntiHypotension Cholinergic
Heterocyclic and Related Antidepressants Comparison Charta
TABLE 8.3
V.
Iooo....l Iooo....l
Tab 25, 50, 75 mg.
(A) 300-600 (M) 150-300
(A) 150-225 (M) 75-150
SPECIFIC SERTONIN REUPTAKE INHIBITORS Fluoxetine Cap 20 mg. (A) (M) Susp 4 mg/mL. Prozac®
20-80 5-40
TRIAZOLOPYRIDINES Tab 50, 100, 150 mg. (A) 200-600 Trazodone (M) 100-400 Desyrel® Various
DIBENZOXAZEPINES Amoxapine Tab 25,50, 100 Asendin® 150 mg. Various
TETRACYCLICS Maprotiline Ludiomil® Various
(A) 150-300 (M) 75-150
Cap 25,50,100 mg.
Trimipramine Surmontil®
c
c
c
200-300 c
c
None
High
Low
Moderate
Moderate
Very Low
70-260 c
30-60 20-40
(A) (M)
Tab 5,10 mg.
Protriptyline Vivactil®
Moderate
50-150 b
(A) 100-200 (M) 50-150
Cap 10, 25, 50 75mg Soln 2 mg/mL.
Nortriptyline Aventyl® Pamelor®
Very Low
Very Low
Low
Moderate
Moderate
Low
Moderate
None
Moderate
Low
Moderate
High
Moderate
Low
"'"'0\
Dosage Forms
c
c
c
c
Therapeutic Plasma Levels (Mg/L)
a. From references 148, 149, 151, 155, 156, 160, 165, 167-169. b. Includes active metabolites. c. Not well established. d. Obsessive-compulsive disorder. e. Maj or depression.
(A) 300-450 (M) 150-300
CHLOROPROPIOPHENONES Bupropion Tab 75,100, mg. Wellbutrin®
10-50 C
50-200
-
Tab 50, 100 mg.
Sertraline Zoloft®
Paroxetine Paxil® (Investi gationalSmith Kline Beecham)
-
SPECIFIC SEROTONIN REUPTAKE INHIBITORS (continued) Fluvoxamine 150-300 c (Investi gationalSolvay, Upjohn)
Drug Class Drug
Usual Daily Adult Dosage Range (Mg) (A) Acute (M) Maintenance
TABLE 8.3 (continued)
None
None
Very Low
None
Sedation
None
None
Very Low
None
None
None
Very Low
None
Relative Frequency Of Side Effects Orthostatic AntiHypotension Cholinergic
Clergy Dealingwith Depression
117
counselees to become more upset and preoccupied with their internal critical thoughts, or to decide that the counselor does not know what to say or do to help. Nondirective responses convey the counselor's agreement with the counselee's hopelessness and should be used sparingly. Sixth, the usual ethics of caregiving should be maintained. This would include such things as respecting the person, avoiding paternalism, maintaining confidentiality, avoiding harm, not attempting to work beyond one's ability, and so forth. We can assume then, based on good evidence, that clergy will interview those who are depressed (see Appendix II for suggestions). Much of the time the depressed will seek us out and ask to talk. We clergy will also recognize some of those in our care or acquaintance who exhibit depressive symptoms and make pastoral visits. Many clergy will make referrals as soon as possible. But since there is no social stigma attached to talking with clergy, as is still too often the case with psychiatrists and other therapists, many depressives will resist referral. Therefore, many clergy by choice and preparation or by default find themselves counseling those who are depressed. That is what this book is all about. Choose one of the theories of therapy set forth in the previous chapters that fits your personality, or even an eclectic selection of methods from two or more of them, and proceed. Work with a physician as has been suggested, and arrange a formal relationship with a supervisor that you will see regularly. Numerous research studies (many of them have been cited in this book) indicate that both psychotherapy alone, and especially psychotherapy combined with drug therapy, are effective in relieving depression. One other frequent issue among people who are depressed is the problem of suicide. Studies indicate that of all depressives, those with bipolar disorder have higher rates of suicide attempts (Schwartz et al., 1987, p. 1368). According to the U.S. Center for Disease Control, suicide is responsible for one death every 20 minutes, and the median age of the suicide victim has fallen to less than 40. The most commonly used method of suicide in the U.S. (39 percent) is guns (though women are more likely than men to use something less defacing). Another very interesting but as yet unexplained phenomenon is that U.S. men between the ages of 15 to 24 are killing themselves at a rate
118
DEALING WITH DEPRESSION
50 percent higher than they were in 1970. The suicide rate for young women increased only two percent since 1970. This makes suicide the second leading cause of death among young people in that age group (Office of Disease Prevention and Health Promotion, 1988, p. 312). The Bible records seven suicides in the Hebrew Scriptures (Abimelech and his armor-bearer, Saul and his armor-bearer, Zimri, Ahithophel, Samson, and one [Judas] in the Christian Scriptures). But more helpful to the pastoral counselor are the five preventions of suicide in the Bible (see Table 8.4). Judeo-Christian theology understands God as the source of life, and therefore assumes that life is a gift, a trust, not private property. "For your own lifeblood I will surely require a reckoning" (Gen. 9:5). Further, "We do not live to ourselves, and we do not die to ourselves" (Rom. 14:7). Table 8.5 gives a variety of questions that can be asked of a suicidal person. At some point in the interview, I usually ask depressed persons, "How bad do things get for you?" Many begin to cry, if they have not already, as they begin to tell me. Then I ask, "Have you thought of hurting yourself?" If their answer is affirmative, I ask, "How would you do it; what is your plan?" All this helps me to evaluate the risk of suicide. If there is an active plan for suicide, and even more if the means are available, the risk is much more dangerous than for persons who just wish they were dead. Next, I ask if there are any reasons why this plan will never be
TABLE 8.4 Suicide Preventions in the Bible Character
Scripture
Moses
Numbers 11
Method Support and practical advice
Job
Renewal of relationship
David
Psalm 22
Renewal of faith in God
Elijah
I Kings 18-19
Protected withdrawal and nurturance
Jonah
Jonah
Protected withdrawal and guidance
Job
Clergy Dealingwith Depression
119
TABLE 8.5 Questions to Ask a Suicidal Patient* Open-ended questions for the initial phase of evaluation.
1. Do you feel depressed, down in the dumps, sad? 2. How bad does it get? Are you feeling trapped? Do you feel nothing will help you?
3. What do you see in the future for yourself? Where do you think you will be in a year?
4. What do you think about suicide or death? 5. Does anyone know how you feel and that you have thoughts of hurting yourself? Affirmative answers to the following questions signify a relatively low suicide risk.
6. Are you feeling so angry toward someone that you "want to get back at them" or show them that you were serious when you threatened to hurt yourself? 7. Is there anything that will prevent you from harming yourself? If so, what are your reasons for living? 8. Do you believe there is a way out of your problem? Affirmative answers to the following questions indicate a high suicide risk.
9. Do you feel like giving up? 10. Are you having thoughts or feelings of hurting yourself now? 11. Do you think you are a burden to your loved ones and that you would be better off dead? Affirmative answers to the following questions indicate a very high suicide risk in the near future.
12. Have you been giving away your precious things lately, like old letters, mementos, etc.? 13. Have you recently taken a life insurance policy? 14. Have you recently made a will or changes in the existing will? 15. Have you written goodbye letter(s}? 16. Have you decided how you would harm yourself? 17. Have you recently bought any lethal weapon(s}? 18. Do you wish you were dead and were united with your loved one? At the end of interview.
19. Did discussing and talking about the problems in your present life situation make you feel better? (Affirmative answer is a good prognostic sign and indicates low risk of suicide.) 20. Does suicide still seem to be the only answer to your problem? (Affirmative answer indicates very high risk of suicide in the near future.) *Bhatia, S., M.H. Khan, and A. Sharma. "Suicide Risk: Evaluation and Management." American Family Practitioner. 34(3} Sept. 1986, p. 171.
120
DEALING WITH DEPRESSION
completed. Most depressives will have a reason or two. I try to help them add another reason or two to the list. They fail to recognize the powetful emotional effect their suicide will have on others, particularly children and other family members. Then I utilize the "contract for life" which originated (I believe) out of Transactional Analysis. I ask them to promise to phone me or contact me before they make any attempt on their life. It is important to get this promise from their Adult ego state, not their Child, which might be teasing. I ask them to shake hands with me to confirm our agreement. If you utilize this technique, you will receive an occasional, desperate phone call and feel rather helpless yourself, but this is our opportunity to save a life. On the other hand, a recent survey found that one out of five therapists will lose a client in the course of their clinical practice. Family members' participation in protecting a suicidal person is vital. I believe the ethical decision to break confidentiality in cases of suicide (or homicide, contagion, or risk to the lives of others) is justifiable. People who have a definite plan to commit suicide and the full intention to do it view suicide as a solution, not a problem. In fact, their emotional state may lighten up after the decision is made. Such people usually need to be hospitalized for their safety. This can be done by taking or sending the person to the hospital Emergency Room. The assistance of the person's family and physician is often essential. There are also many myths and misconceptions about suicide. Table 8.6 summarizes these along with their refutations. One other thing to keep in mind in regard to suicide is that certain factors raise the potential risk that a given person may commit suicide. A list of such items would include: a recent suicide in the community, the family, or among acquaintances; a family history of suicide; white race; 'male; advanced age; living alone; alcoholism; drug addiction; suicidal threats; previous suicidal attempts; and/or giving away precious belongings (Stevens, 1994, p. 54). After a suicide attempt, the pastoral counselor will want to discuss the following questions: 1. Is the counselee glad to be alive? 2. Did the counselee think that he/she would be rescued? 3. Did the counselee believe that the chosen method was lethal?
