Charney & Nestler's Neurobiology of Mental Illness [5 ed.] 019068142X, 9780190681425
In the years following publication of the DSM-5®, the field of psychiatry has seen vigorous debate between the DSM'
2,821 274 117MB
English Pages 1024 Year 2018
Polecaj historie

![Charney amp Nestler's Neurobiology of Mental Illness [5 ed.]
2017046721, 9780190681425](https://dokumen.pub/img/200x200/charney-amp-nestlers-neurobiology-of-mental-illness-5nbsped-2017046721-9780190681425.jpg)
![Neurobiology of mental illness [Fourth edition]
9780199398461, 0199398461, 9780199934959, 0199934959](https://dokumen.pub/img/200x200/neurobiology-of-mental-illness-fourth-edition-9780199398461-0199398461-9780199934959-0199934959.jpg)

![Neurobiology of mental illness [3e edition]
9780199798261, 9780199398461, 0199398461, 0199798265, 9780199857548, 0199857547, 9780199934966, 0199934967, 9781283098335, 1283098334](https://dokumen.pub/img/200x200/neurobiology-of-mental-illness-3e-edition-9780199798261-9780199398461-0199398461-0199798265-9780199857548-0199857547-9780199934966-0199934967-9781283098335-1283098334.jpg)



![Mental Illness [1 ed.]
9780737767636, 9780737762686](https://dokumen.pub/img/200x200/mental-illness-1nbsped-9780737767636-9780737762686.jpg)
![Charney & Nestler's Neurobiology of Mental Illness [5 ed.]
019068142X, 9780190681425](https://dokumen.pub/img/200x200/charney-amp-nestlers-neurobiology-of-mental-illness-5nbsped-019068142x-9780190681425.jpg)
Citation preview
Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press USA - OSO, 2018. 07:30:23.
C H A R N EY & N E S T L E R’S N EU R O B I O L O G Y O F M E N TA L I L L N E S S
Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press USA - OSO, 2018. 07:31:09.
Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press USA - OSO, 2018. 07:31:09.
CHAR NEY & NE ST LER’S NEUROBIOLO GY OF MEN TAL ILLNE SS FIFTH EDITION
EDITED BY
Dennis S. Charney, MD
Pamela Sklar, MD, PhD
ANNE AND JOEL EHRENKRANZ DEAN
MOUNT SINAI PROFESSOR
ICAHN SCHOOL OF MEDICINE
I N P S Y C H I AT R I C G E N O M I C S
AT M O U N T S I N A I
CH A IR , DE PA RTM E N T OF G E N ET I C S
PRESIDENT FOR ACADEMIC AFFAIR S
AND GENOMIC SCIENCES
M O U N T S I N A I H E A LT H S Y S T E M
PROFESSOR OF GENETIC AND GENOMIC
P R O F E S S O R , D E PA RT M E N T S O F P S Y C H I AT R Y,
S C I E N C E S , P S Y C H I AT R Y, A N D N E U R O S C I E N C E
NEUROSCIENCE, AND PHARMACOLOGICAL SCIENCES
I C A H N S C H O O L O F M E D I C I N E AT M O U N T S I N A I
NEW YORK, NEW YORK
NEW YORK, NEW YORK
Joseph D. Buxbaum, PhD
Eric J. Nestler, MD, PhD
P R O F E S S O R O F P S Y C H I AT R Y, N E U R O S C I E N C E , A N D
N A S H FA M ILY P R O F E S S O R O F N E U R O S C IE N C E
GENETICS AND GENOMIC SCIENCES
DIRECTOR OF THE FRIEDMAN
D I R E C T O R O F T H E S E AV E R AU T I S M C E N T E R
BRAIN INSTITUTE
F O R R E S E A R C H A N D T R E AT M E N T
DEAN FOR ACADEMIC AND SCIENTIFIC
ICAHN SCHOOL OF MEDICINE
AFFAIR S ICAHN SCHOOL OF
AT M O U N T S I N A I
M E D I C I N E AT M O U N T S I N A I
NEW YORK, NEW YORK
NEW YORK, NEW YORK
1 Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press USA - OSO, 2018. 07:32:22.
1 Oxford University Press is a department of the University of Oxford. It furthers the University’s objective of excellence in research, scholarship, and education by publishing worldwide. Oxford is a registered trade mark of Oxford University Press in the UK and certain other countries. Published in the United States of America by Oxford University Press 198 Madison Avenue, New York, NY 10016, United States of America. 4th edition: 2013 3rd edition: 2011 2nd edition: 2004 © Oxford University Press 2018 All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, without the prior permission in writing of Oxford University Press, or as expressly permitted by law, by license, or under terms agreed with the appropriate reproduction rights organization. Inquiries concerning reproduction outside the scope of the above should be sent to the Rights Department, Oxford University Press, at the address above. You must not circulate this work in any other form and you must impose this same condition on any acquirer. Library of Congress Cataloging-in-Publication Data Names: Charney, Dennis S., editor. | Sklar, Pamela B., editor. | Buxbaum, Joseph D., editor. | Nestler, Eric J. (Eric Jonathan), 1954– , editor. Title: Charney & Nestler’s neurobiology of mental illness / edited by Dennis S. Charney, Pamela Sklar, Joseph D. Buxbaum, Eric J. Nestler. Other titles: Neurobiology of mental illness. | Charney and Nestler’s neurobiology of mental illness Description: Fifth edition. | New York, NY : Oxford University Press, [2018] | Preceded by Neurobiology of mental illness / edited by Dennis S. Charney ... [et al.]. 4th ed. 2013. | Includes bibliographical references. Identifiers: LCCN 2017046721 | ISBN 9780190681425 (hardcover) Subjects: | MESH: Mental Disorders—etiology | Mental Disorders—physiopathology | Mental Disorders—therapy | Neurobiology Classification: LCC RC341 | NLM WM 140 | DDC 616.8—dc23 LC record available at https://lccn.loc.gov/2017046721 This material is not intended to be, and should not be considered, a substitute for medical or other professional advice. Treatment for the conditions described in this material is highly dependent on the individual circumstances. And, while this material is designed to offer accurate information with respect to the subject matter covered and to be current as of the time it was written, research and knowledge about medical and health issues is constantly evolving and dose schedules for medications are being revised continually, with new side effects recognized and accounted for regularly. Readers must therefore always check the product information and clinical procedures with the most up-to-date published product information and data sheets provided by the manufacturers and the most recent codes of conduct and safety regulation. The publisher and the authors make no representations or warranties to readers, express or implied, as to the accuracy or completeness of this material. Without limiting the foregoing, the publisher and the authors make no representations or warranties as to the accuracy or efficacy of the drug dosages mentioned in the material. The authors and the publisher do not accept, and expressly disclaim, any responsibility for any liability, loss or risk that may be claimed or incurred as a consequence of the use and/ or application of any of the contents of this material. 1 3 5 7 9 8 6 4 2 Printed by Sheridan Books, Inc., United States of America
Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press USA - OSO, 2018. 07:32:56.
CONTENTS
Contributors ix S E C T I O N 1 E M E R G I N G A N D E S TA B L I S H E D TECHNOLOGIES Eric J. Nestler and Karl Deisseroth 1. Genetic Methodologies and Applications Shaun M. Purcell
3
2. Network Methods for Elucidating the Complexity of Common Human Diseases 17 Eric E. Schadt 3. The Human Brain and Its Epigenomes 35 Andrew Chess and Schahram Akbarian 4. Methods for In Vivo Gene Manipulation 43 Lisa M. Monteggia and Wei Xu 5. Application of Stem Cells to Understanding Psychiatric Disorders 55 Kristen Brennand 6. Optogenetics and Related Technologies for Psychiatric Disease Research: Current Status and Challenges 73 Lief E. Fenno and Karl Deisseroth 7. In Vivo Circuit Analysis 87 Ryan Bowman, Hannah Schwennesen, Kafui Dzirasa, and Rainbo Hultman 8. Magnetic Resonance Methodologies 95 Peter A. Bandettini and Hanzhang Lu 9. PET Brain Imaging Methodologies 107 Ansel T. Hillmer, Kelly P. Cosgrove, and Richard E. Carson 10. Neuromodulation and Psychiatric Disorders 121 Wayne K. Goodman and Mark S. George 11. The Neurobiology of Sleep 129 Giulio Tononi and Chiara Cirelli S E C T I O N 2 P S YC H OT I C D I S O R D E R S Pamela Sklar 12. Diagnosis and Epidemiology of Psychotic Disorders Emma Meyer, Julie Walsh-Messinger, and Dolores Malaspina
149
13. Genetics of Schizophrenia and Bipolar Disorder Alexander Charney and Pamela Sklar 14. Neuroimaging of Psychotic Disorders Stephan Heckers, Neil Woodward, and Dost Öngür 15. Animal and Cellular Models of Psychotic Disorders Mikhail V. Pletnikov, Guo-Li Ming, and Christopher A. Ross 16. Cognitive and Motivational Neuroscience of Psychotic Disorders: Animal and Human Studies Jared W. Young, Alan Anticevic, and Deanna M. Barch 17. Synaptic Mechanisms of Psychotic Disorders: Animal and Human Studies Seth G. N. Grant 18. Cellular Mechanisms of Psychotic Disorders: Human Studies Samuel J. Dienel and David A. Lewis 19. Neurodevelopmental Mechanisms for Psychotic Disorders: Animal and Human Studies Nao J. Gamo, Takeshi Sakurai, Hanna Jaaro-Peled, and Akira Sawa 20. The Neurobiology and Treatment of Bipolar Disorder Katherine E. Burdick, Luz H. Ospina, Stephen J. Haggarty, and Roy H. Perlis 21. Novel Approaches for Treating Psychotic Disorders Tiago Reis Marques and Shitij Kapur 22. Current Treatments for Psychotic Disorders Deepak K. Sarpal and Anil K. Malhotra
177 193
209
223
233
245
255
267 277
S E C T I O N 3 DEPRESSION Helen Mayberg 23. Diagnosis and Epidemiology of Depression Nicholas T. Van Dam, Brian M. Iacoviello, and James W. Murrough 24. Genetics of Depression Douglas F. Levinson and Walter E. Nichols 25. Neuroimaging of Depression Michele A. Bertocci and Mary L. Phillips
v USA - OSO, 2018. Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press 07:33:17.
161
289
301 315
26. Animal Models of Mood Disorders Lyonna F. Alcantara, Eric M. Parise, and Carlos A. Bolaños-Guzmán 27. Neurotrophic Mechanisms of Depression: Animal and Human Studies Ronald S. Duman 28. Immune Mechanisms of Depression Caroline Ménard, Madeline L. Pfau, Georgia E. Hodes, and Scott J. Russo 29. Neuroendocrine Mechanisms of Depression: Clinical and Preclinical Evidence Jill M. Goldstein, L. Holsen, S. Cherkerzian, M. Misra, and R.J. Handra 30. New Approaches for Treating Depression Eric J. Nestler 31. Current Treatments for Depression John H. Krystal and Dennis S. Charney
329
341 355
365
377 387
S E C T I O N 4 A N X I ET Y D I S O R D E R S Kerry J. Ressler 32. Diagnosis and Epidemiology of Anxiety, Obsessive-Compulsive, and Trauma and Stressor-Related Disorders Murray B. Stein, Meghan E. Keough, and Peter P. Roy-Byrne 33. Genetics of Anxiety Disorders Takeshi Otowa, Roxann Roberson-Nay, Mandakh Bekhbat, Gretchen N. Neigh, and John M. Hettema 34. Functional Neurocircuitry and Neuroimaging Studies of Anxiety Disorders Madeleine S. Goodkind and Amit Etkin 35. Animal Models and Assays Probing Anxiety Related Behaviors and Neural Circuits Ramon Tasan and Nicolas Singewald 36. What Are Fear and Anxiety? Listening to the Brain Joseph LeDoux 37. Synaptic and Circuit Mechanisms of Anxiety Disorders: Animal and Human Studies Anfei Li and Francis S. Lee 38. The Neurobiology of Resilience Adriana Feder, Sarah R. Horn, Margaret Haglund, Steven M. Southwick, and Dennis S. Charney 39. Novel Approaches for Treating Anxiety Disorders David A. Sturman, Milissa L. Kaufman, Cara E. Bigony, and Kerry J. Ressler 4 0. Current and Experimental Treatments for Anxiety Disorders Adam J. Guastella, Alice Norton, Gail A. Alvares, and Christine Yun Ju Song
409
S E C T I O N 5 S U B S TA N C E U S E D I S O R D E R S Antonelli Bonci and Nora Volkow 41. Epidemiology of Substance Use Disorders Denise B. Kandel, Mei-Chen Hu, Pamela C. Griesler, Bradley T. Kerridge, and Bridget F. Grant 42. The Genetic Basis of Addictive Disorders David Goldman, Zhifeng Zhou, and Colin Hodgkinson 43. Animal Models of Addiction Christopher J. Evans, Brigitte L. Kieffer, David Jentsch, and Rafael J. Maldonado 4 4. Reward Circuitry and Drug Addiction Vaughn R. Steele, Vani Pariyadath, Rita Z. Goldstein, and Elliot A. Stein 45. Molecular Neuroimaging in Addictive Disorders Edythe D. London and Chelsea L. Robertson 4 6. Cellular and Molecular Mechanisms of Addiction Kathryn J. Reissner and Peter W. Kalivas
451 471
477 487
513
531
577
587
601 617
S E C T I O N 6 DEMENTIA Alison M. Goate 50. Diagnosis and Epidemiology of Dementia 673 William C. Kreisl and Christiane Reitz 51. Genetics of Dementia 685 Alan E. Renton and Alison M. Goate 52. Neuroimaging and Cerebrospinal Fluid Biomarkers of Alzheimer’s Disease 703 Brian A. Gordon, Stephanie J.B. Vos, and Anne M. Fagan 53. Animal Models of Alzheimer’s Disease David Morgan 54. Cellular Mechanisms of Dementia: Animal and Human Studies Li Gan 55. Neurobiology of Lewy Body Dementias: Animal and Human Studies James E. Galvin and Jose Tomas Bras 56. Neurobiology of FTD: Animal and Human Studies Dah-eun Chloe Chung, Jeannette N. Stankowski, and Leonard Petrucelli 57. Current Treatments for Alzheimer’s Disease Mary Sano and Judith Neugroschil
• C o n t USA ent s 2018. Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford vi University Press - OSO, 07:33:17.
565
47. Brain Development and the Risk for Substance Abuse 631 Mary M. Heitzeg and B.J. Casey 48. Novel Approaches for Treating Addiction 643 Jane B. Acri and Phil Skolnick 49. Current Approved Pharmacotherapies for Substance Use Disorders 657 Alexis S. Hammond and Eric C. Strain
419
435
547
715
727
737 751
769
S E C T I O N 7 P E D I AT R I C P S YC H I AT R I C D I S O R D E R S Joseph D. Buxbaum 58. Diagnosis and Epidemiology of Pediatric Psychiatric Disorders Elise B. Robinson, Benjamin M. Neale, and Mark J. Daly 59. Genetics of Pediatric Psychiatric Disorders Silvia De Rubeis, M. Pilar Trelles, and Joseph D. Buxbaum 60. Neuroimaging in Pediatric Psychiatric Disorders Timothy P.L. Roberts and Luke Bloy 61. Animal and Cellular Models of Pediatric Psychiatric Disorders Elodie Drapeau, Hala Harony-Nicolas, and Jacqueline N. Crawley 62. Neurodevelopmental Mechanisms of Pediatric Psychiatric Disorders: Animal and Human Studies Silvia De Rubeis, Kathryn Roeder, and Bernie Devlin 63. Neurobiology of Autism Spectrum Disorder and Intellectual Disability: Animal and Human Studies Jesse Costales, Silvia De Rubeis, Jennifer Foss-Feig, Patrick R. Hof, Joseph D. Buxbaum, and Alexander Kolezvon 6 4. Neurobiology of Attention Deficit Hyperactivity Disorder: Animal and Human Studies Stephen V. Faraone, Pradeep G. Bhide, and Joseph Biederman
783
797 807
823
841
855
865
65. The Neurobiology of Tic Disorders and Obsessive- Compulsive Disorder: Animal and Human Studies Christopher Pittenger 66. Neurobiology of Eating Disorders: Animal and Human Studies Thomas Hildebrandt and Ashley Heywood 67. Novel Approaches for Treating Pediatric Psychiatric Disorders Supritha Prasad and Edwin H. Cook, Jr. 68. Current Treatments for Pediatric Psychiatric Disorders M. Pilar Trelles, Paige M. Siper, and Dorothy E. Grice
891
905 915
S E C T I O N 8 F U T U R E O F P S YC H I AT R I C D I AG N O S I S : TOWA R D P R E C I S I O N P S YC H I AT RY Dennis S. Charney 69. DSM-5 Overview and Goals Darrel A. Regier, Sarah E. Morris, and Susan K. Schultz 70. The Present and Future of Psychiatric Diagnosis Steven E. Hyman 71. The NIMH Research Domain Criteria Project: Toward Precision Medicine in Psychiatry Bruce N. Cuthbert 72. Computational Psychiatry and the Bayesian Brain Karl J. Friston and Raymond J. Dolan Index 975
C o n tPress e n tUSA s •- OSO, vii 2018. Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University 07:33:17.
879
935
941
947 963
CONTRIBUTOR S
Jane B. Acri, PhD Chief, Medication Discovery & Toxicology Branch Division of Therapeutics & Medical Consequences National Institute on Drug Abuse National Institutes of Health Bethesda, Maryland Schahram Akbarian, MD, PhD Friedman Brain Institute Departments of Psychiatry and Neuroscience Icahn School of Medicine Mount Sinai New York, New York
Michele A. Bertocci, PhD Department of Psychiatry University of Pittsburgh Western Psychiatric Institute and Clinic Pittsburgh, Pennsylvania Pradeep G. Bhide, PhD Florida State University College of Medicine Pediatric Psychopharmacology Unit of the Child Psychiatry Service Tallahassee, Florida
Lyonna F. Alcantara, MS Department of Psychology Texas A&M University College Station, Texas
Joseph Biederman, MD Pediatric Psychopharmacology Unit Child Psychiatry Service Massachusetts General Hospital Harvard Medical School Boston, Massachusetts
Gail A. Alvares, PhD Brain and Mind Centre Sydney Medical School University of Sydney Sydney, New South Wales, Australia
Cara E. Bigony, BA Department of Psychiatry McLean Hospital Harvard Medical School Belmont, Massachusetts
Alan Anticevic, PhD Department of Psychiatry Yale University School of Medicine NIAAA Center for the Translational Neuroscience of Alcoholism Abraham Ribicoff Research Facilities Connecticut Mental Health Center New Haven, Connecticut
Luke Bloy, PhD Lurie Family Foundations MEG Imaging Center Department of Radiology Children’s Hospital of Philadelphia Philadelphia, Pennsylvania
Peter A. Bandettini, PhD Principal Investigator National Institutes of Mental Health Bethesda, Maryland Deanna M. Barch, PhD Department of Psychological & Brain Sciences Department of Psychiatry Department of Radiology Washington University in St. Louis St. Louis, Missouri Mandakh Bekhbat, BA Department of Physiology Emory University School of Medicine Atlanta, Georgia
Carlos A. Bolaños-Guzmán, PhD Department of Psychology Texas A&M University College Station, Texas Antonelli Bonci, MD Scientific Director National Institute on Drug Abuse Baltimore, Maryland Ryan Bowman Department of Psychiatry Duke University School of Medicine Durham, North Carolina Jose Tomas Bras, PhD Department of Molecular Neuroscience UCL, Institute of Neurology
ix USA - OSO, 2018. Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press 07:33:17.
Kristen Brennand, PhD Associate Professor Genetics and Genomic Sciences, Neuroscience, Psychiatry Icahn School of Medicine at Mount Sinai New York, New York
Kelly P. Cosgrove, PhD Department of Radiology and Biomedical Imaging Department of Psychiatry Yale University New Haven, Connecticut
Katherine E. Burdick, PhD Professor of Psychiatry and Neuroscience Mount Sinai School of Medicine New York, New York
Jesse Costales, MD Seaver Autism Center for Research and Treatment Departments of Psychiatry and Neuroscience Icahn School of Medicine at Mount Sinai New York, New York
Richard E. Carson, PhD Department of Radiology and Biomedical Imaging Department of Biomedical Engineering Yale University New Haven, Connecticut B.J. Casey, PhD Professor of Psychology Yale University New Haven, Connecticut Alexander Charney, MD Instructor, Neuroscience Icahn School of Medicine at Mount Sinai New York, New York S. Cherkerzian, SCD Departments of Psychiatry and Medicine Harvard Medical School Brigham and Women’s Hospital Connors Center for Women’s Health & Gender Biology Boston, Massachusetts Andrew Chess, MD Department of Developmental and Regenerative Biology Icahn School of Medicine Mount Sinai New York, New York Dah-eun Chloe Chung, BA Department of Neuroscience Mayo Clinic Neurobiology of Disease Mayo Clinic Graduate School of Biomedical Sciences Rochester, Maine Chiara Cirelli, PhD Professor, Department of Psychiatry Neuroscience Training Program University of Wisconsin-Madison Madison, Wisconsin Edwin H. Cook, Jr, MD, IJR Department of Psychiatry University of Illinois at Chicago Chicago, Illinois
Jacqueline N. Crawley, PhD Robert E. Chason Endowed Chair in Translational Research MIND Institute Professor, Department of Psychiatry and Behavioral Neuroscience University of California Davis School of Medicine Sacramento, California Bruce N. Cuthbert, PhD Department of Psychiatry University of Pittsburgh Pittsburgh, Pennsylvania Mark J. Daly, PhD Analytic and Translational Genetics Unit Massachusetts General Hospital Program in Medical and Population Genetics Broad Institute of MIT and Harvard Boston, Massachusetts Silvia de Rubeis, PhD Seaver Autism Center for Research and Treatment Department of Psychiatry Icahn School of Medicine at Mount Sinai New York, New York Karl Deisseroth, MD, PhD Howard Hughes Medical Institute Departments of Bioengineering and Psychiatry Stanford University Stanford, California Bernie Devlin, PhD Department of Statistics Carnegie Mellon University Department of Psychiatry University of Pittsburgh School of Medicine Pittsburgh, Pennsylvania Samuel J. Dienel, MD Department of Psychiatry University of Pittsburgh Pittsburgh, Pennsylvania Raymond J. Dolan, FRS Wellcome Trust Centre for Neuroimaging Institute of Neurology University College London London, England, UK
x •University C o n tPress r i bUSA u to r s2018. Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford - OSO, 07:33:17.
Elodie Drapeau, PhD Seaver Autism Center for Research and Treatment Department of Psychiatry Friedman Brain Institute Icahn School of Medicine at Mount Sinai New York, New York Ronald S. Duman, PhD Laboratory of Molecular Psychiatry Departments of Psychiatry and Pharmacology Yale University School of Medicine Connecticut Mental Health Center New Haven, Connecticut Kafui Dzirasa, MD, PhD Department of Psychiatry Duke University School of Medicine Durham, North Carolina Amit Etkin, MD, PhD Associate Professor of Psychiatry and Behavioral Sciences Stanford University School of Medicine Stanford, California Christopher J. Evans, PhD UCLA Brain Research Institute University of California, Los Angeles Los Angeles, California Anne M. Fagan, PhD The Knight Alzheimer’s Disease Research Center Department of Neurology Washington University in St. Louis St. Louis, Missouri Stephen V. Faraone, PhD Department of Psychiatry SUNY Upstate Medical University Center for Brain Repair Department of Biomedical Sciences Syracuse, New York Adriana Feder, MD Associate Professor of Psychiatry Associate Director for Research World Trade Center Mental Health Program Icahn School of Medicine at Mount Sinai New York, New York Lief E. Fenno, MD, PhD Howard Hughes Medical Institute Departments of Bioengineering and Psychiatry Stanford University Stanford, California Jennifer Foss-Feig, PhD Seaver Autism Center for Research and Treatment Departments of Psychiatry and Neuroscience Icahn School of Medicine at Mount Sinai New York, New York
Karl J. Friston, FRS, FMedSci, FRSB Wellcome Trust Centre for Neuroimaging Institute of Neurology University College London London, England, UK James E. Galvin, MD, MPH Comprehensive Center for Brain Health Charles E. Schmidt College of Medicine Florida Atlantic University Boca Raton, Florida Nao J. Gamo, PhD Department of Psychiatry and Behavioral Sciences Johns Hopkins University School of Medicine Baltimore, Maryland Li Gan, PhD Gladstone Institutes University of California, San Francisco San Francisco, California Mark S. George, MD Departments of Psychiatry, Radiology, and Neuroscience Medical University of South Carolina Ralph H. Johnson VA Medical Center Charleston, South Carolina Alison M. Goate, D.Phil Ronald M. Loeb Center for Alzheimer’s Disease Department of Neuroscience Icahn School of Medicine at Mount Sinai New York, New York David Goldman, MD Clinical Assistant Professor Department of Psychiatry NYU Langone Health New York University New York, New York Jill M. Goldstein, PhD Departments of Psychiatry and Medicine Harvard Medical School Brigham and Women’s Hospital Connors Center for Women’s Health & Gender Biology BWH, departments of Psychiatry and Medicine Boston, Massachusetts Rita Z. Goldstein, PhD Departments of Psychiatry & Neuroscience Icahn School of Medicine at Mount Sinai New York, New York Madeleine S. Goodkind, PhD University of California, Berkeley Berkeley, California Wayne K. Goodman, MD Menninger Department of Psychiatry and Behavioral Sciences Baylor College of Medicine Houston, Texas
Co n t r iPress b u to • xi Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University USAr- sOSO, 2018. 07:33:17.
Brian A. Gordon, PhD Department of Radiology The Knight Alzheimer’s Disease Research Center Washington University in St. Louis St. Louis, Missouri
Stephan Heckers, MD Director, Vanderbilt Early Psychosis Program Department of Psychiatry Vanderbilt University Medical Center Nashville, Tennessee
Bridget F. Grant, PhD National Institutes of Health Bethesda, Maryland
Mary M. Heitzeg, PhD Department of Psychiatry University of Michigan Ann Arbor, Michigan
Seth G. N. Grant Centre for Clinical Brain Sciences The University of Edinburgh Edinburgh, Scotland, UK Dorothy E. Grice, MD Division of Tics, OCD and Other Related Disorders Department of Psychiatry Icahn School of Medicine at Mount Sinai New York, New York Pamela C. Griesler Department of Psychiatry Mailman School of Public Health Columbia University School of Medicine New York, New York Adam J. Guastella, PhD Brain and Mind Centre Sydney Medical School University of Sydney Sydney, New South Wales, Australia Stephen J. Haggarty, PhD Associate Professor Department of Neurology Harvard Medical School Boston, Massachusetts Margaret Haglund, MD Department of Psychiatry & Behavioral Neurosciences Cedars-Sinai Medical Group Beverly Hills, California Alexis S. Hammond, MD, PhD Behavioral Pharmacology Research Unit Department of Psychiatry and Behavioral Sciences Johns Hopkins University School of Medicine Baltimore, Maryland R.J. Handra, PhD Department of Biomedical Sciences Colorado State University Fort Collins, Colorado Hala Harony-Nicolas, PhD Seaver Autism Center for Research and Treatment Department of Psychiatry Friedman Brain Institute Icahn School of Medicine at Mount Sinai New York, New York
John M. Hettema, MD, PhD Department of Psychiatry Virginia Institute for Psychiatric and Behavioral Genetics Virginia Commonwealth University Richmond, Virginia Ashley Heywood, BS Icahn School of Medicine at Mount Sinai New York, New York Thomas Hildebrandt, PsyD Icahn School of Medicine at Mount Sinai New York, New York Ansel T. Hillmer, PhD Department of Radiology and Biomedical Imaging Department of Psychiatry Yale University New Haven, Connecticut Georgia E. Hodes, PhD Fishberg Department of Neuroscience Friedman Brain Institute Icahn School of Medicine Mount Sinai New York, New York Colin Hodgkinson, PhD Section of Human Neurogenetics National Institute on Alcohol Abuse and Alcoholism National Institutes of Health Bethesda, Maryland Patrick R. Hof, MD Seaver Autism Center for Research and Treatment Departments of Psychiatry and Neuroscience Icahn School of Medicine at Mount Sinai New York, New York L. Holsen, PhD Departments of Psychiatry and Medicine Harvard Medical School Brigham and Women’s Hospital Connors Center for Women’s Health & Gender Biology BWH, departments of Psychiatry and Medicine Boston, Massachusetts Sarah R. Horn Department of Psychology University of Oregon Eugene, Oregon
xii •University C o n Press trib u to r s2018. Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford USA - OSO, 07:33:17.
Mei-Chen Hu, PhD Associate Research Scientist Department of Psychiatry Columbia University Medical Center New York, New York Rainbo Hultman, PhD Department of Psychiatry Duke University School of Medicine Durham, North Carolina Steven E. Hyman, MD Director, Stanley Center for Psychiatric Research Broad Institute of MIT and Harvard Boston, Massachusetts Brian M. Iacoviello, PhD Mood and Anxiety Disorders Program Department of Psychiatry Icahn School of Medicine Mount Sinai New York, New York Hanna Jaaro-Peled, PhD Department of Psychiatry and Behavioral Sciences Johns Hopkins University School of Medicine Baltimore, Maryland David Jentsch, PhD Professor of Psychiatry Binghamton University, State University of New York Binghamton, New York Peter W. Kalivas, PhD Department of Neurosciences Medical University of South Carolina Charleston, South Carolina
Brigitte L. Kieffer, PhD Scientific Director Douglas Institute Professor Department of Psychiatry McGill University Chair McGill University Montreal, Canada Alexander Kolezvon, MD Seaver Autism Center for Research and Treatment Departments of Psychiatry and Neuroscience Icahn School of Medicine at Mount Sinai New York, New York William C. Kreisl, MD Taub Institute for Research on Alzheimer’s Disease and the Aging Brain Department of Neurology College of Physicians and Surgeons Columbia University New York, New York John H. Krystal, MD Departments of Psychiatry and Neuroscience Yale University School of Medicine Behavioral Health services New Haven Hospital New Haven, Connecticut Clinical Neuroscience Division VA National Center for PTSD VA Connecticut Healthcare System West Haven, Connecticut Joseph LeDoux, PhD New York University New York, New York
Denise B. Kandel, PhD Professor of Sociomedical Sciences in Psychiatry Department of Psychiatry & Mailman School of Public Health Columbia University New York, New York
Francis S. Lee, MD, PhD Sackler Institute for Developmental Psychobiology Weill Cornell Medical College of Cornell University New York, New York
Shitij Kapur, FRCPC, PhD, FMedSci Dean, Faculty of Medicine, Dentistry, and Health Sciences Assistant Vice-Chancellor (Health) University of Melbourne Melbourne, Victoria, Australia
Douglas F. Levinson, MD Professor of Psychiatry Department of Psychiatry Stanford University Palo Alto, California
Milissa L. Kaufman, MD, PhD Department of Psychiatry McLean Hospital Harvard Medical School Belmont, Massachusetts
David A. Lewis, MD Department of Psychiatry University of Pittsburgh Pittsburgh, Pennsylvania
Meghan E. Keough, PhD University of Washington, Seattle Seattle, Washington Bradley T. Kerridge, MD National Institutes of Health Bethesda, Maryland
Anfei Li Sackler Institute for Developmental Psychobiology Department of Psychiatry Weill Cornell Medical College of Cornell University New York, New York
C oUniversity n t r i bPress u to r -sOSO, • xiii Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford USA 2018. 07:33:17.
Edythe D. London, PhD Department of Molecular and Medical Pharmacology Department of Psychiatry and Biobehavioral Sciences David Geffen School of Medicine Brain Research Institute University of California Los Angeles Los Angeles, California Hanzhang Lu, PhD Professor of Radiology and Radiological Science Johns Hopkins University School of Medicine Baltimore, Maryland Dolores Malaspina, MD Department of Psychiatry Columbia University Medical Center New York, New York Rafael J. Maldonado, MD, PhD Department of Experimental and Health Sciences University Pompeu Fabra Barcelona, Catalunya, Spain Anil K. Malhotra, MD Professor, The Center for Psychiatric Neuroscience The Feinstein Institute for Medical Research Director, Psychiatry Research Zucker Hillside Hospital Professor, Molecular Medicine and Psychiatry Hofstra Northwell School of Medicine New York, New York Tiago Reis Marques, MD, PhD Department of Psychosis Studies King’s College London London, England, UK Helen Mayberg, MD Professor of Psychology, Neurology, and Radiology Dorothy C. Fucqua Chair Psychiatric Neuroimaging and Therapeutics Department of Psychiatry and Behavioral Sciences Emory University School of Medicine Atlanta, Georgia Caroline Ménard, PhD Fishberg Department of Neuroscience Friedman Brain Institute Icahn School of Medicine at Mount Sinai New York, New York Emma Meyer, MD Department of Psychiatry New York University School of Medicine New York, New York Guo-Li Ming, MD, PhD Johns Hopkins University School of Medicine Baltimore, Maryland
M. Misra, MD, MPH Departments of Psychiatry and Medicine Harvard Medical School Brigham and Women’s Hospital Connors Center for Women’s Health & Gender Biology BWH, departments of Psychiatry and Medicine Boston, Massachusetts Lisa M. Monteggia, PhD Department of Neuroscience UT Southwestern Medical Center Dallas, Texas David Morgan, PhD CEO, Byrd Alzheimer’s Institute Distinguished Professor of Pharmacology and Physiology University of South Florida Tampa, Florida Sarah E. Morris, PhD Chief, Adult Psychopathology and Psychosocial Intervention Development Branch Associate Head, RDoC Unit Program Officer, Schizophrenia Spectrum Disorders Program National Institute of Mental Health Bethesda, Maryland James W. Murrough, MD Mood and Anxiety Disorders Program Department of Psychiatry Fishberg Department of Neuroscience Friedman Brain Institute Icahn School of Medicine Mount Sinai New York, New York Benjamin M. Neale, PhD Analytic and Translational Genetics Unit Massachusetts General Hospital Program in Medical and Population Genetics Broad Institute of MIT and Harvard Stanley Center for Psychiatric Research Broad Institute of MIT and Harvard Boston, Massachusetts Gretchen N. Neigh, PhD Departments of Anatomy and Neurobiology Virginia Commonwealth University Richmond, Virginia Judith Neugroschil, MD Alzheimer’s Disease Research Center Icahn School of Medicine at Mount Sinai New York, New York
• C o nPress xiv University t r i USA b u to r s2018. Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford - OSO, 07:33:17.
Walter E. Nichols, MD Professor in the School of Medicine Department of Psychiatry Program on the Genetics of Brain Function Stanford University Palo Alto, California Alice Norton, PhD Brain and Mind Centre Sydney Medical School University of Sydney Sydney, New South Wales, Australia Dost Öngür, MD, PhD Chief, Psychotic Disorders Division Director, Schizophrenia and Bipolar Disorder Research Program McLean Hospital Associate Professor of Psychiatry Harvard Medical School Boston, Massachusetts Luz H. Ospina, MA, PhD Icahn School of Medicine at Mount Sinai New York, New York Takeshi Otowa, MD, PhD Graduate School of Clinical Psychology Teikyo Heisei University Tokyo, Japan Eric M. Parise, PhD Fishberg Department of Neuroscience The Mount Sinai School of Medicine New York, New York Vani Pariyadath, PhD National Institute on Drug Abuse Bethesda, Maryland Roy H. Perlis, MD, MSc Professor of Psychiatry Harvard Medical School Director, Center for Experimental Drugs and Diagnostics Center for Genomic Medicine Massachusetts General Hospital Boston, Massachusetts Leonard Petrucelli, PhD Department of Research, Neuroscience Mayo Clinic College of Medicine Jacksonville, Florida Madeline L. Pfau, PhD Fishberg Department of Neuroscience Friedman Brain Institute Icahn School of Medicine Mount Sinai New York, New York
Mary L. Phillips, MD Department of Psychiatry University of Pittsburgh Western Psychiatric Institute and Clinic Pittsburgh, Pennsylvania Christopher Pittenger, MD, PhD Department of Psychiatry Yale University New Haven, Connecticut Mikhail V. Pletnikov, MD, PhD Johns Hopkins University School of Medicine Baltimore, Maryland Supritha Prasad, IJR Department of Psychiatry University of Illinois at Chicago Chicago, Illinois Shaun M. Purcell, PhD Associate Professor, Psychiatry Associate Professor, Genetics and Genomic Sciences Icahn School of Medicine at Mount Sinai New York, New York Darrel A. Regier, MD, MPH Center for the Study of Traumatic Stress Department of Psychiatry Uniformed Services University Bethesda, Maryland Kathryn J. Reissner, PhD Department of Psychology & Neuroscience University of North Carolina at Chapel Hill Chapel Hill, North Carolina Christiane Reitz, MD, PhD Taub Institute for Research on Alzheimer’s Disease and the Aging Brain Department of Neurology Gertrude H. Sergievsky Center Department of Epidemiology Mailman School of Public Health College of Physicians and Surgeons Columbia University New York, New York Alan E. Renton, PhD Ronald M. Loeb Center for Alzheimer’s Disease Department of Neuroscience Icahn School of Medicine at Mount Sinai New York, New York Kerry J. Ressler, MD, PhD Department of Psychiatry McLean Hospital Harvard Medical School Belmont, Massachusetts Department of Psychiatry and Behavioral Sciences Emory University School of Medicine Atlanta, Georgia
Co n t r i Press b u to • xv Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University USAr-sOSO, 2018. 07:33:17.
Roxann Roberson-Nay, PhD Departments of Psychiatry and Psychology Virginia Institute for Psychiatric and Behavioral Genetics Virginia Commonwealth University Richmond, Virginia Timothy P.L. Roberts, PhD Lurie Family Foundations MEG Imaging Center Department of Radiology Children’s Hospital of Philadelphia Philadelphia, Pennsylvania Chelsea L. Robertson, PhD Department of Molecular and Medical Pharmacology Department of Psychiatry and Biobehavioral Sciences David Geffen School of Medicine University of California Los Angeles Los Angeles, California Elise B. Robinson, ScD Analytic and Translational Genetics Unit Massachusetts General Hospital Boston, Massachusetts Kathryn Roeder, PhD Computational Biology Department Carnegie Mellon University Pittsburgh, Pennsylvania Christopher A. Ross, MD Johns Hopkins University School of Medicine Baltimore, Maryland Peter P. Roy-Byrne, MD Professor Emeritus, Department of Psychiatry University of Washington School of Medicine Seattle, Washington Scott J. Russo, PhD Fishberg Department of Neuroscience Friedman Brain Institute Icahn School of Medicine Mount Sinai New York, New York Takeshi Sakurai, MD, PhD Department of Drug Discovery Medicine Medical Innovation Center Kyoto University Graduate School of Medicine Kyoto, Japan Mary Sano, PhD Alzheimer’s Disease Research Center Icahn School of Medicine at Mount Sinai New York, New York James J. Peters VAMC Bronx, New York
Deepak K. Sarpal, MD Assistant Professor of Psychiatry Department of Psychiatry University of Pittsburgh Pittsburgh, Pennsylvania Akira Sawa, MD, PhD Department of Psychiatry and Behavioral Sciences Johns Hopkins University School of Medicine Baltimore, Maryland Eric E. Schadt, PhD Department of Genetics and Genomic Sciences Mount Sinai School of Medicine New York, New York Susan K. Schultz, MD DFAPA Geriatric Psychiatry, James A. Haley Veterans Hospital Professor of Psychiatry, Courtesy University of South Florida College of Medicine Adjunct Professor of Psychiatry University of Iowa Carver College of Medicine Tampa, Florida Hannah Schwennesen, MD Department of Psychiatry Duke University School of Medicine Durham, North Carolina Nicolas Singewald, PhD Department of Pharmacology and Toxicology Inst. Pharmacy and CMBI University of Innsbruck Innsbruck, Austria Paige M. Siper, PhD Seaver Autism Center for Research and Treatment Department of Psychiatry Icahn School of Medicine at Mount Sinai New York, New York Phil Skolnick, PhD, DSC (Hon) Director Division of Therapeutics & Medical Consequences National Institute on Drug Abuse National Institutes of Health Bethesda, Maryland Christine Yun Ju Song, PhD Brain and Mind Centre Sydney Medical School University of Sydney Sydney, New South Wales, Australia Steven M. Southwick, MD Glenn H. Greenberg Professor of Psychiatry Yale University School of Medicine New Haven, Connecticut Jeannette N. Stankowski, PhD Department of Neuroscience Mayo Clinic College of Medicine Jacksonville, Florida
• C o nPress xvi University t r i USA b u to r s2018. Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford - OSO, 07:33:17.
Vaughn R. Steele, PhD Neuroimaging Research Branch National Institute of Drug Abuse Intramural Research Program National Institutes of Health Baltimore, Maryland
Nicholas T. Van Dam, PhD Mood and Anxiety Disorders Program Department of Psychiatry Icahn School of Medicine Mount Sinai New York, New York
Elliot A. Stein, PhD Neuroimaging Research Branch National Institute of Drug Abuse Intramural Research Program National Institutes of Health Baltimore, Maryland
Nora Volkow, MD Senior Investigator, Laboratory of Neuroimaging National Institute on Alcohol Abuse and Alcoholism Director, National Institute on Drug Abuse Rockville, Maryland
Murray B. Stein, MD, MPH, FRCPC Distinguished Professor, Psychiatry Distinguished Professor, Family Medicine and Public Health Vice Chair for Clinical Research in Psychiatry University of California, San Diego San Diego, California Eric C. Strain, MD Behavioral Pharmacology Research Unit Department of Psychiatry and Behavioral Sciences Johns Hopkins University School of Medicine Baltimore, Maryland David A. Sturman, MD, PhD Department of Psychiatry McLean Hospital Harvard Medical School Belmont, Massachusetts MGH/McLean Adult Psychiatry Residency Program Harvard Medical School Boston, Massachusetts Ramon Tasan, PhD Department of Pharmacology Medical University Innsbruck Innsbruck, Austria Giulio Tononi, MD, PhD Professor, Department of Psychiatry Neuroscience Training Program University of Wisconsin-Madison Madison, Wisconsin M. Pilar Trelles, MD Seaver Autism Center for Research and Treatment Department of Psychiatry Icahn School of Medicine at Mount Sinai New York, New York
Stephanie J.B. Vos, PhD Department of Psychiatry and Neuropsychology Alzheimer Center Limburg School for Mental Health and Neuroscience Maastricht University Maastricht, the Netherlands Julie Walsh-Messinger, MA, PhD Assistant Professor Department of Psychiatry University of Dayton Dayton, Ohio Neil Woodward, PhD Vanderbilt Early Psychosis Program Department of Psychiatry Vanderbilt University Medical Center Nashville, Tennessee Wei Xu, PhD Department of Neuroscience UT Southwestern Medical Center Dallas, Texas Jared W. Young, PhD Department of Psychiatry University of California San Diego La Jolla, California Desert-Pacific Mental Illness Research Education and Clinical Center VA San Diego Healthcare System San Diego, California Zhifeng Zhou, PhD Section of Human Neurogenetics National Institute on Alcohol Abuse and Alcoholism Bethesda, Maryland
C oUniversity n t r i bPress u to r s- OSO, • xvii Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford USA 2018. 07:33:17.
Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press USA - OSO, 2018. 07:33:17.
SECTION 1 EMERGING AND ESTABLISHED TECHNOLOGIES
Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press USA - OSO, 2018. 07:33:44.
Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press USA - OSO, 2018. 07:33:44.
1. GENETIC METHODOLOGIES AND APPLICATIONS Shaun M. Purcell
INTRODUCTION The past decade has witnessed tremendous advances in the molecular technologies and data-analytic methods at our disposal for studying the genetic bases of complex diseases and traits. These advances have enabled the creation of comprehensive catalogs of different forms of human genetic variation, as well as large-scale studies focused on specific diseases or traits. In this chapter, we outline the general principles behind some of these advances and discuss their application to studying complex traits, with a focus on neuropsychiatric disease. M OT I VAT I O N S F O R M A P P I N G T H E G E N ET I C BASIS OF DISEASE Genetic epidemiology is fundamentally concerned with relating genotype (i.e., variation between individuals’ genomes) to phenotype (i.e., the presence or absence of a disease, or measure of a trait such as height or cholesterol level) (Altshuler et al., 2008). There are a number of relatively distinct motivations for this work, which can be conceived of both in terms of proximal and distal goals of the research. Recently, there has been a great deal of focus on identifying specific alleles (variable forms of a locus, which is a gene or region) that “explain the heritability” as a primary benchmark and major goal of genetic studies, as discussed later. For many downstream applications, however, perhaps an equally important, but distinct, proximal goal of genetics is to point to the genes and/or gene networks that are causally associated with disease. Following from these proximal goals (identifying the specific alleles that explain heritability and identifying the relevant genes and pathways) there are several distinct, more distal goals or applications, the success of which will depend on different aspects of the genetic discoveries made. In theory, understanding the genetics of a disease could be used for risk prediction, either at the population level or within families (following the model of genetic counseling for Mendelian disease); for prediction of disease course, severity, or drug response in affected individuals; to identify targets for drug discovery research; to inform on the relationships and comorbidities between different diseases; or even to provide a framework for causal inference around environmental effects (Smith and Ebrahim, 2003). More generally, advances in understanding
disease genetics will ultimately, but undoubtedly, provide fundamental insights into human biology, development, and evolution. However, the ease with which genetics will achieve success in these various applications relates to different aspects of the unknown, underlying genetic architecture of any particular disease or trait. The question of the genetic architecture of common disease has been a central one: it relates to the types of approaches that will work best to map genes, as well as to what we can expect to learn from genetic studies in the near future. For a heritable disease, genetic architecture describes how many independent genetic effects contribute to risk, at the level of both the population and the specific individual; it also describes the typical frequency and effect size of these variants, how they combine to produce a phenotype (e.g., additively or interactively), and the extent to which multiple genetic risk factors for a disease coalesce into a smaller number of distinct biological pathways or networks. Other aspects of genetic architecture include the mode of inheritance (e.g., recessive effects), the presence of positive, negative, or balancing selection acting on risk variants, the extent to which genetic effects are shared (or contribute to different disease rates) across populations, the extent to which variants influence multiple outcomes through pleiotropy (one gene having multiple downstream effects), and the extent to which genetic effects are moderated by environmental exposures (gene–environment interaction). The success of risk prediction, for example, in the general population will be crucially dependent on the proportion of variance explained by detected variants, which is a function of both the frequency and penetrance (a measure of effect size that equals the chance that a carrier develops disease) of risk alleles. By learning which specific alleles (the particular variants of genes) increase or decrease risk or type or course of disease, one can in theory predict an individual’s risk or provide tailored medical treatment to patients based on their genotype. In practice, truly personalized genomic medicine is still only a long-term goal in most instances rather than a current or imminent reality, although this is likely to be an area of great progress over the coming decade. However, inasmuch as the distal goals relate to identifying loci, to point to potential drug targets, for example, the extent to which detected variants account for heritability might not be critically relevant: for instance, there are multiple examples of genetic studies that have pointed to weak genetic effects in genes that are already known targets of existing, successful therapies.
3 USA - OSO, 2018. Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press 07:33:44.
Thus, genetic studies have a parallel set of aims that are almost orthogonal to the goal of explaining variability in a population, involving the identification of the networks of genes implicated in disease. Here the aim is to use this information to point to the biological mechanisms involved in disease pathogenesis. C L A S S I C A L G E N ET I C E P I D E M I O L O GY: F R O M FA M I LY S T U D I E S , S E G R E G AT I O N, A N D L I N K AG E A N A LYS I S TO L I N K AG E DISEQUILIBRIUM M APPING Classical genetic epidemiology posed a series of increasingly specific questions: For a particular disease or trait, are there genetic influences? Is the genetic basis simple or complex? Where are those genes located? Which specific forms of the gene cause disease? The tools to answer these questions were, respectively, family and twin studies, segregation analysis, linkage analysis, and association analysis. Twin and family studies are used primarily to estimate the heritability of a trait (the extent to which variation in outcome is due to variation in genes) by contrasting the phenotypic similarity of relatives of differing genetic similarity. More recently, twin and family study designs have also proved useful in molecular studies of genetic and epigenetic variation (van Dongen et al., 2012). One notable family study of schizophrenia and bipolar disorder involved tens of thousands of patients from Sweden and showed clear evidence for a shared genetic basis common to both disorders (Lichtenstein et al., 2009). Looking at a range of first-degree relative classes, such studies estimate the probandwise concordance rate (the probability an individual develops disease given they have an affected relative of a particular type) and the familial relative risk (λ), which, for a given class of relative, is the concordance rate divided by the population prevalence of disease. Both approaches ask how much more likely an individual is to develop disease if he or she has an affected relative. Estimates of λ for MZ twins, full siblings, parent–offspring pairs, and half-siblings track strongly with the extent of genetic similarity in those pairs, indicative of a considerable genetic basis for these diseases. This and other studies put the heritability of schizophrenia to be very high, with estimates from 60% to 80%, for example. Segregation analysis considers the broader pattern of disease within larger pedigrees. For Mendelian disease, segregation analysis can estimate whether there is likely to be a single disease allele in each family, and if so, its mode of inheritance. For complex diseases that are caused by multiple genes and environmental influences, segregation analysis is typically uninformative (beyond demonstrating above- chance levels of familial clustering). Linkage analysis also uses pedigrees to identify (very broad) chromosomal loci that cosegregate with disease in a particular family. Linkage analysis primarily gained popularity after the introduction of molecular marker maps in the 1980s. For example, by genotyping 300–4 00 “microsatellite” markers (short tandem repeats that vary in length between individuals), one can infer the pattern of gene flow in a family (specifically, of shared chromosomal regions coinherited from a single ancestor and so identical-by-descent, IBD) and
then search for chromosomal positions at which the profile of IBD maximally correlates with the coinheritance pattern of the phenotype. Linkage analysis proved spectacularly useful in mapping Mendelian disease genes of major effect: rare mutations that almost always lead to correspondingly rare diseases. In contrast, for complex common diseases, linkage analysis has yielded very few durable results (for neuropsychiatric disease, one notable exception is the DISC1 locus). This is, in large part, because linkage analysis has low power to detect variants of only modest effect. Given that it has, in fact, been widely applied for many complex diseases, including schizophrenia, the failure of linkage analysis suggests that the genetic architecture of most common diseases is unlikely to contain any real “hotspots”—genes or loci at which a sizeable proportion of cases carry a highly (or even moderately) penetrant risk variant. Association analysis (or linkage disequilibrium mapping) has replaced linkage analysis as the workhorse of genetic epidemiology over the past decade. Association analysis is conceptually straightforward: typically in populations of unrelated individuals, association analysis simply looks for specific variants (alleles) that are significantly more frequent in people with the disease compared with those without. Compared with linkage analysis, this approach is more powerful to detect variants of smaller effect (Risch and Merikangas, 1996). To contrast the effect sizes expected for a “major gene” disorder versus a complex, common disease, consider that for a rare disease, say, affecting 1 in 10,000 individuals, a major gene effect may increase risk more than 10,000-fold: for example, if baseline risk in noncarriers of the gene is 0.00003, then the penetrance (risk of disease given genotype) would be 30% or more. In this scenario, even though the gene is not completely Mendelian (deterministic in its effect), a very large proportion (more than one third) of carriers will develop the disease. Conversely, a very large proportion of all affected individuals will carry that particular disease allele (again, more than one third). In comparison, for a common disease with a population prevalence of 1 in 100 individuals, researchers expect effect sizes for common alleles to be at most 1.2-fold, rather than 10,000-fold increases in risk. If a 1.2-fold risk allele has a population frequency of, say, 40%, it implies that carriers have ~1.2% risk of developing disease, and we would expect to see the allele in ~44% of cases compared to ~40% of unaffected individuals. This relatively small difference means that the variant is harder to detect statistically. It also means that this allele, by itself, will have very little predictive utility: in other words, knowing an individual’s genotype at this locus would only marginally improve one’s ability to predict whether or not the individual will develop disease. Of course, for a heritable disease we would expect many such loci to contribute to disease risk, which could be informative for prediction if analyzed collectively. Historically, the principal limitation in applying association analysis broadly was that testing a specific marker for association only queries a tiny proportion of the total extent of variability that exists genome-wide. This arises from the properties of linkage disequilibrium in human populations, as described later. In contrast, linkage analysis only requires a relatively modest number of molecular markers to provide genome-wide surveys of gene flow within families, albeit very
4 • S. ECharney, merging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis et al., Oxford University Press USA - OSO,T2018. 07:33:44.
low resolution ones (because very large chunks of chromosome are shared between closely related individuals). For association studies, it became apparent that hundreds of thousands of markers would be needed to cover the whole genome and capture the majority of common variation. In practice, for a long time this meant that association analysis was limited to testing a small number of variants in a small number of candidate genes. Candidates were usually selected on the basis of prior knowledge, or assumptions, about the pathophysiology of disease. In neuropsychiatric genetics, despite a considerable body of work, studies of candidate genes largely failed to lead to broadly reproducible results. There are multiple reasons to explain this state of affairs (reviewed by Kim et al., 2011). Perhaps most obviously, many of the original hypotheses about the disease may have been incorrect, or at least fundamentally incomplete descriptions of a much more complex process. For a number of diseases such as Type II diabetes and Crohns’ disease, the biology pointed to by recent, robust genetic findings from genome-wide association studies (described later) has often been at odds with the prior assumptions about what would be genetically important. Of course, this is actually a good thing from the perspective of genetic studies, inasmuch as we strive for genetics to be a source of novel insights and hypotheses. Typically error rates in candidate genes studies were high, too: false positives (Type I errors in hypothesis testing) were hard to control, given varying degrees of multiple testing, and false negatives (Type II errors) were also likely as sample sizes used for most candidate gene studies were typically very small by today’s standards. For schizophrenia, as of 2011, 732 autosomal genes had been tested by 1,374 hypothesis-driven candidate gene studies, although most genes were investigated in only one (61%) or two (16%) studies (Kim et al., 2011). Typically no replication was attempted, or it was underpowered, or the statistical evidence was hard to reconcile with the literature. For example, often different markers in the same gene were tested across different studies, or replication was claimed but the direction of effect differed between studies. Furthermore, genetic variation in candidate genes was typically only very poorly captured, even for common variation, often with only one or two markers being genotyped per gene. E X PA N D I N G K N OW L E D G E OF THE HUM AN GENOME Reference maps and databases have been critical in many areas of genomics, from the human genome reference sequence itself to maps of coding and other functional elements in the sequence. Equally important for disease and population genetics has been the more recent construction of maps, or catalogs, of observed variation within and between different human populations. The two most notable efforts are the International HapMap project (International HapMap Consortium, 2007) and the 1000 Genomes Project (1000 Genomes Consortium, 2010). The HapMap project employed large-scale genotyping to type almost 4 million known single- nucleotide polymorphisms (SNPs) in 270 individuals of African, Asian, and European ancestry. As well as generating lists of technically validated
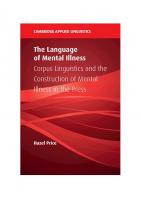
polymorphic sites along with estimates of allele frequencies in multiple populations, a central aim was to characterize and describe the patterns of correlation between nearby variants, referred to as linkage disequilibrium (LD). As illustrated in Figure 1.1, two or more alleles at nearby sites are said to be in LD if they co-occur more than expected by chance, that is, than if they were inherited independently of each other. In reality, haplotypes (collections of alleles on the same physical stretch of chromosome) are the primary unit of inheritance, not individual alleles. Two alleles on the same haplotype will tend to be either both cotransmitted from parent to offspring, or will both be untransmitted, thereby inducing a correlation between the alleles at the population level. The further away two sites physically reside on the chromosome, the more likely that they will be separated by a meiotic recombination event. Thus, LD between any two sites tends to “break down,” or be attenuated, over distance. This property can be used to localize genes, in that it implies that two sites that are in LD are also likely to be physically colocated on the same stretch of chromosome. This is the principle behind linkage disequilibrium mapping. Obtaining genotype data on an individual for two nearby heterozygous sites does not directly reveal the underlying haplotypes carried by that individual, although in families the haplotype can often be inferred straightforwardly. For example, if the individual carries an A/C (heterozygous) genotype for the first site and G/T for the second, there are two possible haplotypic configurations: that the AG haplotype was inherited from one parent and therefore CT from the second, or that AT was inherited from the first and CG from the second. The process of resolving which configuration is more likely is called phasing. As in Figure 1.1, phase is often unambiguous when one studies multiple members of the same family. Alternatively, statistical approaches (based on algorithms such as expectation maximization [EM] or Markov Chain Monte Carlo [MCMC] and population genetic models) can be used to resolve phase in samples of unrelated individuals by considering the observed correlation between sites and treating the unknown phase information statistically in terms of a missing- data problem (Browning and Browning, 2012). In some situations it is also possible to use sequencing to type haplotypes directly, using molecular rather than statistical means, sequencing along the same physical stretch of chromosome. The actual structure and extent of LD in humans reflects both demographic factors and the history of the population studied and biological properties of the genome, influencing the rate of recombination at particular sites. The typical structure and extent of LD is of critical importance to the implementation of association analysis as applied to large genomic regions. Fundamentally, association mapping (sometimes known as linkage disequilibrium mapping, as previously noted) relies on the fact that by testing a particular variant, one is implicitly testing a host of nearby variants for which the genotyped markers act as proxies, or tags. The HapMap project provides a comprehensive empirical description of the typical profiles of LD in the populations studied. To a first approximation, patterns of LD can be well characterized by “haplotype blocks,” meaning that there are regions of the genome (very variable in size, but often on the order of 10 to
1. G enetic ethodologies and pplications Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, etM al., Oxford University Press USA - OSO,A2018. 07:33:44.
Unphased genotypes
(a)
A/A G/T
Resolved haplotypic phase
A/C G/G
A G
C G
A T
A T
A/C G/T
A G
C G
(b)
A/A G/T
A/C G/G
C/C G/G
Estimated haplotype frequencies from a population
C/C G/G
A/A T/T
R2 = 0.351 Haplotype
C/A G/T
A/A G/G
A/C G/G
C/A G/T
C/A G/T
CT AT CG AG
Frequency 0.000 0.300 0.450 0.250
Expectation under LE 0.135 0.165 0.315 0.385
Figure 1.1 Linkage disequilibrium and haplotype phasing. (A) Using family information can often resolve phase unambiguously. Here a trio is genotyped for two biallelic SNPs: for the first site, A or C alleles (top genotype in all plots); for the second site, G or T alleles (bottom genotype in all plots) in this example. From inspection, the mother necessarily transmits the CG haplotype, implying that the offspring carries AT and CG haplotypes, rather than AG and CT haplotypes. (B) In the absence of family data, it is still possible to estimate haplotype frequencies from genotypes at SNPs in linkage equilibrium. In this toy, illustrative example, the EM algorithm would conclude that the CT haplotype does not exist in this population based on this very small sample of 10, meaning that the two SNPs are in LD (here R2 is estimated at 0.351). Individuals would be assigned a combination of AT, CG, and AG haplotypes only, which will be consistent with their SNP genotypes.
100 kilobases (kb); 1 kb = 1000 basepairs) in which there is very high LD, meaning that only a small subset of all possible haplotypes (combinations of alleles in that region) are observed in the population. For example, considering 10 SNPs, each with two alleles, there are 210 = 1024 possible haplotypes, although under very strong LD we may observe only two or three of these at appreciable population frequencies. These “blocks” are separated by “recombination hotspots”—places in the genome with a historically higher rate of recombination—which acts to reduce LD by separating alleles on the recombinant haplotype. The results from the HapMap helped inform the design of experiments that aimed to intelligently select the smallest possible set of markers necessary to capture, or tag, most of the known common variation in a region. In the 10-SNP example, it may only be necessary to genotype 1 or 2 SNPs, for example, without significant loss of information compared with genotyping all 10. A common measure of LD in association studies is R2, where a value of 0 indicates no LD (two sites are statistically independent) and 1 indicates that one marker is effectively a perfect proxy for the second. An intermediate value, say of 0.8, indicates that one marker captures 80% of the information one would obtain if using one marker as a proxy for the other, instead of directly genotyping the second marker. If the untyped marker is a causal risk factor for disease, then one may still expect to observe a statistical signal of association (e.g., based on a simple comparison of case and control allele frequencies) at the genotyped marker, albeit one that is attenuated due to incomplete LD. (In fact, to retain equivalent power to detect association at the marker, in this case one would require 1/R2 = 1/0.8 or 125% of the sample size compared with typing the causal marker directly). By estimating
the average extent of LD, analyses of HapMap data showed that one could expect to capture the majority of common (typically defined as above 5% marker allele frequency) variation in European and Asian populations at a reasonable level of certainty (e.g., R2 > 0.8) by genotyping on the order of 500,000 SNPs genome-wide. This paved the way for the first genome-wide association studies (GWASs), which began typing 100,000–300,000 markers using newly developed, standardized commercial microarrays, soon establishing 500,000–1,000,000 SNPs as routine (Carlson et al., 2004). As described later, association analysis of these datasets has driven many genetic discoveries in the past decade. Superseding the tagging approach in many respects, the more general approach of imputation leverages the actual HapMap sample data itself to fill in data that are “missing” in a GWAS but present in the HapMap, relying on LD information implicit in the HapMap across all SNPs. Imputation allows researchers to probabilistically assign genotypes for all common HapMap SNPs (over 2 million in the European samples), even if only 500,000 have been directly genotyped in the study, by taking advantage of the redundancy due to LD. One of the major applications of imputation is to facilitate the comparison and aggregation of studies that use different GWAS arrays, by mapping everything to the common set of HapMap SNPs. This also obviates many of the practical difficulties that plagued candidate gene studies, in which different markers were typed in different studies. The HapMap and GWAS in general are largely focused on assaying only common genetic variation: typically sites at which at least 5% of chromosomes carry an “alternate” allele compared with the reference sequence. The vast majority of
6 • S. ECharney, merging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis et al., Oxford University Press USA - OSO,T2018. 07:33:44.
variants that have population frequencies below 1% will not be present in the HapMap or on standard microarrays, so will be effectively invisible to GWAS approaches. A major push in recent years has been to leverage advances in so-called next generation sequencing (NGS) technologies to build catalogs of lower frequency variation. This technology employs massively parallel approaches to sequence many millions of small fragments of DNA, generating very large numbers of short reads (around 100 bases) that can be mapped back to the reference sequence and variant sites called in an individual. The 1000 Genomes Project (www.1000genomes.org/) has used this technology to sequence the entire genomes of over 1,000 individuals, in order to create maps of known low-frequency variants and reference panels for imputation. Combining publicly available 1000 Genomes data with standard GWAS data, one can reliable impute over 10,000,000 polymorphic sites, many of which are of low frequency (under 1%) and many of which represent potentially functional polymorphisms (e.g., nonsynonymous allelic substitutions in genes, or short insertions and deletions that shift the reading frame of a gene). To measure very rare mutations that are specific to a family or a particular ancestral group that is not represented in the 1000 Genomes data, it will still be necessary to sequence samples directly. But given current cost constraints, the 1000 Genomes data afford a new lease of life for existing GWAS samples. In addition to utility in imputing a good deal of low-frequency variation, these data may be particularly helpful in ascribing a putative function to associated regions or haplotypes, as a consequence of the near-complete ascertainment of all commonly variable sites. Recent efforts such as the Haplotype Reference Consortium (http://www.haplotype-reference-consortium. org) now allow researchers to perform imputation analysis leveraging tens of thousands of reference samples. Another type of genomic map that has recently been reported, and that will likely play a critical part in both the analysis and interpretation of many genetic studies of disease, is the ENCODE project (Encyclopedia of DNA Elements; http://www.genome.gov/10005107). This project aimed to map all functional elements in the human genome sequence beyond protein-coding genes: for example, regions (that may often be cell-and tissue-specific) related to factors such as chromatin structure, methylation, histone modification, sequence- specific transcription factors, and RNA-binding proteins. As many association signals from GWAS fall outside of known protein-coding genes, a more comprehensive annotation and understanding of the full sequence will be important in translating statistical signal into biological knowledge (Degner et al., 2012). Ultimately, a better accounting of the diversity of cell types in humans, and in particular in the brain, will be necessary to fully understand how genes act and how to interpret association signals in concert with single-cell molecular studies. G E N O M E -W I D E A S S O C I AT I O N S T U D I E S In many respects, the development of reliable, cost effective, high-throughput genotyping technologies, using microarrays
that can simultaneously assay hundreds of thousands of single- nucleotide polymorphisms, has addressed the basic limitations inherent in the early application of association (or linkage disequilibrium) mapping. Because most of the common variation in the genome can be assayed, genetic studies have become fundamentally data-driven enterprises and do not rely on prior biological hypotheses. Order-of-magnitude cheaper per- genotype costs have enabled a large amount of genetic data to be amassed; the use of standardized microarrays (combined with imputation analysis) has also facilitated pooling of data across studies to achieve larger samples through meta-analysis, and therefore greater power, which is vitally important in complex trait genetics (Lohmueller et al., 2003). Also, GWAS studies generally do a more comprehensive job at capturing common variation in a given gene compared with early candidate-based studies using older genotyping technologies, including capturing the vast amount of variation in flanking intergenic and intronic regions. At the same time, the large multiple- testing burden inherent in GWAS forced investigators to address the issue of false positive rates early and head on. Based on empirical and theoretical considerations, most investigators require a p-value of less than 5×10-8 for an association to be declared genome-wide significant. In a well- controlled study, findings that reach this stringent threshold have been shown to have a very high probability of replicating in subsequent studies. A P P L I C AT I O N S O F G E N O M E -W I D E A S S O C I AT I O N M A P P I N G A N D A N A LY T I C I S S U E S Genome- wide association studies have been very widely adopted for a large number of diseases. One of the pioneering studies was of seven diseases and a shared control sample, the Wellcome Trust Case Control Consortium (2007). The U.S. National Human Genome Research Institute (NHGRI) maintains a catalog (www.genome.gov/GWAStudies) of published associations from GWAS for a diverse range of diseases and traits. To date, over 1,600 associations have been published, all meeting the strict threshold of genome-wide significance (Figure 1.2). For most common diseases, these genome-wide findings likely represent the tip of the iceberg of true common variant associations. In many cases, including for neuropsychiatric disease, there are multiple lines of evidence that point to an abundance of true signals below the formal threshold for genome-wide significance. When looking at many replicated genome-wide significant results, the statistical power to detect them (given their frequency and reported effect size) would typically have been low. (In practice, reported effect sizes are often inflated by the so-called “winner’s curse” effect, meaning that variants detected at strict significance thresholds may have the needed “luck of the draw” from sampling variation to push them over the bar). Low power a priori implies either that the investigator was extremely lucky (managing to detect one particular
1. G enetic ethodologies and pplications Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, etM al., Oxford University Press USA - OSO,A2018. 07:33:44.
Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press USA - OSO, 2018.
07:33:44.
The National Human Genome Research Institute GWAS catalog. A list of published GWAS associations (accessed 9/2016) (http://www.ebi.ac.uk/g was/home). Shaded circles indicate different classes of phenotype. Many of these discovered loci were completely novel. Figure 1.2
true positive despite very low chances to do so) or, more parsimoniously, that there must be a substantially larger reservoir of similar effects truly existing, from which this study sampled only a particular subset, in proportion to the statistical power. More directly, one can take sets of independent, subthreshold associations (e.g., SNPs with p- values between 1×10-4 and 5×10-8) and ask whether more than expected are nominally significant in an independent sample (e.g., at P < 0.01 or P < 0.05) or show effects in a consistent direction (above 50% correspondence of risk versus protective effects expected by chance alone, often referred to as a “sign test”). For many diseases, such analyses strongly support the presence of many subthreshold true associations. Furthermore, approaches such as gene set– enrichment analysis applied to lists of subthreshold associations can be used to indicate whether the genes implicated appear to be a random selection of all genes, as would be expected if the associated regions were, in fact, selected purely by chance, as opposed to preferentially belonging to certain known pathways, or clustering in networks, beyond chance expectation—which is consistent with a nontrivial proportion of the associations being true positives. For example, Lango Allen et al. (2010) reported hundreds of variants influencing human height clustered in functionally related pathways. Evidence for a substantial number of likely true subthreshold associations for a given disease can be taken to indicate that larger sample sizes will yield genome-wide significant associations, as more true positives are pushed over the threshold. Other studies have taken more direct approaches to address the idea of highly polygenic disease architectures (i.e., involving hundreds or thousands of distinct genetic loci). In particular, analyses of common variants in GWAS data for various highly heritable phenotypes, including height (Yang
et al., 2010) and schizophrenia (International Schizophrenia Consortium, 2009), have indicated that a sizeable proportion of the total heritability may be due to the combined action of extremely modest effects across many loci (many of which may never be expected to rise to the level of genome-wide significance even in very large samples). Under such models it is likely unrealistic to ever expect a “complete” genetic model of a disease in the sense of accounting for all risk genes and alleles. Nonetheless, it is important to note that although very high polygenicity reduces power to unambiguously detect any one particular variant, it does not by itself preclude progress toward the broader goals of genetic studies, namely, the identification of critical biological pathways and networks and even individual risk prediction and personalized therapies. Table 1.1 gives concrete numbers for the sample sizes required under different genetic models, for both common and rare variants of varying effect sizes. Given the large sample sizes indicated in Table 1.1 for the type of variant that characterizes most “GWAS hits,” meta-analysis (or combined, mega- analysis) has played an increasingly important role in genetic disease studies, in which consortia of studies—and then consortia of consortia—pool results or raw genotype data to collectively achieve greater power to detect variants of small effect. Although it has become clear that Type II errors (false negatives) are the primary hurdle in GWAS (low power to detect small effects), there has also been considerable attention to the issue of Type I errors (false positives). At the dawn of the GWAS era, many researchers were reasonably concerned that the massive multiple testing, as well as the scope for bias from technical artifact or epidemiological confounding, would lead to hopelessly inflated false-positive signals. Given that most GWAS studies have been population-based (utilizing samples of unrelated cases and controls) as opposed to family-based, one concern was that population stratification might give rise
Table 1.1 SAMPLE SIZES REQUIRED (CASE/CONTROL PAIRS FOR A 1% DISEASE) UNDER DIFFERENT GENETIC MODELS CAUSAL ALLELE
GENOTYPED MARKER
MAF
GRR
MAF
0.40
1.2
0.40
1.2
0.50
0.40
1.2
0.10
0.01
3.0
0.01
3.0
0.50
0.01
3.0
0.10
REQUIRED SAMPLE SIZE OF 80% POWER
R2
α = 0.05
α = 5 × 10−8
949
4,792
0.67
1,400
7,064
0.17
5,880
29,668
410
2,070
0.01
21,213
107,030
0.09
2,533
12,780
(Directly typed causal allele)
(Directly typed causal allele)
Contrasting power under two particular scenarios, involving a common and a low-frequency variant. Power calculated using the Genetic Power Calculator (http://pngu. mgh.harvard.edu/purcell/gpc/) and shows the number of case/control pairs required to achieve 80% power (i.e., an 80% chance of correctly rejecting the null hypothesis when the SNP truly has an effect) for two significant thresholds: a nominal 0.05, and genome-wide significant 5 × 10-8. (These α values represent the chance of a falsepositive test result.) The two causal scenarios are not intended to be directly comparable; rather, the numbers presented are meant to show the impact of requiring a strict significance threshold on required sample size, and the impact of incomplete LD (by genotyping a marker instead of directly genotyping the causal variant) under the two scenarios. Aside from the fact that, in general, large sample sizes are required for these types of effects, we see in particular that if the marker has a frequency very different from the causal variant, the R2, which is always set at the highest possible value given the two allele frequencies, it will be necessarily low, and therefore, power will be power, and the sample size required to achieve 80% will be high. The first scenario represents the type of SNP we may expect to find in a GWAS; the second scenario represents (perhaps an optimistically large) effect as one might hope to see in exome sequencing or an exome array study.
1. G enetic ethodologies and pplications Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, etM al., Oxford University Press USA - OSO,A2018. 07:33:44.
to false positives. If cases and controls are not well matched for ancestry, because different populations systematically vary in allele frequency at many sites across the genome for reasons unrelated to the disease being studied, this could induce spurious associations. In contrast, association analyses that adopt a family-based approach (e.g., the transmission disequilibrium test, or TDT, which tests for overtransmission of a specific allele from heterozygous parents to affected offspring) implicitly guard against such confounding effects (e.g., by contrasting transmitted versus untransmitted alleles from within the same parent, in the case of the TDT). In practice, the presence of genome-wide genotypic data allows one to empirically assess the presence of heterogeneity in ancestry in a sample of individuals (Rosenberg et al., 2002) and to correct it statistically in tests of association (using approaches such as principal components analysis). Although most GWASs have been conducted in populations of European descent, there is potentially a lot to be learned from application to a more diverse range of populations, and new analytic challenges, for example, in highly admixed populations (Rosenberg et al., 2010). Quality control procedures play an important role in GWAS—for example, testing for deviations from Hardy-Weinberg equilibrium, or detecting SNPs with particularly high rates of failed genotyping. GWAS can still be prone to false positives from technical bias or other types of analytic error, simply by virtue of the large number of tests performed: in large part, this concern is addressed by placing a strong emphasis on the need to seek replication of any putative signals in independent samples. Although one can, in theory, approach the analysis of genotype–phenotype relations using GWAS data in a number of ways, in practice most substantive findings (as represented in the NHGRI catalog) come from simple, sequential tests of one SNP (either imputed or directly genotyped) at a time. Typically, a technique such as logistic or linear regression is employed, assuming a purely additive dosage model at each site. Simpler alternatives include Armitage trend test or Fisher’s exact test; more complex alternatives include nonparametric regression models, linear mixed models, and Bayesian approaches. In broad terms, it does not appear that the precise choice of statistical machinery employed has altered the general trends of results and substantive conclusions to date, however. Subsequent chapters summarize the results from GWAS and other types of genetic studies for a range of neuropsychiatric diseases. Compared with certain other common diseases such as Crohn’s disease or Type I diabetes, there arguably has been less “low-hanging fruit” to emerge from neuropsychiatric GWAS. Nonetheless, numerous genome-wide significant hits have now been reported, particularly for schizophrenia and bipolar disorder. Also, as noted, consideration of subthreshold results strongly suggests that more are to be expected with larger sample sizes. Most notably, the Psychiatric Genomics Consortium (PGC) reported a combined GWAS of over 35,000 schizophrenia patients and 100,000 controls that detected 108 independent genome-wide significant associated loci (Schizophrenia Working Group of the Psychiatric Genomics Consortium, 2014). More recent work has begun to unpick the underlying causal allelic architecture at individual loci and its relation to disease mechanisms, notably for the
complement component 4 (C4) gene and its impact on synaptic pruning (Sekar et al., 2016). P O LYG E N I C A NA LYS E S WIT H I N A N D B ET WE E N T R A I TS A N D D I S E A S E S
One interesting class of analytic approach to emerge from GWAS focuses on genome-wide patterns of variation in order to make inferences about genetic architecture for individual traits or diseases, and also the genetic overlap between different traits or diseases. Variance components models, implemented in the GCTA package (Yang et al., 2013), can estimate the heritability of a trait without using traditional family-based samples. Using SNP data to infer the degree of distant genetic relatedness between all pairs of individuals in a population-based sample, the same underlying logic of the classical twin study is applied: individuals who are genetically more similar should also be phenotypically more similar if the trait is heritable. Instead of comparing pairs sharing either 100% or 50% of their genome, as identical and fraternal twins do, this approach considers large numbers of individuals that perhaps share ~0.5%, as estimated from the SNP data. Nonetheless, in large samples, using linear mixed models one can estimate heritability arising from the shared SNPs. These models can be extended to consider multiple diseases and to estimate the genetic correlations between them, which represents the proportion of genetic effects that are shared by two diseases. Other approaches to studying pleiotropic gene effects include using polygenic risk scores (International Schizophrenia Consortium, 2009) and LD- score regression (Bulik- Sullivan et al., 2015b). These approaches have demonstrated, for example, that schizophrenia and bipolar disorder are highly genetically correlated (Cross- Disorder Group of the Psychiatric Genomics Consortium, 2013) and are now being routinely applied to broader panels of phenotypes with available GWAS (Bulik-Sullivan et al., 2015a). Studying the genetic, nosological boundaries of disorders will help gene discovery efforts and may lead to better understanding the heterogeneity within disorders. THE FREQUENCY S P E C T RU M O F D I S E A S E ALLELES: MODELS OF RARE A N D C O M M O N VA R I AT I O N Most genetic variation in the human genome is attributable to common polymorphism. For this reason, along with the fact that common SNPs in any one population constitute a relatively limited and easily assayable universe, common variation was an obvious first target for large-scale, genome-wide genetic studies, in the form of SNP-based GWASs. It has, of course, long been recognized that common SNPs are by no means the only class of variation a geneticist may wish to study. Particularly in the context of disease, one can argue (supported by observations in rare, Mendelian disease) that larger types of variant might be more likely to have a strong impact on disease risk, as, unlike SNPs, they impact more than just a single (usually intergenic) nucleotide. Structural variants are one such
10 •S. E merging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford University Press USA - OSO,T 2018. 07:33:44.
class, involving the deletion, duplication, inversion, or translocation of potentially millions of nucleotides. Similarly, evolutionary arguments can be used to suggest that alleles of high penetrance are unlikely to be very common, assuming the disease has had a continued negative impact on fitness over many generations, and so would have been selected against. The hypothesis that rare variants may primarily underlie common disease risk, in the same way they do for rare disease, expresses this logic (Cirulli and Goldstein, 2010). For schizophrenia, examples of very rare structural variants that are large-effect risk alleles were identified over two decades ago, using the classical techniques of cytogenetics and linkage mapping in extended pedigrees. For example, a 1.5–3 Mb microdeletion at 22q11.2 leads to velo-cardio-facial syndrome (VCFS), a phenotypically heterogeneous syndrome, which displays an approximately 30% probability of leading to schizophrenia. Because the deletion occurs at one in ~4,000 live births, this variant is expected to contribute to risk in ~1% of all schizophrenia patients. A second example of a rare and highly penetrant structural variant is the balanced translocation between 1q42 and 11q14, segregating with major psychiatric disease in a single extended Scottish pedigree and mapped using linkage analysis. One of the translocation’s breakpoints was later shown to disrupt a gene, now known as DISC1, “disrupted in schizophrenia 1” (St. Clair et al., 1990). The success of mapping DISC1 prompted a wave of functional studies to investigate its roles in neurodevelopment, although the precise mechanism by which the translocation acts to increase risk for major psychiatric illness in this family still eludes researchers. Whether or not that mechanism is ever fully understood, many would argue that the finding provides a window into the larger, more complex pathways involved in the disease. In its extreme form, the multiple rare variant model is taken to mean that although many rare disease variants may exist in a population, most affected individuals will carry only one, which was sufficient to cause their disease; similarly, most unaffected individuals would not be expected to carry any risk alleles. This model is in contrast to the polygenic common variant model, in which both affected and unaffected individuals would be expected to carry many risk alleles: under this model, cases simply carry more of them on average, as a consequence of the increased genetic burden leading to increased risk of disease. The extreme form of the multiple rare variant model essentially recasts a common disease as a collection of multiple, clinically indistinguishable diseases—that could in theory also be etiologically distinct in a fundamental manner, but that should often be amenable to the same family-based genetic approaches that worked for Mendelian disease (i.e., if most affected families are, in fact, segregating a single, high-penetrance allele). In practice, extreme forms of the multiple rare variant model are unlikely to be the general rule for any common disease—if linkage analysis has been adequately performed in appropriately sized pedigree collections, this model can already be ruled out. Perhaps a better default or working model for most common diseases should instead be that multiple variants of varying effect sizes are likely to exist anywhere across the frequency spectrum (Gibson, 2012; Owen et al., 2010). At least for diseases
with childhood or early-adult onsets, we would expect selection to constrain alleles of larger effect to have lower population frequencies. Although the exact relationship between frequency and effect size that arises from the action of selection is hard to predict generally, it is safe to conclude that common variants of very large effect are unlikely to exist; otherwise, all combinations of variant will likely occur, in proportion to the frequency spectrum of neutral variation. What may make some diseases, including neuropsychiatric disease, particularly challenging from a genetic perspective, is likely to be the sheer number of loci in the genome that, if perturbed by either a rare or common variant, can increase risk for disease. This challenge will be equally pertinent for various study designs, from sequencing to GWAS. STUDIES OF R ARE S T RU C T U R A L VA R I AT I O N : C O P Y N U M B E R VA R I A N T S A N D N E U R O P SYC H I AT R I C DISEASE Structural variants, such as the 22q11.2 deletion previously described, have a well-established role in a range of rare disease phenotypes, as well as genomic alterations that occur in cancers (Mills et al., 2011; Wain et al., 2009). Technologies such as array- CGH (comparative genomic hybridization) are now routinely used in prenatal screening as well as research settings, replacing traditional karyotype techniques for detecting unbalanced chromosomal changes. Rare copy number variants (CNVs, deletions or duplications of genetic material) ranging from 100 kb or less to multiple megabases can also be called from analysis of the same SNP microarrays used in GWAS studies: this fortuitous fact has meant that relatively large GWAS samples have been able to be assayed for changes in copy number variation. For autism and schizophrenia (International Schizophrenia Consortium, 2008; Sebat et al., 2007; Pinto et al, 2010, 2014; Perkins et al, 2016), such events clearly play an important role. Several studies have found, in particular, an increased rate of de novo CNVs in both autism and schizophrenia patients: such events will effectively be uncensored with respect to natural selection. The increased rate of de novo mutation in schizophrenia patients is also consistent with epidemiological observations of increased paternal age (as the probability of a germ line mutation in the father is known to increase with his age also). Approximately a dozen specific loci have been mapped with high statistical confidence, being likely to harbor CNVs that increase risk for disease (Sullivan et al., 2012; Perkins et al., 2016). Such events are typically large (often impacting dozens of genes), rare in the general population (with a frequency under 1/1000), and are estimated to increase risk for disease by up to tenfold or more. Interestingly, the same CNVs have been shown to increase risk both for autism and schizophrenia as well as other neurodevelopmental and behavioral disorders. In addition, autism and schizophrenia patients show a modest but significant increased burden of rare CNVs across their genomes, again consistent with the high polygenicity of neuropsychiatric disease. For other neuropsychiatric diseases, the role of CNVs is either less pronounced or no relationship has yet been clearly established.
1. G enetic ethodologies and A2018. pplications Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, etMal., Oxford University Press USA - OSO, 07:33:44.