Clergy Dealingwith Depression
121
4. Is the precipitating crisis resolved? 5. Does the counselee say that he/she will attempt suicide again? 6. Do family members indicate a covert wish that the counselee die? In my counseling with well over 100 people who were depressed (some of them also suffered from anxiety), I have developed a number of rather commonplace topics which I discuss and suggest to them at various points in therapy. I suggest that they TALK to a spouse, pastor, or trusted friend about their feelings or emotions. I remind them that God created us so that we could express our sad inner feelings by CRYING. Some men may need permission to cry. We can express our happy inside feelings by LAUGHING. I encourage people to put themselves with humorous people, books, movies, and TV programs, and to try to be the first to laugh, the one who laughs loudest, and the last to stop laughing. I recommend 30 minutes of vigorous, aerobic EXERCISE three times a week, to those whose physicians approve. I prescribe eight hours of SLEEP nightly, occasional 15- to 30-minute naps, and the practice of the "sabbath principle." I encourage people to remember their DREAMS by writing notes upon awakening and sharing their dreams with their spouse or a friend. I recommend hard WORK around the house that will likely make them sweat and think they are too important to have to do such work. I tell them that if they have forgotten how to PLAY (and many adults have), they should place their body on the floor of their home and if a child or pet is present, they will soon find them and begin to teach them to play. I also recommend prayer and meditation, including such scripture passages as Lamentations 3:1-3, 31-33; Psalms 37:7 and especially Psalm 88; and Philippians 4:4-9,11. I also recommend use of the "Pleasant Events Schedule" (MacPhillamy and Lewinsohn, 1982, pp. 376-380). It is included in Appendix ill. This paper and pencil inventory will remind people of a number of events they may have forgotten which they enjoy or formerly enjoyed. Depression is a prevalent and complicated problem. Clergy will be called upon to help. My prayer is that by using this book, clergy may be enabled to relieve many persons who suffer from depression.
122
DEALING WITH DEPRESSION TABLE 8.6 Some Myths about Suicide
1. Mentioning suicide may give a person the idea. Talking frankly about suicide can prevent a person from doing it, and suicidal people already have the idea. 2. People who discuss suicide will not commit the act. The fact is that up to three-quarters of those who take their lives have communicated the intent beforehand, perhaps as a cry for help, perhaps to taunt. On the other hand, the vast majority of people who contemplate suicide do not actually attempt to kill themselves. 3. Suicide may be committed without warning. The falseness of this belief is readily indicated by the preceding statement. There seem to be many warnings, such as the person's saying that the world would be better off without him or her, or making unexpected and inexplicable gifts to others, often of his or her most valued possessions. 4. Only people of a certain class commit suicide. Suicide is actually neither the curse of the poor nor the disease of the rich. People in all classes commit suicide. 5. Membership in a particular religious group is a good predictor that a person will not consider suicide. It is mistakenly thought that the strong Catholic prohibition against suicide makes the risk that Catholics will take their lives much lower. This is not supported by the evidence, perhaps because an individual's formal religious indentification is not always an accurate index of true beliefs. 6. The motives for suicide are easily established. The truth is that we have only the poorest understanding of why people commit suicide. For example, the fact that a severe financial setback precedes a suicide does not mean that the setback adequately explains the suicide. 7. All who commit suicide are depressed. This fallacy may account for the tragic fact that signs of impending suicide are overlooked because the person is not depressed. Some experts believe that many of the people who take their lives are not depressed. In fact, some people appear calm and at peace with themselves after having decided to kill themselves. 8. A person with a terminal physical illness is unlikely to commit suicide. A person's awareness of impending death does not preclude suicide. Perhaps the wish to end their own suffering or that of their loved ones impels many to choose the time of their death. 9. To commit suicide is insane. Although most suicidal persons are very unhappy, most do appear to be completely rational and in touch with reality. 10. A tendency to commit suicide is inherited. Since suicides often run in families, the assumption is made that the tendency to think in terms of self-annihilation is inherited. There is no evidence for this. 11. Suicide is influenced by seasons, latitude, weather fronts, barometric pressure, humidity, precipitation, cloudiness, wind speed, temperature, and days of the week. There is no good data to substantiate any of these myths.
Clergy Dealingwith Depression
123
12. Suicide is influenced by cosmic factors such as sunspots and phases of the moon. No evidence confirms this. 13. Improvement in emotional state means lessened risk of suicide. The fact is that people often commit the act after their spirits begin to rise; this appears to be especially true of depressed patients. 14. Suicide is a lonely event. Although the debate whether to commit suicide is waged within the individual's head, deep immersion in a frustrating, hurtful relationship with another person-a spouse, a child, a lover, a colleague-may be a principal cause. 15. Suicidal people clearly want to die. Most people who commit suicide appear to be ambivalent about their own deaths. 16. Suicidal people are beyond help. Actually, the crisis period lasts for only a limited time. A person can get help and improve, but suicidal crises can reoccur. 17. It's not suicide if there is no suicide note. Only about one in four of those who commit suicide leave notes.
BIBLIOGRAPHY Ban, Thomas A. (ed.) Prevention and Treatment of Depression. Baltimore: University Press, 1981. Blazer, Dan G. Depression in Late Life. St. Louis: Mosby, 1982. Burns, David D. Feeling Good: The New Mood Therapy. New York: Morrow, 1980; New York: Avon Books, 1992. Chaisson-Steward, G. Maureen (ed.) Depression in the Elderly. Somerset, NJ: Wiley and Sons, 1985. Dayringer, Richard. God Caresfor You. Nashville: Broadman Press, 1983. Dayringer, Richard. The Heart of Pastoral Counseling. Grand Rapids, MI: Zondervan, 1989. Ellinson, 1., E. Padilla and M. Perkins. Public Image of Mental Health Services. New York: Mental Health Materials Center, 1967. Fann, William E. (ed.) Phenomenology and Treatment of Depression. New York: Spectrum Publishers, 1977. Flach, Frederic F. and Drashi, Suzanne C. The Nature and Treatment of Depression. New York: John Wiley and Sons, 1975. Fosdick, Harry Emerson. The Living of These Days. New York: Harper & Brothers,1956. Frankel, Arthur 1. Four Therapies Integrated: A Behavioral Analysis of Gestalt, I'A. and Ego Psychology. Englewood Cliffs, NJ: Prentice-Hall, Inc., 1984. Fuller, David Otis (ed.) Valiantfor the Truth: A Treasury ofEvangelical Writings. New York: McGraw-Hill, 1961. Gilbert, Paul. Depression: The Evolution of Powerlessness. New York: Guilford Press, 1992.
124
DEALING WITH DEPRESSION
Goldberg, Joseph F. "Manic Depression: Success Story Dims," Science News, 139:410, May 1991. Greist, John H. and James W. Jefferson. Depression and Its Treatment. Washington, DC: American Psychiatry Press, 1984. Heath, Sheldon. Dealing with the Therapist's Vulnerability to Depression. New York: Aronson, 1991. Holinger, Paul. Pastoral Care ofSevere Emotional Disorders. New York: Irvington Publishers, 1985. Hulme, William E., "Ministry in Depression," Journal of Pastoral Care, 48(1):91-94, Spring, 1994. Jamison, Kay Redfield. Touched with Fire: Manic-Depressive Illness and the Artistic Temperament. New York: Free Press, 1993. Jamison, Kay Redfield and Frederick Goodwin. Manic-Depressive Illness. New York: Oxford University Press, 1990. Joint Commission on Mental Illness and Health, Action for Mental Health. New York: Basic Books, 1961. Kendall, Philip C. and David Watson (eds.) Anxiety and Depression. New York: Academic Press, 1989. Klein, Marjorie H., David J. Kupfer and M. Tracie Shea (eds.) Personality and Depression. New York: Guilford Press, 1993. Kline, Nathan S. From Sad to Glad. New York: Ballantine Books, 1974. Kramer, Peter D. Listening to Prozac: A Psychiatrist Explores Antidepressant Drugs and the Remaking ofSelf. New York: Viking, 1993. Leonard, Calista. Understanding and Preventing Suicide. Springfield, IL: Charles C Thomas, 1967. MacPhillamy, Douglas J. and Peter M. Lewinsohn. "The Pleasant Events Schedule: Studies on Reliability, Validity, and Scale Intercorrelation," Journal of Counseling and Clinical Psychology, 50(3):363-380, 1982. Michels, Robert and Peter M. Marzuk. "Progress in Psychiatry," New England Journal ofMedicine, 329(9):628-633, August 26, 1993. Nolen, William A., Joseph Zohar, Stephen P. Roose and Jay D. Amsterdam, Refactory Depression: Current Strategies and Future Directions. Somerset, NJ: Wiley & Sons, 1994. Office of Disease Prevention and Health Promotion, U.S. Public Health Service, Disease Prevention/Health Promotion: The Facts. Palo Alto, CA: Bull Publishing Co., 1988, p. 312. Oster, Gerald D. and Janice E. Oster. Understanding and Treating Depressed Adolescents and Their Families. New York: John Wiley and Sons, 1990. Papolos, Demitri and Janice Papolos. Overcoming Depression. New York: Harper & Row, 1987. Plath, Sylvia. The Bell Jar. New York: Bantam Books, 1972. Rippere, Vicky and Ruth Williams (eds.) Wounded Healers: Mental Health Workers Experiences ofDepression. Somerset, NJ: Wiley and Sons, 1985. Rush, A. John. Short-Term Psychotherapies for Depression: Behavioral, Inter-
Clergy Dealing with Depression
125
personal, Cognitive and Psychodynamic Approaches. New York: Guilford Press, 1982. Schwartz, Jeffrey M., Lewis R. Baxter, John C. Mazziotta, Robert H. Gerner, and Michael E. Phelps. "The Differential Diagnosis of Depression," Journal of the American Medical Association, 258(10):1368-1374, September 11, 1987. Stevens, Nancy. "Guidelines for the Diagnosis and Treatment of Major Depression," Journal of the American Board ofFamily Practice. 7(1):49-54, 1994. Task Force on DSM N, Diagnostic and Statistical Manual ofMental Disorders. (4th edition). Washington, DC: American Psychiatric Association, 1994. Veroff, Joseph, Richard A. Kulka and Elizabeth Douvan. Mental Health in America: Patterns ofSeeking Helpfrom 1957-1976. New York: Basic Books, 1981. Weisman, M.M. and Klerman, G.C. "Sex Differences in the Epidemiology of Depression," Archives of General Psychiatry, 34:98-111,1977. Wolman, Benjamin B. and George Stricker (eds.) Depressive Disorders: Facts, Theories, and Treatment Methods. New York: John Wiley & Sons, 1990. Yapko, Michael D. When Living Hurts: Directivesfor Treating Depression. New York: BrunnerlMazel Publishers, 1988. Yapko, Michael D. Hypnosis and the Treatment of Depression. New York: BrunnerlMazel Publishers, 1992. Zimmerman, Mark. Diagnosing DSM-III-R Psychiatric Disorders in Primary Care Settings. Philadelphia: Psychiatric Press, 1993.
This page intentionally left blank
Appendix I MOOD DISORDERS*
Depressive Disorders Major Depressive Episode A. At least five of the following symptoms have been present during the same two-week period and represent a change from previous functioning; at least one of the symptoms is either (1) depressed mood or (2) loss of interest or pleasure. (1) depressed mood most of the day, nearly every day, as directed by either subjective report (e.g., feels sad or empty) or observation made by others (e.g., appears tearful). Note: in children and adolescents, can be irritable mood. (2) markedly diminished interest or pleasure in all, or almost all, activities most of the day, nearly every day (as indicated either by subjective account or observation made by others) (3) significant weight loss or weight gain when not dieting (e.g., more than 5% of body weight in a month), or decrease or increase in appetite nearly every day. Note: in children, consider failure to make expected weight gains. (4) insomnia or hypersomnia nearly every day (5) psychomotor agitation or retardation nearly every day (observable by others, not merely subjective feelings of being slowed down) (6) fatigue or loss of energy nearly every day (7) feelings of worthlessness or excessive or inappropriate guilt (which may be delusional) nearly every day (not merely self-reproach or guilt about being sick) *Task Force on DSM-IV, DSM-IV Draft Criteria (3-1-93), Washington, DC: American Psychiatric Association, 1993, pp. J:1-16. Used with permission.
127
128
DEALING WITH DEPRESSION
(8) diminished ability to think or concentrate, or indecisiveness, nearly every day (either by subjective account or as observed by others) (9) recurrent thoughts of death (not just fear of dying), recurrent suicidal ideation without a specific plan, or a suicide attempt or a specific plan for committing suicide B. The symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning. C. Not due to the direct effects of a substance (e.g., drugs of abuse, medication) or a general medical condition (e.g., hypothyroidism). D. Not occuning within two months of the loss of a loved one (except if associated with marked functional impairment, morbid preoccupation with worthlessness, suicidal ideation, psychotic symptoms, or psychomotor retardation) Codes for Major Depressive Episode (code in fifth digit):
.xl - Mild: Few, if any, symptoms in excess of those required to make the diagnosis and symptoms result in only minor impairment in occupational functioning or in usual social activities or relationships with others. .x2 - Moderate: Symptoms or functional impairment between "mild" and "severe"
.x3 - Severe without Psychotic Features: Several symptoms in excess of those required to make the diagnosis, and symptoms markedly interfere with occupational functioning or with usual social activities or relationships with others. .x4 - With Psychotic Features: Delusions or hallucinations. If possible, specify whether the psychotic features are mood-congruent or mood-incongruent:
- Mood-congruent Psychotic Features: Delusions or hallucinations whose content is entirely consistent with the typical depressive themes of personal inadequacy, guilt, disease, death, nihilism, or deserved punishment. - Mood-incongruent Psychotic Features: Delusions or hallucina-
Appendix L·Mood Disorders
129
tions whose content does not involve typical depressive themes of personal inadequacy, guilt, disease, death, nihilism, or deserved punishment. Included here are such symptoms as persecutory delusions (not directly related to depressive themes), thought insertion, thought broadcasting, and delusions of control . .x5 - In Partial Remission: Intermediate between "In Full Remission" and "Mild," and no previous Dysthymic Disorder. (If the Major Depressive Episode was superimposed on Dysthymic Disorder, the diagnosis of Dysthymic Disorder alone is given once the full criteria for a Major Depressive Episode are no longer met.)
.x6 - In Full Remission: During the past six months no significant signs or symptoms of the disturbance . .x7 - Unspecified
296.2xMajor Depressive Disorder, Single Episode A. Presence of a major depressive episode. B. The major depressive episode is not better accounted for by Schizoaffective Disorder, and is not superimposed on Schizophrenia, Schizophreniform Disorder, Delusional Disorder, or Psychotic Disorder NOS. C. Has never had a manic episode or unequivocal hypomanic episode. Note: this exclusion does not apply if all of the manic or hypomanic episodes are substance- or treatment-induced.
296.3xMajor Depressive Disorder, Recurrent A. Two or more major depressive episodes. Note: To be considered separate episodes, there must be an interval of at least two months without significant symptoms of depression. B. The major depressive episodes are not due to the direct effects of a substance (e.g., drugs of abuse, medication) or a general medical condition (e.g., hypothyroidism); are not better accounted for by Schizoaffective Disorder, and are not superimposed on Schizophrenia, Schizophreniform Disorder, Delusional Disorder, or Psychotic Disorder NOS.
130
DEALING WITH DEPRESSION
c. Has
never had a manic episode or unequivocal hypomanic episode. Note: this exclusion does not apply if all of the manic or hypomanic episodes are substance- or treatment-induced. 300.4 Dysthymic Disorder
A. Depressed mood (or can be irritable mood in children and adolescents) for most of the day, for more days than not, as indicated either by subjective account or observation made by others, for at least two years (one year for children and adolescents). B. Presence, while depressed, of at least three of the following: (1) low self-esteem or self-confidence, or feelings of inadequacy (2) feelings of pessimism, despair, or hopelessness (3) generalized loss of interest or pleasure (4) social withdrawal (5) chronic fatigue or tiredness (6) feelings of guilt, brooding about the past (7) subjective feelings of irritability or excessive anger (8) decreased activity, effectiveness, or productivity (9) difficulty in thinking reflected by poor concentration, poor memory, or indecisiveness C. During the two-year period (one-year for children or adolescents) of the disturbance, the person has never been without the symptoms in A and B for more than two months at a time. D. No major depressive episode during the first two years of the disturbance (one year for children and adolescents); i.e., not better accounted for by chronic Major Depressive Disorder, or Major Depressive Disorder in partial remission. Note: There may have been a previous major depressive episode provided there was a full remission (no significant signs or symptoms for six months) before development of the Dysthymic Disorder. In addition, after these two years (one year in children or adolescents) of Dysthymic Disorder, there may be superimposed episodes of Major Depressive Disorder in which cases both disgnoses may be given.
Appendix L" Mood Disorders
131
E. Has never had a manic episode or an unequivocal hypomanic episode. F. Does not occur exclusively during the course of a chronic psychotic disorder, such as Schizophrenia or Delusional Disorder. G. Not due to the direct effects of a substance (e.g., drugs of abuse, medication) or a general medical condition (e.g., hypothyroidism). Specify if: early onset: if onset before age 21 late onset: if onset age 21 or older
311 Depressive Disorder Not Otherwise Specified This category includes disorders with depressive features that do not meet the criteria for any specific Depressive Disorder, Adjustment Disorder with Depressed Mood, or Adjustment Disorder with Mixed Anxiety and Depressed Mood. Examples include: (1) premenstrual dysphoric disorder: in most menstrual cycles during the past year, symptoms (e.g., markedly depressed mood, marked anxiety, marked affective lability, decreased interest in activities) regularly occurred during the last week of the luteal phase (and remitted within a few days of the onset of menses). These symptoms must be severe enough "to markedly interfere with work, school, or usual activities." (2) minor depressive disorder: a disorder with episodes of two weeks of depressive symptoms but with fewer than the five items required for Major Depressive Disorder (3) recurrent brief depressive disorder: a disorder with depressive episodes lasting from two days up to two weeks, occurring at least once a month for 12 months (not associated with the menstrual cycle) (4) postpsychotic depression of schizophrenia: a major depressive episode occurring during the residual phase of Schizophrenia (5) a major depressive episode superimposed on Delusional Disorder, Psychotic Disorder NOS, or the active phase of Schizophrenia
132
DEALING WITH DEPRESSION
(6) situations in which the clinician has concluded that a depressive disorder is present but is unable to determine whether it is primary, due to a general medical condition, or substance-induced
BipolarDisorders Manic Episode A. A distinct period of abnormally and persistently elevated, expansive, or irritable mood, lasting at least one week (or any duration if hospitalization is necessary). B. During the period of mood disturbance, at least three of the following symptoms have persisted (four if the mood is only irritable) and have been present to a significant degree: (1) inflated self-esteem or grandiosity (2) decreased need for sleep (e.g., feels rested after only three hours of sleep) (3) more talkative than usual or pressure to keep talking (4) flight of ideas or subjective experience that thoughts are racing (5) distractibility (i.e., attention too easily drawn to unimportant or irrelevant external stimuli) (6) increase in goal-directed activity (either socially, at work or school, or sexually) or psychomotor agitation (7) excessive involvement in pleasurable activities that have a high potential for painful consequences (e.g., the person engages in unrestrained buying sprees, sexual indiscretions, or foolish business investments) C. The mood disturbance is sufficiently severe to cause marked impairment in occupational functioning or in usual social activities or relationships with others, or to necessitate hospitalization to prevent harm to self or others. D. Not due to the direct effects of a substance (e.g., drugs of abuse, medication) or a general medical condition (e.g., hyperthyroidism). Note: Manic episodes that are clearly precipitated by somatic antide-
Appendix L' Mood Disorders
133
pressant treatment (e.g., medication, electroconvulsive therapy, light therapy) should not count towards a diagnosis of Bipolar I Disorder.
Codes for Manic Episode (code in fifth digit): .xl - Mild: Meets minimum symptom criteria for a manic episode . .x2 - Moderate: Extreme increase in activity or impairment in judgment. .x3 - Severe, without Psychotic Features: Almost continual supervision required in order to prevent physical harm to self or others.