N E X T-G E N E R AT I O N S E Q U E N C I N G TECHNOLOGIES AND MEDICAL SEQUENCING
observed in only one of the sequenced samples—and most of these will be novel in the sense that they will not have been previously identified and deposited in databases such as dbSNP (http://www.ncbi.nlm.nih.gov/projects/SNP/), which curThe advent of next-generation sequencing, as well as driving large rently contains around 50 million known variants. This fact genomics projects such the 1000 Genomes, has been widely and alone clearly poses challenges for the analysis of sequence data largely very successfully applied to a host of rare, Mendelian dis- to map risk alleles for disease. In practice, the rarity of individeases over the past few years. One of the most common applica- ual variants means that researchers employ a range of methods tions of NGS to date has been whole-exome sequencing (Bamshad to statistically aggregate multiple mutations across a particular et al., 2011). Here targeted approaches allow investigators to first gene and collectively test them for association with a disease, in greatly enrich the pool of DNA fragments to be sequenced for par- so-called gene-based rare variant analysis. Although large studticular regions of interest: in the case of whole-exome sequencing, ies of thousands of patients and controls are underway, across this involves “capturing” the ~1% of the genome that is known to a range of diseases, unambiguous discoveries are yet to emerge contain exons of protein-coding genes. This relatively small frac- from these studies. For common, complex traits, exome sequenction of the genome can then be sequenced at high depth (i.e., with ing will be much more challenging than for Mendelian disorders, 20 or more reads spanning most targeted bases) to ensure high and very large sample sizes may well be required, as is the case sensitivity to detect if not all then at least the vast majority of var- for studies of common variation (Kiezun et al., 2012). Although iant (nonreference) sites present in an individual’s exome. In com- sample sizes are still small by GWAS standards, early applicaparison with sequencing the whole genome, exome sequencing is tions of exome sequencing to schizophrenia have yet to unamstill considerably cheaper per unit, although per base sequenced biguously pinpoint many specific genes. Consistent with the it is less cost effective. In practice, though, sequence data on the polygenic models from GWAS, there is nonetheless evidence of exome is typically more valuable in the sense that any one vari- an increased burden of rare, damaging mutations across many ant has a higher prior likelihood of being functional, and that one genes, especially for genes involved in brain development and can more readily ascribe and interpret that function in terms of synaptic function (e.g., Genovese et al., 2016). Recently, great its impact on the resulting gene product and what else is known efforts have been made to aggregate data on rare variants across about that gene (e.g., where it is expressed, what other disorders many different exomes sequencing studies (Exome Aggregation are associated with mutations in that gene, what other proteins Consortium, ExAC), which has the potential to empower both interact with the protein coded by that gene). Perhaps the main clinical and research sequencing studies. The large ExAC referdrawback with exome sequencing is the expanding definition ence can help to identify which mutations observed in a given of what is practically implied by “the exome”: other interesting study are more likely to be pathogenic: namely, those that are regions such as regulatory regions near genes, rare transcripts, and truly rare in the large reference panel, and those that occur in noncoding RNAs are typically not captured comprehensively, genes that appear to be intolerant to damaging mutations, based and this fact alone may for many motivate the move to whole- on an analysis of ExAC data (Lek et al., 2016). genome sequencing. The amount of data generated by whole- Because genotyping technology is still cheaper and more genome sequencing is orders-of-magnitude larger than for the accurate than sequencing, a number of groups have collaborated exome, and so computational challenges in analyzing and even to create an exome array: a standard SNP microarray using the storing the data become major concerns for large studies. same technology deployed for GWAS, but that primarily conA typical exome sequencing experiment on one individ- tains approximately 200,000 low-frequency mutations that are ual currently targets around 200,000 genomic intervals, each nonsynonymous (alter the protein’s amino-acid sequence) and usually corresponding to one exon of a protein-coding gene, observed in at least two studies (and so represent variants that around 150 bases in length, targeting around 20,000 RefSeq are segregating in populations at low frequencies, perhaps 0.1%, genes and spanning around 30 Mb of genomic sequence. In a as opposed to truly “private” mutations that may be specific to high-depth sequencing study, each targeted base is often cov- single families and may never be seen again). Although comered, on average, by as many as 50 to 100 “short reads.” These prehensive results from these studies are not yet available, early reads are typically 70–100 bases in length, often physically applications do not suggest that this particular slice of the frepaired such that any two reads are expected to fall at nearby quency spectrum of nonsynonymous SNPs plays the major role genomic locations. Variants are discovered by aligning these or completely accounts for any “missing heritability,” however. reads to the reference sequence and looking for differences: this Other applications of sequencing to map rare variants is a technically involved and potentially error-prone procedure, for common diseases are using families rather than standard although the informatics for this have improved markedly in case control, population-based designs. Families can have a the past few years, in no small part driven by large projects such number of advantages: ascertaining families with an unusuas the 1000 Genomes. From a whole-genome sequencing study, ally high “density” of affected individuals for a given disease one expects to find something on the order of 3 to 4 million increases the probability that a rare highly penetrant varivariant sites; from whole-exome sequencing, this figure is typi- ant is present in that family. One can, in principle, use IBD cally in the range of 15,000–20,000 (depending on experimen- information from linkage analysis to prioritize specific regions tal details as well as the ancestry of the sampled individual). of the genome for sequencing or analysis. One can use famWhen sequencing more than a few individuals, a very large ily information to resolve haplotype phase and to impute proportion of all sites discovered will be “singletons”—variants sequence data across family members (as related individuals, 12 •S. E merging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford University Press USA - OSO,T 2018. 07:33:44.
by definition, represent different combinations of the same smaller set of “founder” chromosomes). One disadvantage is that for many adult-onset diseases it is far harder to collect intact family collections in large numbers. Additionally, one can use families to detect new, or de novo, mutations. In neuropsychiatric disease, and particularly autism and schizophrenia, the hypothesis that de novo mutation may play a significant role in disease risk is attractive to many researchers and is supported by the epidemiological observation that affected individuals tend to have older fathers (which is, in turn, known to correlate within increased germ line mutation that will be transmitted to offspring). A number of exome sequencing studies using trios (affected offspring and two parents) have been published for these two diseases (Neale et al., 2012; De Rubeis et al, 2014; Iossifov et al, 2014; Sanders et al, 2015; Xu et al, 2012; Fromer et al, 2014). The results to date are interesting and do point to nonrandom networks of genes that are enriched for
highly deleterious mutations in patients. At the same time, it does not appear to be the case that a sizeable proportion of affected individuals carry a de novo mutation that is likely to be the sole cause of their disease. In contrast to dozens of genes identified in autism using this approach, for schizophrenia relatively few genes have emerged that are observed to be recurrently hit by de novos across these studies beyond the level expected by chance— again speaking to the very high polygenicity of such diseases. The genes and mutations in specific patients that do emerge from this approach may well be particularly interesting to study, however, in that (because de novo mutations are effectively uncensored with respect to natural selection) they could in theory display a very high penetrance. Such “large-effect” alleles could in many cases be preferable mutations to follow up in functional studies, for example, using induced pluripotent stem cells or animal models. Figure 1.3 illustrates some of the different genetic designs and technologies currently available for relating DNA
Reporting GWAS results: Q-Q, Manhattan, and “regional” plots. These figures are taken from the Psychiatric Genomics Consortium Bipolar Disorder Working Group’s Nature Genetics 2011 report of a mega-analysis of bipolar disorder GWAS data. (A) A so-called “Manhattan plot,” in which individual SNP association statistics are ordered along the x-axis; the p-value is plotted on a –log10(P) scale, so values over 7.3 represent genome-wide significance. (B) The same data are shown in a Q–Q plot (quantile–quantile), which plots the observed statistic (−log10( P)) in rank order against the expected value under the global null hypothesis of no association. Points along the diagonal are therefore consistent with chance. The plots can show evidence of systematic bias (if the entire line grossly departs from the diagonal) or signal that is more likely to be true (if only the top portion of the data does, indicating there are more nominally significant hits than would be expected by chance). (C) A third commonly used plot when reporting GWAS results is a “region” plot. This shows the association statistics in a particular region as well as gives information on the LD (R2) between markers. (Psychiatric GWAS Consortium Bipolar Disorder Working Group, 2011). Figure 1.3
1. G enetic Mal., ethodologies and A 2018. pplications Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et Oxford University Press USA - OSO, 07:33:44.
1/1,000,000
Unique
De novo mutation
“Private” mutations
Exome sequencing in families
1/100,000
“Singletons” Exome sequencing in populations
1/10,000
1/1,000
1/100
1/10
Low-frequency segregating variants
Common polymorphism
Exome arry
GWAS
Summary of genetic study types targeting different intervals of the allelic frequency spectrum. The values along the horizontal bar indicate the minor allele frequency that is targeted by different genetic technologies, from common variation to sequencing for newly arising mutation.
Figure 1.4
variation to phenotype, in relation to the part of the allelic frequency spectrum they are designed to probe. Ultimately, it is likely that approaches that look for convergence of genetic signals across these different studies may be fruitful (Nejentsev et al., 2009).
I N T E G R AT I VE A N A LYS E S O F G E N ET I C N ET WO R K S A N D PAT H WAYS Future progress in complex traits genetics is likely to rely on two factors, no matter what particular type of genetic study is adopted: (1) increasingly large sample collections and (2) integrative modeling approaches that not only consider genetic information from different studies as illustrated in Figure 1.4, but also consider multiple genetic signals in their broader context (Raychaudhuri, 2011). This includes intersection of multilocus genotype data with functional information, from gene expression studies, from protein–protein interaction networks, or from other curated gene sets and pathways. For example, the CommonMind Consortium has used gene expression profiles in postmortem brain samples of schizophrenia patients and controls to help to interpret GWAS signals (Fromer et al., 2016). Jointly modeling the impact of risk variants on intermediate phenotypes or endophenotypes (Gottesman and Gould, 2003), for example, from brain imaging studies, and a fuller analysis of pleiotropic effects, where the same variant influences multiple (and potentially seemingly unconnected) disorders or traits (Cotsapas et al., 2011; Craddock et al., 2009), are both likely to be powerful approaches moving forward, particularly when seeded by solid knowledge of multiple associated loci from the primary genetics studies. A LT E R N AT I VE G E N ET I C M O D E L S The majority of genetic studies assume simple, additive models of effect, whether the variant is common or rare. This is typically a convenient, simplifying assumption made during
analysis, although in practice it is often likely to be a reasonable one. Although there is little empirical evidence for nonadditive effects being a generally important component of the architecture of common disease, finding specific instances of such effects could be very informative. Examples of nonadditive effects include basic dominant/ recessive (and compound heterozygote) models at a single locus and extended regions of homozygosity due to recent inbreeding, unmasking rare recessive effects (Keller et al., 2012), interaction between genes (epistasis as reviewed by Cordell, 2009), and between genes and environments (Thomas, 2010), as well as sex-specific, imprinting, and parent-of-origin effects. Whether or not allowing for these more complex models will help to map disease genes is unclear. Nonetheless, studying the growing number of genes already mapped by the additive models with respect to these alternate models (including pleiotropic effects on other phenotypes) has the potential to be of great value.
S U M M A RY The tools available to the complex trait geneticist have evolved rapidly over the past decade. Consequently, psychiatric genetics has made considerable progress during the same time frame (Sullivan et al., 2012). Different genetic strategies, from studies of de novo variation in exome sequencing, large deletion and duplication copy number variants, and rare and low-frequency variants segregating in populations to common polymorphisms are underway. It seems clear that all approaches will continue to bear fruit in the coming years, although the full promise of neuropsychiatric genetics is not yet achieved. In the (hopefully not too distant) future, the interpretation of multiple genetic associations in their biological context, rather than their initial discovery per se, will increasingly become the central challenge faced, but it will remain critically grounded on the initial gene discovery work going on today. DISCLOSURE Dr. Purcell has no conflicts of interests to disclose.
14 •S. E merging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford University Press USA - OSO,T 2018. 07:33:44.
REFERENCES Altshuler, D., Daly, M.J., et al. (2008). Genetic mapping in human disease. Science 322(5903):881–888. Bamshad, M.J., Ng, S.B., et al. (2011). Exome sequencing as a tool for Mendelian disease gene discovery. Nat Rev Genet. 12(11):745–755. Browning S.R., and Browning, B.L. (2012). Haplotype phasing: existing methods and new developments. Nat Rev Genet 12:703–714. Bulik-Sullivan, B., Fomicame. H.K., et al. (2015a). An atlas of genetic correlations across human diseases and traits.” Nat Genet 47:1236–1241. Bulik-Sullivan, B., Loh, P.R., et al. (2015b). LD Score regression distinguishes confounding from polygenicity in genome-wide association studies,” Nat Genet 47:291–295. Carlson, C.S., Eberle M.A., et al. (2004). Mapping complex disease loci in whole-genome association studies. Nature 429(6990):446–452. Cirulli, E.T., and Goldstein, D.B. (2010). Uncovering the roles of rare variants in common disease through whole-genome sequencing. Nat Rev Genet 11(6):415–425. Cordell H.J. (2009). Detecting gene–gene interactions that underlie human diseases. Nat Rev Genet 10:392–404. Cotsapas C., Voight, B.F., et al. (2011). Pervasive sharing of genetic effects in autoimmune disease. PLoS Genet. 7(8):e1002254. Cross-Disorder Phenotype Group of the Psychiatric GWAS Consortium, Craddock, N., et al. (2009). Dissecting the phenotype in genome-wide association studies of psychiatric illness. Br J Psychiatry 195(2):97–99. Cross-Disorder Group of the Psychiatric Genomics Consortium, Lee, S.H., et al. (2013) Genetic relationship between five psychiatric disorders estimated from genome-wide SNPs. Nat Genet 45(9):984–994. Degner, J.F., Pai, A.A., et al. (2012). DNase I sensitivity QTLs are a major determinant of human expression variation. Nature 482(7385):390–394. De Rubeis., He, X., et al. (2014). Synaptic, transcriptional and chromatin genes disrupted in autism. Nature 515(7526): 209–215. ENCODE Project Consortium. (2012). http://www.nature.com/ encode/. Encyclopedia of DNA Elements. URL http://www.genome.gov/10005107. Fromer M., Pocklington, A.J., et al. ( 2014 ). De novo mutations in schizophrenia implicate synaptic networks. Nature 506, (7487):179–184. Fromer, M., Roussos, P., et al. (2016). Gene expression elucidates functional impact of polygenic risk for schizophrenia. Nat Neurosci 19(11):1442–1453. Genetic Power Calculator. http://pngu.mgh.harvard.edu/purcell/g pc/. Genovese, G., Fromer, M., et al.(2016). Increased burden of ultra-rare protein-altering variants among 4,877 individuals with schizophrenia. Nat Neurosci 19(11):1433–1441. Gibson, G. (2012). Rare and common variants: twenty arguments. Nat Rev Genet 13(2):135–145. Gottesman I., and Gould, T. (2003). The endophenotype concept in psychiatry: etymology and strategic intentions. Am J Psych 160(4):636–645. International HapMap Consortium. (2007). A second generation human haplotype map of over 3.1 million SNPs. Nature 449:851–861. International Schizophrenia Consortium. (2008). Rare chromosomal deletions and duplications increase risk of schizophrenia. Nature 455:237–241. International Schizophrenia Consortium. (2009). Common polygenic variation contributes to risk of schizophrenia and bipolar disorder. Nature 460(7256):748–752. Iossifov I, O’Roask, B.J., et al. (2014). The contribution of de novo coding mutations to autism spectrum disorder. Nature 515(7526):216–221. Keller M.C., Simonson, M.A., et al. (2012). Runs of homozygosity implicate autozygosity as a schizophrenia risk factor. PLoS Genet. 8(4):e1002656. Kiezun, A., Garimella K., et al. (2012). Exome sequencing and the genetic basis of complex traits. Nat Genet. 44(6):623–630. Kim, Y., Zerwas S., et al. (2011). Schizophrenia genetics: where next? Schizophr Bull 37(3):456–463.
Lango Allen H., Estrada, K., et al. (2010). Hundreds of variants clustered in genomic loci and biological pathways affect human height. Nature 467:832–838. Lek, M., Karczewski, E.V., et al. (2016). Analysis of protein-coding genetic variation in 60,706 humans. Nature 536(7616):285–291. Lichtenstein, P., Yip, B.H., et al. (2009). Common genetic determinants of schizophrenia and bipolar disorder in Swedish families: a population- based study. Lancet 373(9659):234–239. Lohmueller, K.E., Pearce, C.L., et al. (2003). Meta-analysis of genetic association studies supports a contribution of common variants to susceptibility to common disease. Nat Genet 33:177–182. Mills, R.E., Walter, K., et al.; 1000 Genomes Project. (2011). Mapping copy number variation by population- scale genome sequencing. Nature 470(7332):59–65. Neale, B.M., Kou, Y., et al. (2012). Patterns and rates of exonic de novo mutations in autism spectrum disorders. Nature 485(7397): 242–245. Nejentsev, S., Walker, N., et al. (2009). Rare variants of IFIH1, a gene implicated in antiviral responses, protect against type 1 diabetes. Science 324(5925):387–9. NHGRI GWAS Catalog: A Catalog of Published Genome- Wide Association Studies. http://www.genome.gov/g wastudies/. Owen M.J., Craddock, N., et al.(2010). Suggestion of roles for both common and rare risk variants in genome-wide studies of schizophrenia. Arch Gen Psychiatry 67(7):667–673. Perkins,O., Pers, T.H., et al. (2016). Contribution of copy number variants to schizophrenia from a genome-wide study of 41,321 subjects. Nat Genet 49(1):27–35.epub. Pinto, D., Pagnamenta, A.T., et al. (2010). Functional impact of global rare copy number variation in autism spectrum disorders. Nature 466(7304):368–372. Pinto, D., Delaby, Y., et al. (2014). Convergence of genes and cellular pathways dysregulated in autism spectrum disorders. Am J Hum Genet 94(5):677–694. Psychiatric GWAS Consortium Bipolar Disorder Working Group. (2011). Large-scale genome-wide association analysis of bipolar disorder identifies a new susceptibility locus near ODZ4. Nat Genet 43(10):977–983. Raychaudhuri, S. (2011). Mapping rare and common causal alleles for complex human diseases. Cell 147(1):57–69. Rosenberg, N.A., Huang, L., et al. (2010). Genome-wide association studies in diverse populations. Nat Rev Genet 11(5):356–366. Rosenberg, N.A., Pritchard J.K., et al. (2002). Genetic structure of human populations. Science 298(5602):2381–2385. Risch, N., and Merikangas, K. (1996). The future of genetic studies of complex human diseases. Science 273(5281):1516–1517. Schizophrenia Working Group of the Psychiatric Genomics Consortium (2014) Biological insights from 108 schizophrenia-associated genetic loci. Nature 511(7510):421–427. Sanders, S.J., He, X., et al. (2015). Insights into autism spectrum disorder genomic architecture and biology from 71 risk loci. Neuron 87(6):1215–1233. Sebat, J., Lakshmi, B., et al. (2007). Strong association of de novo copy number mutations with autism. Science 316:445–449. Sekar, A., Bialas, A.R., et al. (2016). Schizophrenia risk from complex variation of complement component 4. Nature 530(7589): 177–183. Smith, G.D., and Ebrahim, S. (2003). “Mendelian randomization”: can genetic epidemiology contribute to understanding environmental determinants of disease? Int J Epidemiol 32(1):1–22. St Clair, D., Blackwood D., et al. (1990). Association within a family of a balanced autosomal translocation with major mental illness. Lancet 336(8706):13–16. Sullivan, P.F., Daly M.J., et al. (2012). Genetic architectures of psychiatric disorders: the emerging picture and its implications. Nat Rev Genet 13(8):537–551. Thomas, D. (2010). Gene-environment-wide association studies: emerging approaches. Nat Rev Genet 11(4):259–272.
1. G enetic Mal., ethodologies and A 2018. pplications Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et Oxford University Press USA - OSO, 07:33:44.
The 1000 Genomes Project Consortium. (2010). A map of human genome variation from population- scale sequencing. Nature 467(7319): 1061–1073. van Dongen, J., Slagboom, P.E., et al. (2012). The continuing value of twin studies in the omics era. Nat Rev Genet 13:640–653. Wain, L.V., Armour, J.A., et al. (2009). Genomic copy number variation, human health, and disease. Lancet 374(9686):340–350. The Wellcome Trust Case Control Consortium. (2007). Genome-wide association study of 14,000 cases of seven common diseases and 3000 shared controls. Nature 447:661–678.
Xu, B., Ionita-Laza, I., et al. (2012). De novo gene mutations highlight patterns of genetic and neural complexity in schizophrenia. Nat Genet 44(12):1365–1369. Yang, J., Benyamin, B., et al. (2010). Common SNPs explain a large proportion of the heritability for human height. Nat Genet 42(7):565–569. Yang, J., Lee, S.H., et al. (2013). Genome-wide complex trait analysis (GCTA): methods, data analyses, and interpretations. Methods Mol Biol 1019:215–236.
16 •S. E merging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford University Press USA - OSO,T 2018. 07:33:44.
2. NET WORK METHODS FOR ELUCIDATING THE COMPLEXIT Y OF COMMON HUMAN DISEASES Eric E. Schadt
INTRODUCTION Our understandings of common human diseases and how best to treat them are hampered by the complexity of the human system in which they are manifested. Unlike simple Mendelian disorders in which highly expressive, highly penetrant mutations make it possible to identify the causal genes within families segregating traits associated with the disorders, the common human diseases originate from a more complex interplay between constellations of changes in DNA (both rare and common variations) and a broad range of environmental factors like diet, age, sex, and exposure to environmental toxins (R. Chen et al., 2016). With roughly 3 billion nucleotides making up the human genome, the number of nucleotide changes that can affect the activities of a moderate to large number of genes vastly exceeds our ability to experimentally determine the effects of combinations of such changes. Whereas the focus in years past regarding DNA variation and its association to disease had been focused on protein-coding sequences, given declarations of intergenic DNA being composed mainly of “junk” (Smith, Brookhaven National Laboratory et al., 1972) we know today that more than 80% of the human genome is actively bound by proteins that regulate the expression of genes (Ecker et al., 2012), providing a vast array of knobs and switches to modulate not only the activity of genes but also the activity of whole gene networks. Therefore, leveraging naturally occurring DNA variation in human populations can be considered among the most attractive approaches to inferring the constellation of genes that affect disease risk. For most noncancer human diseases such as Alzheimer’s disease, autism, and schizophrenia, changes in DNA that correlate with changes in disease can be inferred as tagging or directly representing causal components of disease (Zhang et al., 2013; Fromer et al., 2016). In this way, the DNA variation directly elucidates disease etiology and so is extremely useful. Genome-wide association studies (GWAS) are now well proven to uncover genetic loci that affect disease risk or disease progression (Witte, 2010; Welter et al., 2014). The complex array of interacting factors does not influence the activity of single genes in isolation but, instead, affects entire network states that, in turn, increase or decrease the risk of disease or affect disease severity. In the context of common human diseases, the disease states can be considered as emergent properties of molecular networks (Schadt, 2009;
Schadt et al., 2009; Califano et al., 2012; Argmann et al., 2016) as opposed to responses to changes in a small number of genes driving core biological processes associated with the disease. Integrating large-scale, high-dimensional molecular and physiological data holds promise in not only defining the molecular networks that directly respond to genetic and environmental perturbations that associate with disease, but also in causally associating such networks with the physiological states associated with disease. Of course, genetics is but one dimension in a big sea of data dimensions that we can now leverage to better understand human conditions such as psychiatric disorders. Models of disease that consider a greater diversity of data that inform on disease will necessarily deliver more accurate diagnoses. In fact, we are in the midst of a big data revolution that permeates nearly every aspect of our lives. Electronic devices that consume much of our attention on a daily basis enable rapid transactions among individuals on unprecedented scales, where all of the information involved in these daily transactions can be seamlessly stored in digital form, whether the transactions involve monitoring of activity levels, cell phone calls, text messages, credit card purchases, e-mail, or visits to the doctor’s office in which all tests carried out are digitized and entered into one’s electronic medical record (Figure 2.1). In fact, devices such as the Apple iPhone now provide platforms such as HealthKit, ResearchKit, and CareKit to facilitate larger scale collections of data around individuals using smart devices such as an iPhone, as well as better engagement around the acquired data to facilitate increased wellness and even impact clinical care decisions. The digital universe of data more generally now far exceeds one zettabyte (that is 21 zeros or one billion terabytes—think 63 billion 16-gigabyte iPhones). Thus, our ability to store and access unimaginable scales of data has been revolutionized by technological innovations, some of which (such as DNA sequencing technologies) have been observed to operate at super Moore’s law rates. The life and biomedical sciences have not stood on the sidelines of this revolution. There has been an incredible wave of new technologies in genomics—such as next-generation sequencing technologies (Eid et al., 2009), sophisticated imaging systems, and mass spectrometry- based flow cytometry (Bandura et al., 2009)—enabling data to be generated at very large scales. As a result we can monitor the expression of tens of thousands of protein-and noncoding genes simultaneously
1 7 USA - OSO, 2018. Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press 07:33:44.
GPS Weather and climate
DATA ANALYTICS
Air traffic
Security and automation
Individual patient
Coronary artery disease
Biomedical research and personal health
Type 2 diabetes
PREDICTIVE MODELS OF DISEASE
Obesity Osteoarthrities
Cell phone, texts, digital music and movies Diagnosis and treatment assignment Diagnostics
Therapies
Real time traffic
Financial markets and services
Big data is all around us, enabled by technological advances in micro-and nanoelectronics, nano materials, interconnectivity provided by sophisticated telecommunication infrastructure, massive network-attached storage capabilities, and commodity-based high-performance compute infrastructures. The ability to store all credit card transactions, all cell phone traffic, all e-mail traffic, video from extensive networks of surveillance devices, and satellite and ground sensing data informing on all aspects of the weather and overall climate, and to now generate and store massive data informing on our personal health including whole-genome sequencing data and extensive imagining data, is driving a revolution in high-end data analytics to make sense of the big data and drive more accurate descriptive and predictive models that inform decision making on every level, whether identifying the next big security threat or making the best diagnosis and treatment choice for a given patient. Figure 2.1
(Y. Chen et al., 2008; Emilsson et al., 2008; Zhang et al., 2013; Franzen et al., 2016), score hundreds of thousands of SNPs (single-nucleotide polymorphisms) in individual samples (R. Shi et al., 2016; Kilpelainen et al., 2016; Lek et al., 2016; Lu et al., 2016), sequence entire human genomes for less than $1000, and relate all of these data patterns to a great diversity of other biologically relevant information (clinical data, biochemical data, social networking data, etc.) Given technologies on the horizon like the IBM DNA transistor with theoretical sequencing limits in the hundreds of millions of bases per second per transistor (imagine millions of these transistors packed together in a single handheld device) (Schadt et al., 2010), we won’t be talking in the future about Google rolling through neighborhoods with Wi-Fi-sniffing equipment (Kravets, 2010); rather, we will be talking about DNA-sniffing equipment rolling through neighborhoods sequencing everything they encounter in real time and then pumping such data into big data clouds to link with all other available information in the digital universe. If we want to achieve understanding from big data, organize it, compute on it, and build predictive models from it, then we must employ statistical reasoning beyond the more classic hypothesis testing of yesteryear. We have moved well beyond
the idea that we can simply repeat experiments to validate findings generated in populations. In fact, while first instances of the central dogma of biology looked something like the simple graph depicted in Figure 2.2 (top), today—given that the complex interplay of multiple dimensions of data (DNA, RNA, protein, metabolite, cellular, physiologic, ecologic, and social structures more generally) demands a more holistic view be taken in which we embrace complexity in its entirety—the central dogma is evolving to look something more like the graph depicted in Figure 2.2 (bottom). Our emerging view of complex biological systems is one of a dynamic, fluid system that is able to reconfigure itself as conditions demand (Barabasi and Oltvai, 2004; Han et al., 2004; Luscombe et al., 2004; Pinto et al., 2004; Zerhouni, 2003). Despite these transformative advances in technology and the need to embrace complexity, it remains difficult to assess where we are with respect to our understanding of living systems relative to a complete comprehension of such systems. One of the primary difficulties in making such an assessment is that the suite of research tools available to us seldom provides insights into aspects of the overall picture of the system that are not directly measured.
18 •S. E merging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford University Press USA - OSO,T 2018. 07:33:44.
Original central dogma of biology
DNA
RNA
Protein
Evolving central dogma of biology Translation tRNA
Transcription
replication
snRNA
snoRNA
mRNA
tmRNA
RNA
viRNA
Epigenetic (modified bases)
rRNA
Proteins miRNA Replication
DNA
piwi RNA
Phosphorylation
siRNA
Prions
scRNA RNA binding proteins
Reverse transcriptase Spliceosome
ADAR (RNA editing)
THE EVOLVING CENTRAL DOGMA OF BIOLOGY The upper panel represents the original central dogma of biology, a simple view driven by early observations with low-resolution tools that uncovered a central relationship between DNA, RNA, and proteins, namely that RNA is transcribed from DNA, and RNA, in turn, is translated into proteins. New higher resolution technologies have enabled a far more complex view of the central dogma to emerge (bottom panel), with epigenetic changes to DNA that are transgenerational, leading to non-Mendelian patterns of inheritance, a complex array of RNA molecules such as microRNA, viRNA, piwiRNA, and siRNA that do not code for proteins but carry out complex regulatory functions, and sophisticated protein complexes involved in splicing, RNA editing, and RNA binding all feeding back on transcription, leading to a more network-oriented view of the central dogma. Figure 2.2
In this chapter I discuss a particular class of modeling approaches that integrate diverse types of data on broad scales in ways that enable others to interpret their data in a more holistic, informative context, to derive predictions that inform decision making on multiple levels, whether deciding on the next set of genes to validate experimentally or the best treatment for a given individual given detailed molecular and higher order data on their condition. Central to these models will be inferring causality among molecular traits and between molecular and higher order traits by leveraging DNA as a systematic source of perturbation. In contrast to the more qualitative approaches biological researchers have employed in the past, getting the most from these new types of high-dimensional, large- scale data requires constructing more complex, predictive models from them; refining the ability of such models to assess disease risk, progression, and best treatment strategies; and ultimately translating these complex models into a clinical setting where doctors can employ them as tools to understand most optimally a patient’s current condition and how best to improve it. Such solutions require a robust engineering approach, where integrating the new breed of large-scale datasets streaming out of the biological sciences and constructing predictive models from them will require approaches more akin to those employed by physicists, climatologists, and other strongly quantitative disciplines that have mastered the collection and predictive modeling of high-dimensional data.
T H E M A N Y M O VI N G P I E C E S O F B I O L O G I C A L SYS T E M S : A M O VI E A N A L O GY Tools to interrogate biological systems in the past were crude and did not permit the more holistic querying of such systems at multiple scales. In fact, if we were to view the full suite of interacting parts in living systems, from the molecular on up to the ecological levels, we would achieve a more complete understanding of the cellular-, organ-, and organism-level processes that underlie complex phenotypes such as disease, much in the same way we achieve understanding by watching a movie. The continuous flow of information in a movie enables our minds to exercise an array of priors that provide the appropriate context and that constrain the possible relationships (structures), not only within a given frame or scene but also over the entire course of the movie. As our senses take in all of the streaming audio and visual information, our internal network reconstruction engine (centered at the brain) pieces the information together to represent highly complex and nonlinear relationships depicted in the movie, so that in the end we are able to achieve an understanding of what the movie intends to convey at a hierarchy of levels. What if we were to view a movie as we have viewed biological systems in the past? What if, instead of viewing a movie as a continuous stream of frames of coherent pixels and sound, we viewed single dimensions of these data, and we viewed them
2 .S.NCharney, etwork A nalyses of USA C omplex Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis et al., Oxford University Press - OSO, 2018. 07:33:44.
independently from one another? Understanding in this case would likely be difficult, if not impossible, to achieve. As an example, consider a 2-hour feature length film composed of 216,000 frames (30 frames per second), where each frame is composed of 1,280 × 720 pixels (roughly one million pixels). First, it is worth noting that the number of pixels of information, roughly 199 billion, represented in this film is quite large (if each pixel were represented by 32 bits, the film would comprise more than 6 terabytes of information). Suppose we decided to use the tools of reductionist biology to view the film, where instead of viewing the film as a rapid succession of frames of one million pixels each, we viewed a single frame in which the intensity value for each pixel across all 216,000 frames in the movie was averaged. This gross, aggregate average would provide very little, if any, information regarding the movie—not unlike our attempts to understand complex living systems by examining single snapshots of a subset of molecular traits in a single cell type and in a single context at a single point in time. Even if we viewed our movie as independent, one-dimensional slices through its frames, where each slice was viewed as pixel intensities across that one dimension changing over time (like a dynamic mass spectrometry trace), this view would provide significantly more information, but it would still be very difficult to understand the meaning of the movie by looking at all of the one-dimensional traces independently, unless more sophisticated mathematical algorithms were employed to link the information together. Despite the complexity of biological systems, even at the cellular level, research in the context of large-scale, high- dimensional omics data has tended to focus on single data dimensions, whether constructing coexpression networks based on gene expression data, carrying out genome-wide association analyses based on DNA variation information, or constructing protein interaction networks based on protein– protein interaction data. While we achieve some understanding in this way, progress is limited because none of the dimensions on their own provide a complete enough context within which to interpret results fully. This type of limitation has become apparent in genome-wide association studies or whole-exome or genome-sequencing studies, where thousands of highly replicated loci have been identified and highly replicated as associated with disease, but our understanding of disease is still limited because the genetic loci do not necessarily inform on the gene affected, on how gene function is altered, or, more generally, how the biological processes involving a given gene are altered at particular points of time or in particular contexts (Altshuler et al., 2008; Y. Chen et al., 2008; Emilsson et al., 2008; Zhang et al., 2013; Franzen et al., 2016). It is apparent that if different biological data dimensions could be formally considered simultaneously, we would achieve a more complete understanding of biological systems (Y. Chen et al., 2008; Emilsson et al., 2008; Zhong, Beaulaurier et al., 2010; Zhu et al., 2012; Zhang et al., 2013; Franzen et al., 2016). (See the documentary film The New Biology at http://www. youtube.com/watch?v=sjTQD6E3lH4.) To form a more complete understanding of complex human diseases like psychiatric disorders, we must not only evolve technologies to sample systems at ever higher rates and with
ever greater breadth, but we must also innovate methods that consider many different dimensions of information to produce more descriptive models (movies) of the system. There are, of course, many different types of modeling approaches that have been and continue to be explored. Descriptive models quantify relationships among variables in data that can, in turn, enable classification of systems under study into different meaningful groups; whether stratifying disease populations into disease subtypes to assign patients to the most appropriate treatment or categorizing customers by product preference, descriptive models are useful for classifying but cannot necessarily be used to predict how any given variable will respond to another at the individual level. For example, while patterns of gene expression such as those identified for breast cancer and now in play at companies like Genomic Health can very well distinguish good from poor prognoses (van’t Veer, Dai et al., 2002; van de Vijver, He et al., 2002), such models are not generally as useful for understanding how genes in patterns associated with disease are causally related or for distinguishing key driver genes from passenger genes. Predictive models, on the other hand, incorporate historic and current data to predict how one variable may respond to another in a particular context or predict response or future states of components of a system at the individual level. In the biological context, predictive models aim to accurately predict (in silico—using the model to run simulations on a computer) molecule expression–level changes, cell state dynamics, and phenotype transitions in response to specific perturbation events. For example, understanding how the constellation of genes identified for diseases like schizophrenia or autism (Roussos et al., 2014; Fromer et al., 2016; Lek et al., 2016) are actually related to one another in probabilistic causal ways can lead to an understanding of how perturbing a given gene (say, for treatment) will impact the corresponding molecular networks and ultimately the pathophysiology of the diseases they impact. Key to constructing predictive models is elucidating causal relationships between traits of interest. Resolving causal relationships requires a systematic source of perturbation, and here I discuss the use of DNA variation as a systematic perturbation source to infer causal relationships among molecular traits and between molecular traits and higher order traits like disease (Schadt et al., 2005; Y. Chen et al., 2008; Emilsson et al., 2008; Zhu et al., 2008; Millstein et al., 2009; Millstein et al., 2011; Zhu et al., 2012; Zhang et al., 2013; Chang et al., 2015; Franzen et al., 2016). However, before diving into this specific type of modeling approach, it is worth reviewing the general ways in which biological data can be modeled. MODELING B I O L O G I C A L DATA A true understanding of complex systems and the complex behaviors they exhibit can only be achieved if we understand the causal relationships among the hierarchy of constituent components comprising the system. However, inferring causality between variables, especially recovering causal networks from observational data, is a particularly challenging task.
20 •S. E merging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford University Press USA - OSO, T 2018. 07:33:44.
Given the complexity of biological data and the complexity of methods that can be applied to deriving meaning from such data, an awareness of the different classes of models is warranted, even though in this chapter I focus primarily on probabilistic causal reasoning. The different types of modeling that can be applied to biological data can be broken down into a number of different classes, with the selection of modeling approach to employ dependent on a number of factors such as extent of prior knowledge, dimensionality of the data to be modeled, the scale of data available to model, and of course what one hopes to derive from the data and the model (Figure 2.3). In the spectrum of modeling classes ranging from those assuming the most complete knowledge of pathways and networks to those assuming no knowledge, preferring instead to learn the network structures directly from the data, the kinetic models are at the most extreme end of the distribution with respect to requiring extensive prior knowledge. Kinetic models are typically represented as systems of ordinary differential equations (ODEs), which require extensive prior knowledge as the ODEs fix the connectivity structure among the variables being modeled (e.g., the pathway is assumed to be known). The model is the defined by a series of parameters that are fit from the data, and with these parameter estimates the behavior of the system can be directly explored via simulations run on the model. Via these simulations, kinetic models provide for greater mechanistic insights. These models can also be fit from smaller, more focused datasets, although
typically this modeling approach is restricted to smaller network structures, and the models can be difficult to calibrate (Azeloglu and Iyengar 2015). Modeling of the dynamics of physiologic glucose-insulin levels, metabolic flux, and drug response are just a few of many examples that have been effectively modeled using this approach. Logic models represent another class of models that require significant prior knowledge, but that also have an adaptive component that can be learned from the data and thus can reduce dependence on the extent of knowledge required to model the biological system of interest. Logic models also maintain a simple and intuitive framework for understanding complex signaling networks (Morris et al., 2010). In addition, this type of modeling approach still provides for direct mechanistic insights to be derived from simulations. Kinetic and logic models are more representative of what I refer to as bottom-up modeling approaches that begin with strong prior knowledge regarding how pathways are put together, but then define the kinetic parameters on those pathways that describe the flow of information through the system. Boolean network modeling is another class of approaches that provide an even more flexible framework for modeling biomolecules as binary variables that directly relate to state information that is relevant to downstream biological processes. However, the regulation of the different states represented are described in a parameter-free way (in contrast to kinetic models that are defined by kinetic parameters), providing for an approach that enables a more exploratory
Fuzzy logic
Limited to small to mode rate #
Larger # of data points needed to fit model
Boolean network
Can have moderate#
Larger # of data points needed to fit model
Bayesian network
Can have moderate to large#
Moderate to large # of data points to fit model
Prior knowledge not required but can be leveraged
Can learn novel causal relationships
PLS regression
Can have large #
Small to moderate # of data points to fit model
Prior knowledge not required, some ability to model prior data
Does not implicitly infer causality but informs on relationships
PCAMultiregression &WGCNA
Can have very large #
Small # of data points to fit model
Prior knowledge not required, limited ability to incorporate prior knowledge
Extensive prior knowledge required Strong prior knowledge required
Less prior knowledge required
Prior knowledge dependence
Very large # of data points needed to fit model
Can reveal strong mechanistic insights
Novel mechanistic insights
(given comparable complexity)
Limited to small #
Model Size (# of variables modeled)
Correlationbased modeling
Can reveal strong mechanistic insights
Kinetic Bottom-up modeling
Top-down modeling
Minimal sample size required to fit model
Characteristics of Model
Type of model
Potential to provide mechanistic insights
Little ability to gain mechanistic insights, association based
Figure 2.3 Modeling biological data using different classes of mathematical modeling approaches. The primary aim of these different approaches is uncovering relationships in the data that may help predict phenotypes of interest, elucidate causal relationships among traits and biological processes, and derive mechanistic insights into the causes of disease, wellness, drug response, and other phenotypes of interest. A more detailed description of the different modeling approaches is given in the main text.
2 .S.NCharney, etwork A nalyses of USA C omplex Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis et al., Oxford University Press - OSO, 2018. 07:33:44.
characterization of the dynamics of a complex system (Albert and Thakar, 2014). While these types of models can represent many more variables than kinetic models, they provide less mechanistic insight. Bayesian network models, the approach discussed in depth in this chapter, provide an even more flexible framework for modeling complex biological processes, requiring no prior knowledge but still providing for a natural and mathematically elegant way to incorporate prior knowledge. Bayesian networks provide a way to learn regulatory relationships directly from the data. With the use of heuristic searching, networks composed of many thousands of variables can be constructed, although equally large sets of data are required to effectively construct this type of model. The causal relationships represented in these models are statistically inferred, so deriving mechanistic insights is more difficult. The Boolean and Bayesian network modeling approaches are examples of what I refer to as top-down modeling approaches that seek to learn relationships directly from the data (structure-based learning). The final classes of modeling approaches are correlation based and are more exploratory in nature, seeking to elucidate the correlation structures in extensive datasets in order to begin to understand the relationships that may be well reflected in them, and that may aid in understanding key processes involved in complex processes associated with phenotypes of interest such as disease. Partial least squares regression and principle component analysis (PCA) multi-regression are examples of two classes of such modeling approaches. They do not require any prior knowledge to fit the models; they can operate on extremely large datasets, scaling to any number of variables that give rise to very large- scale networks; and they are easy to calibrate. However, such models do not explicitly infer causality but rather reflect connections and influences on those connections, a first step for learning important relationships that are involved in complex processes such as disease. In this broad spectrum of methods, Bayesian networks strike a nice balance between resolving mechanisms and structure and more broadly reflecting connections and their influences, thereby providing an efficient path for understanding information flow. Whereas ODEs are hypothesis driven, where the relationships among variables is assumed known, Bayesian methods operate in a hypothesis-free context in which we attempt to infer the relationships among variables given the data. As a result, Bayesian networks have emerged as a state-of-the-art approach for understanding complex systems in which the relationships among the constituent components of the system are not generally known, since they can seamlessly incorporate existing knowledge as structural and parameter priors and then infer directed relationships among the nodes in the network using conditional dependency arguments (Zhu et al., 2008; Zhu et al., 2012; Chang et al., 2015). However, there are also limitations with this modeling approach that relate to the ability Bayesian networks to distinguish causal structures that have equivalent joint probability and conditional independence structures (Markov equivalence). The severity of this problem cannot be understated, since statistically indistinguishable
structures may reflect completely contradictory causal relationships. I will explore how appropriate prior information can be incorporated to help resolve these and related issues. C AU S A L I T Y A S A S TAT I S T I C A L I N F E R E N C E In the life sciences, most researchers are accustomed to thinking about causality from the standpoint of physical interactions. In the molecular biology or biochemistry setting, when two molecular traits are indicated as causally related we typically mean that one of the molecular entities (e.g., a small molecule compound) has been determined experimentally to physically interact with or to induce processes that directly affect the other molecular entity (e.g., the target protein of the small molecule) and consequently leads to a phenotypic change of interest (e.g., lower LDL cholesterol levels). In this case we have an understanding of the causal factors relevant to the activity of interest, so that careful experimental manipulation of these factors allows for the identification of genuine causal relationships. However, in the context of many thousands of variables related in unknown ways, the aim is to examine the behavior of those variables across populations in ways that facilitate statistically inferring causal relationships. For example, statistical associations between changes in DNA, changes in molecular phenotypes, and changes in higher order phenotypes like functional MRI readouts or disease can be examined for patterns of conditional dependency among the variables that allow directionality to be inferred among them. In this case we can employ indirect measures of processes that mediate changes in one trait conditional on another, to make a statistically inferred causal link. This is not unlike the types of statistical inferences that are leveraged in other disciplines to make new discoveries. For example, less than 5% of known extrasolar planets have been directly observed, so that most are observed indirectly. One method for detecting planets that cannot be directly observed considers that when a planet is orbiting a star, the gravitational pull of the planet on the star will place the star into a subtle orbit, which from our vantage point will appear as the star moving closer to and further away from the Earth in a cyclical fashion. Such movement can be measured as displacements in the star’s spectral lines due to the Doppler effect (Eriskine et al., 2005) and so the presence of the planet acting on the star can be statistically inferred. Similarly, consider genetic variants associated with, say, schizophrenia or autism (many such loci have now been identified; see Roussos et al., 2014; Fromer et al., 2016; Lek et al., 2016). Further, suppose the expression of some number of genes assayed in relevant regions of the brain relating to these disorders were also associated with these same genetic variants. By examining the changes in the levels of expression of these genes in response to changes in genotype at any of the genetic loci of interest, one can directly assess the extent to which these expression changes induced by the genetic loci well explain the degree of association between the locus genotypes and disease trait. In this way, just as the characteristic wobble
22 •S. E merging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford University Press USA - OSO, T 2018. 07:33:44.
of a star induced by an orbiting planet predicts the presence of the planet, the characteristic “wobble” of the expression levels of a gene and its association to the disease state predicts a causal path between the gene and disease state, as described in more detail below. Critical to identifying causal relationships is distinguishing between correlation and causation. The old adage, “correlation does not imply causation,” is familiar to most. This is among the first fallacies one learns about in beginning logic courses: post hoc ergo propter hoc (Latin for “after this, therefore because of this”). Measurements taken over time on independent variables can be correlated because trends reflected by such variables are coincidentally similar or changes in each variable are independently caused by a common source, in addition to being correlated as a result of a cause–effect relationship. It is also interesting to note that while correlation and causation are related, our intuitive notation that causation implies correlation is not always correct either. For example, suppose U and V are random variables with the same distribution, and suppose X = U + V and Y = U − V. In this case the covariance between X and Y (defined as E(XY) − E(X)E(Y), where E represents the expectation function) is 0, and so the correlation is 0 even though there is a direct functional dependence between the variables (Feller, 1967). Only when two variables are linearly dependent (which is often the case in research) is our intuitive notion of functional dependence implying perfect correlation correct. Structure learning approaches that seek to infer causal relationships among correlated variables often employ conditional dependency arguments or mutual information measures to resolve causality by introducing a third correlated variable. By conditioning each of the variables on the third and examining the residual correlation between them in each case, a decision can be made as to the direction of the flow of information between the variables. However, this type of reasoning has generally failed to result in predictive causal inference, because in the absence of systematic perturbations the number of graphs that can be represented between just three traits is large (125 graphs representing directed and undirected relationships between three correlated variables are possible), and many of these possible relationships between the traits are not statistically distinguishable (Sieberts and Schadt, 2007). For example, if variables X, Y, and Z are observed in a population to be correlated (e.g., suppose X, Y, and Z represent the expression levels of three genes assayed in a given region of the brain in a population of individuals with schizophrenia) and the true relationship between the variables is X → Z ← Y, this relationship cannot be statistically distinguished from X → Y ← Z and Z → X ← Y, even though these relationships give rise to contradictory causal relationships. To break this type of statistical symmetry, a source of perturbation is required. Classically in biology we have introduced artificial perturbations by knocking a gene out, overexpressing a gene, or chemically perturbing a given protein to assess the consequences on a given trait of interest. More recently, in the neurosciences, optogenetics methods have provided novel ways to perturb genes on the short time
scales needed to elucidate the complexity of networks at play in neurons in living mammals (Boyden et al., 2005). If experimentally controlled artificial perturbations on a given gene cause a change in a trait of interest, then we infer a causal relationship between that gene and trait. However, DNA variation in the germline provides an excellent systematic perturbation source that can also be used to resolve causal relationships in biological systems. Because variations in DNA cause variations in RNA, proteins, metabolites, and subsequently, higher order phenotypes, this source of variation can be leveraged to infer causality. Unlike artificial perturbations such as gene knockouts, transgenics, or chemical or optogenetic perturbations that may induce artificial correlations that are not observed in more natural settings, naturally occurring genetic variation defines those perturbations that give rise to the broad array of phenotypic variations (such as disease and drug response) that we are precisely interested in elucidating. The past 10 years (Nitsch et al., 2006; Lawlor et al., 2008) have demonstrated that causal links between DNA variations and molecular and higher order phenotypes can provide information on causal relationships between those traits (Schadt et al., 2005; Y. Chen et al., 2008; Emilsson et al., 2008; Millstein et al., 2009; Yang et al., 2009; Zhong, Beaulaurier et al., 2010; Zhong, Yang et al., 2010; Zhang et al., 2013; Franzen et al., 2016). Causality in this instance can be inferred because there is random segregation of the chromosomes during gametogenesis, thus providing the appropriate randomization mechanism to protect against confounding, similar to what is achieved in randomized clinical trials by randomly assigning patients to treatments to test the causal effects of a drug of interest (Nitsch et al., 2006; Lawlor et al., 2008). However, quantifying the uncertainty in making such causal calls has been challenging. For example, causal effect estimates often considered in Mendelian randomization approaches can be confounded by pleiotropic effects and reverse causation, limiting the utility of such approaches for problems that involve the reconstruction of regulatory networks, in which pleiotropy is common and there may be little a priori information regarding the structure of the causal relationships between the traits of interest (Millstein et al., 2009). Recently, though, formal statistical tests for inferring causal relationships between quantitative traits mediated by a common genetic locus have been developed (Millstein et al., 2009). To understand how such a test works, consider marker genotypes at a given DNA locus L that are correlated with a given molecular phenotype, G, and a higher order phenotype T (Figure 2.4). The causal relationship G → T is implied if three conditions are satisfied under the assumption that L is sufficiently randomized: (1) L and G are associated, (2) L and T are associated, and (3) L is independent of T given G (i.e., L and T|G are not associated) (L.S. Chen et al., 2007). If a given locus L is independent of G given T (G|T), this is consistent with T being causal for G (T → G), and if L is associated with G|T, then this is consistent with G being causal for T (G → T). We can boil all of these observations down to four conditions from which a statistical test can be formed to test for causality: (1) L and T are
2 .S.NCharney, etwork A nalyses of USA C omplex Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis et al., Oxford University Press - OSO, 2018. 07:33:44.
Independent/hidden model
Independent model G
L
L
H
G
Causal model G
T
Causal/independent model L
T
or similarly
T
L
G
G
T
L
L T Causal/hidden model L
G
T
H Figure 2.4 Given two traits G and T are correlated in a given population with changes in DNA at locus L, there are five basic causal models to consider in testing the hypothesis that variations in trait G cause variations in trait T. Here H denotes an unmeasured molecular or higher order trait.
associated, (2) L is associated with G|T, (3) G is associated with T|L, and (4) L is independent of T|G. Each of these conditions can be assessed with a corresponding statistical test. For example, if we assume the marker corresponding to locus L is biallelic, where L1 and L2 represent indicator variables for the two alleles in a codominant coding scheme, then the four conditions above can be tested in the parameters of the following three regression models: Ti = α1 + β1 L1i + β 2 L2 i + ε1i Gi = α 2 + β3Ti + β 4 L1i + β5 L2 i + ε 2 i Ti = α 3 + β6Gi + β 7 L1i + β8 L2 i + ε 3 i ,
where Gi and Ti represent the gene and trait levels, respectively, for individual i in a population of interest, and the ε ij represents independently distributed random noise variables with 2 variance σ j (L.S. Chen et al., 2007). Given these models the four component tests of interest are:
{
H 0 : {β1 , β 2 = 0}, H 1 : β1,β 2 } ≠ 0
{
{
H 0 : β 4 , β5 = 0}, H 1 : β 4 , β5 } ≠ 0 H 0 : β 6 = 0, H 1 : β 6 ≠ 0
{
{
H 0 : β 7 , β8 ≠ 0}, H 1 : β 7 , β8 } = 0 .
The four conditions of interest can be tested using standard F-tests for linear model coefficients (conditions 1–3) and a slightly more involved test for the last condition, since it is an equivalence testing problem (Millstein et al., 2009). Given these individual statistical tests on the different regression
parameters, a causal inference test can then be carried out by testing the strength of the chain of mathematical conditions that collectively are consistent with causal mediation (i.e., the strength of the chain is only as strong as its weakest link, so that the intersection of the rejection regions of the component tests provides for the causality test we seek). For a series of statistical tests of size α γ and rejection region Rγ , the “intersection union” test with rejection region equal to the intersection over all Rγ , is a level sup(α γ ) test, so that the p- value for the causal inference test corresponds to the p-value for an intersection union test, or, simply, the supremum of the four p-values for the component tests (L.S. Chen et al., 2007). This test has been implemented as the CIT package in the R statistical programming language and is freely available. Applications of this type of test can be applied to resolve the types of causal relationships depicted in Figure 2.4. Application of these ideas in segregating mouse populations have led to the identification and validation of many genes causal for a number of metabolic traits, including obesity, diabetes, and heart disease. In one such population constructed between the B6 and DBA inbred strains of mouse, 111 F2 intercross animals were placed on a high-fat, atherogenic diet for 4 months at 12 months of age. All animals were genotyped using a genome-wide panel of markers, clinically characterized with respect to a number of metabolic traits, and the livers were expression profiled using a comprehensive gene expression microarray. Given the pattern of genetic association between the metabolic and gene expression traits, causal inference testing was carried out to identify the genes in this population best supported as causal of obesity-related traits (Monks et al., 2004; Schadt et al., 2005). Of the top nine genes identified in this study supported as causal for obesity- related traits, eight of the genes were ultimately experimentally validated (Millstein et al., 2009). The only gene that failed to validate was an X-linked gene that was lethal if completely knocked out and so represented a more complicated example for which the appropriate tools to validate could not be constructed. Of course, this exact same type of reasoning can be used to causally relate imaging traits, DNA variation, and expression data to clinical phenotype data in the context of psychiatric disorders (Figure 2.5). Consider associations identified between SNP genotypes and gene expression traits assayed in dorsal-lateral prefrontal cortex (DLPFC). Given the association of SNPs with expression in DLPFC, such SNPs are of interest for testing association to functional MRI (fMRI) traits. Given a set of SNPs in which there is an association between gene expression in DLFPC, fMRI, and schizophrenia status, we can statistically model whether the relationship between the traits is causal, reactive, or independent as described above (Figure 2.5). This provides a causal statistical inference procedure applied to functional MRI and disease trait data, using DNA variation as the systematic perturbation source that can address the pressing question of whether changes in neuroimaging traits are the result of schizophrenia or whether these changes lead to the schizophrenia phenotype.
24 •S. E merging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford University Press USA - OSO, T 2018. 07:33:44.
VB,600 intersection, 162 samples fMRI
3 2 1
SNP
Schizophrenia
0 –1 –2 –3
SNP
fMRI
Schizop hrenia
SNP
Schizop hrenia
fMRI
Causal model
Reactive model
fMRI
SNP
Schizop hrenia
Independent model
Inferring causal relationships between functional MRI traits and schizophrenia traits using SNPs that associate with the expression of genes in the dorsal-lateral prefrontal cortex as a perturbation source. The heat map represents a two-dimensional hierarchical clustering of functional MRI traits in which the highlighted cluster distinguishes schizophrenia cases from controls. Associations between functional MRI traits, gene expression, disease status, and SNP genotypes can be integrated to infer causal relationships between functional MRI traits and disease status. Figure 2.5
F R O M A S S E S S I N G C AU S A L R E L AT I O N S H I P S A M O N G T R A I T PA I R S TO P R E D I C T I VE G E N E N ET WO R K S Leveraging DNA variation as a systematic perturbation source to resolve the causal relationships among traits is necessary but not sufficient for understanding the complexity of living systems. Cells are composed of many tens of thousands of proteins, metabolites, RNA, and DNA, all interacting in complex ways. Complex biological systems are composed of many different types of cells operating within and between many different types of tissues that make up different organ systems, all of which interact in complex ways to give rise to a vast array of phenotypes that manifest themselves in living systems. Modeling the extent of such relationships between molecular entities, between cells, and between organ systems is a daunting task. Networks are a convenient framework for representing the relationships among these different variables. In the context of biological systems, a network can be viewed as a graphical model that represents relationships among DNA, RNA, protein, metabolite, and higher order phenotypes like disease state. In this way, networks provide a way to represent extremely large-scale and complex relationships among molecular and higher order phenotypes like disease in any given context. BU I L D I N G F RO M T H E B OT TO M U P O R TO P D OWN ?
Two fundamental approaches to the reconstruction of molecular networks dominate computational biology today. The
first is what is referred to as the bottom-up approach, in which fundamental relationships between small sets of genes that may comprise a given pathway are established, thus providing the fundamental building blocks of higher order processes that are then constructed from the bottom up. This approach typically assumes that we have more complete knowledge regarding the fundamental topology (connectivity structure) of pathways, and, given this knowledge, models are constructed that precisely detail how changes to any component of the pathway affect other components as well as the known functions carried out by the pathway (i.e., bottom-up approaches are hypothesis driven). The second approach is referred to as a top-down approach in which we take into account all data and our existing understanding of systems and construct a model that reflects whole-system behavior, and from there tease apart the fundamental components from the top down. This approach typically assumes that our understanding of how the network is actually wired is sufficiently incomplete, that our knowledge is sufficiently incomplete, and that we must objectively infer the relationships by considering large-scale, high- dimensional data that informs on all relationships of interest (i.e., top-down approaches are data driven). Given our incomplete understanding of more general networks and pathways in living systems, in this chapter I focus on a top-down approach to reconstructing predictive networks, given that this type of structure learning from data is critical to derive hypotheses that cannot otherwise be efficiently proposed in the context of what is known (from the literature, pathway databases, or other such sources). However, top- down and bottom-up approaches are complementary to one
2 .S.NCharney, etwork A nalyses of USA C omplex Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis et al., Oxford University Press - OSO, 2018. 07:33:44.
another, although these approaches have largely been pursued as separate disciplines with, interestingly, little crosstalk occurring between them. One of the future directions I discuss in the conclusion is the need to mathematically unify these two classes of predictive modeling to produce probabilistic causal networks that more maximally leverage all available data and knowledge. In the context of integrating genetic, molecular profiling, and higher order phenotypic data, biological networks are composed of nodes that represent molecular entities that are observed to vary in a given population under study (e.g., DNA variations, RNA levels, protein states, or metabolite levels). Edges between the nodes represent relationships between the molecular entities, and these edges can either be directed, indicating a cause–effect relationship, or undirected, indicating an association or interaction. For example, a DNA node in the network representing a given locus that varies in a population of interest may be connected to a transcript abundance trait, indicating that changes at the particular DNA locus induce changes in the levels of the transcript. The potentially millions of such relationships represented in a network define the overall connectivity structure of the network, or what is otherwise known as the topology of the network. Any realistic network topology will be necessarily complicated and nonlinear from the standpoint of the more classic biochemical pathway diagrams represented in textbooks and pathway databases like KEGG (Kanehisa et al., 2016). The more classic pathway view represents molecular processes on an individual level, while networks represent global (population-level) metrics that describe variation between individuals in a population of interest, which, in turn, define coherent biological processes in the tissue or cells associated with the network. One way to manage the complexity of network structures that can obtain is to impose constraints on network structures to make them more computationally tractable. For example, it is common when learning network structures to disallow loops or cycles in the network structure (otherwise known as the network topology, the connectivity structure of the network), in which cases we refer to the network as acyclic. The neurosciences have a rich history of employing network- based approaches to understand the complexity of the human brain and the causes of psychiatric illnesses. Resources like the Allen Brain Atlas (http://www.alleninstitute.org) provide an anatomically comprehensive map of gene expression of the human brain that can facilitate network- based analyses (Ding et al., 2016). Others have employed techniques developed for constructing gene coexpression networks to construct interaction networks on fMRI data (Mumford et al., 2010), and others still have generated protein interaction networks to reflect features of the network architecture in brains of those with illnesses such as Huntington’s disease (Shirasaki et al., 2012). Larger scale efforts have also been undertaken to integrate large-scale transcriptomic data in the context of diseases like autism to understand how changes in these networks may give rise to autism or reflect the types of pathways or biological processes involved in such a disease (Voineagu et al., 2011). These efforts are important not only for better understanding psychiatric diseases, but also for
elucidating novel drug targets or biomarkers that better assess disease risk or severity. However, most of these current efforts do not lead to predictive models of disease but, rather, provide a descriptive framework within which to uncover associations between a myriad of molecular, cellular, imaging, and clinical traits and disease. A N I N T EG R AT I V E G E N O M I C S A P P ROAC H TO C O NS T RU C T I V E P R E D I C T I VE N ET WO R K MO D E L S
Systematically integrating different types of data into probabilistic networks using Bayesian networks has been proposed and applied for the purpose of predicting protein–protein interactions ( Jansen et al., 2003) and protein function (Lee et al., 2004). However, these Bayesian networks are still based on associations between nodes in the network as opposed to causal relationships. As discussed for the simple case of two traits, from these types of networks we cannot infer whether a specific perturbation will affect a complex disease trait. To make such predictions, we need networks capable of representing causal relationships. Probabilistic causal networks are one way to model from the top down such relationships, where causality again in this context reflects a probabilistic belief that one node in the network affects the behavior of another. Bayesian networks (Pearl, 1988) are one type of probabilistic causal network that provides a natural framework for integrating highly dissimilar types of data. Bayesian networks are directed acyclic graphs in which the edges of the graph are defined by conditional probabilities that characterize the distribution of states of each node given the state of its parents (Pearl, 1988). The network topology defines a partitioned joint probability distribution over all nodes in a network, such that the probability distribution of states of a node depends only on the states of its parent nodes: formally, a joint probability distribution p( X ) on a set of nodes X can be decomposed as p( X ) = Πp( X i | Pa( X i )), where Pa( X i ) represents the parent set of X i. The biological networks of interest we wish to construct are composed of nodes that represent a quantitative trait such as the transcript abundance of a given gene or levels of a given metabolite. The conditional probabilities reflect not only relationships between genes, but also the stochastic nature of these relationships, as well as noise in the data used to reconstruct the network. The aim in any network reconstruction such as this is to find the best model—the model that best reflects the relationships between all of the variables under consideration, given a set of data that informs on the variables of interest. In a probabilistic sense, we want to search the space of all possible networks (or models) for that network that gives the highest likelihood of occurring given the data. Bayes’ formula allows us to determine the likelihood of a network model M given observed data D as a function of our prior belief that the model is correct and the probability of the observed data given the model is: P( M | D) ∝ P( D | M )P( M ). The number of possible network structures grows superexponentially with the number of nodes, so an exhaustive search of all possible structures to find the one best supported by the data is not feasible,
26 •S. E merging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford University Press USA - OSO, T 2018. 07:33:44.
even for a relatively small number of nodes. A number of algorithms exist to find the optimal network without searching exhaustively, like the Monte Carlo Markov Chain (MCMC) (Madigan and York, 1995) simulation. With the MCMC algorithm, optimal networks are constructed from a set of starting conditions. This algorithm is run thousands of times to identify different plausible networks, each time beginning with different starting conditions. These most plausible networks can then be combined to obtain a consensus network. For each of the reconstructions using the MCMC algorithm, the starting point is a null network. Small random changes are made to the network by flipping, adding, or deleting individual edges, ultimately accepting those changes that lead to an overall improvement in the fit of the network to the data. To assess whether a change improves the network model or not, information measures like the Bayesian Information Criterion (BIC) (Schwarz, 1978) are employed, which reduces overfitting by imposing a cost on the addition of new parameters. This is equivalent to imposing a lower prior probability P( M ) on models with larger numbers of parameters. Even though edges in Bayesian networks are directed, we cannot in general infer causal relationships from the structure directly, just as I discussed in relation to the causal inference test. For a network with three nodes, X1, X 2, and X 3, there are multiple groups of structures that are mathematically equivalent. For example, the three models M1 : X1 → X 2 , X 2 → X 3 ; M2 : X 2 → X1 , X 2 → X 3; and M3 : X 2 → X1 , X 3 → X 2 are all Markov-equivalent, meaning that they all encode for the same conditional independence relationship: X1 ⊥ X 3 X 2 , X1, and X 3 are independent conditional on X 2. In addition, these models are mathematically equivalent:
Bayesian networks are directed graphs. However, the Bayesian network reconstruction algorithm can take advantage of genetic data to break the symmetry among nodes in the network that lead to Markov-equivalent structures, thereby providing a way to infer causal directions in the network in an unambiguous fashion (Zhu et al., 2004) The reconstruction algorithm can be modified to incorporate genetic data as prior evidence that two quantitative traits may be causally related based on previously a described causality test (Zhu et al., 2004). The genetic priors can be constructed from three basic sources. First, gene expression traits associated with DNA variants that are coincident with the gene’s physical location (referred to as cis-acting expression quantitative trait loci or cis eQTLs) (Doss et al., 2005) are allowed to be parent nodes of genes with coincident trans eQTLs (the gene in this case does not physically reside at the genetic locus of interest), p(cis → trans ) = 1, but genes with trans eQTLs are not allowed to be parents of genes with cis eQTLs, p(trans → cis ) = 0. Second, after identifying all associations between different genetic loci and expression traits at some reasonable significance threshold, genes from this analysis with cis-or trans eQTL can be tested individually for pleiotropic effects at each of their eQTLs to determine whether any other genes in the set are driven by common eQTLs (Lum et al., 2006). If such pleiotropic effects are detected, the corresponding gene pair and locus giving rise to the pleiotropic effect can then be used to infer a causal/ reactive or independent relationship based on the causality test described. If an independent relationship is inferred, then the prior probability that gene A is a parent of gene B can be scaled as
p ( X ) = p ( M1 D ) = p ( X 2 X 1 ) p ( X 1 ) p ( X 3 X 2 )
p( A → B) = 1 −
= p ( M2 D ) = p ( X 1 X 2 ) p ( X 2 ) p ( X 3 X 2 )
(
)
= p ( M3 D ) = p X 2 X 3 p ( X 3 ) p ( X 1 X 2 )
Thus, from correlation data alone we cannot infer from these types of structures whether X1 is causal for X 2 or vice versa. It is worth noting, however, that there is a class of structures, V-shape structures (e.g., Mv : X1 → X 2 , X 3 → X 2 ), that have no Markov-equivalent structure. In such cases it is not possible based on correlation data alone to infer causal relationships. Because there are more parameters to estimate in the Mv model than in the M1, M2, or M3 models, there is a large penalty in the BIC score for the Mv model. Therefore, in practice, a large sample size is needed to differentiate the Mv model from the M1, M2, or M3 models.
∑ p ( A ⊥ B A, B, l ) , ∑1 i
i
i
where the sums are taken over all loci used to infer the relationship. If a causal or reactive relationship is inferred, then the prior probability is scaled as p( A → B) =
2 ∑ p ( A → B A, B, l i ) i
∑ p ( A → B A, B, l ) + p ( B → A A, B, l ) i
i
p.
i
Finally, if the causal/ reactive relationship between genes A and B cannot be determined from the first two sources, the complexity of the eQTL signature for each gene can be taken into consideration. Genes with a simpler, albeit stronger, eQTL signature (i.e., a small number of eQTL that explain the genetic variance component for the gene, with a significant I N T EG R AT I N G G E N ET I C DATA A S proportion of the overall variance explained by the genetic A S T RU C T U R E P R I O R TO E N H A N C E C AUS A L effects) can be considered as more likely to be causal compared I N FE R E N C E I N T H E BAY E S I A N N ET WO R K with genes with more complex and possibly weaker eQTL sigR E C O N S T RU C T I O N P RO C E S S natures (i.e., a larger number of eQTLs explaining the genetic In general, Bayesian networks can only be solved to Markov- variance component for the gene, with less of the overall variequivalent structures, so it is often not possible to determine ance explained by the genetic effects). The structure prior that the causal direction of a link between two nodes even though gene A is a parent of gene B can then be taken to be 2 .S.NCharney, etwork A nalyses of USA C omplex Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis et al., Oxford University Press - OSO, 2018. 07:33:44.
p( A → B) = 2
1+ n( B) , 2 + n( A) + n( B)
where n(A) and n(B) are the number of eQTLs at some predetermined significance level for genes A and B, respectively. I N C O R P O R AT I N G OT H E R O M I C S DATA A S N ET WO R K P R I O R S I N T H E BAY E S I A N N ET WO R K R EC O N S T RU C T I O N P RO C E S S
Just as genetic data can be incorporated as a network prior in the Bayesian network reconstruction algorithm, so can other types of data such as transcription factor binding site (TFBS) data, protein–protein interaction (PPI) data, and protein–small molecule interaction data. PPI data can be used to infer protein complexes to enhance the set of manually curated protein complexes (Guldener et al., 2006). PPI- inferred protein complexes can be combined with manually curated sets, and each protein complex can then be examined for common transcription factor binding sites at the corresponding genes. If some proportion of the genes in a protein complex (e.g., half ) carry a given TFBS, then all genes in the complex can be included in the TFBS gene set as being under the control of the corresponding transcription factor. Given that the scale-free property is a general property of biological networks (i.e., most nodes in the network are linked to a small number of nodes, whereas a smaller number of nodes are linked to many nodes) (Albert et al., 2000), inferred and experimentally determined TFBS data can be incorporated into the network reconstruction process by constructing scale-free priors in a manner similar to the scale-free priors others have constructed to integrate expression and genetic data (Lee et al., 2006). Given a transcription factor T, and a set of genes G that contain the binding site of T, the TF prior, ptf , can be defined so that it is proportional to the number of expression traits correlated with the TF expression levels, for genes carrying the corresponding TFBS:
Small molecule–protein interactions can also be incorporated into the Bayesian network reconstruction process. Chemical reactions reflected in biochemical pathways and the associated catalyzing enzymes can be identified as metabolite– enzyme pairs from existing pathway databases like KEGG. These relationships can then be stored in an adjacency matrix in which a 1 in a cell represents a direct connection between the metabolite and the enzyme. The shortest distance dm ,e from an enzyme e to a metabolite m can then be calculated using the repeated matrix multiplication algorithm. The structure prior for the gene expression of an enzyme e affecting the metabolite concentration is related to their shortest distance dm ,e as p(m → e) ∝ e − λdm ,e . The shorter the distance, the stronger the prior. I L LUS T R AT I N G T H E C O NS T RU C T I O N O F P R E D I C T I VE BAY E S I A N N ET WO R K S WIT H A N E X A M P L E
To illustrate how different types of data can be integrated to construct predictive gene networks, we can consider a simple model system, yeast, that makes the point on how different pieces of molecular information can be brought together to infer causal networks. A yeast example in this instance is preferable to one involving psychiatric disorders, given the latter would be complicated and the validations less straightforward than we can demonstrate in a simple model system. However, the procedures applied and steps indicated would be essentially the same for any disease or system of interest, given that the Bayesian network reconstruction algorithm described is generally applicable to data collected in any population and for any phenotype of interest. In our simple yeast system, consider the following two classes of data: (1) DNA variation, gene expression, and metabolite data measured in a previously described cross between laboratory (BY) and wild (RM) yeast strains (referred to here as the BXR cross) for which DNA variation, RNA expression, and metabolite levels have been assessed (Brem et al., 2002; Brem and Kruglyak 2005; Zhu et al., 2012); and (2) protein– DNA binding, protein–protein interaction, and metabolite– log ptf (T → g ) ∝ log ∑ pqtl (T → g i ) δ protein interaction data available from public data sources and gi∈G generated independently of the BXR cross (referred to here as where pqtl (T → g ) is the prior for the QTL and non-BXR data). The BXR yeast data are reflected as nodes in the network to be constructed, where edges in the network 1, if corr(T , g i )≥ rcutoff δ = 0, if corr T , g < r . The correlation cutoff rcutoff can be reflect statistically inferred causal relationships among the ( i ) cutoff expression and metabolite traits. The non-BXR interaction determined by permuting the data and then selecting the data from public sources are used to derive the types of strucmaximum correlation values in the permuted datasets (cor- ture priors discussed on the network to both constrain the size responding to some predetermined, reasonable false discov- of the search space in finding the best network and enhance ery rate). This form of the structure prior favors transcription the ability to infer causal relationships between the network factors that have a large number of correlated responding nodes (Zhu et al., 2008; Zhu et al., 2012). genes. From the set of priors computed from the inferred and To illustrate the steps in the type of Bayesian network experimentally determined TFBS set, only nonnegative priors reconstruction procedure described and detailed more forshould be used to reconstruct the Bayesian network. For those mally (Zhu et al., 2008; Zhu et al., 2012) and to examine conprotein complexes that could not be integrated into the net- tributions from the different data types used to construct the work reconstruction process using scale-free priors, uniform network, I focus on genes and metabolites involved in the de priors were used for pairs of genes in these complexes (i.e., novo biosynthesis of pyrimidine ribonucleotides (Figure 2.6). p pc g i → g j = p pc g j → g i = c ). For simplicity I focus on the reconstruction of this smaller
(
(
)
)
(
)
28 •S. E merging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford University Press USA - OSO, T 2018. 07:33:44.
EXAMPLE YEAST NETWORK (A) Subnetwork identified in a previously constructed whole-genome yeast network in which URA3 was predicted as the causal regulator for genes and metabolites linked to a genetic locus on chromosome 5 coincident with the physical location of URA3. Red nodes are genes or metabolites whose variations are linked to the chromosome 5 locus. Hexagon-shaped nodes represent metabolites, circular nodes represent genes, and diamond-shaped nodes represent genes with cis eQTLs. (B) Trait values of nodes compared with genotype data for the URA3 subnetwork. eQTLs and metQTLs are prominently featured as residing in the chromosome 5 URA3 locus. (C) Bayesian network reconstructed using only trait data. (D) Bayesian network reconstructed using trait data and priors derived from other types of data. Figure 2.6
subset of genes, although the steps are similar if building a network from a more comprehensive set of genes. The subnetwork depicted in Figure 2.6a was identified from the full Bayesian network constructed from the BXR data. URA3 in this network was predicted as a causal regulator of gene expression traits linked to the URA3 locus. That is, using the full Bayesian network, in silico perturbations were carried out by simulating changes in each of the nodes and identifying those nodes that resulted in the most significant changes in other nodes in the network. As a result of this simulation, URA3 was identified as the regulator modulating the most significant number of nodes in the subnetwork in a causal fashion (Figure 2.6a). A deletion of URA3 was engineered in the parental strain RM11-1a as a selectable marker, and segregation of this locus among the BXR progeny is the most likely cause for expression variation of uracil biosynthesis genes linked to this locus (Brem et al., 2002). Variations of two metabolites are also linked to
this locus: dihydroorotic acid, which is converted to orotic acid by the enzyme Ura1p, and orotic acid itself, reflecting the functional consequence of transcriptional variation in genes involved in de novo pyrimidine base biosynthetic processes on metabolite levels. The causal relationships between URA1, orotic acid, and dihydroorotic acid as well as the subnetwork for genes linked to the URA3 locus recapitulate the known pyrimidine base biosynthesis pathway (Zhu et al., 2008; Zhu et al., 2012). This subnetwork not only captures the coregulation of gene expression and metabolite abundance but also elucidates the mechanism of how genetic variation in URA3 affects orotic acid and dihydroorotic acid levels. Step 1: Identification of the URA3-centered de novo biosynthesis of pyrimidine ribonucleotides subnetwork. There are 18 nodes in the subnetwork shown in Figure 2.6a. These nodes are highly correlated with
2 .S.NCharney, etwork A nalyses of USA C omplex Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis et al., Oxford University Press - OSO, 2018. 07:33:44.
one another, with 68% of all pairwise relationships significant at the 0.01 significance level. The continuous gene expression data for these 18 genes can then be discretized into three states representing downregulated, no-change, and upregulated states, and then the mutual information of all pairs of nodes are calculated. In this case, 54% of all pairs are significant at p < 0.01 (the mutual information of the permutated data is calculated and fit into a normal distribution, which is then used to assess significance of the mutual information of the observed data). All 18 of the trait values corresponding to these nodes are significantly associated with the genotypes at the URA3 locus (Figure 2.6c). Step 2: Reconstructing networks using only expression and metabolite traits (excluding DNA variation data). The process of reconstructing networks using only trait data is straightforward. The trait data are input into a standard Bayesian network reconstruction program in which 1,000 network structures are generated from a Monte Carlo Markov Chain process using different random seed numbers (1,000 random seed numbers are generated by a master process, then each slave process starts an MCMC process using one of the generated seed numbers). Once the 1,000 network structures have been generated, common features are extracted to derive a consensus network. With this construction, the consensus network may contain loops, which are prohibited in Bayesian networks. Therefore, to ensure the consensus network structure is a directed acyclic graph, the edges in the original consensus network are removed if and only if (1) the edge was involved in a loop, and (2) the edge was the most weakly supported of all edges making up the loop. The network resulting from this process is depicted in Figure 2.6b. Step 3: Constructing priors using eQTL data. The network in Step 2 is constructed without considering any of the genetic data. Because eQTL data represent a systematic source of perturbation on the expression data, integrating these data has the potential to better resolve causal relationships. Toward this end, expression and genotype data in the BXR cross are compared to detect eQTLs. The red nodes in Figure 2.6a indicate that nearly all of the nodes have QTLs linked to a single locus on chromosome 5. Expression traits that associate with a common eQTL are then subjected to a statistical test to infer causal relationships between the traits, as described. Among the nodes tested, URA3 and YEL016C have cis-acting eQTLs linked to the chromosome 5 locus. Nodes with cis-acting eQTLs are allowed to be causal parent nodes to nodes with trans-acting QTLs. However, nodes with trans-QTLs are not allowed to be causal parent nodes to nodes with cis-acting eQTLs. Step 4: Constructing priors using KEGG data. The network constructed in Step 2 also does not consider known
relationships among genes and metabolites as defined by canonical pathways. The relationships between enzymes and metabolites are well established in many cases. To incorporate this knowledge into the network reconstruction process, we construct priors using canonical pathway data in the following way. There are two metabolites in the URA3 subnetwork. Their distances to each other and related enzymes are defined in the KEGG database. The structure prior for the gene expression of an enzyme e affecting a metabolite concentration is constructed using their − λd shortest distance dm ,e as p(m → e) ∝ e m, e . Step 5: Constructing networks using expression data, metabolite data, and the genetic and canonical pathway priors defined in Steps 3 and 4. The process of reconstructing networks using trait data and priors from other data types is similar to the reconstruction process applied to trait data only, described in Step 2. In addition to trait data, priors derived from other data types are also input into the standard Bayesian network reconstruction process. The trait data of the 18 nodes and related priors are input into the network reconstruction process, and the resulting network is shown in Figure 2.6d. The root node of the Bayesian network is URA3, which is the gene with the cis-acting eQTL associated with other traits in the network. Step 6: Comparing the networks constructed in Steps 2 and 5. The main difference between the networks depicted in Figure 2.6b and 2.6d are the head nodes. In general, directed links in a Bayesian network do not necessarily represent causal relationships (Chang et al., 2015). The network constructed from the trait data only reflects relationships not supported by the genetic perturbation data. The genetic relationships are well captured by the more integrated network described in Step 5. For example, the link RIB4 → URA3 depicted in Figure 2.6b is opposite that identified in Figure 2.6d. Because the genetic perturbation at the URA3 locus affects the expression activity of that gene in cis, and the expression activity of the gene RIB4 in trans, the experimentally supported relationship is URA3 → RIB4. I note that the enzyme/metabolite and metabolite/metabolite relationships are similar with or without the priors derived from the KEGG pathways. All data and software used to construct the Bayesian networks for this example are available at http:// www.mssm.edu/ research/institutes/genomics-institute/rimbanet. E LU C I DAT I N G T H E C O M P L E X IT Y O F HU M A N D I S E A S E : FRO M T H E M ETA B O L I C TO T H E P SYC H I AT R I C
We have carried out studies using the modeling described in detail for the yeast cross but in human and mouse populations, segregating a number of different diseases such as
30 •S. E merging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford University Press USA - OSO, T 2018. 07:33:44.
obesity, diabetes, and heart disease (Figure 2.7). For example, in a segregating mouse population in which an extensive suite of disease traits associated with metabolic syndrome were manifested, including obesity, diabetes, and atherosclerosis (Chen et al., 2008), we carried out the type of network analysis discussed using genetic data typed in all animals and gene expression data generated from the liver and adipose tissues of all animals in the population. With this approach we found that of the many functional units (subnetworks) identified in the networks that reflected core biological processes specific to the liver and adipose tissues, only a handful were strongly causally associated with the metabolic syndrome traits. One module (referred to here as the inflammatome module) in particular stood out, not only because it was conserved across the liver and adipose tissues, between the sexes, and between species (Emilsson et al., 2008), but also because it was supported as strongly causal for nearly all of the metabolic traits scored in the cross (fat mass, weight, plasma glucose, insulin, and lipid levels, and aortic lesions) (Chen et al., 2008; Yang et al., 2009). Again, the causal relationship between the inflammatome module and the disease traits was established by leveraging the changes in DNA in this population that were simultaneously associated with disease and expression traits. The entire subnetwork was shown to be under the control of genomic loci associated with the metabolic traits, while the predictive network modeling strongly indicated that the module was causal for the disease traits and was not simply reacting to or acting independently of these traits. Of the more than 100 genes supported in the inflammatome module as causal for metabolic disease traits like obesity and diabetes, many genes like Zfp90, Alox5, C3ar1, and Tgfbr2 (a)
Generation of Networks Experimental Populations
Epigenomcs
Human Populations
Transcriptomics Proteomics Metabolomics
Network generation
Genomics
Panomics
Sample collection
had been previously identified and validated as causal for metabolic traits (Mehrabian et al., 2005; Yang et al., 2009; Lamb et al., 2011). In addition, three other genes were selected for validation because they were independently supported as causal for metabolic traits in other studies (Lpl and Lactb) or because they were supported as causal for such a wide variety of metabolic traits (Ppm1l) (Y.L. Chen et al., 2008). Interestingly, the degree of connectivity in this causal metabolic subnetwork was extreme. Perturbations to genes in this module that were previously validated as causal for the metabolic traits caused expression changes in many other genes validated as causal for metabolic traits. For example, overexpression of Zfp90 in mouse not only generated an expression response that was significantly overlapping with the causal metabolic module but also caused changes in other genes like Pparg known to have an impact on metabolic traits (Y.L. Chen et al., 2008). More recently we have applied this approach to identify novel drivers of cardiovascular disease (Franzen et al., 2016). Beyond these metabolic disease areas, these same approaches have been applied to brain-related disorders, such as Alzheimer disease and schizophrenia (Zhang et al., 2013; Roussos et al., 2014; Fromer et al., 2016). In fact, we had previously more fully characterized the inflammatome module described, linking it to 11 different diseases: atherosclerosis, obesity, diabetes, inflammatory pain, COPD (chronic obstructive pulmonary disease), asthma, fibrosis, stroke, neuropathic pain, sarcopenia, and inflammation (Wang et al., 2012). This same module can also be seen to be significantly enriched not only for genes that are differentially expressed in brain between Alzheimers’ and control subjects, but also for genes that are differentially expressed in different brain regions in
Network
(c)
Modifier genes
Phenomics
Generation of Disease/Wellness Phenotypes Disease Models
Genomics Epigenomcs
iPSCs Biopsy
Panomics
Sample collection
Molecular defined disease
Patients/Patient derived material
Transcriptomics Proteomics Metabolomics Phenomics
Disease/wellness signature sets
(b)
Network outputs/impact
Modifying biology Novel targets
Isolate disease/wellness subnetwork
Key driver analysis
Hypotheses
Patient subtyping Improved clinical care Better screens/drugs Effective therapies Other disease insights
Disease/Wellness Signature Sets
Integrating multiscale omics technologies and network approaches to elucidate the complexity of common human diseases. A) Omics data generated from samples collected in large-scale human and experimental organism populations can be integrated alongside publicly available databases across multiple biological dimensions to construct predictive models of disease. B) The network models can be used as a framework to understand disease phenotypes assessed in a multi-omic setting on patients manifesting disease as well as controls. For example, disease signature sets generated on disease populations or experimental populations can be projected onto the network models to reveal disease-associated networks. C) Given the causal probabilistic nature of these disease associated networks (or networks associated with other traits or phenotypes of interest such as wellness), master regulators of these networks (key drivers) can be identified using statistical algorithms. Further, functional and therapeutic insights can also be derived via annotation of the network gene members. Figure 2.7
2 .S.NCharney, etwork A nalyses of USA C omplex Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis et al., Oxford University Press - OSO, 2018. 07:33:44.
in whole populations in a comprehensive manner, the information is not complete: rare variation, DNA variation other than SNP/copy number, variation in noncoding RNA levels, and variation in the different isoforms of genes are far from being completely characterized in any sample, let alone in entire populations. In addition, single cell sequencing-based assays are beginning to mature and will add a new level of complexity to the construction of molecular networks, so networks within a cell will have to be integrated with cross-cell and tissue networks. Beyond DNA and RNA, measuring all protein- associated traits, interactions between proteins and DNA/ RNA, metabolite levels, epigenetic changes, and other molecular entities important to the functioning of living systems are not yet possible with existing technologies. Further, the types C O N C LU S I O N A N D FUTURE DIRECTIONS of high-dimensional data we are able to routinely generate today in populations represent only a snapshot at a single time The generation of ever higher dimensional data (DNA point, which may enable the identification of the functional sequencing, RNA sequencing, epigenomic profiling, pro- units of the system under study and how these units relate to teomic profiling, metabolomic profiling, and so on) at ever one another, but it does not enable a complete understanding higher scales demands sophisticated mathematical approaches of how the functional units are put together, the mechanistic to integrate these data in more holistic ways to uncover not underpinnings of the complex set of functions carried out by only patterns of molecular, cellular, and higher order activities individual cells and by entire organs and whole systems comthat underlie the biological processes that define physiological posed of multiple organs. One of the future developments expected to be most states of interest, but also causal relationships among molecular and cellular phenotypes and between these phenotypes impactful in this context is the unification of bottom-up and and clinical traits like disease or drug response. Among the top-down modeling approaches that maximally leverage the more successful frameworks for representing large-scale, high- strengths of each approach while minimizing the weaknesses. dimensional data are networks. Here I have detailed one par- Integrating models derived from bottom-up approaches into ticular approach to reconstructing predictive network models top-down approaches is currently hampered by the fact that of living systems that leverages DNA variation as a systematic the existing approaches do not typically fully parametervariation source and Bayesian network reconstruction algo- ize the network structure in ways that match the intrinsic rithms to take a top-down approach to modeling complex quantitative nature of top-down approaches. In bottom-up systems. Because state-of-the-art therapies in the future will approaches, the structural information detailing how different be based on targeting combinations of genes (Schadt, 2009; molecular entities are connected is typically derived from the Schadt et al., 2009; Califano et al., 2012; Argmann et al., literature or pathway databases, but such structural informa2016), for such applications not only is it important to infer tion is only qualitative, failing to define quantitatively how the direction of each interaction (i.e., do you antagonize or one node responds to another. On the other hand, in existing activate a given target?), but also one must be able to predict top-down approaches, unless a tremendous amount of trainthe degree to which each gene should be knocked down or ing data are available to cover all of the categories represented activated (in a quantitative sense). Only by generating accu- in the conditional probability distribution defining how rate predictive models of complex phenotypes can we most nodes are connected in the network (such as with Bayesian efficiently search for such combinations to pursue for exper- network reconstruction approaches), it is not generally possiimental proof of concept. ble to accurately estimate the full set of parameters associated The success of modeling complex systems in the future will with the reconstructed network structure. Worse, carrying out depend on constructing networks that are predictive of com- parameter estimation on a network structure that is not corplex behavior, not merely descriptive. In order to achieve these rect can be misleading, given false-positive and false-negative more predictive models in complex systems like humans, we predictions. In cases where heuristic searches are used to orimust expand existing networks so that they reflect relation- ent the edges in a given network structure, the end result is ships between cell types and tissues, not just within a single that model parameters have not been fitted accurately because cell type or tissue; capture a greater range of molecular pheno- the network itself is not correct. Without proper parameteritypes to enhance understanding of relevant functional units zation of network structures from these conventional systems that define biological processes of interest; and improve mod- biology approaches, the networks serve only as descriptive eling capabilities, ideally drawing on the expertise of other models that are not generally capable of generating in silico fields that have pioneered causality-type reasoning. The com- predictions. plex phenotype-associated molecular networks we can conThe limitations of bottom-up and top-down approaches struct today are necessarily based on grossly incomplete sets of can be addressed by devising bottom-up modeling approaches data. Even given the ability to assay DNA and RNA variation that deliver structures that can serve as prior information for Alzheimer, Huntington’s, and schizophrenia patients versus controls. That is, the intersection between the set of genes identified as differentially expressed in Alzheimer, Huntington’s, and schizophrenia patients is very significantly enriched for genes that are in the inflammatome module (Zhang et al., 2013; Narayanan et al., 2014; Fromer et al., 2016). Therefore, the extensive research carried out on the inflammatome module, the causal networks that have been constructed for this network, may hold clues regarding inflammation-related processes that are at play in brain-associated disorders such as Alzheimer disease, Huntington’s disease, and schizophrenia.
32 •S. E merging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford University Press USA - OSO, T 2018. 07:33:44.
top-down approaches, thereby providing a direct path for parameterizing bottom-up models in the context of a richer set of omics data and network architectures, while simultaneously reducing the size of the search space for top-down approaches. Such bottom-up approaches are beginning to emerge (Chang et al., 2011; Chang et al., 2015). By automatically parameterizing large networks given a particular network structure and corresponding interaction functions (e.g., activation or repression of gene activity) associated with all node pairs by either leveraging prior information or performing a heuristic search, bottom-up approaches will be capable of generating direct quantitative predictions that are compatible with top-down approaches. Central to the success of this approach is the observation that the complexity of the structure of biological networks leads to robust parameter estimates in a constrained parameter space (Wilhelm et al., 2004; Wu et al., 2009; Blanchini and Franco, 2011) and the fact that a statistical model’s parameters are, in fact, constrained to a cubic space (e.g., the conditional probabilities that represent parameters in our modeling approach are constrained to fall between 0 and 1). This stands in contrast to current bottom- up modeling approaches like continuous ordinary differential equation (ODE) modeling in which the parameter space is generally unconstrained (infinitely large). Current systems biology approaches relating to network learning and modeling have exclusively utilized a top-down (reverse-engineering) approach to learn network structure based on association scores (Stuart et al., 2003; Margolin et al., 2006; Zhu et al., 2008; Fiedler et al., 2009; Carro et al., 2010; Zhu et al., 2012; Zhang et al., 2013). Association scores are designed to uncover the best correlations between variables. Bayesian networks are among the most popular models for this purpose. In theory, it is known that learning the optimal (global maximum) Bayesian network structure from the data is a problem that cannot be solved in polynomial time (what is referred to as an NP-hard problem); further, because many substructures that must be considered during the reconstruction process are from classes of structures that are equivalent (the Markov equivalence issue noted), the statistical scores for all of the structures in a given equivalence class are equal, so that completely contradictory causal relationships are indistinguishable from one another. The integration of bottom-up and top-down approaches in a more holistic mathematical framework has the potential to further address these issues, potentially enhancing the power to uncover true causal relationships. REFERENCES Albert, R., Jeong, H., and Barabasi, A.L. (2000). Error and attack tolerance of complex networks. Nature 406(6794):378–382. Albert, R., and Thakar, J. (2014). Boolean modeling: a logic- based dynamic approach for understanding signaling and regulatory networks and for making useful predictions. Wiley Interdiscip Rev Syst Biol Med 6(5):353–369. Altshuler, D., Daly, M.J., & Lander, E. S. (2008). Genetic mapping in human disease. Science. 322(5903):881–888.
Argmann, C.A., Houten, S.M., et al. (2016). A next generation multiscale view of inborn errors of metabolism. Cell Metab 23(1):13–26. Azeloglu, E.U., and Iyengar, R. (2015). Good practices for building dynamical models in systems biology. Sci Signal 8(371):fs8. Bandura, D.R., Baranov, V.I., et al. (2009). Mass cytometry: technique for real time single cell multitarget immunoassay based on inductively coupled plasma time-of-flight mass spectrometry. Anal Chem 81(16):6813–6822. Barabási, A.L., and Oltvai, Z.N. (2004). Network biology: understanding the cell's functional organization. Nat Rev Genet 5(2):101–113. Blanchini, F., and Franco, E. (2011). Structurally robust biological networks. BMC Syst Biol 5:74. Boyden, E.S., Zhang, F., et al. (2005). Millisecond-timescale, genetically targeted optical control of neural activity. Nat Neurosci 8(9):1263–1268. Brem, R.B., and Kruglyak, L. (2005). The landscape of genetic complexity across 5,700 gene expression traits in yeast. Proc Natl Acad Sci U S A 102(5):1572–1577. Brem, R.B., Yvert, G., et al. (2002). Genetic dissection of transcriptional regulation in budding yeast. Science 296(5568):752–755. Califano, A., Butte A.J., et al. (2012). Leveraging models of cell regulation and GWAS data in integrative network-based association studies. Nat Genet 44(8):841–847. Carro, M.S., Lim W.K., et al. (2010). The transcriptional network for mesenchymal transformation of brain tumours. Nature 463(7279):318–325. Chang, R., Karr, J.R., and Schadt, E. E. (2015). Causal inference in biology networks with integrated belief propagation. Pac Symp Biocomput: 359–370. Chang, R., Shoemaker, R., and Wang, W. (2011). Systematic search for recipes to generate induced pluripotent stem cells. PLoS Comput Biol 7(12):e1002300. Chen, L.S., Emmert-Streib, F., and Storey, J.D. (2007). Harnessing naturally randomized transcription to infer regulatory relationships among genes. Genome Biol 8(10):R219. Chen, R., Shi, L., et al. (2016). Analysis of 589,306 genomes identifies individuals resilient to severe Mendelian childhood diseases. Nat Biotechnol 34(5):531–538. Chen, Y., Zhu, J., et al. (2008). Variations in DNA elucidate molecular networks that cause disease. Nature 452(7186):429–435. Ding, S.L., Royall, J.J., et al. (2016). Comprehensive cellular-resolution atlas of the adult human brain. J Comp Neurol 524(16):3127–3481. Doss, S., Schadt, E.E., et al. (2005). Cis-acting expression quantitative trait loci in mice. Genome Res 15(5):681–691. Ecker, J. R., Bickmore, W.A., et al. (2012). Genomics: ENCODE explained. Nature 489(7414):52–55. Eid, J., Fehr, A., et al. (2009). Real-time DNA sequencing from single polymerase molecules. Science 323(5910):133–138. Emilsson, V., Thorleifsson, G., et al. (2008). Genetics of gene expression and its effect on disease. Nature 452(7186):423–428. Eriskine, D.J., Edelstein, J., et al. (2005). Externally dispersed interferometry for planetary studies. Proc SPIE 5905:249–260. Feller, W. (1967). An introduction to probability theory and its applications. New York: Wiley. Fiedler, D., Braberg, H., et al. (2009). Functional organization of the S. cerevisiae phosphorylation network. Cell 136(5):952–963. Franzen, O., Ermel, R., et al. (2016). Cardiometabolic risk loci share downstream cis-and trans-gene regulation across tissues and diseases. Science 353(6301):827–830. Fromer, M., Roussos, P., et al. (2016). Gene expression elucidates functional impact of polygenic risk for schizophrenia. Nat Neurosci 19:1442–1453. Guldener, U., Munsterkotter, M., et al. (2006). MPact: the MIPS protein interaction resource on yeast. Nucleic Acids Res 34(Database issue):D436–D441. Han, J.D., Bertin, N., et al. (2004). Evidence for dynamically organized modularity in the yeast protein-protein interaction network. Nature 430(6995):88–93.
2 .S.NCharney, etwork A nalyses of USA C omplex Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis et al., Oxford University Press - OSO, 2018. 07:33:44.
Jansen, R., Yu, H., et al. (2003). A Bayesian networks approach for predicting protein– protein interactions from genomic data. Science 302(5644):449–453. Kanehisa, M., Sato, Y., et al.(2016). KEGG as a reference resource for gene and protein annotation. Nucleic Acids Res 44(D1):D457–D462. Kilpelainen, T.O., Carli, J. F., et al. (2016). Genome-wide meta-analysis uncovers novel loci influencing circulating leptin levels. Nat Commun 7:10494. Kravets, D. (2010). Privacy in peril: lawyers, nations clamor for Google Wi-Fi data. Wired Magazine. https://www.wired.com/2010/06/ privacy-in-peril/. Lamb, J.R., Zhang, C., et al. (2011). Predictive genes in adjacent normal tissue are preferentially altered by sCNV during tumorigenesis in liver cancer and may rate limiting. PLoS One 6(7):e20090. Lawlor, D.A., Harbord, R.M., et al. (2008). Mendelian randomization: using genes as instruments for making causal inferences in epidemiology. Stat Med 27(8):1133–1163. Lee, I., Date, S.V., et al. (2004). A probabilistic functional network of yeast genes. Science 306(5701):1555–1558. Lee, S.I., Pe’er, D., et al. (2006). Identifying regulatory mechanisms using individual variation reveals key role for chromatin modification. Proc Natl Acad Sci U S A 103(38):14062–14067. Lek, M., Karczewski, K.J., et al., and Exome Aggregation Consortium. (2016). Analysis of protein-coding genetic variation in 60,706 humans. Nature 536(7616):285–291. Lu, Y., Day, F.R., et al. (2016). New loci for body fat percentage reveal link between adiposity and cardiometabolic disease risk. Nat Commun 7:10495. Lum, P.Y., Chen, Y., et al.J (2006). Elucidating the murine brain transcriptional network in a segregating mouse population to identify core functional modules for obesity and diabetes. J Neurochem 97(Suppl 1):50–62. Luscombe, N.M., Babu, M.M., et al. (2004). Genomic analysis of regulatory network dynamics reveals large topological changes. Nature 431(7006):308–312. Madigan, D., and York, J. (1995). Bayesian graphical models for discrete data. Int Stat Rev 63:215–232. Margolin, A.A., Wang, K., et al. (2006). Reverse engineering cellular networks. Nat Protoc 1(2):662–671. Mehrabian, M., Allayee, H., et al. (2005). Integrating genotypic and expression data in a segregating mouse population to identify 5- lipoxygenase as a susceptibility gene for obesity and bone traits. Nat Genet 37(11):1224–1233. Millstein, J., Winrow, C.J., et al. (2011). Identification of causal genes, networks, and transcriptional regulators of REM sleep and wake. Sleep 34(11):1469–1477. Millstein, J., Zhang, B., et al. (2009). Disentangling molecular relationships with a causal inference test. BMC Genet 10:23. Monks, S.A., Leonardson, A., et al. (2004). Genetic inheritance of gene expression in human cell lines. Am J Hum Genet 75(6):1094–1105. Morris, M.K., Saez-Rodriguez, J., et al. (2010). Logic-based models for the analysis of cell signaling networks. Biochemistry 49(15): 3216–3224. Mumford, J.A., Horvath, S., et al. (2010). Detecting network modules in fMRI time series: a weighted network analysis approach. Neuroimage 52(4):1465–1476. Narayanan, M., Huynh, J.L., et al. (2014). Common dysregulation network in the human prefrontal cortex underlies two neurodegenerative diseases. Mol Syst Biol 10:743. Nitsch, D., Molokhia, M., et al. (2006). Limits to causal inference based on Mendelian randomization: a comparison with randomized controlled trials. Am J Epidemiol 163(5):397–403. Pearl, J. (1988). Probabilistic reasoning in intelligent systems: networks of plausible inference. San Mateo, CA: Morgan Kaufmann Publishers. Pinto, D., Pagnamenta, A.T., et al. (2010). Functional impact of global rare copy number variation in autism spectrum disorders. Nature 466(7304):368–372.
Roussos, P., Mitchell, A.C., et al. (2014). A role for noncoding variation in schizophrenia. Cell Rep 9(4):1417–1429. Schadt, E.E. (2009). Molecular networks as sensors and drivers of common human diseases. Nature 461(7261):218–223. Schadt, E.E., Friend, S.H., and Shaywitz, D.A. (2009). A network view of disease and compound screening. Nat Rev Drug Discov 8(4):286–295. Schadt, E.E., Lamb, J., et al. (2005). An integrative genomics approach to infer causal associations between gene expression and disease. Nat Genet 37(7):710–717. Schadt, E.E., Turner, S., and Kasarskis, A. (2010). A window into third- generation sequencing. Hum Mol Genet 19(R2):R227–R240. Schwarz, G. (1978). Estimating the dimension of a model. Ann Stat 6(2):461–464. Shirasaki, D.I., Greiner, E.R., et al. (2012). Network organization of the huntingtin proteomic interactome in mammalian brain. Neuron 75(1):41–57. Sieberts, S.K., and Schadt, E.E. (2007). Moving toward a system genetics view of disease. Mamm Genome 18(6-7):389–401. Smith, H.H., Brookhaven National Laboratory, and U.S. Atomic Energy Commission. (1972). Evolution of genetic systems. New York: Gordon and Breach. Stuart, J.M., Segal, E., et al. (2003). A gene-coexpression network for global discovery of conserved genetic modules. Science 302(5643):249–255. van de Vijver, M.J., He, Y.D., et al. (2002). A gene-expression signature as a predictor of survival in breast cancer. N Engl J Med 347(25):1999–2009. van’t Veer, L.J., Dai, H., et al. (2002). Gene expression profiling predicts clinical outcome of breast cancer. Nature 415(6871):530–536. Voineagu, I., Wang, X., et al. (2011). Transcriptomic analysis of autistic brain reveals convergent molecular pathology. Nature 474(7351): 380–384. Wang, I.M., Zhang, B., et al. (2012). Systems analysis of eleven rodent disease models reveals an inflammatome signature and key drivers. Mol Syst Biol 8:594. Welter, D., MacArthur, J., et al. (2014). The NHGRI GWAS Catalog, a curated resource of SNP- trait associations. Nucleic Acids Res 42(Database issue):D1001–D1006. Wilhelm, T., Behre, J., and Schuster, S. (2004). Analysis of structural robustness of metabolic networks. Syst Biol (Stevenage) 1(1):114–120. Witte, J.S. (2010). Genome-wide association studies and beyond. Annu Rev Public Health 31:9–20. Wu, Y., Zhang, X., et al. (2009). Identification of a topological characteristic responsible for the biological robustness of regulatory networks. PLoS Comput Biol 5(7):e1000442. Yang, X., Deignan, J.L., et al. (2009). Validation of candidate causal genes for obesity that affect shared metabolic pathways and networks. Nat Genet 41(4):415–423. Zerhouni, E. (2003). Medicine. The NIH Roadmap. Science 302(5642): 63–72. Zhang, B., Gaiteri, C., et al. (2013). Integrated systems approach identifies genetic nodes and networks in late-onset Alzheimer’s disease. Cell 153(3):707–720. Zhong, H., Beaulaurier, J., et al. (2010). Liver and adipose expression associated SNPs are enriched for association to type 2 diabetes. PLoS Genet 6(5):e1000932. Zhong, H., Yang, X., et al. (2010). Integrating pathway analysis and genetics of gene expression for genome-wide association studies. Am J Hum Genet 86(4):581–591. Zhu, J., Lum, P. Y., et al. (2004). An integrative genomics approach to the reconstruction of gene networks in segregating populations. Cytogenet Genome Res 105(2-4):363–374. Zhu, J., Sova, P., et al. (2012). Stitching together multiple data dimensions reveals interacting metabolomic and transcriptomic networks that modulate cell regulation. PLoS Biol 10(4):e1001301. Zhu, J., Zhang, B., et al. (2008). Integrating large-scale functional genomic data to dissect the complexity of yeast regulatory networks. Nat Genet 40(7):854–861.
34 •S. E merging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford University Press USA - OSO, T 2018. 07:33:44.
3. THE HUMAN BRAIN AND ITS EPIGENOMES Andrew Chess and Schahram Akbarian
INTRODUCTION Psychiatric disorders, including autism, mood and anxiety or psychosis spectrum disorders, substance abuse, and addiction each lack a unifying molecular or cellular pathology, and most cases are believed to be of multifactorial etiology with numerous environmental and genetic components involved. This, taken together with the fact that laboratory animal models, including rats and mice, do not reflect the full complexities surrounding disorders of higher cognition and emotion, poses a formidable challenge in our quest for deeper understanding of the underlying pathophysiology of disease. Consider that conventional psychopharmacology, including drugs targeting monoamine signaling (e.g., dopaminergic, serotonergic, and noradrenergic pathways) elicits an insufficient therapeutic response in one half or less of patients diagnosed with schizophrenia and related illnesses (Lehman et al., 2004) or depression and anxiety (Krishnan and Nestler, 2010). Thus, it will be necessary to further explore the neurobiology and molecular pathology of mental disorders in order to develop novel treatment strategies of higher efficacy. One promising avenue of research is epi-(Greek for over, above) genetics (Labrie, Pai, and Petronis, 2012), a field that has continually been a “hot topic” at annual conventions of neuroscientists and psychiatrists for at least 15 years. Excitement regarding epigenetics stems from a number of avenues. First, human and animal brain studies have shown that many epigenetic markings, including DNA methylation and many types of histone modifications, remain “plastic” throughout all periods of development and aging, with ongoing dynamic regulation even in neurons and other differentiated cells. Changes in neuronal activity, learning, and memory, including the establishment of reward and addiction–related behaviors, and numerous other paradigms all have been shown to be associated with DNA methylation and histone modification, and histone variant changes at specific genomic sequences in brain chromatin (Day and Sweatt, 2011; Maze et al., 2015; Robison and Nestler, 2011). Obviously, epigenetics represents molecular systems operating at the genome–environment intersect, a concept deeply rooted in modern psychology including the behavioral sciences (Weaver et al., 2004). Second, recent work has revealed that causative mutations in a subset of monogenetic neurological disorders (including Rubinstein-Taybi, Kleefstra
and Rett syndromes to name a few examples) disrupt protein function involved in the regulation of chromatin structure and function. These findings from clinical genetics have indicated that the developing brain indeed is sensitive to dysregulation of the epigenetic machinery, and neurological disease could arise from more widespread chromatin defects affecting the immature brain. Moreover, mutations in chromatin regulatory proteins were subsequently found even in some cases with adult-onset psychosis or dementia. This would imply that “chromatin disorders” go beyond “static” lesions confined to the developing nervous system ( Jakocevski and Akbarian, 2012). Third, a subset of chromatin modifying drugs—compounds with inhibitory activity directed against histone deacetylases are a well-known example—have demonstrated a promising therapeutic potential in animal models for cognitive and neurodegenerative conditions (Fischer et al., 2010). In addition, a subset of disease-associated DNA structural variants, including common polymorphisms and multi–base pair deletions and duplications are thought to involve regulatory and probably noncoding DNA. Mapping and superimposing epigenomic landscapes with the genetic risk architecture of common psychiatric disease such as schizophrenia and autism is starting to illuminate disease-relevant function for an increasing number of noncoding sequences (Fullard et al., 2016). In the following, we will, after a concise introduction to the various markings and molecules that define a cell’s epigenome, touch upon the points raised. T H E E P I G E N O M E — GENERAL PRINCIPLES The elementary unit of chromatin is the nucleosome, or 146 bp of genomic DNA wrapped around an octamer of core histones, connected by linker DNA and linker histones. The collective set of covalent DNA and histone modifications and variant histones provide the major building blocks for the “epigenome,” or the epigenetic landscapes that define the functional architecture of the genome, including its organization into many tens of thousands of transcriptional units, clusters of condensed chromatin, and other features that are differentially regulated in different cell types and developmental stages of the organism. An in-depth description of all epigenetic markings would be far beyond this review chapter,
3 5 USA - OSO, 2018. Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press 07:33:44.
but there are multiple reviews providing excellent starting points for the reader interested to learn more (Ederveen et al., 2011; Kinney et al., 2011; Soshnev et al., 2016; Zhou et al., 2011). Here, we confine the discussion to a subset of the epigenetic markings repeatedly explored in human and animal brain. Common terminology used in chromatin studies includes nucleosomes, composed of a protein octamer of four small proteins, the nucleosome core histones around which 146bp of DNA is wrapped. Transcription start sites are often defined by a nucleosome-free interval, probably for increased access of the transcriptional initiation complex and other regulators of gene expression. Arrays of nucleosomes, connected by linker DNA and linker histones, comprise the 10nm “beads-on-a- string” chromatin fiber. Euchromatin defines loose chromatin typically at sites of actively transcribed genes and units poised for transcription. Heterochromatin defines tightly packed nucleosomal arrays. Constitutive heterochromatin remains highly condensed in most interphase nuclei. Examples include centromeric and telomeric repeat DNA, the inactivated X- chromosome (“Barr body”) of female somatic cells, and other chromosomal structures often found in close proximity to the nuclear envelope and also around the nucleolus (see Figure 3.1). Facultative heterochromatin includes silenced genes that, upon differentiation or other stimuli, could switch to a state of active transcription. D NA M ET H Y L AT I O N
Two related but functionally very different types of DNA cytosine modifications, methylation (5mC) and hydroxymethylation (5hmC) of the fifth carbon of cytosines in CpG dinucleotides, provide the bulk of the epigenetic modifications in vertebrate DNA (Kriaucionis and Heintz, 2009) together with some of their chemical intermediates (Ito, et al., 2011). These are most encountered at the site of CpG dinucleotides, but there many sites of nonCpG cytosines methylated in brain tissue (Xie et al., 2012). There are many studies that report changes in promoter DNA methylation (mostly in conjunction with decreased gene expression) in preclinical models of psychosis, depression, and addiction, as well as in brain tissue in subjects diagnosed with one of these conditions. Interestingly, however, while the largest amount, or 97%, of 5mCs are found in intragenic and intergenic sequences and within DNA repeats (Maunakea et al., 2010), only a few of these studies have explored brain DNA methylation changes at repeat DNA and other sequences outside of promoters. For an overview on DNA methylation and hydroxymethylation in the context of human brain development and disease see Kato and Iwamoto (2014). In addition, there is increasing evidence for a second type of DNA methylation at the adenine N6 residue. However, the amount of methyl-adenine, already very low in stem cells, appears to be even lower in differentiated tissues including brain (Koziol et al., 2016), and the functional significance of this non-cytosine DNA methylation type remains to be explored. Likewise, the significance of the recently reported N(6)methyladenosine modification in a very small subset of
RNA adenosine residues (Chen et al., 2015) remains incompletely understood. H I S TO N E MO D I FI C AT I O NS
Chromatin regulation by virtue of chemical histone modifications is much more complex than the DNA methylation discussed, and it is now thought that there are far more than 100 amino acid residue–specific posttranslational modifications (PTMs) in a typical vertebrate cell (Tan et al., 2011). These include, for example, residue-specific mono (me1), di (me2)-and tri (me3) methylation, acetylation, and crotonylation (Baumann, 2015). These site-and residue-specific PTMs are typically explored in the context of chromatin structure and function, with an epigenetic histone code (a combinatorial set of histone PTMs that differentiates between promoters, gene bodies, enhancer, and other regulatory sequences), condensed heterochromatin, and so on (Zhou et al., 2011). See Figure 3.1, providing a very basic overview of the molecular building blocks (but by far not an exhaustive illustration) of the epigenome. It is important to emphasize that histone PTMs rarely occur in isolation; rather, multiple histone PTMs appear to be co-regulated and, as a group, define the aforementioned chromatin states (Berger, 2007). Many active promoters, for example, are defined by high levels of histone H3 lysine 4 methylation and various histone lysine acetylation markings (Zhou et al., 2011). Furthermore, there is also evidence for a coordinated and sequential regulation; phosphorylation of histone H3 at the serine (S)10 position often serves as a trigger for subsequent acetylation of neighboring lysine residues H3K9 and H3K14 in the context of transcriptional activation, while at the same time blocking repression-associated methylation of H3K9 (Nowak and Corces, 2004). H I S TO N E VA R I A N TS
In addition to the core histones H2A/H2B/H3/H4, histone variants such as H3.3, H2A.Z, and H2A.X exist (Figure 3.1). The role of these variant histones, which differ from the canonical histone only at very few amino acid positions, is often discussed in the context of replication- independent expression and assembly (Woodcock, 2006), and several histone variants robustly affect nucleosome stability and compaction ( Jin and Felsenfeld, 2007). One popular model postulates that during the process of gene expression, RNA polymerase and the transcriptional activation and elongator complexes destabilize nucleosomes, which in turn promotes nucleosome remodeling and variant histone incorporation, which then further potentiate or stabilize gene expression (Bintu et al., 2011; Sutcliffe et al., 2009). Recent studies have shown that replication- independent turnover of nucleosomes provides a highly dynamic regulatory mechanism throughout the entire lifespan of the brain, with two specific histone variants, H3.3 and H2A.Z, assigned an essential role in cognition, learning, and synaptic plasticity (Maze et al., 2015; Wenderski and Maze, 2016; Zovkic et al., 2014).
36 •S. E merging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford University Press USA - OSO, T 2018. 07:33:44.
The epigenome, from nucleus to nucleosome. Schematic illustration of (green) gene poised for transcription by polymerase II (Pol II) initiation complex, with nucleosome free interval at transcription start site (TSS). (blue) distal enhancer sequence which in loop-like structure moves in close proximity to active gene. (red) marks a small subset of heterochromatic portions of the genome, including silenced gene and heterochromatic structures bordering the nuclear envelope and pore complex, and also the nucleolar periphery. A small subset of representative histone variants and histone H3 site-specific lysine (K) residues at N-terminal tail (K4, K9, K27, K36, K79) and H4K20 residue are shown as indicated, together with panel of mono-and trimethyl, or acetyl modifications that differentiate between active promoters, transcribed gene bodies, and repressive chromatin, as indicated. DNA cytosines that are hydroxymethylated at the C5 position are mostly found at active promoters, while methylated cytosines are positioned within the body of actively transcribed genes and around repressed promoters and in constitutive heterochromatin. Figure 3.1
HIGHER ORDER C H RO M AT I N S T RU C T U R E S
The epigenome is packaged into higher order chromatin structures. Epigenetic decoration of nucleosomes, including the DNA and histone modifications, and histone variants described, in themselves would fall short to adequately describe the epigenome or even the localized chromatin architecture at any given (genomic) locus. This is because nucleosomal organization leads to only a sevenfold increase in packaging density of the genetic material, as compared to naked DNA; however, the actual level of compaction in the vertebrate nucleus in interphase (which defines the nucleus during the time period a cell is not dividing, including postmitotic cells such as neurons) is about three orders of magnitude higher (Belmont, 2006). The chromosomal arrangements in the interphase nucleus are not random, however. Specifically, loci at sites of active gene expression are more likely to be clustered together and positioned toward a central point within the nucleus, while heterochromatin and silenced loci move more toward the nuclear periphery (Cremer and Cremer, 2001; Duan et al., 2010). Chromatin loopings, in particular, are among the most highly regulated “supranucleosomal” structures, and are associated with transcriptional regulation by, for example, positioning distal regulatory enhancer or silencer elements that—in the linear genome—are positioned potentially many hundred kilobases apart from a gene, to interact directly with that specific promoter. Scaffolding and regulatory proteins play a critical role for the spatial conformations of the chromosomal materials. Such key protein components
include the cohesin complex and the CCCTC-binding factor/zinc finger protein CTCF. Ring-like protein structures are thought to entrap chromosomal loopings, and represent the assembled cohesion complex with its five core subunits SMC1, SMC3, RAD21/REC8, and STAG1-3 in humans (Nasmyth and Haering, 2009). In addition, accessory proteins load or release the cohesion complex onto chromosomes (Nasmyth and Haering, 2009). CTCF orchestrates cohesin enrichment at select binding sites (Wendt et al., 2008). As a result, chromosomal loopings co-occupied by cohesins and CTCF at both ends often associate with broader stretches of regulatory domains, marking the co-regulated repression or expression of groups of genes in a cell type–specific manner (Dowen et al., 2014). Three-dimensional chromatin architectures are commonly mapped using derivatives of chromosome conformation capture (3C). This technique was originally developed for simple eukaryote systems such as yeast (Dekkeretal., 2002) but has been further advanced to include 4C, 5C, HiC, and ChIA- PET (Simonis et al., 2007). This has allowed the mapping of chromosomal architectures across many megabases, or, in case of HiC and ChIA-PET, even genome-wide. At its core, the technique explores physical interactions between DNA fragments separated by interspersed sequence (chromosome architecture in cis) or between sequences positioned in different chromosomes (interactions in trans). Crosslinked chromatin is digested with a specific restriction enzyme, religated, and amplified using primer pairs for which forward and reverse primers match to different portions of the genomic
he Het uman rain and I ts E pigenomes Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis3.S.T Charney, al., OxfordBUniversity Press USA - OSO, 2018. 07:33:44.
locus of interest. Of note, there is evidence that higher order chromatin structures, including chromosomal loopings and other types of chromosomal conformations capture, are maintained for many hours in postmortem brain tissue after death (Mitchell et al., 2014). Following this observation, early studies already are drawing links between the genetic risk architecture of schizophrenia, noncoding DNA, and chromosomal loop- bound regulatory DNA elements (Bharadwaj et al., 2014; Roussos et al., 2014). A P R I M E R O N D E E P S EQ U E N C I N G T EC H N O L O GY
Comprehensive genome-scale mapping of the transcriptome and epigenome from normal and diseased tissues and cells has emerged as a widely adopted approach in all areas of medicine, including psychiatry and translational neuroscience. Typically, the DNA and RNA samples collected from specimens or cells are processed as (DNA) libraries by “deep sequencing.” This involves the generation and sequencing of many millions of short DNA strands from each sample, followed by bioinformatical analyses to assign, for each locus of the genome, (1) levels of RNA (RNA-seq), (2) histone modifications (histone ChIP-seq; ChIP stands for chromatin immunoprecipitation), or (3) chromosomal loopings and conformations (Hi-C), just to mention three examples. For an overview on deep sequencing (also called “next-generation” sequencing) approaches and challenges in neurogenomics, see Maze et al. (2014).
C H R O M AT I N M A R K I N G S A N D T H E N E U R O B I O L O GY O F P SYC H I AT R I C D I S E A S E D EV E L O PM E N TA L P L A S T I C IT Y O F BRAIN EPIGENOMES
Most or perhaps all epigenetic markings studied to date, including DNA methylation, are now thought to be reversible and subject to bidirectional regulation in somatic tissues including brain, and there is no a priori reason for the unidirectional accumulation of a specific epigenetic mark while the brain is maturing and aging. Nonetheless, multiple lines of evidence suggest that there is substantial reorganization of chromatin structures during the course of postnatal development and aging. Human cerebral cortex, for example, shows complex and gene-specific changes in the amount of 5mC (cytosine methylated at the carbon 5 position). There is a fast rise in 5mC at many promoters during the transition from perinatal to postnatal ages that continues at a slower pace into old age in conjunction with subtle changes (mostly a decline) in expression of transcripts originating from these promoters (Hernandez et al., 2011; Numata et al., 2012; Siegmund et al., 2007). Such types of age-related changes in DNA methylation levels in the immature brain are of interest even in the context of adult-onset common psychiatric disorders such as schizophrenia, as illustrated by the following example: In a recent postmortem study of
prefrontal cortex ( Jaffe et al., 2015) DNA methylation was examined genome-wide in >520 subjects collected across a wide age range, from the 14th week of gestation to 80- year-old subjects, with 191 subjects diagnosed with schizophrenia included in the adult cohort. There was large-scale DNA methylation remodeling (with >230,000 of 456,000 autosomal CpG dinucleotides affected) during the transition from second fetal trimester to postnatal life, apparently primarily because of shifts in cell type composition, attributed to decreasing progenitor pools, emergence of glia, and neuronal differentiation in the more mature tissue samples. Interestingly, 94% of the 2104 CpGs that were differentially methylated in prefrontal cortex of adult schizophrenia subjects (as compared to adult controls) showed significant differential methylation during the transition from fetal to postnatal life (representing a 16.5-fold enrichment above expected by chance). Only 31 of the 2104 (1.5%) showed significant differential methylation during the transition (amongst controls) from adolescence to adult (representing a depletion of ~4 fold compared to expected). The authors ( Jaffe et al., 2015) conclude that most DNA methylation changes observed in adult schizophrenia brains, as compared to control brains, are sites that normally undergo methylation changes in early neurodevelopment. Like the aforementioned dynamic changes in DNA methylation during the course of development and aging, the epigenetic landscapes of histone modifications and histone variants also undergo substantial reorganization across the lifespan of the human brain. For example, approximately 1500 loci in the neuronal genomes from the human prefrontal cortex undergo age-related changes in histone H3K4 trimethylation, a process that starts before birth and that appears to continue at least until early adulthood (Shulha et al., 2013). Furthermore, the hippocampus of aged, 16-month-old wild- type mice shows deficits in acetylated histone H3-lysine 12 (H4K12) (Peleg et al., 2010), a histone PTM that is broadly correlated with the transcriptional elongation process (Peleg et al., 2010). It is possible that age-related drifts in brain epigenomes negatively affect neuronal (Fischer et al., 2010; Lu et al., 2004) and oligodendroglial (Copray et al., 2009) transcriptomes, thereby contributing to a decline in the signaling capacity of nerve cells, defects in axon myelination, and other molecular defects that have been linked to cognitive disorders of the adult brain. These include Alzheimer’s disease, aneurodegenerative disease (Yankner et al., 2008), and conditions such as schizophrenia that are not accompanied by ongoing loss of nerve cells (Tang et al., 2009). Furthermore, histone variants such as H3.3 show rapid accumulation in bulk chromatin during postnatal maturation of human and mouse brain, apparently with different kinetics in neuronal versus non-neuronal nuclei (Maze et al., 2015). Subsequently, H3.3 levels plateau in neuronal and glial genomes of the adult brain, with dynamic turnover limited to actively regulated transcription start sites and possibly other types of cis- regulatory sequences associated with gene expression (Maze et al., 2015). Taken together, these examples affirm that brain epigenomes are indeed subject to dynamic changes throughout all periods of maturation and aging.
38 •S. E merging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford University Press USA - OSO, T 2018. 07:33:44.
M O N O G E N ET I C ET I O L O G I E S O F N E U R O P SYC H I AT R I C D I S E A S E The importance of proper regulation of chromatin structure and function for normal human brain development and function is further underscored by findings from clinical genetics, associating a rapidly increasing list of genes encoding specific chromatin regulators with monogenic forms of psychiatric disease (Ronan et al., 2013). This may not be too surprising, given that there are many hundreds of genes that encode proteins that either write, erase, or read the molecular markings of the epigenome. A detailed description of the epigenome’s molecular machineries, or an exhaustive discussion of disease- associated genetic syndromes, would be beyond the scope of this book chapter. However, we would like to emphasize that mutations and maladaptations of the epigenetic machinery cover a wide continuum of neurological disease, from developmental syndromes to adult-onset neurodegenerative disease. Mutations in DNA cytosine methyltransferase genes could serve as a case in point. Hypomorphic (partial lossof-function) mutations in the DNA methyltransferase gene DNMT3B are associated with a multiorgan syndrome—Immunodeficiency, Centromere Instability, Facial anomalies (ICF 1)—mental retardation, and defective brain development (Hansen et al., 1999; Okano et al., 1999). However, mutations in a different DNA methyltransferase, DNMT1, are responsible for some cases of hereditary sensory and autonomic neuropathy, type 1 (HSAN1), with adult-onset dementia (Klein et al., 2011). In other pedigrees, DNMT1 mutations were linked to narcolepsy and late-onset deafness and cerebellar ataxia (Winkelmann et al., 2012). Likewise, DNA variants and mutations encompassing the KMT1D gene (9q34.3) encoding a histone H3- lysine 9 specific methyltransferase, were initially recognized as the causative gene responsible for a distinct neurodevelopmental and multiorgan syndome (the Kleefstra mental retardation syndrome; see Kleefstra et al., 2009). However, KMT1D mutations are also responsible for some cases with schizophrenia or nonspecific psychiatric and neurodegenerative disease in the post adolescent period ( Jakovcevski and Akbarian, 2012). Likewise, mutations in the gene encoding SETD1A encoding a histone H3-lysine 4-specific methyltransferase have been linked both to autism as a disorder of early childhood and to schizophrenia as a disorder with onset in young adulthood. These examples, taken together, clearly show that epigenomic dysregulation could negatively impact brain function across a very wide age range. Importantly, deleterious mutations in genes encoding scaffolding proteins for proper 3-dimensional foldings of the chromosomal material inside the cell nuclei (including of postmitotic cells) have also been linked to psychiatric disease. These include intellectual disability, psychosis, and adult- onset progressive demyelination (Boyle et al., 2015; Finnsson et al., 2015; Nasmyth and Haering, 2009; Yan et al., 2009). The underlying genetic defect includes microdeletions and copy number variations affecting core members of the cohesin complex including SMC1A and SMC3, and the accessory subunit NIPBL (Boyle et al., 2015). In addition, genetic mutations in CTCF, as a key organizer for chromosomal loopings,
have been linked to monogenic causes of microcephaly and cognitive disorder (Gregor et al., 2013; Watson et al., 2014). E P I G E N O M I C A P P R OAC H E S TOWA R D D I S E A S E -A S S O C I AT E D NONCODING DNA S T RU C T U R A L VA R I A N T S A significant portion of (psychiatric) disease-associated mutations and polymorphisms are thought to cause functional changes other than alterations in protein coding sequence. This is unsurprising considering that less than 2% of the human genome encodes protein, but it poses a potential challenge because the functional role of noncoding DNA sequence and the (disease-related) structural variants may be hard to discern by sequence analyses alone. It is noteworthy that whole genome sequencing studies are beginning to identify psychiatric disease cases with no apparent disease-associated mutations in the exome (the protein-coding portion of the genome), but instead mutations in noncoding DNA sensitive to DNAse I digest, an indicator for nucleosome-free regulatory DNA bound by transcription factors (Turner et al., 2016). Many of these noncoding DNA deletions and duplications are within 100kb of a well established neurodevelopmental risk gene (such as, for example, DSCAM, encoding Down Syndrome Cell Adhesion Molecule, and SCN2A encoding a sodium voltage-gated channel subunit implicated in autism and seizure disorder (Turner et al., 2016). Pending further investigations, these cases may represent monogenic forms of neurodevelopmental disease due to loss of regulatory elements important for transcriptional and epigenomic regulation of associated genes. Furthermore, genome-wide association (GWA) studies have produced over 100 blocks of genome sequence (“haplotypes”), each defined by a set of common polymorphisms (mostly SNPs) in linkage disequilibrium, with each haplotype contributing a small fraction to the genetic liability of schizophrenia (Schizophrenia Working Group of the Psychiatric Genomics, 2014). With some studies now including hundreds of thousands of probands, genetic risk haplotypes are even emerging for psychiatric conditions such as depression and neuroticism that were previously considered less tractable in GWA studies (Okbay et al., 2016). However, the disease- associated genomic regions are frequently large and often contained multiple implicated genetic variants due to local linkage disequilibrium patterns. In order to understand these associations mechanistically, it is critical to develop strategies for honing in on regions and genetic variants more likely to have functional effects. Thus, the elucidation of the function of noncoding disease-associated loci through neuroepigenomics is an important next step toward the development of testable hypotheses regarding biological processes involved in the pathogenesis of neuropsychiatric disorders. Importantly, a proportion of genome-wide associated variants in transcriptional regulatory mechanisms involve expression quantitative trait loci (eQTL), defined by the polymorphism correlating with expression of a gene located elsewhere on the same or a different chromosome as the SNP, including modulation
he Het uman rain and I ts E pigenomes Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis3.S.T Charney, al., OxfordBUniversity Press USA - OSO, 2018. 07:33:44.
of cis-regulatory elements (CREs) (Cookson et al., 2009; Harismendy et al., 2011; Maurano et al., 2012; Musunuru et al., 2010). A CRE, such as a promoter, enhancer or silencer, is a noncoding DNA sequence in, near or distal to a gene that contains binding sites for regulatory factors and is required for proper spatiotemporal expression of the gene. The proposed mechanism is that disease-associated variants that lie within CREs, affect the binding of regulatory proteins, such as transcription factors, leading to allele-specific differences in transcription and subsequent disease-related alterations in molecular pathways. Efforts are underway to superimpose the epigenomic landscape from human brain tissue, including histone methylation profiles and promoter/enhancer CREs, onto the genetic risk map of schizophrenia. Early studies using this approach were able to define numerous risk-associated CREs mechanistically linked to long-range chromosomal loop formations bypassing hundreds of kilobases of linear genome in order to physically interact with gene transcription start sites (Roussos et al., 2014). It is likely that in the near future many noncoding sequences will be assigned to neurological function and disease vulnerability via transcriptional mechanisms. OUTLOOK “Neuroepigenetics” is a new discipline which presently takes center stage in the field of mental health research, mainly because (1) recent findings suggest that the epigenetic landscapes of the human brain remain “plastic” throughout all periods of brain development and aging, with ongoing dynamic regulation even in neurons and other postmitotic constituents (Cheung et al., 2010; Hernandez et al., 2011; Numata et al., 2012; Siegmund et al., 2007); (2) the range of neurological conditions due to a primary chromatin defect extends far beyond the early developmental period and may even include a subset of cases with adult-onset psychosis, or dementia and other neurodegenerative disease; (3) chromatin-modifying drugs could lead to novel treatments for neurological and psychiatric disease ( Jakovcevski and Akbarian, 2012); and (4) exploration of chromatin structures could be expected to uncover, in a substantial portion of cases, the functional impact of disease-relevant mutations in regulatory and other sequences that are otherwise difficult to “capture” by DNA sequence analyses alone. Indeed, the important role of epigenetically regulated noncoding DNA was ascertained by recent bioinformatical studies showing that many noncoding DNA sequences are generally deficient of SNP and underwent a purifying selection (Tolstorukov et al., 2011). It is important to mention that to date, the vast majority of transcriptome and epigenome studies in diseased tissue and in preclinical models have used tissue homogenate or some pools of many thousands of cells as input. Given the enormous cellular heterogeneity of brain tissue, parsing such types of meta-epigenomes into distinct subtypes will be ultimately accomplished using single-cell approaches. Single-cell RNA-seq approaches are rapidly getting more efficient and cost effective, so it is reasonable to predict that in the next few years many new cell types in rodents will be predicted by
molecular fingerprint, triggering a wave of validation studies with, for example, transgenic approaches. For example, a recent single-cell RNA-seq study in rodent hippocampus and cerebral cortex identified 47 cell types contributing to the brain’s neuronal and glial populations and microvasculature (Zeisel et al., 2015). Another RNA-seq study conducted on neuronal nuclei collected from human cerebral cortex identified 16 different neuronal subtypes (Lake et al., 2016). An important recent advance is the incorporation of a unique molecular index at the stage of reverse transcription. These short random sequences allow one to avoid multiple counting of the same RNA from a single cell, which was a problem plaguing earlier single-cell RNA-seq experiments since most single-cell RNA-seq experiments rely to some extent on PCR (Islam et al., 2014). In a variety of neuronal systems, new subtypes of neurons are likely to emerge from principal component analysis and recent innovative methods of dimensionality reduction (Arsenio et al., 2014) to define new candidate subtypes to be further tested using molecular and physiologic approaches. With newly defined neuronal subtypes in hand, fluorescence-activated cell sorting could be used to purify cells for subsequent epigenetic analyses. To this end, single-cell epigenomic approaches looking at DNA methylation became possible two decades ago (Mostoslavsky et al., 1998) and have advanced markedly with the advent of next-g eneration sequencing, even allowing for simultaneous genome-wide transcriptome and DNA methylome profiling from single neurons (Hu et al., 2016). Single-cell technologies for other epigenomic determinants, including “3D genome” chromosomal conformations (single cell Hi-C) are rapidly emerging (Nagano et al., 2013) and are promising avenues for future work, although sorting out technical noise from true biological differences will be an ongoing challenge. Finally, it is worth mentioning that, based on next- generation sequencing of epigenetic markings in sperm, perhaps as much as 4% of the human genome could maintain nucleosomal organization and many types of epigenetic decoration when transmitted through the germline. This includes many loci considered of critical importance for early pre-and postimplantation development, imprinted gene clusters, microRNA clusters, homeobox (HOX) gene clusters, and the promoters of many stand-alone developmental transcription and signaling factors (Hammoud et al., 2010). These and related findings will most certainly further stimulate research aimed at uncovering evidence for transgenerational epigenetic heritability of psychiatric disease, including depression, schizophrenia, and addiction, to name a few—which all have in common that the elucidated genetic risk architecture does not, at least yet, explain the full extent of disease heritability. Without doubt, psychiatric epigenetics will remain a most productive area of research for many years to come. DISCLOSURES Conflict of interest: The authors declare no conflict of interest.
40 •S. E merging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford University Press USA - OSO, T 2018. 07:33:44.
Acknowledgments: Work conducted in the authors’ laboratories is sponsored by the National Institutes of Health.
Ito, S., Shen L., et al. (2011). Tet proteins can convert 5- methylcytosine to 5-formylcytosine and 5-carboxylcytosine. Science 333(6047):1300–1303. Hernandez, D.G., Nalls, M.A., et al. (2011). Distinct DNA methylation changes highly correlated with chronological age in the human brain. Hum Mol Genet 20(6):1164–1172. REFERENCES Hu, Y., Huang, K., et al. (2016). Simultaneous profiling of transcriptome and DNA methylome from a single cell. Genome Biol 17:88. Arsenio, J., Kakaradov, B., et al. (2014). Early specification of CD8+ T Islam, S., Zeisel, et al. (2014). Quantitative single-cell RNA-seq with unique molecular identifiers. Nat Methods 11(2):163–166. lymphocyte fates during adaptive immunity revealed by single-cell Jaffe, A.E., Gao Y., et al. (2015). Mapping DNA methylation across develgene-expression analyses. Nat Immunol 15(4):365–372. opment, genotype, and schizophrenia in the human frontal cortex. Nat Baumann, K. (2015). Post-translational modifications: Crotonylation verNeurosci 19(1):40–47. sus acetylation. Nat Rev Mol Cell Biol 16(5):265. Belmont, A.S. (2006). Mitotic chromosome structure and condensation. Jakocevski, M., and Akbarian, S. (2012). Epigenetic mechanisms in neurodevelopmental and neurodegenerative disease. Nature Medicine Curr Opin Cell Biol 18(6):632–638. 19(11):1473–1477. Berger, S.L. (2007). The complex language of chromatin regulation during Jakovcevski, M., and Akbarian, S. (2012). Epigenetic mechanisms in neutranscription. Nature 447(7143):407–412. rological disease. Nat Med 18(8):1194–1204. Bharadwaj, R., Peter, C.J., et al. (2014). Conserved higher-order chromatin regulates NMDA receptor gene expression and cognition. Neuron Jin, C., and Felsenfeld, G. (2007). Nucleosome stability mediated by histone variants H3.3 and H2A.Z. Genes Dev 21(12):1519–1529. 84(5):997–1008. Bintu, L., Kopaczynska, M., et al. (2011). The elongation rate of RNA Kato, T., and Iwamoto, K. (2014). Comprehensive DNA methylation and hydroxymethylation analysis in the human brain and its implication in polymerase determines the fate of transcribed nucleosomes. Nat Struct mental disorders. Neuropharmacology 80:133–139. Mol Biol 18(12):1394–1399. Boyle, M.I., Jespersgaard, C., et al. (2015). Cornelia de Lange syndrome. Kinney, S.M., Chin, H.G., et al. (2011). Tissue-specific distribution and dynamic changes of 5-hydroxymethylcytosine in mammalian genomes. Clin Genet 88(1):1–12. J Biol Chem 286(28):24685–24693. Chen, T., Hao, Y.J., et al. (2015). m(6)A RNA methylation is regulated by microRNAs and promotes reprogramming to pluripotency. Cell Stem Kleefstra, T., van Zelst-Stams, W.A., et al. (2009). Further clinical and molecular delineation of the 9q subtelomeric deletion syndrome supCell 16(3):289–301. ports a major contribution of EHMT1 haploinsufficiency to the core Cheung, I., Shulha, H.P., et al. (2010). Developmental regulation and phenotype. J Med Genet 46(9):598–606. individual differences of neuronal H3K4me3 epigenomes in the preKlein, C.J., Botuyan, M.V., et al. (2011). Mutations in DNMT1 cause frontal cortex. Proc Natl Acad Sci U S A 107(19):8824–8829.] hereditary sensory neuropathy with dementia and hearing loss. Nat Cookson, W., Liang, L., et al. (2009). Mapping complex disease traits with Genet 43(6):595–600. global gene expression. Nat Rev Genet 10(3):184–194. Copray, S., Huynh, J.L., et al. (2009). Epigenetic mechanisms facili- Koziol, M.J., Bradshaw, C.R., et al. (2016). Identification of methylated deoxyadenosines in vertebrates reveals diversity in DNA modificatating oligodendrocyte development, maturation, and aging. Glia tions. Nat Struct Mol Biol 23(1):24–30. 57(15):1579–1587. Cremer, T., and Cremer, C. (2001). Chromosome territories, nuclear Kriaucionis, S., and Heintz, N. (2009). The nuclear DNA base 5- hydroxymethylcytosine is present in Purkinje neurons and the brain. architecture and gene regulation in mammalian cells. Nat Rev Genet Science 324(5929):929–930. 2(4):292–301. Day, J.J., and Sweatt, J.D. (2011). Epigenetic mechanisms in cognition. Krishnan, V., and Nestler, E.J. (2010). Linking molecules to mood: new insight into the biology of depression. Am J Psychiatry Neuron 70(5):813–829. 167(11):1305–1320. Dekker, J., Rippe, K., et al. (2002). Capturing chromosome conformation. Labrie, V., Pai, S., and Petronis, A. (2012). Epigenetics of major psychoScience 295(5558):1306–1311. sis: progress, problems and perspectives. Trends Genet 28(9):427–435. Dowen, J.M., Fan, Z.P., et al. (2014). Control of cell identity genes occurs in insulated neighborhoods in mammalian chromosomes. Cell Lake, B.B., Ai, R., et al. (2016). Neuronal subtypes and diversity revealed by single- nucleus RNA sequencing of the human brain. Science 159(2):374–387. 352(6293):1586–1590. Duan, Z., Andronescu, M., et al. (2010). A three-dimensional model of Lehman, A.F., Lieberman, J.A., et al. (2004). Practice guideline for the the yeast genome. Nature 465(7296):363–367. treatment of patients with schizophrenia, second edition. Am J Ederveen, T.H., Mandemaker, I.K., and Logie, C. (2011). The human histone Psychiatry 161(2 Suppl):1–56. H3 complement anno 2011. Biochim Biophys Acta 1809(10):577–586. Finnsson, J., Sundblom, J., et al. (2015). LMNB1-related autosomal- Lu, T., Pan, Y., et al. (2004). Gene regulation and DNA damage in the ageing human brain. Nature 429(6994):883–891. dominant leukodystrophy: clinical and radiological course. Ann Maunakea, A.K., Nagarajan, R.P., et al. (2010). Conserved role of intraNeurol 78(3):412–425. genic DNA methylation in regulating alternative promoters. Nature Fischer, A., Sananbenesi, F., et al. (2010). Targeting the correct HDAC(s) 466(7303):253–257. to treat cognitive disorders. Trends Pharmacol Sci 31(12):605–617. Fullard, J.F., Halene, T.B., et al. (2016). Understanding the genetic lia- Maurano, M.T., Humbert, R., et al. (2012). Systematic localization of common disease- associated variation in regulatory DNA. Science bility to schizophrenia through the neuroepigenome. Schizophr Res 337(6099):1190–1195. 177(1-3):115–124. Gregor, A., Oti, M., et al. (2013). De novo mutations in the genome organizer Maze, I., Shen, L., et al. (2014). Analytical tools and current challenges in the modern era of neuroepigenomics. Nat Neurosci 17(11): CTCF cause intellectual disability. Am J Hum Genet 93(1):124–131. 1476–1490. Hammoud, S.S., Purwar, J., et al. (2010). Alterations in sperm DNA methylation patterns at imprinted loci in two classes of infertility. Fertil Maze, I., Wenderski, W., et al. (2015). Critical role of histone turnover in neuronal transcription and plasticity. Neuron 87(1):77–94. Steril 94(5):1728–1733. Hansen, R.S., Wijmenga, C., et al. (1999). The DNMT3B DNA methyl- Mitchell, A.C., Bharadwaj, R., et al. (2014). The genome in three dimensions: a new frontier in human brain research. Biol Psychiatry transferase gene is mutated in the ICF immunodeficiency syndrome. 75(12):961–969. Proc Natl Acad Sci U S A 96(25):14412–14417. Harismendy, O., Notani, D., et al. (2011). 9p21 DNA variants associ- Mostoslavsky, R., Singh, N., et al. (1998). Kappa chain monoallelic demethylation and the establishment of allelic exclusion. Genes Dev ated with coronary artery disease impair interferon-gamma signalling 12(12):1801–1811. response. Nature 470(7333):264–268.
he Hetuman rain and I ts E pigenomes Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis3.S.T Charney, al., OxfordBUniversity Press USA - OSO, 2018. 07:33:44.
Musunuru, K., Strong, A., et al. (2010). From noncoding variant to phenotype via SORT1 at the 1p13 cholesterol locus. Nature 466(7307):714–719. Nagano, T., Lubling, et al. (2013). Single-cell Hi-C reveals cell-to-cell variability in chromosome structure. Nature 502(7469):59–64. Nasmyth, K., and Haering, C. H. (2009). Cohesin: its roles and mechanisms. Annu Rev Genet 43:525–558. Nowak, S.J., and Corces, V.G. (2004). Phosphorylation of histone H3: a balancing act between chromosome condensation and transcriptional activation. Trends Genet 20(4):214–220. Numata, S., Ye, T., et al. (2012). DNA methylation signatures in development and aging of the human prefrontal cortex. Am J Hum Genet 90(2):260–272. Okano, M., Bell, D.W., et al. (1999). DNA methyltransferases Dnmt3a and Dnmt3b are essential for de novo methylation and mammalian development. Cell 99(3):247–257. Okbay, A., Baselmans, B.M., et al. (2016). Genetic variants associated with subjective well-being, depressive symptoms, and neuroticism identified through genome-wide analyses. Nat Genet 48(6):624–633. Peleg, S., Sananbenesi, F., et al. (2010). Altered histone acetylation is associated with age-dependent memory impairment in mice. Science 328(5979):753–756. Robison, A.J., and Nestler, E.J. (2011). Transcriptional and epigenetic mechanisms of addiction. Nat Rev Neurosci 12(11):623–637. Ronan, J.L., Wu, W., and Crabtree, G.R. (2013). From neural development to cognition: unexpected roles for chromatin. Nat Rev Genet 14(5):347–359. Roussos, P., Mitchell, A.C., et al. (2014). A role for noncoding variation in schizophrenia. Cell Rep 9(4):1417–1429. Schizophrenia Working Group of the Psychiatric Genomics, C. (2014). Biological insights from 108 schizophrenia-associated genetic loci. Nature 511(7510):421–427. Shulha, H.P., Cheung, I., et al. (2013). Coordinated cell type-specific epigenetic remodeling in prefrontal cortex begins before birth and continues into early adulthood. PLoS Genet 9(4):e1003433. Siegmund, K.D., Connor, C.M., et al. (2007). DNA methylation in the human cerebral cortex is dynamically regulated throughout the life span and involves differentiated neurons. PLoS One 2(9):e895. Simonis, M., Kooren, J., and de Laat, W. (2007). An evaluation of 3C-based methods to capture DNA interactions. Nat Methods 4(11):895–901. Soshnev, A.A., Josefowicz, S.Z., and Allis, C.D. (2016). Greater than the sum of parts: complexity of the dynamic epigenome. Mol Cell 62(5):681–694. Sutcliffe, E.L., Parish, I.A., et al. (2009). Dynamic histone variant exchange accompanies gene induction in T cells. Mol Cell Biol 29(7):1972–1986.
Tan, M., Luo, H., et al. (2011). Identification of 67 histone marks and histone lysine crotonylation as a new type of histone modification. Cell 146(6):1016–1028. Tang, B., Chang, W.L., et al. (2009). Normal human aging and early- stage schizophrenia share common molecular profiles. Aging Cell 8(3):339–342. Tolstorukov, M.Y., Volfovsky, N., et al. (2011). Impact of chromatin structure on sequence variability in the human genome. Nat Struct Mol Biol 18(4):510–515. Turner, T.N., Hormozdiari, F., et al. (2016). Genome sequencing of autism-affected families reveals disruption of putative noncoding regulatory DNA. Am J Hum Genet 98(1):58–74. Watson, L.A., Wang, X., et al. (2014). Dual effect of CTCF loss on neuroprogenitor differentiation and survival. J Neurosci 34(8):2860–2870. Weaver, I.C., Cervoni, N., et al. (2004). Epigenetic programming by maternal behavior. Nat Neurosci 7(8):847–854. Wenderski, W., and Maze, I. (2016). Histone turnover and chromatin accessibility: Critical mediators of neurological development, plasticity, and disease. Bioessays 38(5):410–419. Wendt, K.S., Yoshida, K., et al. (2008). Cohesin mediates transcriptional insulation by CCCTC-binding factor. Nature 451(7180):796–801. Winkelmann, J., Lin, L., et al. (2012). Mutations in DNMT1 cause autosomal dominant cerebellar ataxia, deafness and narcolepsy. Hum Mol Genet 21(10):2205–2210. Woodcock, C.L. (2006). Chromatin architecture. Curr Opin Struct Biol 16(2):213–220. Xie, W., Barr, C.L., et al. (2012). Base-resolution analyses of sequence and parent-of-origin dependent DNA methylation in the mouse genome. Cell 148(4):816–831. Yan, J., Zhang, F., et al. (2009). Genomic duplication resulting in increased copy number of genes encoding the sister chromatid cohesion complex conveys clinical consequences distinct from Cornelia de Lange. J Med Genet 46(9):626–634. Yankner, B.A., Lu, T., and Loerch, P. (2008). The aging brain. Annu Rev Pathol 3:41–66. Zeisel, A., Munoz-Manchado, A.B., et al. (2015). Brain structure. Cell types in the mouse cortex and hippocampus revealed by single-cell RNA-seq. Science 347(6226):1138–1142. Zhou, V.W., Goren, A., and Bernstein, B.E. (2011). Charting histone modifications and the functional organization of mammalian genomes. Nat Rev Genet 12(1):7–18. Zovkic, I.B., Paulukaitis, B.S., et al. (2014). Histone H2A.Z subunit exchange controls consolidation of recent and remote memory. Nature 515(7528):582–586.
42 •S. E merging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford University Press USA - OSO, T 2018. 07:33:44.
4. METHODS FOR IN VIVO GENE MANIPULATION Lisa M. Monteggia and Wei Xu
had far reaching effects in neuroscience in allowing a particular gene to be studied in vivo. Transgenic mice are genRecent advances in mouse genetics have opened many new ave- erated by microinjecting DNA into fertilized oocytes. The nues of research in which to explore gene function in the brain, DNA construct usually inserts into a single random site of and potentially to the pathophysiology and treatment of psychi- the genome as multiple copies; however, the lack of control atric disorders. The use of the mouse to explore gene function has of the integration site as well as copies of the gene can be contributed a better understanding of the role of specific genes caveats to the approach. Transgenic mouse lines can be rapin the nervous system as well as circuit analysis and the impact on idly generated, as the DNA integration typically occurs early behavior. Mutagenesis centers generating novel mouse mutants enough in development that the progeny born can transmit that display various phenotypes have been important in identify- the targeted DNA through their germ line. Nevertheless, ing genes that contribute to particular phenotypes/cellular pro- the random DNA integration requires that multiple cesses. With mouse “reverse genetic” approaches, specific genes founder lines be created to ensure any observed phenotype are introduced or deleted from the genome, and the impact in is due to the expression of the exogenous DNA and not vivo can be assessed. While Drosophila and Caenorhabditis ele- with the interference, or influence of regulatory regions, of gans are important genetic models to investigate and identify endogenous genes. The size of the DNA construct that can be microingene function, the use of the mouse has been a more widely used approach for in vivo behavioral studies. Indeed, the advances in jected into the fertilized oocyte is an important considmouse genetics have brought it to the forefront of circuit analy- eration. Typically, small DNA constructs can be injected sis and behavior, surpassing the use of rats that were used in clas- without a problem. However, given the large size of mammalian genes, larger DNA constructs are often needed and sical behavioral studies. The goal of this chapter is to provide information on rely on using bacterial artificial chromosomes (BACs) and genetic approaches that alter gene expression in animal mod- yeast artificial chromosomes to generate large clone transels. Genetically modified mice have allowed the investigation genic mice. The technical advance of using larger DNA of the role of particular genes in vivo. This information has constructs in creating transgenic mice has also allowed provided novel insight into gene function, allowed the valida- for the expression of reporter proteins, such as green fluotion of specific pharmacological drugs, and triggered the inves- rescent protein (GFP), that label a cell to identify what tigation into the pathophysiology and treatment of psychiatric type of cell it is (Heintz, 2004). The use of BAC reporter disorders. While psychiatric disorders are complex and likely mice have been important in distinguishing specific popuinvolve the interaction of many genes as well as environmental lations of neurons to aid in circuit function and characfactors, the ability to start to elucidate the function of specific terization of electrophysiological properties of particular genes and how they influence particular cells, circuits, and ulti- neuronal types. While transgenic mice can be important in expressing mately behavior is an important first step. We discuss transgenic approaches, in which a gene of interest is added to the a particular gene to study its function or dose sensitivity, it animal, and knockout mice, in which a gene of interest is dis- can also be used to express a mutant gene. Dominant negarupted or inactivated. We also discuss recent advances in viral- tive mutations, when expressed, act on the wild-type allele to mediated gene transfer that allow for more defined spatial and antagonize its expression. The expression of a gene that acts temporal control over gene function. Finally, we discuss the use against the wild-type endogenous allele can provide critiof these approaches for controlling neuronal function and cir- cal insight into whether the mutation is a gain of function. cuitry with implications for molecular psychiatry. While the generation of transgenic mouse lines has provided critical information on gene function, as well as identification of specific cell populations, there are differences between the physiology and anatomy of mice and humans. Other species, TR ANSGENIC MICE particularly rats, are being developed as transgenics for certain Transgenic mice are created by introducing exogenous genes research areas including addiction, as rats have been better into the genome. This technical advance in mouse genetics studied in some fields. INTRODUCTION
4 3 USA - OSO, 2018. Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press 07:33:44.
C O N S T I T U T I VE K N O C KO U T M I C E Genetic knockouts involve the deletion of endogenous genes. The generation of knockout mice involves the gene of interest to be targeted for removal rather than a random integration event of the DNA. Homologous recombination is a process that involves recombination occurring between introduced DNA and the genome, a rather rare event compared to random integration. Homologous recombination is performed in embryonic stem (ES) cells and then the cells are screened for the desired recombination event (Mansour et al., 1988). The ES cells with the selected recombination event are then expanded and introduced into a developing mouse embryo, and the resulting chimeric mouse, once screened for the targeted DNA construct, can be bred and should pass on the genetic alterations to its progeny. This approach can be used to generate constitutive homozygous gene knockout or knock- in mice, in which recombination events replace the original gene with a mutated version of the gene or a reporter gene. The generation of knockout mice has allowed researchers to examine the contribution of specific genes to brain function as well as the pathophysiology and treatment of mental disorders. Knockouts have also been useful in testing the specificity of pharmacological drugs. Homologous recombination approaches can be used to generate knockout mice that are null for a particular targeted gene. However, disorders due to the loss of function of only one allele can also be studied. These haploinsufficiency disorders can be studied using heterozygous mice missing only one copy of a gene. The study of heterozygous mice can also allow one to investigate whether there is a gene dosage effect for a particular phenotype. While knockout studies have been performed mainly in mice, recent work has started to examine rat knockout models. Many areas of neuroscience have a long history of research utilizing rat models. However, with the advent of mouse genetics there has been a shift toward the mouse, although there are behavioral differences between mice and rats. The completion of the rat genome project (Gibbs et al., 2004) has created opportunities to target the rat genome. A robust method for establishing rat ES cells has recently been developed, which also made it possible to efficiently generate knockout or knock-in rats (Li et al., 2008). The use of rat models may be particularly valuable in disorders in which a particular knockout mouse shows varying phenotypes depending on the genetic background. Knockout null mice have strongly impacted the field of neuroscience and molecular psychiatry and have provided a wealth of data on the role of particular genes in vivo. However, as with all techniques there are limitations. The generation of constitutive knockout mice is a timely and costly endeavor. The deletion of a gene crucial for survival can result in early death and preclude characterization of the gene loss. Constitutive null mice may have a functional redundancy to the gene of interest, resulting in genetic compensation that masks potential phenotypes from being revealed. The use of constitutive knockout mice also precludes clear interpretations regarding a regional and temporal role for the gene of study.
CONDITIONAL TA R G ET I N G S T R AT E G I E S Conditional genetic approaches involve the targeting of recombination events in a spatial and temporal dependent manner. Site-specific recombinases are enzymes that catalyze recombination events between specific DNA sites. The Cre/ loxP system is widely used and involves Cre recombinase creating recombination between locus of recombination (loxP) sequences which can delete or activate a gene of interest. The FLP/FRT system is similar to the Cre/loxP system, but has not been as widely utilized in mammals and involves the FLP recombinase creating recombination between FLP recombinase target (FRT) sequences. The Cre/loxP system results in recombination occurring only in those tissues that express Cre recombinase. Typically, the Cre/loxP system is used by crossing a Cre mouse, which contains the Cre recombinase under the control of the particular promoter, with a floxed mouse which contains loxP sites flanking a particular exon (or exons) of a gene of interest. The resulting conditional knockouts are mice in which the deletion of the gene of interest only occurs in a particular tissue. Recombinase events do not normally occur in the mammalian genome, thus the targeting approach should be specific. The Cre mouse should have wild-type levels of the gene of interest, since there are no loxP sites present, and only express Cre recombinase under the direct control of a particular promoter that can be turned on in a tissue-specific, development- specific, or an inducible-specific manner with compounds such as doxycycline and tamoxifen. The floxed mice are initially generated by targeting loxP sites to a particular target region of DNA in ES cells, such that it does not interfere with the endogenous gene of interest, then screening the ES cells for the floxed gene in a manner similar to that used to generate conventional knockouts. The location and orientation of the loxP sites can result in deletion, translocations, or inversion of the gene of interest once Cre recombinase is expressed. The generation of conditional knockout mice has proven important in the study of genes that, when deleted by constitutive knockouts approaches, result in early death. The use of conditional knockout animals has also allowed the investigation of the role of genes in a particular brain region or type of cell. The ability to target a knockout to a particular brain region in delineating the role of a particular protein may contribute to our understanding of specific mechanisms that underlie psychiatric disorders. While conditional targeting approaches, particularly conditional knockouts, have greatly advanced our understanding of the role of particular genes in brain function, the generation of these mice can be time consuming and costly. N O VE L G E N E E D I T I N G TO O L S Traditionally, genetic editing was achieved through homologous recombination in ES cells, which is a time consuming and costly screening and breeding process to obtain genetically modified animals; plus, it does not apply to animal species with no available ES cells. In recent years, multiple novel
44 •S. E merging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford University Press USA - OSO, T 2018. 07:33:44.
genetic editing tools have been developed that have massively increased the efficiency and speed of introducing genetic modifications. These new developments include the engineering of site-specific DNA nucleases including zinc finger nucleases (ZFNs), transcription activator–like effector nucleases (TALENs), and RNA-g uided DNA endonucleases such as clustered regulatory interspaced short palindromic repeat (CRISPR-Cas) systems (Gaj et al., 2013). The key features of these tools lie in their efficiency in recognizing specific sequences in the genome and making precise double strand breaks (DSB) at the site. The DSBs can trigger two types of cellular DNA repair mechanisms: the error-prone nonhomologous end joining (NHEJ), or homology-directed repair (HDR). NHEJ may introduce deletions or insertions of various lengths and lead to knockout of a targeted gene, while HDR occurs in the presence of a template for repairing and produces accurate genetic modifications of the target locus.
These site-specific nucleases, especially Crispr-Cas9 systems, have demonstrated multiple advantages and have been widely adopted by researchers. First, they bypass the need for generating germ line mutations to make direct genetic editing. Cas9 has been successfully applied to knockout gene expression in adult brains and in cultured brain slices (Swiech et al., 2015). Second, they do not depend on the availability of ES cells, and thus enable across-species gene editing. This is especially important for research involving species such as fish and primates, which were traditionally difficult for targeting genetic manipulations. For instance, TALEN has been used to generate a primate model for the neurological disorder, Rett syndrome, by targeting the gene methyl CpG binding protein 2 (MeCP2) into the genome (Liu et al., 2014). Third, multiplex gene targeting becomes easy. Conceptually, ZFN, TALEN, and CRISPR-Cas systems can be used to target multiple genes simultaneously. In practice, the CRISPR-Cas system provides the greatest convenience in multiplex targeting, which can be achieved by simply adding multiple sgRNAs. In fact, large- Z F N S A N D TA L E N S scale sgRNA libraries have been generated and used to screen ZFN and TALEN recognize DNA sequences through specific for genes critical for certain functions (Zhou et al., 2014). The site-specific DNA nucleases, especially CRISPR-Cas9 protein-DNA binding. Both of them are composed of a customizable DNA binding module which can be programmed systems, also demonstrate high efficiency in gene editing. to bind to specific genomic sequences, and an effector DNA When plasmids carrying Cas9 and a sgRNA were electronuclease domain which introduces DSB. The DNA binding porated into neurons in culture brain slices, nearly all neumodule of ZNF is composed of zinc finger domains (Urnov rons transfected showed disruption of the targeted genes). et al., 2010). Each zinc finger is made up of ~30 amino acids Similarly, when Cas9 and sgRNA were introduced into neuand recognizes 3-base pairs in the major groove of DNA. The rons in the brain with adeno-associated virus (AAV) it was zinc fingers can be selected from existing libraries or made found that around 70% of the neurons showed knockout of through a rational design. Normally more than three zinc fin- the targeted gene (Incontro et al., 2014). Due to their high effigers are joined together by a conserved linker sequence to rec- ciency the Cas system and TALEN can also be recruited to ognize DNA sequences of 9–18 bp in length, which confer the accelerate the generation of genetically modified animals. In specificity of ZFN in genomic targeting. The DNA binding this situation gene editing can be conducted at the single-cell module of TALEN is made up of a series of repeat domains of embryo stage, thus eliminating the time-consuming screening 33–35 amino acids which recognize single base pairs ( Joung of ES cells and the subsequent animal breeding. Among these gene editing tools, the CRISPR-Cas sysand Sander, 2013). Compared to ZFN, TALEN does not require reengineering the linker region and can construct tem appears to be superior in many aspects including ease in larger arrays of the repeats to target longer DNA sequences, custom design, high efficacy, minimal off-targeting, and convenience in multiplex targeting. Working as one-component leading to high targeting accuracy. systems, ZFN or TALEN can be a good choice when codelivery of sgRNA is not ideal. Compared to ZFN, TALEN C R I S P R/C A S S Y S T E M appears to be easier in design, able to target longer sequences, Unlike ZFNs and TALENs, Cas proteins mediate RNA- and therefore reducing the possibility of off-targeting. Although the current major applications of the ZFN, guided recognition of specific DNA sequences. The CRISPR/ Cas systems originate in the bacterial mediators for acquired TALE, and Cas proteins have been to direct nucleases to a immunity against foreign DNA (Doudna and Charpentier, desired locus and introduce DSB, it needs to be noted that the 2014; Heidenreich and Zhang, 2016). In bacteria, invaded zinc fingers, TALE, and enzymatically inactive Cas9 (dCas9) foreign DNA is integrated within the CRISPR genomic loci can target other genetic effectors to a specific locus. For examand transcribed into short CRISPR RNA (crRNA). The ple, dCas9 has been fused to a transactivator or repressor to crRNAs anneal to transactivating crRNAs (tracrRNAs) and achieve activation or inhibition of targeted genes (Gilbert direct sequence-specific DNA cleavage. In the engineered et al., 2013). two-component CRISPR/Cas systems, crRNA is fused to tracrRNA to form a single-g uide RNA (sgRNA) to carry the VI R A L VE C TO R S A N D specific targeting sequence. When the Cas protein is introM O L E C U L A R TO O L S duced into mammalian cells together with sgRNAs, it makes DSB at the locus containing the sequences matching that of the sgRNAs. In addition to Cas proteins, a single RNA-g uided Viruses are tiny organisms on the nanometer scale. Neurotropic viruses have long been used as tools in neuroscience research, nuclease, Cpf1, is also employed for gene editing. 4 . MS.ethods n Vivo G ene M anipulation Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al.,for OxfordI University Press USA - OSO, 2018. 07:33:44.
and in the early days they were predominantly exploited to trace neuronal pathways in the brain (Martin and Dolivo, 1983). A few types of virus, including pseudorabies virus (PRV), rabies virus, and herpes simplex viruses (HSVs), contain desirable characteristics that render them amenable to circuit tracing. In recent years, multiple types of virus have been genetically engineered, leading to more efficient, versatile, and safer tools for both dissecting and manipulating the brain circuits. In addition to their use in scientific research, some of the vectors have demonstrated potential in clinical applications. The primary use of modern viral vectors in neurobiology is to deliver genetic materials to specific brain regions or specific types of cells in the brain. The genetic materials can be used to either express exogenous genes, including various molecular tools, or to regulate the expression of endogenous genes. The effects of the viral vectors on brain functions depend on several factors including the biological properties of the specific types of vector, the genetic cargo the vectors carry, and the way the vectors are introduced into the brain. Here we will first discuss the biological properties of the commonly used viral vectors and then go over the genetic components of viral vectors, and what the virus vectors and the molecular tools they carry can do for neurobiological research. C O M M O N LY US E D VI R A L VE C TO R S
Multiple viral vectors have been engineered and adapted for neuroscience research, including but not limited to AAVs, adenovirus, retrovirus, lentivirus, pseudorabies virus, rabies virus, and herpes simplex virus. Each type of virus has its own advantages and limitations. Here we will focus on a few of the most commonly used vectors.
Adeno-Associated Virus AAVs are non-enveloped viruses with a small size of ~20 nm in diameter. They are single-stranded DNA viruses. The AAV genome contains two inverted terminal repeats (ITRs) that are the only sequences required in cis for viral replication and packaging. The replication of AAV depends on the presence of adenovirus as the helper virus; however, a helper virus–free packaging system has been developed and is now widely used. In human cells, AAV can integrate at a specific site at chromosome 19. But most of the viral genomes exist as episomes in infected cells and mediate long-term gene expression (Deyle and Russell, 2009). The virus is not known to cause human diseases and is classified as a biosafety level 1 material. AAVs have multiple desirable properties for neuroscience research. First, AAV can diffuse to large areas in the brain. High-titer AAV introduced by a single local injection can diffuse and infect neurons spanning an area of around 4 cm2 or even more (Xu et al., 2012; Xu and Sudhof, 2013; Liang et al., 2015). This makes AAV an ideal vector for targeting large brain regions. Second, AAVs have a high infection rate. In the majority of targeted brain regions (with a few exceptions, such as the cerebellum granule cells) stereotactic injection of some serotypes of AAVs can produce an infection rate of close to 100% at the injection sites and adjacent regions. Third, AAV infections can
mediate stable, high-level, and long-term transgene expression. Finally, the virus itself demonstrates minimal cell toxicity even at high titers. AAVs come in various serotypes with distinct biological properties, including substantial differences in their cellular and subcellular tropism. For example, when injected into the hippocampus AAV2 preferentially infects the neurons in the hilar region in the dentate gyrus, while AAV-DJ produces broad infection (Xu et al., 2012; Burger et al., 2004). Some AAV serotypes show preferential uptake by axonal terminals, thus mediating retrograde labeling of neurons projecting to the injection site. AAV1, AAV5, and AAV9 are known to demonstrate pronounced retrograde transport (Burger et al., 2004; Cook-Snyder et al., 2015). Certain types of AAV— AAV9 for example—can pass the blood–brain barrier when systemically administered. AAV9 was found to produce neuronal infection in neonatal animals when injected into tail veins. In adult mice, the same procedure appears to produce infection of mainly glial cells (Foust et al., 2009). One significant limitation of AAV is the strict limit of its packaging capacity. Usually the virus DNA cannot exceed 4.8–5.0 kb in size (Dong et al., 1996). Although in certain reports infectious AAV was packaged with plasmids carrying a viral genome of over 8 kb, others demonstrated that in such situations the viral DNA was actually truncated to no more than 5.2 kb (Wu et al., 2010). The size limit makes it difficult to express large genes or to express multiple genes in the same viral vectors. A few strategies have been employed to increase this size limit, but the efficiency of these systems remains to be further evaluated (Yan et al., 2000).
Lentivirus Lentivirus is a single-stranded positive-sense RNA virus with a genome size of about 10 kb. The virions are enveloped and measure 80–100 nm in diameter. Commonly used lentiviral vectors are the replication-deficient vectors derived from human immunodeficiency virus (HIV) (Matrai et al., 2010). As a special type of retrovirus, lentivirus can transfer genes into both dividing and nondividing cells including neurons, and integrates into the genome of infected cells to mediate stable and heritable gene expression (Parr-Brownlie et al., 2015). Lentivirus usually spreads to a limited area after being injected into the brain. A local injection with high-titer lentivirus in the rodent cortex can infect neurons spanning an area of 500–800 µm. Therefore, compared to AAV, lentivirus is preferred when accurate targeting of a small area is required. The infection rate of lentivirus varies significantly among brain regions. It has a high infection rate in brain regions such as the striatum, the thalamus, and the brain stem structures, while the infection rate drops in regions where neuronal soma are densely packed together, such as the pyramidal layer/granule layer in the hippocampus and the granule cell layer of the cerebellum. The low infection rate becomes a desirable property when infected neurons need to be compared to neighboring noninfected neurons. Cell-specific enhancer/promoters have been successfully used with lentivirus to control gene expression in specific types of neurons. However, due to the random
46 •S. E merging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford University Press USA - OSO, T 2018. 07:33:44.
nature of the integration of lentivirus, cell-specific expression may be influenced by the chromatin environment of the particular integration events. Beside the lentiviral vectors derived from HIV, some lentiviral vectors are derived from other types of lentivirus, such as equine infectious anemia virus (EIAV) and caprine arthritis encephalitis virus (CAEV) (Olsen, 2001). The vectors derived from nonprimate lentiviruses may be even safer for the experimenters. Lentiviral vectors normally do not mediate retrograde gene transfer. However, when pseudotyped with glycoprotein containing the ectodomain of rabies virus, they can be retrogradely transported (Hirano et al., 2013). Engineering the glycoprotein may also enable infection that is specific to certain types of cells (Matrai et al., 2010).