- Mood-congruent psychotic features: Delusions or hallucinations whose content is entirely consistent with the typical manic themes of inflated worth, power, knowledge, identity, or special relationship to a diety or famous person. - Mood-incongruent psychotic features: Delusions or hallucinations whose content does not involve typical manic themes of inflated worth, power, knowledge, identity, or special relationship to a diety or famous person. Included are such symptoms as persecutory delusions (not directly related to grandiose ideas or themes), thought insertion, and delusions of being controlled. .x5 - In Partial Remission: Full criteria were previously, but are not currently, met; some signs or symptoms of the disturbance have persisted. .x6 - In Full Remission: Full criteria were previously met, but there have been no significant signs or symptoms of the disturbance for at least six months .
.xO - Unspecified.
Hypomanic Episode A. A distinct period of sustained elevated, expansive, or irritable mood, lasting throughout four days, that is clearly different from the usual nondepressed mood. B. During the period of mood disturbance, at least three of the
134
DEALING WITH DEPRESSION
following symptoms have persisted (four if the mood is only irritable) and have been present to a significant degree: (1) inflated self-esteem or grandiosity (2) decreased need for sleep (e.g., feels rested after only three hours of sleep (3) more talkative than usual or pressure to keep talking (4) flight of ideas or subjective experience that thoughts are racing (5) distractibility (i.e., attention too easily drawn to unimportant or irrelevant external stimuli) (6) increase in goal-directed activity (either socially, at work or school, or sexually) or psychomotor agitation (7) excessive involvement in pleasurable activities that have a high potential for painful consequences (e.g., the person engages in unrestrained buying sprees, sexual indiscretions, or foolish business investments) C. The episode is associated with an unequivocal change in functioning that is uncharacteristic of the person when not symptomatic. D. The disturbance in mood and the change in functioning are observable by others. E. The episode is not severe enough to cause marked impairment in social or occupational functioning, or to necessitate hospitalization, and there are no psychotic features. F. Not due to the direct effects of a substance (e.g., drugs of abuse, medication) or a general medical condition (e.g., hyperthyroidism). Note: Hypomanic episodes that are clearly precipitated by somatic antidepressant treatment (e.g., medication, electroconvulsive therapy, light therapy) should not count towards a diagnosis of Bipolar II Disorder. 296. Ox BipolarI Disorder, Single Manic Episode A. Presence of only one manic episode and no past major depressive episodes. B. The manic episode is not better accounted for by Schizoaffec-
Appendix 1· Mood Disorders
135
tive Disorder, and is not superimposed on Schizophrenia, Schizophreniform Disorder, Delusional Disorder, or Psychotic Disorder NOS.
296.4x BipolarI Disorder, Most Recent Episode Hypomanic A. Currently (or most recently) in a hypomanic episode. B. There has previously been at least one manic episode. Note: To be considered separate episodes, there must be an interval of at least two months without significant symptoms of mania or hypomania, or a change in polarity. C. The mood episodes in A and B are not better accounted for by Schizoaffective Disorder, and are not superimposed on Schizophrenia, Schizophreniform Disorder, Delusional Disorder, or Psychotic Disorder NOS.
296.4x BipolarI Disorder, Most Recent Episode Manic A. Currently (or most recently) in a manic episode. B. Either (1) or (2); (1) there has previously been at least one major depressive episode (2) there has previously been at least one hypomanic or manic episode Note: Tobe considered separate episodes, there must be an interval of at least two .months without significant symptoms of mania or hypomania or a change in polarity. C. The mood episodes in A and B are not better accounted for by Schizoaffective Disorder, and are not superimposed on Schizophrenia, Schizophreniform Disorder, Delusional Disorder, or Psychotic Disorder NOS.
296.6x BipolarI Disorder, Most Recent Episode Mixed A. Currently (or most recently) in a mixed episode, i.e., for every day during at least a one-week period, the criteria for a major
136
DEALING WITH DEPRESSION
depressive episode (except for duration) and a manic episode are both met. B. Either (1) or (2); (1) there has previously been at least one major depressive episode (2) there has previously been at least one hypomanic or manic episode Note: To be considered separate episodes, there must be an interval of at least two months without significant symptoms of mania or hypomania or a change in polarity. C. The mood episodes in A and B are not better accounted for by Schizoaffective Disorder, and are not superimposed on Schizophrenia, Schizophreniform Disorder, Delusional Disorder, or Psychotic Disorder NOS.
296.5x BipolarI Disorder, Most Recent Episode Depressed A. Currently (or most recently) in a major depressive episode. B. There has previously been at least one manic episode. C. The mood episodes in A and B are not better accounted for by Schizo affective Disorder, and are not superimposed on Schizophrenia, Schizophreniform Disorder, Delusional Disorder, or Psychotic Disorder NOS.
296.7BipolarI Disorder, Most Recent Episode Unspecified A. Currently (or most recently) meets criteria for a manic, hypomanic or major depressive episode except for duration. B. There has previously been at least one manic episode. C. The mood symptoms in A cause clinically significant distress or impairment in social, occupational, or other important areas of functioning. D. The mood symptoms in A and B are not better accounted for
Appendix L· Mood Disorders
137
by Schizoaffective Disorder, and are not superimposed on Schizophrenia, Schizophreniform Disorder, Delusional Disorder, or Psychotic Disorder NOS.
296.89BipolarII Disorder (Recurrentmajor depressive episodes with hypomania) A. One or more major depressive episodes. B. Presence of at least one hypomanic episode. Note: Hypomanic episodes that are clearly precipitated by somatic antidepressant treatment (e.g., medication, electroconvulsive therapy, light therapy) should not count toward a diagnosis of Bipolar II Disorder. C. Has never had a manic episode. D. The mood symptoms in A and B are not better accounted for by Schizoaffective Disorder, and are not superimposed on Schizophrenia, Schizophreniform Disorder, Delusional Disorder, or Psychotic Disorder NOS. Specify Current or Most Recent Episode:
Hypomanic: if currently (or most recently) in a hypomanic episode Depressed: if currently (or most recently) in a major depressive episode
301.13 Cyclothymic Disorder A. For at least two years (one year for children and adolescents), presence of numerous periods with hypomanic symptoms and numerous periods with depressed mood or loss of interest or pleasure (that did not meet criteria for a major depressive episode). B. During the above two-year period (one year in children and adolescents), the person has not been without the symptoms in A for more than two months at a time. C. Has never met criteria for a major depressive episode. D. No clear evidence of a manic episode during the first two years of the disturbance. Note: After the initial two years (one
138
DEALING WITH DEPRESSION
year in children or adolescents) of Cyclothymic Disorder, there may be superimposed manic episodes in which case both Bipolar I Disorder and Cyclothymic Disorder may be diagnosed. E. The symptoms in A are not better accounted for by Schizoaffective Disorder, and are not superimposed on Schizophrenia, Schizophreniform Disorder, Delusional Disorder, or Psychotic Disorder NOS. F. Not due to the direct effects of a substance, (e.g., drugs of abuse, medication) or a general medical condition (e.g., hyperthyroidism).
296.80 Bipolar Disorder Not Otherwise Specified This category includes disorders with bipolar features that do not meet criteria for any specific bipolar disorder. Examples include: (1) recurrent hypomanic episodes without intercurrent depressive symptoms (2) a manic episode superimposed on Delusional Disorder, residual Schizophrenia, or Psychotic Disorder NOS (3) situations in which the clinician has concluded that a bipolar disorder is present but is unable to determine whether it is primary, due to a general medical condition, or substance-induced
293.83 Mood Disorder Due to a General Medical Condition A. A prominent and persistent disturbance in mood characterized by either (or both) of the following: (1) depressed mood or markedly diminished interest or pleasure in all, or almost all, activities (2) elevated, expansive, or irritable mood B. There is evidence from the history, physical examination, or laboratory findings of a general medical condition judged to be etiologically related to the disturbance. C. The disturbance is not better accounted for by another mental disorder (e.g., Adjustment Disorder with Depressed Mood, in response to the stress of having a general medical condition).
Appendix L· Mood Disorders
139
D. The symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning. E. The disturbance does not occur exclusively during the course of Delirium or Dementia. Specify type:
With Manic Features: if the predominant mood is elevated, euphoric, or irritable.
With Depressive Features: if the predominant mood is depressed.
With Mixed Features: if symptoms of both mania and depression are present and neither predominates.
Substance-Induced Mood Disorder A. A prominent and persisent disturbance in mood characterizedby either (or both) of the following: (1) depressed mood or markedly diminished interest or pleasure in all, or almost all, activities (2) elevated, expansive, or irritable mood B. There is evidence from the history, physical examination, or laboratory findings of substance intoxication or withdrawal, and the symptoms in A developed during, or within a month of, significant substance intoxication or withdrawal. C. The disturbance is not better accounted for by a Mood Disorder that is not substance-induced. Evidence that the symptoms are better accounted for by a Mood Disorder that is not substance-induced might include: the symptoms precede the onset of the substance abuse or dependence; persist for a substantial period of time (e.g., about a month) after the cessation of acute withdrawal or severe intoxication; are substantially in excess of what would be expected given the character, duration, or amount of the substance used; or there is other evidence suggesting the existence of an independent non-substance-induced mood disorder (e.g., a history of recurrent non-substance-related major depressive episodes). D. The symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning.
140
DEALING WITH DEPRESSION
E. The disturbance does not occur exclusively during the course of Delirium. Code: (Specific Substance) Mood Disorder (291.8 Alcohol, 292.84 Amphetamine [or Related Substance], 292.84 Cocaine, 292.84 Hallucinogen, 292.84 Inhalant, 292.84 Opioid, 292.84 Phencyclidine [or Related Substance], 292.84 Sedative, Hypnotic, or Anxiolytic, 292.84 Other [or Unknown] Substance) Coding note: also code substance-specific Intoxication or Withdrawal if criteria are met. Specify type:
With Manic Features: if the predominant mood is elevated, euphoric, or irritable. With Depressive Features: if the predominant mood is depressed. With Mixed Features: if symptoms of both mania and depression are present and neither predominates. Specify if: with onset during intoxication with onset during withdrawal
296.90MoodDisorder Not Otherwise Specified This category includes disorders with mood symptoms that do not meet the criteria for any specific mood disorder and in which it is difficult to choose between Depressive Disorder NOS and Bipolar Disorder NOS (e.g., acute agitation).