Rabies and Pseudorabies Virus (PRV)s Rabies viruses are enveloped, single-stranded, negative-sense RNA viruses with a genome size of around 12 kb. PRV is a double-stranded DNA virus with a genome around 143 kb. Rabies virus and PRV have been traditionally used for neuronal pathway tracing as they exhibit several features desirable for this purpose (Callaway, 2008; Ekstrand et al., 2008). Rabies and PRVs show a preferential uptake by synaptic terminals with a minimal uptake by passing axons. Rabies and PRVs can self-replicate to generate strong labeling and pass multiple tiers of synaptic connections. PRV can be either retrogradely or anterogradely transported depending on the specific strains of virus, with the molecular determination for the directionality identified (Curanovic and Enquist, 2009). Both rabies and PRV have been subjected to extensive engineering in recent years. A key modification was to abolish their ability of replication or trans-synaptic spread by removing an essential gene from the viral genome. For example, when the glycoprotein of rabies virus is removed from the viral genome but provided in packaging cells, infectious virus can be produced. The virus can enter axonal terminals and thus mediate gene expression in the transduced neurons, but it cannot spread beyond initially infected cells (Wickersham et al., 2007). A similar strategy has been applied to modify PRV by removing the early immediate gene IE180 or thymidine kinase (TK) genes, both essential for PRV replication (Oyibo et al., 2014; Kondoh et al., 2016). These genes meant to control viral replication can then be provided in trans in neurons to allow monosynaptic spreading of the virus. In a widely adopted strategy, the glycoprotein deleted rabies virus is pseudotyped with an avian virus envelope protein (EnvA), which binds to its receptor, TVA. When TVA is coexpressed with rabies virus glycoprotein in specific types of neurons (starter neurons), the pseudotyped rabies virus can infect these neurons. Expression of glycoprotein in the starter neurons allows the virus to spread in a retrograde direction across one synaptic connection, thus revealing the neurons directly connected to the starter cells (Wickersham et al., 2007; Osakada et al., 2011). Pursuing a similar strategy to that used in rabies virus, a method has recently been developed to provide TK gene to PRV in a cell type–specific manner (Kondoh et al., 2016).
Though powerful anatomical tools, recombinant rabies virus, and the replication-capable PRV exhibit high levels of cell toxicity, which has limited their use as tools to manipulate neuronal functions. Recent findings indicate that rabies viral vectors based on a less virulent strain demonstrate less toxicity and may significantly broaden the applications of these vectors (Reardon et al., 2016). In contrast, the replication-deficit PRV, which lacks the gene of IE180, does not show high levels of cell toxicity, albeit the gene expression level mediated by this vector is low (Oyibo et al., 2014).
Other Types of Viral Vectors There are other types of viral vectors with unique properties that satisfy special needs. For example, gene transfer by retrovirus relies on cell cycles and cannot occur in mature neurons. Therefore, retrovirus can be used to monitor adult neurogenesis by selectively labeling the newly generated neurons (van Praag et al., 2002). Canine adenovirus serotypes 2 (CAV-2) demonstrated relatively efficient axonal uptake and retrograde transport with less cell toxicity (compared to rabies virus) ( Junyent and Kremer, 2015). Similar to PRV, herpes simplex virus type 1 (HSV-1) is usually retrogradely transported, however the H129 strain of HSV-1 spreads primarily in anterograde direction making this the choice for targeting neurons with specific input or output patterns (Wojaczynski et al., 2015). C O M MO N G E N ET I C C O M P O N E N T S O F V I R A L V EC TO R S
Viral vectors, like compact nano-machines, can regulate gene expression in the transduced cells with the genetic materials they carry. Despite the diverse types of viral vectors, these genetic materials, used for transcription of mRNAs or small noncoding RNAs, consist of a few common components, each serving different purposes (Fig. 4.1). To mediate high-level expressions of genes, the enhancer- promoters, polyadenylation [poly(A)] signals, and WPRE (abbreviation for woodchuck hepatitis virus posttranscriptional regulatory element) are the critical components. Many different types of promoters and enhancers have been used to express proteins. The cytomegalovirus (CMV) early enhancer/ chicken beta actin (CAG) promoter and human ubiquitin c (Ubc) promoter mediate high levels of gene transcription in most cell types. Some promoters mediate selective expression in specific cell types, such as the synapsin promoter in neurons or glial fibrillary acidic protein promoter in astroglial cells. The calcium/calmodulin-dependent protein kinase II (CaMK2) promoter is preferentially active in excitatory neurons, while the somatostatin promoter is preferentially active in inhibitory interneurons (Nathanson et al., 2009). However, depending on the types of viral vector, the chromatin environment of the same promoters may exhibit different behavior. For example, in AAV vectors cell type–specific promoters may lose their selectivity due to the partial enhancer activity of the viral ITRs. A frequently encountered scenario of virus- mediated expression is the massive overexpression when strong
4 . MS.ethods n Vivo G ene M anipulation Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al.,for OxfordI University Press USA - OSO, 2018. 07:33:44.
promoter AAV
ITR
ORF1
IRES
ORF2
WPRE
Poly A
ITR
promoter Lentivirus
Rabies virus (G-deleted)
HIV-1 Y
LTR
N
cPPT/CTS
P
ORF
M
ORF1
Transcription start
WPRE
ORF2
LTR
L
Transcription stop
Figure 4.1 Genetic organization of commonly used viral vectors. Recombinant AAV vectors are flanked by two inverted terminal repeats (ITRs), which are the only sequences required in cis for viral replication and packaging. The other genetic components, including promoter, poly (A) signal, and Woodchuck Hepatitis Virus Posttranscriptional Regulatory Element (WPRE), can be selected and arranged to achieve desired expression level of the genes encoded by the open reading frames (ORFs). Internal ribosome entry site (IRES) can be used to mediate bicistronic expression. Recombinant lentiviral vectors contain a few genetic elements required for viral replication and packaging, including long terminal repeats (LTRs), packaging signal (Ψ), Rev response element (RRE), and central polypurine tract/central termination sequence (cPPT/CTS). They follow similar rules for the arrangement of promoters and other genetic elements except that poly (A) signals are avoided. The recombinant rabies viral vectors contain the majority of the viral genome including the coding and regulatory sequences for genes N, P, M, and L. Gene G encoding the glycoprotein is deleted, and one or two exogenous genes can be placed in its locus. [Revised from Osakada et al., 2011].
promoters are used. Overload of a protein in cells may alter its targeting, functions, and even produce toxic aggregations. To keep protein expression levels in check, a negative feedback can be set up between the gene product and its own enhancer/ promoter. In a smart design, this was realized by fusing a target protein to a transcription regulatory tag, which bound to the promoter/enhancer region of that particular gene and negatively regulated the transcription (Gross et al., 2013). Protein expression levels are impacted by the stability of mRNAs, which are significantly influenced by the presence of poly (A) signals. The most widely used poly (A) signals include human growth hormone (hGH) poly (A) and simian virus 40 (SV40) poly (A) signals. Different poly (A) signals differ in their lengths and efficacy. In addition to the regulation of transcription and mRNA stability, protein translation is another regulatory step. WPRE was shown to increase the translation of mRNAs (Zufferey et al., 1999). This is especially valuable to some RNA viruses, such as lentiviral or retroviral vectors, where the presence of poly (A) signal will impair the packaging of viruses. A few genetic components can temporally and/or spatially control the expression of genes. DNA recombinases and their recognition sequences, such as Cre/loxP or FLP/FRT, and transactivators like the tetracycline-on or tetracycline- off systems, respectively, are commonly used for this purpose. FLEX switches composed of two pairs of loxP or FRT sites are commonly used for conditional gene expression (Schnutgen et al., 2003). In addition to controlling at the transcription level, some protein tags can be used to regulate protein level by controlling degradation. FKBP12 and ecDHFR are such
tags, which mediate degradation of a protein in the absence of a drug, Shield-1, or trimethoprim (TMP) (Iwamoto et al., 2010). Since TMP is an antibiotic with efficient penetration of the blood–brain barrier, this is an attractive method for use in vivo. When viral vectors are used to express more than one gene in the same cells, an internal ribosome entry site (IRES) or 2A sequences are frequently employed to link the coding sequences of two proteins together in one transcript. IRES mediates ribosome reentry following the completion of the translation of the gene upstream to it. When IRES is used, both genes have their own start and stop codons; but the downstream gene needs to be in frame with the start codon (ATG) at the c-terminus of IRES. Obviously, a key advantage of the IRES system is that it mediates bicistronic expression with minimal or no impact on the protein coding sequences. However, the IRES system is not without its caveats, including the production of unequal protein expression levels. The expression of the two coding sequences may not be equal, and the expression of the downstream gene may vary from construct to construct, with expression of the downstream gene frequently insufficient. The 2A self-cleaving peptide (2A) system is another tool to express two genes within one transcript, and it exhibits complementary advantages and disadvantages to IRES. 2A is a short peptide sequence of 19–22 amino acids mediating ribosome skipping, in which a glycyl-prolyl peptide bond is skipped between the last two amino acids of 2A peptides. A major advantage of the 2A system is that the two genes have equal molar expression. A major shortcoming of 2A system lies in the fact that 18 or more amino acids will be added to the carboxyl terminus of
48 •S. E merging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford University Press USA - OSO, T 2018. 07:33:44.
the upstream gene, and another one amino acid, normally proline, is placed at the amino-terminus of the downstream gene. Another potential caveat of the 2A system is that the ribosome skipping is not 100% efficient, resulting in some fusion protein of the two genes expressed, which may significantly alter the function of the genes. A few 2A sequences have been identified, of which P2A, T2A, and F2A are most commonly used and show different levels of efficiency in producing two separate proteins (Kim et al., 2011). A P P L I C AT I O N S O F VI R A L VEC TO R S
The application of viral vectors in neurobiology can be largely divided into the following three categories: introducing into neurons exogenous genes, especially molecular tools for visualizing, tracing, or manipulating brain circuits; regulating the expression of endogenous genes; and selective targeting of specific brain regions or cell types. The combinatorial usage further increases the versatility of viral vectors.
1) Expression of exogenous genes. Viral vectors can carry essentially any exogenous genes into transduced cells. An exciting advance in current neuroscience research is the invention of molecular tools to enable one to delineate, monitor, and functionally manipulate the brain circuits. The majority of these tools rely on viral vectors for delivery into the brain. The genetically encoded tools for delineating brain circuit: The brain is a complex structure made up of numerous types of neurons connected together. Various genetically encoded markers, including fluorescent proteins, affinity tags, and enzymes have been developed and incorporated into viral vectors, which enable both microscopic and macroscopic dissection of the brain circuits. Expression of these markers can be conditional or inducible to label specific types of neurons. Methods have also been devised to express different tags in neighboring neurons so that each of the neurons can be distinguished from each other. One sophisticatedly designed tool is the “brainbow vectors,” which use genetic tricks to mediate the expression of different combinations of fluorescent proteins upon recombination of the vectors (Cai et al., 2013). The diffusible fluorescent proteins or affinity tags normally fill the whole neurons and reveal the structure of the cells, including dendritic spines and axonal velocities. Recently, genetically encoded peroxidase derivatives were optimized to label genetically identifiable neurons for electron microscope imaging such that serial ultrathin sectioning can be collected to reconstruct the detailed morphological features of neurons ( Joesch et al., 2016). Viral vectors carrying specific markers can be targeted to selected cell compartments, such as the dendrites, axons, cellular organelles, or synapses. Fluorescent
proteins fused to synaptic vesicle proteins such as synaptobrevin and synatophysin are commonly used to label presynaptic terminals, while those fused to PSD95 or gephyrin can label excitatory or inhibitory postsynaptic compartments, respectively. Since overexpression of synaptic proteins may lead to unexpected functional consequences, recombinant antibody-like proteins recognizing PSD95 or gephyrin were identified and fused with fluorescent proteins for synaptic labeling. Viral vectors carrying these synaptic markers successfully tagged the excitatory or inhibitory synapses selectively without apparent alteration of synaptic functions (Gross et al., 2013). Neurons are highly polarized cells. To reveal a complete picture of their distinct compartments, different markers can be combined to demonstrate the various aspects of neuronal morphological properties at the same time. SynaptoTAG AAV is designed such that the infected neurons express diffusible red florescent mCherry and EGFP fused to the synaptic protein synaptobrevin. The mCherry fills the whole cell, labeling the soma, dendrites, and axonal projections, while EGFP selectively targets synaptic terminals and exposes the synaptic connectivity of the infected neurons (Xu and Sudhof, 2013). A similar approach has been taken with recombinant rabies virus, in which two fluorescent proteins were expressed to generate strong labeling of different neuronal compartments (Wickersham et al., 2013). In the brain, synapses may form selectively between specific types of neurons. Tools have been developed to tag synapses between two selected groups of neurons. One of these approaches takes advantage of a split fluorescent proteins system. The two domains of EGFP, N-GFP, and C-GFP are fused to presynaptic- or postsynaptic-targeting proteins, respectively. The reconstitution of EGFP inside the synaptic clefts reports the formation of synapses between the two chosen groups of neurons (Kim et al., 2012). Another attractive design has been put forward to utilize the trans-synaptic activation of gene expression to reveal the functional connectivity. This so-called Tango-trace system takes advantage of the transmembrane signal transduction mechanisms involving proteolytic release of a transactivator from a membrane anchor ( Jagadish et al., 2014). A major advantage of this system is that it not only reveals the connectivity between neurons but also holds the potential for functional manipulations of the postsynaptic neurons. The genetically encoded indicators of neuronal activity: The molecular tools carried by viral vectors can reveal the structural organization of the brain as well as the real-time actions in the neuronal network. Neuronal or synaptic activities can be visualized by tools that have been developed, or are actively being developed, including genetically encoded indicators
4 . MS.ethods n Vivo G ene M anipulation Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al.,for OxfordI University Press USA - OSO, 2018. 07:33:44.
for calcium transients, membrane voltage, release of neurotransmitters, or activation of specific signal transduction pathways. The transient elevation of cytosolic free calcium caused by either calcium influx through membrane channels or release from internal stores is a critical intracellular signaling mechanism. Previously, synthetic fluorescent dyes were the major probes to visualize calcium transients. Fluorescent proteins which detect calcium via an increase in fluorescence upon the binding of calcium have been used for a long time but are crippled with low sensitivity. In recent years, the invention and improvement of the GCaMP family of indicators have revolutionized calcium imaging (Nakai et al., 2001). GCaMP6, including several variants, exhibits similar or even superior sensitivity and signal strength to synthetic dyes. The GCamP6 variants, GCamP6f, 6m, and 6s, have different sensitivity, kinetics, and signal strength in response to calcium. Selection among these variants depends on specific experimental emphasis, in particular the kinetics or sensitivity. Viral vectors enabling expression of these indicators in selected brain regions or types of neurons have found broad applications in various in vitro and in vivo imaging experiments and have facilitated the imaging of neuronal activity in behaving animals, both head-fixed and free- moving (Chen et al., 2013). The viral vectors carrying GCaMP6 fused to synaptic proteins have also used to selectively image calcium activity in the presynaptic terminals or postsynaptic sites. Recently, a series of red fluorescent calcium indicators have been generated with sensitivity comparable to GCaMP6 (Dana et al., 2016). A photoswitch version of genetically encoded calcium indicator was developed that switches its fluorescence from green to red at the moment cytosolic free calcium concentration is high. This photoswitch version makes it an indicator to report the neuronal activity of both a past time point (the moment of the photoswitch) and the current moment (Fosque et al., 2015). A limitation of calcium imaging is the relative slow kinetics compared to fast neuronal events such as action potentials. To achieve high temporal resolution for detection of fast neuronal activity, including individual action potentials, it has become a focus of bioengineering research to develop sensitive genetically encoded voltage sensors. A few different designs have been presented and tested (St-Pierre et al., 2015). AAV vectors carrying some of these voltage indicators were used for imaging action potentials in the brain (Gong et al., 2015). However, since the duration of an action potential is just 1–2 ms, reliable detection of the signal from voltage indicators will require highly sensitive and high-speed cameras, which currently make it difficult to image the action potentials in free-moving animals.
Besides observing neuronal firing–related activities, membrane voltage, and calcium transients, additional genetically encoded sensors have been developed to detect other aspects of neuronal functions. For example, the sensor for neurotransmitter glutamate was shown to detect synaptically released glutamate (Marvin et al., 2013). Specific sensors for the activation of secondary signal transduction in the brain have also been invented. Genetically encoded regulators of neuronal activity: In addition to visualizing the biological events in the brain, multiple approaches have been developed to control neuronal, synaptic, or molecular functions. Among the recent advances, optogenetic tools have been broadly adopted for high temporal precision in controlling neuronal activity. Besides optogenetics, multiple molecular tools have emerged which can regulate neuronal excitability. In early attempts, the potassium channel KV1.2 was overexpressed in neurons to silence them. Recently, pharmacogenetic tools have appeared with which neuronal excitability or other activities can be increased or reduced upon the application of certain chemicals. With these methods, the neuronal excitability can be selectively manipulated in a desired time window. For example, an inhibitory glutamate receptor originating from C. elegans, GluClαβ, was expressed with viral vectors in the mammalian brain (Lerchner et al., 2007). Administration of the ligand ivermectin activates this chloride channel and leads to selective silencing of the neurons expressing this protein. In a similar strategy a peptide ligand, allatostatin, was used to gate an inhibitory G-protein- coupled receptor, AlstR originating from flies, to silence mammalian neurons (Lechner et al., 2002). In a more sophisticated design, chemistry and protein engineering were combined to generate a series of tools which either inhibit or excite neurons when certain chemicals are applied (Magnus et al., 2011). Among these chemogenetic tools regulating neuronal excitability, the Designer Receptors Exclusively Activated by Designer Drugs (DREADD) system has gained popularity for its effectiveness, versatility, and convenience (Roth, 2016). DREADD systems are made from engineered G-protein coupled receptors (GPCRs). The ligand, clozapine-N-oxide, acts on the engineered GPCRs, which are coupled to either excitatory (Gs) or inhibitory (Gi) signaling pathways and lead to the excitation or inhibition of neurons, respectively. Besides directly controlling neuronal excitability, the DREADD system utilizing Gq pathway can be used to alter the cAMP level in cells. In addition to regulating function at a neuronal level, genetically encoded tools have been invented to control synaptic activity with the application of optical or chemical stimulations. One example is
50 •S. E merging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford University Press USA - OSO, T 2018. 07:33:44.
miniSOG, a singlet oxygen generator, fused to proteins that are localized to synaptic vesicles. Upon optical stimulation, miniSOG generates reactive oxygen species that disrupt the proteins fused to miniSOG and shut down synaptic release of transmitters (Lin et al., 2013). In addition to optical and chemical approaches to control brain functions, magnetic force has been adapted to achieve wireless control of neuronal activity in the brain. This has been realized through various different ways including making a single-component magnetic sensor by coupling paramagnetic ferritin protein to TRPV4, a nonselective cation channel sensitive to mechanical stress and temperature. The magnetic torque generated by ferritin opens TRPV4 and activates the neurons. This magnetic sensor, when transduced into neurons by AAV vectors, was shown to be effective in stimulating neurons in behaving animals upon the application of a static magnetic field (Wheeler et al., 2016).
2) Regulating expression of endogenous genes: Viral vectors can be used to either increase or decrease the expression of endogenous genes. Increasing gene expression levels can be achieved by introducing the cells with extra copies of the coding sequences with viral vectors. By selecting proper genetic components for the viral vectors, such as promoters and poly (A) signal as mentioned, the level of expression can be fine-tuned. Expression of endogenous genes can also be increased by enhancing the transcription or translation. For example, catalytically inactive CRISPR-associated nuclease-9 (dCas9) fused to a transactivator can recognize specific loci in the genome and activate the expression of the targeted genes at the presence of guide RNAs (Maeder et al., 2013). Similarly, viral vectors can be used to express regulatory noncoding RNAs to increase the expression of endogenous genes. Viral vectors can also reduce the expression of endogenous genes by targeting the multiple steps from genomic coding, gene transcription, and mRNAs stability to protein turnover. Gene targeting to remove exons or to introduce frame-shifting mutations in the genes can abolish the expression of genes (knockout). The highly efficient CRISPR-Cas system makes it possible to alter the genome of neurons in the brain with viral vectors (Swiech et al., 2015). In addition to disrupting gene sequences, targeted gene silencing can be induced at specific sites in the genome with dCas9 fused to a transcription repressor in the presence of guide RNAs (Gilbert et al., 2013). Selective degradation of the mRNAs is the most common way to reduce gene expression level. RNA
interference (RNAi) is the major approach to produce the degradation of mRNAs. RNAi can be induced by loading the cells with short hairpin RNAs (shRNAs). Two types of designs are frequently adopted in viral vectors to stably produce shRNAs (McManus and Sharp, 2002). One uses Pol III promoters to drive the expression of shRNAs in the cells. The short transcripts of shRNAs will be processed into 19–21 nucleotide double-stranded RNAs to trigger RNA inference. The other one imbeds shRNA sequences in a miRNA transcript. A main advantage of the latter system is that the transcription of miRNA can be driven by a Pol II promoter and placed in the 3’ UTR of a protein transcript. The yield of shRNAs in this system is normally less than that produced by Pol III promoters and thus reduces the possibility of nonspecific stress responses. The efficiency of knockdown by RNAi depends on the sequence incorporated in shRNA and is gene-specific. Although a few algorithms have been developed to identify efficient sequences, knockdown efficiency still needs to be empirically determined. A properly designed shRNA can be used to knockdown multiple members of a gene family by targeting their common mRNA sequences. shRNA can also selectively knockdown one single splicing variant of multiple transcripts from the same gene. The RNAi approach is not limited to knocking down the mRNAs of proteins, but can also knockdown other gene products including various types of regulatory RNAs such as the miRNA and enhancer RNAs. Viral vectors can also be used to carry specific tags to mediate targeted degradation of endogenous protein. A common strategy is to target a protein degradation epitope to selected genes. For example, nanobodies or protein affinity tags can target an E3 ubiquitin ligase or a CMA-targeting motif (CMA: Chaperone- mediated autophagy) to endogenous synaptic proteins and trigger selective degradation of these proteins (Fan et al., 2014; Gross et al., 2016). In addition to simply increasing or decreasing gene expression, viral techniques can be used to modify the gene products themselves, especially proteins. One common approach for this purpose is the molecular replacement method, which is a combination of gene knockdown/knockout with rescuing expression of an altered coding sequence. For example, in a viral vector the H1 promoter is used to express a shRNA sequence to knockdown a gene while the Ubc promoter is used to express the same gene but with an altered coding sequence.
3) Selective targeting of specific brain regions or cell types: One advantage offered by viral vectors in neurobiology is that they can be targeted to specific brain regions or cell types. Brain region specificity can
4. M n Vivo G ene M anipulation Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S.ethods Charney, et al.,for OxfordIUniversity Press USA - OSO, 2018. 07:33:44.
be achieved through targeted delivery of viral vectors into the brain, for example, with stereotaxic injections. Using this approach, the size of the infected brain region will be determined by the type of viral vector, volume of injection, and viral titer.Cell type–specific gene transduction can be achieved through multiple ways. First, different viral vectors show distinct tropisms to certain cell types. The selective tropisms may arise from the innate properties of the virus, like the different
AAV serotypes which preferentially transduce certain neuronal types (Xu et al., 2012 ; Burger et al., 2004), or from intentional engineering, like the glycoprotein of lentiviral vectors which are modified to selectively bind to certain cell surface markers specific to certain types of cells (Buchholz et al., 2015). Second, cell type–specific enhancer-promoters can be incorporated in viral vectors to drive cell type–specific gene expression as discussed. Similarly, gene expression mediated by viral vectors can
Tracing and selective targeting of brain circuits with viral vectors. (A) Tracing synaptic outputs from CA3 region of the hippocampus. SynaptoTag AAV, which encodes a diffusible red fluorescent protein mCherry to reveal neuronal cell bodies and axons and green fluorescent protein EGFP fused to synaptobrevin to mark synaptic terminals (Liang et al., 2015), was injected ipsilaterally into the CA3 region (the inset is the enlargement of CA3 region; the arrow points to pyramidal cell layer). The red fluorescence indicates the infected neurons at CA3 pyramidal cell layer and their axonal fibers in the hippocampus and fimbria. The green fluorescence shows the synaptic terminals distributed in the hippocampus and septum which originate from CA3 neurons. (B) Selective targeting neurons based on their connectivity. Replication-deficient pseudorabies encoding Cre recombinase (PRV-Cre, Oyibo et al., 2014) were injected into the lateral septum of a reporter mouse, which expresses red fluorescent protein tdTomato in cells expressing Cre. PRV-Cre was uptaken by axonal terminals in septum and retrogradely transported to CA3 and turned on the expression of tdTomato in CA3 neurons (the inserts shows the tdTomato-positive neurons at CA3 pyramidal cell layer as indicated by the arrow. The red fluorescence in the other layers in the hippocampus indicates the distribution of the axons originate from the tdTomato-expressing neurons. Figure 4.2
52 •S. E merging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford University Press USA - OSO,T 2018. 07:33:44.
be conditionally turned on or off in the presence of DNA recombinase or transactivators. When conditional viral vectors are applied to animals that express DNA recombinase or transactivators in specific types of cells, cell type–specific gene expression can be activated. A huge collection of driver mouse lines is available for researchers. Stereotaxic injection of conditional viral vectors into the brains of driver mouse lines is currently the major approach to manipulate brain circuits in a region-specific and cell type–specific manner. Third, viral vectors that are retrogradely or anterogradely transported in the neural circuit, such as PRV, rabies virus, or CAV2, can be used to selectively target neurons with specific inputs or outputs (Figure 4.2). Furthermore, all above approaches can be combined to achieve high-level specificity.
Fan, X., Jin, W.Y., et al. (2014). Rapid and reversible knockdown of endogenous proteins by peptide-directed lysosomal degradation. Nat Neurosci 17(3):471–480. Fosque, B.F., Sun, Y., et al. (2015). Neural circuits. Labeling of active neural circuits in vivo with designed calcium integrators. Science 347(6223):755–760. Foust, K.D., Nurre, E., et al. (2009). Intravascular AAV9 preferentially targets neonatal neurons and adult astrocytes. Nat Biotechnol 27(1):59–65. Gaj, T., Gersbach, C.A., and Barbas, C.F., 3rd. (2013). ZFN, TALEN, and CRISPR/Cas-based methods for genome engineering. Trends Biotechnol 31(7):397–405. Gibbs, R.A., Weinstock, G.M., et al. (2004). Genome sequence of the Brown Norway rat yields insights into mammalian evolution. Nature 428(6982):493–521. Gilbert, L.A., Larson, M.H., et al. (2013). CRISPR-mediated modular RNA- g uided regulation of transcription in eukaryotes Cell 154(2):442–451. Gong, Y., Huang, C., et al. (2015). High-speed recording of neural spikes in awake mice and flies with a fluorescent voltage sensor. Science 350(6266):1361–1366. Gross, G.G., Junge, J.A., et al. (2013). Recombinant probes for visualIn summary, modern neurobiology has made great strides in izing endogenous synaptic proteins in living neurons. Neuron 78(6): technological and methodological approaches in the last two 971–985. decades to manipulate gene expression in vivo. The advances in Gross, G.G., Straub, C., et al. (2016). An E3-ligase-based method for ablating inhibitory synapses. Nat Methods 13(8):673–678. mouse genetics, combined with the technological progress in viral manipulation in particular, have enabled a better under- Heidenreich, M., and Zhang, F. (2016). Applications of CRISPR-Cas systems in neuroscience. Nat Rev Neurosci 17(1):36–44. standing of the role of specific genes in brain and the impact Heintz, N. (2004). Gene expression nervous system atlas (GENSAT). Nat of these genes on cell function, neural circuits, and ultimately Neurosci 7(5):483. behavior, as we seek a better understanding of the neurobio- Hirano, M., Kato, S., et al. (2013). Highly efficient retrograde gene transfer into motor neurons by a lentiviral vector pseudotyped with fusion logical basis of psychiatric disorders and ultimately treatments. glycoprotein. PloS One 8(9):e75896. Incontro, S., Asensio, C.S., et al. (2014). Efficient, complete deletion of synaptic proteins using CRISPR. Neuron 83(5):1051–1057. Iwamoto, M., Bjorklund, T., et al. (2010). A general chemical method to REFERENCES regulate protein stability in the mammalian central nervous system. Chem Biol 17(9):981–988. Buchholz, C.J., Friedel, T., and Buning, H. (2015). Surface-engineered Jagadish, S., Barnea, G., et al. (2014). Identifying functional connections of the inner photoreceptors in Drosophila using Tango-Trace. Neuron viral vectors for selective and cell type-specific gene delivery. Trends 83(3):630–644. Biotechnol 33(12):777–790. Burger, C., Gorbatyuk, O.S., et al. (2004). Recombinant AAV viral vectors Joesch, M., Mankus, D., et al. (2016). Reconstruction of genetically identified neurons imaged by serial-section electron microscopy. Elife;5. pseudotyped with viral capsids from serotypes 1, 2, and 5 display differential efficiency and cell tropism after delivery to different regions of Joung, J.K., and Sander, J.D. (2013). TALENs: a widely applicable technology for targeted genome editing Nat Rev Mol Cell Biol 14(1):49–55. the central nervous system. Mol Ther 10(2):302–317. Cai, D., Cohen, K.B., et al. (2013). Improved tools for the Brainbow tool- Junyent, F., and Kremer, E.J. (2015). CAV-2—why a canine virus is a neurobiologist’s best friend. Curr Opin Pharmacol 24:86–93. box. Nat Methods 10(6):540–547. Callaway, E.M. Transneuronal circuit tracing with neurotropic viruses. Kim, J., Zhao, T., et al. (2012). mGRASP enables mapping mammalian synaptic connectivity with light microscopy. Nat Methods 9(1):96–102. 2008 Curr Opin Neurobiol 18(6):617–623. Chen, T.W., Wardill, T.J., et al. (2013). Ultrasensitive fluorescent proteins Kim, J.H., Lee, S.R., et al. (2011). High cleavage efficiency of a 2A peptide derived from porcine teschovirus-1 in human cell lines, zebrafish and for imaging neuronal activity. Nature 499(7458):295–300. mice. PloS One 6(4):e18556. Cook-Snyder, D.R., Jones, A., and Reijmers, L.G. 2015 A retrograde adeno-associated virus for collecting ribosome-bound mRNA from Kondoh, K., Lu, Z., et al. (2016). A specific area of olfactory cortex involved in stress hormone responses to predator odours. Nature anatomically defined projection neurons. Front Mol Neurosci 8:56. 532(7597):103–106. Curanovic, D., and Enquist, L. (2009). Directional transneuronal spread Lechner, H.A., Lein, E.S., and Callaway, E.M. (2002). A genetic method of alpha-herpesvirus infection. Future Virol 4(6):591. for selective and quickly reversible silencing of mammalian neurons. J Dana, H., Mohar, B., et al. (2016). Sensitive red protein calcium indicators Neurosci 22(13):5287–5290. for imaging neural activity. Elife;5. Deyle, D.R., and Russell, D.W. (2009). Adeno-associated virus vector Lerchner, W., Xiao, C., et al. (2007). Reversible silencing of neuronal excitability in behaving mice by a genetically targeted, ivermectin- integration. Curr Opin Mol Ther 11(4):442–447. gated Cl-channel. Neuron 54(1):35–49. Dong, J.Y., Fan, P.D., and Frizzell, R.A. 1996 Quantitative analysis of the packaging capacity of recombinant adeno-associated virus. Hum Gene Li, P., Tong, C., et al. (2008). Germline competent embryonic stem cells derived from rat blastocysts. Cell 135(7):1299–1310. Ther 10;7(17):2101–2112. Doudna, J.A., and Charpentier E. (2014). Genome editing. The Liang, J., Xu, W., et al. (2015). Conditional neuroligin-2 knockout in adult medial prefrontal cortex links chronic changes in synaptic inhinew frontier of genome engineering with CRISPR-Cas9. Science bition to cognitive impairments. Mol Psychiatry 20(7):850–859. 346(6213):1258096. Ekstrand, M.I., Enquist, L.W., and Pomeranz, L.E. (2008). The alpha- Lin, J.Y., Sann, S.B., et al. (2013). Optogenetic inhibition of synaptic release with chromophore-assisted light inactivation (CALI). Neuron herpesviruses: molecular pathfinders in nervous system circuits. 79(2):241–253. Trends Mol Med 14(3):134–140.
4 . MS.ethods n Vivo G ene M anipulation Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al.,for OxfordI University Press USA - OSO, 2018. 07:33:44.
Liu, H., Chen, Y., et al. (2014). TALEN-mediated gene mutagenesis in rhesus and cynomolgus monkeys. Cell Stem Cell 14(3):323–328. Maeder, M.L., Linder, S.J., et al. (2013). CRISPR RNA-g uided activation of endogenous human genes. Nat Methods 10(10):977–979. Magnus, C.J., Lee, P.H., et al. (2011). Chemical and genetic engineering of selective ion channel- ligand interactions. Science 333(6047):1292–1296. Mansour, S.L., Thomas, K.R., and Capecchi, M.R. (1988). Disruption of the proto-oncogene int-2 in mouse embryo-derived stem cells: a general strategy for targeting mutations to non-selectable genes. Nature 336(6197):348–352. Martin, X., and Dolivo, M. 1983 Neuronal and transneuronal tracing in the trigeminal system of the rat using the herpes virus suis. Brain Res 273(2):253–276. Marvin, J.S., Borghuis, B.G., et al. (2013). An optimized fluorescent probe for visualizing glutamate neurotransmission. Nat Methods 10(2):162–170. Matrai, J., Chuah, M.K., and VandenDriessche, T. (2010). Recent advances in lentiviral vector development and applications. Mol Ther 18(3):477–490. McManus, M.T., and Sharp, P.A. (2002). Gene silencing in mammals by small interfering RNAs. Nat Rev Genet 3(10):737–747. Nakai, J., Ohkura, M., and Imoto, K. (2001). A high signal-to-noise Ca(2+) probe composed of a single green fluorescent protein. Nat Biotechnol 19(2):137–141. Nathanson, J.L., Jappelli, R., et al. (2009). Short promoters in viral vectors drive selective expression in mammalian inhibitory neurons, but do not restrict activity to specific inhibitory cell-types. Front Neural Circuits 3:19. Olsen, J.C. (2001). EIAV, CAEV and other lentivirus vector systems. Somat Cell Mol Genet 26(1-6):131–145. Osakada, F., Mori, T., et al. (2011). New rabies virus variants for monitoring and manipulating activity and gene expression in defined neural circuits. Neuron 71(4):617–631. Oyibo, H.K., Znamenskiy, P., et al. (2014). Long-term Cre-mediated retrograde tagging of neurons using a novel recombinant pseudorabies virus. Front Neuroanat 8:86. Parr-Brownlie, L.C., Bosch-Bouju, C., et al. (2015). Lentiviral vectors as tools to understand central nervous system biology in mammalian model organisms. Front Mol Neurosci 8:14. Reardon, T.R., Murray, A.J., et al. (2016). Rabies virus CVS-N2c(DeltaG) strain enhances retrograde synaptic transfer and neuronal viability. Neuron 89(4):711–724. Roth, B.L. (2016). DREADDs for neuroscientists. Neuron 89(4):683–694.
Schnutgen, F., Doerflinger, N., et al. (2003). A directional strategy for monitoring Cre-mediated recombination at the cellular level in the mouse. Nat Biotechnol 21(5):562–565. St-Pierre, F., Chavarha, M., and Lin, M.Z. (2015). Designs and sensing mechanisms of genetically encoded fluorescent voltage indicators. Curr Opin Chem Biol 27:31–38. Swiech, L., Heidenreich, M., et al. (2015). In vivo interrogation of gene function in the mammalian brain using CRISPR-Cas9. Nat Biotechnol 33(1):102–106. Urnov, F.D., Rebar, E.J., et al. (2010). Genome editing with engineered zinc finger nucleases Nat Rev Genet 11(9):636–646. van Praag, H., Schinder, A.F., et al. (2002). Functional neurogenesis in the adult hippocampus. Nature 415(6875):1030–1034. Wheeler, M.A., Smith, C.J., et al. (2016). Genetically targeted magnetic control of the nervous system. Nat Neurosci 19(5):756–761. Wickersham, I.R., Finke, S., et al. (2007). Retrograde neuronal tracing with a deletion-mutant rabies virus. Nat Methods 4(1):47–49. Wickersham, I.R., Lyon, D.C., et al. (2007). Monosynaptic restriction of transsynaptic tracing from single, genetically targeted neurons. Neuron 53(5):639–647. Wickersham, I.R., Sullivan, H.A., and Seung, H.S. (2013). Axonal and subcellular labelling using modified rabies viral vectors. Nat Commun 4:2332. Wojaczynski, G.J., Engel, E.A., et al. (2015). The neuroinvasive profiles of H129 (herpes simplex virus type 1) recombinants with putative anterograde-only transneuronal spread properties. Brain Struct Funct 220(3):1395–1420. Wu, Z., Yang, H., and Colosi, P. (2010). Effect of genome size on AAV vector packaging. Mol Ther 18(1):80–86. Xu, W., Morishita, W., et al. (2012). Distinct neuronal coding schemes in memory revealed by selective erasure of fast synchronous synaptic transmission. Neuron 73(5):990–1001. Xu, W., and Sudhof, T.C. (2013). A neural circuit for memory specificity and generalization. Science 339(6125):1290–1295. Yan, Z., Zhang, Y., Duan, D., and Engelhardt, J.F. (2000). Trans-splicing vectors expand the utility of adeno-associated virus for gene therapy. Proc Natl Acad Sci U S A 97(12):6716–6721. Zhou, Y., Zhu, S., et al. (2014). High-throughput screening of a CRISPR/ Cas9 library for functional genomics in human cells. Nature 509(7501):487–491. Zufferey, R., Donello, J.E., et al. (1999). Woodchuck hepatitis virus posttranscriptional regulatory element enhances expression of transgenes delivered by retroviral vectors. J Virol 73(4):2886–2892.
54 •S. E merging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford University Press USA - OSO, T 2018. 07:33:44.
5. APPLICATION OF STEM CELLS TO UNDER STANDING PSYCHIATRIC DISORDER S Kristen Brennand
namely, unlimited self-renewal and the capacity to differentiate into different cell types. By harnessing the potential of Despite decades of research, the earliest cell types affected stem cells to undergo unlimited self-renewal and specific difin psychiatric disease, as well as the molecular, structural, ferentiation, we are now able to generate a renewable source of and functional deficits that underlie the predisposition and living human neurons to study under controlled experimental clinical onset, remain to a large extent unresolved. Recent conditions. This provides us with an exciting opportunity to advances in brain imaging studies have great potential to expose human neural components to rigorous investigation define the structural and circuit-based abnormalities contrib- and establish a translational bridge between animal studies uting to psychiatric disease (reviewed in Linden, 2012, see and the diagnosis and treatment of disease. Although the chapter 14). But such clinical studies are best suited to unravel human brain remains largely inaccessible to direct maniputhe biology of the disease state rather than factors of predis- lation, investigating elemental units of neuronal communicaposition that could have preceded the onset of symptoms by tion and function may lead to a deeper understanding of the years or even decades. While human postmortem samples cellular mechanics that contribute to systemic dysregulation. provide clues to the state of the brain after a prolonged ill- Stem cell research will not supplant animal models or noninness (reviewed in Kleinman et al., 2011, see c hapters 17–18), vasive studies of patients, but it is a vital complement to these the availability of samples is limited (in cohorts that are fre- approaches and heralds a paradigm shift in our investigation quently confounded by variables including treatment history, of the neural substrates of mental disorders. Whereas “cellular reprogramming” describes the condrug/alcohol use, cause of death, postmortem interval, and ethnicity). Moreover, as these samples capture the end-stage version of somatic cells into pluripotent stem cells, “neural of disease, they provide limited insight into the factors con- induction” describes a more lateral conversion of somatic tributing to disease onset. Conversely, although animal mod- (or stem) cells directly to neural stem cells or neurons. Both els allow developmental study (before and after phenotypic processes can occur via forced expression of specific tranonset) of factors contributing to disease risk and onset (see scription factors (Pang et al., 2011; Takahashi et al., 2007) or Chapter 15), they cannot recapitulate the polygenic origins of small molecular treatment (Hou et al., 2013; Li et al., 2015). human neuropsychiatric disease, the relevant human-specific The prospective utility of expanding reprogramming and brain circuitry, or many of the clinical phenotypes that define induction methodologies for reducing the burden of neurothe disease state in humans. To date, the most commonly used degenerative and neuropsychiatric disease derives from two approach for studying psychiatric disease in vivo has been to overarching goals: first, that stem cells represent a source of utilize animal models; however, the complex genetic archi- material from which to generate specific cell types to replace tecture of psychiatric disease (reviewed in Hoischen et al., neural populations damaged by injury or disease; and second, 2014, see c hapter 13) is inadequately reflected in even the best that the generation of a renewable source of genetically tractable human neurons and glial cells will facilitate both the study mouse models. In humans, cellular changes in neurons resulting from neu- of the mechanisms underlying pathological development and ropsychiatric disease are difficult to study, owing in large part serve as a high throughput drug screening platform to idento the lack of live brain tissue from clinical patients. What tify novel therapeutics capable of preventing or reversing disclinical studies of neuropsychiatric disease have so far failed ease processes. The field is progressing at a rapid pace, and the to resolve is whether disease progression reflects developmen- number of reports using reprogramming and/or induction to tal aberrations during neuronal differentiation or activity- investigate the mechanistic basis of neuropsychiatric disorders dependent perturbations of neuronal dendrites or synapses in will likely increase exponentially in the near future. At this nascent stage, the most striking advances in mature neurons—a question that may be resolved using human cell-based models of SZ. Stem cell research has opened a new human reprogramming technology are driven by disease- avenue by which researchers can investigate the cellular and specific questions as researchers begin to work on transmolecular processes underlying human brain development forming some of the most vexing issues in the investigation and pathogenesis. Stem cells exhibit two hallmark properties, of the human central nervous system into tractable research INTRODUCTION
5 5 USA - OSO, 2018. Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press 07:33:44.
problems. Whether the focus is on identifying unknown etiology, engineering genetic rescue, or discovering a novel therapeutic compound, investigators are being challenged to find innovative solutions to unique problems, and the approaches they develop may be generalized to other domains. As the field matures, the cross-pollination of ideas from diverse research programs should facilitate generation of target cell populations and efficacious methods to characterize and rescue relevant phenotypes. In this chapter, we first introduce different types of stem cells used to investigate psychiatric disorders and then highlight some novel approaches in the field of reprogramming and neural induction, with examples that use these methods to understand psychiatric disorders. We conclude with discussion of some of the central challenges in the field. Interested readers can consult other detailed review articles (Mertens et al., 2016; Sandoe and Eggan, 2013). STEM CELLS FROM DIFFERENT SOURCES E M B RYO N I C S T E M C E L L S
Stem cells are defined by two essential characteristics—the capacity for self-renewal and the ability to generate multiple cell types. Although stem cells exist in many adult tissues, their fate choices are typically constrained to a few cell types. Conversely, embryonic stem cells (ESCs) can be maintained in culture indefinitely and exhibit no restriction on fate specification. Human embryonic stem cell (hESC) lines derived from human blastocysts were first characterized in 1998 and exhibited the essential properties of self-renewal and pluripotency observed in mouse ESC lines (Thomson et al., 1998). A growing number of protocols have been developed by which to differentiate both mouse and human ESCs into a variety of types of neurons in the CNS and PNS as well as glial cells (reviewed in Tabar and Studer, 2014). The creation of these early hESC lines was invaluable to the study of early human development and offered the first real possibility of generating a renewable source of diverse cell types in the human nervous system. However, the practical and ethical issues surrounding the acquisition of source material for hESCs constrained the development of additional lines, limiting applicability to a genetically diverse population. Moreover, because hESCs are derived from preimplantation embryos rather than adult patients (and therefore prior to disease onset), one cannot predict which, if any, complex genetic disorders any hESC line might be appropriate for studying. Consequently, hESCs cannot model the multitude of genes at play in most psychiatric disorders, many of which are unresolved. I N D U C E D P LU R I P OT E N T S T E M C E L L S
One of the most significant technological advances in stem cell biology was the seminal series of studies by Takahashi and Yamanaka demonstrating that both embryonic and adult
fibroblasts from mice and humans could be reprogrammed to a state of pluripotency through the retroviral-mediated introduction of four transcription factors—Oct3/4 , Sox2, c-MYC, and Klf4 (Takahashi et al., 2007)—work that was rapidly confirmed by numerous independent laboratories (Maherali et al., 2007; Wernig et al., 2007; Yu et al., 2007). These human- induced pluripotent stem cells (hiPSCs) exhibited all the classic hallmarks of stem cells, including self- renewal and the capability of differentiating into cells from all three embryonic germ layers. Because Epstein-Barr virus (EBV) immortalized lymphoblastoid B-cell lines have been widely banked for studying a variety of diseases, they represent a highly desirable source of cells for reprogramming; unexpectedly, the reprogramming of these transformed cells yields hiPSCs with no detectable EBV elements (Rajesh et al., 2011), although functional neurons have not yet been demonstrated. Perhaps the most salient and exciting aspect of this technology is that differentiated cells arising from hiPSCs retain the genetic information of the fibroblast donor, thus providing a renewable, genetically tractable resource for different types of human cells. This cardinal feature has a profound impact for investigating human disease in that it allows direct observation of hiPSC-derived neurons and glial cells that have a clinically relevant genetic profile. Efforts to validate pluripotency and stability of hiPSC lines have converged on an array of standard assays to demonstrate fundamental properties of stem cells and similarity to hESCs (Figure 5.1). Depending on the method of reprogramming, it may be necessary to show the silencing of viral-mediated introduction of transgenes. Karyotyping is typically performed to ensure that there are no gross chromosomal abnormalities. hiPSC colonies should be positive for typical pluripotency markers, including NANOG, SOX2, OCT4, SSEA4, and TRA-1-60 (Figure 5.1A–C). Competency to generate all three embryonic germ layers following differentiation can be demonstrated through expression of layer-specific markers for ectoderm (e.g., Tuj1), mesoderm (e.g., αSMA), and endoderm (e.g., AFP) (Figure 5.1D–F). Once pluripotency has been achieved, the resultant hiPSCs can be induced to differentiate toward specific lineages, including neural progenitors (Figure 5.1G), which give rise to immature neurons (Figure 5.1H) and finally mature neurons expressing synaptic markers (Figure 5.1H). While the original reprogramming methodologies relied on introducing reprogramming factors via retroviral and/ or lentiviral vectors (Maherali et al., 2008; Takahashi et al., 2007; Yu et al., 2007), a desire to avoid unnecessary genetic mutations spurred the development of integration-free methods such as plasmids, episomes, artificial chromosomes, non- integrating adenoviruses, removable reprogramming cassettes, direct delivery of recombinant proteins and chemical induction, modified mRNAs, or sendai viruses (compared in in (Schlaeger et al., 2015)). Today, both mRNA-based and sendai virus–based reprogramming reagents are commercially available, and several fee-for-service hiPSC production facilities offer service for the generation and banking of large cohorts of hiPSCs.
56 •S. E merging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford University Press USA - OSO, T 2018. 07:33:44.
Reprogramming and validation of hiPSCs from human somatic cells. (A–C) Confocal images of hiPSC colonies expressing pluripotency markers: (A) NANOG (green), OCT4 (red), DAPI (blue); (B) SOX2 (green), SSEA4 (red), DAPI (blue); (C) SOX2 (green), TRA-1–60 (red), DAPI (blue). (D–F) In vitro differentiation into three embryonic germ layers revealed by immunostaining for markers of α-fetoprotein (endoderm) (D), α- smooth muscle actin (mesoderm) (E), and Tuj1 (ectoderm) (F). (G–I) Neuronal differentiation: (G) Neural progenitors cells 7 d after neural induction stained for NESTIN (green), SOX2 (red), and DAPI (blue); (H) immature neurons 7 d after differentiation, stained for MAP2 (green), DCX (red), and DAPI (blue); (I) 4 week-old neurons stained for MAP2 (green), DCX (blue), and synapsin (red). Scale bar = 20 µm. Figure 5.1
D I R E C T E D D I F F E R E N T I AT I O N O F hiP S C S TO N EU RO N S
Directed differentiation attempts to recapitulate embryonic development using small molecules and/or morphogens to mimic the embryonic signaling cues involved in the patterning, specification, and commitment of defined cell types in vivo (Figure 5.2). The most widely used of these cues is combinatorial inhibition of BMP and TGF-β activity, so-called dual SMAD inhibition (Chambers et al., 2016), which rapidly initiates general neural differentiation; this strategy has been applied to all standard differentiation methodologies. In classical differentiations, hiPSCs are grown in suspension as embryoid bodies (EBs), leading to the spontaneous
formation of neural rosettes that express neural progenitor markers such as SOX2, PAX6, NESTIN, and NCAM. These NPCs can (but need not necessarily) be expanded in vitro prior to being further differentiated to neurons (Topol et al., 2015) (Figure 5.2a). This approach has been applied to generate populations of functionally mature cortical excitatory glutamatergic or inhibitory GABAergic neurons from hiPSCs, both populations having the ability to engraft and project when transplanted in vivo (Espuny-Camacho et al., 2013; Mariani et al., 2012; Nicholas et al., 2013; Shi et al., 2012). Conversely, in monolayer differentiation protocols, hiPSCs are subjected to single cell dissociation and then differentiated in an adherent paradigm (Kriks et al., 2011). Perhaps owing to
5. AS.pplication ofUniversity S temPress C ells to 2018. P sychiatry Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford USA - OSO, 07:33:44.
(a)
(b)
(c)
Three general strategies are currently used to differentiate neurons from hiPSCs. (A) Classical EB-based differentiations can yield an expandable population of NPCs. Left: hiPSC-derived NPCs labeled with NESTIN (green), SOX2 (red) and DAPI (blue). Right: hiPSC- derived neurons labeled with MAP2AB (green), TUJ1 (red) and DAPI (blue). (B) Monolayer midbrain dopaminergic differentiation protocol. Left: hiPSC-derived midbrain floorplate precursors labeled with NESTIN (green) and FOX2A (red). Right: hiPSC-derived midbrain dopaminergic neurons labeled with LMX1A (green), TUJ1 (red) and FOXA2 (blue). (C) Neural differentiations in 3D organoids spontaneously recapitulate inside-out pattern of corticogenesis. Cortical neurons labeled with CTIP2 (green), SATB2 (red) and Hoeschst (blue). Adapted with permission: Brennand et al., 2011; Kriks et al., 2011; Pasca et al., 2015. Figure 5.2
a more straightforward dosing of differentiation cues, monolayer protocols represent the most rapid and efficient neuronal differentiation of hiPSCs (Figure 5.2b). This strategy has been used to generate functionally mature dopaminergic and inhibitory GABAergic neurons with remarkably high efficiency, again with the ability to engraft and function when transplanted in vivo (Kriks et al., 2011; Maroof et al., 2013). Most recently, three- dimensional (3D) cerebral organoid (a)
(b)
methodologies, which permit extended differentiation of hiPSCs for up to a year, have been shown to demonstrate a level of self-organization beyond what is possible in 2D cultures, and so may be ideally suited for studies of microcephaly and macrocephaly (Lancaster et al., 2013; Mariani et al., 2015; Pasca et al., 2015; Qian et al., 2016) (Figure 5.2c). Across all three methodologies, hiPSC- derived neural cells most resemble fetal brain tissue (Brennand et al., 2015; Mariani et al., 2012; Nicholas et al., 2013; Pasca et al., 2015); therefore, ongoing research is investigating the extent to which novel media formulations (Bardy et al., 2015) or strategies to express molecular hallmarks of age (Miller et al., 2013) accelerate the maturity and/or aging of hiPSC-derived neurons (reviewed in Studer et al., 2015). There are advantages and limitations to each differentiation strategy. Substantial time and resources are required to generate and validate NPCs, but once established they are a remarkably robust and scalable intermediate cell type. While monolayer differentiations are fast and yield relatively pure populations, they typically generate single cell types and so poorly model network effects. Within 3D cerebral organoid differentiations, it seems that complex structures and networks spontaneously arise, unequivocally making them the best in vitro model for corticogenesis; however, these protocols require up to a year. Within these constraints, the optimal methodology should be rationally selected for each experimental question. N EU RO NA L I N D U C T I O N
A rapidly evolving technology is the direct conversion of somatic cells to neuronal lineages (reviewed in Suzuki and Vanderhaeghen, 2015) (Figure 5.3). An early study demonstrating the possibility of direct programming described direct conversion of human somatic cells to functional neurons using a set of four neural lineage– specific transcription factors, ASCl1, BRN2, MYT1L, and NEUROD1 (Pang et al., 2011). Independent laboratories used a partially overlapping set of transcription factors in combination with specific microRNAs (miRNAs), such as miRNA-9 and miRNA-124, to achieve similar results (Ambasudhan et al., 2011; Yoo et al., 2011). Relative to neuronal differentiation protocols, neuronal induction is extremely rapid, producing functional neurons in less than three weeks (Pang et al., 2011). Although early studies reported low neuronal induction efficiencies (less than 10%), simply adding a selection for transduced cells improved yields to nearly (c)
Direct induction of lineage-specific population of neurons from fibroblasts or hiPSCs. (A) 21-day-old NGN2 hiPSC-induced excitatory neurons labeled with lentiviral-NGN2-GFP (green) and MAP2AB (red). (B) 16-day-old fibroblast-induced dopamergic neurons labeled with TH (green) and TUJ1 (red). TH-promoter-GFP (green) and DAT (red) and DAPI (blue). (C). 21-day-old fibroblast-induced serotonergic neurons labeled with TPH (green) and MAP2AB (red). Adapted with permission: Caiazzo et al., 2011; Zhang et al., 2013. Figure 5.3
58 •S. E merging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford University Press USA - OSO, T 2018. 07:33:44.
100% (when starting from hiPSCs or NPCs) (Ho et al., 2016; Zhang et al., 2013). For example, the forced expression of one lineage-specific transcription factor, Ngn2, yields a nearly pure population of excitatory neurons with synapse formation capabilities within 21 days (Zhang et al., 2013). Today, functionally mature neurons—including specific populations of excitatory (Zhang et al., 2013) (Figure 5.3a), dopaminergic (Caiazzo et al., 2011) (Figure 5.3b), serotonergic (Vadodaria et al., 2016; Xu et al., 2016) (Figure 5.3c) and motor neuron (Son et al., 2011) neurotransmitter identities—can be rapidly generated via the forced expression of lineage-specific neural genes. Because neuronal induction can bypass neuronal development, there were early concerns that developmental cellular phenotypes contributing to disease initiation could be missed in disease modeling studies; however, this methodology has now been applied to recapitulate a number of autism-related neuronal phenotypes in human neurons (Chanda et al., 2013; Pak et al., 2015; Yi et al., 2016). Moreover, whereas reprogramming leads to erasure of all age-related epigenetic marks in hiPSCs and their differentiated progeny (Miller et al., 2013), neuronal induction straight from patient somatic cells retains aging-associated transcriptomic signatures (Mertens et al., 2015a). Consequently, neuronal induction is a robust approach that should be uniquely amenable to specific human cell–based disease modeling approaches. Moving forward, efforts to characterize expression patterns across human (Bakken et al., 2016; Darmanis et al., 2015; Lake et al., 2016; Miller et al., 2014; Zhang et al., 2016) development, brain regions, and single cell types will facilitate improved identification, purification, and/or induction of specific populations of neurons and glia.
et al., 2012; Marchetto et al., 2010), fragile X syndrome (Liu et al., 2012; Sheridan et al., 2011; Urbach et al., 2010), Phelan– McDermid syndrome (Bidinosti et al., 2016; Shcheglovitov et al., 2013; Yi et al., 2016), and Timothy syndrome (Krey et al., 2013; Pasca et al., 2011) are all associated with mutations in single genes and will be instructive in developing technologies for genetically mediated rescue or screening for biochemical compounds to ameliorate or reverse cellular phenotypes. R ET T SY N D RO M E
Capitalizing on the opportunity to investigate a monogenic ASD developmental disorder marked by both cognitive and motor impairments, several laboratories have generated and begun to characterize neurons derived from Rett syndrome (RTT) patients. Caused by a mutation in the X-linked gene, methyl-CpG-binding protein 2 (MeCP2), symptoms of RTT emerge in females around 6–18 months of age, following a period of unremarkable and grossly normal development (reviewed in Chahrour and Zoghbi, 2007). The first characterization of RTT patient–derived neurons revealed several morphological and electrophysiological phenotypes, including altered soma size, spine density, synapse number, calcium signaling, and evoked activity, compared with neurons derived from controls (Marchetto et al., 2010). Partial rescue of the decrease in synapse number in RTT neurons was achieved through application of the nonspecific growth factor, IGF1. Because the majority of causative MECP2 variants are nonsense mutations, the authors then explored the possibility of using a pharmacological approach to impair ribosomal proofreading and allow read-through of the premature stop codon to restore MECP2 expression; low-dose application of the antibiotic gentamicin was able to enhance MECP2 expression and showed a similar effect to that of IGF1 in increasing synM O D E L I N G P SYC H I AT R I C apse number. Using two fundamentally different mechanisms DISORDER S USING for pharmacological rescue of phenotypes, this study demonSTEM CELLS strated that at least some facets of cellular dysregulation could be reversed in human neurons. Following this initial report MONOGENIC DISEASES and consistent with its findings, four independent studies The most approachable diseases to investigate mechanisti- have also reported neuronal maturation defects, decreased cally remain those associated with highly or completely pene- neuronal soma size, and reduced excitatory synapse number trant single gene mutations. This genetic determinism reduces and function in patient-derived neurons (Ananiev et al., 2011; complexity, permitting the study of smaller patient cohorts Cheung et al., 2011; Farra et al., 2012; Kim et al., 2011). By coupling targeted deletion of MECP2 in hESC- and narrowing the investigative focus for characterization of the relevant pathology. To date, the most significant break- derived neurons with unbiased and TALEN-edited isogenic throughs in terms of identifying potential strategies to reverse genome-wide comparisons of global gene expression patterns, or prevent phenotypic disturbances have come from the study it was revealed that MECP2 functions as a global activator of monogenic diseases (Table 5.1). Starting from a functional in neurons but not in neural progenitor cells (Li et al., 2013). evaluation of a circumscribed genetic domain, two general Moreover, reduced transcription of MECP2 in hESC-derived approaches are being developed that show considerable prom- neurons resulted in decreased protein synthesis, reduced ise in being able to rescue cellular phenotypes observed during AKT/mTOR pathway activity, and impaired mitochondrial the differentiation of neurons from patient-specific hiPSCs— function. Activation of AKT/mTOR signaling both increased protein synthesis and ameliorated disease phenotypes in biochemical rescue and targeted gene editing (Figure 5.2). Although psychiatric disease generally has a complex mutant neurons (Li et al., 2013). Increased dosage of MeCP2 also leads to a severe neurodegenetic etiology, there are a few examples of monogenic diseases, particularly a subset of autism spectrum disorders velopmental disorder in males; cortical neurons differentiated (ASD) for which a causative genetic locus has been identified. from hiPSCs derived from patients with MECP2 duplication Rett Syndrome (Ananiev et al., 2011; Cheung et al., 2011; Farra syndrome (MECP2dup) showed increased synaptogenesis 5. AS.pplication ofUniversity S temPress C ells to 2018. P sychiatry Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford USA - OSO, 07:33:44.
07:33:44.
Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press USA - OSO, 2018.
Table 5.1 PATIENT-S PECIFIC HIPSC STUDIES OF PSYCHIATRIC DISORDERS DISEASE
MUTATION
CASES/C ONTROLS
REPROGRAMMING METHOD
DIFFERENTIATION
PHENOTYPE
RESCUE
REFERENCE
ASD
NRXN1
2 isogenic pairs (1 conditional knockout, 1 conditional truncation)
ESCs
Ngn2-induced excitatory neurons and forebrain (glutamatergic and GABAergic) neurons
Impaired neurotransmitter release
—
Pak et al., 2015
ASD
TRPC6
2 cases, 2 controls
Retrovirus (OCT4, SOX2, KLF4, c-MYC)
NPCs and forebrain (glutamatergic and GABAergic) neurons
Decreased neurite length and complexity and dendritic spine density, reduced calcium influx
TRPC6 overexpression, IGF1 or TRPC6 agonist treatments increased TRPC6 levels and dendritic spine density
Griesi-Oliveira et al., 2015
ASD
15q11-q13.1 Dup
5 cases, 1 control
Retrovirus, Lentivirus and Integration-free episomes (OCT4, SOX2, KLF4, c-MYC, LIN28)
Forebrain (glutamatergic and GABAergic) neurons
15q11-q13.1 transcript levels did not consistently correlate with copy number
—
Germain et al., 2014
ASD
7q11.23 Del & Dup
7 cases, 1 related control, two unrelated controls
mRNAs (OCT4, SOX2, KLF4, c-MYC, LIN28)
Forebrain (glutamatergic and GABAergic) neurons
7q11.23 dosage affects disease relevant transcriptional programs, specifically caused by dosage imbalances in GTF2I
—
Adamo et al., 2014
ASD
Not known
4 male cases, 4 unaffected fathers
Retrovirus (OCT4, SOX2, KLF4, c-MYC) Integration-free episomes
Cerebral organoid
Accelerated cell cycle and overproduction of GABAergic inhibitory neurons
FOXG1 knockdown reversed overproduction of GABAergic neurons
Mariani et al., 2015
ASD
Not known
8 cases, 5 controls
Retrovirus (OCT4, SOX2, KLF4, c-MYC)
NPCs and forebrain (glutamatergic and GABAergic) neurons
Overproliferation of NPCs, reduced synaptogenesis and synchronization of neuronal networks.
LiCl increased β- catenin activity and reduced proliferation; IGF1 normalized neuronal network activity
Marchetto et al., 2017
BD
Not known
3 cases, 3 controls
Retrovirus (OCT4, SOX2, KLF4, c-MYC)
Forebrain (glutamatergic and GABAergic) neurons
Bias towards expression of ventral telencephalic fate (GABAergic) genes; reduced amplitude of calcium transients
LiCl treatment increased dorsal patterning
Chen et al., 2014
BD
Not known
6 cases, 6 controls
Retrovirus (OCT4, SOX2, KLF4, c-MYC)
Forebrain (glutamatergic and GABAergic) neurons
Reduced amplitude of calcium transients
LiCl treatment increased calcium transient amplitude
O’Shea and McInnis, 2015
BD
Not known
12 cases, 6 controls
iNeurons
miR-9/9*-124, NEUROD2, ASCL1 and MYT1L iNeurons
Altered cellular adhesion correlated to patient clinical lithium responsiveness
—(Acute LiCl effect tested but not observed
Wang et al., 2014
Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press USA - OSO, 2018.
07:33:44.
BD
Not known
3 Li-responsive cases, Li-non- responsive cases, 4 controls
Sendai virus
Hippocampal dentate gyrus granule neurons
Mitochondrial abnormalities, hyperactive action- potential firing (via patch- clamp recording and somatic Ca2+ imaging)
LiCl treatment selectively reversed hyperexcitability in responsive cases
Mertens et al., 2015
BD
Not known
2 cases, 2 controls
Retrovirus (OCT4, SOX2, KLF4, c-MYC)
NPCs
Reduced proliferation and abnormal expression of WNT pathway genes
Inhibition of GSK3 rescued proliferation defects
Madison et al., 2015
BD
Not known
1 case, 1 control (hiPSC); 5 cases, 3 controls (iNeurons)
Retrovirus (OCT4, SOX2, KLF4, c-MYC)
NPCs and neurons miR-9/9*-124, NEUROD2, ASCL1 and MYT1L iNeurons
Increased miR-34a expression
—
Bavamian et al., 2015
FXS
FMR1
3 cases
Retrovirus (OCT4, SOX2, KLF4, c-MYC)
—
—
—
Urbach et al. (2011)
FXS
FMR1 CGG repeat expansions (one mosaic patient, two with >600 repeats)
3 cases
Retrovirus (OCT4, SOX2, KLF4, c-MYC)
Neurons, glia
Neuronal differentiation, process morphology, increased glia
—
Sheridan et al., 2011
FXS
FMR1 premutation −30, 94 CGG repeat
Retrovirus (OCT4, SOX2, KLF4, c-MYC)
Neurons
Reduced neurite length, synaptic puncta, PSD-95
—
Liu et al., 2012
PMS
SHANK3
2 cases; 2 controls
Retrovirus (OCT4, SOX2, KLF4, c-MYC)
Layer-specific cortical neurons
Reduced SHANK3 expression and major defects in excitatory, but not inhibitory, synaptic transmission
IGF1 promoted formation of mature excitatory synapses
Shcheglovitov et al., 2013
PMS
SHANK3
2 cases; 2 controls
Retrovirus (OCT4, SOX2, KLF4, c-MYC)
Layer-specific cortical neurons
Reduced frequency of spontaneous EPSCs; impaired AKT activity
AKT activation (SC79 or TG003) increased EPSCs
Bidinosti et al., 2016
PMS
SHANK3
SHANK3 conditional heterozygous and homozygous knockouts
ESCs
Ngn2-induced excitatory neurons
Impaired Ih channels, neuronal morphology and synaptic connectivity
—
Yi et al., 2016
RTT
MeCP2 (1155del3, Q244X, T158M, R306C) missense, nonsense, and frameshift mutations
4 cases
Retrovirus (OCT4, SOX2, KLF4, c-MYC)
Forebrain (glutamatergic and GABAergic) neurons
Reduced soma size, number of spines, glutamatergic synapses; altered Ca2+ transients, sEPSCs, sIPSCs
IGF1partially increased synapse number; gentamycin restored MeCP2 expression in nonsense mutation
Marchetto et al., 2010
(continued)
07:33:44.
Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press USA - OSO, 2018.
Table 5.1 CONTINUED DISEASE
MUTATION
CASES/C ONTROLS
REPROGRAMMING METHOD
DIFFERENTIATION
PHENOTYPE
RESCUE
REFERENCE
RTT
MeCP2-null mutation
3 cases
Retrovirus (OCT4, SOX2, KLF4, c-MYC)
Neurons
Soma size reduction
—
Cheung et al., 2011
RTT
MeCP2 (T158M, E235fs, Q244X, R306C, X487W)
5 cases
Retrovirus (OCT4, SOX2, KLF4, c-MYC)
Forebrain (glutamatergic and GABAergic) neurons
Decreased neuronal differentiation
—
Kim et al., 2011
RTT
MeCP2 (T158M, V247X, R306C, R294X)
4 cases and isogenic X-inactivation controls
Lentivirus (OCT4, NANOG, SOX2, LIN28), Retrovirus (OCT4, SOX2, KLF4, c-MYC)
Forebrain (glutamatergic and GABAergic) neurons
Decreased nuclear and neuron size
—
Ananiev et al., 2011
RTT
MeCP2
2 isogenic pairs (knockout)
ESCs
Forebrain (glutamatergic and GABAergic) neurons
Decreased transcription and protein synthesis, defect in AKT/mTOR activity, impaired mitochondrial function, decreased soma size and neurite complexity
BDNF, IGF1 or depletion of PTEN restored protein synthesis and soma size and neurite complexity
Li et al., 2013
RTT
MeCP2 (R294X)
1 case; 1 isogenic control
Lentivirus (OCT4, NANOG, SOX2, LIN28)
Astrocytes
Altered microtubule- dependent vesicle transport is altered
Epothilone D restored microtubule dynamics
Delepine et al., 2016)
RTT
MeCP2 duplication
3 cases, 3 controls
Retrovirus (OCT4, SOX2, KLF4, c-MYC)
Forebrain (glutamatergic and GABAergic) neurons
Increased synaptic gene expression and dendritic arborization
—
(Nageshappa et al., 2016)
SZ
4bp deletion in DISC1- frameshift
Integration-free episomes
—
—
—
Chiang et al. (2011)
SZ
4bp deletion in DISC1- frameshift
2 cases; 2 related controls, 1 unrelated control, 2 TALEN-isogenic controls
Integration-free episomes
Forebrain glutamatergic neurons
Increased soma size and total dendritic length in immature neurons, decreased SV2+ puncti, frequency of sEPSCs and synaptic vesicle release
—
Wen et al. (2014)
SZ
Not known
4 cases; 6 controls
Tetracycline-inducible lentivirus (OCT4, SOX2, KLF4, c-MYC, LIN28)
Forebrain (glutamatergic and GABAergic) neurons
Decreased neuronal connectivity, increased NRG1 expression
Loxapine rescue of neuronal connectivity deficits, NRG1 expression
Brennand et al. (2011)
SZ
Not known
4 cases; 4 controls
Tetracycline-inducible lentivirus (OCT4, SOX2, KLF4, c-MYC, LIN28)
Hippocampal dentate gyrus granule neurons
Deficits in generation of DG granule neurons, decreased neuronal activity and sEPSC frequency and amplitude
—
Yu et al. (2014)
SZ
Not known
4 cases; 6 controls
Tetracycline-inducible lentivirus (OCT4, SOX2, KLF4, c-MYC, LIN28)
NPCs
Perturbed responses to environmental stressors
—
Hashimoto-Torii et al. (2014)
Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press USA - OSO, 2018.
07:33:44.
SZ
Not known
4 cases; 6 controls
Tetracycline-inducible lentivirus (OCT4, SOX2, KLF4, c-MYC, LIN28)
NPCs
Increased protein translation
—
Topol et al. (2015)
SZ
Not known
4 cases; 6 controls
Tetracycline-inducible lentivirus (OCT4, SOX2, KLF4, c-MYC, LIN28)
NPCs
Aberrant migration, increased oxidative stress (mitochondrial membrane potential (MMP))
—
Brennand et al. (2015)
SZ
Not known Idiopathic including some CNVs
4 cases; 6 controls 10 cases, 10 controls
Tetracycline-inducible lentivirus (OCT4, SOX2, KLF4, c-MYC, LIN28) Sendai virus
NPCs
Decreased miR9 in a subset of SZ NPCs
Increased miR-9 ameliorated aberrant migration and some gene expression differences
Topol et al. (2016)
SZ
Not known
1 case, 1 control
Retrovirus (OCT4, SOX2, KLF4, c-MYC)
NPCs
Increased extramitochondrial oxygen consumption and reactive oxygen species (ROS)
Valproic acid decreased ROS levels
Paulsen Bda et al. (2012)
SZ
Not known
3 cases, 2 controls
Polycistronic lentivirus (OCT4, SOX2, KLF4, c-MYC)
Glutamatergic and dopaminergic NPCs and neurons
Decreased neural maturation of glutamatergic neurons, impaired ability to generated dopaminergic neurons, increased oxidative stress (MMP)
—
Robicsek et al. (2013)
SZ
15q11.2
3 cases, 3 controls (and 2 DISC1 cases)
Integration-free episomes or sendai virus
NPCs
Defects with apical polarity and adherent junctions
—
Yoon et al. (2014)
SZ
22q11.2
6 cases, 6 controls
Integration-free episomes
Neurons
Recapitulation of miRNA expression pattern expected of 22q11.2 haploinsufficiency
—
Zhao et al. (2015)
TS
CACNA1C point mutation
2 cases, 2 controls
Retrovirus (OCT4, SOX2, KLF4, c-MYC)
Layer-specific cortical neurons
Differential gene expression; TH expression
—
Pasca et al. (2011)
TS
CACNA1C point mutation
2 cases, 2 controls
Retrovirus (OCT4, SOX2, KLF4, c-MYC)
Layer-specific cortical neurons
KCl-induced dendritic retraction
—
Krey et al. (2013)
TS
CACNA1C point mutation
1 case, 2 controls
Retrovirus (OCT4, SOX2, KLF4, c-MYC)
Layer-specific cortical neurons
TS-associated transcriptional changes were predicted to be co-regulated by calcium- dependent transcriptional regulators
—
Tian et al. (2014)
and dendritic complexity coupled with altered neuronal network synchronization (Nageshappa et al., 2016). The authors tested a library of compounds with defined activity on epigenetic pathways on mature MECP2dup hiPSC neurons, finding that one histone deacetylase inhibitor, NCH-51, reduced the synaptic density and dendritic complexity of patient-derived neurons (Nageshappa et al., 2016). This ability to test the effect of both increased and decreased MECP2 activity in hiPSC- derived functional human neurons in vitro should improve our understanding of mechanisms through which perturbed MECP2 levels lead to neurodevelopmental disorders. Recent studies have revealed that astrocytes play a critical role in Rett syndrome, with perturbed MeCP2-deficient astrocyte function contributing noncell autonomous influences on neurons (Okabe et al., 2012); in globally MeCP2-deficient mice, reexpression of Mecp2 preferentially in astrocytes improved neuronal dendritic morphology and synaptic density concomitant with behavioral deficits and reduced lifespan (Lioy et al., 2011). Consistent with this, hiPSC-derived MeCP2-deficient astrocytes show altered microtubule dynamics and vesicular transport (Delepine et al., 2016). Critically, studies of X-linked disorders are complicated by the loss of X chromosome dosage compensation overtime in hiPSCs; although low-passage female hiPSCs retain the inactive X chromosome of the source somatic cell, X chromosome inactivation is eroded through continuous culture (Mekhoubad et al., 2012; Nazor et al., 2012). Therefore, one procedural complication in the evaluation of female hiPSC lines is the ability to accurately characterize the status of X-inactivation in clonal progeny, an issue that has been central to the investigation of RTT patient hiPSCs. Initially, it was reported that reactivation of the silenced X chromosome occurred during reprogramming, resulting in a differentiated population of human neurons that exhibited random X-inactivation based on variable expression of an epigenetic silencing marker, trimethylated histone 3 lysine 27 (me3H3K27), and the loss of Xist RNA, a noncoding transcript involved in silencing the inactive X chromosome (Marchetto et al., 2010). Other studies, however, found that hiPSCs retained the allelic X- inactivation from the founder somatic cell, which was transcriptionally maintained despite the emergent loss of Xist over extended passaging of the hiPSCs (Ananiev et al., 2011; Cheung et al., 2011; Tchieu et al., 2010). Still others have shown that reprogramming does not alter X-inactivation status from the parent cell, but that late-passage hiPSCs can lose both Xist RNA and me3H3K27 markers, which is believed to signal transcriptional de-repression of the inactive X chromosome (Mekhoubad et al., 2012). Collectively, the preponderance of current evidence suggests that, unlike reprogramming of murine cells, human cells do not typically undergo transient reactivation of both X chromosomes, and that skewing toward a dominant X-chromosome may impact the reprogramming, differentiation, and neuronal phenotyping of female hiPSCs. F R AG I L E X S Y N D RO M E
Fragile X syndrome (FXS) is a genetically mediated ASD and the most common form of inherited intellectual disability.
Caused by an expansion of a CGG repeat (>200 repeats) in the X chromosome–linked fragile X mental retardation gene 1 (FMR1) gene, which leads to the absence of expression of the fragile X mental retardation 1 (FMR1) gene (O’Donnell and Warren, 2002), the extent of cognitive deficits can range from mild to severe. The first published report of hiPSCs from FXS patients compared FXS-hiPSC lines from three unrelated males with a clinical diagnosis of FXS and CGG repeat length in the full mutation range (Sheridan et al., 2011). Retroviral- mediated reprogramming resulted in several hiPSC lines in which the CGG repeat length differed slightly from the donor fibroblast, but it was uncertain whether this change reflected an undetected mosaicism in the fibroblast population or was a consequence of the reprogramming itself. While initial characterization of the patient lines revealed no significant difference in the capacity to differentiate to a neuronal lineage; neural progenitor cells had reduced length and decreased complexity of neural processes. A subsequent study focused on premutation CGG repeat length, generating hiPSCs from a female with both a normal repeat length (30) and a premutation repeat length (94) on separate X chromosome alleles (Liu et al., 2012). Functional characterization of differentiated neurons revealed several phenotypes, including decreased neurite length, decreased expression of the synaptic marker, PSD-95, elevated spontaneous calcium transients, and heightened responses to glutamate, while repeat length appeared stable throughout reprogramming and differentiation. Together, these studies provide initial evidence of morphological and synaptic abnormalities that are consistent between FXS patients and a carrier of a premutation length CGG repeat sequence and suggest the existence of a graded phenotype associated with repeat-level regulation of FMR1 expression. As with Rett Syndrome, hiPSC-based models of fragile X are also complicated by the extent and stability of X- inactivation in vitro. Critically, following reprogramming, the FMR1 gene remained inactive in all FX hiPSC lines, unlike FX embryonic stem cell lines (Sheridan et al., 2011; Urbach et al., 2010). Consequently, it remains unclear when FX- hiPSCs can be used to model the differentiation-dependent silencing of the FMR1 gene. P H E L A N MC D E R M IT T SY N D RO M E
Phelan McDermitt syndrome (PMS) is caused by heterozygous deletion of chromosome 22q13.3, which includes the loss of the postsynaptic protein SHANK3; clinical manifestations include ASD, attention deficits, absent or delayed speech, mild to moderate intellectual disability, and motor alterations (Phelan and Betancur, 2011). Because genetic deletions and loss-of-function point mutations in SHANK3 produce the same core neuropsychiatric phenotypes as the larger 22q13 deletions, it seems that loss of SHANK3 is sufficient to account for the key neuropsychiatric phenotypes in PMS. SHANK3 is a scaffolding protein that forms the core of the postsynaptic density and functions as a platform on which many additional proteins accrete (Maezawa et al., 2009). Three groups have independently shown that hiPSC- derived PMS neurons show reduced SHANK3 expression
64 •S. E merging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford University Press USA - OSO, T 2018. 07:33:44.
together with impaired dendritic arborization and major deficits in specifically in excitatory, but not inhibitory, synaptic activity (Bidinosti et al., 2016; Shcheglovitov et al., 2013; Yi et al., 2016). Isogenic comparisons of CRISPR-engineered heterozygous and homozygous SHANK3 mutations demonstrated that SHANK3- deficiency causes functionally impaired hyperpolarization- activated cation (Ih) currents, likely through its ability to interact with and organize the hyperpolarization-activated cyclic nucleotide-gated (HCN) channels that mediate Ih currents. Moreover, chronic pharmacological blockage of Ih channels reproduced the alterations in neuronal morphology and synaptic connectivity observed in SHANK3-deficient neurons (Yi et al., 2016). Excitatory synaptic transmission in PMS neurons can be corrected by restoring SHANK3 expression activity (Shcheglovitov et al., 2013); by treating neurons with IGF1 (as with Rett syndrome), promoting formation of mature excitatory synapses that lack SHANK3 but contain PSD95 and N-methyl-D- aspartate (NMDA) receptors (Shcheglovitov et al., 2013); or by pharmacological and genetic activation of Akt or inhibition of Cdc2-like kinase 2 activity (identified through an unbiased proteomic screen) (Bidinosti et al., 2016). Overall, these hiPSC-based studies indicate that PMS results from a disruption in the ratio of cellular excitation and inhibition in patient neurons. T I MOT H Y SY N D RO M E
Caused by a single-point mutation in the CACNA1C gene, Timothy syndrome (TS) is a rare disorder that has a pervasive impact on the developing central nervous system and leads to autism or ASD, in conjunction with other deficits including cardiac arrhythmia and intermittent hypoglycemia. CACNA1C encodes the alpha-1 subunit of the L-type calcium channel, Cav1.2, and the missense mutation responsible for TS impairs voltage-dependent channel inactivation. To identify the functional impact of the single point mutation on human neurons, hiPSCs from TS patients were generated and compared with neurons derived from control subjects without the disease (Pasca et al., 2011). Consistent with the proposed role of the point mutation in regulating Cav1.2 inactivation kinetics, action potentials recorded from TS neurons exhibited a broader profile, and there was an elevated increase in intracellular calcium following depolarization. This change in intracellular calcium had consequent effects on Ca2+-mediated activity-dependent gene expression through the CREB pathway as evidenced by whole-genome expression profiles. Downstream targets of CREB include tyrosine hydroxylase (TH), the rate-limiting enzyme necessary for dopamine and norepinephrine production. In TS-derived neurons, baseline TH levels were higher, and in contrast to control neurons, there was no downregulation of TH following prolonged depolarization. The differentiation protocol used in this study was designed to promote the generation of cortical neurons. One of the most striking phenotypes observed in the population- level analysis of TS-derived neurons was a propensity for differentiation into upper-layer cortical neurons. This finding
suggests a new investigative target for postmortem studies to determine whether patients have an imbalance in the composition of cortical neurons. A bias toward upper-layer neurons would effectively increase the proportion of neurons projecting to subcortical regions at the expense of callosal projections and could significantly alter signaling pathways among distributed neural systems. Finally, in an attempt to define the specificity of the mutation and role of the L-type calcium channels in the observed pathology, application of roscovitine, which increases inactivation of this channel subtype, was highly effective in ameliorating expression of TH in differentiated neurons. Follow- up studies by the same group subsequently observed that hiPSC-derived TS neurons undergo dendritic retraction, rather than growth, in response to depolarization (Krey et al., 2013). Dendrite retraction was independent of calcium permeation through the mutant CaV1.2 channel; instead, it was associated with ectopic activation of RhoA, a direct regulator of dendritic arborization, via the CaV1.2 channel-associated protein GTPase Gem (Krey et al., 2013). Additionally, a genome-wide weighted coexpression network analysis (WGCNA) of TS and control-derived neurons, with and without neuronal depolarization, predicted that TS- associated transcriptional changes were likely modulated by calcium-dependent transcriptional regulators such as NFAT, MEF2, CREB, and FOXO (Tian et al., 2014). Altogether, these studies suggest that the molecular and cellular effects observed in TS likely result from both calcium-dependent and independent functions of CaV1.2. P O LYG E N I C D I S E A S E S
For most psychiatric disorders there is no single identified genetic cause. These complex polygenic diseases, which are known to include schizophrenia, affective disorders, and the vast majority of ASDs, are instead associated with several hundred “risk” genes that may increase the probability of disease onset to variable degrees but alone are not causally sufficient to induce the disease (Eichler et al., 2010). Because these genes confer only susceptibility, there are several other factors that can modify the net risk for a given individual. Any number of combinations of environmental influences, epigenetic mechanisms, and genetic interactions could enhance susceptibility for disease. Disentangling the individual contributions of each factor to the pathophysiology is extremely challenging. Using hiPSCs to address this issue should proceed in a systematic fashion starting from known parameters. If the donor material is obtained from patients, the one certainty is that the genetic background is at least permissive for the disease state. Building upon that knowledge, it is then feasible to explore the impact of additional influences on cellular integrity. AU T I S M
An alternative to using patient-derived neurons is to precisely engineer a mutation found in patients into a control hiPSC line, which permits the exclusive study of the disease-relevant mutation in a control genetic background. When hESCs with
5. AS.pplication ofUniversity S temPress C ells to 2018. P sychiatry Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford USA - OSO, 07:33:44.
two different heterozygous conditional NRXN1 deletions were generated, heterozygous NRXN1 neurons showed that, without any associated changes in neuronal differentiation or synapse formation, NRXN1 deletions selectively impaired neurotransmitter release (Pak et al., 2015). This is consistent with findings from neurexin-1α-knockout mice, which show behavioral deficits arising from defects in synaptic calcium channel function resulting in impaired neurotransmitter release (Etherton et al., 2009; Rabaneda et al., 2014). hiPSC-based studies have been successfully applied to functionally characterize a novel genetic mutation in a nonsyndromic autistic individual. Having identified a de novo balanced translocation disruption of the cation channel TRPC6, patient- derived hiPSCs were used to demonstrate that TRPC6 haploinsufficiency leads to altered neuronal development, morphology, and function (Griesi-Oliveira et al., 2015). These neuronal phenotypes could be rescued by either genetic trpc6 complementation or by treatment with IGF1 or a TRPC6-specific agonist (Griesi-Oliveira et al., 2015). While the aforementioned hiPSC-based models of autism focused on the effect of rare and highly penetrant mutations, groups are now instead focusing on the complexity of idiopathic autism spectrum disorder (Table 5.1). Using a cohort of four patients with increased head size (macrocephaly) and poorer clinical outcome, ASD hiPSC- derived organoids revealed increased GABAergic differentiation and increased synaptogenesis (Mariani et al., 2015). Transcriptome analysis of cortical organoids identified FOXG1 to be elevated in ASD organoids; subsequently, they showed that knockdown of FOXG1 normalized the shift in GABA phenotype in ASD cortical organoids, suggesting that FOXG1 perturbations may link a genetically diverse cohort of ASD patients (Mariani et al., 2015). In a second hiPSC-based study of idiopathic autism using an independent cohort comprised of eight ASD individuals with early brain overgrowth and five non-ASD controls with normal brain size, ASD-derived NPCs showed increased cell proliferation while ASD-neurons had abnormal neurogenesis and reduced synaptogenesis; defects in these ASD- neuronal networks were rescued by IGF1 (Marchetto et al., 2017). Somewhat consistent with the transcriptome analysis of Mariani et al., this report also noted a downregulation of GABA-related genes in ASD-neurons and an upregulation of genes related to early stages of neural differentiation, including FOXG1 (Marchetto et al., 2017). Altogether, these hiPSC-based studies of monogenic and polygenic demonstrate an array of phenotypes both in the patterning of neural progenitors and the function of postmitotic neurons. There has been substantial reproducibility of hiPSC- based observations between independent studies and patient cohorts, particularly with respect to monogenic ASD, where that has also been strong concordance between hiPSC-based findings and those in corresponding animal models. SCHIZOPHRENIA
hiPSC- based studies of syndromic and idiopathic forms of SZ have reported a striking convergence of cellular and
molecular phenotypes (Table 5.1). While SZ hiPSC-derived NPCs display aberrant migration (Brennand et al., 2015), adherens junctions polarity (Yoon et al., 2014), increased oxidative stress (Brennand et al., 2015; Paulsen Bda et al., 2012; Robicsek et al., 2013), perturbed responses to environmental stressors (Hashimoto-Torii et al., 2014), and increased protein translation (Topol et al., 2015a). SZ hiPSC-derived neurons exhibit decreased synaptic maturation (Brennand et al., 2011; Robicsek et al., 2013; Wen et al., 2014; Yu et al., 2014) and activity (Wen et al., 2014; Yu et al., 2014). Taken together, these studies represent complementary strategies to identify relevant pathology and etiological factors contributing to predisposition to SZ, which is already seemingly converging on a common set of developmental mechanisms that are vulnerable to dysregulation in individuals at risk for SZ. Early hiPSC-based studies of SZ focused primarily on genetically heterogeneous collections of SZ patients, largely reflecting the availability of patient-derived fibroblasts during this period. We first reported aberrant gene expression, reduced neuronal connectivity, neurite number, and synaptic maturation in neurons derived from four idiopathic SZ cases (Brennand et al., 2011), and then later demonstrated abnormal cytoskeletal remodeling and oxidative stress in NPCs derived from these same patients (Brennand et al., 2015). When a novel hippocampal dentate gyrus (DG) granule neuron differentiation protocol was applied to this same cohort, reduced neuronal (percentage active neurons identified by spontaneous calcium transient activity) and synaptic activity (decreased spontaneous excitatory synaptic current [sEPSC] frequency and amplitude) was observed (Yu et al., 2014). A second group observed both impaired synaptic maturation and mitochondrial dysfunction in SZ NPCs and neurons derived from an independent cohort of three idiopathic SZ cases (Robicsek et al., 2013). Consistent with these findings, a third group demonstrated elevated levels of reactive oxygen species and aberrant mitochondrial oxygen consumption in NPCs derived from one SZ patient (Paulsen Bda et al., 2012). To date, few studies have attempted to identify a shared molecular mechanism driving these phenotypic differences in idiopathic SZ patient hiPSC–derived NPCs or neurons. However, converging evidence indicates that miRNAs may contribute to SZ risk. For example, genome-wide association studies (GWAS) have consistently shown an association of the miR-137 locus and an enrichment of predicted miR-137 targets within SZ-associated genes (Ripke et al.,2011, 2013; Schizophrenia Working Group, 2014). Concomitant with a bioinformatic analysis identifying an enrichment of predicted miR-137 and miR-9 targets amongst SZ-associated genes (Hauberg et al., 2016), we found that miR-9 was not only abundantly expressed in hiPSC-derived control NPCs but also significantly downregulated in a subset of SZ NPCs (Topol et al., 2016). Moreover, we observed a strong correlation between miR-9 expression and miR-9 regulatory activity, and that overexpression of miR-9 was sufficient to ameliorate our previously reported neural migration deficit in SZ NPCs (Brennand et al., 2015) whereas knockdown partially phenocopied aberrant migration in control NPCs (Topol et al., 2016). Unexpectedly, proteomic-based and gene
66 •S. E merging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford University Press USA - OSO, T 2018. 07:33:44.
expression–based analysis revealed that these effects were mediated primarily by small changes in expression of indirect miR-9 targets rather than large changes in direct miR-9 targets, indicating that aberrant levels and activity of miR-9 may be one of the many factors that contribute to SZ risk, at least in a subset of patients (Topol et al., 2016). These results illustrate both the potential utility of patient- derived hiPSCs to identify novel gene interactions in complex genetic disorders and the constraints imposed by the technical challenges of generating multiple hiPSC lines on a large enough scale to validate the role of these interactions in cellular phenotypes in diverse patient populations. Importantly, however, this study effectively demonstrates how a genetically complex disease can be probed mechanistically through patient-specific hiPSCs and lead to the identification of novel cellular targets of pathology. Although SZ is a genetically complex disease, several genes have emerged as prominent risk factors. In fact, the first report of SZ hiPSCs were from patients carrying a DISC1 mutation (Chiang et al., 2011). Originally identified at the breakpoint of a balanced (1;11) (q42;q14) chromosome translocation in a large Scottish family, mutations in DISC1 have been shown to segregate with SZ, schizoaffective disorders, and major depression in several studies (reviewed in Porteous et al., 2011). However, similar to the heterogeneity observed in the clinical profile of patients and family members with DISC1 mutations, the behavioral deficits observed in the rodent models also varied across studies using different strategies to disrupt DISC1 expression. In an early study showing that reprogramming efficiency and differentiation capacity were similar between DISC1 patients and control hiPSCs, an episomal vector– based approach was used for integration-free reprogramming of fibroblasts from several family members who harbor a 4 bp mutation in the DISC1 gene (Chiang et al., 2011). More recently, a study of patient-derived cortical neurons from two cases with a DISC1 frameshift mutation showed synaptic vesicle release deficits as well as perturbed expression of synaptic genes, both of which could be corrected following genetic repair of the DISC1 mutation, or replicated following introduction of the DISC1 mutation into a control hiPSC line (Wen et al., 2014). Beyond just hiPSC-derived neurons from two DISC1 patients with differing diagnoses (SZ and major depression), two unaffected related controls, and one unaffected unrelated control, this group produced perfect isogenic controls through TALEN-based gene editing. DISC1 mutant neurons exhibit increased soma size and total dendritic length in immature neurons, together with decreased synapse number (SV2+ puncti), spontaneous activity (sEPSCs) and synaptic vesicle release. Critically, correction of the DISC1 locus in a patient hiPSC line perfectly rescued these neuronal phenotypes, while introducing the DISC1 frameshift mutation into two control hiPSC lines was sufficient to recapitulate the neuronal defects observed in patients. Given the high penetrance of this DISC1 mutation, and the perfect phenotypic amelioration/recapitulation with TALEN-targeted corrections/ mutations, the results clearly demonstrate phenotypic effects resulting from the frameshift DISC1 mutation. Even more intriguingly, the authors demonstrate that mutant DISC1
protein is capable of depleting wildtype DISC1 levels, likely by increasing wildtype DISC1 ubiquitination and also causing large-scale transcriptional dysregulation in human neurons. Mutant DISC1 seems to function as a hub for transcriptional regulation of many genes (>89) implicated in psychiatric disorders (Wen et al., 2014). hiPSC-based models have also been used to query which gene (or genes) within a larger copy number variation (CNV) are sufficient to causally contribute to disease relevant phenotypes. In two patients with 15q11.2 deletions, defects with apical polarity and adherent junctions were observed in hiPSC-derived NPCs; subsequent lentiviral overexpression and short hairpin RNA knockdown studies demonstrated that these cellular phenotypes resulted from haploinsufficiency of CYFIP1, a component of the WAVE signaling complex that regulates cytoskeletal dynamics (Yoon et al., 2014). Building on this finding, the authors demonstrated that CYFP1 deficiency in the developing mouse cortex leads to ectopic placement of radial glial cells outside of the ventricular zone (Yoon et al., 2014). There is a notable convergence of cellular phenotypes observed in hiPSC-based studies across independent cohorts comprised of genetically heterogeneous SZ patients, suggesting that the myriad genetic mechanisms contributing to SZ predisposition may act through a more limited number of cellular outcomes. BIPOLAR DISORDER
The application of hiPSC-based models to bipolar disorder (BD) has lagged behind that of ASD and SZ (Table 5.1), perhaps reflecting that fewer highly penetrant BD mutations have been identified and that there are limited genetic mouse models of the disease to serve as a basis for comparison. To date, idiopathic hiPSC-based models of BD have focused on the excitatory–inhibitory balance and the concomittant neuronal firing patterns; given the well-defined lithium responsiveness of a substanial minority of BD patients, it is perhaps unsurprising that these studies included a heavy focus on neuronal lithium response (Chen et al., 2014; Mertens et al., 2015b; O’Shea and McInnis, 2015; Wang et al., 2014). An early gene-expression based characterization of BD hiPSC–derived neurons from three patients and three controls reported increased patterning of patient neurons to a GABAergic fate, a change that could be prevented by pretreatment with lithium during neural differentiation (Chen et al., 2014). Moreover, from a now-expanded cohort of six patients and six controls, this group observed reduced neuronal firing (assayed by spontanous calcium activity), which could be ameliorated by lithium treatment, although the researchers did not specifically attempt to correlate patient clinical and hiPSC-based lithium responsiveness (O’Shea and McInnis, 2015). Across an independent cohort by a second group, induced neurons from twelve lithium-treated BD patients and six healthy controls showed changes in cell adhesion that were associated with patient lithium response (Wang et al., 2014). Most recently, a third study specifically characterized three BD patients with known clinical lithium responsiveness and
5. AS.pplication ofUniversity S temPress C ells to 2018. P sychiatry Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford USA - OSO, 07:33:44.
three with known nonresponsiveness (Mertens et al., 2015b). Here, consistent with a genetic mechanism underlying clinical lithium response, a hyperactive neuronal firing in BD patient– derived neurons was selectively reversed by lithium treatment only in neurons derived from those BD patients who had a demonstrated clinical response to lithium treatment (Mertens et al., 2015b). Cellular phenotypes have also been observed in BD patient–derived NPCs, prior to neuronal maturation. In a family with two BD male offspring and their two unaffected parents, patient NPCs showed reduced cellular replication and perturbed expression of WNT genes; both were rescued by treatment with a WNT agonist (CHIR-99021) (Madison et al., 2015). Given the known influences of mood stabilizers on miR-34a levels, miR-34 levels were queried across two patient cohorts; increased miR-34a levels were observed in both NPCs and differentiated neurons (from one patient and one control) and iNeurons (five patients and three controls) generated from BD cases (Bavamian et al., 2015). This finding was replicated in postmortem cerebellar tissue (29 patients). Subsequent overexpression of miR-34a in control hiPSC neurons led to reduced levels of several miR-34 target genes (ANK3 and CACNB3) that are known BD risk genes, together with reducing dendritic branching and delaying synaptic maturation (Bavamian et al., 2015). While independent hiPSC-based studies have not yet shown the same extent of convergent cellular and mechanistic phenotypes described in ASD and SZ hiPSC studies, only in BD have strong correlations been so well correlated between patient clinical pharmacological response and in vitro neuronal phenotypic rescue. For this reason, BD hiPSC models may best demonstrate the potential clinical utility of hiPSC- based drug screens. C H A L L E N G E S F O R MO D E L I N G P S YC H I AT R I C D I S O R D E R S
Tremendous progress has been made in the effort to generate renewable sources of human neurons for mechanistic investigation of psychiatric disease, but many significant challenges remain. With the publication of each new study the field evolves, and new information emerges about critical variables that may influence effective reprogramming, neuronal generation, and the variability in hiPSCs, all of which could impact the investigation of disease-specific and patient-invariant phenotypes necessary for the development of widely applicable therapeutic approaches. During embryonic development, epigenetic mechanisms constrain and direct cell fate, transforming totipotent stem cells into lineage-specific progenitors and, ultimately, terminally differentiated cell types. A goal of cellular reprogramming is to maintain the genetic integrity of donor cells while erasing the epigenetic signature of the source tissue, creating a cellular tabula rasa from which researchers can direct fate specification to the desired cell type. Nonetheless, both genetic (Gore et al., 2011; Hussein et al., 2011; Mayshar et al., 2010) and epigenetic (Lister et al., 2011; Ma et al., 2014; Mekhoubad et al., 2012; Nazor et al., 2012; Ruiz et al., 2012) errors can occur as part of
the reprogramming process. Some reprogramming-associated genetic mutations preexist in the source cells (Gore et al., 2011), while others seem to occur via cellular replication (Lu et al., 2014); the mutation rate is does not reflect the somatic source cell (Ruiz et al., 2013). Incomplete reprogramming occurs independent of the somatic cell type of origin (Ma et al., 2014) and is maintained throughout hiPSC differentiation (Ruiz et al., 2012). Characterizing the extent of residual genetic and epigenetic somatic memory in hiPSCs remains an ongoing challenge, but the frequency of genetic and epigenetic abnormalities does not seem to differ between patients and controls; it is experimentally addressed by including multiple hiPSCs from each individual. Good experimental design includes multiple hiPSC clones from each patient, control, and/or isogenic-edited hiPSC line. The optimization of specific protocols to direct targeted differentiation or induce increasingly refined neuronal subtypes remains very much a work in progress. Researchers are just beginning to refine differentiation and induction protocols to produce specific cell populations of GABAergic, glutamatergic, dopaminergic, and layer-specific cortical neurons as well as astrocytes and oligodendrocytes (reviewed in Velasco et al., 2014). However, reprogramming erases all age-related epigenetic marks in hiPSCs and their differentiated progeny (Miller et al., 2013); therefore, across all existing methodologies, hiPSC-derived neural cells continue to most resemble fetal brain tissue (Brennand et al., 2015; Mariani et al., 2012; Nicholas et al., 2013; Pasca et al., 2015). Earlier in this chapter we discussed ongoing strategies to address this limitation, but at present one must carefully consider that hiPSC-based models are best suited for the study of genetic predisposition to psychiatric disease, not the disease-state itself. Finally, in the investigation of psychiatric disease, the study of genetically mediated cell-autonomous pathology should be countered by an equally vigorous attempt to understand dysfunction within integrated neural networks. One approach will be to pursue in vivo transplantation strategies, but another would be to develop small-scale models of neuronal interactions in vitro. By modeling features of endogenous cell distributions in a given brain region, it may be possible to isolate discrete signaling defects between specific neural subtypes and begin to approximate physiological conditions. Certainly, this represents one of the most significant challenges looking forward—how to ask the right questions so that we can observe signatures of neuronal dysfunction in vitro that may be relevant to disease etiology. Newly differentiated human neurons in vitro exist in an environment that is temporally and spatially distinct from the system we are trying to understand. Many of the specific phenotypes observed thus far in patient-derived hiPSCs are remarkably congruent with data from animal models or postmortem studies and support current working hypotheses. However, many of the patient- derived neurons exhibit minimal or unexpected phenotypes when compared with controls. Our current methodological tools may not have the resolution and sensitivity to detect all the environmental influences on cellular function, which properties are specific to neurons in a dish versus neurons in a brain, and how the history and age of the neuron affects its function.
68 •S. E merging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford University Press USA - OSO, T 2018. 07:33:44.
C O N C LU S I O N Both conceptually and empirically, there is a huge chasm between traditional animal models of psychiatric illness and the limited range of information we have been able to garner from studies of patients and postmortem analysis of human brains. Cellular reprogramming has enabled us to partially fill this gap by establishing a new intermediate level of investigation. Physicians often lament that for many neuropsychiatric disorders, their only option is to treat the symptoms of disease as opposed to its underlying cause. Stem cell technology has the potential to transform this palliative approach to one in which novel therapies are generated from rational design based on causal mechanisms. It remains to be seen whether this field will live up to its promise and whether some of the most troubling issues can be resolved in order to enable revolutionary new therapies for patients. Also uncertain is the extent to which fundamental principles that evolve from a focus on the most prominent psychiatric disorders, namely, affective disorders, SZ, and ASD, can be successfully applied to other disorders such as compulsive and dissociative disorders. In principle, generalization is possible—but for many of these less well-studied disorders, there is a paucity of data on putative risk genes, postmortem analyses, and validated behavioral correlates in animals, all of which are critical to the generation of testable hypotheses using patient-derived human neurons. But what is appealing about the use of hiPSCs and investigations of patient-specific human neurons is the possibility to redefine diagnostic criteria of disease based on a mechanistic understanding of the features underlying relevant pathology. Identification of etiological factors can inform the discussion over whether a categorical or dimensional approach to the diagnosis and treatment of patients is most efficacious. What has been missing in this debate over the years is a mechanistic understanding of symptomatology that may transcend traditional boundaries of behavioral categorization. For example, positive and negative symptoms of SZ may have different neural substrates, but the negative symptoms may be mechanistically similar to features of depressive disorders. Stem cell researchers should build upon this diagnostic framework to test discrete hypotheses regarding neural structure and function while adopting an agnostic stance toward the possibility of shared mechanisms among categorically distinct diseases. In vitro derivation of human neurons that are isogenic to patients reflects a remarkable achievement and a putative turning point in our attempt to understand human neurological diseases. But mental illness is humbling in its complexity, and we are a long way from being able to answer the questions posed at the outset of this chapter. Nor can we expect that hiPSCs will provide the consummate solution. We will not be able to delineate the phenomenology of mental illness by investigating neurons in a dish. Psychiatric disorders are often characterized by complex deficits such an impairment in exerting volitional control over behavior, the persistence of aberrant sensory processing, or maladaptive responses to external demands. We cannot expect that investigations of dissociated human neurons will be able to
provide a comprehensive explanation for what is ultimately an embodied phenomenon, and it is a mistake to presume that a cell-based reductionist strategy will be able to capture all the relevant features of psychiatric disease. Our brains are composed of neurons and glia and a rich milieu of chemical neurotransmitters and modulators. What cellular reprogramming has given us is a means to examine the building blocks of the human brain to search for patient-invariant phenotypes and molecular mechanisms associated with complex diseases. For the first time, we can generate and manipulate human neurons that have confirmed disease-relevant genetic profiles. While the majority of psychiatric diseases may not be immediately amenable to cell-replacement strategies, there is a wealth of information to be gleaned from an understanding of the basic mechanisms. The promise of this technology is nearly boundless, and it is our sincere hope that the excitement, innovation, and productivity expressed by researchers thus far will continue to grow and contribute to a better understanding of how dysfunction of neural components and processes can lead to some of the most devastating ailments. Most importantly, we may learn how to reverse or prevent dysfunction to alleviate the suffering of people who have limited information about why or how their symptoms emerge. A better mechanistic understanding of mental illness will not only enable the development of new therapeutic approaches but will also help affirm that these diseases are the consequence of specific neural pathology and dysregulation of discrete neural processes. AC K N OW L E D G M E N T S This chapter is based heavily on Chapter 9: Application of Stem Cells to Understanding Psychiatric Disorders, Neurobiology of Mental Illness, 4th Edition, written by Kimberly M. Christin, Hongjun Song, and Guo-Li Ming. DISCLOSURES Dr. Brennand has no conflicts of interest to disclose and receives funding from the NIH, the New York Stem Cell Foundation, Brain & Behavior Research Foundation, and the Brain Research Foundation. REFERENCES Adamo, A., Atashpaz, S., et al. (2015). 7q11.23 dosage-dependent dysregulation in human pluripotent stem cells affects transcriptional programs in disease-relevant lineages. Nat Genet 47:132–141. Ambasudhan, R., Talantova, M., et al. (2011). Direct reprogramming of adult human fibroblasts to functional neurons under defined conditions. Cell Stem Cell 9:113–118. Ananiev, G., Williams, E.C., et al. (2011). Isogenic pairs of wild type and mutant induced pluripotent stem cell (iPSC) lines from Rett syndrome patients as in vitro disease model. PLoS One 6:e25255. Bakken, T.E., Miller, J.A., et al. (2016). A comprehensive transcriptional map of primate brain development. Nature 535(7612):367–375.
5. AS.pplication ofUniversity S temPress C ells to 2018. P sychiatry Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford USA - OSO, 07:33:44.
Bardy, C., van den Hurk, M., et al. (2015). Neuronal medium that supports basic synaptic functions and activity of human neurons in vitro. Proc Natl Acad Sci U S A 112:E2725–E2734. Bavamian, S., Mellios, N., et al. (2015). Dysregulation of miR-34a links neuronal development to genetic risk factors for bipolar disorder. Mol Psychiatry 20:573–584. Bidinosti, M., Botta, P., et al. (2016). CLK2 inhibition ameliorates autistic features associated with SHANK3 deficiency. Science 351: 1199–1203. Brennand, K., Savas, J.N., et al. (2015). Phenotypic differences in hiPSC NPCs derived from patients with schizophrenia. Mol Psychiatry 20:361–368. Brennand, K.J., Simone, A., et al. (2011). Modelling schizophrenia using human induced pluripotent stem cells. Nature 473:221–225. Caiazzo, M., Dell’Anno, M.T., et al. (2011). Direct generation of functional dopaminergic neurons from mouse and human fibroblasts. Nature 476:224–227. Chahrour, M., and Zoghbi, H.Y. (2007). The story of Rett syndrome: from clinic to neurobiology. Neuron 56:422–437. Chambers, S.M., Mica, Y., et al. (2016). Dual-SMAD inhibition/WNT activation-based methods to induce neural crest and derivatives from human pluripotent stem cells. Methods Mol Biol 1607:329–343. Chanda, S., Marro, S., et al. (2013). Neurons generated by direct conversion of fibroblasts reproduce synaptic phenotype caused by autism-associated neuroligin-3 mutation. Proc Natl Acad Sci U S A 110:16622–16627. Chen, H.M., DeLong, C.J., et al. (2014). Transcripts involved in calcium signaling and telencephalic neuronal fate are altered in induced pluripotent stem cells from bipolar disorder patients. Transl Psychiatry 4:e375. Cheung, A.Y., Horvath, L.M., et al. (2011). Isolation of MECP2-null Rett Syndrome patient hiPS cells and isogenic controls through X- chromosome inactivation. Hum Mol Genet 20:2103–2115. Chiang, C.H., Su, Y., et al. (2011). Integration-free induced pluripotent stem cells derived from schizophrenia patients with a DISC1 mutation. Mol Psychiatry 16:358–360. Darmanis, S., Sloan, S.A., et al. (2015). A survey of human brain transcriptome diversity at the single cell level. Proc Natl Acad Sci U S A 112:7285–7290. Delepine, C., Meziane, H., et al. (2016). Altered microtubule dynamics and vesicular transport in mouse and human MeCP2-deficient astrocytes. Hum Mol Genet 25:146–157. Eichler, E.E., Flint, J., et al. (2010). Missing heritability and strategies for finding the underlying causes of complex disease. Nat Rev Genet 11:446–450. Espuny-Camacho, I., Michelsen, K.A., et al. (2013). Pyramidal neurons derived from human pluripotent stem cells integrate efficiently into mouse brain circuits in vivo. Neuron 77:440–456. Etherton, M.R., Blaiss, C.A., et al. (2009). Mouse neurexin-1alpha deletion causes correlated electrophysiological and behavioral changes consistent with cognitive impairments. Proc Natl Acad Sci U S A 106:17998–18003. Farra, N., Zhang, W.B., et al. (2012). Rett syndrome induced pluripotent stem cell-derived neurons reveal novel neurophysiological alterations. Mol Psychiatry 17:1261–1271. Germain, N.D., Chen, P.F., et al. (2014). Gene expression analysis of human induced pluripotent stem cell-derived neurons carrying copy number variants of chromosome 15q11-q13.1. Mol Autism 5:44. Gore, A., Li, Z., et al. (2011). Somatic coding mutations in human induced pluripotent stem cells. Nature 471:63–67. Griesi-Oliveira, K., Acab, A., et al. (2015). Modeling non-syndromic autism and the impact of TRPC6 disruption in human neurons. Mol Psychiatry 20:1350–1365. Hashimoto-Torii, K., Torii, M., et al. (2014). Roles of heat shock factor 1 in neuronal response to fetal environmental risks and its relevance to brain disorders. Neuron 82:560–572. Hauberg, M.E., Roussos, P., et al. (2016). Analyzing the role of microRNAs in schizophrenia in the context of common genetic risk variants. JAMA Psychiatry 73: 369–377.
Ho, S.M., Hartley, B.J., et al. (2016). Rapid Ngn2-induction of excitatory neurons from hiPSC-derived neural progenitor cells. Methods 101:113–124. Hoischen, A., Krumm, N., and Eichler, E.E. (2014). Prioritization of neurodevelopmental disease genes by discovery of new mutations. Nat Neurosci 17:764–772. Hou, P., Li, Y., et al. (2013). Pluripotent stem cells induced from mouse somatic cells by small-molecule compounds. Science 341:651–654. Hussein, S.M., Batada, N.N., et al. (2011). Copy number variation and selection during reprogramming to pluripotency. Nature 471:58–62. Kim, K.Y., Hysolli, E., and Park, I.H. (2011). Neuronal maturation defect in induced pluripotent stem cells from patients with Rett syndrome. Proc Natl Acad Sci U S A 108:14169–14174. Kleinman, J.E., Law, A.J., et al. (2011). Genetic neuropathology of schizophrenia: new approaches to an old question and new uses for postmortem human brains. Biol Psychiatry 69:140–145. Krey, J.F., Pasca, S.P., et al. (2013). Timothy syndrome is associated with activity-dependent dendritic retraction in rodent and human neurons. Nat Neurosci 16:201–209. Kriks, S., Shim, J.W., et al. (2011). Dopamine neurons derived from human ES cells efficiently engraft in animal models of Parkinson’s disease. Nature 480:547–551. Lake, B.B., Ai, R., et al. (2016). Neuronal subtypes and diversity revealed by single- nucleus RNA sequencing of the human brain. Science 352:1586–1590. Lancaster, M.A., Renner, M., et al. (2013). Cerebral organoids model human brain development and microcephaly. Nature 501:373–379. Li, X., Zuo, X., et al. (2015). Small-molecule-driven direct reprogramming of mouse fibroblasts into functional neurons. Cell Stem Cell 17:195–203. Li, Y., Wang, H., et al. (2013). Global transcriptional and translational repression in human-embryonic-stem-cell-derived Rett syndrome neurons. Cell Stem Cell 13:446–458. Linden, D.E. (2012). The challenges and promise of neuroimaging in psychiatry. Neuron 73:8–22. Lioy, D.T., Garg, S.K., et al. (2011). A role for glia in the progression of Rett’s syndrome. Nature 475:497–500. Lister, R., Pelizzola, M., et al. (2011). Hotspots of aberrant epigenomic reprogramming in human induced pluripotent stem cells. Nature 471:68–73. Liu, J., Koscielska, K.A., et al. (2012a). Signaling defects in iPSC-derived fragile X premutation neurons. Hum Mol Genet 21:3795–3805. Lu, J., Li, H., et al. (2014). The distribution of genomic variations in human iPSCs is related to replication-timing reorganization during reprogramming. Cell Reports 7:70–78. Ma, H., Morey, R., et al. (2014). Abnormalities in human pluripotent cells due to reprogramming mechanisms. Nature 511:177–183. Madison, J.M., Zhou, F., et al. (2015). Characterization of bipolar disorder patient-specific induced pluripotent stem cells from a family reveals neurodevelopmental and mRNA expression abnormalities. Mol Psychiatry 20:703–717. Maezawa, I., Swanberg, S., et al. (2009). Rett syndrome astrocytes are abnormal and spread MeCP2 deficiency through gap junctions. J Neurosci 29:5051–5061. Maherali, N., Ahfeldt, T., et al. (2008). A high-efficiency system for the generation and study of human induced pluripotent stem cells. Cell Stem Cell 3:340–345. Maherali, N., Sridharan, R., et al. (2007). Directly reprogrammed fibroblasts show global epigenetic remodeling and widespread tissue contribution. Cell Stem Cell 1:55–70. Marchetto, M.C., Belinson, H., et al. (2017). Altered proliferation and networks in neural cells derived from idiopathic autistic individuals. Mol Psychiatry 22:820–835. Marchetto, M.C., Carromeu, C., et al. (2010). A model for neural development and treatment of rett syndrome using human induced pluripotent stem cells. Cell 143:527–539. Mariani, J., Coppola, G., et al. (2015). FOXG1-dependent dysregulation of GABA/glutamate neuron differentiation in autism spectrum disorders. Cell 162:375–390.
70 •S. E merging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford University Press USA - OSO, T 2018. 07:33:44.
Mariani, J., Simonini, M.V., et al. (2012). Modeling human cortical development in vitro using induced pluripotent stem cells. Proc Natl Acad Sci U S A 109:12770–12775. Maroof, A.M., Keros, S., et al. (2013). Directed differentiation and functional maturation of cortical interneurons from human embryonic stem cells. Cell Stem Cell 12:559–572. Mayshar, Y., Ben-David, U., et al. (2010). Identification and classification of chromosomal aberrations in human induced pluripotent stem cells. Cell Stem Cell 7:521–531. Mekhoubad, S., Bock, C., et al. (2012). Erosion of dosage compensation impacts human iPSC disease modeling. Cell Stem Cell 10:595–609. Mertens, J., Marchetto, M.C., et al. (2016). Evaluating cell reprogramming, differentiation and conversion technologies in neuroscience. Nat Rev Neurosci 17:424–437. Mertens, J., Paquola, A.C., et al. (2015a). Directly reprogrammed human neurons retain aging-associated transcriptomic signatures and reveal age-related nucleocytoplasmic defects. Cell Stem Cell 17:705–718. Mertens, J., Wang, Q.W., et al. (2015b). Differential responses to lithium in hyperexcitable neurons from patients with bipolar disorder. Nature 527:95–99. Miller, J.A., Ding, S.L., et al. (2014). Transcriptional landscape of the prenatal human brain. Nature 508:199–206. Miller, J.D., Ganat, Y.M., et al. (2013). Human iPSC-based modeling of late-onset disease via progerin-induced aging. Cell Stem Cell 13:691–705. Nageshappa, S., Carromeu, C., et al. (2016). Altered neuronal network and rescue in a human MECP2 duplication model. Mol Psychiatry 21:178–188. Nazor, K.L., Altun, G., et al. (2012). Recurrent variations in DNA methylation in human pluripotent stem cells and their differentiated derivatives. Cell Stem Cell 10:620–634. Nicholas, C.R., Chen, J., et al. (2013). Functional maturation of hPSC- derived forebrain interneurons requires an extended timeline and mimics human neural development. Cell Stem Cell 12:573–586. O’Donnell, W.T., and Warren, S.T. (2002). A decade of molecular studies of fragile X syndrome. Annu Rev Neurosci 25:315–338. O’Shea, K.S., and McInnis, M.G. (2015). Induced pluripotent stem cell (iPSC) models of bipolar disorder. Neuropsychopharmacology 40:248–249. Okabe, Y., Takahashi, T., et al. (2012). Alterations of gene expression and glutamate clearance in astrocytes derived from an MeCP2-null mouse model of Rett syndrome. PLoS One 7:e35354. Pak, C., Danko, T., et al. (2015). Human neuropsychiatric disease modeling using conditional deletion reveals synaptic transmission defects caused by heterozygous mutations in NRXN1. Cell Stem Cell 17:316–328. Pang, Z.P., Yang, N., et al. (2011). Induction of human neuronal cells by defined transcription factors. Nature 476:220–223. Pasca, A.M., Sloan, S.A., et al. (2015). Functional cortical neurons and astrocytes from human pluripotent stem cells in 3D culture. Nat Methods 12:671–678. Pasca, S.P., Portmann, T., et al. (2011). Using iPSC-derived neurons to uncover cellular phenotypes associated with Timothy syndrome. Nat Med 17:1657–1662. Paulsen Bda, S., de Moraes Maciel, R., et al. (2012). Altered oxygen metabolism associated to neurogenesis of induced pluripotent stem cells derived from a schizophrenic patient. Cell Transplant 21:1547–1559. Phelan, K., and Betancur, C. (2011). Clinical utility gene card for: deletion 22q13 syndrome. Eur J Hum Genet 19:4. Porteous, D.J., Millar, J.K., et al. (2011). DISC1 at 10: connecting psychiatric genetics and neuroscience. Trends Mol Med 17:699–706. Qian, X., Nguyen, H.N., et al. (2016). Brain- region- specific organoids using mini- bioreactors for modeling ZIKV exposure. Cell 165:1238–1254. Rabaneda, L.G., Robles-Lanuza, E., et al. (2014). Neurexin dysfunction in adult neurons results in autistic-like behavior in mice. Cell Reports 8:338–346. Rajesh, D., Dickerson, S.J., et al. (2011). Human lymphoblastoid B-cell lines reprogrammed to EBV-free induced pluripotent stem cells. Blood 118:1797–1800.
Ripke, S., O’Dushlaine, C., et al. (2013). Genome- wide association analysis identifies 13 new risk loci for schizophrenia. Nat Genet 45:1150–1159. Ripke, S., Sanders, A.R., et al. (2011). Genome-wide association study identifies five new schizophrenia loci. Nat Genet 43:969–976. Robicsek, O., Karry, R., et al. (2013). Abnormal neuronal differentiation and mitochondrial dysfunction in hair follicle-derived induced pluripotent stem cells of schizophrenia patients. Mol Psychiatry 18:1067–1076. Ruiz, S., Diep, D., et al. (2012). Identification of a specific reprogramming- associated epigenetic signature in human induced pluripotent stem cells. Proc Natl Acad Sci U S A 109:16196–16201. Ruiz, S., Gore, A., et al. (2013). Analysis of protein-coding mutations in hiPSCs and their possible role during somatic cell reprogramming. Nat Commun 4:1382. Sandoe, J., and Eggan, K. (2013). Opportunities and challenges of pluripotent stem cell neurodegenerative disease models. Nat Neurosci 16:780–789. Schizophrenia Working Group of the Psychiatric Genomics Consortium. (2014). Biological insights from 108 schizophrenia-associated genetic loci. Nature 511:421–427. Schlaeger, T.M., Daheron, L., et al. (2015). A comparison of non- integrating reprogramming methods. Nat Biotechnol 33:58–63. Shcheglovitov, A., Shcheglovitova, O., et al. (2013). SHANK3 and IGF1 restore synaptic deficits in neurons from 22q13 deletion syndrome patients. Nature 503:267–271. Sheridan, S.D., Theriault, K.M., et al. (2011). Epigenetic characterization of the FMR1 gene and aberrant neurodevelopment in human induced pluripotent stem cell models of fragile x syndrome. PLoS One 6:e26203. Shi, Y., Kirwan, P., et al. (2012). Human cerebral cortex development from pluripotent stem cells to functional excitatory synapses. Nat Neurosci 15:477–486:S471. Son, E.Y., Ichida, J.K., et al. (2011). Conversion of mouse and human fibroblasts into functional spinal motor neurons. Cell Stem Cell 9:205–218. Studer, L., Vera, E., and Cornacchia, D. (2015). Programming and reprogramming cellular age in the era of induced pluripotency. Cell Stem Cell 16:591–600. Suzuki, I.K., and Vanderhaeghen, P. (2015). Is this a brain which I see before me? Modeling human neural development with pluripotent stem cells. Development 142:3138–3150. Tabar, V., and Studer, L. (2014). Pluripotent stem cells in regenerative medicine: challenges and recent progress. Nat Rev Genet 15:82–92. Takahashi, K., Tanabe, K., et al. (2007). Induction of pluripotent stem cells from adult human fibroblasts by defined factors. Cell 131:861–872. Tchieu, J., Kuoy, E., et al. (2010). Female human iPSCs retain an inactive X chromosome. Cell Stem Cell 7:329–342. Thomson, J.A., Itskovitz-Eldor, J., et al. (1998). Embryonic stem cell lines derived from human blastocysts. Science 282:1145–1147. Tian, Y., Voineagu, I., et al. (2014). Alteration in basal and depolarization induced transcriptional network in iPSC derived neurons from Timothy syndrome. Genome Med 6:75. Topol, A., Tran, N.N., and Brennand, K.J. (2015). A guide to generating and using hiPSC derived NPCs for the study of neurological diseases. JoVE:e52495. Topol, A., Zhu, S., et al. (2016). Dysregulation of miRNA-9 in a subset of schizophrenia patient-derived neural progenitor cells. Cell Rep 15:1024–1036. Urbach, A., Bar-Nur, O., et al. (2010). Differential modeling of fragile X syndrome by human embryonic stem cells and induced pluripotent stem cells. Cell Stem Cell 6:407–411. Vadodaria, K.C., Mertens, J., et al. (2016). Generation of functional human serotonergic neurons from fibroblasts. Mol Psychiatry 21:49–61. Velasco, I., Salazar, P., et al. (2014). Concise review: Generation of neurons from somatic cells of healthy individuals and neurological patients through induced pluripotency or direct conversion. Stem Cells 32:2811–2817. Wang, J.L., Shamah, S.M., et al. (2014). Label-free, live optical imaging of reprogrammed bipolar disorder patient-derived cells reveals a functional correlate of lithium responsiveness. Trans Psychiatry 4:e428. Wen, Z., Nguyen, H.N., et al. (2014). Synaptic dysregulation in a human iPS cell model of mental disorders. Nature. 515:414–418.
5. AS.pplication ofUniversity S temPress C ells to 2018. P sychiatry Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford USA - OSO, 07:33:44.
Wernig, M., Meissner, A., et al. (2007). In vitro reprogramming of fibroblasts into a pluripotent ES-cell-like state. Nature 448:318–324. Xu, Z., Jiang, H., et al. (2016). Direct conversion of human fibroblasts to induced serotonergic neurons. Mol Psychiatry 21:62–70. Yi, F., Danko, T., et al. (2016). Autism-associated SHANK3 haploinsufficiency causes Ih channelopathy in human neurons. Science. 352:aaf2669. Yoo, A.S., Sun, A.X., et al. (2011). MicroRNA-mediated conversion of human fibroblasts to neurons. Nature 476:228–231. Yoon, K.J., Nguyen, H.N., et al. (2014). Modeling a genetic risk for schizophrenia in iPSCs and mice reveals neural stem cell deficits associated with adherens junctions and polarity. Cell Stem Cell 15:79–91. Yu, D.X., Di Giorgio, F.P., et al. (2014). Modeling hippocampal neurogenesis using human pluripotent stem cells. Stem Cell Rep 2:295–310.
Yu, J., Vodyanik, M.A., et al. (2007). Induced pluripotent stem cell lines derived from human somatic cells. Science 318:1917–1920. Zeisel, A., Munoz-Manchado, A.B., et al. (2015). Brain structure. Cell types in the mouse cortex and hippocampus revealed by single-cell RNA-seq. Science 347:1138–1142. Zhao, D., Lin, M., et al. (2015). MicroRNA profiling of neurons generated using induced pluripotent stem cells derived from patients with schizophrenia and schizoaffective disorder, and 22q11.2 Del. PLoS One 10:e0132387. Zhang, Y., Pak, C., et al. (2013). Rapid single-step induction of functional neurons from human pluripotent stem cells. Neuron 78:785–798. Zhang, Y., Sloan, S.A., et al. (2016). Purification and characterization of progenitor and mature human astrocytes reveals transcriptional and functional differences with mouse. Neuron 89:37–53.
72 •S. E merging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford University Press USA - OSO, T 2018. 07:33:44.
6. OPTOGENETICS AND RELATED TECHNOLOGIES FOR PSYCHIATRIC DISEASE RESEARCH C U R R E N T S TAT U S A N D C H A L L E N G E S
Lief E. Fenno and Karl Deisseroth
INTRODUCTION Studying intact systems with simultaneous local precision and global scope is a fundamental challenge in biology. This familiar tradeoff leads to important conceptual and experimental difficulties in psychiatric disease research and indeed throughout the study of complex biological systems. Part of a solution may arise from the technology of optogenetics: the combination of genetic and optical methods to achieve gain-or loss-of-function of temporally defined events in specific cells embedded within intact living tissue or organisms (Deisseroth. 2010, 2012, 2015; Deisseroth et al., 2006; Fenno et al., 2011; Rajasethupathy et al., 2016; Scanziani and Hausser, 2009). Such precise causal control within the functioning intact system can be achieved via introduction of genes that confer to cells both light-detection capability and specific effector function. For example, microbial opsin genes can be expressed in mammalian neurons to mediate millisecond-precision and reliable elicitation or inhibition of action potential firing in response to light pulses, while hybrid opsin-receptor proteins called optoXRs can recruit defined biochemical signaling pathways in response to light (Figure 6.1) (Yizhar et al., 2011a; Zhang et al., 2011). A broad array of optogenetic tool variants and neuroscience applications have driven the wide adoption of optogenetics as a standard reagent in neuroscience (Deisseroth, 2015). This approach has now been used to control neuronal activity in a wide range of organisms, resulting in insights into fundamental aspects of circuit function as well as circuit dysfunction and treatment in pathological states (Deisseroth, 2012; Deisseroth et al., 2015; Rajasethupathy et al., 2016; Tye and Deisseroth, 2012). The precise manipulation enabled by optogenetics underpins basic neuroscience efforts outlined by national and international efforts to discover the biological underpinnings of neuropsychiatric disease (e.g., the U.S. BRAIN initiative, see Bargmann et al., 2014; the European Human Brain Project, see Consortium, 2012). The wide utility of optogenetic tools is apparent in recent translational efforts to treat human central nervous system disease directly (use of ChR2 in human patients; Clinical Trial NCT02556736) and indirectly (optogenetics-g uided use of TMS in humans
with cocaine addiction; see Ferenczi and Deisseroth, 2016). Here we review the current state of optogenetics for neuroscience and psychiatry and address the evolving challenges and future opportunities. Despite rapid growth, wide scope of applications, and progress in addressing experimental caveats in recent years, many questions and opportunities remain. B AC KG R O U N D : C U R R E N T F U N C T I O N A L I T Y O F TO O L S Diverse and elegant mechanisms have evolved to enable organisms to harvest light for survival functions. For example, opsin genes encode 7-transmembrane (TM) proteins that (when bound to the small organic chromophore all-trans retinal) constitute light-sensitive rhodopsins, which are found across all kingdoms of life (Fenno et al., 2011). Many prokaryotes employ these proteins to control proton gradients and to maintain membrane potential and ionic homeostasis, and many motile microorganisms have evolved opsin-based photoreceptors to modulate flagellar motors and thereby direct phototaxis toward environments with optimal light intensities for photosynthesis. Owing to their structural simplicity (both light-sensing and effector domains are encoded within a single gene) and fast kinetics, microbial opsins can be treated as precise and modular photosensitization components for introduction into non–light sensitive cells to enable rapid optical control of specific cellular processes. For example, most channelrhodopsins (Figure 6.1a,b) such as ChR2 induce nonselective cationic photocurrents in response to illumination, resulting in net depolarization and spike firing in neurons, first demonstrated in 2005 (Boyden et al., 2005). Halorhodopsins (Figure 6.1a–c) pump chloride, and bacteriorhodopsin and related opsins pump protons in response to illumination, both hyperpolarizing neurons (Chow et al., 2010; Zhang et al., 2007, 2011; reviewed in Mattis et al., 2012; Yizhar et al., 2011a). Many other non-opsin classes of naturally occurring protein have been explored as well, including flavin chromophore- utilizing light- activated adenylyl cyclases as well as artificially engineered systems in which light-sensation modules become physically linked to effector
7 3 USA - OSO, 2018. Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press 07:33:44.
07:33:44.
Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press USA - OSO, 2018.
ChR2
Nucleus accumbens optrode recording
opto-d1r
mPFC intracellular pyramidal neuron recording
iC++
M1 motor cortex optrode recording
NpHR
Dentate gyrus optrode recording
H+
K+ Na+
1s
K+
H+ K+ K+ H+
473 nm
H+
475 nm
K+
K+
ChR2
473 nm
560 nm
Cl–
NpHR
Cl–
Cl–
Cl–
Cl–
Cl–
Cl–
Cl–
Cl–
Cl–
Cl– Cl–
Cl– Cl–
Cl–
Cl– Cl–
iC++
Cl–
Cl–
Cl–
Cl–
Cl–
Cl– Cl–
(c)
Cl– Cl–
Cl–
Cl–
Gq
0
25
50
75
100
0 mW
iC++
DAT-Cre mouse
Gs
iC++
[cAMP]
Gi
Arch3.0
Gq
[cAMP]
light on
[cAMP]
Gs
CNO
Gi
CNO CNO
5 mW
light off
[IP3 ] [DAG]
DREADD
0.5 mW Light power
eNpHR3.0
Arch3.0
eNpHR3.0
[cAMP]
optical fiber
[IP3 ] [DAG]
Opto-XR
CNO
CNO
Optogenetics a) Most channelrhodopsins, such as ChR2, induce nonselective cationic photocurrents in response to illumination, resulting in a net depolarization and spike firing in neurons. One exception to this is the synthetic channelrhodopsin iC++, that has been designed to pass only chloride, thereby resulting in hyperpolarization and shunting currents, thereby preventing spiking in neurons when it is activated. Ion pumps, such as halorhodopsins (NpHR) conduct chloride and bacteriorhodopsin and related opsins conduct protons (not shown) in response to illumination, both hyperpolarizing neurons. The optoXRs and DREADDs are chimeric proteins that elicit biochemical signal cascades in response to either illumination (opto-XR) or designer drugs, such as clozapine-N-oxide (CNO; DREADDs). The specific biochemical cascade is determined by the source of the intracellular loops. b) Examples of neurophysiological modulation by optogenetic tools. ChR2 and the opto-XR family member opto-D1r increase in vivo neuronal activity in response to light, while NpHR and iC++ decrease spontaneous in vivo (NpHR) or induced in vitro (ic++) spiking. c) An example of the behavioral modulation achievable with these tools is exemplified by conditioned place aversion induced by inhibition of dopaminergic neurons of the ventral tegmental area (top) by iC++ (blue), eNpHR3.0 (green), or Arch3.0 (red). The degree of aversive learning is dependent on light power (bottom). Panel a adapted from Fenno et al., 2011. Panel b adopted from Berndt et al., 2016; Gradinaru et al., 2010; Gunaydin et al., 2014. Panel c from Berndt et al., 2016.
Figure 6.1
(b)
intracellular
extracellular
Na+ Na+ Na+ Na+ Ca+ Na+ Na+ Na+ Na+ Na+ Na+ Na+ Ca+ Ca+ + H+ H
% time in light paired side
(a)
modules (Airan et al., 2009; Cosentino et al., 2015; Gulyani et al., 2011; Janovjak et al., 2010; Moglich and Moffat 2007; Stierl et al., 2011; Wu et al., 2009). The genomically identified are complemented by an ever- increasing portfolio of derivatives designed to manipulate peak wavelength, current magnitude, and inactivation time constant (tauoff). Tauoff is an intrinsic property that describes the time taken for an opsin to spontaneously relax from the ion-conducting state to the nonconducting state after the cessation of light. The tauoff of ChR2 is ~12 ms, whereas (for example) that of the mutant ChR2-H134R is approximately doubled (Mattis et al., 2012); this property in part determines the maximum frequency at which a neuron may produce precisely timed light-initiated action potentials (Gunaydin et al., 2010; Mattis et al., 2012). Indeed, an opportunity was seen to speed up optogenetic control function by modulating tauoff; destabilizing the open state of the channel could lead to a more rapid spontaneous reversion to the nonconducting state of ChR2 following light cessation, thereby increasing the frequency ceiling for driving neurons—an especially important consideration for some classes of fast-spiking inhibitory interneurons, including those expressing parvalbumin (PV). By applying observations in the bacteriorhodopsin literature to ChR2 based on the high degree of homology among type I rhodopsins, it was found that shifting a single amino acid residue was sufficient to approximately halve the tauoff (ChETA; see Gunaydin et al., 2010; Mattis et al., 2012), thereby increasing the top high-fidelity frequency to at least 200 Hz and increasing overall performance. A separate creative approach to creating a channelrhodopsin with a rapid tauoff arose from chimeras of ChR1 and ChR2 (ChEF/ChIEF) (Figure 6.2). Opsins optimized for rapid closure and high frequency stimulation are complemented by ChR2 variants designed to remain in the “active” ion-conducting state and induce prolonged depolarization after light cessation. The engineering approach to design these proteins also took advantage of homology between ChR2 and bacteriorhodopsin to produce variants that stabilize, as opposed to destabilize, the active retinal conformer. These “step-function opsins” (SFO) allow precise induction and inactivation of a depolarizing current “step” into the population of neurons, the duration of which is dependent upon the particular mutation (C128S: 100s, Berndt et al., 2009; D156A: 6.9 min, Bamann et al., 2008; C128S/D156A: 29 min [Stabilized Step Function Opsins/ SSFO], Yizhar et al., 2011b) (Figure 6.2). As these are derivatives of ChR2, they are activated by blue (470 nm) light. This depolarizing step can then be terminated with yellow light (590 nm), which drives the opsin to its resting state. In the case of SSFO, the most stable of the SFOs, the depolarization step occurs without crossing the sodium channel activation threshold, which has the useful effect of modestly sensitizing a population of neurons to incoming excitatory input. One additional benefit of an extended tauoff is that the cell expressing the protein may effectively act as a photon integrator: in the case of SSFO, once a channel has been activated it remains open for a period approximately 150,000 times longer than native ChR2 (Yizhar et al., 2011b). The implication of cellular photon integration is that the total number of photons
needed to induce a maximal photocurrent in the cell may be spread over a longer period of time (in contrast to stimulation parameters of ChR2 that require a high density of photons in order to activate enough channels to move the neuron beyond action potential threshold). In the context of behavioral neuroscience, this property has been exploited to allow for extracerebral light delivery, obviating the need to implant fiber optic light delivery devices into animals for behavioral trials at depths of at least 2.8 mm (Yizhar et al., 2011b). A second dimension into which considerable engineering resources have been invested is “red-shifting” the maximum excitation wavelength of channelrhodopsins (Figure 6.2). A tool that is sufficiently red-activated might be able to be modulated independently of blue light–activated ChR2, thus allowing for the manipulation of multiple, independent populations of neurons within the same space (Klapoetke et al., 2014; Yizhar et al., 2011b; Zhang et al., 2008)(Figure 6.2a–d). VChR1, the first green-activated ChR described, does not produce sufficient photocurrents to reliably drive suprathreshold events in neural populations. The first red-shifted opsin with currents sufficient to reliably drive neuron activity were not derived from any one organism, but arose as a chimera between ChR1 and VChR1 (C1V1; Figure 6.2c, d). Resulting currents were significantly larger than for ChR2 (Mattis et al., 2012; Yizhar et al., 2011b), and action potentials may be elicited by 630nm red light (Yizhar et al., 2011b). C1V1 was shown to independently modulate cell bodies and terminals in the same tissue as neurons expressing ChR2 (experiments conducted in brain slice, in anesthetized (“optrode”) recordings in vivo, and in awake, behaving animals (Yizhar et al., 2011b). Since the development of C1V1, engineering efforts (Lin et al., 2013) and genomic screens (Klapoetke et al., 2014) have expanded the number of opsins activated by red (630 nm) light. Independent modulation of multiple populations of neurons is of immediate utility in understanding the dynamics of circuits; further optimization of one red-light- activated ChR for use in vivo (termed bReaChES; Figure 6.2e, f ) was recently combined with green-light activated calcium indicator GCaMP6m to stimulate long- range, presynaptic terminals with red light while simultaneously imaging postsynaptic calcium transients with green light, in order to examine synaptic strength before and after fear conditioning, revealing rapid reorganization of how top-down cortical circuit elements recruit hippocampal memory representations (Rajasethupathy et al., 2015). In summary, the explosion of diversity in channelrhodopsins, mutational variants, and chimeras since the original introduction of ChRs into neurons in 2005 has included the engineering of tools differently specialized for increased photocurrent, for driving action potentials at high frequencies, for depolarizing neurons for extended periods in the absence of direct action potential generation, and for combinatorial control via red-shifting of excitation wavelength. However, while using channelrhodopsins to control the excitability of a population of neurons with fine temporal resolution allows neuroscientists to ask if the activity of a genetically and/or anatomically specified population of neurons is sufficient to cause a given outcome, the reverse side of this experimental
6. O S. p togenetics R elated T echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford and University Press USA - OSO, 2018. 07:33:44.
(a)
400
500
600
R-CaMP2
ex
GCaMP6
ex
700
em
em
ChR2 NpHR iC++
% max response
100
bReaChES opto-XR
50
0
400
500 wavelength (nm)
600
Photocurrent (pA)
(b) PYR
ChR2 & NpHR 100 mV
500 ms
(c)
1000
590 nm 445 nm
500
0
PYR cell expressing C1V1
700
400
500 600 wavelength (nm)
(d) PYR
VB (ChR2)
20 mV
VB
0.5 s
nRT cell
TC
Cortex (C1V1) PYR
CT
5Hz 560 nm
CT (561 nm) TC (405 nm)
5Hz 405 nm
PYR cell expressing ChR2(H134R)
PYR
20 mV 0.5s 5Hz 405nm 5Hz 560nm
(e)
–70 mV
(f) DA
5
* *
Reward
3
*
0
Tail shock
–3
camera reward
reward trial
0
1s
470 nm 594 nm
*
bREACH stim 470 nm control
Time
0.5 s
mean response size (% df/F)
410 nm
% dF/F
10% dF/F
VTA (DA) R-CaMP2 VTA (non-DA) GCaMP6m
bReaChES & GCaMP6f 5% dF/F
560 nm 470 nm
% dF/F
R-CaMP2 GCaMP6m
25 20 15 10 5 0
* 0 1 2 light power (mW)
Combinatorial Optogenetics a) Approximate action spectra of genetically encoded calcium sensors GCaMP and R-CaMP (bars, top) and certain optogenetic tools (line plots, bottom) important for experiments using more than one light-activated tool simultaneously. Many other opsins exist, not all shown for the sake of clarity; other opsins are reviewed elsewhere (e.g., Grosenick et al., 2015) and include the proton-conducting variety (proton pumps such as eArch3.0 and highly proton-conducting channelrhodopsins such as DChR1 and Chrimson are omitted here since optically- elicited proton flux has been shown to cause mixed-valence and non-cell autonomous effects; Ferenczi et al., Scientific Reports 2016; Mahn et al., 2016). b) Single neurons expressing both depolarizing opsin ChR2 and hyperpolarizing opsin NpHR can be excited with trains of blue light and inhibited with pulses of yellow light, even simultaneously (left); wavelength and light intensity must be carefully chosen, as the spectra of these two opsins is partially overlapping (right). c) The development of red-shifted, excitatory opsins, such as C1V1 (whose spectra is similar to bReaChES; left) enables separate channels of excitatory control for modulation of different neurons, within the same space. d) Expression of ChR2 (activated with 405 nm purple light) Figure 6.2
Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press USA - OSO, 2018. 07:33:44.
coin is to ask if the activity of these elements is necessary for the outcome. To obtain direct evidence of necessity, a tool is required that is able to silence the activity of a targeted population of neurons while leaving others unaffected. The light-activated halorhodopsin (HR) is an electrogenic pump producing inward chloride flux that can hyperpolarize and thereby inhibit neurons (e.g., the HR from Natronomonas pharaonis, or NpHR; reviewed in Zhang et al., 2011; Figure 6.1a–c). Optogenetic function of proton efflux pumps that can hyperpolarize neurons have since also been described (reviewed in Mattis et al., 2012; Zhang et al., 2011); however, these cause local environmental acidification that has been shown to drive action- potential- independent vesicle fusion resulting from pH-dependent calcium flux and a potential paradoxical increase in synaptic transmission when attempting to silence neurons (Mahn et al., 2016). In addition to limitations in the number of naturally sourced inhibitory opsins, and unpredictable effects resulting from changes in local pH, optogenetic ion-pumping tools transport a maximum of one ion across the cell membrane per photon absorbed, limiting their efficiency in light-scattering brain tissue. Because inhibitory opsins are true ion pumps, the application of engineering approaches used to diversify the excitatory channelrhodopsin toolbox has been limited. High- resolution crystal structures now available for all the major opsin classes (e.g., Kolbe et al., 2000), including most recently channelrhodopsin (ChR; Kato et al., 2012) have been of enormous value, not only for enhancing understanding of microbial opsin-based channels but also for guiding optogenetics in the generation of variants with novel function related to spectrum, selectivity, and kinetics, most recently to create a new class of chloride-conducting ChR (Berndt et al., 2014; Wietek et al., 2014) (Figure. 6.1a– c). Chloride- conducting channelrhodopsins inhibit neuron firing through a combination of membrane hyperpolarization and decreasing membrane resistance by up to 50% (shunting inhibition). Since these initial efforts, the evolution of inhibitory ChRs has largely followed that of their excitatory relatives, albeit on an accelerated timeline. This includes variants with improved photocurrents, further hyperpolarized reversal potentials, increased efficiency (Berndt et al., 2016) and the discovery of naturally occurring light-activated anion channels (Govorunova et al., 2015).
In addition to optically modulated mediators of neuronal membrane potential, a class of tools for optical control of biochemical signaling cascades (the optoXRs) now exists for temporally precise manipulation of G-protein coupled receptor (GPCR) signaling cascades (Figure 6.1a,b). These chimeric proteins are composed of the light-sensing extracellular domain of the type II mammalian rhodopsin and the intracellular domain of a given GPCR, for instance, alpha-1 and beta-2 adrenergic receptors (Gq-and Gs-coupled, respectively; Airan et al., 2009; Kim et al., 2005), 5-HT1a (Gi/o-coupled; Oh et al., 2010), D1r (Gs-coupled; Gunaydin et al., 2014), and MOR (Gi/o-coupled; Siuda et al., 2015) and precisely activate native signaling pathways in response to light. These receptors are activated by 500nm light and are useful for control of biochemical signaling both in vivo (Airan et al., 2009; Gunaydin et al., 2014; Siuda et al., 2015) and in vitro (Airan et al., 2009; Gunaydin et al., 2014; Kim et al., 2005; Oh et al., 2010; Siuda et al., 2015). A related but nonoptical approach combines GPCR- effector domains with extracellular-receptor domains designed to bind and be activated by exogenously introduced ligands; particularly since they do not occupy optical bandwidth, these can act as a complementary set of tools for basic neuroscience and are known as DREADDs (Designer Receptors Exclusively Activated by Designer Drugs; reviewed in Urban and Roth 2015; Figure 6.1a) or PSAMs (Pharmacologically Selective Activator Molecules; Magnus et al., 2011). These are activated by ligands introduced via the venous circulation that are able to cross the blood–brain barrier and are thought to be otherwise innocuous, allowing for the chronic increase or decrease in activity of genetically defined neural populations. As a complementary method to optogenetics, these “chemogenetic” approaches do not require chronically implanted hardware (such as fiber optic or micro-LED light-delivery components) and allow for uniform exposure of the activator (membrane-bound channel) to its ligand (an experimental consideration with optogenetics, as photon density drops off to the fourth power with distance and has a wavelength- dependent scattering component, especially important when recruiting neurons across large volumes of brain parenchyma). These advantages come at the expense of the temporal precision, magnitude of depolarization/hyperpolarization (and thus strength of manipulation), reliable circuit targeting for
in thalamocortical VB neurons and C1V1 (activated with 561 nm green light) in corticothalamic pyramidal neurons was used to probe the importance of timing of these two convergent inputs in driving spikes in reticulothalamic (nRT) neurons—important in understanding the physiological underpinning of certain types of epilepsy and impossible without the use of optogenetics. e) In addition to separate channels of control, spectral engineering has been applied to read-out tools, such as genetically encoded calcium sensors, in order to allow for simultaneous recording of multiple populations of neurons within the same space, such as using red-light activated R-CaMP2 in dopaminergic (DA) and green-light activated GCaMP6 in non-dopaminergic (non-DA) neurons of the ventral tegmental area (VTA; left). The change in fluorescence (dF/F) of these populations during a rewarding task (right top) and aversive task (right bottom) revealed context-dependent behavior that differs based on genetic signature. f ) Optogenetic tools may be combined with calcium sensors in order to independently control and read-out activity of neurons within the same space in order to tune optogenetic stimulation to mimic natural neuron responses. Here, red-light activated bReaChES and green-light activated GCaMP were simultaneously expressed in VTA DA neurons and activity was both read-in and read-out through a single fiberoptic implant while the animal was either given a reward or had VTA DA activity optically driven using bReaChES (left). GCaMP6 calcium signals of natural neuron dynamics during reward (light blue) were similar in magnitude to those acquired with 0.5 mW of yellow light, but less than with higher intensities of yellow light (middle, right). The 470 nm blue light used for calcium imaging with GCaMP caused negligible cross-stimulation of bReaChES. Panel a adapted from Airan et al., 2009; Berndt et al., 2016; Chen et al., 2013b; Inoue et al., 2015; Rajasethupathy et al., 2015. Panels b adapted from Gradinaru et al., 2010; panels c and d adapted from Yizhar et al., 2011b; panels e and f adapted from Kim et al., 2016a.
6. O S. p togenetics R elated T echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford and University Press USA - OSO, 2018. 07:33:44.
elements defined by origin and target, and ability to manipulate neurons at the subcellular (synapse) level, all inherent to optogenetic tools. Maturation of the optogenetic toolbox has been paralleled by advances in molecular delivery and targeting strategies. Refined approaches to expressing optogenetic tools in specific neuron subtypes is a crucial advancement, as few relevant cell types can be specified by only a single descriptor such as cell body location, projection target, or activity of one promoter/enhancer region. A single-virus approach dependent on multiple recombinases allowing for flexible Boolean logic targeting based on genetic or connectivity parameters (INTRSECT; see Fenno et al., 2014; Figure 6.4) has been successfully applied to pinpoint key neural circuit components salient to anxiety (Marcinkiewcz et al., 2016; Tovote et al., 2016; see detailed description of these experiments) and habit formation (Gremel et al., 2016). This approach combines the activity of independent recombinases, synthetic introns, and transgenic animals to refine neuron targeting based on logical combinations of genetic or projection criteria (e.g., neurons that express gene A AND project to downstream region B, or neurons that express gene A AND NOT gene B; see Figure 6.4). As these descriptions show, the experimental potential of optogenetics has triggered a surge of genome prospecting and molecular engineering to expand the repertoire of tools and generate new functionality, in turn catalyzing further mechanistic studies of microbial proteins. The high- resolution crystal-structural insights have been used to help guide the assembly of light-sensitive modules, together with effector modules, into artificial proteins to solve critical deficiencies in the optogenetic toolbox. CURRENT NEUROSCIENCE A PP L I C AT I O N S A N D DISEASE MODELS This diversity of optogenetic tool function will be important for making significant headway in our understanding both of normal brain function and of dysfunctional processes in neuropsychiatric disease (for example, many disease states may relate to impaired interaction of multiple distinct cell or projection types, pointing to the experimental value of achieving multiple- color excitation and multiple- color inhibition optogenetically within the same living mammalian brain) (Deisseroth, 2012; Rajasethupathy et al., 2016; Tye and Deisseroth, 2012). Indeed, recent years have already seen a swiftly growing wave of applications of optogenetics to questions in neuropsychiatric disease, with the deployment of millisecond-precision optical excitation or inhibition of specific circuit elements within behaving mammals. Overall this line of work is very timely at the societal level; psychiatric disease represents the leading cause of disability worldwide, but major pharmaceutical companies are withdrawing from developing new treatments, and many are shutting down psychiatry programs—a situation with major medical, social, and economic implications. Reasons cited include the lack of
neural circuit-level understanding of symptom states, which impairs identification of final common pathways for treatment and hobbles development of predictive animal models. Identification of simplifying hypotheses and unifying theories by optogenetic or other means is one of the most pressing needs and exciting avenues of research into neurological and psychiatric disease. Optogenetic technology now exists in a special relationship with psychiatry, because one of the unique and most versatile features of optogenetics—modulation of defined neural projections by fiber-optic-based “projection targeting,” in which cells are transduced with opsin in region A but illumination is delivered in region B where only a subset of the expressing cells from A send axonal projections (Figure 6.3; Gradinaru et al., 2007, 2009, 2010; Petreanu et al., 2009; Stuber et al., 2011; Tye et al., 2011; Yizhar et al., 2011a)—is well-aligned with what may be a core feature of psychiatric disease, namely altered function along pathways of neural communication. The fiber-optic neural interface not only allows this selective recruitment of cells defined by projection target but also overcomes the depth limitations caused by light scattering, and allows access to (and optogenetic control of ) any brain region even in freely moving mammals. This device debuted in 2007 (Aravanis et al., 2007) and was first applied that year (Adamantidis et al., 2007) to address questions relevant to narcolepsy and sleep–wake transitions. Specific activity patterns were played into hypocretin neurons (genetically targeted by use of a cell type–specific promoter that was functional in an injected opsin-bearing viral vector) in the lateral hypothalamus in freely moving mice. Certain patterns but not others were found to favor sleep–wake transitions, providing the first causal understanding of specific activity patterns in well-defined cells underlying mammalian behaviors. The continued development of circuit-and cell type–specific molecular targeting approaches has driven an explosion of studies that identify and describe patterns of activity within defined circuit elements sufficient and necessary to modulate behavior. Dopamine, a neurotransmitter commonly modulated by psychotropic medications, has wide-ranging receptors throughout cortical and subcortical structures but originates from discrete nuclei in the central nervous system, including the ventral tegmental area (VTA) and substantia nigra (SNc). Understanding the role of dopamine in behavioral contexts has benefited from a versatile cell type–targeting approach using Cre-driver lines in which the enzyme Cre-recombinase is expressed across generations as a transgene, only in targeted cells. Cre-dependent viruses are constructed and injected that will therefore express opsin only in the targeted (Cre-expressing) cells (for instance, see Figure. 6.2e,f ). Cre-dependent targeting led to the first control of dopaminergic neurons in freely moving mice (Tsai et al., 2009) via selective opsin expression in tyrosine hydroxylase–expressing neurons in the VTA, to probe reward and conditioning. Since this first study, optogenetic approaches have been combined with activity-dependent imaging and connectivity- dependent optogenetic targeting to delineate that dopaminergic neurons of the VTA are not a homogenous population but have distinct upstream and downstream synaptic partners, which independently modulate reward and
78 •S. E m erging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford University Press USA - OSO,T 2018. 07:33:44.
Injection Site
(a)
Viral Expression
Light Delivery
Virally encoded opsin A
Local Cell Body
Laser A
C B
Single viral injection into B
(b)
A
C
C
B
B
Opsin expression throughout B
Illumination of B cell bodies projecting to A and C Laser
Virally en coded recombinase- or promoterdependent opsin A
Recombinasedependent or promoter-based
A
C B
Single viral injection into mixed population of neurons in B
(c)
A
C
C
B
B
Illumination of B cell bodies and modulation of recombinase- or promoter-expressing cells
Opsin expression only in neurons expressing recombinase or with a ctive promoter in B
Laser
Virally encoded opsin A
Projection
A
C B
Single viral injection into B
(d) A
Opsin expression throughout B
C
A
B
Double viral injection into B and A. Recombinase expressed in A moves transcellularly to cells in B.
(e)
Laser or
A
C
Illumination of B terminals in A but not C Laser
B
Transcellular
C B
Virally en coded recombinasedependent opsin
Virally encoded lectin recombinase
A
C B
C B
Opsin expression in B neurons that project to A
Illumination of B cell bodies or B terminals in A without modulation of C Laser 1
Mixture of virally encoded opsins A
Combinatorial Somata
B
Independent virally-encoded opsins
(f) A
C
A
B
Single mixed viral injection into mixed population of neurons in B
Combinatorial Projection
Laser 2 A
C
C B
Viral injection of spectrally separated opsins into A and C
Opsin expression in B cell bodies according to viral promoters
C B
Precisely temporally separable illumination of mixed neuronal populations in B with two colors of light Laser 1 Laser 2
A
C B
Opsin expression in A and C cell bodies according to viral promoters
A
C B
Illumination of mixed neuronal projections in B activate independent terminals from A and C
In Vivo Optogenetic Targeting Strategies a) Viral targeting of a neuron population based on promoter specificity followed by stimulation of the same area as the injection. b) Viral targeting of a neuron population based on expression of Cre recombinase followed by stimulation of the same area as the viral injection. c) Viral targeting of a neuron population followed by stimulation of a downstream target region; noted that this will likely be a subset of the total population of neurons expressing opsin. d) Dual viral targeting of a downstream population with lectin-recombinase (e.g., WGA- CRE) and upstream injection of Cre-dependent DIO virus followed by stimulation of either the somata or axons of opsin-expressing population. e) Injection of multiple opsins expressed in separate populations within the same space based on promoter or recombinase-mediated specificity followed by multi-wavelength stimulation at the somata. f ) Trans-synaptic or retrograde targeting of axons in two separate locations followed by central multi- wavelength stimulation location to differentially modulate somata of neurons based on their projections. Adapted from Yizhar et al., 2011a. Figure 6.3
Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press USA - OSO, 2018. 07:33:44.
Refined Neuron Targeting with INTRSECT INTRSECT targeting allows for the restricted expression of any genetically encoded payload within cells defined based on multiple genetic or projection-based criteria by combining the activity of Cre and Flp, two independent recombinases that manipulated the direction of DNA sequences, artificial introns, and the starting orientation of the resulting exons. a) ChR2-EYFP, a common fusion of channelrhodopsin-2 and yellow fluorescent protein, here has two artificial introns containing recognition sites for Cre recombinases situated within its coding frame (left). The first and third exon have been reversed and inverted, which prevents expression at baseline (left top). When Cre and Flp are both present (left middle), the exons are rearranged into the proper orientation. The introns are removed during mRNA processing (left bottom), allowing for expression of ChR2-EYFP. The recombinase-dependent reorientation of the exons is a standardized process that is independent of the gene of interest (right). b) This approach allows for the targeting of different cell populations in a Boolean manner (left top) through the simple reorientation of the exon starting direction (left bottom). ChR2-EYFP is used as an example for Cre AND Flp, Cre AND NOT Flp, and Flp AND NOT Cre (right; Cre is blue, Flp is red, ChR2-EYFP is green). ChR2-EYFP expression is restricted to the correct recombinase condition. c, d) This approach has been recently used to dissect fear response circuitry with a degree of resolution not otherwise possible. c) Single recombinase (DIO) dependent expression of ChR2 in glutamatergic neurons of the ventral-lateral periaqueductal gray (vlPAG) in transgenic mice expressing Cre recombinase in this population (left) suggests that these neurons induce fear behaviors, such as freezing, when activated (middle) as well as increase pain tolerance (analgesia; right). d) Injection of a Flp-expressing, retrograde traveling virus into downstream fear behavior circuit magnocellular neurons of the medulla (MC) allows for INTRSECT-dependent expression of ChR2 in only double Cre/Flp positive neurons within the vlPAG, representing neurons that are glutamatergic AND project to MC. This population of neurons continues to drive fear behavior (center) but no longer has an effect on analgesia (right), indicating separate, glutamatergic circuits independently driving these two behavioral effects. Panels a and b adapted from Figure 6.4
Fenno et al., 2014; panels c and d adapted from Tovote et al., 2016.
Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press USA - OSO, 2018. 07:33:44.
aversion (Lammel et al., 2012; Nieh et al., 2016). Further work (Gunaydin et al., 2014) has extended these findings to social behavior, finding that specific dopaminergic projections from the VTA to the nucleus accumbens were necessary, sufficient, and specific for social interaction with novel animals but not with novel objects, providing a new avenue of research or therapeutic intervention in human patients with social dysfunction. Following results that the VTA could be divided into distinct, functional subpopulations, a similar approach has recently found that the SNpc, known widely for its etiological role in Parkinson’s disease, also harbors a functional diversity of dopaminergic neurons that may be divided based on their downstream synaptic partners in the dorsal-lateral or dorsal-medial striatum, which in turn may modulate valence to aversive stimuli and provide important considerations for treatment of neuropsychiatric disease thought to be underpinned by dopaminergic dysfunction (Lerner et al., 2015). Targeting neurons, such as the dopaminergic neurons of the midbrain, using Cre or Flp recombinase, is a versatile approach used for myriad studies, including to control the intriguing parvalbumin or fast-spiking inhibitory neurons (Sohal et al., 2009). Prior pioneering work had shown that these neurons are altered in schizophrenia, and they had long been suggested to be involved in modulating certain kinds of brain rhythmicity such as gamma oscillations, which are also known to be abnormal in schizophrenia. Optogenetic studies were able to define a causal role of these neurons in the modulation of gamma oscillations, which in turn were found to modulate information flow within neocortical circuitry (Sohal et al., 2009). Altered gamma oscillations are also seen in autism, which, like schizophrenia, is known to involve deficits in information processing and social function (although with a markedly different quality). A long-standing hypothesis in the field had been that elevated excitation–inhibition imbalance could give rise to social dysfunction of the kind seen in autism, but the physiology (unlike the genetics) had been difficult to test in causal fashion. Optogenetic interventions were able to directly and causally implicate excitation–inhibition balance changes in setting up abnormal social function as well as giving rise to abnormal information processing and gamma oscillations (Yizhar et al., 2011b) of the kind seen in autism and schizophrenia. Memory deficits (notably in working memory but also in aspects of long-term episodic or declarative memory) are seen in autism and schizophrenia, but more prominently in cognitive impairment and dementia. The persistence of episodic memories is also highly relevant to posttraumatic stress disorder (PTSD) and other anxiety disorders, in which the memory can be a contextual fear memory. Work using optogenetics has now found that long-term contextual fear memories surprisingly involve both hippocampus and neocortex, even in the remote phase (Goshen et al., 2011). The combined use of recently developed, red- shifted excitatory optogenetic tools and fluorescent calcium indicators have furthered understanding of the relationship between cortical and subcortical structures in memory retrieval, with the description of a previously unknown projection from anterior cingulate
cortex to the CA region of hippocampus. This projection is strengthened by learning, and the activity of these sparse neurons leads to widespread and synchronous hippocampal activity (Rajasethupathy et al., 2015). This work may help inform our understanding of PTSD and attempts to ameliorate the debilitating consequences of this disease. Other optogenetics- based studies have explored diverse aspects of fear memory formation and expression in amygdala, hippocampus, neocortex, and other neural circuits in freely moving mammals (Ciocchi et al., 2010; Haubensak et al., 2010; Liu et al., 2012). Optogenetic methods have also been used to probe unconditioned anxiety, and a specific intra-amygdala pathway has been optogenetically resolved that appears to bidirectionally set anxiety expression level in real time as mammals behave (Tye et al., 2011). While the above neocortical and subcortical interventions were able to describe the contribution of genetically or topologically defined neurons to behavior, they are limited in describing, at most, the inputs and outputs of a single component of what are presumably complicated and distributed circuits with multiple regulatory inputs. The maturation of optogenetic tools has been paralleled by molecular and viral targeting approaches (e.g., INTRSECT, described, and the adaptation and modification of neurotropic viruses such as rabies and herpes for monosynaptic, retrograde molecular tool delivery). The combination of these approaches has been used successfully to delineate the identity and role of independent circuit elements regulating conserved behaviors that may underlie psychiatric disease (see Deisseroth, 2015; Fenno et al., 2014; Rajasethupathy et al., 2016 for review). One drawback of current retrograde viruses is limited expression time due to viral toxicity; however, engineering approaches to address this issue are underway (Kim et al., 2016b). This combined recombinase-expressing transgenic mice, optogenetic intersectional delivery, and viral circuit tracing approach was integral to a study from Tovote, Esposito, Luthi, and others (Tovote et al., 2016) describing the genetic identity, anatomic location, and regulatory inputs governing the action of a neural circuit driving fear- and anxiety-related freezing behavior in mice that includes subnuclei of the amygdala, thalamus, and medulla; divisions of the periaqueductal grey (PAG); and the spinal motor neuron pool (Figure 6.4c,d). Their approach to dissecting this circuit involved modulating highly refined neuron populations using depolarizing or hyperpolarizing optogenetic tools in awake, behaving animals, and acute slice preparations and systematically varying single experimental design elements (anatomic location, glutamatergic/ GABAergic/ cholinergic recombinase-expressing transgenic animal, excitatory/inhibitory opsin, viral expression logic gate, or behavioral assay). Initial experiments using glutamatergic-selective Vglut2-Cre transgenic mice with Cre-dependent, depolarizing ChR2 or hyperpolarizing Arch injected in ventral-lateral PAG (vlPAG) found that stimulation of this population of neurons was necessary and sufficient for freezing behavior in mice. ChR2-mediated stimulation of this population of neurons also had a significant analgesic effect, increasing latency to tail withdrawal from hot water.
6. O S. p togenetics R elated T echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford and University Press USA - OSO, 2018. 07:33:44.
To screen for modulatory inputs to this population of neurons, this group injected retrobeads into vlPAG and found a strong projection from the central amygdala (CeA; previously identified as an important modulator of fear and anxiety behavior; see Tye et al., 2011). Using either Vglut2-Cre or GABAergic selective Gad1-Cre mice in combination with genetically selective rabies virus, the group identified a strong inhibitory projection from CeA to GABAergic vlPAG neurons; these in turn were found to synapse onto and inhibit the output vlPAG glutamatergic neurons, thereby delineating three elements of this circuit. To identify downstream components, the group injected genetically specific rabies into the spinal cord motor neuron pool of cholinergic-specific Chat- Cre mice, and an anterograde tracer into vlPAG, finding that these converged on neurons of the magnocellular nucleus of the medulla (MC), thereby identifying five separate circuit components. Interestingly, while validating the vlPAG-MC glutamatergic synapse by combining Vglut2-Cre mice, genetically specific retrograde herpes virus carrying Flp recombinase injected in MC, and INTRSECT ChR2 requiring both Cre AND Flp for expression in vlPAG, the authors found that this subset of vlPAG neurons projecting to MC, while sufficient to drive freezing behavior, did not modulate analgesia, unlike their earlier result using the entire pool of vlPAG glutamatergic neurons and illustrating an experimental result that would not have been possible to obtain without the INTRSECT approach. After detailing five components of the freezing circuit, from amygdala to spinal cord, they last found that the dorsal-lateral PAG (dlPAG) neuron pool positively modulates analgesia and flight response while simultaneously and directly decreasing freezing behavior through direct GABAergic inhibition of vlPAG. An initial screen for its regulatory elements suggested a unique and strong input from the pre-mammillary nucleus of the thalamus. Taken together, the combination of powerful optical, viral, and genetic approaches in this study enabled the description of a detailed circuit diagram beginning in amygdala, traversing the PAG and medulla, and ending in the ventral spinal cord that is responsible for modulating stereotyped fear and anxiety behavior directly relevant to human psychiatric disease, including anxiety disorders, PTSD, and phobia, thereby providing novel potential therapeutic targets for translational studies. In summary, the expanding optogenetic toolbox is beginning to pay dividends in addressing mysteries and challenges in psychiatric disease research that have long been out of reach (including in the studies of many others, e.g., Abbott et al., 2009; Busskamp and Roska, 2011; Covington et al., 2010; Ivanova and Pan, 2009; Lobo et al., 2010; Paz et al., 2011; Tan et al., 2008, 2012; Tonnesen et al., 2009). Optogenetic work has even begun to provide clues to treatment mechanisms and refinement; for example, in the case of deep brain stimulation (DBS) mechanisms, optogenetic studies have suggested that the likely direct initial target of DBS (at least in the case of Parkinson’s disease) is not local cell bodies but afferent axons to the region (in this case, to the subthalamic nucleus), which may arise from globally distributed brain regions (Gradinaru et al., 2009). Last, as an example of how optogenetic work has directly guided clinical studies, chronic cocaine
self-administration in rats was found to suppress the basal excitability of deep-layer mPFC pyramidal neurons (Chen et al., 2013a). Compensating or exacerbating this hypoexcitability using optogenetic tools either reduced or increased cocaine-seeking behavior, suggesting a potential target and manipulation for patients with substance abuse disorders. Transcranial magnetic stimulation of human dorsolateral prefrontal cortex has now been found to decrease cocaine use and craving in human cocaine addicts (Shen et al., 2016; Terraneo et al., 2016). Despite important advances in basic neuroscience, psychiatric disease research, and translational success, major areas of optogenetic tool advancement are nevertheless required in the future, as detailed next. U N S O LVE D P R O B L E M S A N D O P E N Q U E S T I O N S : T E C H N O L O GY F R O M C E L L B I O L O GY, O P T I C S , A N D B E H AVI O R One group of technological challenges to be addressed in optogenetics lies within the natural domain of mammalian biology. First, the development of improved subcellular trafficking will be important. Membrane trafficking strategies have improved the expression of opsins at the membrane (Gradinaru et al., 2008, 2010; Zhao et al., 2008), but further exploration in this area may produce targeting strategies that allow selective opsin (or other complementary genetic tools) expression in subcellular compartments such as dendrites, soma, or axon terminals. Indeed, while efforts have been made in this regard, achieving truly robust (near 100%) exclusion of heterologously expressed optogenetic proteins from axons would prevent undesired optical drive of axons of passage during illumination of an opsin-expressing brain region. While the expression of opsins in axons is one of the most useful features of this approach in allowing “projection targeting”– based recruitment of cells defined only by selective illumination and projection pattern, this effect also confounds certain kinds of functional mapping procedures that employ optogenetics (Petreanu et al., 2009). Projection-targeting approaches will additionally be facilitated by molecular advancements to speed opsin expression and trafficking (as with the 3’ untranslated region of neuritin described in Ye et al. 2016, which was found to accelerate axonal expression of transgene-derived proteins). This is a crucial consideration when working with long-distance projections in the rodent brain and will be especially important as optogenetic approaches are more widely used in larger mammals or humans. Second, it would be valuable to develop a robust and versatile optical (nonpharmacological) strategy to (when desired) prevent the propagation of optogenetically elicited action potentials in the antidromic direction or along axon collaterals during projection targeting experiments. Again, sometimes this antidromic drive is desired, but in other cases it is not (wherein the experimenter seeks to allow generalizable selective excitation only of spatially defined projections, and wishes to not take advantage of the existing capability to recruit cells defined by projection).