Cross-Sectional Symptom Features Specify if: With Melancholic Features (can be applied to major depressive episodes occurring in Maj or Depressive Disorder, Bipolar I Disorder or Bipolar II Disorder): A. Either of the following, occurring during the most severe period of the current episode:
Appendix L' Mood Disorders
141
(1) loss of pleasure in all, or almost all, activities (2) lack of reactivity to usually pleasurable stimuli (does not feel much better, even temporarily, when something good happens) B. At least three of the following: (1) distinct quality of depressed mood (i.e., the depressed mood is perceived as distinctly different from the kind of feeling experienced after the death of a loved one) (2) the depression is regularly worse in the mornings (3) early morning awakening (at least two hours before usual time of awakening) (4) marked psychomotor retardation or agitation (5) significant anorexia or weight loss (6) excessive or inappropriate guilt Specify if: With Atypical Features (can be applied to the most recent major depressive in Major Depressive Disorder, Bipolar I Disorder, or Bipolar II Disorder, or to Dysthymic Disorder): A. Mood reactivity (i.e., mood brightens in response to actual or potential positive events). B. Two of the following features, present for most of the time, for at least two weeks: (1) significant weight gain or increase in appetite (2) hypersomnia (3) leaden paralysis (i.e., heavy, leaden feelings in arms or legs) (4) longstanding pattern of interpersonal rejection sensitivity (not limited to episodes of mood disturbance) resulting in significant social or occupational impairment C. Does not meet criteria for "With Melancholic Features" during the same episode. Specify if: With Catatonic Features (can be applied to the most recent manic episode of major depressive episode in Major Depressive Disorder, Bipolar I Disorder, or Bipolar II Disorder):
142
DEALING WITH DEPRESSION
The clinical picture is dominated by at least two of the following: (1) motoric immobility as evidenced by catalepsy (including waxy flexibility) or stupor (2) excessive motor activity (that is apparently purposeless and not influenced by external stimuli) (3) extreme negativism (an apparently motiveless resistance to all instructions or maintenance of a rigid posture against attempts to be moved) or mutism (4) peculiarities of voluntary movement as evidenced by posturing (voluntary assumption of inappropriate or bizarre postures), stereotyped movements, prominent mannerisms, or prominent grimacing (5) echolalia or echopraxia
Course Specifiers: Specify if: With Rapid Cycling (can be applied to Bipolar I Disorder or Bipolar II Disorder): At least four episodes or a mood disturbance in the previous 12 months that meet criteria for a manic episode, a hypomanic episode, or a major depressive episode. Note: episodes are demarcated by a switch to an episode of opposite polarity (e.g., depressed mood to manic mood) or by a period of remission. Specify if: With Seasonal Pattern (can be applied to Bipolar I Disorder, Bipolar II Disorder, and Major Depressive Disorder, Recurrent) : A. There has been a regular temporal relationship between the onset of an episode of Bipolar I or Bipolar II Disorder or Major Depressive Disorder, Recurrent, and a particular time of the year (e.g., regular appearance of depression in the fall or winter). B. Full remissions (or a change from depression to mania or hypomania) also occur at a characteristic time of the year (e.g., depression disappears in the spring). C. In the last two years, two episodes have occurred that demonstrate the temporal seasonal relationship defined in A and B, and no nonseasonal episodes have occurred during that same period. D. Seasonal episodes of mood disturbance, as described above,
Appendix I: Mood Disorders
143
substantially outnumber any nonseasonal episodes of such disturbance that may have occurred over the individual's lifetime. Specify if: With Postpartum Onset (can be applied to major depressive or manic episodes in Bipolar I Disorder, Bipolar II Disorder, or Major Depressive Disorder; or to Brief Psychotic Disorder): Onset of episode within 4 weeks postpartum.
This page intentionally left blank
Appendix II MANIA/HYPOMANIA * Diagnostic Notes: (1) In diagnosing mania at least 3 items are required from B if the predominant mood is euphoric, at least 4 items are required if the predominant mood is irritable. (2) Criterion C is required to diagnose mania. If criterion C is is not met, and the other criteria are present, the diagnosis is hypomania.
(A) A distinct period ofabnormally and persistently elevated, expansive, or irritable mood. Have there been times lasting at least a couple of days when you felt the opposite of depressed, that is when you were very cheerful or high and this felt different than your normal self? IF YES or UNCLEAR: Did you feel hyper, or like you were high on drugs, even though you hadn't taken anything? Did anything cause your good mood? How long did it last? So, was this more than just feeling good? When did this occur? How many periods like this have you had? IF NO: What about a period lasting at least a couple of days when you were unusually irritable and excitable, and quick to argue or fight? *Mark Zimmerman. Diagnosing DSM-III-R Psychiatric Disorders in Primary Care Settings: An Interview Guide for the Nonpsychiatric Physician. Philadelphia: Psychiatric Press, 1993, pp. 24-33.
145
146
DEALING WITH DEPRESSION
IF YES: Describe what that was like. Were you using drugs or alcohol? Did you get into many arguments or fights? How long did this period last? Was there a reason you felt that way? When did it occur? How many periods like this have you had? Now I'm going to ask about some other things that you might have been thinking or feeling when you were feeling HIGH, HYPER, EUPHORIC, IRRITABLE, etc.
#1 Inflated self-esteem or grandiosity. What was your self-esteem like? Did you feel more self-confident than usual? Did you think you had special talents, abilities, or powers?
IF YES: Like what? When some people feel HIGH, EUPHORIC, etc., they may think they're going to become famous or do great things. Did you have any thoughts like that? IF YES: Like what?
#2 Decreased needfor sleep, e.g., feels restedafter only three hours of sleep. During this time, how did you sleep? Did you need less sleep than usual in order to feel rested?
#3 More talkative than usual orpressureto keep talking. Were you more talkative than usual? Did you talk on and on so that peoplecouldn't shutyouup or intenupt? Did you talk faster than normal?
Appendix II: Mania/Hypomania
147
IF YES: Did you talk so fast that people couldn't understand you?
#4 Flight ofideas or subjective experiences that thoughts are racing. During this time, did it feel like your thoughts were going very fast and racing through your mind?
#5 Distractibility, i.e., attention too easily drawn to unimportant or irrelevant externalstimuli. Were you easily distracted so that any little thing could get you off track? IF YES: What was that like?
#6 Increase in goal-directed activity (either socially, at workor school, or sexually) orpsychomotor agitation. Were you more active than usual? For example, did you do more chores around the house? Were you so energetic that instead of sleeping you did household chores or worked throughout the night? Did you start new projects or take on added responsibilities? Did you work more? Did you call friends more? Were you sexually more active than usual? Did you feel physically restless so that it was hard to sit still and you were always moving or pacing back and forth?
#7 Excessive involvement in pleasurable activities which have a high potentialfor painful consequences, e.g., the person engages in unrestrained buying sprees, sexual indiscretions, orfoolish businessinvestments. Did you do anything that you enjoyed at the time but that could have caused problems for you or your family? For example, when some
148
DEALING WITH DEPRESSION
people feel (MANIC MOOD) they go on spending sprees, write bad checks, invest money foolishly, or do things sexually that are unusual for them. Did you do anything like that?
IF YES: Like what? C. Mooddisturbance sufficiently severe to causemarked impairment in occupational functioning or in usual social activities or relationships with others, or to necessitate hospitalization to prevent harm to self or others. What effect did this episode have on your life at the time it was going on? Did it cause major problems in your ... · .. job (school)? . ? ... marnage.
· .. relationships with friends or family? · . . social life?
IF YES TO ANY ITEM: What happened? Did you get treatment?
IF YES: Were you hospitalized?
D. Exclude the diagnosis if during the course ofthe illnessthe patient had delusions or hallucinations for at leasttwo weeks in the absence ofprominent mood symptoms. In such cases the diagnosis is schizophrenia, schizoaffective disorder, delusional disorder, schizophreniform disorder, orpsychoticdisorder NOS. (See pages 20-23 for psychosis questions.)
IF PSYCHOTIC: Was there a time when you (PSYCHOTIC SYMPTOM) but did not feel (MANIC MOOD) and have problems with (MANIC SYMPTOMS)? IF YES: How long did you have (PSYCHOTIC SYMPTOMS) only?
Appendix II: Mania/Hypomania
149
When did the (MANIC MOOD AND SYMPTOMS) begin in relation to this?
E. Exclude the diagnosis ifthe manic syndrome is superimposed on schizophrenia, schizophreniform disorder, delusional disorder, orpsychotic disorder NOS. R Exclude the diagnosis if manic syndrome is due to physical illness (e.g., hyperthyroidism, or streetdrugs such as amphetamines or cocaine). MAJOR DEPRESSION Note: For each symptom you must inquire about duration. (For how long have you . • . ) and persistence. (Do you feel like that nearly every day?) Al Depressed moodmost of the day, nearly every day. How is your mood? Have you been feeling sad, blue, down, or depressed?
IF YES: For how long have you been feeling (DEPRESSED, DOWN, etc.)? Do you feel that way nearly every day? How much of the day does it last? How bad is the feeling?
A2 Markedly diminished interestorpleasure in all, or almostall, activities most ofthe day, nearlyevery day. Have you lost interest in or do you get less pleasure from the things you used to enjoy?
IF YES: What do you normally enjoy doing? (Television? Reading? Sports? Shopping? Socializing? Eating? Hobbies? Sex?) What do you still enjoy?
150
DEALING WITH DEPRESSION
What have you lost interest in? For how long have you not enjoyed these things like you used to? Is it like that nearly every day?
A3 Significant weightloss or weightgain when not dieting (e.g., more than 5% ofbody weightin a month), or decrease or increase in appetite nearly everyday. Has there been any change in your appetite?
IF INCREASED OR DECREASED: How much more/less have you been eating? Is it like that nearly every day? For how long has your appetite been increased/decreased? Have you gained/lost any weight?