82 •S. E m erging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford University Press USA - OSO, T 2018. 07:33:44.
Third, improved high-speed volumetric (3D) light delivery strategies with single-cell resolution would be of great value, so that populations of cells even within intact mammalian brain tissue could be recruited optogenetically with any required extent of synchrony or asynchrony. Optogenetic applications in vivo to questions in mammalian circuit dynamics and behavior have typically involved synchronous optogenetic control of entire genetically targeted cell populations over millimeter-scale spatial domains, for example in studies of sleep–wake transitions, Parkinsonian circuitry, gamma rhythms, feeding behavior, olfaction, aggression, and memory consolidation. Yet, methods for guiding spatial delivery of light excitation itself in 3D volumes could allow much improved precision and complexity in optogenetic modulation, taking the next step beyond the single-photon guided-light strategies that have already been used in mammalian tissue for applications such as refined optogenetic circuit mapping and dissection of anxiety circuitry (Tye et al., 2011). Improved optogenetic two-photon illumination, in combination with opsins activated by less-scattering red-shifted wavelengths (Packer et al., 2012; Prakash et al., 2012) theoretically could provide a distinct means to manipulate single or multiple genetically and spatially targeted cells with high temporal resolution over sustained intervals and within intact tissue volumes, in order to delineate and define components that work in concert to generate circuit dynamics or behavior. The adaptation of approaches combining novel computational methods and improved optical components for simultaneous volumetric imaging (Yang et al., 2015) to optogenetics is in its early days, but rapidly expanding in both resolution and precision. The combined use of imaging and optogenetic approaches to “close the loop” for all-optical, online control of neural activity in awake, behaving animals is now within reach (reviewed in Grosenick et al., 2015). Fourth, it would be immensely valuable to develop methods to rapidly and efficiently extract brainwide wiring (connectomic) patterns, or at least projection patterns, from predefined cells, including those driven optogenetically (Deisseroth, 2012). The development of approaches to whole- brain intact imaging (CLARITY; Chung and Deisseroth, 2013) and their integration of in situ labeling techniques (Sylwestrak et al., 2016) brings this goal one step closer to reality. Improved imaging pipelines optimized for large-volume samples, including entire human brain, computational methods for extracting connection patterns, and standardized approaches with central data repositories, will further this goal (Ye et al., 2016). Fifth, robust extension of optogenetic tool-targeting strategies to non–genetically tractable species or cell types will be enormously helpful. The generation of Cre-driver rats has been important (Witten et al., 2011), and projection targeting provides an independent step forward. Recently described nanobody- based techniques for conditional expression of ChR2 in the absence of recombinases (Tang et al., 2015, 2016) provide a starting point to integrating nontransgenic model organisms with the molecular neuroscience toolkit. Separately, small/ strong/ specific promoters and enhancers would enable targeted viral expression without the need
for recombinases. Regardless of approach, a concerted effort to supplant the current ad-hoc nature of targeting approach development would represent a major advance for basic neuroscience and facilitate integration of data across studies and model organisms. Sixth, true retrograde and anterograde wiring-based strategies (i.e., targeting cells that project to a particular region, or cells that receive projections from a particular region) would greatly enhance the flexibility of optogenetic control, both in mice and in other species; such strategies exist but are not always robust or well tolerated. Progress in this domain has been made by modifying retrograde rabies (Kim et al., 2016b) and anterograde herpes (Lo and Anderson, 2011) viruses, but these retain their toxic properties, limiting their utility. Seventh, it would be of great value to rapidly and efficiently extract the brainwide elicited-activity patterns arising from optogenetic control of a targeted population. This can be achieved to some extent with ofMRI (optogenetic functional magnetic resonance imaging; Ferenczi et al., 2016; Lee et al., 2010), an optogenetic method that enables unbiased global assessment of the neural circuits upstream and downstream of focal stimulation. However, fMRI methods in general suffer from poor spatial and temporal resolution. Whether the optimal method to obtain brainwide activity records in freely moving animals would be through activity imaging compatible with optogenetics, or with deposition of some recoverable permanent activity trace (Deisseroth, 2012) in the cellular population of interest (since light-based imaging methods encounter fundamental limitations of resolution arising from scattering in mammalian brain tissue) remains to be seen. In general, improved integration of optogenetic control with readouts will be important—whether behavioral, electrophysiological (e.g., Anikeeva et al., 2012), or imaging (Kim et al., 2016a). Moreover, it will be important to develop computational methods to “reverse engineer” the studied circuitry in the brain in vivo. Addressing the technological challenges, all squarely in the domain of modern neuroscience, will help provide experimental leverage that may lead to key insights into neural circuit function and dysfunction, which would be difficult or impossible to establish by other means. U N S O LVE D P R O B L E M S A N D O P E N Q U E S T I O N S : G E N O M I C S A N D B I O P H YS I C S Another group of technological challenges to be addressed in optogenetics falls more into the natural domain of microbial biologists and biophysicists (although of course many laboratories and investigators span the mammalian and the microbial realms). First, the ongoing identification of additional genomically identified tools (via searching databases, broad-based sequencing efforts, and ecological genome mining) will profoundly improve our ability to perturb and understand biological systems. Many thousands of new opsin genes alone, to say nothing of other classes of light-sensitive modules, will
6. O S. p togenetics R elated T echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford and University Press USA - OSO, 2018. 07:33:44.
be accessible in this way. For example, even though known opsins already span most of the visual spectrum and a very broad kinetics space (Fenno et al., 2011; Yizhar et al., 2011a), it is very likely that new kinds of light sensitivity, kinetic properties, and even ion selectivity will emerge (as in Govorunova et al., 2015). One important goal is moving closer to the infrared, which will achieve (1) deeper light-penetration at a given irradiance value, (2) reduced scattering for improved resolution, and (3) provision of an additional control channel; infrared actuation has already been achieved for certain non–opsin-based optogenetic approaches, but possibly pushes against certain physics-based limitations for retinal- based photoreceptors. Second, engineering of these known or new tools for narrowed (as well as shifted) action spectrum would enable more clean separation of control channels. For example, engineering of blue-shifted hyperpolarizing opsins with narrower activation wavelength spectra could ultimately allow for enhanced combinatorial neuronal inhibition experiments within scattering mammalian tissues. While action spectrum peaks for existing tools span the visible spectrum and beyond, the broad shoulders of relevant action spectra may prevent use of more than two or three channels of control at once, unless spectra can be narrowed. Such efforts might involve mutations that prevent access of the photocycle to specific states or intermediates that have shifted absorbance properties. This class of opsin engineering will be facilitated by structure-based insights into wavelength sensitivity as well as the ChR photocycle; further structural studies of the absorption- structure relationship (Thoen et al., 2014) as well as more ChR structures beyond the current closed-state (Kato et al., 2012), including of open and intermediate photocycle states, and of other opsins, are clearly needed. These efforts may also lead to the generation of mutants with novel kinetic properties. Third, engineering the light sensors of optogenetics for higher quantum efficiency, greater light sensitivity, and/or increased current elicited per optogenetic-protein molecule, would be of substantial value in allowing the use of lower irradiances for targeting a given tissue volume or depth, which may be important in minimizing photodamage, heating, or power use/deposition constraints. While for opsins many orders of magnitude increased light sensitivity can be achieved with the bistable or step-function approach, this comes at a kinetic cost (slowing down the deactivation after light-off; Berndt et al., 2009). Fourth, the development of an inhibitory, single- component optogenetic potassium channel (Cosentino et al., 2015; Janovjak et al., 2010; Kang et al., 2013) that has kinetics and conductance relevant to neuroscience would be of immense value. Currently available inhibitory chloride channels provide strong, shunting inhibition with increased photon efficiency over chloride pumps. Even so, these will be influenced by variable chloride balance in different cells, cellular compartments, and developmental stages, just as with native inhibitory chloride channels like the GABA-A receptor. Moreover, the number of channels that must be recruited to provide inhibition requires high expression levels and light intensity, difficult to achieve uniformly in intact tissue.
Potassium concentrations are less variable, and potassium has a reversal potential that is more hyperpolarized than the resting membrane potential. Fifth, “dead” optogenetic tool mutants with expression and targeting properties comparable to active tools, but with no light-induced effector function, would be useful as controls. Currently, controls for optogenetic experiments often include XFP-expressing organisms or viruses, but this approach may not fully account for potential side effects of expressing the optogenetic tools themselves on parameters such as membrane capacitance and endogenous protein trafficking. Again, knowledge of pore structure (and pump mechanisms) may facilitate the generation of such tools. Sixth, in addition to light-sensitive pumps and channels, continued expansion of optically recruited biochemical signaling will be important, with increasing attention to strategies for modular and easily programmable pathway recruitment, improved specificity, expanded spectral responsivity bands, and adaptation to additional classes of native chromophores (such as flavins, biliverdins, and the like). The optoXR family of light-activated 7TM neurotransmitter/neuromodulator receptors will see addition of novel tools based on chimeras between vertebrate rhodopsins and both well-known and orphan GPCRs, and will complement chemogenetic tools such as DREADDs and PSAMs. And light-sensitive domains are being added to an increasing number of receptor and even intracellular signaling proteins, so that optogenetics will expand to occupy the full breadth of cell signaling, far beyond the study of neural activity. C O N C LU S I O N In summary, continued investigation from the microbial and biophysical side into ecological diversity, high- resolution structures, photocycle properties, and functional phylogenetics of light-sensitive protein modules will enable the discovery and engineering of new and improved classes of optogenetic control. Moreover, investigation from the neuroscience side into targeting, trafficking, selective spatiotemporal properties of illumination, precise circuit-element recruitment, and diverse compatible readout engineering will fundamentally advance the scope and precision of resulting insights into complex intact biological systems. Existing methods represent only the tip of the iceberg in terms of what could be ultimately achieved for neuroscience and neuropsychiatry disease research, in maximally enabling the principled design and application of optogenetics. REFERENCES Abbott, S.B., Stornetta, R.L., et al. (2009). Photostimulation of retrotrapezoid nucleus phox2b-expressing neurons in vivo produces long- lasting activation of breathing in rats. J Neurosci 29:5806–5819. Adamantidis, A.R., Zhang, F., et al. (2007). Neural substrates of awakening probed with optogenetic control of hypocretin neurons. Nature 450:420–424.
84 •S. E m erging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford University Press USA - OSO, T 2018. 07:33:44.
Airan, R.D., Thompson, K.R., et al. (2009). Temporally precise in vivo control of intracellular signalling. Nature 458:1025–1029. Anikeeva, P., Andalman, A.S., et al. (2012). Optetrode: a multichannel readout for optogenetic control in freely moving mice. Nat Neurosci 15:163–170. Aravanis, A.M., Wang, L.P., et al. (2007). An optical neural interface:in vivo control of rodent motor cortex with integrated fiberoptic and optogenetic technology. J Neural Eng 4:S143–S156. Bamann, C., Kirsch, T., et al. (2008). Spectral characteristics of the photocycle of channelrhodopsin-2 and its implication for channel function. J Mol Biol 375:686–694. Bargmann, C., Newsome, W., et al. (2014). BRAIN 2025: a scientific vision. Brain Research Through Advancing Innovative Neurotechnologies (BRAIN) Working Group Report to the Advisory Committee to the Director, NIH. Available online at:http://www.nih.gov/science/ brain/2025/. US National Institutes of Health, 2014. Berndt, A., Lee, S.Y., et al. (2014). Structure-g uided transformation of channelrhodopsin into a light- activated chloride channel. Science 344:420–424. Berndt, A., Lee, S.Y., et al. (2016). Structural foundations of optogenetics: Determinants of channelrhodopsin ion selectivity. Proc Natl Acad Sci U S A 113:822–829. Berndt, A., Yizhar, O., et al. (2009). Bi-stable neural state switches. Nat Neurosci 12:229–234. Boyden, E.S., Zhang, F., et al. (2005). Millisecond-timescale, genetically targeted optical control of neural activity. Nat Neurosci 8:1263–1268. Busskamp, V., Roska, B. (2011). Optogenetic approaches to restoring visual function in retinitis pigmentosa. Curr Opin Neurobiol 21:942–946. Chen, B.T., Yau, H.J., et al. (2013a). Rescuing cocaine-induced prefrontal cortex hypoactivity prevents compulsive cocaine seeking. Nature 496:359–362. Chen, T.W., Wardill, T.J., et al. (2013b). Ultrasensitive fluorescent proteins for imaging neuronal activity. Nature 499:295–300. Chow, B.Y., Han, X., et al. (2010). High-performance genetically targetable optical neural silencing by light-driven proton pumps. Nature 463:98–102. Chung, K., and Deisseroth, K. (2013). CLARITY for mapping the nervous system. Nat Methods 10:508–513. Ciocchi, S., Herry, C., et al. (2010). Encoding of conditioned fear in central amygdala inhibitory circuits. Nature 468:277–282. Consortium, T.H.-P. (2012). The Human Brain Project: A Report to the European Commission, Lausanne. Cosentino, C., Alberio, L., et al. (2015). Optogenetics. Engineering of a light-gated potassium channel. Science 348:707–710 Covington, H.E. 3rd, Lobo, M.K., et al. (2010). Antidepressant effect of optogenetic stimulation of the medial prefrontal cortex. J Neurosci 30:16082–16090. Deisseroth, K. (2010). Optogenetics: controlling the brain with light [extended version]. SciAm 303(5):48–55. Deisseroth, K. (2012). Optogenetics and psychiatry: applications, challenges, and opportunities. Biol Psychiatry 71:1030–1032. Deisseroth, K. (2015). Optogenetics:10 years of microbial opsins in neuroscience. Nat Neurosci 18:1213–1225. Deisseroth, K., Etkin, A., and Malenka, R.C. (2015). Optogenetics and the circuit dynamics of psychiatric disease. JAMA 313:2019–2020. Deisseroth, K., Feng, G., et al. (2006). Next-generation optical technologies for illuminating genetically targeted brain circuits. J Neurosci 26:10380–10386. Fenno, L., Yizhar, O., and Deisseroth, K. (2011). The development and application of optogenetics. Annu Rev Neurosci 34:389–412. Fenno, L.E., Mattis, J., et al. (2014). Targeting cells with single vectors using multiple-feature Boolean logic. Nat Methods 11:763–772. Ferenczi, E., and Deisseroth, K. (2016). Illuminating next-generation brain therapies. Nat Neurosci 19:414–416. Ferenczi, E.A., Zalocusky, K.A., et al. (2016). Prefrontal cortical regulation of brainwide circuit dynamics and reward-related behavior. Science 351:aac9698. Goshen, I., Brodsky, M., et al. (2011). Dynamics of retrieval strategies for remote memories. Cell 147:678–689.
Govorunova, E.G., Sineshchekov, O.A., et al. (2015). NEUROSCIENCE. Natural light-gated anion channels: A family of microbial rhodopsins for advanced optogenetics. Science 349:647–650. Gradinaru, V., Mogri, M., et al. (2009). Optical deconstruction of Parkinsonian neural circuitry. Science 324:354–359 Gradinaru, V., Thompson, K.R., and Deisseroth, K. (2008). eNpHR:a Natronomonas halorhodopsin enhanced for optogenetic applications. Brain Cell Biol 36:129–139. Gradinaru, V., Thompson, K.R., et al. (2007). Targeting and readout strategies for fast optical neural control in vitro and in vivo. J Neurosci 27:14231–14238. Gradinaru, V., Zhang, F., et al. (2010). Molecular and cellular approaches for diversifying and extending optogenetics. Cell 141:154–165. Gremel, C.M., Chancey, J.H., et al. (2016). Endocannabinoid modulation of orbitostriatal circuits gates habit formation. Neuron 90:1312–1324. Grosenick, L., Marshel, J.H., and Deisseroth, K. (2015). Closed-loop and activity-g uided optogenetic control. Neuron 86:106–139. Gulyani, A., Vitriol, E., Allen, R., et al. (2011). A biosensor generated via high-throughput screening quantifies cell edge Src dynamics. Nat Chem Biol 7:437–444. Gunaydin, L.A., Grosenick, L., et al. (2014). Natural neural projection dynamics underlying social behavior. Cell 157:1535–1551. Gunaydin, L.A., Yizhar, O., et al. (2010). Ultrafast optogenetic control. Nat Neurosci 13:387–392. Haubensak, W., Kunwar, P.S., et al. (2010). Genetic dissection of an amygdala microcircuit that gates conditioned fear. Nature 468:270–276. Inoue, M., Takeuchi, A., et al. (2015). Rational design of a high-affinity, fast, red calcium indicator R-CaMP2. Nat Methods 12:64–70. Ivanova, E., and Pan, Z.H. (2009). Evaluation of the adeno-associated virus mediated long-term expression of channelrhodopsin-2 in the mouse retina. Mol Vis 15:1680–1689. Janovjak, H., Szobota, S., et al. (2010). A light-gated, potassium-selective glutamate receptor for the optical inhibition of neuronal firing. Nat Neurosci 13:1027–1032. Kang, J.Y., Kawaguchi, D., et al. (2013). In vivo expression of a light- activatable potassium channel using unnatural amino acids. Neuron 80:358–370. Kato, H.E., Zhang, F., et al. (2012). Crystal structure of the channelrhodopsin light-gated cation channel. Nature 482:369–374. Kim, C.K., Yang, S.J., et al. (2016a). Simultaneous fast measurement of circuit dynamics at multiple sites across the mammalian brain. Nat Methods 13:325–328. Kim, E.J., Jacobs, M.W., et al. (2016b). Improved monosynaptic neural circuit tracing using engineered rabies virus glycoproteins. Cell Rep pii: S2211–1247(16)30356–4. Kim, J.M., Hwa, J., et al. (2005). Light-driven activation of beta 2- adrenergic receptor signaling by a chimeric rhodopsin containing the beta 2-adrenergic receptor cytoplasmic loops. Biochemistry 44: 2284–2292. Klapoetke, N.C., Murata, Y., et al. (2014). Independent optical excitation of distinct neural populations. Nat Methods 11:338–346. Kolbe, M., Besir, H., et al. (2000). Structure of the light-driven chloride pump halorhodopsin at 1.8 A resolution. Science 288:1390–1396. Lammel, S., Lim, B.K., et al. (2012). Input-specific control of reward and aversion in the ventral tegmental area. Nature 491:212–217. Lee, J.H., Durand, R., et al. (2010). Global and local fMRI signals driven by neurons defined optogenetically by type and wiring. Nature 465:788–792. Lerner, T.N., Shilyansky, C., et al. (2015). Intact-brain analyses reveal distinct information carried by SNc dopamine subcircuits. Cell 162:635–647. Lin, J.Y., Knutsen, P.M., et al. (2013). ReaChR:a red-shifted variant of channelrhodopsin enables deep transcranial optogenetic excitation. Nat Neurosci 16:1499–1508. Liu, X., Ramirez, S., et al. (2012). Optogenetic stimulation of a hippocampal engram activates fear memory recall. Nature 484:381–385. Lo, L., and Anderson, D.J. (2011). A Cre-dependent, anterograde transsynaptic viral tracer for mapping output pathways of genetically marked neurons. Neuron 72:938–950.
6. O S. p togenetics R elated T echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford and University Press USA - OSO, 2018. 07:33:44.
Lobo, M.K., Covington, H.E. 3rd, et al. (2010). Cell type-specific loss of BDNF signaling mimics optogenetic control of cocaine reward. Science 330:385–390. Magnus, C.J., Lee, P.H., et al. (2011). Chemical and genetic engineering of selective ion channel-ligand interactions. Science 333:1292–1296. Mahn, M., Prigge, M., et al. (2016). Biophysical constraints of optogenetic inhibition at presynaptic terminals. Nat Neurosci 19:554–556. Marcinkiewcz, C.A., Mazzone, C.M., et al. (2016). Serotonin engages an anxiety and fear-promoting circuit in the extended amygdala. Nature 537:97–101. Mattis, J., Tye, K.M., et al. (2012). Principles for applying optogenetic tools derived from direct comparative analysis of microbial opsins. Nat Methods 9:159–172. Moglich, A., and Moffat, K. (2007). Structural basis for light-dependent signaling in the dimeric, LOV domain of the photosensor YtvA. J Mol Biol 373:112–126. Nieh, E.H., Vander Weele, C.M., et al. (2016). Inhibitory input from the lateral hypothalamus to the ventral tegmental area disinhibits dopamine neurons and promotes behavioral activation. Neuron 90:1286–1298. Oh, E., Maejima, T., et al. (2010). Substitution of 5-HT1A receptor signaling by a light-activated G protein-coupled receptor. J Biol Chem 285:30825–30836. Packer, A.M., Peterka, D.S., et al. (2012). Two-photon optogenetics of dendritic spines and neural circuits. Nat Methods 9:1202–1205. Paz, J.T., Bryant, A.S., et al. (2011). A new mode of corticothalamic transmission revealed in the Gria4(-/-) model of absence epilepsy. Nat Neurosci 14:1167–1173. Petreanu, L., Mao, T., et al. (2009). The subcellular organization of neocortical excitatory connections. Nature 457:1142–1145. Prakash, R., Yizhar, O., et al. (2012). Two-photon optogenetic toolbox for fast inhibition, excitation and bistable modulation. Nat Methods 9:1171–1179. Rajasethupathy, P., Ferenczi, E., and Deisseroth, K. (2016). Targeting neural circuits. Cell 165:524–534. Rajasethupathy, P., Sankaran, S., et al. (2015). Projections from neocortex mediate top-down control of memory retrieval. Nature 526:653–659. Rickgauer, J.P., Deisseroth, K., and Tank, D.W. (2014). Simultaneous cellular-resolution optical perturbation and imaging of place cell firing fields. Nat Neurosci 17:1816–1824. Scanziani, M., and Hausser, M. (2009). Electrophysiology in the age of light. Nature 461:930–939. Shen, Y., Cao, X., et al. (2016). 10-Hz repetitive transcranial magnetic stimulation of the left dorsolateral prefrontal cortex reduces heroin cue craving in long-term addicts. Biol Psychiatry 80:e13–e14. Siuda, E.R., Copits, B.A., et al. (2015). Spatiotemporal control of opioid signaling and behavior. Neuron 86:923–935. Sohal, V.S., Zhang, F., et al. (2009). Parvalbumin neurons and gamma rhythms enhance cortical circuit performance. Nature 459:698–702. Stierl, M., Stumpf, P., et al. (2011). Light modulation of cellular cAMP by a small bacterial photoactivated adenylyl cyclase, bPAC, of the soil bacterium Beggiatoa. J Biol Chem 286:1181–1188. Stuber, G.D., Sparta, D.R., et al. (2011). Excitatory transmission from the amygdala to nucleus accumbens facilitates reward seeking. Nature 475:377–380.
Sylwestrak, E.L., Rajasethupathy, P., et al. (2016). Multiplexed intact- tissue transcriptional analysis at cellular resolution. Cell 164:792–804. Tan, K.R., Yvon, C., al. (2012). GABA neurons of the VTA drive conditioned place aversion. Neuron 73:1173–1183. Tan, W., Janczewski, W.A., et al. (2008). Silencing preBotzinger complex somatostatin-expressing neurons induces persistent apnea in awake rat. Nat Neurosci 11:538–540. Tang, J.C., Drokhlyansky, E., et al. (2016). Detection and manipulation of live antigen-expressing cells using conditionally stable nanobodies. Elife 5:pii: e15312. Tang, J.C., Rudolph, S., et al. (2015). Cell type-specific manipulation with, GFP-dependent Cre recombinase. Nat Neurosci 18:1334–1341. Terraneo, A., Leggio, L., et al. (2016). Transcranial magnetic stimulation of dorsolateral prefrontal cortex reduces cocaine use:A pilot study. Eur Neuropsychopharmacol 26:37–44. Thoen, H.H., How, M.J., et al. (2014). A different form of color vision in mantis shrimp. Science 343:411–413. Tonnesen, J., Sorensen, A.T., et al. (2009). Optogenetic control of epileptiform activity. Proc Natl Acad Sci U S A 106:12162–12167 Tovote, P., Esposito, M.S., et al. (2016). Midbrain circuits for defensive behaviour. Nature 534:206–212. Tsai, H.C., Zhang, F., et al. (2009). Phasic firing in dopaminergic neurons is sufficient for behavioral conditioning. Science 324:1080–1084. Tye, K.M., and Deisseroth, K. (2012). Optogenetic investigation of neural circuits underlying brain disease in animal models. Nat Rev Neurosci 13:251–266. Tye, K.M., Prakash, R., et al. (2011). Amygdala circuitry mediating reversible and bidirectional control of anxiety. Nature 471:358–362. Urban, D.J., and Roth, B.L. (2015). DREADDs (designer receptors exclusively activated by designer drugs): chemogenetic tools with therapeutic utility. Annu Rev Pharmacol Toxicol 55:399–417. Wietek, J., Wiegert, J.S., et al. (2014). Conversion of channelrhodopsin into a light-gated chloride channel. Science 344:409–412. Witten, I.B., Steinberg, E.E., et al. (2011). Recombinase- driver rat lines: tools, techniques, and optogenetic application to dopamine- mediated reinforcement. Neuron 72:721–733. Wu, Y.I., Frey, D., et al. (2009). A genetically encoded photoactivatable Rac controls the motility of living cells. Nature 461:104–108. Yang, W., Miller, J.E., et al. (2016). Simultaneous multi-plane imaging of neural circuits. Neuron 89:269–284. Ye, L., Allen, W.E., et al. (2016). Wiring and molecular features of prefrontal ensembles representing distinct experiences. Cell 165:1776–1788. Yizhar, O., Fenno, L.E., et al. (2011a). Optogenetics in neural systems. Neuron 71:9–34. Yizhar, O., Fenno, L.E., et al. (2011b). Neocortical excitation/inhibition balance in information processing and social dysfunction. Nature 477:171–178. Zhang, F., Prigge, M., et al. (2008). Red-shifted optogenetic excitation: a tool for fast neural control derived from V. carteri. Nat Neurosci 11:631–633. Zhang, F., Vierock, J., et al. (2011). The microbial opsin family of optogenetic tools. Cell 147:1446–1457. Zhang, F., Wang, L.P., et al. (2007). Multimodal fast optical interrogation of neural circuitry. Nature 446:633–639. Zhao, S., Cunha, C., et al. (2008). Improved expression of halorhodopsin for light-induced silencing of neuronal activity. Brain Cell Biol 36:141–154.
86 •S. E m erging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford University Press USA - OSO, T 2018. 07:33:44.
7. IN VIVO CIRCUIT ANALYSIS Ryan Bowman, Hannah Schwennesen, Kafui Dzirasa, and Rainbo Hultman
NEUR AL CIRCUIT C O MP O S I T I O N
INTRODUCTION With the explosion of research on mental illness over the past century, scientists have recognized that brain dysfunction contributes to psychological pathologies. Translational neuroscience research has expanded rapidly as a result. In particular, there has been a growing appreciation for studies interrogating multiple levels of analysis across genes, cells, and coordinated neural circuits that effectively address the complexities of mental illnesses (Jorgenson et al., 2015; Morris et al., 2015). In this chapter we will focus primarily on the use of in vivo neural activity as a powerful means of understanding complex behaviors. Neural circuit data collected using several different methods in both rodents and humans have in many cases provided complementary pictures of well-orchestrated brain network activity related to specific neural states and emotional behaviors. For example, classic studies linking amygdala and fear response (Phelps, 2006) led researchers to investigate the relationship between amygdala reactivity prior to stress and psychological vulnerability after exposure to stress. In human subjects, it has been found that heightened amygdala activity (during exposure to fearful faces) prior to the stress exposure correlated with maladaptive responses to stressful life events Swartz et al., 2015). Animal models extend our understanding of this relationship. Using a rodent behavioral model of chronic stress (Berton et al., 2006; Krishnan et al., 2007), it has been possible to probe this phenomenon more deeply, understanding the precise timing, cause, and coordinated brain regions conferring such stress susceptibility (Hultman et al., 2016; Kumar et al., 2014). Conclusions reached from these significant studies have indicated that (1) high-risk individuals with susceptibility to stress can be identified prior to stress for intervention before entering high-stress situations (e.g., military service, etc.); and (2) amygdala reactivity is tightly controlled by the precise timing of several other brain regions, enabling additional therapeutic targets and modalities within the corticolimbic networks. Thus, by examining hypotheses generated from human research in animal models, neuroscientists and clinicians are able to uncover the intricacies of brain functioning that underlie neuropsychiatric disorders, as well as new paths to therapeutics. Advances in the techniques used to observe and manipulate brain activity in animals lay the foundation for highly specific treatments addressing mental illnesses and neurological disorders, perhaps utilizing molecular or genetic targeting methods to alter circuit dysfunction (Gordon, 2016).
Large groups of neurons function in concert to propagate information throughout the nervous system. Neural circuits comprise these cell groups in the brain. Within any given circuit, cells are given one of three classifications: afferent cells are neurons that bring new information into the circuit; interneurons synapse onto other cells within the circuit and help parse and modulate the input; and efferent cells carry the signal out of the circuit to other nerves or circuits. Dozens of different circuits have been identified both within the peripheral nervous system (for motor function, reflexes and sensory processing) and the central nervous system underlying more complex behaviors. Our growing understanding of neural circuits and how they relate to behavior has allowed a number of key breakthroughs in the comprehension and treatment of neurological and psychological disorders. One key example of this the emergence of deep brain stimulation as a potential therapeutic for treatment of refractory major depressive disorder (Mayberg et al., 2005). Finally, it is important to note that these neuronal circuits are functioning within a rich environment with many other types of cells, hormones, and other secreted factors that impact their activity. A large number of cells in the brain (there is significant debate over just what percentage, somewhere between 50% and 90%) are not neurons (Azevedo et al., 2009; Hilgetag and Barbas, 2009). They are the glial cells which provide metabolic, immune, insulation, and other crucial auxiliary functions. An increasing number of neurological and psychological diseases (e.g., depression, schizophrenia, autism, OCD, and Tourette’s) have been associated with dysfunctional glial cells in the brain (Frick et al., 2013). Even more pertinently, astrocyte glia have been shown to interact with up to 100,000 different synapses, and modulate their firing patterns through the release and reuptake of ions and proteins (Halassa and Haydon, 2010). O VE RVI EW O F N E U R A L C I R C U I T O B S E RVAT I O N S A N D W H AT T H EY T E L L U S A B O U T B E H AVI O R Over the decades of psychiatric and neuroscientific research, a wide variety of techniques have been developed in order to
8 7 USA - OSO, 2018. Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press 07:33:44.
observe and record circuit activity in humans and in animal models. Animal models provide a number of unique tools that are not feasible in human subjects due to necessary genetic or physiological manipulations. These tools have nonetheless proven crucial in elucidating the functions of the brain’s circuitry. While more limited in their ability to achieve both high spatial and high temporal resolution of brain activity, there are still a large number of different methods that are useful for measuring circuit activity in human patients. Functional magnetic resonance imaging (fMRI) uses large magnets to visualize blood flow to different areas of the brain. Active regions require more oxygen to fuel their metabolic processes, so the measure of deoxygenated hemoglobin (the protein which carries oxygen in blood) is a useful indirect measure of activity (Logothetis, 2008). These data can give a snapshot of large changes in brain activity on the order of seconds. Similarly, positron emission tomography (PET) can use radioactive molecules to quantify local blood flow, glucose utilization, or other measures of activity. Such activity can be measured across several minutes and can be used to detect activity of a number of different brain chemicals (e.g., dopmaine) (Laruelle and Abi-Dargham, 1999). A technique called functional near- infrared spectroscopy (fNIR) is another noninvasive measure of activity via blood flow. FNIR utilizes the differences in light absorbancy between brain tissue and hemoglobin to measure blood flow; it is significantly restricted in the depth into the brain it can be measured, but allows for greater mobility and shorter time durations of data collection than fMRI and PET (Chance et al., 1998). For the greater part of the last century, scientists and clinicians have measured brain activity using electrodes placed on the scalp. These electroencephalographic (EEG) signals provide large-scale measures of brain activity with high temporal resolution (much higher than the methods discussed so far). Nevertheless, EEG is unable to detect activity deep within the brain. Furthermore, the skull operates as a low-pass filter of electrical activity. As a result, EEG fails to resolve brain activity at high spatial resolution. Emerging approaches, including magnetoencephalograpy (MEG), better resolve higher frequency activity at the surface of the brain, but also fail to measure and resolve activity at deeper structures. Finally, advances in human neurosurgical and brain machine interface approaches have yielded a new array of tools that allow single- neuron activity to be resolved in human brain. Recording and stimulation electrodes have been implanted directly onto or within the brain surface, allowing for the intraoperative or chronic monitoring of neural activity in a similar manner as EEG but with much better spatial resolution and a much wider range of targets. These electrodes are typically designed to measure changes in voltage surrounding a group of cells, as well as to provide a measure of single cell neural activity. Nevertheless, given the invasive nature of these approaches, their application is generally limited to clinical disorders in which there is high potential for clinical benefit (Parkinson’s disease, obsessive compulsive disorder, epilepsy, and paralysis). Each of these of these approaches has also been applied in preclinical animal models.
Advances in optical imaging have also yielded emerging tools for monitoring that are almost exclusively used in animal models. These approaches include two-photon excitation microscopy and microendoscopy, which now allow for large-scale cell type–specific activity to be resolved within the brain (Deisseroth et al., 2006). By integrating these methods with an emerging toolbox of genetically encoded indicators of neuronal activity (fluorophores), including calcium and voltage sensors, investigators are garnering critical insights into structure–function relationships across the brain. WHY ARE ANIMAL MODELS U S E F U L F O R S T U DY I N G BR AIN CIRCUITS AND N E U R O P SYC H I AT R I C DISORDER S? There are numerous advantages to utilizing animal models in the study of the neural circuitry of neuropsychiatric disorders. One of the greatest advantages is that in animal models, causality can be tested using tightly controlled experimental conditions and neural circuit manipulations. In humans it is often the case that studies can be conducted correlating a particular condition with a particular neural circuit readout; but without actually performing manipulations of neural circuitry in humans, it is impossible to directly test whether these correlated factors are actually causal. Furthermore, a lab animal’s environment can be controlled from birth, we can have complete knowledge of its genetic makeup, and we can control its diet, daily routine, and so forth (contrary to the diverse set of variables that accompany the history of most humans). A much greater variety of tools exist that can be safely and ethically utilized in animal models than in human subjects. In animal models, we are able to easily and quickly introduce a particular protein, drug, genetic alteration, electrical stimulation, hormone, or other probe. We have much greater flexibility when experimenting on an animal brain than a human brain. In particular, a tool that is unique to animal studies is genetic modification. It is possible to screen subjects in a human study by genotype; however, the results of such studies are correlative at best, and it is logistically difficult and limited compared to the ability to mutate the genome of animal subjects. Furthermore, it is much easier in lab animals to limit confounding variables such as variation in environmental influences, compared to human subjects with different lifestyles and diverse backgrounds. Additionally, experimental methods available for use in animals afford a degree of specificity and detail currently impossible when studying humans. The techniques outlined examine aspects of circuitry underlying behavior at the molecular and cellular level. With genetic manipulations that target specific cell types or proteins, experimenters can determine the exact source of dysfunction in a maladaptive behavior and explore potential solutions. The current state of human research does not allow for safe execution of invasive experimental techniques. Therefore, it is imperative that researchers of neural circuitry continue their quest for novel techniques
88 •S. E m erging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al., Oxford University Press USA - OSO, T 2018. 07:33:44.
and characterization of systems in animals that are applicable to neurobiology in humans. ME ASURING CIRCUITS Neuroscientists utilize a wide variety of techniques to capture different facets of neuronal circuits. Information can be captured at the level of a single neuron, a small population of neurons contacting one another, entire brain regions with coordinated activity, or globally, using brain imaging. A myriad of studies have utilized imaging modalities to probe brain–behavior relationships in animal models of psychiatric disease. As previously discussed, fMRI is a noninvasive tool that measures energy usage by a neural population based on changes in blood flow within brain structures using an applied magnetic field. One of the major advantages of fMRI imaging is that it allows for images to be acquired across the entire brain. Thus investigators can quantify the effect of their experimental manipulations on regionally distributed cellular populations (voxels of activity) and their interactions with each other. Another major advantage of this approach is that the same physiological assessments of brain activity can be made in animals and the human disorders they model. For example, human imaging studies have raised the hypothesis that altered activity in prefrontal cortex is a hallmark feature of major depressive disorder Greicius et al., 2007). Supporting this hypothesis, rodent studies with induced prefrontal cortex dysfunction exhibit deficits in appetitive behavior and altered signaling in neural circuits that contribute to hedonia in humans (Ferenczi et al., 2016). Nevertheless, there are several limitations of using large-scale brain imaging to probe neural circuits responsible for behavioral deficits in animal models. First, fMRI data has low temporal resolution, as blood flow is relatively slow (100s of milliseconds) compared to voltage fluctuations during an action potential ( t*, where t* is simply determined by assessing when the plot becomes a straight line. This method has the advantage of plotting the data (known as the Logan plot) to visually confirm linearization. However, under conditions of noisy data, this method underestimates VT (Slifstein and Laruelle, 2000). An alternative approach arranges the linear equations such that the tissue concentration CT(t) is the dependent variable, and the integral terms are the independent variables, which serves to reduce the bias of parameter estimation in situations of noisy data. The functional equation of this multilinear analysis (MA1) is as follows (Ichise et al., 2002): C T (t ) = −
t
where b is intercept term in the Logan equation. Again using a linearization time t > t*, VT is then estimated as the negative ratio of the two integral coefficients (VT = –β1/β2). Thus MA1 allows for efficient parameter estimation that is less biased by noise. Note that MA1 has the disadvantage of not being easily graphed to demonstrate linearity, as is the case for the Logan plot. R E FE R E N C E R EG I O NS A P P ROAC H E S
While arterial blood sampling can provide a complete characterization of the pharmacokinetic parameters for a given scan, there are significant logistical drawbacks. First, the placement of an arterial cannula can cause subject discomfort and requires additional technical proficiency from medical staff. Second, metabolite analysis of blood samples requires considerable staffing and technical expertise for accurate measurement of the parent input function. Moreover, the arterial input function is susceptible to high noise, particular with short-lived radiolabels such as 11C and radiotracers with very low parent fractions at late scanning times. Therefore, reference region approaches were developed to provide direct estimation of kinetic parameters completely from the PET data without the need for arterial blood sampling. Reference region methods estimate BPND by using a region devoid of detectable specific radiotracer binding as a proxy of nondisplaceable kinetics, known as a reference region. The critical assumption of negligible specific radiotracer binding in a reference region should be experimentally validated with pharmacological blocking studies. These experiments administer large cold doses of a ligand that binds specifically to the radiotracer target site, usually administered prior to radiotracer injection. A suitable reference region should show no significant difference in VT between baseline scans and blocking scans. Additionally, physiological differences between species can result in different radiotracer characteristics in the same brain region, thus reference region validation should ideally be performed within the same species with the same radiotracer. The simplified reference tissue model (SRTM) was an initial reference region analysis technique for PET data
• Charney, 114 S. E m erging and E stablished echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis et al., Oxford University Press USA - OSO, T 2018. 07:33:44.
t
VT 1 C P ( τ ) d τ + ∫C T ( τ ) d τ ∫ b 0 b0
(Lammertsma and Hume, 1996). In addition to the assumption of negligible specific radiotracer uptake in the reference region, SRTM assumes that the radiotracer kinetic properties are fast such that compartment model techniques cannot distinguish specifically bound and nonspecifically bound radiotracer in the tissue (e.g., the radiotracer is best described by 1TCM). Additionally, the VND in the reference region and regions of specific radioligand uptake are assumed to be uniform. This is a common assumption, but one that requires blocking studies for validation (Xia et al., 2015). Based on these assumptions, the solution to the 1TCM differential equation can be rearranged to express the operational SRTM equation as follows:
{
}
C T ( t ) = R1C R ( t ) + R1 k2′ − k2 C R ( t ) ⊗ exp ( − k2 t )
where CR(t) is the concentration of radiotracer in the reference region at time t and ⊗ is the convolution operator. K1′ and k2′ are the radioligand plasma to tissue and tissue efflux rate constants, respectively, in the reference region, and k2 is the tissue efflux rate constant in the target tissue region (an area of specific radiotracer uptake). R1 is the ratio of the uptake rate in the target region (K1) to that in the reference region (K1′). BPND can be calculated from the 3 parameters, as follows: BPND =
VT R k′ −1 = 1 2 −1 V ND k2
To solve SRTM, the parameters R1, k2′, and k2 are fit to the observed PET data, and then BPND is calculated. The term VT/VND is also known as the distribution volume ratio, or DVR. The SRTM parameters can be estimated in a computationally efficient fashion by using a basis function approach to estimate BPND at the voxel level (Gunn et al., 1997, 2002). Interestingly, violations of the SRTM assumption that the radiotracer conforms to 1TCM kinetics may or may not bias outcome parameter estimation. Noise can be reduced in SRTM by determining one global value for the reference region clearance constant (k2′) using the SRTM2 approach (Wu and Carson, 2002); however, this approach depends more strongly on the 1TCM assumption. In either case, a validation of BPND values estimated with SRTM or SRTM2 compared with those estimated with compartment modeling approaches as the gold standard should be performed to assess the suitability of this analysis method for a new radiotracer. Reference region approaches for BPND (or DVR) estimation in linearized forms, analogous to the previously discussed approaches to VT estimation, are also useful. These methods again assume negligible specific uptake of the radiotracer in the reference region and uniform VND values for the reference region and target tissue region. The functional equation for the Logan reference region approach (Logan et al., 1996) is as follows: t
tC ( τ ) d τ C R (t ) ∫ 0 R + + int VND C T ( t ) k2’ C T ( t )
∫ C (τ ) d τ = V 0
T
C T (t )
T
Similar to the Logan approach with blood sampling, the PET data is fit to the above operational equation once the above relationship becomes linear at time t > t* to estimate the slope. The slope VT/VND (DVR) is used to estimate BPND as BPND = DVR–1. To improve parameter estimation by hastening linearization of this equation, the parameter k2′ can be fixed a priori if it is well characterized for the radiotracer in the population under study. Alternatively, if the CR(t)/CT(t) term becomes constant quickly, then this term can be lumped with the intercept, and the k2′ parameter becomes unnecessary. In that case, the linearization time t* for this equation becomes later than the case where k2’ is known, so it is most appropriate for radiotracers with faster kinetic properties. The Logan reference region approach underestimates BPND in situations of high noise and large BPND, as previously discussed for estimation of VT with blood sampling. Thus, by using a similar strategy of placing CT(t) as the dependent variable and integral terms as the independent variables, the multilinear reference tissue model (MRTM; Ichise et al., 2003) can be derived: C T (t ) = −
This equation can be fit using all three parameters (β) to estimate β1 = –BPND/b, β2 = –BPND/(bk2′), and β3 = 1/b, producing the outcome measure estimate BPND = –β1/β3. Alternatively, k2′ can be set to a fixed value and a reduced set of two parameters β1 = –BPND/b and β2 = 1/b are estimated, with BPND similarly estimated as BPND = –β1/β2. The k2′ parameter can be fixed a priori based on previous knowledge of the parameter in the subject population. Alternatively, if fitting is performed at the voxel level, a subject-specific value of k2′ can be estimated by fitting all the data with the 3-parameter MRTM first, and the average k2′ value across all voxels of brain tissue is estimated, and then parameter estimation is performed again with the fixed value of k2′—a process also known as MRTM2 (Ichise et al., 2003). S TA N DA R D I Z E D U P TA K E VA LU E S
The standardized uptake value (SUV) and associated SUV ratio (SUVr) are the simplest molecular imaging outcome measures. The SUV is calculated by normalizing the observed radiotracer concentration (Bq/cc) in the tissue by the injected dose (d, Bq) and subject body weight (w) in grams (SUV = CT × w/d), with a unitless result. An SUV value gives an index of the radiotracer uptake in the tissue, with an SUV of 1 meaning that the tracer is uniformly distributed throughout the body. SUV values for successful brain PET tracers typically are >2. For molecular brain imaging studies, estimates of SUVr, the ratio of SUV in a given brain region relative to a reference region with negligible specific radiotracer uptake, provide rough estimates of specific radiotracer uptake. Mathematically, SUVr is estimated as SUVr = CT/CR, and for bolus injection scans is best estimated at late times after radiotracer injection when radiotracer concentrations are in pseudo-or transient
9.Charney, P ET Betrain I mUniversity aging Methodologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. al., Oxford Press USA - OSO, 2018. 07:33:44.
1 t BPND t 1 C τ d τ + C t ) ) ( ( R + ∫C T ( τ ) d τ R b ∫0 k2′ b 0
equilibrium. SUVr estimation is mathematically identical to the estimation of DVR for constant infusion of radiotracer, with the important exception that true equilibrium is NOT present between radiotracer in the tissue and radiotracer in the arterial plasma. Due to the lack of true equilibrium, SUVr overestimates the true DVR, and this overestimation is greater with larger BPND values and with faster radiotracer clearance from plasma (Carson et al., 1993). The advantages of SUVr as an outcome measure are that it is computationally simple and is a static measurement. Since no dynamic data are required to estimate SUVr, then the subject can be imaged for only 10–20 minutes at a preselected time. This advantage can be particularly important for subject populations unable to tolerate long imaging periods, such as patients with Alzheimer’s disease. However, since SUVr estimates are not equilibrium measures, they should be considered semi- quantitative metrics of specific radiotracer uptake. A common use of SUVr values in brain imaging is to estimate Aβ accumulation because scanning time is short for patients, DVR values for these radiotracers are low (typically 75 µV). N3 is also defined as slow wave sleep, delta sleep, or deep sleep, because arousal threshold increases incrementally from stage N1 to N3. Until recently, slow wave sleep was subdivided according to the proportion of slow waves in the epoch (stage 3, 20%–50%; stage 4, >50%), but the validity and biological significance of this subdivision has been called into question, and stages 3 and 4 are now together called stage N3 (Silber et al., 2007). Eye movements cease during stages N2 and N3, and EMG activity decreases further. The process of awakening
S L E E P D U R I N G T H E L I F E S PA N Sleep patterns change markedly across the life span (Carskadon, 2011; Colrain and Baker, 2011; Ringli and Huber, 2011). Newborn infants spend 16–18 hours per day sleeping, with an early version of REM sleep, called active sleep, occupying about half of their sleep time. At approximately three to four months of age, when sleep starts to become consolidated
• Charney, 130 S. E m erging and E stablished T echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis et al., Oxford University Press USA - OSO, 2018. 07:33:44.
REM Waking Stage 1 Stage 2 Stage 3 Stage 4 0
1
4 3 Recording time (hours)
2
5
6
7
Hypnogram for an all-night recording in a young man. Note the occurrence of five sleep cycles, the predominance of slow wave sleep (stages 3 and 4) early in the night, and the increasing length of REM sleep episodes later in the night. Figure 11.2
during the night, the sleep EEG shows more mature waveforms characteristic of NREM and REM sleep, and NREM sleep can be subdivided into stages. This is possible because at four to six months of age some EEG hallmarks of NREM sleep typical of stage 2, sleep spindles and K complexes, emerge, most likely reflecting the maturation of the thalamocortical system. During early childhood, total sleep time decreases, and REM sleep proportion drops to adult levels. The proportion of NREM sleep spent in slow wave sleep increases during the first year of life, reaches a peak, declines during adolescence and adulthood, and may disappear entirely by age 60.
show greater phasic activity. The proportion of time spent in each stage and the pattern of stages across the night is fairly consistent in normal adults, and no consistent male versus female differences have been found in this group. A healthy young adult will typically spend about 5% of the sleep period in stage N1 sleep, about 50% in stage N2 sleep, 20%–25% in slow wave sleep (N3), and 20%–25% in REM sleep. B R A I N C E N T E R S R E GU L AT I N G WA K E F U L N E S S A N D S L E E P
Two antagonistic sets of brain structures are responsible for orchestrating the regular alternation between wakefulness and sleep. The neuronal groups that promote wakefulness are The succession of NREM sleep stages followed by an episode located in the basal forebrain, posterior hypothalamus, and in of REM sleep is called a sleep cycle and lasts approximately 90– the upper brain stem, whereas those promoting NREM sleep 110 minutes in adults (it is shorter, 50 minutes, during infancy, are located in the anterior hypothalamus and basal forebrain and gradually increases with age until adulthood). As shown (Figure. 11.3) (Brown et al., 2012). Other cellular groups in the in Figure 11.2, there are a total of four to five cycles every night. dorsal part of the pons and in the medulla, as well as in the latSlow wave sleep is prominent early in the night, especially dur- eral hypothalamus, control REM sleep (Figure. 11.3) (Brown ing the first sleep cycle, and diminishes as the night progresses. et al., 2012, Luppi et al., 2012). The circadian clock, centered As slow wave sleep wanes, periods of REM sleep lengthen and on the suprachiasmatic nucleus of the hypothalamus, exerts T H E S L E E P C YC L E
CX
Mi vPAG Cb 5-HT
Th
DR
NA Ach
P
Me Glu
LC LDT, PPT
Glu
VTA DA
Or RF
BF
Hy LH
GABA Glu Ach
H TMN
Figure 11.3
The major brain areas involved in initiating and maintaining wakefulness are shown in red, and their projections in light and dark blue (Glu, glutamate; Ach, acetylcholine; DA, dopamine; NA, noradrenaline; H, histamine; ore, orexin; 5-HT, serotonin). Neurons active during NREM sleep in the anterior hypothalamus and basal forebrain are shown in green, and those active during REM sleep in ventral medulla, dorsal pons, and posterior/lateral hypothalamus are shown in yellow (for clarity their projections are not shown). BF, basal forebrain; Cb, cerebellum; Cx, cerebral cortex; DR, dorsal raphe; Hy, hypothalamus; LC, locus coeruleus; LDT, lateral dorsal tegmental nucleus; LH, lateral hypothalamus; Me, medulla; Mi, midbrain; P, pons; PPT, pedunculopontine tegmental nucleus; RF, reticular formation; Th, thalamus; TMN, tuberomammilary nucleus; vPAG, ventral periaqueductal grey; VTA, ventral tegmental area.
11. Tethe N eurobiology S2018. lee Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, al., Oxford University Press USA -of OSO, 07:33:44.
an overall control on many of these brain areas to ensure that sleep occurs at the appropriate time of the 24-hour light–dark cycle (Saper et al., 2005). Maintenance of wakefulness is dependent on several heterogeneous cell groups extending from the upper pons and midbrain (the so-called reticular activating system, RAS; Moruzzi and Magoun, 1949) to the posterior hypothalamus and basal forebrain. These cell groups are strategically placed so that they can release, over wide regions of the brain, neuromodulators and neurotransmitters that produce EEG activation, such as acetylcholine, hypocretin, histamine, norepinephrine, and glutamate. The main mechanism by which these neuromodulators and neurotransmitters produce cortical activation is by closing leakage potassium channels on the cell membrane of cortical and thalamic neurons, thus keeping cells depolarized and ready to fire. AC ET Y L C H O L I N E
Cholinergic cells are located in the basal forebrain and in two small nuclei in the pons: the pedunculopontine tegmental and lateral dorsal tegmental nuclei (PPT/LDT). Basal forebrain and pontine cholinergic cells fire at high rates in wakefulness and REM sleep and decrease or stop firing during NREM sleep. Pontine cholinergic cells project to the thalamus, where they help depolarize specific and intralaminar thalamic nuclei. The latter, which are dispersed throughout the thalamus and project diffusely to the cortex, fire at very high frequencies during wakefulness and REM sleep and help to synchronize cortical firing in the gamma (>28 Hz) range. Optogenetic stimulation of cholinergic cells in the basal forebrain promotes wake and decreases NREM sleep (Han et al., 2014; Xu et al., 2015). This effect is likely mediated by direct cortical cholinergic projections, as well as by the local release of acetylcholine in the basal forebrain, which leads to the activation of cortically projecting GABAergic neurons (Zant et al., 2016). Indeed, drugs with anticholinergic activity, including tricyclic antidepressants and atropine, can cause sedation and produce slow waves in the EEG (Domino et al., 1968). On the other hand, cholinergic agonists (e.g., nicotine) usually enhance arousal (Gillin et al., 2005). In patients with Alzheimer’s disease, loss of cholinergic cells is associated with slowing of the cortical EEG.
over-the-counter antihistaminergic drugs are used all over the world to facilitate the induction of sleep. G LU TA M AT E
Probably the largest contingent of the wakefulness-promoting system is made up by cells dispersed throughout the brainstem reticular formation and the basal forebrain that do not release conventional neuromodulators but rather the ubiquitous neurotransmitter glutamate (Brown et al., 2012). By binding to metabotropic receptors, glutamate can act as a neuromodulator and influence the excitability of target cells. Most glutamatergic neurons in the basal forebrain discharge at their fastest rates during wakefulness (a subgroup also during REM sleep), although some are most active during slow wave sleep (Xu et al., 2015). Extracellular glutamate levels in the cortex increase progressively during wakefulness and REM sleep (Dash et al., 2009), and optogenetic stimulation of glutamatergic neurons in the basal forebrain induces wakefulness (Xu et al., 2015). The wake-promoting effect of glutamate may also be indirect, via activation of hypothalamic neurons containing hypocretin and histamine. NOREPINEPHRINE
Noradrenergic cells are concentrated in the locus coeruleus in the upper pons, from where they project throughout the brain (Aston-Jones and Cohen, 2005; Berridge and Waterhouse, 2003). They fire tonically during wakefulness and emit short, phasic bursts of activity during behavioral choices or salient events, associated with increased cortical levels of noradrenaline (Aston-Jones and Bloom, 1981b, a). Noradrenergic cells start increasing their firing just before awakening (Takahashi et al., 2010), and their optogenetic stimulation reliably wakes up a mouse from both NREM sleep and REM sleep (Carter et al., 2010). The release of norepinephrine increases the response of cortical neurons to incoming stimuli and is essential, during wake, for the induction of genes involved in synaptic potentiation and thereby in learning (Cirelli et al., 1996). By contrast, locus coeruleus neurons decrease their firing during NREM sleep and cease firing altogether during REM sleep: in this way, neural activity during sleep does not translate into long-term synaptic potentiation, so we do not end up learning the wrong things and confuse dreams for reality.
H I S TA M I N E
Cholinergic neurons in the pons also project to the posterior hypothalamus, where histaminergic neurons are located in the tuberomammillary nucleus (Brown et al., 2001). Histaminergic neurons, which project throughout the cortex, fire at the highest rates during wakefulness and are inhibited during NREM and REM sleep (Takahashi et al., 2006). Upon awakening, however, they resume firing with some delay, suggesting that they are not necessary to initiate wakefulness (Takahashi et al., 2010). Still, they do have an important wakefulness-promoting function, most likely by activating glutamatergic neurons in thalamus and cortex and cholinergic neurons in the basal forebrain and pons. Indeed,
S E ROTO N I N
Serotoninergic cells from the dorsal raphé nucleus also project widely throughout the brain. Serotoninergic neurons, like noradrenergic neurons, fire at higher levels in waking, lower levels in NREM sleep, and fall silent during REM sleep. However, in contrast to noradrenergic neurons, serotoninergic neurons are inactive when animals make behavioral choices or orient to salient stimuli, and fire instead during repetitive motor activity such as locomoting, grooming, or feeding. The inactivity of serotonin cells during sleep may contribute to the sensory disconnection from the environment that occurs during sleep. Overall, serotonin has been shown to promote relaxed wake
• Charney, 132 S. E m erging and E stablished T echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis et al., Oxford University Press USA - OSO, 2018. 07:33:44.
with reduced cortical activation (it blocks fast rhythms such as theta and gamma) and to facilitate the onset of NREM sleep, at least in part by inhibiting the cholinergic system (Brown et al., 2012).
decreasing levels of acetylcholine and other wake-promoting neuromodulators and neurotransmitters lead to the opening of leak potassium channels in cortical and thalamic neurons, which become hyperpolarized and begin oscillating at low frequencies. The importance of hypothalamic structures for sleep D O PA M I N E induction was recognized at the beginning of the 20th cenAnother aminergic neuromodulator is dopamine (DA). tury during an epidemic of a viral infection of the brain called Dopamine-containing neurons located in the substantia nigra encephalitis lethargica. Von Economo concluded that if the and ventral tegmental area innervate the frontal cortex, basal infection destroyed the posterior hypothalamus, patients forebrain, and limbic structures (Monti and Monti, 2007). became indeed lethargic; but if the anterior hypothalamus was Unlike other aminergic cells, dopaminergic neurons do not lesioned, patients became severely insomniac (von Economo, appear to change their overall firing rate depending on behav- 1931). Subsequent studies confirmed that cell groups within ioral state. However, their bursting activity, which is known the anterior hypothalamus are involved in the initiation and to induce large synaptic DA release, increases during the con- maintenance of sleep. These groups include the ventrolateral sumption of palatable food and during REM sleep relative to preoptic area and other neurons scattered through the anteNREM sleep (Dahan et al., 2007). Moreover, lesions of areas rior hypothalamus, including the median preoptic nucleus. containing dopaminergic cell bodies in the ventral midbrain These neurons tend to fire during sleep and stop firing duror their ascending pathways can lead to loss of behavioral ing wakefulness. When they are active, many of them release arousal while maintaining cortical activation. Dopamine- γ-aminobutyric acid (GABA) and the peptide galanin, and containing neurons located in the ventral periaqueductal grey inhibit most wake-promoting areas including cholinergic, are also active in wake, and their lesion promotes sleep (Lu noradrenergic, histaminergic, hypocretinergic, and serotoet al., 2006). Finally, psychostimulants such as amphetamines nergic cells. In turn, the latter inhibit several sleep-promoting and cocaine that block reuptake of monoamines including neuronal groups (Brown et al., 2012). Many GABAergic neunorepinephrine, DA, and serotonin, promote prolonged rons are also located in the basal forebrain, but they do not wakefulness and increase cortical activation and behavioral form a homogenous population, some (somatostatin-positive) arousal (Monti and Jantos, 2008). Thus, the evidence for a being active in sleep and others (parvalbumin-positive) in role of dopamine as a wake-promoting neurotransmitter is wakefulness (Xu et al., 2015). Optogenetic or chemogenetic activation of GABAergic cells in the basal forebrain, many of substantial. which have long-range cortical projections, promote wakefulness and cortical activation (Anaclet et al., 2015; Kim et al., H Y P O C R ET I N 2015; Xu et al., 2015). The peptide hypocretin (also known as orexin) is produced by cells in the dorsolateral hypothalamus that provide excitT H E R E M S L E E P G E N E R ATO R atory input to all components of the waking system, most prominently the noradrenergic cells (Sakurai, 2007). Orexin Lesions in the dorsal part of the pons and in the ventral medulla cells, too, are most active during waking, especially in rela- eliminate REM sleep without significantly disrupting NREM tion to motor activity and exploratory behavior, and almost sleep, and a state characterized by muscle atonia and REMs stop firing during NREM and REM sleep. Specific activa- still persists after transections that eliminate all structures rostion of hypocretin cells, via optogenetic or pharmacogenetic tral to the pons, demonstrating that the brainstem is necessary stimulation, facilitates arousal and increases time spent awake and sufficient to initiate and maintain REM sleep ( Jouvet, (Adamantidis et al., 2007, Sasaki et al., 2011). Most patients 1962). Early studies in cats showed that the cholinergic agowith narcolepsy, a disorder characterized by excessive somno- nist carbachol greatly increases REM sleep when injected in lence and cataplectic attacks, have low or undetectable levels the dorsal pons, suggesting that cholinergic and cholinoceptic of hypocretin in the cerebrospinal fluid, and progressive elim- cells in this region are key players in the generation of REM ination of hypocretin cells in mice mimics many aspects of sleep. More recent studies in rodents, however, found that many glutamatergic and GABAergic cells in the brainstem are human narcolepsy (Tabuchi et al., 2014). maximally active in REM sleep (Boucetta et al., 2014). Thus, in the current model of REM sleep generation, glutamatergic H Y P OT H A L A MUS , BA S A L F O R E B R A I N, cells in the dorsal pons play a key role; they project rostrally A N D S L E E P to the intralaminar thalamic nuclei, the posterior hypothalaAs we seek a quiet, dark, and silent place to fall asleep and close mus, and the basal forebrain (EEG activation), and caudally to our eyes, the activity of the wake-promoting neuronal groups neurons in the ventral medulla that inhibit spinal motorneuis decreased because of reduced sensory input. In addition, rons through glycinergic and GABAergic projections (REM several of these brain areas are actively inhibited by antago- sleep atonia). The lateral and posterior hypothalamus also nistic neuronal populations located in the hypothalamus and includes many GABAergic cells that are active during REM basal forebrain, and become active at sleep onset. When the sleep, and some of them (~1/3) express the neuropeptide wake-promoting neuronal groups become nearly silent, the MCH (melanin-concentrating hormone). MCH neurons fire 11. Tethe N eurobiology S2018. lee Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, al., Oxford University Press USA -of OSO, 07:33:44.
exclusively during (but not before) REM sleep (Hassani et al., 2009), and their optogenetic stimulation increases REM sleep ( Jego et al., 2013). The remaining GABA+ neurons that do not express MCH fire maximally in REM sleep, and their firing increases progressively from quiet wake through NREM sleep, suggesting that they may be important to initiate REM sleep (Hassani et al., 2010). With the exception of the cholinergic system, wake-promoting neuronal groups—the noradrenergic, histaminergic, hypocretinergic, and serotonergic neurons—are inhibited during REM sleep and their reactivation may be a crucial step to end REM sleep. REM sleep can be eliminated by certain antidepressants, especially monoamine oxidase inhibitors. T H E C I RC A D I A N C L O C K
Circadin clocks have endogenous rhythms of ~24 hours that allow them to anticipate daily events. Clocks can be entrained by environmental signals (zeitgebers), the most potent of which is light. In mammals, the dominant circadian clock is the suprachiasmatic nucleus (SCN) of the hypothalamus, which regulates sleep/wake, core body temperature, heart rate and blood pressure, mental alertness, hormone secretion, and other rhythms. Like the SCN, most peripheral tissues also have a molecular clock, which can be viewed as a network of transcriptional, translational, and posttranslational positive and negative feedback loops that regulate the expression of core clock genes and output genes. SCN cells are, however, “special” because they receive direct photic inputs from the retina (SCN entrains to the light/dark cycle), and are internally coupled (synchronized to one another even in constant darkness). The strong coupling makes the SCN resistant to phase shifts due to changes in temperature (peripheral oscillators are instead very sensitive). SCN cells generate a strong circadian rhythm of neuronal firing, and through this output, mainly via hypothalamic and thalamic projections, they directly or indirectly synchronize other cells in the body (Mohawk et al., 2012). Overall, ~43% of all genes show circadian changes in expression in one or more tissues, and in each tissue the expression of up to 10% of genes is rhythmic (fewer in the brain). However, “rhythmic” genes in different tissues do not overlap, because they depend on the specific function of that tissue (Zhang et al., 2014). The SCN drives the 24-hour temperature cycle and uses it as a universal entrainment signal for peripheral tissues, likely via the transcription factor heat shock factor 1. In diurnal animals, the SCN activates wake- promoting areas and inhibits sleep-promoting areas during the day, maximally at the end of the day, whereas the converse is true at night. This makes it difficult to sleep in the early evening or to be awake in the early morning. In animals in which the SCN has been lesioned, sleep is no longer concentrated in one main episode but is dispersed across the entire 24-hour cycle. In humans living in isolation without time clues, the sleep/wake cycle can desynchronize from the core body temperature cycle driven by the SCN, so that the former becomes much longer or shorter than the latter. Under these conditions high core body temperature predicts a short sleep/wake cycle, and low core body temperature a long sleep/wake cycle (Daan et al., 2013).
HU M O R A L FAC TO R S
For a long time, it was assumed that sleep was mediated by the accumulation of some humoral factor during wakefulness—a kind of hypnotoxin. Many “sleep factors” have been identified in the past, including delta sleep–inducing peptide, uridine, muramyl dipeptide (aka factor S), and prostaglandin D2, but only a few have a well-defined role in sleep physiology. One of the best-studied substances is adenosine, a byproduct of brain metabolism that links neuronal activity with sleep (Brown et al., 2012). Glutamatergic activity increases adenosine levels, and systemic and central injections of adenosine or adenosine receptor agonists induce sleep and/or sleepiness. Adenosine levels in basal forebrain and cortex increase with time spent awake, and the increase in the basal forebrain is smaller after lesions of the cholinergic cells. The most widely used wake- promoting agent, caffeine, is an adenosine A1 and A2a receptor antagonist. Adenosine most likely promotes sleep through multiple mechansims, including the inhibition of wake-active cholinergic neurons, orexin neurons, and cortical glutamatergic neurons via A1 receptors, as well as the excitation of sleep-active neurons in the preoptic area via A2a receptors. Prostaglandin D2, another sleep-promoting substance acting on the prostaglandin D (PGD) receptor, indirectly activates adenosine A2A-dependent pathways in the basal forebrain (Huang et al., 2007). However, neither A1 nor PGD receptor knockout mice have abnormal baseline sleep. Similarly, a number of lymphokines, such as interleukin-1 (IL-1) and tumor necrosis factor (TNF) alpha, modulate sleep. These effects are often species-specific and could be most relevant in the context of acute inflammation or infection. However, the TNF and IL-1 type I receptor knockouts have abnormal sleep, suggesting also a role in baseline sleep regulation (Krueger et al., 2001). The pineal hormone melatonin is strongly regulated by the circadian clock and peaks at night in diurnal and nocturnal animals (it has been called the “darkness hormone”). Melatonin receptors are highly expressed in the SCN, and melatonin can help reset circadian rhythms and thereby influence sleep. Light and melatonin can be used to alleviate and correct circadian rhythm disorders and conditions such as jet lag and night shift work. Melatonin is also effective in regularizing the sleep–wake schedule of light-blind subjects whose sleep–wake periods tend to free-run, as well as in children and in the elderly with brain disorders, for example in the treatment of the “sundowning” often seen in dementia. S L E E P R EGU L AT I O N A N D S L E E P D E P R I VAT I O N
If we are not allowed to sleep and are forced to stay awake longer than usual, sleep pressure mounts and soon becomes overwhelming. Thus, sleep is homeostatically regulated: the more we stay awake, the longer and more intensely we sleep afterwards: arousal thresholds increase, there are fewer awakenings, and during NREM sleep the amplitude and prevalence of slow waves becomes much higher and there can be a rebound of REM sleep. Sleep pressure only diminishes if one is allowed to sleep, and the number and amplitude of sleep slow waves gradually diminishes (Figure 11.4).
• Charney, 134 S. E m erging and E stablished T echnologies Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis et al., Oxford University Press USA - OSO, 2018. 07:33:44.
6800
SWA 1200
Slow-wave activity (µV2)
10000 Fz Cz P4
8000
6000
4000
2000
0
0
2
4
6
8
Hours
Sleep slow waves as a marker of sleep pressure. Bottom panel: During early sleep, at the end of a day of wakefulness, sleep pressure is maximal. This is reflected in frequent and large sleep slow waves, measured here as slow wave activity (power in the 0.5–4 Hz band, in red for a frontal electroencephalogram (EEG) channel, green for a central channel, and blue for a posterior channel). During sleep, slow wave activity decreases exponentially, reflecting a reduction of sleep pressure. The transitory drops in slow wave activity correspond to episodes of rapid-eye-movement (REM) sleep. Top panel: Topographic display of slow wave activity over the scalp for the four sleep cycles. Notice the frontal predominance and the progressive decline in the course of the night. Figure 11.4
In humans, the most prominent effect of total sleep deprivation, and even of sleep restriction (for several nights), is cognitive impairment, with striking practical consequences (Killgore, 2010; Goel et al., 2013). A person who is sleep deprived tends to take longer to respond to stimuli, particularly when tasks are monotonous and low in cognitive demands. However, sleep deprivation produces more than just decreased alertness. Tasks emphasizing higher cognitive functions, such as logical reasoning, encoding, decoding, and parsing complex sentences; complex subtraction tasks; and tasks involving a flexible thinking style and the ability to focus on a large number of goals simultaneously, are all significantly affected even after one single night of sleep deprivation. Tasks requiring sustained attention, such as those including goal-directed activities, can be impaired by even a few hours of sleep loss. For example, medical interns made more frequent serious diagnostic errors when they worked frequent shifts of 24 hours or more than when they worked shorter shifts. Unfortunately, sleep deprived subjects underestimate the severity of their cognitive impairment, often with tragic consequences. Also, lack of sleep does not completely eliminate the capacity to perform but rather makes the performance inconsistent and unreliable. Thus, people may still be able to transiently perform at baseline levels in short tests even after three–four days of sleep deprivation. However, the same subjects will perform very poorly when
engaged in tasks requiring sustained attention. An important issue that remains unresolved is whether the cognitive impairment seen after sleep deprivation and sleep restriction is exclusively caused by sleepiness—the increasing internal pressure to fall asleep presumably mediated by the sleep-promoting areas discussed before—or to progressive cellular dysfunctions in cortical and other circuits that have been awake too long, a veritable form of neuronal tiredness. Performance deficit after sleep loss shows large interindividual variability, some of which is due to genetic factors (Kuna et al., 2012). It should be mentioned that several well-controlled studies have discredited the once-popular notion that loss of REM sleep might lead to psychosis and suicide. Indeed, REM sleep deprivation, as well as total sleep deprivation or selective slow wave deprivation, improves mood in approximately 50% of people who are depressed (Hemmeter et al., 2010; Landsness et al., 2011). N E U R A L C O R R E L AT E S O F WA K E F U L N E S S A N D S L E E P Wakefulness and NREM and REM sleep are accompanied by distinctive molecular changes, changes in spontaneous neural activity and metabolism, and responsiveness to stimuli.
11. Tethe N eurobiology S2018. lee Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, al., Oxford University Press USA -of OSO, 07:33:44.
MO L E C U L A R C H A N G E S I N N EU RO NS A N D G L I A
Several studies in the past 15 years measured gene expression in brain homogenates that contain both neurons and glia, and found that ~5% of all transcripts (messenger ribonucleic acids [mRNAs]) change with sleep and wake. Hundreds of mRNAs are expressed at higher levels in the waking brain, and different sets of transcripts are expressed at higher levels in sleep (Cirelli, 2009). Transcripts upregulated in the cerebral cortex during wakefulness code for proteins that help the brain to face high- energy demand, high synaptic excitatory transmission, and high transcriptional activity, as well as the cellular stress that may derive from one or more of these processes. Moreover, wakefulness is associated with the increased expression of several genes that are involved in long-term potentiation of synaptic strength (Cirelli et al., 1996), and one of the underlying mechanisms, as discussed before, is the release of norepinephrine, which is high during wakefulness, when animals make decisions and learn about the environment, but is low during sleep. By contrast, the genes that increase their expression during sleep include several that may be involved in long-term depression of synaptic strength and possibly in synaptic consolidation (Cirelli, 2009). Other sleep-related genes appear to favor the rate of protein synthesis, which is also increased in sleep. Finally, many sleep-related genes play a significant role in membrane trafficking and maintenance. Thus, these findings suggest that although sleep is a state of behavioral inactivity, it is associated not only with intense neural activity, but also with the increased expression of many genes that may favor specific cellular functions. More recent experiments assessed the effects of sleep and wake on specific cell types using TRAP (translating ribosome affinity purification) technology combined with microarrays. One study found that 2.1% of the genes expressed in oligodendrocytes are modulated by behavioral state: genes upregulated during wake are preferentially involved in apoptosis and cellular stress response, as well as cell differentiation and development. Oligodendrocytes may be especially vulnerable to cellular stress because they are among the metabolically most active cells in the brain, with high rates of synthetic activity required to produce and maintain vast amounts of myelin. Genes upregulated during sleep instead are involved in lipid metabolism (including phospholipid synthesis and myelination) in mature cells, and in cell proliferation in immature oligodendrocytes (Bellesi et al., 2013). Indeed, the proliferation of oligodendrocyte precursor cells (OPC) doubles during sleep, whereas OPC differentiation is higher during wake (Bellesi et al., 2013). Another study focused on astrocytes and found that their number of state-dependent genes is smaller (1.4%) than in oligodendrocytes, and more than seven-fold higher in wake than in sleep (396 vs. 55 genes) (Bellesi et al., 2015). Many astrocytic genes modulated by behavioral state are related to the extracellular matrix and/or the cytoskeleton, suggesting that astrocytic pathways involved in cytoskeleton modification and elongation of peripheral astrocytic processes are modulated by sleep and wake. This prediction was confirmed using serial block-face scanning electron microscopy: a few hours of
wakefulness are sufficient to bring astrocytic processes closer to the synaptic cleft, while chronic sleep restriction also extends the overall astrocytic coverage of the synapse, including at the axon/spine interface, and increases the available astrocytic surface in the neuropil (Bellesi et al., 2015). These changes likely reflect the housekeeping functions of astrocytes, from glutamate clearance to maintenance of ionic balance in the extracellular space, and suggest that the need for these functions increases with wakefulness, especially prolonged wakefulness. S P O N TA N E O U S N E U R A L AC T I VI T Y WA K E F U L N E S S
The waking EEG, characterized by the presence of low-voltage fast- activity, is known as activated because most cortical neurons are steadily depolarized close to their firing threshold (Figure 11.5A), and are thus ready to respond to the slightest change in their inputs. The steady depolarization is caused by the release of acetylcholine and other neurotransmitters and neuromodulators, which close leakage potassium channels on the membrane of cortical neurons. The readiness to respond of cortical and thalamic neurons enables fast and effective interactions among distributed regions of the thalamocortical system, resulting in a continuously changing sequence of specific firing patterns. Because these firing patterns are not globally synchronous across the cortex, the EEG displays rapid fluctuations of low amplitude rather than high-voltage, low-frequency waves. Nevertheless, superimposed on the low-voltage, fast-activity background of wakefulness one frequently observes rhythmic oscillatory episodes within the alpha (8–13 Hz), beta (14–28 Hz), and gamma (>28 Hz) range, which are usually localized to specific cortical areas. These waking rhythms are due to the activation of oscillatory mechanisms intrinsic to each cell, as well as to the entrainment of oscillatory circuits among excitatory and inhibitory neurons. N R E M S L E E P
The EEG of NREM sleep is characterized by the occurrence of slow waves (aka delta waves; 50%) of the lifetime low or questionable severity or duration. When present, halduration of illness to warrant the diagnosis of schizoaffective lucinations are rated 2 if they are mild, which indicates there disorder. Especially this last change is intended to improve diag- is little pressure to act upon voices or the patient is not very nostic reliability (which was quite poor for schizoaffective dis- bothered by the voices; 3 if the voices are moderate, with some order in the past, given the imprecise and variably interpreted pressure to respond to the voices or being somewhat bothered requirement that a mood episode was present “for a substantial by them, and 4 if they are severe, with pressure to respond to part” of the overall duration of illness (American Psychiatric voices or being very bothered by voices. Symptoms that are Association, 2000: p. 323). No single psychotic symptom or ill- only rated as equivocal do not meet the all-or-none criteria ness feature can be used to distinguish who will receive a diag- for inclusion within the categorical disorders. By contrast, the nosis of a bipolar or other psychotic affective disorder versus a information conveyed by the categorical diagnosis of a psyschizophrenia spectrum psychosis; the diagnostic distinctions chotic condition only indicates that the patient minimally of the psychoses in the DSM-5 entail the clinician’s determi- experienced delusions, hallucinations, or disorganized speech, nation of the relative duration and overlap of any manic and/ and additionally either had another of these symptoms or had or depressive episodes as they occurred with psychotic symp- grossly abnormal psychomotor behavior such as catatonia, or toms (of course this process presumes that medical, substance- a negative symptom of restricted affect or avolition/asociality. The addition of the dimensional assessments yields clinrelated, and other exclusionary causes of psychosis have been ruled out). The overlap of bipolar and schizophrenia conditions ically important information on the presence and severity is certainly evident in the frequent shift of an individual’s diag- of these and other common symptoms that can be used for nosis among schizophrenia, bipolar or other affective psychosis. the planning and evaluation of treatment interventions and The revised diagnostic criteria will not eliminate such longitu- for prognosis. The pattern and changes in symptoms are also dinal instability, but the cross-sectional reliability of diagnoses expected to be useful to designing person-specific treatments made by different clinicians is expected to improve. Specifically, and to shed light on etiological factors and neural circuitry it is expected that fewer schizophrenia cases should be misdiag- that can be targeted by novel treatments. nosed as having schizoaffective disorder. Other changes in the DSM-5 include an elevation of the T H E M A J O R R AT I N G S C A L E S catatonia concept in the schiozophrenia spectrum chapter, F O R P SYC H I AT R I C D I AG N O S I S such that the condition may stand on its own or accompany a host of other conditions (including both psychotic and affective disorders) (see Tandon, Heckers, et al., 2013), and the Distinguishing between different psychotic illnesses in a reliinclusion of increased energy/activity as a core symptom of able way is often challenging for clinicians and researchers. Manic and Hypomanic Episodes in the bipolar spectrum chap- Numerous structured and semistructured diagnostic interter. Attenuated Psychosis Syndrome is added to Section III views have been developed to provide standardized ways for (“Emerging Measures and Models”) as a condition for fur- clinicians to collect the information necessary to make a differther study in an effort to better understand the adolescent ential diagnosis, thus increasing reliability across clinician diagand young adult transitions to psychotic disorders (see Tsuang noses. The most common of these interviews are the Structured et al., 2013). Included in Section III is also a proposed dimen- Clinical Interview for DSM Disorders (SCID; Spitzer et al., 1992), the Diagnostic Interview for Genetic Studies (DIGS; sional framework for assessment of psychosis. • P sychotic D isorders Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et156 al., Oxford University Press USA - OSO, 2018. 07:34:22.
Nurnberger et al., 1994), and the Schedule for Affective Disorders and Schizophrenia (SADS; Endicott and Spitzer, 1978), all of which have demonstrated reliability (Keller et al., 1981; Lobbestael et al., 2011; Nurnberger et al., 1994). While these interviews all provide structured questions and prompts aimed at gathering the same basic data (e.g., identifying information, developmental history, psychiatric history, medical history, and current symptomatology), the interviews differ in the diagnostic criteria to which the information corresponds. For example, the SCID was initially developed based on DSM-III criteria and had to be revised following the publication of the DSM-IV in 2000 and the DSM-5 in 2013. Similarly, the SADS was developed based on the Research Diagnostic Criteria (RDC). As a result, the SCID most directly corresponds to DSM criteria and the SADS most directly corresponds to the RDC criteria, which may present a challenge for clinicians who want to apply the information obtained from these interviews to a different set of diagnostic criteria. An advantage that the DIGS has over the other two interviews is that the questions and prompts were written to collect information that allows clinicians to make diagnoses based on multiple diagnostic criteria. The OPerational CRITeria (OPCRIT; Craddock et al., 1996), which is embedded in the DIGS, is a checklist of criteria from all of the major diagnostic classification systems that can be entered into computerized software, which then allows for the generation of diagnoses across the major diagnostic systems. This system allows for easy, standardized, and reliable comparison of diagnosis across multiple diagnostic systems and has demonstrated good to excellent agreement with multiple clinician consensus diagnoses. RESE ARCH DOMAIN CRITERIA : T H E F U T U R E O F P SYC H I AT R I C D I AG N O S I S ? The established diagnostic systems are plagued by phenomenological, genetic, neurobiological, and epidemiological heterogeneity within, and overlap between, the schizophrenia and bipolar-related disorders. DSM/ICD diagnoses are merely syndromes— observable phenomena organized by expert consensus—but have been accepted by the clinical, research, and lay communities as real disease entities (for further discussion, see Kozak and Cuthbert, 2016). Reification of these provisional constructs has led to the often false assumption of unitary pathophysiology and psychopathology, but the search for underlying etiology has yielded neurobiological and genetic findings that do not always map in one-to-one fashion onto existing diagnoses (for example, some genetic risk factors for schizophrenia have been found to overlap with those for BPD, MDD, intellectual disability, and autism) (Fanous, 2016). Further, the categorical nature of the DSM/ICD systems leads to dismissal of subsyndromal presentations and obscures the dimensional nature of symptoms associated with psychosis. As discussed above, the DSM-5 attempts to address dimensionality with the Clinician-Rated Dimensions of Psychosis Symptom Severity included in Section III, but critics assert that the relatively coarse level of granularity of the measures
assessed may make them difficult to correlate with underlying etiological mechanisms (for instance, hallucinations are found across several disorders, including schizophrenia, OCD, and some borderline states, and differ in their phenomenology and likely etiology) (see Cuthbert and Insel, 2013). The Research Domain Criteria (RDoC) is the response of the NIMH to the perceived lack of validity of the current categorical diagnostic systems (in contrast, to the aforementioned RDC aimed to address reliability). The intent is to provide a framework for research that will elucidate causal relationships and yield biomarkers that could allow for person-specific treatment; RDoC is not intended for clinical application. For more information about the development and structure of RDoC, the reader is referred to Chapter 71 later in this volume. Briefly, the initiative aims to deconstruct the categorical mental illnesses into their component dimensions of observable behavior and neurobiological measures, thereby freeing the research community from “diagnostic orthodoxy” (see discussion in Cuthbert and Insel, 2013). RDoC is organized around five provisional “domains” of psychological and behavioral function: Positive Valence (systems that respond to positive stimuli/contexts), Negative Valence, Cognitive Systems, Social Processes, and Arousal and Regulatory Systems. These domains are further composed of proposed “constructs”—that is, units of behavioral or cognitive function that correspond to a known neural circuit or specific biological system. The constructs are to be measured at various “units of analysis” including genes, molecules, circuits, physiology, behavior, and self-report. The resulting “matrix” is available publicly on the NIMH website and is seen as a work in progress, with research to fill in squares as well as to amend, add, or remove constructs. The critical influences of neurodevelopment and the environment on normal and pathological function is emphasized by the inclusion of these as “axes” in the RDoC classification system (www.nimh.gov). How can RDoC be applied to our understanding of schizophrenia and related psychoses? The RDoC framework encourages exploration of neurobehavioral constructs along the full spectrum of function. Its explicit dimensionality and lack of delineation between healthy and diseased states intends to accommodate heterogeneity within existing disease classifications as well as to recognize etiological continuity of traits appearing in healthy and diseased individuals (see discussion in Fanous, 2015). Cognitive impairment and depression are two symptoms found in psychotic individuals that are clearly also found in patients with nonpsychotic mental illness and to varying degrees in individuals with no diagnosable illness; even starkly abnormal symptoms including delusions and hallucinations are found in lesser forms (i.e., unusual thoughts and perceptual disturbances) in nonpsychotic individuals. Experimental paradigms that conform to RDoC concepts will use one or multiple neurobehavioral constructs to explore a clinically important, generally narrow aspect of psychotic phenomena, ideally recruiting a study population that represents the full dimension of the neurobehavioral construct (rather than the traditional Diagnosis vs. Healthy Controls). The hope is that RDoC-generated knowledge could inform diagnostic criteria and boundaries in the near term (for modest revisions of the current system: DSM 5.1, 5.2, etc.) and in
12. Det iagnosis andPress E pide io2018. l ogy Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, al., Oxford University USA - m OSO, 07:34:22.
the longer term could lead to a more biologically based diagnostic system. The first RDoC grants were founded in 2012, and it remains to be seen whether the framework will generate findings useful for treatment and prevention of psychotic illness. Critics have pointed out the challenges of applying RDoC to the psychoses (Carpenter, 2016;Weinberger, 2015). While it is intuitive that disruptions in the RDoC domains of cognitive systems and positive valence could, respectively, lead to cognitive impairment and the negative symptom of anhedonia, it is less clear which domains/constructs are relevant to the understanding of psychotic symptoms such as paranoid delusions or auditory hallucinations (the latter of which likely involves disruptions in the domains/constructs of cognitive systems/ perception, cognitive systems/language, social processes/perception and understanding of self, negative valence/ acute threat, and others . . . ). Furthermore, although studying symptoms in samples that cross diagnostic boundaries is a possible benefit of the RDoC framework, it is not clear that this will yield treatment advances. For example, while a study involving the fear construct of the negative valence domain may find similar findings across multiple units of analysis (circuits, behavior, etc.) in both psychotic and anxious patients, clinical psychopharmacologic experience has suggested that anxiety is treated differently in the two populations. Etiological continuity between conditions does not necessarily translate to clinical utility. Schizophrenia and bipolar disorder have been shown to share some genetic susceptibilities; so, however, have Crohn disease and multiple sclerosis, yet we know that both the pathophysiology and treatments for these conditions diverge widely (see further discussion in Weinberger et al., 2015). Note that RDoC is not the only approach to deconstructing conventional categories of psychotic disorders. One example of promising “endophenotype” work comes from the Bipolar- Schizophrenia Network on Intermediate Phenotypes, which has distinguished subtypes of psychosis using neurobiological measures rather than clinical features. Among a group of subjects meeting DSM criteria for schizophrenia, schizoaffective disorder, or bipolar disorder with psychotic features, the investigators delineated three brain-based psychosis biotypes using heterogeneity in a panel of neurobiological measures (including cognitive tests, pro-and anti-saccade tasks, EEG, MRI). The biotypes were distinguished by multivariate biomarker measures termed cognitive control and sensorimotor reactivity, and outperformed DSM diagnostic classes in between-group divergence of external measures including social functioning, brain structure, and characteristics of biological relatives (Clementz et al., 2016).
are numerous epidemiological studies of the schizophrenia- related disorders, but the incidence and prevalence of psychotic affective disorders are typically subsumed under depression or bipolar disorder without regard to psychotic features, further confounding knowledge about the origins and risk factors for psychosis across disorders. Estimates for the lifetime prevalence of schizophrenia range from 0.3%–0.7%, with a recent systematic review of population-based studies reporting median estimate of lifetime prevalence of 0.48% (IQR = 0.34%–0.85%) (McGrath et al., 2008; Simeone et al., 2015). Previously the worldwide prevalence of schizophrenia was commonly reported to be 1%, but this statistic obscures the substantial local differences in the risk for the disorder as well as the variation that is associated by race/ethnicity, immigration, and other risk factors. The peak age of onset for the first psychotic episode in schizophrenia is early to mid-20s for men and late 20s for women. Women also have a second midlife peak after 40 years (these late-onset cases tend to differ phenomenologically, with relative prominence of positive symptoms and preserved social/ affective functioning) (McGrath et al., 2008). The majority of individuals gradually develop symptoms including depression and/or cognitive impairment prior to the first psychotic episode. The course and outcome is variable and generally worse in men, who have on average lower premorbid adjustment and more prominent negative and cognitive symptoms (Álvarez- Jiménez et al., 2012). All but a small number of cases have a chronic course; some experience series of decompensations and remissions, and others a progressive decline. Psychotic symptoms may sometimes lessen with aging, but negative symptoms and cognitive deficits remain (Tamminga et al., 1998). Schizoaffective and bipolar disorders also generally emerge in young adulthood, but onset can range across lifespan (DSM-5). The Kraepelin distinction between schizophrenia and bipolar disorder that remains even in the DSM-5 is largely based on the episodic course and better prognosis of the latter, but many individuals with bipolar disorder also exhibit functional deficits, including cognitive, interpersonal, and occupational impairments between affective episodes, and deterioration over time (Schoeyen et al., 2011). In general, individuals with schizoaffective disorder have a better prognosis than those with schizophrenia, but worse than those with bipolar disorder (Harrow et al., 2000). In the DSM-5, specific criteria for distinguishing schizoaffective disorder from schizophrenia are introduced for the first time, specifying that mood symptoms meeting full criteria for an affective syndrome must be present for a majority of the total life-course duration of psychosis for a case to be diagnosed with a schizoaffective disorder instead of schizophrenia. This change is in acknowledgement that the E P I D E M I O L O GY largest proportions of schizophrenia cases also have mood disO F P SYC H OT I C D I S O R D E R S orders. (Malaspina et al., 2013). Males have an earlier average age of onset of schizophrenia The most common forms of psychosis are the schizophrenia- related conditions and psychotic affective disorders, particu- and show more negative symptoms. Studies that emphasize larly bipolar disorder with psychosis. The best fitting diagnosis negative symptoms and a shorter duration of illness are biased for a person with psychosis can change over time, termed diag- toward finding more male cases, whereas those focused on nostic instability, and the diagnosis at any given time can fur- cases with a shorter duration of illness or affective symptoms thermore demonstrate substantial confusability, even with demonstrate equal sex ratios (Roy et al., 2001; Beauchamp and the use of structured interviews (Faraone et al., 1996). There Gagnon, 2004).
• P sychotic D isorders Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et158 al., Oxford University Press USA - OSO, 2018. 07:34:22.
Schizoaffective disorder shows a lifetime prevalence of 0.3%, being about one-third as common as schizophrenia, showing a higher incidence in females due to their more frequent incidence of depression (Perälä et al., 2007). Bipolar I disorder has a lifetime prevalence of 0.6% with a slightly higher prevalence in males (1.1:1) (Merikangas et al., 2011). However, estimating the prevalence of the affective psychoses is difficult, as described, since most epidemiological studies are conducted by DSM diagnoses and do not include the “with psychotic features” specifier. Studies have suggested a number of genetic, physiologic, and environmental risk factors for the psychosis. These include shared and distinct genetic susceptibilities for schizophrenia, schizoaffective disorder, and bipolar disorder, with some risk alleles being more broadly associated with depression, autism spectrum disorder, and intellectual disability (Smoller et al., 2013; Mortensen et al., 2010). Having a family member with schizophrenia, schizoaffective disorder, or bipolar disorder increases the risk for other conditions in first-degree relatives (VanSnellenberg and deCandia, 2009; Laursen et al., 2005). More specific environmental risk factors include growing up in an urban environment for schizophrenia (March et al., 2008) and having a higher family income for bipolar disorder (Ormel et al., 2008). Some shared risk factors for schizophrenia-related disorders and psychotic affective disorders include obstetric complications, premorbid childhood psychopathology, cognitive deficits, and motor dysfunction (Laurens et al., 2015). Later paternal age, a well-known risk factor for schizophrenia, is strongly associated with psychotic bipolar disorder but is unrelated to nonpsychotic bipolar disorder (Lehrer et al., 2015). The available findings suggest that there is continuity between schizophrenia and psychotic affective disorders, even if the risk factors for nonpsychotic affective disorders are dichotomous. The rarity of data that separately considered psychotic affective disorders is a major roadblock to advancing our knowledge about the specific etiopathologies for psychosis that cut across disorders. C O N C LU S I O N Over the past century there have been shifts in the understanding of psychotic symptoms with respect to the affective and nonaffective psychosis. While Kraepelin proposed dichotomous underpinnings for these psychoses, a unitary model is receiving more emphasis, in which psychosis has a common neurobiological origin as it manifests across a broad range of separate psychiatric disorders. By contrast, current diagnostic criteria (DSM-5 and ICD-10) remain consistent with Kraepelin’s dichotomy and the Feighner Criteria in distinguishing between primary psychotic illnesses (e.g., schizophrenia) and the functional/affective psychoses. The robust evidence of overlap is manifested in the many individuals with schizoaffective disorder, who meet criterion A for schizophrenia and criteria for affective episodes amounting to more than half of the total course of the disorder in DSM-5. Earlier DSM editions were more vague about the overlap of psychotic and affective conditions that comprised schizoaffective disorder. DSM-5 recognizes that most persons
with schizophrenia will have some affective episodes, reserving the schizoaffective diagnosis for instances when the course is predominated by overlapping psychotic and affective symptoms. New behavioral domain approaches to psychopathology research, such as the NIMH’s RDoC initiative, will provide approaches to assessment that are not bound by diagnostic categories, which may clarify these diagnostic categories over time and provide treatment targets for psychosis across conditions. DISCLOSURES The chapter authors have no conflicts of interest to disclose. REFERENCES Álvarez-Jiménez, M., Gleeson, J.F., et al. (2012). Road to full recovery: longitudinal relationship between symptomatic remission and psychosocial recovery in first-episode psychosis over 7.5 years. Psychol Med 42(3):595–606. American Psychiatric Association. (1952). Diagnostic and Statistical Manual of Mental Disorders, 1st Edition. Washington, DC: Author. American Psychiatric Association. (1968). Diagnostic and Statistical Manual of Mental Disorders, 2nd Edition. Washington, DC: Author. American Psychiatric Association. (1980). Diagnostic and Statistical Manual of Mental Disorders, 3rd Edition. Washington, DC: Author. American Psychiatric Association. (1994). Diagnostic and Statistical Manual of Mental Disorders, 4th Edition. Washington, DC: Author. American Psychiatric Association. (2000). Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision. Washington, DC: Author. American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders, 5th Edition. Washington, DC: Author. Andreasen, N.C., Arndt, S., et al. (1995). Symptoms of schizophrenia: methods, meanings, and mechanisms. Arch Gen Psychiatry 52:341–351. Andreasen, N.C. (2007). DSM and the death of phenomenology in America: an example of unintended consequences. Schizophr Bull 33: 108–112. Barch, D.M., Bustillo, J., et al. (2013). Logic and justification for dimensional assessment of symptoms and related clinical phenomena in psychosis: relevance to DSM-5. Schizophr Res 150(1):15–20. Beauchamp, G., and Gagnon, A. (2004). Influence of diagnostic classification on gender ratio in schizophrenia— a meta- analysis of youths hospitalized for psychosis. Soc Psychiatry Psychiatr Epidemiol 39(12):1017–1022. Burgy, M. (2008). The concept of psychosis: historical and phenomenological aspects. Schizophr Bull 34:1200–1210. Carpenter, W.T. (2016). The RDoC Controversy: Alternate paradigm or dominant paradigm? Am J Psychiatry 173(6):562–563. Cheniaux, E., Landeira-Fernandez, J., et al. (2009). The diagnoses of schizophrenia, schizoaffective disorder, bipolar disorder and unipolar depression: interrater reliability and congruence between DSM-IV and ICD-10. Psychopathology 42:293–298. Clementz, B.A., Sweeney, J.A., et al. (2016). Identification of distinct psychosis biotypes using brain-based biomarkers. Am J Psychiatry 173(4):373–384. Craddock, M., Asherson, M.P., et al. (1996). Concurrent validity of the OPCRIT diagnostic system: comparison of OPCRIT diagnoses with consensus best-estimate lifetime diagnoses. Br J Psychiatry 169:58–63. Crow, T.J. (1995). A continuum of psychosis, one human gene, and not much else—the case for homogeneity. Schizophr Res 17(2):135–145. Cuthbert, B.N. (2015). Research Domain Criteria: toward future psychiatric nosologies. Dialogues Clin Neurosci 17(1):89–97.
12. Det iagnosis andPress E pide io2018. l ogy Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, al., Oxford University USA - m OSO, 07:34:22.
Cuthbert, B.N., and Insel, T.R. (2013). Toward the future of psychiatric diagnosis: the seven pillars of RDoC. BMC Med 11:126. Endicott, J., and Spitzer, R.L. (1978). A diagnostic interview: the schedule for affective disorders and schizophrenia. Arch Gen Psychiatry 35:837–844. Fanous, A.H. (2015). Can genomics help usher schizophrenia into the age of RDoC and DSM-6? Schizophr Bull 41(3):535–541. Faraone, S., Blehar, M., et al. Diagnostic accuracy and confusability analyses: an application to the Diagnostic Interview for Genetic Studies. (1996). Psychol Med 26(2):401–410. Feighner, J.P., Robins, E., et al. (1972). Diagnostic criteria for use in psychiatric research. Arch Gen Psychiatry 26:57–63. Harrow, M., Grossman, L.S., et al. (2000). Ten-year outcome: patients with schizoaffective disorders, schizophrenia, affective disorders and mood-incongruent psychotic symptoms. Br J Psychiatry 177:421–426. Heckers, S., Barch, D.M., et al. (2013). Structure of the psychotic disorders classification in DSM-5. Schizophr Res 150(1):11–14. Ivleva, E., Thaker, G., et al. (2008). Comparing genes and phenomenology in the major psychoses: schizophrenia and bipolar 1 disorder. Schizophr Bull 34:734–742. Jager, M., Haack, S., et al. (2011). Schizoaffective disorder—an ongoing challenge for psychiatric nosology. Eur Psychiatry 26:159–165. Javitt, D.C. (2016). Biotypes in psychosis: has the RDoC era arrived? Am J Psychiatry 173(4):313–314. Kasanin, J. (1933). The acute schizoaffective psychoses. Am J Psych 90:97–126. Keller, M.B., Lavori, P.W., et al. (1981). Test-retest reliability of assessing psychiatrically ill patients in a multi-center design. J Psychiat Res 16:213–227. Kozak, M.J., and Cuthbert, B.N. (2016). The NIMH Research Domain Criteria Initiative: background, issues, and pragmatics. Psychophysiology 53(3):286–297. Laurens, K.R., Luo, L., et al. (2015). Common or distinct pathways to psychosis? A systematic review of evidence from prospective studies for developmental risk factors and antecedents of the schizophrenia spectrum disorders and affective psychoses. BMC Psychiatry 15:205. Laursen, T.M., Labouriau, R., et al. (2005). Family history of psychiatric illness as a risk factor for schizoaffective disorder: a Danish register- based cohort study. Arch Gen Psychiatry 62(8):841–848. Lehrer, D.S., Pato, M.T., et al. (2016). Paternal age effect: replication in schizophrenia with intriguing dissociation between bipolar with and without psychosis. Am J Med Genet B Neuropsychiatr Genet 171(4):495–505. Lobbestael, J., Leurgans, M. et al. (2011). Inter-rater reliability of the Structured Clinical Interview for DSM-IV Axis I Disorders (SCID I) and Axis II Disorders (SCID II). Clin Psychol Psychother 18:75–79. Malaspina, D., Owen, M.J., et al. (2013). Schizoaffective disorder in the DSM-5. Schizophr Res 150(1):21–25. March, D., Hatch, S.L., et al. (2008). Psychosis and place. Epidemiol Rev 30:84–100. McGrath, J., Saha, S., et al. (2008). Schizophrenia: a concise overview of incidence, prevalence, and mortality. Epidemiol Rev 30:67–76. Merikangas, K.R., Jin, R., et al. (2011). Prevalence and correlates of bipolar spectrum disorder in the world mental health survey initiative. Arch Gen Psychiatry 68(3):241–251. Moller, H.J. (2003). Bipolar disorder and schizophrenia: distinct illnesses or a continuum? J Clin Psychiatry 64(Suppl 6):23–27. Mortensen, P.B., Pedersen, M.G., and Pedersen, C.B. (2010). Psychiatric family history and schizophrenia risk in Denmark: which mental disorders are relevant? Psychol Med 40(2): 201–210.
Nurnberger, J.I., Blehar, M.C., et al. (1994). Diagnostic interview for genetic studies: rationale, unique features, and training. Arch Gen Psychiatry 51:849–859. Ormel, J., Petukhova, M., et al. (2008). Disability and treatment of specific mental and physical disorders across the world. Br J Psychiatry 192(5):368–375. Owen, M.J., Craddock, N., and O’Donovan, M.C. (2010). Suggestion of roles for both common and rare risk variants in genome-wide studies of schizophrenia. Arch Gen Psychiatry 67(7):667–673. Perälä, J., Suvisaari, J., et al. (2007). Lifetime prevalence of psychotic and bipolar I disorders in a general population. Arch Gen Psychiatry 64(1):19–28. Research Domain Criteria (RDoC). National Institute of Mental Health. https://www.nimh.nih.gov/research-priorities/rdoc/index.shtml. Accessed June 2016. Roy, M.A., Maziade, M., et al. (2001). Male gender is associated with deficit schizophrenia: a meta-analysis. Schizophr Res 47(2-3):141–147. Schneider, K. (1959). Clinical psychopathology. New York: Grune & Stratton. Schoeyen, H.K., Birkenaes, A.B., et al. (2011). Bipolar disorder patients have similar levels of education but lower socio-economic status than the general population. J Affect Disord 129(1-3):68–74 Simeone, J.C., Ward, A.J., et al. (2015). An evaluation of variation in published estimates of schizophrenia prevalence from 1990–2013: a systematic literature review. BMC Psychiatry 15:193. Smoller, J.W., Craddock, N., et al. (2013). Identification of risk loci within shared effects on five major psychiatric disorders: a genome-wide analysis. Lancet 381(9875):1371–1379. Spitzer, R.L., Endicott, J., et al. (1970). The psychiatric status schedule: a technique for evaluating psychopathology and impairment in role functioning. Arch Gen Psychiatry 23:41–55. Spitzer, R.L., Endicott, J., et al. (1978). Research diagnostic criteria: rationale and reliability. Arch Gen Psychiatry 35:773–782. Spitzer, R.L., Williams, J.B., et al. (1992). The structured clinical interview for DSM-III-R (SCID). I: History, rationale, and description. Arch Gen Psychiatry 49:624–629. Tamminga, C.A., Buchanan, R.W., et al. (1998). The role of negative symptoms and cognitive dysfunction in schizophrenia outcome. Int Clin Psychopharmacol 13 (Suppl 3):S21–S26. Tandon, R., Gaebel, W., et al. (2013). Definition and description of schizophrenia in the DSM-5. Schizophr Res 150(1):3–10. Tandon, R., Heckers, S., et al. (2013). Catatonia in DSM-5. Schizophr Res 150(1):26–30. Tsuang, M.T., Van Os, J., et al. (2013). Attenuated psychosis syndrome in DSM-5. Schizophr Res 150(1):31–5. Van Snellenberg, J.X., and de Candia, T. (2009). Meta-analytic evidence for familial coaggregation of schizophrenia and bipolar disorder. Arch Gen Psychiatry 66(7):748–755. Weinberger, D.R., Glick, I.D., and Klein, D.F. (2015). Whither Research Domain Criteria (RDoC)?: the good, the bad, and the ugly. JAMA Psychiatry 72(12):1161–1162. Wing, J.K., Cooper, J.E., et al. (1974). Present state examination. London: Cambridge University Press. World Health Organization. (1992a). Classification of mental and behavioural disorders, clinical descriptions and diagnostic guidelines. Geneva: Author. World Health Organization. (1992b). International statistical classification of diseases and related health problems (ICD-10), tenth revision. Volumes 1–3. Geneva: Author. Zubin, J., and Gurland, B.J. (1977). The United States–United Kingdom project on diagnosis of the mental disorders. Ann NY Acad Sci 285:676–686.
• P sychotic D isorders Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et160 al., Oxford University Press USA - OSO, 2018. 07:34:22.
13. GENETICS OF SCHIZOPHRENIA AND BIPOLAR DISORDER Alexander Charney and Pamela Sklar
INTRODUCTION This chapter provides an overview of the genetics of schizophrenia and bipolar disorder. The evolution of genetic information has rapidly expanded over the last century or so, from epidemiological observations of families and twins to genetic linkage and positional cloning in pedigrees, candidate gene association studies, and finally the genome-wide microarray and sequencing studies of the current genomic era. The latter have provided important new insights, and we can expect this expansion in genetic knowledge to continue and likely escalate. This chapter will cover information supporting several basic ideas. First, that there is strong and consistent evidence that both disorders are genetic. Second, neither disorder is caused by a single abnormal gene. Third, biological candidate genes and traditional linkage studies proved inadequate to identify genetic causes for reasons that are now largely understood. Fourth, copy number variation plays an important role in schizophrenia but less so in bipolar disorder. Fifth, genome-wide association studies have identified multiple significant loci for schizophrenia and bipolar disorder. Sixth, next generation sequencing studies are beginning to catalogue rare variants and their potential role in schizophrenia and bipolar disorder. Seventh, fine mapping, gene expression, and epigenomic studies are leading to mechanistic insights for GWAS and other associated loci. Finally, integration of all of the various sources of genetic risk information will be difficult and will require interdisciplinary work and new biological strategies. G E N ET I C E P I D E M I O L O GY Schizophrenia and bipolar disorder are both strongly familial. It is only over the last ~120 years that they have been investigated as separate, distinct disorders. This distinction, based on clinical observations and symptoms, was codified by Emil Kraepelin in the late 1890s, when “manic-depressive insanity” (bipolar disorder) was split from “dementia praecox” (schizophrenia) (Kraepelin, 1921). Recent systematic re-review of extant literature confirms that the lifetime risk of schizophrenia is approximately 1%. Several recent studies of schizophrenia using Scandinavian
hospital registers suggest the prevalence may be somewhat lower (Lichtenstein et al., 2009). Estimating the lifetime risk of bipolar disorder is more difficult as diagnostic schemes have changed significantly over time, particularly with the formulation of bipolar II disorder in DSM-III-R in 1987. Subsequent changes have tended to broaden the diagnostic spectrum and increase the overall prevalence. However, discussion of the accuracy and potential impacts of these diagnostic changes are beyond the scope of this chapter (Yutzy et al., 2012). The initial bipolar I disorder and bipolar II disorder distinction was based primarily on a different longitudinal course, as differences were not observed in family loading (Dunner et al., 1976) or lithium responsiveness (Fieve et al., 1976). The exact prevalence of each clinical subtype remains uncertain, with the most recent large epidemiological study reporting lifetime prevalence of 0.6% for bipolar I disorder and 0.4% for bipolar II disorder (Merikangas et al., 2011), similar to a recent systematic review (Ferrari, Baxter, & Whiteford, 2011) but lower than previously reported (Angst, 1998; Merikangas et al., 2007). Registry-based retrospective epidemiological studies of bipolar disorder suggest these estimates fluctuate over time according to a variety of biopsychosocial factors (Carlborg et al., 2015), although the extent to which such studies inform interpretation of large prospective epidemiological studies remains unclear given the different approaches to diagnosis (i.e., medical records vs. structured clinical interview). FA M I LY A N D T WI N S T U D I E S I N SCHIZOPHRENIA
As described in Chapter 1, the first step in gene mapping is to establish whether a trait or disease has a genetic liability, typically undertaken through family and twin studies. The first family study of schizophrenia was carried out almost one hundred years ago by Ernst Rudin. Even though his work predated the development of modern statistical methods for analyzing these data, he was able to appreciate that schizophrenia ran in families, although not in a manner consistent with Mendel’s laws. Since then, the rates of transmission in hundreds of families have been studied with consistent results. In fact, even application of modern statistical methods to Rudin’s original data confirm these observations (Kendler and Zerbin-Rudin, 1996). The relative risk for first-degree relatives of an individual with schizophrenia is ~10. This has recently been confirmed and extended
1 6 1 USA - OSO, 2018. Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press 07:34:22.
in a large Swedish population-based registry of 32,536 individuals with schizophrenia and their family members (Lichtenstein et al., 2006). Further investigation using twin studies supports underlying genetic factors for the observed familial clustering. The concordance rate (the likelihood that the second twin will develop the disorder once the first is diagnosed) between genetically identical monozygotic twins is high (41%–65%), and substantially lower for dizygotic twins (0%–28%) (Cardno & Gottesman, 2000). A meta-analysis of 12 twin studies derived a heritability estimate of 81% (Sullivan et al., 2003). Heritability estimates based on Swedish and Danish registry data were somewhat lower (67%) and may represent diagnostic differences in the newer studies. However, the larger registry-based studies are likely to be more broadly representative of the types of samples that are used in the genome-wide studies discussed below (Wray and Gottesman, 2012). It is frequently stated that most patients with schizophrenia do not have affected relatives and are thus “sporadic” in nature. However, Yang and colleagues have demonstrated that a low rate of affected relatives would be expected with a disease that is uncommon (1% prevalence), highly heritable, and highly polygenetic with risk mediated by many common variants of small effects (Yang et al., 2010). Thus, the lack of close relatives alone is insufficient to support an exclusively sporadic or noninherited component to the etiology of schizophrenia. FA M I LY A N D T WI N S T U D I E S IN BIPOLAR DISORDER
Early family studies of bipolar disorder did not distinguish between individuals with depressive episodes only, or what is now classified as major depressive disorder, from individuals with depressive episodes as well as manic episodes, what is now classified as bipolar disorder. More recent studies have done so, and the most recent have further included separate analyses of bipolar II disorder. In the modern studies that included control populations and that used a population risk of 1%–2%, the relative risk for first-degree relatives of bipolar patients is approximately 7–10 (Barnett and Smoller, 2009). Family studies of bipolar II disorder are indeterminate. This is likely because bipolar II disorder symptomatically resembles both major depression and bipolar I disorder and may be genetically related to one, or both. Complicating this is a lower inter-rater reliability for the diagnosis of bipolar II disorder, as well as the small sample sizes available (Smoller and Finn, 2003). Family studies also point to familial enrichment of several other phenotypes that may prove useful in refining genetic studies once genes and loci have been identified. These include observing evidence for familial clustering of early age of onset, mania versus depression on first onset, mood episode frequency, psychosis, lithium responsiveness, rapid cycling, and panic disorder (Barnett and Smoller, 2009). Like schizophrenia, twin studies of bipolar disorder support a genetic underpinning to the family study results. The most recent studies find the concordance rate for monozygotic twins is higher (0.5–0.6) then for dizygotic twins (0.39–0.43) resulting in heritability estimates of 79%–93% (Kendler et al., 1995; Kieseppa et al., 2004; McGuffin et al., 2003).
E P I D E M I O L O G I C A L OVE R L A P B ET WE E N SCHIZOPHRENIA AND BIPOLAR DISORDER
For the traditional linkage studies described below, families with the clearest inheritance of either schizophrenia or bipolar disorder, but not both, were sought. This approach was supported by two family studies from the early 1990’s that indicated there was no genetic overlap in families (Kendler et al., 1993; Maier et al., 1993). However, evidence to the contrary has recently emerged from two studies that found increased risk of affective disorder in the families of schizophrenia patients (Mortensen et al., 2003) and increased risk of schizophrenia in affective disorder families (Maier et al., 2002). In 2009, the very large Swedeish population-based study mentioned above took advantage of the quality of information in the Swedish Hospital Discharge Registry to more definitively answer the question of the familial relationships by calculating the relative risk for a wide variety of family pairs and adoptive relationships (Lichtenstein et al., 2009). Table 13.1 displays these results. For schizophrenia probands, the relative risk of schizophrenia was highest for first-degree relatives, but the relative risk of developing bipolar disorder was also elevated, although not as high. The reverse applied to bipolar disorder probands, who had increased risks of both bipolar disorder and schizophrenia in their first-degree relatives. In fact, there was sufficient power in this study to look at a variety of adoptive relationships confirming earlier studies that adopted away children with a biologic parent with schizophrenic or bipolar disorder are at increased risk of developing the same disease as their biological parent. Shared phenotypes between schizophrenia and bipolar disorder are also highlighted by patients with schizoaffective disorder, which is often referred to as a schizophrenia spectrum disorder. Patients with the manic/bipolar subtype meet diagnostic criteria for both schizophrenia and bipolar disorder, while the depressed subtype meet criteria for schizophrenia and major depressive disorder. Some work suggests increased familial risk of bipolar disorder and schizophrenia for each subtype, respectively. However, not all family and twin studies concur. Molecular genetic overlap that will be discussed below reinvigorates the discussion and may provide additional data to improve nosology. E N VI RO N M E N TA L A N D N O N I N H E R IT E D G E N ET I C FAC TO R S
Several nongenetic risk factors for schizophrenia have been reproducibly identified (Brown, 2011). The most well- documented of these are obstetrical complications, urban birth, season of birth, latitude, famine while in utero, migration, prenatal infections, and cannabis use (McGrathet al., 2008). Advancing paternal age has also been associated with increased risk of schizophrenia (Miller et al., 2011). Patients with schizophrenia have decreased reproductive fitness as measured by reduced fecundity measure as a fertility ratio in comparison to siblings, particularly in males (78% vs. 53% in females) that is not offset by increased fecundity in siblings (Power et al., 2012). This implies that negative selection is at work, and that new mutations are occurring that contribute
• P sychotic D isorders Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et162 al., Oxford University Press USA - OSO, 2018. 07:34:22.
Table 13.1 RECURRENCE RISKS FOR SCHIZOPHRENIA AND BIPOLAR DISORDER RISK FOR BIPOLAR RISK FOR SCHIZOPHRENIA DISORDER WHEN PROBAND HAS WHEN PROBAND HAS BIPOLAR DISORDER SCHIZOPHRENIA RELATION TO PROBAND
RR
95% CI
RR
RISK FOR SCHIZOPHRENIA WHEN PROBAND HAS BIPOLAR DISORDER
95% CI
RISK FOR BIPOLAR DISORDER WHEN PROBAND HAS SCHIZOPHRENIA
RR
95% CI
RR
95% CI
Biological relationships Parent
Offspring
9.9
8.5–11.6
6.4
5.9–7.1
2.4
2.1–2.6
5.2
4.4–6.2
Sibling
Sibling
9.0
8.1–9.9
7.9
7.1–8.8
3.9
3.4–4.4
3.7
3.2–4.2
Sibling
Maternal half-sibling
3.6
23–5.5
4.5
2.7–74
1.4
07–2.6
1.2
0.6–24
Sibling
Paternal half-sibling
2.7
1.9–3.8
2.4
1.4–4.1
1.6
1.0–2.7
2.2
1.3–3.8
Adoptive relationships Biological Adopted away parent offspring*
13.7
6.1–30.8
4.3
2.0–9.5
4.5
1.8–10.9
6.0
2.3–15.2
Sibling
Adopted away biological sibling
7.6
0.7–87.8
..
..
3.9
0.2–63.3
5.0
03–79.9
Adoptive parent
Adoptee
..
..
13
0.5–3.6
1.5
07–3.5
..
..
Sibling
Non-biological sibling
1.3
04–15.1
..
..
..
..
2.0
0.1–37.8
RR=relative risk. *Adopted children whose biological parents have disease. Used with permission from: Lichtenstein, Lancet, 2009, 373:17–23
to the risk of schizophrenia. In a whole-g enome sequencing study in Iceland, paternal age was estimated to explain most of the increased de novo mutation rate observed (Kong et al., 2012), providing a potential molecular correlate. Hypotheses that do not rely on an increased mutation rate are also consistent with the epidemiological data; such models incorporate a weak correlation between age at first child and liability to psychiatric illness (Gratten et al., 2016). There are fewer studies investigating environmental factors in bipolar disorder. However, there is some evidence of effects on risk from seasonality of birth, advanced paternal age, and stressful life events (Alloy et al., 2005; Disanto et al., 2012; Frans et al., 2008). E A R LY G E N ET I C S T U D I E S / T R A D I T I O N A L G E N ET I C M ET H O D S L I N K AG E A NA LY S E S
The familial observations described above led to searches for the responsible genes. As genome-wide markers became available in the 1980s, they were used for linkage studies in families with schizophrenia or bipolar disorder. As discussed in Chapter 1, linkage analysis follows the transmission of
disease and particular genetic markers in families to identify chromosomal segments for closer follow-up, and have primarily been successful in diseases caused by mutations with large effect sizes in a single or small number of genes. Many linkage studies of both disorders have been performed, and the overall conclusion that can be drawn is that no genomic loci are likely to harbor large effect genes that account for a substantial portion of genetic liability. Even a meta-analysis of 32 independent linkage studies using data from 7,413 schizophrenia cases in 3,255 pedigrees was not able to identify significant loci above the chance level (Ng et al., 2009). While the overall number of linkage studies in bipolar disorder is more modest, the overall observation was the same in the meta-analysis of 18 studies of 2,437 bipolar cases in 592 pedigrees (Segurado et al., 2003). This was extended using a linkage panel of 6,000 single nucleotide markers to achieve more complete linkage information across the genome in 2,782 bipolar disorder cases without producing significant results (Badner et al., 2012). Phenotypic heterogeneity and diagnostic inaccuracy have often been postulated as a primary explanation for lack of clear success in linkage studies. However, similar diagnostic methods and patient samples were used in the genome-wide association studies (GWAS) of common variants and rare copy number variants with strikingly different results that will be
13. GS.enetics S chizophrenia and Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney, et al.,of Oxford University Press USA - OSO, 2018. 07:34:22.
described below. Furthermore, it is often argued that there are some suggestive regions that overlap in several studies and might contain loci, but the most likely explanation for the overlap is random chance resulting from the large number of studies performed and the relative lack of fine-scale genomic resolution of linkage analysis. Despite this, positional cloning—the process whereby specific genes are identified within a linkage peak—has been carried out in some suggestive linkage regions, particularly on chromosomes 8p12 and 6p22.3. In those regions, two candidate genes were of focus, neuregulin1 (NRG1) and dysbindin (DTNBP1) respectively. Neurobiological investigations of these genes will be discussed in a later chapter. Disrupted in Schizophrenia 1 (DISC1) is another gene that grew of interest from early linkage studies. It is a gene interrupted by a balanced chromosomal translocation between chromosomes 1 and 11 (t(1;11) (q42;q14)) that segregates in a single Scottish family with schizophrenia, bipolar disorder, and major depression. No other families with translocations or other clear segregating structural abnormalities in DISC1 have been found. Numerous genetic association studies have focused on this gene in both schizophrenia and bipolar disorder, with inconsistent results. A meta-analysis of data from 11,626 cases and 15,237 controls did not find evidence for association for any of the 1,241 single nucleotide polymorphisms (SNPs) in DISC1 that were tested (Mathieson et al., 2012), and the gene is not identified in the large GWAS studies described below. In addition, studies have generally not found an excess of rare variants at this locus. Despite the paucity of evidence for a major role in genetic risk of schizophrenia, there have been many interesting biological studies of this gene that will be described in later chapters. C A N D I DAT E G E N E S S T U D I E S O F SCHIZOPHRENIA AND BIPOLAR DISORDER
Hundreds of candidate gene association studies have been performed over the last decade. Most were defined as candidates based on biological theories from pharmacological observations or secondary to abnormalities observed in postmortem human brain tissue from patients. Taken as a whole, the results of these studies are inconsistent and may represent poor candidate choices because of our fundamental lack of understanding of the underlying biology and/or poor gene coverage and/or small sample sizes. It is of note that initial results from GWAS did not find the prior biological candidate genes enriched among significant or nearly significant loci (Collins et al., 2012), although as GWAS sample sizes have increased some traditional candidate genes have been associated. The most extensively investigated are covered in other chapters of this section. Candidate genes in bipolar disorder have focused on BDNF, circadian genes, phosphinositide signaling, and Wnt/GSK3beta signaling (Martinowich et al., 2009). As with schizophrenia, initial results from GWAS do not find the prior biological candidates enriched among significant or nearly significant loci (Seifuddin et al., 2012). Of course, the large number of loci being identified in GWAS
will likely include some prior candidate genes, but at much smaller effect sizes. C O P Y N U M B E R VA R I AT I O N Copy number variants (CNVs) are deletions or duplications of genetic material and can range from several base pairs (often called indels) to millions of bases. The risk of developing schizophrenia is markedly elevated in the presence of certain CNVs. A large body of work reviewed in detail elsewhere (Malhotra and Sebat, 2012) has defined the following principles of the CNVs associated with schizophrenia from studying over 10,000 samples, initially using array- comparative genomic hybridization and subsequently from SNP microarrays. • Genome-wide rates of large (>100kb), rare (300 for inclusion. Moffit and Caspi suggest that smaller studies use stronger methods (e.g., direct interviews), which are more likely to support the hpothesis. They did not provide supporting evidence. The results of the Culverhouse et al. consortium have not yet been published. An important issue here is whether all
Table 24.3 META-A NALYSES OF EFFECT OF 5-H TTLPR GENOTYPE X STRESS INTERACTION ON DEPRESSION RISK FIRST AUTHOR , YEAR
NUMBER OF STUDIES FOUND
EFFECT
ELIGIBLE INCLUDED
N
STRESS
GENOTYPE
INTERACTION
COMMENT
Munafo, 2009
32
10
5
6,699
OR = 2.08 CI (1.77–2.44) p1) to that of PE treatment. The structure of such sessions is typically one to three eight-hour drug-assisted sessions preceded and followed by several follow-up nondrug sessions (Mithoefer et al., 2011, 2013; Oehen et al., 2013). The mechanism by which MDMA S E ROTO N E RG I C S Y S T E M may lead to improved PTSD is unknown. Recent preclinical Although many current pharmacotherapies for anxiety disor- studies suggest that MDMA may enhance extinction of fear ders, such as SSRIs, SNRIs, TCAs, MAOIs, and buspirone, via enhanced oxytocin signaling (Young et al., 2015). Another all affect serotonergic signaling, the mechanism(s) by which hypothesis is that MDMA reduces the acute experience of fear they exert their benefit is unknown. One possibility is through and enhances trust, leading one to enter an “optimal arousal the enhancement of fear extinction through activation of 5- zone” such that patients can recall their trauma without feelHT1A and 5-HT2A receptors. Serotonergic signaling mod- ing numb or overwhelmed by anxiety. Thus it could facilitate ulates communication between amygdala and prefrontal emotional engagement with traumatic memories that may cortical regions, and preclinical studies have found that selec- otherwise be too difficult for the patient to experience without tive activation of these receptors enhances extinction learning voluntary or involuntary avoidance (Mithoefer et al., 2011). (Singewald et al., 2015). This section will review a number of There is also evidence that healthy test subjects that ingest novel therapeutic approaches using serotonergic compounds. MDMA exhibit a positive emotion bias and report their worst Several small clinical studies have examined the potential autobiographical memories as less negative than those who do benefit of dimethyltryptamine (DMT), psilocybin, and lyser- not ingest the drug (Carhart-Harris et al., 2014). This raises gic acid (LSD) in anxiety disorders (Dos Santos et al., 2016). the possibility that MDMA may also assist in reframing the These compounds are pharmacologically related and produce meaning or significance of traumatic experiences. Given the hallucinogenic experiences that have been a part of ritual cere- political, ethical, and scientific questions that remain with monies of indigenous cultures. They are all agonists at 5-HT1A, psychotropic medications, caution must be exerted, but as 5-HT2A, and 5-HT2C receptors. A small double-blind pla- described the early studies are quite intriguing. cebo controlled pilot study of adults with advanced-stage cancer administered low-dose psilocybin demonstrated tolerability M E L ATO N E RG I C SYS T E M and reduced scores on measures of anxiety one and three months after a single administration (Grob et al., 2011). Similarly, a Agomelatine is a melatonin MT1, MT2 agonist and 5-HT2C small study of individuals with high anxiety associated with life- receptor antagonist approved in Europe for treatment of major threatening conditions exhibited substantial reductions in anx- depressive disorder (MDD). Melatonin is known primarily iety (effects size >1) after receiving psychotherapy along with for its activity in regulating circadian rhythms through activity LSD. These effects persisted at 12-month follow-up, despite a in the suprachiasmatic nucleus of the hypothalamus; however, design that involved only two treatment sessions (and two with MT1 and MT2 receptors are also expressed in many regions active placebo) (Gasser et al., 2014). In an unblinded study of including the prefrontal cortex, hippocampus, thalamus, and psilocybin in nine patients with OCD, there was both general basal ganglia. There is some evidence from preclinical studies tolerability and reduction in OCD symptoms. Multiple studies of synergism between agomelatine’s activation MT1/MT2 have demonstrated effects after administration of these com- receptors and antagonism of 5-HT2C in producing its antidepounds that persist for weeks or months. Some authors refer to pressant effects, enhancing neurogenesis, and reducing stress- this as an “inverse posttraumatic stress disorder-like effect” in induced glutamate release in the prefrontal cortex (PFC) which experiences on these compounds lead to a highly person- (Tardito et al., 2012; Soumier et al., 2009). Though early, ally significant positive experience that has a lasting effect (Dos several studies by Stein and colleagues have demonstrated a Santos et al., 2016). For a variety of reasons, the size and num- reduction in anxiety symptoms with agomelatine in GAD and ber of such studies are small, reflecting regulatory hurdles and a in those with comorbid MDD, including one RCT demonlegacy of stigma associated with these molecules. A recent sys- strating comparable efficacy to that of several SSRIs and the tematic literature review of such studies from 1990–2015 found SNRI venlafaxine (Stein et al., 2008, 2012, 2013, 2014). only five human studies, all of them small, and only three were blinded (Dos Santos et al., 2016). D O PA M I N E RG I C SYS T E M 3,4- methylenedioxymethamphetamine (MDMA), is structurally similar to the hallucinogenic drug mescaline and Animal and human studies have found that boosting dopahas activity at 5-HT2 receptors, though it also affects dopa- minergic signaling through the administration of the dopamine, oxytocin, prolactin, and cortisol signaling. It is associated mine precursor L-dopa facilitates extinction (Haaker et al., chronic trauma/ complex PTSD (Ludäscher et al., 2015). There is some evidence supporting the use of hydrocortisone in PTSD as augmentation to prolonged exposure (PE) therapy. In a RCT of military veterans randomized to placebo or hydrocortisone preceding sessions 3–10 of manualized PE therapy, there were substantially improved outcomes in those randomized to hydrocortisone, primarily due to a much stronger propensity for these subjects to continue with treatment rather than drop out (rates of 8.3% vs. 58% respectively) (Yehuda et al., 2015).
39. NS.ovel p roaches T reating Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney,Aetpal., Oxford Universityfor Press USA - OSO, 2018. 15:10:22.
associated with fear of flying (Meyerbroeker et al., 2012). Yohimbine is acutely anxiogenic, again marking a contrast between potentially elevated state anxiety and a treatment that may facilitate lasting symptom reduction. PTSD is actually associated with increased noradrenergic tone and exaggerated noradrenergic activation, thought to be mediated by activation of presynaptic alpha-2 autoreceptor. This mechanism may then lead to autonomic hyperactivity and hypervigilance seen in this disorder. Short-term symptom reduction in PTSD is often approached with alpha-1 antagonism and alpha-2 agonism (rather than antagonism, as with yohimbine) (Strawn and Geracioti, 2008). The alpha-1 antagonist prazosin is frequently used to reduce PTSD-related nightmares, insomnia, and intrusive reexperiencing symptoms (Raskind et al., 2003). Clonidine, an alpha-2 agonist, has been used for decades to decrease hyperarousal, hypervigilance, sleep disruption, and exaggerated startle in PTSD (Strawn and Geracioti, 2008). Guanfacine, another alpha-2 receptor agonist with greater specificity for the alpha-2a subtype (while clonidine has activity at alpha-2a, 2b, and 2c receptors) has also been used, but there is less evidence for its efficacy in PTSD with most studies demonstrating negative results (Murrough et al., 2015; Belkin and Schwartz, 2015). Propranolol is a nonselective beta-blocker that has long been used to reduce autonomic symptoms that may cause an interoceptive feedback loop facilitating further anxiety, such as that associated with public performance. It may also have a promising role in the more specific approach of blocking memory consolidation following trauma in order to prevent the development of PTSD. Preclinical studies have demonstrated that beta- blockade in the rat amygdala blocks memory consolidation, and several subsequent open-label and nonrandomized trials have found some evidence of reduced development of PTSD when individuals are administered propranolol immediately following a trauma (Pitman et al., 2002; Brunet et al., 2008; Vaiva et al., 2003). However, a systematic Cochrane review from 2014, which excluded less rigorously designed studies, did not find enough evidence to support the use of propranolol for this N O R A D R E N E RG I C SY S T E M purpose [RR 0.62, 0.24, 1.59] (Amos et al., 2014). Nepicastat is a selective dopamine beta-hydroxylase (DBH) Although it is associated with states of heightened anxiety, and also necessary for the formation of fear memories, inhibitor that blocks the conversion of dopamine to norepithe noradrenergic system is also critical for fear extinction. nephrine. Two clinical trials for this compound in PTSD have Lesions of noradrenergic cell bodies in the locus coeruleus been completed without published results (NCT00659230, impair extinction, as do blockade of alpha-1 and beta recep- NCT00641511). One small placebo controlled RCT of nepitors (Singewald et al., 2015). There is some evidence support- castat examined the potential interaction between utility of ing alpha-2 receptor antagonism enhancing fear extinction this agent and the genetic polymorphism [rs1611115 (1021C- in preclinical models (Cain et al., 2004). Enhancement of >T/C-970T)] which leads to higher plasma activity of DBH. extinction appears to be through downstream facilitation of This trial found a DBH genotype effect on outcome but found beta-adrenergic transmission and BDNF expression (Furini no primary treatment effect or gene x nepicastat treatment et al., 2010). Furthermore, polymorphisms within the beta- interaction (Graham et al., 2014). Though this compound adrenergic receptor have been associated with PTSD in unbi- may have some promise in treating alcohol and/or cocaine use disorders (Murrough et al., 2015), there is currently no clear ased discovery genetic studies (Liberzon et al., 2014). There have been two clinical trials demonstrating that evidence supporting its use in anxiety disorders. CBT exposure therapy enhanced with the alpha-2 antagonist yohimbine leads to reduced anxiety when compared to CBT N EU RO P E P T I D E SYS T E M S exposure therapy plus placebo in social anxiety and claustrophobia (Smits et al., 2014; Powers et al., 2009), although There has been significant interest in multiple neuropeptides another study detected no difference in anxiety reduction that have been implicated in fear and extinction learning 2013), and the disruption of dopamine signaling in the PFC is known to impair extinction memory formation in rats (Fernandez Espejo, 2003). Although to our knowledge there have been no clinical trials of L-dopa (by itself or in conjunction with psychotherapy) such an approach makes some theoretical sense, especially in light of emerging evidence for MDMA-assisted psychotherapy in PTSD. Patients with Parkinson’s disease frequently experience mood and anxiety symptoms along with motor and other manifestations. In such patients, an acute dose-dependent reduction in depressive and anxiety symptoms is seen with L-dopa administration (Kulisevsky et al., 2007; Maricle et al., 1995), though there is no consistent reduction in anxiety with chronic administration (Nègre-Pagès et al., 2010) and there is some suggestion from animal studies of a mild acute anxiogenic effect of chronic L-dopa administration (Eskow Jaunarajs et al., 2010). Interestingly, although enhancement of dopaminergic transmission may be beneficial to anxiety via enhancement of fear extinction, there is evidence for reduced anxiety with several second generation antipsychotics, antagonists at dopamine D2 receptors (although they also affect serotonergic, adrenergic, histaminergic, cholinergic, and other signaling pathways). A systematic Cochrane review of ten short-term trials and one long-term trial found the most evidence for quetiapine in improving anxiety symptoms in GAD. These treatment effects were on par with those of antidepressants, although there were more adverse effects with quetiapine (Depping et al., 2010). A systematic review of second generation antipsychotics for panic disorder, however, found a general lack of efficacy in reducing symptoms (Giampaolo et al., 2016). The seeming contradictory finding that enhanced dopaminergic transmission and dopaminergic D2 blockade could have roles in treating anxiety disorders may reflect the distinction between treating acute anxiety (state) symptoms versus treating one’s longer term propensity toward further symptoms (trait).
• A 520 nxiety isorders Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University PressD USA - OSO, 2018. 15:10:22.
(Bukalo et al., 2014; Lin, 2012). Some of the most promising neuropeptide targets for anxiety disorders are corticotropin releasing factor (CRF), oxytocin (OXT), neuropeptide Y (NPY), substance P, and cholecystokinin (CCK), though others are potentially relevant.
early-phase extinction, though ultimately subjects in the OXT group showed enhanced extinction learning and reduced fear reactivity (Eckstein et al., 2015, 2016). There is also evidence that OXT reduces the startle response to an acoustic stimulus in healthy subjects (Ellenbogen et al., 2014). Intranasal OXT did not enhance the effects of exposure therapy in subjects with SAD, though these subjects did C O RT I C OT RO P I N R E L E A S I N G FAC TO R exhibit greater appraisals of self-appearance and performance CRF is a major regulator of the HPA axis which, as previously (Guastella et al., 2009). A meta-analysis of OXT administradiscussed in the context of glucocorticoids, plays an essential tion found an average effect size of 0.42 in reduction of anxrole in fear learning and extinction. The CRF system consists iety symptoms across multiple disorders, though studies were of CRF, along with urocortins 1–3, that bind two G-protein- typically small and heterogeneous (Hofmann et al., 2015b). coupled receptors (CRF1 and CRF2). These receptors are A number of clinical trials have been registered to examexpressed in the BNST and part of the extended amygdala, as ine potential therapeutic benefit of OXT in anxiety disorwell as the cortex and septum. Administration of CRF1 recep- ders (e.g., NCT00989937; NCT01039766; NCT01551303; tor antagonists has demonstrated acute anxiolytic effects in NCT02336568) and despite some previous mixed results, preclinical models (Lin, 2012). Higher levels of CRF in cere- this system may be a promising target for future treatments. brospinal fluid have been found in individuals with PTSD and It is also important to note that the mechanism (e.g., how do OCD (Baker et al., 2005; Fossey et al., 1996). Several CRF1 the medications penetrate the brain) and efficacy of intranareceptor antagonists are under investigation for use in anxiety sal dosing of medications remains unclear, with more work to disorders. One such compound, R121919, showed promise in be done before recommended standard clinical use of these reducing symptoms of both depression and anxiety, although administration approaches. development was stopped due to concerns about potential hepatotoxic effects (Zorrilla and Koob, 2010). Though the N EU RO P E P T I D E Y results of several small phase I trials of CRF1 antagonists have been encouraging, a larger multicenter RCT of the CRF1 NPY is a 36 amino acid peptide that is expressed throughout receptor inhibitor pexacertfont did not exhibit efficacy com- the brain, and with particularly high levels in the cortex, locus pared to placebo in GAD, and was inferior to escitalopram coeruleus, amygdala, and other structures relevant to anxiety (Coric et al., 2010). Unfortunately no CRF1 receptor antag- disorders. There are five known NPY receptors (Y1, Y2, Y4, onist has yet completed a phase III clinical trial (Koob and Y5, and Y6) that each bind to G-proteins that inhibit cAMP Zorilla, 2012). synthesis. Preclinical studies of this system in models of anxiety suggest that activation of the Y1 receptor produces an acute anxiolytic effect, while Y1 blockade increases expression OX Y TO C I N of anxiety (Wu et al., 2011). The opposite pattern has been OXT has become the subject of substantial interest in recent seen with Y2 (which can act as an autoreceptor) and Y4 recepdecades due to its role in complex social behavior, attachment, tors. Infusion of a Y2 agonist in the basolateral amygdala has aggression, and anxiety (Meyer- Lindenberg et al., 2011). shown anxiogenic effects at low doses and anxiolytic effects at This small peptide hormone is synthesized in the supraoptic higher doses (Lin, 2012). Combat veterans with PTSD have lower baseline serum nucleus of the hypothalamus and exerts central and peripheral effects. The OXT receptor is widely expressed through- and CSF NPY levels compared with healthy controls out cortical and subcortical regions, including limbic regions, (Rasmusson et al., 2000; Sah et al., 2009), and higher plasma NPY levels are associated with reduced PTSD symptoms basal ganglia, thalamus, and hypothalamus. Preclinical studies of central and peripheral exogenous (Yehuda et al., 2006). A clinical study of intranasal adminisadministration of OXT or OXT receptor agonists have pro- tration of NPY on mood and anxiety symptoms in combat duced dose-dependent acute anxiolytic effects (Lin, 2012). In veterans with PTSD is underway (NCT01533519). Although healthy human subjects OXT administration strongly modu- a potentially promising target, further research is needed to lates amygdala activity, reducing activation to fear-inducing support the safety and efficacy of targeting the NPY system in stimuli. Intranasal administration of OXT reduced anxiety humans with anxiety disorders. in response to interpersonal stress in a subset of women classified as having high emotion-oriented coping, but not other S U B S TA N C E P women or men (Cardoso et al., 2012). This raises the possibility that individual differences in coping style could modulate Also known as neurokinin 1, substance P is widely expressed treatment strategy. Furthermore, it points to potential sex- in the brain, including the amygdala, BNST, basal ganglia, and related physiological differences in anxiety disorders. This is other regions. It binds the GPCRs NK1 and NK2 receptors. an intriguing possibility given the higher prevalence of anxiety Preclinical models of NK2 receptor antagonists demonstrate disorders in women than men. Using a Pavlovian fear condi- anxiolytic effects (Lin, 2012). However, clinical trials of NK2 tioning paradigm in healthy human subjects, OXT enhanced antagonists have not demonstrated efficacy in GAD, SAD, or fear learning and potentiated the fear response initially during PTSD (Griebel and Holsboer, 2012). 39. NS.ovel p roaches T reating Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney,Aetpal., Oxford Universityfor Press USA - OSO, 2018. 15:10:22.
C H O L E C Y S TO K I N I N
VAGUS N E RVE S T I MU L AT I O N
There is some data supporting a role of CCK signaling in fear extinction. Systemic administration and infusion into the basolateral amygdala of the CCK2 receptor agonist pentagastrin impairs extinction in preclinical studies (Chhatwal et al., 2009). Conversely, blockade of the CCK2 receptor reverses extinction deficits induced by blockade of the cannabinoid CB1 receptor. Preclinical data have been mixed, and to date clinical trials with CCK2 receptor antagonists in anxiety disorders have not been successful (Griebel and Holmes, 2013).
VNS is another surgical approach, although it does not require craniotomy or access to the brain directly. Instead, electrodes are placed around a portion of the left vagus nerve in the neck. Afferents comprise 80% of these nerve fibers, sending signals to the nucleus of the solitary tract, which sends projections to other regions such as the amygdala and hypothalamus (Marin et al., 2014). The FDA has approved VNS for multiple applications including depression. Stimulation of the vagus nerve increases norepinephrine release in the amygdala, which could theoretically facilitate extinction learning, consistent with preclinical evidence (Peña et al., 2014). A human trial to test whether VNS enhances extinction learning in healthy subjects has been registered (NCT02113306), and further research is needed to demonstrate its potential utility in anxiety disorders. Newer noninvasive VNS devices may further increase the opportunities for this technology.
B R A I N S T I MU L AT I O N TECHNIQUES In recent years, brain stimulation techniques have been used to treat a number of psychiatric conditions. Techniques like deep brain stimulation (DBS), transcranial magnetic stimulation (TMS), transcranial direct current stimulation (tDCS), and vagus nerve stimulation (VNS) are modalities that deliver controlled electrical currents in order to theoretically disrupt maladaptive patterns of neural activity and connectivity (Marin et al., 2014). To this end, there has been increasing, if nascent, research for stimulation techniques for anxiety disorders. D E E P B R A I N S T I MU L AT I O N
In DBS, an electrode is implanted into subcortical tissue and connected to a stimulator that delivers controlled electrical pulses. This invasive technique has gained recognition for its application in Parkinson’s disease and dystonias, and in recent years it has demonstrated some utility in depression and OCD (Velasques et al., 2014). In 2009, after ten years of clinical use, the FDA approved DBS to the ventral capsule/ventral striatum for treatment-refractory OCD. Although the mechanism for its therapeutic effects is unknown, stimulation of the ventral capsule has led to significant improvement in symptoms in two-thirds of treatment-refractory OCD patients, without any reports of deleterious effects on personality or neuropsychological testing (Velasques et al., 2014; Greenberg et al., 2010). As the ventral striatum has strong connections to regions involved in fear extinction such as the PL/d ACC and IL/vmPFC, this target may lead to facilitation of extinction learning. Preclinical studies of DBS targeting a dorsal portion of the ventral striatum found enhanced extinction recall, and potentially with markers of neuroplasticity (e.g., BDNF and/or pERK) in PL, IL, and orbitofrontal cortex (OFC) (Rodriguez-Romaguera et al., 2012m 2015; Do-Monte et al., 2013). In a different preclinical model of PTSD, unilateral amygdala-targeted DBS was beneficial (Langevin et al., 2010). Although presently there is no available data for humans receiving DBS for PTSD, a recently published protocol describes a planned clinical trial targeting the basolateral amygdala in six subjects with combat-related treatment-refractory PTSD (Koek et al., 2014).
T R A NS C R A N I A L M AG N ET I C S T I MU L AT I O N
TMS is a method by which an electric current generates a magnetic field that travels through the skull, and a secondary electrical current activates target cortical neurons. In 2008 the FDA approved TMS for the treatment of major depressive disorder. Based on the role of IL in preclinical models of extinction and its homolog in humans, the vmPFC would be a natural target to facilitate extinction learning. Limitations of the technique do not permit directly targeting the vmPFC; however, this region can potentially be modulated indirectly via activation of the dorsolateral prefrontal cortex (DLPFC). Though limited in size and number, several studies have found repetitive TMS (rTMS) over the DLPFC to be effective treating symptoms of PTSD (Berlim and Van Den Eynde, 2014). There is also some evidence to support the use of rTMS in PD as well (Mantovani et al., 2013; Prasco et al., 2007), although further research is needed to confirm this benefit in PD and support its potential in other anxiety disorders (Li et al., 2014). T R A NS C R A N I A L D I R EC T CU R R E N T S T I MU L AT I O N
Like TMS, tDCS is a noninvasive technique. It applies direct current through the skull to alter cortical activity. The electrical current in tDCS does not directly stimulate (i.e., depolarize) neurons; rather, it functions as a modulator affecting membrane potentials and thus the probability of neuronal firing. tDCS has been tested in studies of learning, attention, and working memory (Marin et al., 2014). One human study found that tDCS enhanced late but not early extinction learning (van ‘t Wout et al., 2016). Another study found disruption of fear memory consolidation with tDCS targeting the left DLPFC (Asthana et al., 2013). tDCS to the DLPFC has also reduced vigilance (as operationally defined based on
• A 522 nxiety isorders Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University PressD USA - OSO, 2018. 15:10:22.
reaction time differences to a dot-probe task) to fearful and angry faces (“threatening stimuli”), suggestive of an acute anxiolytic effect (Ironside et al., 2016). In another recent study, physiological reactivity was reduced to unpredictable threat (audio of a scream) in the context of tDCS targeting the inferior frontal gyrus (Herrman et al., 2016). To date there is limited literature of tDCS in patients with anxiety disorders. However, in one encouraging case study of tDCS targeting the left DLPFC, a patient with GAD had full remission of symptoms after a two-week protocol that was lasting at one month follow-up (Shiozawa et al., 2014). Further clinical studies are needed to support this approach in treating anxiety disorders.
Interpretive bias modification (CBM-I) trains individuals to have more positive interpretations. The most frequently employed task involves a training phase in which subjects who have to make a decision about the final word in read narratives of ambiguous social scenarios (Mathews and Mackintosh, 2000; Beard, 2011). In the positive interpretation direction, the final words disambiguate in a positive way. After multiple such trials, subjects develop a more positive interpretive bias of such ambiguous situations. Clinical data are limited, though there is some indication for reduction of negative biases and social anxiety symptoms in children and adults (Klein et al., 2015; Mobini et al., 2014). MINDFULNESS
C O G N I T I VE T R A I N I N G A N D P SYC H OT H E R A P Y Cognitive behavioral therapy (CBT) is an effective and commonly used treatment for anxiety disorders. Linking anxiety symptoms bidirectionally to maladaptive thoughts and behaviors, the approach involves evaluating and challenging such thoughts and using behavioral methods to diminish the anxiogenic properties of interoceptive and external stimuli. In many ways, CBT is didactic, teaching patients how to deliberately apply a set of principles and directly and explicitly address the thoughts, feelings, and behaviors associated with symptoms. CBM similarly addresses propensity toward negative interpretations of ambiguous information, such as that observed in SAD (Beard and Amir, 2009). Unlike CBT, CBM uses computerized behavioral tasks to subliminally train individuals to adjust the target of their attention and/or their appraisals in a more positive way. Attention bias modification (CBM-A) is typically performed with a dot-probe task. Subjects are instructed to indicate the screen location of a target probe which follows presentation of valenced or neutral words or images. If reaction times are shorter to target probes that follow threatening stimuli, the subject is said to have a threat bias. The standard interpretation is that greater attentional resources are placed on the threatening stimulus, making the determination of dot-probe location faster. To modify this bias, the subject is presented with multiple trials with the probe away from the threat stimulus, such that over time, attentional resources will tend to be allocated away from the threatening stimulus. This approach has shown some promise for reducing anxiety symptoms in multiple anxiety disorders, such as GAD and SAD (Amir et al., 2009; Linetzky et al., 2015; Schmidt et al., 2009; Hakamata et al., 2010). However, evidence remains limited and a recent meta-analysis found that CBM-A was effective only when administered in a laboratory and was less effective for SAD than Internet-delivered CBT or virtual reality–based exposure therapy (Kampmann et al., 2016). Furthermore, a recent study found that CBM-A with a visual probe task did not generalize to other contexts in which attention bias could be assessed (Van Bockstaele et al., 2015).
The popularity of mindfulness has increased in recent years. It is explicitly combined with elements of CBT in Dialectical Behavioral Therapy and also plays a central role in Acceptance and Commitment Therapy. The practice of mindfulness involves the nonjudgmental and minimally interpretive concrete observations in the present moment of one’s internal experience and of external stimuli. This includes two components: self-regulation of attention toward present experience, and an open and accepting attitude toward all internal and external stimuli (Bishop et al., 2004). This approach has intuitive appeal for anxiety disorders, as worries about future threats and catastrophic interpretations of present thoughts and feelings are common. One systematic review found improvements in symptoms of SAD with mindfulness, though these were equivalent to or less than those seen with CBT. Unfortunately, the literature on mindfulness is frequently confounded, since hybrid treatments combining mindfulness with other treatments are often lumped together (e.g., with CBT or other treatments). Therefore, evidence remains limited for mindfulness by itself as a treatment for anxiety (Norton et al., 2015). S E L F-R EGU L AT I O N O F B R E AT H I N G
Deep slow breathing inhibits sympathetic tone (Seals et al., 1990) and is thought to produce a shift toward increased parasympathetic tone via hyperpolarization of neurons within the amygdala and thalamus ( Jerath et al., 2012). As anxiety disorders are frequently associated with increased amygdala activity and activation of the sympathetic autonomic nervous system, self-regulation of breathing has been proposed as a primary treatment for anxiety ( Jerath et al., 2015). Though used for thousands of years in the context of meditation, breathing techniques are yet to gain widespread acceptance as a central approach to anxiety rather than as a momentary coping strategy. There is some evidence that an instructed deep breath, but not an instructed breath hold, leads to immediate anxiety relief and reduction of muscle tension in individuals with high anxiety sensitivity (Vlemincx et al., 2016). Based on the favorable risk profile and immediate accessibility of breathing techniques, further research is warranted to establish its potential benefit and identify optimal breathing strategies for anxiety symptom reduction.
39. NS.ovel p roaches T reating Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney,Aetpal., Oxford Universityfor Press USA - OSO, 2018. 15:10:22.
N O VE L T E C H N O L O G I C A L A PP R OAC H E S
anxiety that may facilitate and/or perpetuate ongoing symptoms. A recent systematic review found 43 studies that utilized biofeedback methods (such as electroencephalogram, Technological advances of the past two decades have led to electromyelogram, heart rate, heart rate variability, respiranew treatment strategies and novel twists on older approaches tory rate, skin temperature, and skin conductance) in anxiety that may increase the efficacy and accessibility of anxiety dis- disorders (GAD, OCD, PD, PTSD, specific phobia). These order treatments. These include ICBT and telemental health, studies were generally small and heterogeneous, though two- biofeedback, virtual reality–based exposure therapy (VRET), thirds of them found significant symptomatic improvement and smartphone applications. in clinical ratings of anxiety, including all studies that used a multimodal approach (N = 5) (Schoenberg and David, 2014). Real- time functional magnetic resonance imaging (rt- I N T E R N ET-BA S E D T H E R A P Y fMRI) is a promising and more recent biofeedback modality. A N D T E L E M E N TA L H E A LT H In one study, subjects with OCD-related contamination anxBoth computer-based and clinician-assisted ICBT treatments iety were trained to reduce BOLD activity in their OFC in are novel therapeutic approaches that can enhance the availa- the context of a contamination cue. This training paradigm bility of treatment by reducing financial and geographical barri- led to reduced measures of resting-state functional connectivers. It may also diminish the potential barrier of anxiety-related ity between regions such as the amygdala, insula, and hippoavoidance of face-to-face encounters that accompanies SAD campus, as well as reduced resting-state OFC activity. It also and other anxiety disorders, which could account for the two- led to reduced contamination-related anxiety several days folthirds who do not seek treatment for SAD and other disorders lowing training, and changes in functional activity were also (Kampmann et al., 2016). A recent Cochrane systematic review sustained and associated with symptomatic improvement of ICBT for multiple anxiety disorders (including SAD, GAD, (Scheinost et al., 2013; Hampson et al., 2012). Another small PD, PTSD, OCD, and mixed anxiety) found ICBT to reduce pilot study found rt-f MRI targeting downregulation of insula anxiety symptoms and improve quality of life. No outcome dif- activity was similarly helpful in OCD-related contamination ferences were observed between therapist-supported ICBT ver- anxiety (Buyukturkoglu et al., 2015). Further research with sus unguided ICBT, though few studies compared them. There this approach is needed to assess longer term symptom reducwere also no differences in anxiety outcome measures between tion, as well as applicability to other anxiety disorders. therapist-supported ICBT and face-to-face group and individual CBT (Olthuis et al., 2016). This is consistent with other VI RT UA L R E A L IT Y E X P O S U R E T H E R A P Y meta-analyses finding medium-to-large ICBT treatment effect sizes across disorders (e.g., d = 0.5-1) (Barak et al., 2008; Spek VRET uses computer-generated virtual situations to facilet al., 2007). These promising findings speak to the potential for itate systematic exposure to feared contexts. One potential a paradigm shift in the availability and delivery of CBT. advantage of VRET over standard exposure therapies is the As with the Internet paving the way for ICBT treatment, potential for greater willingness of patients to engage in treatadvances in telecommunication are opening the door to tele- ment. As most patients with anxiety disorders do not seek mental health more broadly. This includes both psychother- treatment, removal of any treatment barriers, including that apy and psychopharmacology visits. Using videoconferencing of the patient’s own avoidance, could have a decisive impact. technology, telemedicine allows clinicians to see patients off For example, a patient with a phobia of flying may be more site, allowing them to potentially reach individuals in dis- willing to initially engage in VRET. VRET also has the potentant and more remote geographical locations. Multiple stud- tial advantage over typical exposure therapy as it allows for ies have demonstrated the effectiveness of telemedicine to the creation and controlled administration of virtual scenaradminister psychotherapy modalities for PTSD (Morland ios that could be difficult to recreate in office-based settings. et al., 2014; Frueh et al., 2007; Yuen et al., 2015) and OCD Multiple studies and systematic meta-analyses of VRET have (Goetter et al., 2014). Though limited and not specific to anx- found substantial improvements in anxiety symptoms for iety, there is some evidence suggesting comparable outcomes multiple disorders including SAD, specific phobias, PD, and for telemental health for psychopharmacology visits as well PTSD (Kampmann et al., 2016; Opris et al., 2012). These (O’Reilly et al., 2007; Ruskin et al., 2004). Telemental health studies indicate that VRET has a powerful real-life impact may improve accessibility to treatment, especially for those comparable but not superior to existing treatments, with the in rural and underserved areas, though there are a variety of possible exception of greater efficacy in treating fear of flying technical, safety, and privacy considerations. The American with VRET (Opris et al., 2012). Psychological Association, American Psychiatric Association, and other professional organizations have published guideP H O N E A P P L I C AT I O NS lines for telemental health treatment to address these issues. With the advent and ubiquity of smartphones, there are numerous phone applications (apps) marketed to enhance B I O FE E D BAC K mental health, including for those with anxiety disorders. In the context of anxiety, biofeedback is the process by which A recent study identified 208 such apps from searching mulindividuals learn to dampen physiological manifestation of tiple psychiatric conditions and related terms (Radovic et al., • A 524 nxiety isorders Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University PressD USA - OSO, 2018. 15:10:22.
2016; Anthes, 2016). As previously mentioned, a substantial majority of patients with anxiety disorders do not seek treatment with mental health clinicians. Many such patients may turn to these apps, though there is considerable uncertainty about their safety, utility, and privacy. In the coming years, clinicians may integrate various apps into their treatments, such as those geared toward CBT or relaxation techniques. CURRENT CHALLENGES AND FUTURE DIRECTIONS Despite great strides in our understanding of the neurobiology of fear conditioning and multiple candidate targets/mechanisms, attempts to translate preclinical research into novel therapies for anxiety disorders have generally been disappointing (Griebel and Holmes, 2013). Why is the development of novel anxiety disorder treatments so difficult? A number of factors contribute to make this translational work particularly challenging. First is the issue of how we conceptualize and define diagnostic entities. What exactly are we treating? The modern categorical DSM/ICD system (since the DSM-III), in which conditions are defined based on symptom clusters, provides a framework that allows for greater interclinician reliability. However, a significant criticism remains that these diagnostic entities are not valid constructs with distinct pathophysiology. Just as agoraphobia was classified as a form of dizziness in the nineteenth century, might our current anxiety disorder constructs unduly emphasize certain features that are less essential from a translational neuroscience perspective? By using an exclusively symptom-based approach to diagnosis, we may be grouping together multiple conditions that merely lead to final common pathway anxiety syndromes, analogous to “inflammation” or “fibrosis” in cellular pathology, that do not indicate etiology. The phenomenology of anxiety and various frameworks for understanding the anxiety constructs are of central importance as we consider what exactly a “novel therapy” may seek to treat, and the extent to which preclinical models may or may not capture essential features of these phenomena. At least five broad frameworks for understanding fear and anxiety have been described: physiological-neuropsychological; functionalism; learning theory; existential; and psychodynamic (Moehle and Levitt, 1991). Preclinical rodent studies, for example, may draw exclusively from physiological-neuropsychological and learning theory frameworks and not capture other aspects of anxiety, such as the existential and psychodynamic aspects reflected in excessive worries about relationship failures or not living up to one’s perceived occupational expectations. Although clusters of signs and symptoms guide clinicians in the formation of differential diagnosis throughout medicine, these diagnoses are ideally taken as initial working hypotheses. Other tools (e.g., imaging and laboratory tests) are commonly used to confirm or rule out diagnoses and guide a treatment approach. Such tools have some, though minimal application in psychiatry currently. Patients who currently meet diagnostic criteria for a specific anxiety disorder
may someday be stratified into one of many subtypes based on underlying vulnerabilities, distinct physiology, and/or markers predictive of treatment response. The RDoC framework sidesteps some of the current diagnostic pitfalls by emphasizing “dimensions of observable behavior and neurobiological measures” (Lang et al., 2016). This shift may facilitate a deeper understanding of the neurobiology of transdiagnostic features such as the physiology of fear. There are pitfalls of using the RDoC framework as well, including a potential difficulty of translating back toward novel treatments in the clinical DSM/ICD categorical system, which remains the dominant nosology for mental health practice and which is a framework with some utility for clinicians and patients. For example, while it may be useful to consider the continuous nature of a variable’s expression from a neurobiological perspective, clinicians rely on discrete boundaries to separate normal from pathology to guide consistent treatment. This is true whether the diagnostic construct (based on otherwise continuous variables) is hypertension, diabetes, or GAD. Another obstacle to developing novel treatments for anxiety disorders is the limitations of our preclinical models. Although many such models exist, their fidelity to the conditions they represent may be incomplete or even misleading. As discussed, the approach-avoidance conflict models may better reflect acute anxiety symptoms, or state, and not the predisposition toward such symptoms reflecting an anxiety disorder, or trait. Developments in our understanding of the neurobiology of fear learning and extinction has been a major advance in recent years and has guided significant research on therapeutic targets. Though here too, the model may capture features of some anxiety disorders while missing essential features of others, such as functional impairment due to excessive worries about one’s work or relationships. Finally, it is worth noting that the majority of rodent models use only males, while there is a higher prevalence of anxiety disorders in women than men. The possibility of sex-specific physiological mechanisms should be further addressed. Getting past conceptual limitations of these diagnostic constructs and issues of validity of preclinical models, there remains a significant challenge: developing targeted treatments. Medications lack specificity in that they frequently interact with multiple receptor subtypes within a class as well as across different classes. In addition to lacking specificity in terms of receptor type, there is also the issue of lacking regional specificity in the brain, with drugs potentially exerting effects in any region that happens to express the target receptor(s). Extinction learning may be enhanced with local infusion of a compound into a particular brain region, while administering the same compound systemically may have no or even opposite net effects. Drugs may also exert differential and countervailing effects on extinction learning, consolidation, and retrieval (Singewald et al., 2015). Systemic administration of medications that interact with multiple neurotransmitter systems and in multiple regions is a recipe for unintended consequences, including side effects that make a compound undesirable as a treatment for anxiety disorders. Some brain stimulation techniques (e.g., TMS, tDCS) are initially more
39. NS.ovel p roaches T reating Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney,Aetpal., Oxford Universityfor Press USA - OSO, 2018. 15:10:22.
focal in their targeting, though they too are blunt instruments without the specificity to target only relevant cells within a circuit of interest. This too could lead to the downstream activation or deactivation of other circuits that are not the desired target of treatment. Therefore, even when therapeutic target mechanisms are identified, there are a variety of challenges that can impede the subsequent development of a relevant novel treatment. C O N C LU S I O N Despite significant challenges to the development of novel anxiety disorder treatments there is some cause for optimism. Advances in basic research, such as optogenetics, have already yielded significant insights into the biology of fear conditioning and extinction at the level of specific cell types within regions of the fear learning and extinction learning circuits (Bukalo et al., 2014). Such work clarifies the fundamental mechanisms and points to novel targets. Work in several areas such as neuropeptides, brain stimulation, and rt-f MRI biofeedback remain in nascent stages, though they (along with a number of other strategies) show some promise. Technological developments such as ICBT and telemental health may also improve access to existing treatments and could benefit millions with untreated or undertreated anxiety disorders. DISCLOSURES Drs. Sturman and Kaufman and Ms. Bigony declare no conflict of interest to disclose. Dr. Ressler is on the Scientific Advisory Boards for Resilience Therapeutics, Sheppard Pratt-Lieber Research Institute, Laureate Institute for Brain Research, The Army STARRS Project, and the Anxiety and Depression Association of America. He holds patents for use of DCS and psychotherapy, targeting PAC1 receptor for extinction, targeting tachykinin 2 for prevention of fear, targeting angiotensin to improve extinction of fear. Dr. Ressler is also founding member of Extinction Pharmaceuticals to develop d-Cycloserine to augment the effectiveness of psychotherapy, for which he has received no equity or income within the last 3 years. He receives or has received research funding from NIMH, HHMI, NARSAD, and the Burroughs Wellcome Foundation. REFERENCES Aerni, A., Traber, R., et al. (2004). Low-dose cortisol for symptoms of posttraumatic stress disorder. Am J Psychiatry 161(8):1488–1490. Amir, N., Beard, C., et al. (2009). Attention modification program in individuals with generalized anxiety disorder. J Abnorm Psychol 118(1):28–33. Amos, T., Stein, D.J., and Ipser, J.C. (2014). Pharmacological interventions for preventing post-traumatic stress disorder (PTSD). Cochrane Database Syst Rev (7):CD006239. Anthes, E. (2016). Mental health: there’s an app for that. Nature 532 (7597):20–23.
Asthana, M., Nueckel, K., et al. (2013). Effects of transcranial direct current stimulation on consolidation of fear memory. Front Psychiatry 4:107. Baker, D.G., Ekhator, N.N., et al. (2005). Higher levels of basal serial CSF cortisol in combat veterans with posttraumatic stress disorder. Am J Psychiatry 162(5):992–994. Barak, A., Hen, L., et al. (2008). A comprehensive review and a meta- analysis of the effectiveness of internet-based psychotherapeutic interventions. J Technol Hum Serv 26(2–4):109–160. Beard, C. (2011). Cognitive bias modification for anxiety: current evidence and future directions. Expert Rev Neurother 11(2):299–311. Beard, C., and Amir, N. (2009). Interpretation in social anxiety: when meaning precedes ambiguity. Cognit Ther Res 33(4):406–415. Belkin, M.R., and Schwartz, T.L. (2015). Alpha-2 receptor agonists for the treatment of posttraumatic stress disorder. Drugs Context 4:212286. Berardi, A., Schelling, G., and Campolongo, P. (2016). The endocannabinoid system and Post Traumatic Stress Disorder (PTSD): From preclinical findings to innovative therapeutic approaches in clinical settings. Pharmacol Res 111:668–678. Berlim, M.T., and Van Den Eynde, F. (2014). Repetitive transcranial magnetic stimulation over the dorsolateral prefrontal cortex for treating posttraumatic stress disorder: an exploratory meta-analysis of randomized, double-blind and sham-controlled trials. Can J Psychiatry 59(9):487–496. Bishop, S.R., Lau, M., et al. (2004). Mindfulness: a proposed operational definition. Clinical Psychol Sci Pract 11(3):230–241. Bowers, M.E. and Ressler, K.J. (2015). An overview of translationally informed treatments for PTSD: animal models of Pavlovian fear conditioning to human clinical Trials. Biol Psychiatry 78(5):e15–27. Brunet, A., Orr, S.P., et al. (2008). Effect of post-retrieval propranolol on psychophysiologic responding during subsequent script- driven traumatic imagery in post-traumatic stress disorder. J Psychiatr Res 42(6):503–506. Bukalo, O., Pinard, C.R., and Holmes, A. (2014). Mechanisms to medicines: elucidating neural and molecular substrates of fear extinction to identify novel treatments for anxiety disorders. Br J Pharmacol 171(20):4690–4718. Buyukturkoglu, K., Roettgers, H., et al. (2015). Self-regulation of anterior insula with real- time fMRI and its behavioral effects in obsessive-compulsive disorder: a feasibility study. PLoS One 10(8):e0135872. Cain, C.K., Blouin, A.M., and Barad, M. (2004). Adrenergic transmission facilitates extinction of conditional fear in mice. Learn Mem 11(2):179–187. Cameron, C., Watson, D., and Robinson, J. (2014). Use of a synthetic cannabinoid in a correctional population for posttraumatic stress disorder- related insomnia and nightmares, chronic pain, harm reduction, and other indications: a retrospective evaluation. J Clin Psychopharmacol 34(5):559–564. Cardoso, C., Linnen, A.-M, et al. (2012). Coping style moderates the effect of intranasal oxytocin on the mood response to interpersonal stress. Exp Clin Psychopharmacol 20(2):84–91. Carhart-Harris, R.L., Wall, M.B., et al. (2014). The effect of acutely administered MDMA on subjective and BOLD-f MRI responses to favourite and worst autobiographical memories. Int J Neuropsychopharmacol 17(4):527–540. Chhatwal, J.P., Gutman, A.R., et al. (2009). Functional interactions between endocannabinoid and CCK neurotransmitter systems may be critical for extinction learning. Neuropsychopharmacology 34(2):509–521. Coric, V., Feldman, H.H., et al. (2010). Multicenter, randomized, double-blind, active comparator and placebo-controlled trial of a corticotropin-releasing factor receptor-1 antagonist in generalized anxiety disorder. Depress Anxiety 27(5):417–425. Cuthbert, B.N. (2014). The RDoC framework: facilitating transition from ICD/DSM to dimensional approaches that integrate neuroscience and psychopathology. World Psychiatry 13(1):28–35. de Quervain, D.J.- F., Bentz, D., et al. (2011). Glucocorticoids enhance extinction-based psychotherapy. Proc Natl Acad Sci U S A 108(16):6621–6625.
• A 526 nxiety isorders Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University PressD USA - OSO, 2018. 15:10:22.