IF YES: How much? Since when?
A4 Insomnia or hypersomnianearly everyday. How have you been sleeping? How many hours per night have you been sleeping? How does this compare to normal?
IF INCREASED OR DECREASED: Is it a problem nearly every day? For how long have you had sleep problems?
IF DECREASED: Do you have problems falling asleep, staying asleep, or waking up too early in the morning? AS Psychomotor agitation or retardation nearly every day
(observable by others, not merely subjective feelings of restlessness or being sloweddown). Observation of psychomotor agitation (fidgety while sitting; pacing;
Appendix II: Mania/Hypomania
151
pulling on hair, skin, or clothing; handwringing; crossing and uncrossing legs frequently) and/or psychomotor retardation (slowed speech; long pauses before answering or between words; mute; slowed body movements) by interviewers or others. Agitation: Have you been more fidgety and having problems sitting still? IF YES: Do you pace back and forth? Have others noticed your restlessness? Retardation: Have you felt slowed down, like you were moving in slow motion or stuck in mud? IF YES: Have others noticed this?
A6 Fatigue or loss ofenergynearly every day. How has your energy level been? Have you been feeling tired or worn out? IF YES: Duration and persistence questions. (See top of pg. 28). A7 Feelings of worthlessness or excessive or inappropriate guilt
nearly every day (not merelyself-reproach or guilt about being sick). How have you been feeling about yourself? What has your self-esteem been like? IF LOW: What type of thoughts do you have about yourself? Do you feel like you're worthless or a failure? IF YES: Tell me about it. Have you been blaming yourself for things? IF YES: Like what? Do you feel guilty? IF YES: About what?
152
DEALING WITH DEPRESSION
Do you think about things from the past and feel guilty about them?
IF EVIDENCE OF GUILT OR WORTHLESSNESS. How often do you actually think (PATIENT'S DESCRIPTION
OF GUILT OR WORTHLESSNESS)?
A8 Diminishedability to think or concentrate, or indecisiveness, nearly every day. Have you been having problems thinking or concentrating?
IF YES: In what way? Are you able to read? Watch TV? Follow a conversation? Duration and persistence questions. Is it harder to make decisions than before?
IF YES: What kind of decisions are harder to make? Duration and persistence questions.
A9 Recurrent thoughts ofdeath (notjust fear ofdying), recurrent suicidalideation without a specific plan, or a suicideattemptor a specificplan for committingsuicide. Sometimes when a person feels down or depressed they might think about dying. Have you been having any thoughts like that?
IF YES: Tell me about it. Have you thought about taking your life? IF YES: Did you think of a way to do it? How close have you come to doing it?
IF NO: Do you wish you were dead? When you go to sleep, do you often wish you would not wake up?
B1 Exclude the diagnosis if due to physical illness (endocrine disorder), medication (antihypertensives), or street drugs (alcohol, cocaine withdrawal, PCP, steroids).
Appendix II· Mania/Hypomania
153
B2 Exclude the diagnosis if the depression is a normal reaction to the death of a loved one. C. Exclude the diagnosis if during the course of the illness the patient had delusions or hallucinations for at least two weeks in the absence ofprominent mood symptoms. In such cases the diagnosis is schizophrenia, schizoaffective disorder, delusional disorder, schizophreniform disorder, psychotic disorder NOS. IF PSYCHOTIC: Was there a time when you (PSYCHOTIC SYMPTOM) but did not feel sad or depressed and have problems with (DEPRESSIVE
SYMPTOMS)? IF YES: How long did you have (PSYCHOTIC SYMPTOMS) only? When did the depression begin in relation to this?
D. Exclude the diagnosis if the depressive syndrome is superimposed on schizophrenia, schizophreniform disorder, delusional disorder, or psychotic disorder NOS. DYSTHYMIA
A. Depressed mood for most of the day, more days than not, for at least two years. How is your mood? Have you been feeling sad, blue, down, or depressed?
IF YES: How often? (On more days than not?) For how long have you felt this way? (Has it been at least two years?)
Diagnostic Note: Dysthymia refers to a chronic low grade depression lasting at least two years during which time the individual does not meet criteria for a major depressive episode. Thus, to establish a time
DEALING WITH DEPRESSION
154
frame to diagnose dysthymia you must determine if major depression is currently present, or has been present in the past two years. Recently, have you been more severely depressed than usual?
IF NO: Was there a time in the past two years lasting at least a couple of weeks when you felt more severely depressed than usual?
IF YES TO EITHER: See pages for major depression questions. IF CURRENT MAJOR DEPRESSION: For how long have you been feeling severely depressed with symptoms like (PRESENT DEPRESSIVE SYMPTOMS)? Before that, were you still bothered by a low level of depression?
IF YES: Was that low level of depression present on most days? IF YES: So, even before this current episode of more severe depression, you were bothered by a milder depression on most days. Right? For how long did you have the milder depression?
IF MAJOR DEPRESSION DURING PAST TWO YEARS Since you improved from your serious depression occurring last (DATE), have you still felt sad, blue, or depressed on most days?
IF YES: Is that how you were before you got more severely depressed?
IF YES: For how long before the serious depression were you bothered by the milder depression?
B. Presence, whiledepressed, ofat leasttwo ofthe following. During this chronic low-level depression, do you often ... (1)
lose your appetite or overeat?
(2)
have difficulty sleeping or oversleeping?
(3)
feel tired?
(4)
feel down on yourself, or have low self-esteem?
Appendix II: Mania/Hypomania
(5)
have problems concentrating or making decisions?
(6)
feel hopeless or pessimistic about the future?
155
c. During a two-year period ofthe disturbance, never withoutthe symptoms in A for morethan two months at a time. During the (DYSTHYMIA TIME PERIOD) were you ever free of depression or sadness for a couple of months or more?
D. Exclude the diagnosis if a majordepression occurred during thefirst twoyears ofthe dysthymia. When did the low level depression begin? See pages 28-31 for major depression questions, and determine if major depressive episode occurred during first two years of onset of dysthymia.
E. Exclude the diagnosis if the individual has a history ofa manic or hypomanic episode.
if the symptoms are superimposed on a chronic psychotic disorder such as schizophrenia or delusional disorder.
F. Exclude diagnosis
G. Exclude the diagnosis if the symptoms are due to an organic cause such as physical illness (e.g., hypothyroidism), prescribed medications (e.g., betablockers, reserpine, methyldopa), or drug use (e.g., recurrent cocaine or alcoholwithdrawal).
This page intentionally left blank
Appendix III PLEASANT EVENTS SCHEDULE: FORM III-S* This schedule is designed to find out about the things you have enjoyed during the past month. The schedule contains a list of events or activities that people sometimes enjoy. You will be asked to go over the list twice, the first time rating each event on how many times it has happened in the past month and the second time rating each event on how pleasant it has been for you. There are no right or wrong answers. Please rate every event. Work quickly; there are many items and you will not be asked to make fine distinctions on your ratings. The schedule should take about an hour to complete. Please make your ratings on the sheets provided.
Directions-Question A On the following pages you will find a list of activities, events, and experiences. How often have these events happened in your life in the past month? Please answer this question by rating each item on the following scale:
o = This has not happened in the past 30 days. 1 = This has happened a few times (1 to 6) in the past 30 days. 2 = This has happened often (7 or more) in the past 30 days. Place your rating for each item on the sheet under "A." Here is an example: Item number 1 is "Being in the country." Suppose you have been in the country three times during the past 30 days. Then you would mark a "1" on the answer sheet for item number 1. *MacPhillamy, Douglas J. and Peter M. Lewinsohn. "The Pleasant Events Schedule: Studies in Reliability, Validity, and Scale Intercorrelation," Journal of Consulting and Clinical Psychology, 50(3):376-380, 1982.
157
158
DEALING WITH DEPRESSION
Important: Some items will list more than one event; for these items, mark how often you have done any of the listed events. For example, item number 12 is "Doing art work (painting, sculpture, drawing, movie-making, etc.)." You should rate item 12 on how often you have done any form of art work in the past month. Since this list contains events that might happen to a wide variety of people, you may find that many of the events have not happened to you in the past 30 days. It is not expected that anyone will have done all of these things in one month. Now tum the page and begin.
Appendix III: Pleasant Events Schedule
159
A B 1. Being in the country. 2. Wearing expensive or formal clothes. 3. Making contributions to religious, charitable, or other groups. 4. Talking about sports. 5. Meeting someone new of the same sex. 6. Taking tests when well prepared. 7. Going to a rock concert. 8. Playing baseball or softball. 9. Planning trips or vacations. 10 Buying things for myself. 11. Being at the beach. 12. Doing art work (painting, sculpture, drawing, moviemaking, etc.). 13. Rock climbing or mountaineering. 14. Reading the Scriptures or other sacred works. 15. Playing golf. 16. Taking part in military activities. 17. Re-arranging or redecorating my room or house. 18. Going naked. 19. Going to a sports event. 20. Reading a "How to Do It" book or article. 21. Going to the races (horse, car, boat, etc.). 23. Going to a bar, tavern, club, etc. 24. Going to lectures or hearing speakers. 25. Driving skillfully. 26. Breathing clean air. 27. Thinking up or arranging songs or music. 28. Getting drunk. 29. Saying something clearly. 30. Boating (canoeing, kayaking, motorboating, sailing, etc.). 31. Pleasing my parents. 32. Restoring antiques, refinishing furniture, etc. 33. Watching TV 34. Talking to myself. 35. Camping.
160
DEALING WITH DEPRESSION
A B 36. Working in politics. 37. Working on machines (cars, bikes, motorcycles, tractors, etc.). 38. Thinking about something good in the future. 39. Playing cards. 40. Completing a difficult task. 41. Laughing. 42. Solving a problem, puzzle, crossword, etc. 43. Being at weddings, baptisms, confirmations, etc. 44. Criticizing someone. 45. Shaving. 46. Having lunch with friends or associates. 47. Taking powetful drugs. 48. Playing tennis. 49. Taking a shower. 50. Driving long distances. 51. Woodworking, carpentry. 52. Writing stories, novels, plays, or poetry. 53. Being with animals. 54. Riding in an airplane. 55. Exploring (hiking away from known routes, spelunking, etc.). 56. Having a frank and open conversation. 57. Singing in a group. 58. Thinking about myself or my problems. 59. Working on my job. 60. Going to a party. 61. Going to church functions (socials, classes, bazaars, etc.). 62. Speaking a foreign language. 63. Going to service, civic, or social club meetings. 64. Going to a business meeting or convention. 65. Being in a sporty or expensive car. 66. Playing a musical instrument. 67. Making snacks. 68. Snow skiing.
Appendix iu. Pleasant Events Schedule
161
AB 69. 70. 71. 72. 73. 74. 75. 76. 77. 78. 79. 80. 81. 82. 83. 84. 85. 86. 87. 88. 89. 90. 91. 92. 93. 94. 95. 96. 97. 98. 99. 100. 101. 102.
Being helped. Wearing informal clothes. Combing or brushing my hair. Acting. Taking a nap. Being with friends. Canning, freezing, making preserves, etc. Driving fast. Solving a personal problem. Being in a city. Taking a bath. Singing to myself. Making food or crafts to sell or give away. Playing pool or billiards. Being with my grandchildren. Playing chess or checkers. Doing craft work (pottery, jewelry, leather, beads, weaving, etc.). Weighing myself. Scratching myself. Putting on make-up, fixing my hair, etc. Designing or drafting. Visiting people who are sick, shut in, or in trouble. Cheering, rooting. Bowling. Being popular at a gathering. Watching wild animals. Having an original idea. Gardening, landscaping, or doing yard work. Shoplifting. Reading essays or technical, academic, or professional literature. Wearing new clothes. Dancing. Sitting in the sun. Riding a motorcycle.
162
DEALING WITH DEPRESSION
A B 103. 104. 105. 106. 107. 108. 109. 110. 111. 112. 113. 114. 115. 116. 117. 118. 119. 120. 121. 122. 123. 124. 125. 126. 127. 128. 129. 130. 131. 132. 133. 134.
Just sitting and thinking. Social drinking. Seeing good things happen to my family or friends. Going to a fair, carnival, circus, zoo, or amusement park. Talking about philosophy or religion. Gambling. Planning or organizing something. Smoking marijuana. Having a drink by myself. Listening to the sounds of nature. Dating, courting, etc. Having a lively talk. Racing in a car, motorcycle, boat, etc. Listening to the radio. Having friends come to visit. Playing a sporting competition. Introducing people who I think would like each other. Giving gifts. Going to school or government meetings, court sessions, etc. Getting massages or backrubs. Getting letters, cards, or notes. Watching the sky, clouds, or a storm. Going on outings (to the park, a picnic, a barbecue, etc.). Playing basketball. Buying something for my family. Photography. Giving a speech or lecture. Reading maps. Gathering natural objects (wild foods or fruit, rocks, driftwood, etc.). Working on my finances. Wearing clean clothes. Making a major purchase or investment (car, appliance, house, stocks, etc.).
Appendix III: Pleasant Events Schedule
163
A B 135. Helping someone. 136. Being in the mountains. 137. Getting a job advancement (being promoted, given a raise, or offered a better job, accepted into a better school, etc.). 138. Hearing jokes. 139. Winning a bet. 140. Talking about my children or grandchildren. 141. Meeting someone new of the opposite sex. 142. Going to a revival or crusade. 143. Talking about my health. 144. Seeing beautiful scenery. 145. Eating good meals. 146. Improving my health (having my teeth fixed, getting new glasses, changing my diet, etc.). 147. Being downtown. 148. Wrestling or boxing. 149. Hunting or shooting. 150. Playing in a musical group. 151. Hiking. 152. Going to a museum or exhibit. 153. Writing papers, essays, articles, reports, memos, etc. 154. Doing a job well. 155. Having spare time. 156. Fishing. 157. Loaning something. 158. Being noticed as sexually attractive. 159. Pleasing employers, teachers, etc. 160. Counseling someone. 161. Going to a health club, sauna bath, etc. 162. Having someone criticize me. 163. Learning to do something new. 164. Going to a "Drive-in" (Dairy Queen, MacDonald's, etc.). 165. Complimenting or praising someone. 166. Thinking about people I like.
164
DEALING WITH DEPRESSION
AB 167. 168. 169. 170.. 171.. 172. 173. 174. 175. 176. 177. 178. 179. 180. 181. 182. 183. 184. 185. 186. 187. 188. 189. 190. 191. 192. 193. 194. 195. 196. 197. 198. 199. 200. 201.
Being at a fraternity or sorority. Taking revenge on someone. Being with my parents. Horseback riding. Protesting social, political, or environmental conditions. Talking on the telephone. Having daydreams. Kicking leaves, sand, pebbles, etc. Playing lawn sports (badminton, croquet, shuffleboard, horseshoes, etc.). Going to school reunions, alumni meetings, etc. Seeing famous people. Going to the movies. Kissing. Being alone. Budgeting my time. Cooking meals. Being praised by people I admire. Outwitting a "superior." Feeling the presence of the Lord in my life. Doing a project in my own way. Doing "odd jobs" around the house. Crying. Being told I am needed. Being at a family reunion or get-together. Giving a party or get-together. Washing my hair. Coaching someone. Going to a restaurant. Seeing or smelling a flower or plant. Being invited out. Receiving honors (civic, military, etc.). Using cologne, perfume, or aftershave. Having someone agree with me. Reminiscing, talking about old times. Getting up early in the morning.
Appendix III: Pleasant Events Schedule
165
A B 202. 203. 204. 205. 206. 207. 208. 209. 210. 212. 213. 214. 215. 216. 217. 218. 219. 220. 221. 222. 223. 224. 225. 226. 227. 228. 229. 230. 231. 232. 233. 234.
Having peace and quiet. Doing experiments or other scientific work. Visiting friends. Writing in a diary. Playing football. Being counseled. Saying prayers. Giving massages or backrubs. Hitchhiking. Seeing a fight. Doing favors for people. Talking with people on the job or in class. Being relaxed. Being asked for my help or advice. Thinking about other people's problems. Playing board games (Monopoly, Scrabble, etc.). Sleeping soundly at night. Doing heavy outdoor work (cutting or chopping wood, clearing land, farm work, etc.). Reading the newspaper. Shocking people, swearing, making obscene gestures, etc. Snowmobiling or dune-buggy riding. Being in a body-awareness, sensitivity, encounter, therapy, or "rap" group. Dreaming at night. Playing ping pong. Brushing my teeth. Swimming. Being in a fight. Running, jogging, or doing gymnastic, fitness, or field exercises. Walking barefoot. Playing frisbee or catch. Doing housework or laundry; cleaning things. Being with my roommate.
166
DEALING WITH DEPRESSION
AB 235. 236. 237. 238. 239. 240. 241. 242. 243. 244. 244. 245. 246. 247. 248. 249. 250. 251. 252. 253. 254. 255. 256. 257. 258. 259. 260. 261. 262. 263. 264. 265. 266. 267. 268. 269.
Listening to music. Arguing. Knitting, crocheting, embroidery, or fancy needlework. Petting, necking. Amusing people. Talking about sex. Going to a barber or beautician. Having house guests. Being with someone I love. Reading magazines. Reading magazines. Sleeping late. Starting a new project. Being stubborn. Having sexualrelations with a partnerof the opposite sex. Having other sexual satisfactions. Going to the library. Playing soccer, rugby, hockey, lacrosse, etc. Preparing a new or special food. Birdwatching. Shopping. Watching people. Building or watching a fire. Winning an argument. Selling or trading something. Finishing a project or task. Confessing or apologizing. Repairing things. Working with others as a team. Bicycling. Telling people what to do. Being with happy people. Playing party games. Writing letters, cards, or notes. Talking about politics or public affairs. Asking for help or advice.
Appendix IlL· Pleasant Events Schedule
167
A B 270. 271. 272. 273. 274. 275. 276. 277. 278. 279. 280. 281. 282. 283. 284. 285. 286. 287. 288. 289. 290. 291. 292. 293. 294. 295. 296. 297. 298. 299. 300. 301. 302.
Going to banquets, luncheons, potlucks, etc. Talking about my hobby or special interest. Watching attractive women or men. Smiling at people. Playing in sand, a stream, the grass, etc. Talking about other people. Being with my husband or wife. Having people show interest in what I have said. Going on field trips, nature walks, etc. Expressing my love to someone. Smoking tobacco. Caring for houseplants. Having coffee, tea, a coke, etc., with friends. Taking a walk. Collecting things. Playing handball, paddleball, squash, etc. Sewing. Suffering for a good cause. Remembering a departed friend or loved one, visiting the cemetery. Doing things with children. Beachcombing. Being complimented or told I have done well. Being told I am loved. Eating snacks. Staying up late. Having family members or friends do something that makes me proud of them. Being with my children. Going to auctions, garage sales, etc. Thinking about an interesting question. Doing volunteer work; working on community service projects. Water skiing, surfing, scuba diving. Receiving money. Defending or protectingsomeone; stoppingfraud or abuse.
168
DEALING WITH DEPRESSION
AB 303. 304. 305. 306. 307. 308. 309. 310. 311. 312. 313.
Hearing a good sermon. Picking up a hitchhiker. Winning a competition. Making a new friend. Talking about my job or school. Reading cartoons, comic books, or comic strips. Borrowing something. Traveling with a group. Seeing old friends. Teaching someone. Using my strength.
314. 315. 316. 317. 319. 320.
Traveling. Going to office parties or departmental get-togethers. Attending a concert, opera, or ballet. Playing with pets. Looking at the stars or moon. Being coached.
STOP If you have just gone through the list for the first time, go to the next page and follow the directions for Question B. If you have just finished answering Question B, you have completed the test.
Directions-Question B Now please go over the list once again. This time the question is: HOW PLEASANT, ENJOYABLE, OR REWARDING WAS EACH EVENT DURING THE PAST MONTH? Please answer this question by rating each event on the following scale:
o = This was not pleasant. (Use this rating for events that were either neutral or unpleasant.)
Appendix III: Pleasant Events Schedule
169
1 =This was somewhat pleasant. (Use this rating for events that were mildly or moderately pleasant.) 2 = This was very pleasant. (Use this rating for events that were strongly or extremely pleasant.)
Important: If an event has happened to you more than once in the past month, try to rate roughly how pleasant it was on the average. If an event has not happened to you during the past month, then rate it according to how much fun you think it would have been. When an item lists more than one event, rate it on the events you have actually done. (If you haven't done any of the events in such an item, give it the average rating of the events in that item which you would like to have done.) Place your rating for each event on the sheet under "B." Here is an example: Event number 1 is "Being in the country." Suppose that each time you were in the country in the past 30 days you enjoyed it a great deal. Then you would rate this event "2," since it was "very pleasant. " The list of items may have some events that you would not enjoy. The list was made for a wide variety of people, and it is not expected that one person would enjoy all of them. Now go back to the list of events, start with item 1, and go through the entire list rating each event on roughly how pleasant it was (or would have been) during the past 30 days. Please be sure that you rate each item on the sheet.
This page intentionally left blank
Index ABC theory, 72 Abel, 37 Abraham, 35-36 Adam, 38 Adult ego state, 16 Affirmation, 34,36,37,104 Aggression, 46 Alcoholics, 109 American Association of Pastoral Counselors, 110 Anger, 9,65,82,88,92,103 Anhedonia, 3 Antidepressants, 112,114-116 Anxiety, 58,65,109 Arbitrary inference, 74 Assertiveness, 65,66,105 Authoritarianism, 58 Authorization, 35 Automatic thoughts, 74,77,78,79,82 Aversive therapy, 55,56,59,99,100. See also Punishment Avoidance, 56,59,99 "Awfullizing",73 Beck, Aaron, 9,71,72,73,74,78,79 Beck Depression Inventory, 9,76,108 Behavior rehearsal, 46 Behavioral therapy, 10,51-67 defined, 51 treatment, 101 Berne, Eric, 15,88 Bible. See Scripture references Bipolar disorder, 7,83,107-108, 132-137 hypomanic episode, 133-134 manic episode, 132-133 single manic episode, 135-136
Birth order, 36 Blackmail, emotional, 46 Blessing, 35-37,98 Borderline personality disorder, 76 Boundary, 42 Breath expiration, 30,31 inspiration, 30,31 Burns, David, 75,76,78,79,82
Cain, 37 Catharsis, 58 Change, 22-23 Child ego state, 16 Church, 88,89,92,96 members depressed, 4 Clinical Pastoral Education, 85 Cognitive errors, 74 Cognitive therapy, 10,71-83 cognitive-behavioral therapy, 72 defined, 71 principles, 75 research, 75,76 Compulsive behavior, 100 personalities, 15,76 Concentration, 5 Conclusions, jumping to, 78 Confession, 31 Confrontation, 59,60 Conscience, 15,31 Contract for life, 21,120 Counselor counseling, brief, 110 depression of, 33,109 ethics of, 117,120 Cowper, William, 1
171
172
DEALING WITH DEPRESSION
Cyclothymia, 7,108 clyclothymic disorder, 137-138
Death, 19,34 Demons, 35,88,90,91,97,102, 103,104 exorcism, 86 of fear, 95 possession by, 86,87,92,93,94 Denial, 42 Dependency, 55 Depletion, 28,30,32 Depression behavior symptoms, 62 behavioral theory, 10 biochemical theory, 9,15 causes of, 9-10 characterological, 57 cognitive theory, 10 contagiousness of, 109 counselor's, 33,109 defined, iv,13 diagnosis, 3-4 double, 7 existential, 10 facial features, 4 family systems theory, 10 Gestalt theory, 10 hereditary theory, 9 at holidays, 8 major, 127-130,149-153 manic, 6-7 masked, 5 physical symptoms, 5 postpartum, 8 purpose of, 38 reactive, 8 religious theory, 10 smiling, 5 statistics about, iii-iv,1,2 synonyms, 2,3 Desensitization, 67 Despair, 30 Devil, 86,88,91,100
Dexamethasone suppression test, 108 Discrimination, 43,57,101 Dominance, 44,101 Dreams, 88-89 Dysphoria, 3 Dysthymic disorder, 7,82,83,108, 130-131,153-155 Electroconvulsive therapy, 20,113 Ego states Adult, 16 Child, 16 Parent, 17-19 Elijah, 2 Ellis, Albert, 71-74 Emptiness, 32 Environmental manipulation, 68 Error fortune teller, 78 systematic, 78 Esau,37 Escape, 56 Ethics, 117,120 Euphoria, 6 Exorcism, 86 Exorcist, The, 34,93,97 Extinction, 51,57,60,61,64 Family, 105,109,120 Fear, 19,88,95,100,104 Feelings, 20,65 clients, 83 Figures daily record of dysfunctional thoughts, 80 frequency counting, 62 stuck point, 41 triple-column technique, 81 types of depression, 5 Flight of ideas, 6 Forgiveness, 18,31,89,97 Fosdick, Harry Emerson, 109,110 Frequency-counting, 60,61
173
Index
Frustration, 44,48 Future, 14,21,31,63
Gestalt therapy, 10,41-49 defined, 41 purpose of, 102 God, 29-30,34,35,94,98,100,101,121 Grandiosity, 6 Greed, 48 Grief, 5,8,38,52,54,58,64 Group therapy, 89,104,105 Guilt, 82,86,89,91,152
Hamlet, 2,34 Heirlooms, 37 Help, 45 helplessness, 57,99,101 helplessness, learned, 57 Heredity, 9,15 Homework, 77,79,82,83 Hopeless, 20 hopelessness, 77,117 Hulme, William, E., 113 Humor, sense of, i,83. See also Laughter Hypnotism, 90
Impasse, 41 Introjection, 41-43,46 introjector, 101 Isaac, 35,37
Jacob, 37 Jesus, 2,23,30,36
Labeling, 79,82 Laughter, 33,42. See also Humor Law of effect, 52 Laziness, 48,57 Learning behavior, 51
Loss, 4,5,19 Love, 15,18,19,20,28,37 tender loving care, 20,21 Maclaren, Alexander, 109 Mania, 6,145-149 May, Rollo, 43,44 Meaning, 10,29,73 Mind-reading, 78 Moses, 32-33 "MUSTurbation", 73 Negative triad, 73 Neurosis, depressive, 7,109 Newton, John, 1 Nothingness, 41,42 Number one, 29 Obligations, 28 Obsessiveness, 59,76,88,101 Olsson, Karl, 30 Overgeneralization, 74,78 Pain, 29,104 Parent ego state, 17 nurturing, 19 punishing, 18 Party, 30-32 Past, 77 Patience, 47 Pavlov, Ivan, 51 Perfectionism, 59,82,96,98,100 Perls, Frederick, 41,42,45 Personalization, 79 Physician, 107,108,110,117,120 Pleasant events schedule, 123,157 thoughts, 65 pleasure, 77 words, 75 Positive, disqualifying, 78,82 Power, 44
174
DEALING WITH DEPRESSION
Prejudice, 18 Prernacktechnique,66 Procrastination, 60 Pronouns, use of, 46,102 Psychoanalytic theory, 9,15 Punishment, 54-56. See also Aversive therapy
Questions, use of, 44,118,119,120
Rage, 104 Ratio, 52,53,59,60,99 Rational-emotive therapy, 71,72 Rearrangement, 44 Referral, 107,110,117 Reinforcement, 51-53,55,58,60,63 duration, 54 positive, 100 Relationship, therapeutic, 60 Relaxation, 67 tape, 87 Religion, 18,33 Research, iii-iv,1,2,107 Resistance, 43,44,101 Responsibility, 104 Rewards, 53 Role-playing, 19,46,78 reverse, 79 Romance, 54 Rubber-band snapping, 64,87 Rules, 47
Sadness, iv,2,3,4,5,13,19,29,99 active, 41 and self-esteem, 76 emotional, 77 mood, 75 Schema, 74 Scripture references Gen., 9:5, 118 I Kings, 18-19,2,118 Job, 118
Scripture references (continued) Jonah, 118 Lam., 3:13,31-33,123 Num.,11,118 Phil., 4:4-9, 11,123 Psalms, 22, 22:118, 37:7, 123 Rom., 14:7, 118 Seasonal affective disorder, 7 Selective abstraction, 74 Self-esteem and sadness, 76 building, 82 inflated, 6 loss of, 9 low, 2,8 undermined, 10 Self-rating Depression Scale, 87 Sensory deprivation, 66 Sex, 88,89,91,103-104 Shakespeare Hamlet, 2,34 Merchant a/Venice, 29 Shame, 104 Should statements, 43,44,79 Silences, in therapy, 113,117 Sin sinfulness, 4 sinner, 13 unpardonable, 18 Skinner, B. F., 51 Sleep early awakening, 14 insomnia, 5 patterns, 2,4,6,9 Speech patterns, 43,46 Statistics, iii-iv,1,2,107 Stop-thought method, 64 Strokes, 29,53 Stuck point, 41 Suicide, iii,1,5,20,113,120 Bible, in the, 118 methods, 117 myths about, 122-123 rate, 118
175
Index Suicide (continued) risk factors, 120 threats, 45 Supervision, 110,117
Tables antidepressant comparison chart, 114-116 medical illnesses associated with depression, 111 medications associated with depression, 112 myths about suicide, 122-123 questions to ask a suicidal patient, 119 suicide preventions in the Bible, 118 Terms, outdated, 109 Therapy, insight-oriented, 57,58 Thoughts dysfunctional, 79,80,81,82
Thoughts (continued) mental filter, 78 negative, 75 thinking, all-or-nothing, 78 Time projection, 63 Token economy, 66-67 Transference, 105 Transactional analysis, 13-25 basic concepts, 16 ego states, 16-23 transaction, 27 Truett, George W., 28
Understanding, 22
Ventilate, 113
Worthlessness, 20