Depping, A.M., Komossa, K., et al. (2010). Second-generation antipsychotics for anxiety disorders. Cochrane Database Syst Rev (12): CD008120. Do-Monte, F.H., Rodriguez-Romaguera, J., et al. (2013). Deep brain stimulation of the ventral striatum increases BDNF in the fear extinction circuit. Front Behav Neurosci 7:102. Dos Santos, R.G., Osório, F.L., et al. (2016). Antidepressive, anxiolytic, and antiaddictive effects of ayahuasca, psilocybin and lysergic acid diethylamide (LSD): a systematic review of clinical trials published in the last 25 years. Ther Adv Psychopharmacol 6(3):193–213. Eckstein, M., Becker, B., et al. (2015). Oxytocin facilitates the extinction of conditioned fear in humans. Biol Psychiatry 78(3):194–202. Eckstein, M., Scheele, D., et al. (2016). Oxytocin facilitates Pavlovian fear learning in males. Neuropsychopharmacology 41(4):932–939. Ellenbogen, M.A., Linnen, A.-M, et al. (2014). Intranasal oxytocin attenuates the human acoustic startle response independent of emotional modulation. Psychophysiology 51(11):1169–1177. Endler, N.S., and Kocovski, N.L. (2001). State and trait anxiety revisited. J Anxiety Disord 15(3):231–245. Eskow Jaunarajs, K.L., Dupre, K.B., et al. (2010). Behavioral and neurochemical effects of chronic L-DOPA treatment on nonmotor sequelae in the hemiparkinsonian rat. Behav Pharmacol 21(7):627–637. Feder, A., Parides, M.K., et al. (2014). Efficacy of intravenous ketamine for treatment of chronic posttraumatic stress disorder: a randomized clinical trial. JAMA Psychiatry 71(6):681–688. Fernandez Espejo, E. (2003). Prefrontocortical dopamine loss in rats delays long- term extinction of contextual conditioned fear, and reduces social interaction without affecting short-term social interaction memory. Neuropsychopharmacology 28(3):490–498. Fossey, M.D., Lydiard, R.B., et al. (1996). Cerebrospinal fluid corticotropin- releasing factor concentrations in patients with anxiety disorders and normal comparison subjects. Biol Psychiatry 39(8):703–707. Fraser, G.A. (2009). The use of a synthetic cannabinoid in the management of treatment-resistant nightmares in posttraumatic stress disorder (PTSD). CNS Neurosci Ther 15(1):84–88. Frueh, B.C., Monnier, J., et al. (2007). A randomized trial of telepsychiatry for post-traumatic stress disorder. J Telemed Telecare 13(3):142–147. Furini, C.R., Rossato, J.I., et al. (2010). Beta-adrenergic receptors link NO/sGC/PKG signaling to BDNF expression during the consolidation of object recognition long-term memory. Hippocampus 20(5): 672–683. Gasser, P., Holstein, D., et al. (2014). Safety and efficacy of lysergic acid diethylamide-assisted psychotherapy for anxiety associated with life- threatening diseases. J Nerv Ment Dis 202(7):513–520. Giampaolo, P., Alessandra, A., et al. (2016). Is there room for second-generation antipsychotics in the pharmacotherapy of panic disorder? A Systematic review based on PRISMA guidelines. Int J Mol Sci 17(4). Glas, G. (2003). A conceptual history of anxiety and depression. In: den Boer. J.A., and Sitsen, J.N., eds. Handbook on Anxiety and Depression, pp. 1–48. New York: Marcel Dekker. Goetter, E.M., Herbert, J.D., et al. (2014). An open trial of videoconference- mediated exposure and ritual prevention for obsessive-compulsive disorder. J Anxiety Disord 28(5):460–462. Graham, D.P., Nielsen, D.A., et al. (2014). Examining the utility of using genotype and functional biology in a clinical pharmacology trial: pilot testing dopamine β-hydroxylase, norepinephrine, and post-traumatic stress disorder. Psychiatr Genet 24(4):181–182. Greenberg, B.D., Gabriels, L.A., et al. (2010). Deep brain stimulation of the ventral internal capsule/ventral striatum for obsessive-compulsive disorder: worldwide experience. Mol Psychiatry 15(1):64–79. Griebel, G., and Holsboer, F. (2012). Neuropeptide receptor ligands as drugs for psychiatric diseases: the end of the beginning? Nat Rev Drug Discov 11(6):462–478. Griebel, G., and Holmes, A. (2013). 50 years of hurdles and hope in anxiolytic drug discovery. Nat Rev Drug Discov 12(9):667–687. Grob, C.S., Danforth, A.L., et al. (2011). Pilot study of psilocybin treatment for anxiety in patients with advanced-stage cancer. Arch Gen Psychiatry 68(1):71–78.
Guastella, A.J., Dadds, M.R., et al. (2007). A randomized controlled trial of the effect of D-cycloserine on exposure therapy for spider fear. J Psychiatr Res 41(6):466–471. Guastella, A.J., Richardson, R., et al. (2008). A randomized controlled trial of D-cycloserine enhancement of exposure therapy for social anxi ety disorder. Biol Psychiatry 63(6):544–549. Guastella, A.J., Howard, A.L., et al. (2009). A randomized controlled trial of intranasal oxytocin as an adjunct to exposure therapy for social anxi ety disorder. Psychoneuroendocrinology 34(6):917–923. Haaker, J., Gaburro, S., et al. (2013). Single dose of L-dopa makes extinction memories context-independent and prevents the return of fear. Proc Natl Acad Sci U S A 110(26):E2428–E2436. Hakamata, Y., Lissek, S., et al. (2010). Attention bias modification treatment: a meta-analysis toward the establishment of novel treatment for anxiety. Biol Psychiatry 68(11):982–990. Haller, J., Aliczki, M., et al. (2013). Classical and novel approaches to the preclinical testing of anxiolytics: A critical evaluation. Neurosci Biobehav Rev 37(10):2318–2330. Hampson, M., Stoica, T., et al. (2012). Real-time fMRI biofeedback targeting the orbitofrontal cortex for contamination anxiety. J Vis Exp (59): pii: 3535. Hart, G., Panayi, M.C., et al. (2014). Benzodiazepine treatment can impair or spare extinction, depending on when it is given. Behav Res Ther 56:22–29. Heilbronner, S.R., Rodriguez-Romaguera, J., et al. (2016) Circuit-based corticostriatal homologies between rat and primate. Biol Psychiatry 80(7):509–521. Herrmann, M.J., Beier, J.S., et al. (2016). Transcranial direct current stimulation (tDCS) of the right inferior frontal gyrus attenuates skin conductance responses to unpredictable threat conditions. Front Hum Neurosci 10:352. Higgins, E.T., Klein, R., and Strauman, T. (1985). Self-concept discrepancy theory: A psychological model for distinguishing among different aspects of depression and anxiety. Soc Cogn 3(1):51. Hofmann, S.G. (2014). D-cycloserine for treating anxiety disorders: making good exposures better and bad exposures worse. Depress Anxiety 31(3):175–177. Hofmann, S.G., Otto, M.W., et al. (2015a). D-cycloserine augmentation of cognitive behavioral therapy for anxiety disorders: an update. Curr Psychiatry Rep 17(1):532. Hofmann, S.G., Fang, A., and Brager, D.N. (2015b). Effect of intranasal oxytocin administration on psychiatric symptoms: a meta-analysis of placebo-controlled studies. Psychiatry Res 228(3):708–714. Ironside, M., O’Shea, J., et al. (2016). Frontal cortex stimulation reduces vigilance to threat: implications for the treatment of depression and anxiety. Biol Psychiatry 79(10):823–830. Jerath, R., Barnes, V.A., et al. (2012). Dynamic change of awareness during meditation techniques: neural and physiological correlates. Front Hum Neurosci 6:131. Jerath, R., Crawford, M.W., et al. (2015). Self-regulation of breathing as a primary treatment for anxiety. Appl Psychophysiol Biofeedback 40(2):107–115. Jetly, R., Heber, A., et al. (2015). The efficacy of nabilone, a synthetic cannabinoid, in the treatment of PTSD-associated nightmares: a preliminary randomized, double-blind, placebo-controlled cross-over design study. Psychoneuroendocrinology 51:585–588. Kampmann, I.L., Emmelkamp, P.M.G, and Morina, N. (2016). Meta- analysis of technology-assisted interventions for social anxiety disorder. J Anxiety Disord 42:71–84. Kessler, R.C., Aguilar-Gaxiola, S., et al. (2009). The global burden of mental disorders: an update from the WHO World Mental Health (WMH) surveys. Epidemiol Psichiatr Soc 18(1):23–33. Klein, A.M., Rapee, R.M., et al. (2015). Interpretation modification training reduces social anxiety in clinically anxious children. Behav Res Ther 75:78–84. Koek, R.J., Langevin, J.-P, et al. (2014). Deep brain stimulation of the basolateral amygdala for treatment-refractory combat post-traumatic stress disorder (PTSD): study protocol for a pilot randomized controlled trial with blinded, staggered onset of stimulation. Trials 15:356.
39. NS.ovel p roaches T reating Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney,Aetpal., Oxford Universityfor Press USA - OSO, 2018. 15:10:22.
Koob, G.F., and Zorrilla, E.P. (2012). Update on corticotropin-releasing factor pharmacotherapy for psychiatric disorders: a revisionist view. Neuropsychopharmacology 37(1):308–309. Kulisevsky, J., Pascual-Sedano, B., et al. (2007). Acute effects of immediate and controlled-release levodopa on mood in Parkinson’s disease: A double-blind study. Mov Disord 22(1):62–67. Kushner, M.G., Kim, S.W., et al. (2007). D- cycloserine augmented exposure therapy for obsessive-compulsive disorder. Biol Psychiatry 62(8):835–838. Lang, P.J., McTeague, L.M., and Bradley, M.M. (2016). RDoC, DSM, and the reflex physiology of fear: a biodimensional analysis of the anxiety disorders spectrum. Psychophysiology 53(3):336–347. Langevin, J.-P, De Salles, A.A.F, et al. (2010). Deep brain stimulation of the amygdala alleviates post-traumatic stress disorder symptoms in a rat model. J Psychiatr Res 44(16):1241–1245. Li, H., Wang, J., et al. (2014). Repetitive transcranial magnetic stimulation (rTMS) for panic disorder in adults. Cochrane Database Syst Rev (9):CD009083. Liberzon, I., King, A.P., et al. (2014). Interaction of the ADRB2 gene polymorphism with childhood trauma in predicting adult symptoms of PTSD. JAMA Psychiatry 71(10):1174–1182. Lin, E.-J.D. (2012). Neuropeptides as therapeutic targets in anxiety disorders. Curr Pharm Des 18(35):5709–5727. Linetzky, M., Pergamin-Hight, L., et al. (2015). Quantitative evaluation of the clinical efficacy of attention bias modification treatment for anxiety disorders. Depress Anxiety 32(6):383–391. Ludäscher, P., Schmahl, C., et al. (2015). No evidence for differential dose effects of hydrocortisone on intrusive memories in female patients with complex post-traumatic stress disorder—a randomized, double-blind, placebo-controlled, crossover study. J Psychopharmacol 29(10):1077–1084. Mahan, A.L., and Ressler, K.J. (2012). Fear conditioning, synaptic plasticity and the amygdala: implications for posttraumatic stress disorder. Trends Neurosci 35(1):24–35. Mantovani, A., Aly, M., et al. (2013). Randomized sham controlled trial of repetitive transcranial magnetic stimulation to the dorsolateral prefrontal cortex for the treatment of panic disorder with comorbid major depression. J Affect Disord 144(1-2):153–159. Maricle, R.A., Nutt, J.G., et al. (1995). Dose-response relationship of levodopa with mood and anxiety in fluctuating Parkinson’s disease: a double- blind, placebo- controlled study. Neurology 45(9):1757–1760. Marin, M.-F, Camprodon, J.A., et al. (2014). Device-based brain stimulation to augment fear extinction: implications for PTSD treatment and beyond. Depress Anxiety 31(4):269–278. Marks, I.M., Swinson, R.P., et al. (1993). Alprazolam and exposure alone and combined in panic disorder with agoraphobia. A controlled study in London and Toronto. Br J Psychiatry 162:776–787. Mathews, A., and Mackintosh, B. (2000). Induced emotional interpretation bias and anxiety. J Abnorm Psychol 109(4):602–615. Meyerbroeker, K., Powers, M.B., et al. (2012). Does yohimbine hydrochloride facilitate fear extinction in virtual reality treatment of fear of flying? A randomized placebo-controlled trial. Psychother Psychosom 81(1):29–37. Meyer-Lindenberg, A., Domes, G., et al. (2011). Oxytocin and vasopressin in the human brain: social neuropeptides for translational medicine. Nat Rev Neurosci 12(9):524–538. Mithoefer, M.C., Wagner, M.T., et al. (2011). The safety and efficacy of {+/-} 3,4-methylenedioxymethamphetamine-assisted psychotherapy in subjects with chronic, treatment-resistant posttraumatic stress disorder: the first randomized controlled pilot study. J Psychopharmacol 25(4):439–452. Mithoefer, M.C., Wagner, M.T., et al. (2013). Durability of improvement in post-traumatic stress disorder symptoms and absence of harmful effects or drug dependency after 3,4- methylenedioxymethamphetamine- assisted psychotherapy: a prospective long-term follow-up study. J Psychopharmacol 27(1):28–39. Mobini, S., Mackintosh, B., et al. (2014). Effects of standard and explicit cognitive bias modification and computer- administered
cognitive-behaviour therapy on cognitive biases and social anxiety. J Behav Ther Exp Psychiatry 45(2):272–279. Moehle, K.A. and Levitt, E.E. (1991). The history of the concepts of fear and anxiety. In: Eugene, W.C, ed. Clinical psychology: historical and research foundations (pp. 159–182). Springer. Morland, L.A., Mackintosh, M.-A, et al. (2014). Cognitive processing therapy for posttraumatic stress disorder delivered to rural veterans via telemental health: a randomized noninferiority clinical trial. J Clin Psychiatry 75(5):470–476. Morrison, F.G., and Ressler, K.J. (2014). From the neurobiology of extinction to improved clinical treatments. Depress Anxiety 31(4):279–290. Murrough, J.W., Yaqubi, S., et al. (2015). Emerging drugs for the treatment of anxiety. Expert Opin Emerg Drugs 20(3):393–406. Nègre-Pagès, L., Grandjean, H., et al. (2010). Anxious and depressive symptoms in Parkinson’s disease: the French cross-sectional DoPaMiP study. Mov Disord 25(2):157–166. Neumeister, A., Normandin, M.D., et al. (2013). Elevated brain cannabinoid CB1 receptor availability in post-traumatic stress disorder: a positron emission tomography study. Mol Psychiatry 18(9):1034–1040. Norberg, M.M., Krystal, J.H., and Tolin, D.F. (2008). A meta-analysis of D-cycloserine and the facilitation of fear extinction and exposure therapy. Biol Psychiatry 63(12):1118–1126. Norton, A.R., Abbott, M.J., et al. (2015). A systematic review of mindfulness and acceptance-based treatments for social anxiety disorder. J Clin Psychol 71(4):283–301. O’Reilly, R., Bishop, J., et al. (2007). Is telepsychiatry equivalent to face- to-face psychiatry? Results from a randomized controlled equivalence trial. Psychiatr Serv 58(6):836–843. Oehen, P., Traber, R., et al. (2013). A randomized, controlled pilot study of MDMA (± 3,4-methylenedioxymethamphetamine)-assisted psychotherapy for treatment of resistant, chronic post-traumatic stress disorder (PTSD). J Psychopharmacol 27(1):40–52. Olthuis, J.V., Watt, M.C., et al. (2016). Therapist-supported Internet cognitive behavioural therapy for anxiety disorders in adults. Cochrane Database Syst Rev 3:CD011565. Opriş D, Pintea, S., et al. (2012). Virtual reality exposure therapy in anxiety disorders: a quantitative meta-analysis. Depress Anxiety 29(2): 85–93. Ori, R., Amos, T., et al. (2015). Augmentation of cognitive and behavioural therapies (CBT) with d-cycloserine for anxiety and related disorders. Cochrane Database Syst Rev (5):CD007803. Oyebode, F. (2008). Sims’ symptoms in the mind: an introduction to descriptive psychopathology. New York: Elsevier Health Sciences UK. Parsons, R. and Ressler, K.J. (2013). Implications of memory modulation for post-traumatic stress and fear disorders. Nat Neurosci 16(2):146–153. Peña, D.F., Childs, J.E., et al. (2014). Vagus nerve stimulation enhances extinction of conditioned fear and modulates plasticity in the pathway from the ventromedial prefrontal cortex to the amygdala. Front Behav Neurosci 8:327. Pitman, R.K., Sanders, K.M., et al. (2002). Pilot study of secondary prevention of posttraumatic stress disorder with propranolol. Biol Psychiatry 51(2):189–192. Powers, M.B., Smits, J.A.J., et al. (2009). Facilitation of fear extinction in phobic participants with a novel cognitive enhancer: a randomized placebo controlled trial of yohimbine augmentation. J Anxiety Disord 23(3):350–356. Prasko, J., Záleský, R., et al. (2007). The effect of repetitive transcranial magnetic stimulation (rTMS) add on serotonin reuptake inhibitors in patients with panic disorder: a randomized, double blind sham controlled study. Neuro Endocrinol Lett 28(1):33–38. Rabinak, C.A., and Phan, K.L. (2014). Cannabinoid modulation of fear extinction brain circuits: a novel target to advance anxiety treatment. Curr Pharm Des 20(13):2212–2217. Radovic, A., Vona, P.L., et al. (2016). Smartphone applications for mental health. Cyberpsychol Behav Soc Netw 19(7):465–470. Raskind, M.A., Peskind, E.R., et al. (2003). Reduction of nightmares and other PTSD symptoms in combat veterans by prazosin: a placebo- controlled study. Am J Psychiatry 160(2):371–373.
• A 528 nxiety isorders Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University PressD USA - OSO, 2018. 15:10:22.
Rasmusson, A.M., Hauger, R.L., et al. (2000). Low baseline and yohimbine- stimulated plasma neuropeptide Y (NPY) levels in combat-related PTSD. Biol Psychiatry 47(6):526–539. Rejón Altable, C. (2012). Logic structure of clinical judgment and its relation to medical and psychiatric semiology. Psychopathology 45(6):344–351. Ressler, K.J., Rothbaum, B.O., et al. (2004). Cognitive enhancers as adjuncts to psychotherapy: use of D-cycloserine in phobic individuals to facilitate extinction of fear. Arch Gen Psychiatry 61(11): 1136–1144. Riebe, C.J., Pamplona, F.A., et al. (2012). Fear relief—toward a new conceptual framework and what endocannabinoids gotta do with it. Neuroscience 204:159–185. Rodrigues, H., Figueira, I., et al. (2014). Does D-cycloserine enhance exposure therapy for anxiety disorders in humans? A meta-analysis. PLoS One 9(7):e93519. Rodriguez-Romaguera, J., Do-Monte, F.H.M, and Quirk, G.J. (2012). Deep brain stimulation of the ventral striatum enhances extinction of conditioned fear. Proc Natl Acad Sci U S A 109(22):8764–8769. Rodriguez-Romaguera, J., Do-Monte, F.H., et al. (2015). Enhancement of fear extinction with deep brain stimulation: evidence for medial orbitofrontal involvement. Neuropsychopharmacology 40(7): 1726–1733. Ruskin, P.E., Silver-Aylaian, M., et al. (2004). Treatment outcomes in depression: comparison of remote treatment through telepsychiatry to in-person treatment. Am J Psychiatry 161(8):1471–1476. Sah, R., Ekhator, N.N., et al. (2009). Low cerebrospinal fluid neuropeptide Y concentrations in posttraumatic stress disorder. Biol Psychiatry 66(7):705–707. Scheinost, D., Stoica, T., et al. (2013). Orbitofrontal cortex neurofeedback produces lasting changes in contamination anxiety and resting- state connectivity. Transl Psychiatry 3:e250. Schmidt, N.B., Richey, J.A., et al. (2009). Attention training for generalized social anxiety disorder. J Abnorm Psychol 118(1):5–14. Schoenberg, P.L.A, and David, A.S. (2014). Biofeedback for psychiatric disorders: a systematic review. Appl Psychophysiol Biofeedback 39(2):109–135. Seals, D.R., Suwarno, N.O., and Dempsey, J.A. (1990). Influence of lung volume on sympathetic nerve discharge in normal humans. Circ Res 67(1):130–141. Shiozawa, P., Leiva A.P.G., et al. (2014). Transcranial direct current stimulation for generalized anxiety disorder: a case study. Biol Psychiatry 75(11):e17–e18. Singewald, N., Schmuckermair, C., et al. (2015). Pharmacology of cognitive enhancers for exposure-based therapy of fear, anxiety and trauma- related disorders. Pharmacol Ther 149:150–190. Smits, J.A.J, Rosenfield, D., et al. (2014). Yohimbine enhancement of exposure therapy for social anxiety disorder—a randomized controlled trial. Biol Psychiatry 75(11):840–846. Soravia, L.M., Heinrichs, M., et al. (2014). Glucocorticoids enhance in vivo exposure-based therapy of spider phobia. Depress Anxiety 31(5):429–435. Soumier, A., Banasr, M., et al. (2009). Mechanisms contributing to the phase-dependent regulation of neurogenesis by the novel antidepressant, agomelatine, in the adult rat hippocampus. Neuropsycho pharmacology 34(11):2390–2403. Spek, V., Cuijpers, P., et al. (2007). Internet-based cognitive behaviour therapy for symptoms of depression and anxiety: a meta-analysis. Psychol Med 37(3):319–328.
Stein, D.J., Ahokas, A., et al. (2012). Agomelatine prevents relapse in generalized anxiety disorder: a 6- month randomized, double- blind, placebo-controlled discontinuation study. J Clin Psychiatry 73(7):1002–1008. Stein, D.J., Ahokas, A., et al. (2014). Agomelatine in generalized anxiety disorder: an active comparator and placebo-controlled study. J Clin Psychiatry 75(4):362–368. Stein, D.J., Ahokas, A.A., and de Bodinat, C. (2008). Efficacy of agomelatine in generalized anxiety disorder: a randomized, double- blind, placebo-controlled study. J Clin Psychopharmacol 28(5): 561–566. Stein, D.J., Picarel-Blanchot, F., Kennedy, S.H. (2013). Efficacy of the novel antidepressant agomelatine for anxiety symptoms in major depression. Hum Psychopharmacol 28(2):151–159. Strawn, J.R., and Geracioti, T.D. Jr. (2008). Noradrenergic dysfunction and the psychopharmacology of posttraumatic stress disorder. Depress Anxiety 25(3):260–271. Tardito, D., Molteni, R., et al. (2012). Synergistic mechanisms involved in the antidepressant effects of agomelatine. Eur Neuropsychopharmacol 22(Suppl 3):S482–S486. Taylor, S., Abramowitz, J.S., McKay, D. (2012). Non-adherence and non-response in the treatment of anxiety disorders. J Anxiety Disord 26(5):583–589. Vaiva, G., Ducrocq, F., et al. (2003). Immediate treatment with propranolol decreases posttraumatic stress disorder two months after trauma. Biol Psychiatry 54(9):947–949. van ‘t Wout, M., Mariano, T.Y., et al. (2016). Can transcranial direct current stimulation augment extinction of conditioned fear? Brain Stimul 9(4):529–536. Van Bockstaele, B., Salemink, E., et al. (2015). Limited generalisation of changes in attentional bias following attentional bias modification with the visual probe task. Cogn Emot 1–8. Velasques, B., Diniz, C., et al. (2014). Deep brain stimulation: a new treatment in mood and anxiety disorders. CNS Neurol Disord Drug Targets 13(6):961–971. Vlemincx, E., Van Diest, I., and Van den Bergh, O. (2016). A sigh of relief or a sigh to relieve: the psychological and physiological relief effect of deep breaths. Physiol Behav 165:127–135. Wu, G., Feder, A., et al. (2011). Central functions of neuropeptide Y in mood and anxiety disorders. Expert Opin Ther Targets 15(11):1317–1331. Yehuda, R., Brand, S., and Yang, R.- K . (2006). Plasma neuropeptide Y concentrations in combat exposed veterans: relationship to trauma exposure, recovery from PTSD, and coping. Biol Psychiatry 59(7):660–663. Yehuda, R., Bierer, L.M., et al. (2015). Cortisol augmentation of a psychological treatment for warfighters with posttraumatic stress disorder: randomized trial showing improved treatment retention and outcome. Psychoneuroendocrinology 51:589–597. Young, M.B., Andero, R., et al. (2015). 3,4,- Methylene- dioxymethamphetamine facilitates fear extinction learning. Transl Psychiatry 5:e634. Yuen, E.K., Gros, D.F., et al. (2015). Randomized controlled trial of home- based telehealth versus in- person prolonged exposure for combat-related PTSD in veterans: preliminary results. J Clin Psychol 71(6):500–512. Zorrilla, E.P., and Koob, G.F. (2010). Progress in corticotropin-releasing factor- 1 antagonist development. Drug Discov Today 15(9–10): 371–383.
39. NS.ovel p roaches T reating Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis Charney,Aetpal., Oxford Universityfor Press USA - OSO, 2018. 15:10:22.
Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press USA - OSO, 2018. 15:10:22.
40. CURRENT AND EXPERIMENTAL TREATMENTS FOR ANXIET Y DISORDER S Adam J. Guastella, Alice Norton, Gail A. Alvares, and Christine Yun Ju Song
INTRODUCTION Anxiety is conceptualized as a coherent structure of cognitive and affective components within the defensive motivational system that responds to perceived future threat or danger (Barlow, 2002). This complex system responds to perceived threatening information with cognitive and affective processes, physiological reactions, and behavioral responses, which relate to the well-known defensive behaviors of “freeze, fight, or flight” involved in the fear response. While anxiety is an adaptive response that serves both to alert and prepare the organism for potential threat (Barlow, 2002), pathological anxiety is characterized by its excessive expression across dimensions of duration, frequency, and/ or intensity (Barlow, 2002). Anxiety disorders are thereby considered disorders of fear dysregulation (Myers and Davis, 2007). A remarkable amount of progress has been made in the development of effective and acceptable treatments for anxiety disorders. Although evidence-based psychological and pharmacological treatments show clinical efficacy across randomized controlled trials (RCTs), a significant number of individuals do not respond to treatment, or they relapse after treatment cessation. Such problems have led to a surge of interest in recent years toward the development of novel approaches in the treatment of anxi ety disorders. Key priorities include the need to identify and target the mechanisms (behavioral, cognitive, neurobiological) that underlie anxiety and to develop comprehensive bio-psycho-social models that take into account factors involved in adherence and treatment response (Taylor et al., 2012). The aim of this chapter, therefore, is to review evidence for recent and promising novel approaches to treat anxiety disorders that extend upon and augment existing best-practice interventions. After a discussion of the current state of evidence-based treatments for anxiety, evidence will be reviewed for several novel pharmacological, cognitive, and technological interventions, with reference to the specific neurobiological mechanisms of anxiety targeted in each. The interventions reviewed in this chapter are summarized in Table 40.2.
C U R R E N T S TAT E O F E VI D E N C E - B A S E D T R E AT M E N T S F O R A N X I ET Y D I S O R D E R S Existing psychological and pharmacological treatments for anxiety are well established in clinical settings. Although other psychotherapies (such as mindfulness-based therapy) have received some empirical support, cognitive behavioral therapy (CBT) continues to be the gold standard for psychological treatment of both child and adult anxiety disorders (Barlow et al., 2002). CBT aims to redress the maladaptive cognitive, behavioral, and affective patterns related to the focus of an individuals’ anxiety. Common components of CBT packages for anxiety include psychoeducation, conscious cognitive restructuring of negatively biased thinking, and behavioral exposure (physical or imaginal) to the focus of anxiety to reduce fear and avoidance. Despite robust empirical support, a number of issues remain. CBT is not universally efficacious, nor is it acceptable to all patients, with considerable rates of nonresponders or partial responders to treatment and treatment nonadherence (Taylor et al., 2012). Nonadherence is particularly concerning given that attendance and completion of therapy homework appear to play a role in treatment outcome with CBT (Taylor et al., 2012). The quality of treatment with CBT also varies depending on the therapist, the therapeutic alliance, and the extent to which the therapist’s methods reflect guidelines for evidence-based practice. Pharmacological treatments for anxiety disorders depend upon both the disorder and needs of the individual (see reviews in Bandelow et al., 2012). The preferred psychotropic medication across anxiety disorders are selective serotonin reuptake inhibitors, or SSRIs (Bandelow et al., 2012), which inhibit reuptake at the presynaptic serotonin transporter pump. Overall, the tolerability, efficacy, and safety of this class of medication are acceptable, although drug–drug interactions and side effects during or upon termination of treatment are noted difficulties. Serotonin- norepinephrine reuptake inhibitors (SNRIs) are a more recently developed class of medications that work to inhibit the reuptake of serotonin and norepinephrine, with selectivity for the two neurotransmitters varying across dose and drug. They have adequate
5 3 1 USA - OSO, 2018. Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press 15:10:22.
tolerability and efficacy and are considered alternate first-line treatments to the SSRIs, although these are also not without side effects (Bandelow et al., 2012). Although both tricyclic antidepressants and monoamine oxidase inhibitors (MAOIs) have received support in clinical trials with certain anxiety disorders, they are generally considered third-or fourth-line treatment options because of their side effect profiles and tolerability issues (Ravindran and Stein, 2010). Benzodiazepines are also often prescribed for anxiety disorders, but they work to potentiate the action of the inhibitory neurotransmitter γ-aminobutyric acid (GABA). Although generally effective in reducing acute anxiety, they carry risks of adverse effects, tolerance, and dependence (Bandelow et al., 2012). Further, they have no recognized antidepressant effects or effectiveness as a longer term treatment for chronic anxiety symptoms (Ravindran and Stein, 2010). Other psychotropic medications such as anticonvulsants, azapirones, and atypical antipsychotics do not have a sufficient evidence base at this time to justify their use over other anxiolytic agents for anxiety treatment (Ravindran and Stein, 2010). ß-adrenergic antagonists are often prescribed for social anxiety and there is some evidence that they have efficacy in reducing the physical symptoms associated with this condition. Overall, however, many anxiety disorder patients, refuse to undergo pharmacological treatment for their anxiety, and a substantial proportion of those who do consent fail to respond to medication or adhere to their treatment regime. For many, nonadherence appears to be in part a result of adverse side effects (Taylor et al., 2012). Previous meta-analyses have reported mean dropout rates of 16% and 24% for CBT and serotonergic pharmacotherapy treatment trials, respectively, with mean nonresponse rates of 35% and 30% for the two treatments (Taylor et al., 2012). A common strategy in clinical settings has been to combine psychotherapy and pharmacotherapy, with the assumption that the combination will be more efficacious (Otto et al., 2016). This assumption has either been not been empirically supported, or supported only in the case of some disorders and not when one examines longer term outcomes (Otto et al., 2016). There are also issues surrounding access to current treatments for those in need. In particular, CBT is costly to implement and requires regular meetings with a trained clinician, which reduces accessibility for patients from isolated areas, with low socioeconomic status, limited transport, time, or mobility (Taylor et al., 2012). These individual psychological and practical barriers contribute to a failure to seek treatment and treatment nonadherence (Taylor et al., 2012). There is also increasing acknowledgment of the difficulty involved in ensuring that empirically supported treatments such as CBT are well disseminated by health care professionals, and the lack of rigorous training in CBT techniques among training and registration programs for psychologists (Taylor et al., 2012). There is, therefore, great potential for improvement in uptake and response rates for both psychotherapy and pharmacotherapy for anxiety disorders. Thus, the development of novel augmentation approaches to existing anxiety treatments has the potential to further enhance the cost effectiveness, accessibility, and efficacy of treatment within the community.
N O VE L P H A R M AC O L O G I C A L A PP R OAC H E S As described previously, substantial research and clinical effort has been placed into the augmentation of psychotherapy with traditional anxiolytic medications, despite the lack of consistent evidence for substantive additive benefits (Otto et al., 2016). More recently, however, research efforts have been focused on the development of novel pharmacological adjuncts that capitalize on the neurobiological mechanisms involved in overcoming anxiety to augment the learning processes that take place during psychotherapy. Novel compounds that have shown such promise as cognitive enhancers for psychotherapy include yohimbine hydrochloride, glucocorticoids, and d-cycloserine (DCS; see review in Otto et al., 2016; Singewald et al., 2015). Much of our current understanding of psychological anxiety treatments, and exposure therapy in particular, is based on associative Pavlovian fear conditioning and extinction models. In brief, fear conditioning involves a harmless stimulus (conditioned stimulus, CS) being repeatedly paired with an innately aversive stimulus (unconditioned stimulus, US) that naturally elicits a fear response (unconditioned response, UCR). This can include the initiation of reflexes (e.g., startle and eyeblink responses), release of stress hormones, defensive behaviors, and autonomic arousal. After repeated pairings, the CS comes to elicit the same innate fear response as the US, known as the conditioned response (CR). This conditioned response in animal models is used as an experimental analogue of the human fear response (Barlow, 2002). In order to eliminate this learned fear response, the CS is presented repeatedly without the aversive US (Myers and Davis, 2007). This process is known as extinction and is a major component of successful anxiety reduction. It is likely that there are multiple neural mechanisms involved in fear extinction (Myers and Davis, 2007). Fear conditioning likely involves the formation of an excitatory association between the mental representations of the CS and US (Myers and Davis, 2007). Extinction appears to involve more than a mere forgetting or even “unlearning” of this maladaptive association; rather, it additionally includes the formation of a new competing association that inhibits the excitatory association representing the learned fear response (Myers and Davis, 2007). Evidence in support of this view shows that the fear response can return after the US is unexpectedly presented again (termed reinstatement), when contexts change (renewal), or it may spontaneously reappear after a length of time (Myers and Davis, 2007). Hence, while successful extinction alleviates fear in one context, this may only be temporary and may not generalize to other contexts. There appear to be a number of structures involved in fear conditioning and extinction. In particular, a substantial body of evidence in animals and humans point to the amygdala (especially the basolateral complex or BLA), hippocampus, and prefrontal cortical structures including the medial prefrontal cortex (mPFC), orbital cortex, and insula in humans and the prelimbic and infralimbic cortices in rats (see reviews in Bishop, 2007; Herry et al., 2010;). The amygdala plays a
• A 532 nxiety isorders Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University PressD USA - OSO, 2018. 15:10:22.
central role in threat processing and is generally acknowledged to be critical to the acquisition and expression of conditioned fear, serving not only as the site where sensory CS and US information converges but also that from which efferent projections initiate the various (autonomic, endocrine, and behavioral) aspects of the conditioned fear response (Herry et al., 2010). Animal studies implicate plasticity within the BLA in the formation of memory traces for fear conditioning and fear extinction (Myers and Davis, 2007), through the process of long-term potentiation. Neuroimaging studies have consistently demonstrated amygdala activation during fear conditioning (Herry et al., 2007). There is evidence to suggest that prefrontal cortical structures may modulate amygdala activity, such that the amygdala is involved in rapid fear conditioning and responses to salient stimuli while prefrontal cortical structures control more complex cognitive processing of fear stimuli, prediction of outcomes, and moderation of behavioral responses according to instrumental contingencies (Bishop, 2007). The N-methyl-d-aspartate (NMDA) receptor, which is activated by the neurotransmitter glutamate, is the most extensively studied glutamate receptor in relation to fear extinction and plays a key role in memory and learning (Otto et al., 2016). Extinction acquisition, and thus the overcoming of the fear response, involves activation of NMDA receptors in the amygdala, while plasticity within the mPFC contributes to extinction consolidation and inhibition of the fear response (Otto et al., 2016; Singewald et al., 2015). That is, the mPFC is crucial for short-and long-term memory of extinction learning, thus the retrieval of extinction of memory (Myers and Davis, 2007). The hippocampus is also a key structure in this process, playing a pivotal role in the consolidation of extinction (Quirk and Mueller, 2008) and contextual conditioning (Herry et al., 2010; Alvarez et., 2008; Andreatta et al., 2015). G LU C O C O RT I C O I D S
Glucocorticoids (cortisol in humans and corticosterone in most animals) are a class of steroid hormones that are the major component of adaptive stress responses. Stressful situations produce a range of automatic, behavioral, and endocrine responses, including activation of the hypothalamic–pituitary–adrenal (HPA) axis. The end product of HPA axis activation is increased endogenous glucocorticoid levels that act to increase blood glucose levels, break down protein and fat, and increase inflammatory responses. Later, they also inhibit further HPA axis activity (Tsigos and Chrousos, 2002). Importantly, glucocorticoids play a critical role in learning and memory processes, particularly for emotional stimuli, through their actions at glucocorticoid receptors found in high density in the hippocampus, amygdala, and frontal lobes (Myers and Davis, 2007). While endogenous levels of glucocorticoids increase in response to stress in both animal and human models, acutely administered glucocorticoid agonists selectively enhance and impair memory processes. In rats, glucocorticoid administration dose-dependently enhances memory consolidation of new information when given prior to or immediately after extinction
training, and impairs memory retrieval for stored aversive information (de Quervain et al., 2009). In humans, exogenous administration of cortisol facilitates extinction processes and impairs retrieval of stored fear memories. The effects of cortisol on memory are most strongly observed for emotionally arousing stimuli. Glucocorticoid administration has been shown to enhance memory consolidation and impair recall of words across a number of contexts, with strongest effects observed in the context of emotional arousal (as reviewed in Wolf, 2008). Results of placebo-controlled clinical studies to date suggest that glucocorticoid administration may enhance the extinction of clinical fear. In one study, acute administration of cortisone to individuals with social anxiety disorder prior to a psychosocial stressor reduced self-reported fear across the task (Soravia et al., 2014). For those participants given placebo, individuals with higher endogenous cortisol exhibited less subjective fear, which suggests that higher levels of cortisol may buffer fear in stressful situations. In the same article, the authors also reported that acute hydrocortisone progressively reduced fear induced by pictures of spiders among individuals with arachnophobia. Further, this effect was maintained two days after the last administration, implying a long-term memory consolidation effect. In patients with chronic posttraumatic stress disorder (PTSD), daily low-dose cortisol reduced intensity of reexperiencing symptoms, physiological distress, and frequency of nightmares (Aerni et al., 2004). Lastly, acute cortisol administered in conjunction with exposure- based therapy resulted in significantly fewer fear symptoms at both posttreatment and one-month follow-up in acrophobia patients (de Quervain et al., 2011). Cumulative evidence from preclinical and clinical studies therefore provides promising initial support for the suggestion that both acute and repeated doses of cortisol may reduce anxiety symptoms. Whether cortisol supplemented with CBT for nonphobic anxiety disorders facilitates fear inhibition is still being evaluated (Singewald et al., 2015). Further, more recent evidence suggests that cortisol may enhance consolidation of newly learned associations after successful exposure therapy, implying that an augmentative approach involving combination with exposure-based therapy may provide the strongest clinical effects. YO H I M B I N E H Y D RO C H L O R I D E
Yohimbine, an African plant derivative, is a dietary supplement often used to treat sexual dysfunction and to metabolize fat. A selective competitive α2 adrenergic autoreceptor antagonist, yohimbine acts on the noradrenergic system to modulate the formation and maintenance of emotional and fear memories (Myers and Davis, 2007). In particular, yohimbine increases norepinephrine levels in the hippocampus, amygdala, and prefrontal cortex, areas known to mediate fear extinction (reviewed in Holmes and Quirk, 2010). Initial preclinical findings indicated that mice treated with yohimbine prior to extinction retained cued and contextual extinction memories, even when tested drug- free the next day (Cain et al., 2004; Cain et al., 2012). Paradoxically, yohimbine seems to increase arousal and anxiety in both animals and humans. This finding
4 0. C urrent T reatments nxiety Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press USAfor - OSO, A 2018. 15:10:22.
sparked interest into the ways in which the compound could be used as an adjunct for behavioral exposure- based therapies, especially in relation to treatment-resistant anxiety disorders. That is, Cain et al. (2004) argued that yohimbine may be able to enhance the acute effects of exposure-based treatments where other treatments have failed. However, studies have shown that rats administered yohimbine significantly reduce freezing behavior after extinction but fail to eliminate this fear memory, as return of freezing is evident when tested out of the original context (Morris and Bouton, 2007). This suggests that gains may be context-specific and return of fear may occur upon leaving the therapeutic context. In terms of clinical utility in humans, a study in participants with claustrophobia demonstrated that although acutely administered yohimbine did not initially improve the efficacy of in vivo exposure sessions, at a one-week follow-up yohimbine participants exhibited significantly reduced fear (Powers et al., 2009). This is consistent with animal findings suggestive of stronger effects of yohimbine on memory consolidation after extinction than on initial extinction learning. Another study has also shown that individuals with a fear of flying were given yohimbine or placebo prior to five virtual reality exposure sessions (Meyerbroeker et al., 2012). Results indicated that while noradrenaline activity was increased by yohimbine as expected, no additional effect of the active drug was found on measures of anxiety or treatment outcome. However, an important caveat is that no follow-up assessment was conducted. Given the findings from the previous study by Powers et al. (2009), time of assessment seems to be a critical factor in determining the success of facilitatory effects of yohimbine on exposure therapy. Positive effects in social anxiety disorder (SAD) have also been observed following four sessions consisting of yohimbine being administered prior to a CBT session. This yohimbine augmented CBT-induced improvement was sustained after a 21- day follow-up (Smits et al., 2014). Thus, preliminary evidence suggests that although yohimbine may enhance the outcomes of exposure-based therapies for anxiety disorders, this seems to be only evident after a period of consolidation or in specific contexts, which may limit potential clinical applications. D -C YC L O S E R I N E ( D C S )
DCS is a partial agonist of the glycine binding site in the NMDA receptor complex, which acts to cofacilitate glutamatergic activation of the receptor (Otto et al., 2016). In contrast with the drugs combined with psychotherapy in previous augmentation studies, DCS does not appear to have a direct anx iolytic or anxiogenic effect. Rather, acute doses of DCS appear to augment learning during extinction and thus facilitate exposure therapy (Norberg et al., 2008). It appears that DCS has two facilitatory effects on neuroplasticity in extinction training: first, it facilitates NMDA-dependent potentiation of GABA neurons within the BLA to enhance the learning that normally takes place during extinction, and second, it facilitates NMDA-dependent depotentiation of glutamate neurons in the amygdala (Myers and Davis, 2007).
Empirical Evidence DCS administered systemically or into the amygdala prior to conditioned fear extinction facilitates memory consolidation in rats, with antagonists to the NMDA glycine binding site blocking these effects (as reviewed in Myers and Davis, 2007). Rodent studies indicate that DCS is most effective when given immediately before or after extinction training, which suggests that it works to moderate memory consolidation (Myers and Davis, 2007; Norberg et al., 2008). Research also suggests that DCS may not only enhance fear extinction to target CS, but also reduce fear responses to other stimuli that have been previously paired with the aversive US but are not specifically targeted in extinction training. That is, DCS may promote generalized fear extinction. One way in which these results have been interpreted is that DCS works to devalue the mental representation of the feared US (Myers and Davis, 2007). It suggests that DCS may work not only to speed up fear extinction (see Norberg et al., 2008) but also to enhance the strength of the effect. DCS may also reduce the risk of relapse after exposure-based therapy; in rodent models, DCS reduces reinstatement of fear responses following extinction training (Otto et al., 2016). In conjunction with observed effects of DCS on protein expression and synaptic activity in the amygdala from rodent studies, it has been suggested that this indicates DCS enhances the development of new safe memories that compete with feared memories associated with fear expression (Myers and Davis, 2007; Singewald et al., 2015). Based on the parallels between extinction training and exposure therapy, it was hypothesized that DCS could be utilized as a novel adjunctive treatment to enhance learning in exposure-based psychotherapy (Myers and Davis, 2007; Singewald et al., 2015). A number of RCTs to date investigating the use of DCS as an adjunct to exposure therapy in clini cal anxiety populations have demonstrated promising initial findings (reviewed in Guastella and Alvares, 2012). Of note, the use of DCS has been examined in SAD, specific phobias, PTSD, panic disorder, and obsessive- compulsive disorder (OCD). For example, individuals with panic disorder exhibit mean reductions in symptoms following DCS-augmented CBT (Otto et al., 2016). A meta-analysis by Norberg et al. (2008) found a moderate to large effect size favoring use of DCS over placebo when added to extinction or exposure therapy across both animal and clinical human studies. Examining the studies separately, the effect for animal studies was larger, more significant, and more robust. The clinical human studies exhibited a moderate yet significant effect size. The most consistent positive results for DCS-facilitated exposure therapy have been observed in RCTs for SAD and specific phobia (reviewed in Guastella and Alvares, 2012). The first adjunctive DCS study with exposure-based treatment, conducted by Ressler and colleagues (2004), demonstrated that DCS facilitated reductions in subjective fear after virtual reality treatment for fear of heights. This immediate effect generalized to improved outcomes at one-week and three- month follow-up assessments, with greater numbers of self- exposures to real-world heights among those receiving DCS,
• A 534 nxiety isorders Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University PressD USA - OSO, 2018. 15:10:22.
indicative of greater clinical efficacy outside of a therapeutic context. Three RCTs for SAD have demonstrated similar results. In the first, Hofmann and colleagues (2006) demonstrated that DCS administered prior to four exposure sessions significantly reduced self-reported social anxiety symptoms compared with placebo, with the greatest difference observed at a one-month follow-up assessment. We replicated these findings (Guastella et al., 2008) in 56 social anxiety patients who received either DCS or placebo prior to four exposure- based therapy sessions. DCS-administered patients reported fewer social fear and avoidance symptoms, fewer dysfunctional cognitions, and greater overall improved functioning in everyday life posttreatment. Moderate effect sizes were found on most measures, and near-significant effects suggested that fewer DCS-treated patients may have dropped out of treatment in comparison with placebo. Further, treatment effects emerged early, with differences between drug groups emerging at the third exposure session. These studies demonstrated a positive relationship between DCS enhancement of therapy outcomes and the amount of learning achieved between exposure therapy sessions. Notably, indirect evidence suggests that the greater the amount of learning achieved within exposure therapy sessions, the greater the effectiveness of DCS in combination with exposure therapy (Guastella and Alvares, 2012). These effects were partially replicated and extended by a more recent study by Hofmann and colleagues (2013). Currently the largest trial of DCS to be conducted to date, the authors gave 144 participants 50mg of DCS or placebo one hour before five group-based exposure therapy sessions. In this study, the treatment was provided within the context of a larger 12-week CBT treatment program. Up to the sixth session of treatment, results showed that DCS augmentation was associated with an accelerated reduction in anxiety symptoms. By the end of the 12-week program, however, results suggested similar response rates between placebo and DCS- administered participants. Despite the success from social anxiety and specific phobia clinical trials, mixed results have been reported for OCD and panic disorder, with several studies reporting beneficial effects of DCS only in more symptomatic patients or at midtreatment, but not posttreatment or follow-up (Guastella and
Alvares, 2012). Similar studies that administered DCS adjunctively to an exposure-based protocol for OCD found that while some moderate gains emerged midtreatment, these disappeared by the end of the ten sessions (Otto et al., 2016). This suggests that DCS may be useful in speeding up or enhancing the effectiveness of the initial phase of exposure-based treatment (Guastella and Alvares, 2012), and is in agreement with mixed findings from panic disorder clinical trials. It further indicates that DCS may be sensitive to the number of administrations and insufficient within-session fear inhibition (Otto et al., 2016). Indeed, multiple DCS administrations prior to extinction training appears to reduce potential efficacy (Otto et a., 2016), implying a potential tolerance of NMDA receptors associated with chronic administration. Such a toler ability effect may, in part, explain some of the inconclusive findings from OCD clinical trials. It may also be that, for some patients, ceiling effects emerge in terms of treatment efficacy. For example, in a recent study examining the combination of DCS with exposure-based therapy in PTSD patients (de Kleine et al., 2012), no significant effect of DCS was found on symptom reduction across the total sample. However, subgroup analyses suggested beneficial effects of DCS for regular, as opposed to early, completers of exposure-based therapy. As suggested by the authors, this may imply that only more severe patients are likely to benefit from DCS augmentation, while others recover relatively quickly from exposure-based therapy alone. DIRECTIONS FOR FUTURE RESEARCH Although RCTs of DCS in anxiety disorders have shown promising findings, conclusions about the outcomes of DCS- facilitated exposure therapy from these studies are limited by a number of factors such as study design heterogeneity, dosage, timing of administration, and number of adjunctive therapy sessions (Guastella and Alvares, 2012; Otto et al., 2016). These factors have been summarized in Table 40.1. Given that the drug absorbs relatively slowly and takes approximately two to four hours to reach peak plasma levels,
Table 4 0.1 ADMINISTRATION AND DOSAGE FACTORS THAT MAY INFLUENCE THE EFFECTS OF DCS ADMINISTRATION ON LEARNING IN EXPOSURE THERAPY FACTOR
RELATIONSHIP WITH EFFECTS OF DCS
Time of administration relative to therapy
Has been used successfully with administration both before and after exposure therapy. Greater time interval between administration and therapy appears to reduce efficacy, although window yet to be clearly defined (Ganasen et., al 2010; Myers and Davis, 2007; Norberg et al., 2008).
Chronic versus isolated administration
Evidence indicates that repeated chronic administration reduces or eliminates beneficial effects of DCS on extinction learning (Boje et al., 1993; Quartermain et al., 1994). Optimal number of doses and interval between doses yet to be established.
Dose
Unclear, yet to be systematically investigated (Guastella and Alvares, 2012; Hofmann, 2007; Norberg et al., 2008).
Previous use of other medications
Rodent studies suggest that previous use of antidepressants may reduce efficacy of DCS (Hoffmann, 2007; Norberg et al., 2008).
4 0. C urrent T reatments nxiety Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press USAfor - OSO,A 2018. 15:10:22.
it has been suggested that null effects in some studies could reflect administration too soon before therapy to facilitate learning (Otto et al., 2016). Studies are therefore needed that directly compare the effectiveness of DCS administered at different times relative to exposure, and administration before versus after therapy. Rodent studies indicate significant effects of DCS even when administered a relatively long time after extinction training. One advantage of administration after therapy is that DCS could be given only in sessions where within-session extinction has actually occurred, and thus where there is learning to consolidate, in order to minimize the risk of tolerance effects following chronic administration (Norberg et al., 2008). Administration only after successful exposure therapy sessions may therefore further enhance potential efficacy and treatment acceptability in the clinic. An additional factor is that of dose; systematic dose response studies with DCS are needed to determine the optimal dose for each administration. Most previous human studies have used 50 mg, and few have directly compared the effects of administering doses of varying levels (Guastella and Alvares, 2012; Norberg et al., 2008). It has also been suggested that prior exposure to antidepressants may limit DCS efficacy on NMDA receptor functioning. For example, rodents previously administered with the antidepressant imipramine exhibit reduced DCS facilitation of extinction training (Norberg et al., 2008). Further research is needed to investigate whether this also occurs with other drugs commonly coadministered in clinical practice, such as benzodiazepines or SSRIs, and to investigate whether these effects are short-or long-term in nature (Otto et al., 2016). Further, it appears that DCS is best used in isolated doses; both preclinical rodent and clinical human studies indicate that any beneficial effects become less pronounced or disappear across repeated or chronic administration (Myers and Davis, 2007). This may reflect tolerance effects or a modification of the structure and function of the NMDA receptor complex through repeated activation (Myers and Davis, 2007). Although available evidence indicates that acute administration is most effective, and efficacy declines with repeated administration, the optimal number of doses and interval between repeated administrations of DCS still needs to be defined (Otto et al., 2016). N O V E LT Y A N D C L I N I C A L P OT E N T I A L
Bearing in mind a number of factors that may limit initial conclusions about its efficacy in clinical practice, the findings of these RCTs provide the strongest evidence to suggest that DCS enhances exposure-based therapy for disorders that respond strongly to CBT, such as specific phobias and SAD. Novel augmentative approaches to anxiety treatment have a number of clinical benefits over traditional approaches. Speeding treatment response allows for efficient treatment delivery, benefiting both the patient and therapist. Augmentation of exposure therapy with DCS may also enhance the therapeutic response in nonresponders, especially for those who demonstrate insufficient learning of the required safety associations
for successful fear extinction (Norberg et al., 2008). This may result in more cost-effective outcomes and decrease attrition rates across services. An additional perspective comes from stepped-care models, in which treatments that are less intensive in terms of cost or therapist time are used as first-line treatments and more intensive treatments are reserved for either nonresponders to first- line treatment or patients initially identified as potential nonresponders. Such a model offers the potential to tailor treatment level to patient characteristics and severity in order to reduce costs and enhance efficacy. Considered within this framework, DCS could be utilized as a second-line treatment for individuals who do not initially respond to exposure-based protocols. The real potential for DCS is that, for a limited cost, it may substantially improve a simple evidence-based treatment, thus making an already relatively effective intervention more accessible and efficient. N O VE L C O G N I T I VE A PP R OAC H E S Cognitive models of anxiety emphasize that biased or irratio nal cognitive processes (thoughts, attitudes, beliefs, and infor mation processes) and consequent maladaptive emotions and behaviors are crucial etiological and maintenance factors in anxiety (Clark and Beck, 2010). Many contemporary learning theories go beyond purely behavioral accounts to acknowledge additional cognitive factors in anxiety, such as social and observational learning, CS–US contingencies and expectancies, and perceived control and predictability (Barlow, 2002). However, cognitive models differ in that cognitive processes are seen as a cause rather than merely a consequence of pathological anxiety (Clark and Beck, 2010). As reviewed by Clark and Beck (2010), the strength of cognitive models are bolstered by neurobiological evidence concerning the extensive connections between the amygdala and the hippocampal and higher order cortical structures (prefrontal, anterior cingulate, and orbital cortical regions) involved in conscious cognitive processes, as well as the role of these structures in moderating fear responses and contextual fear conditioning. Cognitive processes have formed a key target in the treatment of anxiety for quite some time, particularly in the form of CBT, which, as mentioned earlier, is currently the “gold standard” in terms of psychological treatments for anxiety. As reviewed by Porto et al. (2009), neuroimaging studies suggest that treatment with CBT is associated with changes in the activity of neural areas identified as playing a critical role in the fear response (including the insula, anterior cingulate cortex, prefrontal cortex, amygdala, and hippocampus). More recently, the cognitive anxiety literature has focused on the potential role of biases in information processes (including attention, interpretation, memory, imagery, and appraisal) in the etiology and maintenance of anxiety (see recent reviews in Beard, 2011; Macleod and Mathews, 2012). Attentional and interpretive biases toward threatening information among clinically anxious individuals are well supported by empirical evidence. A substantial body of evidence (see Bar-Haim et al., 2007; Ouimet et al., 2009) indicates that, relative to healthy controls, clinically anxious populations tend to preferentially
• A 536 nxiety isorders Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University PressD USA - OSO, 2018. 15:10:22.
attend to threatening (as opposed to nonthreatening) stimuli (i.e., display an attentional bias) and to interpret ambiguous information as threatening rather than positive (i.e., display an interpretive bias). For instance, a socially anxious individual might be more likely to attend to others’ negative facial expressions and also more likely to interpret ambiguous body language in a negative manner (e.g., as a sign of distaste for themselves rather than unrelated situational factors). Based on the hypothesis that these biases may play a role in the etiology and/or maintenance of the anxiety disorders, they have been proposed as a potential target mechanism for novel anxiety treatment approaches (Beard, 2011). As the majority of research thus far has focused on the modification of attentional and interpretive biases, these will form the focus of the present section. According to biased competition models, attention is mediated by both automatic deployment through a “bottom-up,” amygdala-based threat evaluation system that directs attention toward salient stimuli, and a more flexible “top-down,” prefrontal cortical attentional control signal that is evoked when there are conflicting demands placed on attention (see in Bishop, 2007; Browning et al., 2010a). These signals direct processing resources in the sensory and association cortices toward the preferred stimulus. It has been argued that the biased competition model used to account for attentional processes can also be applied to the interpretation of ambiguous stimuli, such that competition between alternate interpretations is resolved through the interaction of an amygdala-based threat evaluation system and a top-down prefrontal control system (Bishop, 2007). It appears that both automatic and controlled cognitive processes are involved in attention and interpretation (Bar- Haim et al., 2007; Macleod and Mathews, 2012; Ouimet et al., 2009). In a meta-analytic study, Bar-Haim et al. (2007) found that attentional bias toward threat is robust across anxiety disorders for both consciously perceived stimuli and stimuli presented outside of awareness. Attention consists of three primary stages: orientation and engagement, disengagement, and avoidance (Ouimet et al., 2009), with biases toward threat observed among clinically anxious individuals at all three stages. That is, during earlier stages of processing anxious individuals are likely to preferentially allocate attention to threat (facilitated attention). Once engaged they are also likely to experience trouble disengaging from threatening stimuli to focus on other stimuli (difficulty disengaging). Finally, at later, more strategic stages of processing they may be seen to divert attention away from threatening stimuli (attentional avoidance), which is hypothesized to maintain anxiety by preventing elaborative processing that reduces the threatening value of the stimulus (Bar-Haim et al., 2007). Indeed, evidence to date suggests a bidirectional and maintaining relationship between anxiety and attentional biases (Van Bockstaele et al., 2014). As Bishop (2007) notes, the literature concerning the neurocircuitry of attentional and interpretive processes in anxiety is less developed than that of fear conditioning and extinction learning. However, neurobiological evidence from
animal models and neuroimaging studies in humans implicate perturbations in both the amygdala-based and prefrontal fear systems when explaining biased information processing (see reviews in Bishop, 2007). More specifically, pathological anxiety is hypothesized to involve both hyperactivation of the amygdala-based threat evaluation system and insufficient downregulation of the fear response by prefrontal control mechanisms. This neurobiological perturbation results in heightened activation of threat-related representations and failure to activate nonthreatening representations, and has been used to account for both interpretive and attentional biases in the literature (Bishop, 2007; Cisler and Koster, 2010). Cisler and Koster (2010) have proposed that hyperactivity of the amygdala-based system is likely to account for automatic vigilance and facilitated attention to threat, while failure of the higher order prefrontal system to downregulate amygdala activity and direct attention to task-relevant stimuli may explain difficulty disengaging from threat. The attentional avoidance component of attentional biases also appears to reflect activity in the prefrontal region, through its role in strategic emotion regulation. Similarly, in their cognitive- neurobiological information processing model, Otto et al. (2016) also emphasize the role of subcortical networks in hypervigilance and facilitated attention to threat and prefrontal cortical structures in higher order regulation of anxiety responses. C O G N IT I VE B I A S MO D I FI C AT I O N (C B M )
Recognition of the association between information processing biases and pathological anxiety led to the development of CBM treatments for anxiety disorders. These treatments aim to modify these biases to subsequently alleviate anxiety symptoms. AT T E N T I O N B I A S MO D I FI C AT I O N (C B M-A )
Attention bias modification focuses specifically on retraining attentional biases toward threat. Typically, this is done using a “dot-probe task” (depicted in Figure 40.1), where participants are asked to discriminate between two variants of a probe (e.g., “.” and “.”) and respond by pressing the corresponding one of two keyboard keys. These probes are presented behind two stimuli (e.g., words or pictures), one threatening and one neutral. In the original task, developed to assess attentional biases, the target probe is presented behind the threatening stimulus 50% of the time. A threat bias is indicated when participants are faster to identify probes presented behind a threatening stimulus relative to those presented behind a neutral stimulus. An extension of the dot-probe task manipulates or retrains this attentional bias toward threat. In the modified paradigm, the target probe is presented consistently behind either the threatening (attend-threat training) or neutral (avoid-threat training) stimulus. Since attending to the relevant stimulus results in the correct identification of the target probe, repeated trials should implicitly train the individual to preferentially allocate attention either toward or away from threat, depending on the training contingency.
4 0. C urrent T reatments nxiety Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press USAfor - OSO, A 2018. 15:10:22.
E M P I R I C A L EVI D E N C E SUN
.
+
+
HATE
..
Phase 1
Phase 2
Phase 3
Phase 1
Fixation cross
Stimuli
Probe
Fixation cross
Trial 1
Trial 1
Trial 1
Trial 2
A typical protocol for attentional bias assessment or training using the dot-probe paradigm. A typical dot-probe attention bias task, where the target probe is the single dot (denoted in gray). The participant is instructed to fixate on the cross, then press the keyboard key that corresponds to the location of the target probe, and finally refixate on the cross for the start of the next trial. Between the presentation of the cross and the probe, two emotionally valenced stimuli are presented in the locations where the probes will appear. In attentional bias assessment (or control training with no contingency), the target probe appears behind the threatening and neutral stimuli with equal probability (i.e., 50% of the time for each). In avoid-threat attentional bias training, the target probe is always presented behind the nonthreatening stimulus. In attend-threat training, the target probe is always presented behind the threatening stimulus. Figure 40.1
I N T E R P R ET I VE B I A S M O D I F I C AT I O N (C B M-I )
Interpretive biases can be assessed in two broad ways (Macleod and Mathews, 2012). Online measures assess interpretations at the time of encountering ambiguous information, usually by assessing latency to read targets that either confirm or disconfirm possible threatening interpretations of ambiguous primes. Targets that confirm the participant’s interpretation of the ambiguous prime are read or identified more quickly than those that disconfirm their interpretation. Offline measures assess interpretations either before or after encountering ambiguous information, usually through self-report. Studies using offline measures have consistently shown a negative interpretive bias in clinically anxious populations, while those using online measures have found mixed results but generally support either the presence of a negative interpretive bias or the absence of the emotionally positive bias often present in nonanxious controls (Macleod and Mathews, 2012). A common means of CBM-I involves the presentation of a series of ambiguous homographs or situations, followed by a word fragment target that must be completed after reading the stimulus (Beard, 2011; Macleod and Mathews, 2012). The emotional valence of the ambiguous stimulus can only be interpreted by using the subsequent target. The individual can be compelled to interpret these ambiguous stimuli in either a negative or positive manner through the consistent presentation of word fragment targets that relate to either the negative or positive interpretation. Thus, over repeated trials, the participant develops a positive or negative interpretive bias.
Many CBM studies have been conducted under a diathesis– stress model of anxiety, which suggests that CBM may reduce what is known as stress reactivity or vulnerability (i.e., the level of anxiety in response to a stressor) but not necessarily anxiety symptoms per se. Hence, the beneficial effects of CBM on anxiety should only be apparent once patients are exposed to a stressor (Hallion and Ruscio, 2011). Empirical studies have therefore investigated the impact of CBM on anxiety symptoms either immediately posttraining or in reaction to a stressor (laboratory-induced or naturalistic). A number of recent reviews and meta-analyses have been conducted to consolidate findings from previous CBM-A studies (Hakamata et al., 2010; Linetzky et al., 2015; Mogoaşe et al., 2014) and CBM studies more generally (Beard, 2011; Cristea et al., 2015; Macleod and Mathews, 2012). C B M-A
The majority of CBM-A studies conducted thus far have employed a modified dot- probe paradigm (Macleod and Mathews, 2012). Studies in nonclinical populations compare avoid-threat training to either an attend-threat or a no-training placebo control (no-training contingency) condition. While these studies have consistently demonstrated that it is possible to induce an attentional bias toward or away from threat, the impact of CBM-A on anxiety scores posttraining and in response to a stressor have been mixed (Beard, 2011). More specifically, there is stronger evidence in support of reduced stress reactivity (i.e., anxiety in response to a stressor) following avoid-threat training than there is for reductions in posttraining state and trait anxiety. In clinical populations, CBM-A studies have predominantly been conducted in SAD and generalized anxiety disorder (GAD) patients, typically allocated to either avoid-threat or a no-training placebo control (Linetzky et al., 2015). These studies have consistently demonstrated that CBM-A can be used to retrain attentional biases away from threat toward neutral information. Furthermore, significant reductions in both anxiety symptoms and stress reactivity have been found for those participants allocated to avoid-threat training. These outcomes have been found following both single-and multisession attention training, and have been shown to persist over time to follow-up assessment up to four months later (Macleod and Mathews, 2012). Hakamata et al. (2010) conducted a meta-analysis of 12 CBM-A studies employing the dot-probe paradigm (among nonclinical populations, GAD, and SAD patients), including only studies where the control group was a no-training placebo rather than attend-threat training. This analysis demonstrated a large and significant effect size of avoid-threat training on attention bias. It also found a medium and significant effect on anxiety symptoms (relative to control training placebo). It is important to note, however, that the effect on anxiety symptoms included both posttraining measures of anxiety symptoms and measures of anxiety symptoms following exposure to a stressor (i.e., stress reactivity). Effect sizes for the impact of CBM-A on anxiety symptoms did not differ significantly
• A 538 nxiety isorders Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University PressD USA - OSO, 2018. 15:10:22.
between patients and nonclinical samples. Interestingly, the effect of CBM-A on magnitude of attention bias change (but not on magnitude of anxiety symptom change) was significantly moderated by the number of sessions involved. For attention bias change, a greater number of sessions was associated with a greater amount of change. These positive outcomes are supported by two recent meta- analyses (Heeren et al., 2015; Linetzky et al., 2015). Based on 11 dot-probe-based CBM-A studies including only clinically diagnosed anxious patients (SAD, GAD, PTSD, mixed pediatric anxiety disorders), Linetzky and colleagues (2015) reported significant and greater reductions in attentional bias in CBM-A compared to control training. Importantly, the analysis yielded a significant medium between-groups effect on clinician-rated anxiety, reflective of greater reductions in anxiety at posttest following CBM-A compared to control training, and reported that gains can be maintained to several months posttest. Additionally, a meta-analysis of 15 studies specific to CBM-A for social anxiety yielded small but significant effect sizes for reductions in social anxiety symptoms, stress reactivity to a social threat task, and attentional bias at posttest (Heeren et al., 2015). However, the findings of these meta-analyses are tentative given the small number of studies concerned. It is also noteworthy that findings are inconsistent across studies, and gains are not always maintained over the long term. Some studies have found CBM-A to be no more beneficial than control training (e.g., Carleton et al., 2015), to demonstrate significant effects only on select outcomes (e.g., clinican rated but not self-report measures of anxiety; Linetzy et al., 2015), or to yield benefits at posttest but not follow-up (e.g., Heeren et al., 2015). C B M-I
As reviewed in Beard (2011) and Macleod and Mathews (2012), single-and multiple-session versions of CBM-I have been used in nonclinical populations to successfully induce positive and negative interpretive biases. In these studies, interpret-positive and interpret-negative training have been compared with each other or to a no-training placebo control. Although a few studies have reported null findings, others have found significant reductions in outcome measures (state and trait anxiety and/or stress reactivity) for those allocated to the interpret- positive condition. Studies in GAD patients and populations with high trait or state anxiety (including worry, social anxiety, spider fear, and trait anxiety) have compared the impact of single-or multiple-session interpret-positive training versus a no-training placebo control on stress reactivity and anxiety symptoms. In both clinical and nonclinical populations, interpretive bias modification from single-session training has been shown to persist over time up to 24 hours later (Macleod and Mathews, 2012). In terms of clinical outcomes, several studies have found that interpret-positive training induces a positive interpretive bias and reduces state and trait anxiety, anxiety symptoms, and/or stress reactivity. However, results have been mixed depending on the specific anxiety disorder and outcome measure concerned. First, CBM-I has not yet been shown to
significantly reduce spider fear (Macleod and Mathews, 2012). Further, its effect on posttraining anxiety versus stress reactivity is still unclear. Some studies have shown significant reductions in state and trait anxiety from CBM-I but no effect on specific anxiety symptoms (e.g., social anxiety scales) or stress reactivity, while others have found the opposite (Beard, 2011). Hallion and Ruscio (2011) conducted a meta-analysis to examine the effect of CBM (both CBM-I and CBM-A) on cognitive biases and anxiety symptoms posttraining and poststressor across both anxiety and depression. Their review included both clinical and nonclinical populations and, unlike Hakamata et al., did not exclude CBM-A studies using an alternative to the dot-probe paradigm or those comparing avoid-threat training to attend-threat training rather than a no-training placebo. Across anxiety and depression, this comprehensive review found a significantly larger effect of CBM on interpretive biases (medium effect size) than on attention biases (small effect size). After correcting for publication bias, the effect of CBM on anxiety and depression symptoms was significant following exposure to a stressor (with a small effect size), but not immediately posttraining. This echoes the mixed findings of narrative reviews outlined previously in relation to the effect of CBM on posttraining anxiety versus stress reactivity, although again it is important to bear in mind the inclusion of studies concerning both anxious and depressive symptoms. When anxiety studies were examined separately, there was a small but significant effect of CBM on symptoms both posttraining and after exposure to a stressor. However, a recent meta-analysis (Cristea et al., 2015) suggested that CBM may have limited clinical utility. The analysis examined the effect of CBM interventions (CBM-A and CBM-I) in anxiety and depression, and reported small effect sizes across outcome categories for clinical samples with anxiety disorders. However, considerable heterogeneity was found among studies, and removal of outliers considerably reduced effect sizes. The authors argue that studies investigating CBM are substandard and that high risk of bias across studies may artificially inflate effect sizes. Cristea et al. (2015) contend that considerable methodologically superior evidence is required to support the clinical application of CBM. H Y P OT H E S I Z E D M E C H A N I S M O F AC T I O N A key assumption of CBM and associated models of anxiety is that information processing biases are a causal factor in the etiology and maintenance of anxiety disorders rather than merely a consequence of anxiety (Hallion and Ruscio, 2011). That is, CBM assumes that information processing biases precipitate negative thoughts and subsequent maladaptive behavioral and emotional patterns. This assumption about the causal role of information processing biases in anxiety disorders requires further empirical validation. Prospective studies have provided preliminary support, demonstrating that information processing biases are capable of predicting the presence and severity of anxiety disorders as well as stress reactivity (as reviewed in Beard, 2011; Mathews and MacLeod, 2005).
4 0. C urrent T reatments nxiety Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press USAfor - OSO,A 2018. 15:10:22.
These associations could, however, be a product of a third stable personality variable that predicts both cognitive biases and anxiety outcome measures (MacLeod and Mathews, 2012). Further support comes from the results of intervention studies outlined earlier, which have shown that CBM can be used both to modify cognitive biases (toward and away from threat) and accordingly increase or reduce anxiety levels. Further, in their CBM-A review Hakamata et al. (2010) reported a strong correlation between the degree of attention bias change and the degree of change in anxiety scores that approached significance. In their meta-analysis of CBM for anxiety and depression, Hallion and Ruscio (2011) found that change in cognitive biases did not significantly moderate the effect of CBM on symptoms, although the effect did approach significance. They note that this finding should be interpreted cautiously given the diverse array of trials included in their analysis, and indeed a substantial number of individual trials have demonstrated that change in cognitive biases mediated change in anxiety symptoms (Beard, 2011). In addition, the meta-analysis of CBM for anxiety and depression by Cristea et al. (2015) found some evidence that changes in cognitive bias mediated the associated between CBM training and emotional outcomes. However, these findings must be considered preliminary as only 11 out 49 studies conducted formal mediation analyses. Together, existing evidence provides partial support for a causal role of biased information processing in anxiety and a mediational role of cognitive bias change in clinical outcomes of CBM interventions. Preliminary research has been conducted to explore the neurobiological mechanisms underlying change following CBM-A. It has been suggested that CBM-A may serve to modify attentional control processes, as opposed to the more “bottom-up” threat evaluation processes (Beard, 2011). As reviewed in Beard (2011), anxious individuals with strong attentional control may not show an attentional bias, which suggests that attentional control could moderate the relationship between attention bias and anxiety. Further, neurobiological evidence suggests that CBM-A may serve to modify attention through effects on prefrontal attentional control processes (Browning et al., 2010a). A first CBM-A neuroimaging study (Browning et al., 2010b) among healthy individuals found significant differences in the activity of prefrontal cortical, but not amygdala-based, structures between those who had completed attend-threat versus avoid-threat training in a subsequent task. Further, Koster et al. (2010) found that avoid-threat CBM-A influenced late but not early stages of threat processing, hypothesizing that the procedure influences later stage attentional avoidance rather than earlier hypervigilance and facilitated attention processes. Little is known at present about the specific mechanism of action by which CBM-I modifies interpretive processes. Some research has been conducted to explore whether artifacts are responsible for the changes in interpretive bias that occur. Evidence suggests that they do not simply reflect a response bias or demand effects induced by repeated trials, they are not fully accounted for by semantic priming effects alone, nor are they entirely dependent on changes in mood and state anxiety that may occur as a result of exposure to emotionally salient
stimuli during training (Beard, 2011; Macleod and Mathews, 2012). It appears that active generation of interpretations rather than mere passive processing is necessary for CBM-I to have a significant impact on anxiety levels (Beard, 2011). Macleod and Mathews (2012) have suggested that this highlights a potential mechanism of action for CBM-I, specifically the acquisition of a particular processing style for emotionally salient information. That is, through interpretive training the individual may learn a new style of seeking and selecting specific types of emotional meanings, which is then unintentionally elicited and implemented when encountering subsequent ambiguous events in real life. N O VE LT Y A N D C L I N I C A L P OT E N T I A L The critical finding from CBM trials has been evidence that these procedures have potential to produce treatment effect sizes comparable to traditional psychological and pharmacological interventions for anxiety disorders, while requiring relatively minimal time and clinician input. Furthermore, its convenience, accessibility, and low operating costs may be particularly beneficial in terms of facilitating ongoing practice and engagement in treatment and so potentially reduce the risk of attrition and relapse and promote maintenance of treatment gains. However, inconsistency across studies and meta-analyses indicate the need for caution in application of CBM (Cristea et al., 2015). Indeed there is not yet sufficient evidence to suggest that CBM can be used as a stand-alone treatment for anxiety disorders, and the relatively small effect sizes of some meta-analyses compared to CBT suggest that CBM requires refinement prior to dissemination (Heeren et al., 2015; Macleod and Mathews, 2012). Nonetheless, the outcomes from CBM trials imply that it may be useful as an adjunct to CBT, with the potential to be used as a preparatory step to exposure-based CBT in more severe patients, to reduce anxiety to a point where they can participate in behavioral experiments (Macleod & Mathews, 2012). Preliminary investigations of this possibility in social anxiety have been mixed, with one study finding that CBM-A demonstrated no additive benefit as an augmentation to traditional group CBT for SAD (Rapee et al., 2013), and another demonstrating that CBM-I enhanced the efficacy of computerized CBT for nonclinical social anxiety on interpretation biases and social anxiety symptoms (Butler et al., 2015). CBM- A may also be a useful adjunctive treatment to psychotropic medications for anxiety (Browning et al., 2010a), or integrated into stepped-care models as a preliminary step for patients who are seen to require less intensive intervention. In the future, computerized bias modification therapy could be made accessible on a range of technological platforms such as personal computers and mobile phones, and even over the Internet, for patients who are unable or unwilling to attend in-person therapy sessions. In this way, it offers the potential to address many practical barriers to participation in therapy. An initial study of Internet-delivered CBM- A (Carlbring et al., 2012) found it had no significant effect
• A 540 nxiety isorders Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University PressD USA - OSO, 2018. 15:10:22.
on social anxiety symptoms and general anxiety levels among individuals with social anxiety disorder. However, studies of Internet-delivered CBM-I have been more promising, with an RCT for mixed anxiety disorders demonstrating significant benefits on interpretations but not emotions compared to controls (Salemink et al., 2014), and a pilot study for SAD yielded significant within- subjects reductions in interpretive biases and symptomatology (Brettschneider et al., 2015). Thus, further investigation into the impact of delivery mode on treatment outcome for CBM is needed before implementation of Internet-based CBM treatment programs. DIRECTIONS FOR FUTURE RESEARCH Many potential avenues for improving both efficacy and utility of CBM remain. Further exploration into the role of other information processing biases aside from interpretation and attention (such as memory, imagery, and appraisal) in anxiety, and the development of relevant bias modification therapies, should be undertaken (Macleod and Mathews, 2012). It may well be that the type of CBM offered to patients could be customized to their particular information processing biases. It has also been proposed that the impact of CBM could be boosted by using training packages targeted at modifying multiple cognitive biases (Hallion and Ruscio, 2011). Although recent pilot studies found that a combined interpretive and attentional CBM training package significantly improved anxiety symptoms among patients with SAD (Beard, 2011), it remains to be seen whether this combination approach results in significantly greater symptom reduction than programs targeting one type of cognitive bias. Further research is also needed to ensure gains resulting from CBM are maintained over time, to compare CBM with established anxiety treatments (e.g., CBT), and to assess the efficacy of CBM as an adjunct to CBT for anxiety disorders (MacLeod and Matthews, 2012). Future studies should also focus on using cognitive theory and knowledge of the cognitive mechanisms underpinning anxiety to enhance the efficacy of CBM. At present, technology is being used to enhance CBM through the development of programs delivered through the Internet or smartphones, meaning that patients can be exposed to treatment over extended periods of time and across multiple settings (Macleod and Mathews, 2012; Salemink et al., 2014). Methods of enhancing the ecological validity of CBM procedures also warrant investigation. The possibility of using novel pharmacological compounds, such as DCS, to enhance the potency of bias modification interventions may also be investigated. Another possible means of enhancing efficacy involves the modification of specific components of CBM. This could include the tailoring of stimuli to the specific informational domains related to each anxiety disorder (such as faces or other socially relevant stimuli in CBM-A for social anxiety; see Hakamata et al., 2010), based on findings that patients’ information processing biases are most evident when assessed on stimuli related to their particular disorder.
Finally, in CBM, participants are generally not explicitly informed of the training contingency but instead implicitly learn it through the completion of repeated trials. Hence, although some CBT packages also include attentional training or interpretive restructuring exercises, a crucial distinction between CBM and these CBT exercises are that CBM aims to implicitly retrain information processing biases rather than to consciously challenge and modify thoughts and behaviors (Beard, 2011). An area for further investigation is the impact of adding explicit instructions to CBM training, which may either facilitate or impair learning of the training contingency. As outlined in Macleod and Mathews (2012), only two CBM-A studies to date have compared explicit and implicit instruction conditions, reporting contradictory findings such that explicit instruction either enhanced or eliminated the therapeutic effects of CBM-A on anxiety. Therefore, the grounding of CBM in cognitive theory means that it has immense potential to be developed and enhanced as a treatment for anxiety. The strength of this approach will be further bolstered by integration with neuroimaging techniques and circuitry models of both cognitive processes and the etiology and maintenance of anxiety disorders. As the neurocircuitry of these cognitive processes (attention and interpretation) and the ways in which they are altered among individuals suffering from pathological levels of anxiety are better understood, CBM interventions can be developed that specifically aim to rectify these perturbations (such as enhancing prefrontal control of attention). C O S T E F F E C T I VE N E S S A N D AC C E P TA B I L I T Y O F N O VE L I N T E RVE N T I O N S Following on from further empirical and theoretical validation, effectiveness trials will now need to be undertaken with these novel treatment approaches in order to investigate their potential translation into clinical practice. Compared with patients enrolled in many RCTs, patient populations are less homogenous and exhibit significant comorbidity with other psychiatric disorders, which may play a role in treatment nonresponse. Outside the laboratory, it may also be difficult to regulate specific aspects of treatment regimes, such as timing of administration and the nature of exposure therapy in the case of DCS (Guastella and Alvares, 2012). Similarly, cost effectiveness and acceptability to key stakeholders are important factors to consider when evaluating new treatment approaches and are reviewed in the next section. DCS
As larger scale RCTs of DCS are only now beginning to emerge, there is limited evidence surrounding its acceptability and cost effectiveness. If, as empirical results suggest, DCS can be used to enhance clinical efficacy and/or the speed and efficiency of treatment, it may improve patient satisfaction and
4 0. C urrent T reatments nxiety Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press USAfor - OSO,A 2018. 15:10:22.
treatment outcomes and reduce attrition to enhance both the cost effectiveness and acceptability of exposure-based therapy (Norberg et al., 2008). No studies have examined the cost effectiveness of DCS-augmented CBT or compared it with nonaugmented CBT. In relation to acceptability, it appears that DCS is well tolerated with minimal side effects. CBM
Although the cost effectiveness of CBM has not yet been studied specifically, it has the potential to be an effective treatment for anxiety that requires minimal therapist input and time and has relatively low operating costs. In a review of CBM (Beard, 2011), the authors note that the relatively low attrition rates in previous studies (0%–8%) may not be an indication of the acceptability of CBM in the “real world” due to the incentive of participant reimbursement. In their own pilot study assessing multisession CBM (combined CBM-A and CBM-I) in real treatment settings without remuneration, Beard (2011) reported a substantially greater attrition rate (33%), although those patients who completed the program reported high levels of satisfaction on a standardized questionnaire. Qualitative results of CBM studies indicate that treatment credibility is an issue (see review in Beard, 2011); as CBM involves implicit retraining using repeated practice on a cognitive task, it may be viewed by some patients as monotonous, obscure, or pointless. These concerns are particularly relevant to CBM- A, which appears to have lower perceived face validity than CBM-I (Beard, 2011). Unfortunately, negative attitudes are likely to influence not only the likelihood of uptake but also the success of treatment, given that perceived treatment credibility and treatment preferences are known to play a key role in adherence and treatment outcomes (Taylor et al., 2012). One important final consideration relates to the generalizability, longevity, and real-world applicability of laboratory treatment effects for CBM (MacLeod and Mathews,
2012). Consideration of context-specific learning effects has led to the development of home-based training programs to promote transfer of learning to naturalistic environments (Macleod and Mathews, 2012); however, some studies suggest that CBM training is less effective outside a clinic setting (Linetzky et al., 2015). However, more work needs to be done to assess the generalizability of treatment gains across a variety of stimuli, particularly given that many studies have assessed bias change using the same cognitive task on which participants were trained. Those studies that have included independent measures of cognitive biases to assess generalizability have reported mixed results (Beard, 2011). Future studies should also focus on incorporating longer term assessment of cognitive biases, and the development of bias modification programs designed to maximize the duration of bias change (e.g., using spaced learning and booster sessions) (Macleod and Mathews, 2012). C O N C LU S I O N As summarized in Table 40.2, the novel treatment approaches explored here differ greatly in terms of their nature and the specific mechanisms of anxiety they target. However, they share a common goal of harnessing knowledge of the cognitive, behavioral, and neurobiological mechanisms underlying anxiety to enhance treatment outcomes. Future research should continue to assess and further improve the clinical efficacy, cost effectiveness, and acceptability of these interventions. In particular, their efficacy across different anxiety disorders needs to be established to inform evidence-based treatment guidelines. As outlined in Table 40.3, most evidence for the efficacy of these interventions is either still forthcoming or has exhibited mixed results. Aside from further refining and extending these existing novel approaches, future research should continue within this
Table 4 0.2 PROPOSED THERAPEUTIC MECHANISM OF ACTION AND NEURAL TARGET SITE FOR EACH OF THE NOVEL PHARMACOLOGICAL, COGNITIVE, AND TECHNOLOGICAL INTERVENTIONS REVIEWED IN THIS CHAPTER PROPOSED TARGET SITE/ NEURAL MECHANISM OF ACTION
INTERVENTION
(POTENTIAL) THERAPEUTIC EFFECT
Cortisol
Impairs retrieval of fear memories, enhances consolidation of fear extinction training/exposure therapy (Wolf, 2008)
Acts on glucocorticoid receptors; impaired retrieval relates to medial temporal lobe activity (Wolf, 2008); fear extinction mediated by the basolateral amygdala (Myers and Davis, 2007)
Yohimbine
Enhances learning in fear extinction training/ exposure therapy (Holmes and Quirk, 2010)
α2-adrenoreceptor antagonist in the hippocampus, amygdala, and prefrontal cortex; increases extracellular norepinephrine (Holmes and Quirk, 2010)
DCS
Enhances learning in fear extinction training/ exposure therapy
Cofacilitates glutamatergic activation of NMDA receptors in the amygdala at glycine binding site (Myers and Davis, 2007)
CBM-A
Reduces threat-related attention bias
Not yet well established; may modify prefrontal activity (Beard, 2011)
CBM-I
Reduces threat-related interpretive bias
Not yet established
• A 542 nxiety isorders Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University PressD USA - OSO, 2018. 15:10:22.
Table 4 0.3 STATE OF CURRENT EVIDENCE FOR THE EFFECTIVENESS OF EACH NOVEL INTERVENTION IN THE REDUCTION OF ANXIETY SYMPTOMS ACROSS THE VARIOUS ANXIETY DISORDERS GAD
SAD
SPECIFIC PHOBIA
PTSD
OCD
PANIC DISORDER
Cortisol
—
✓
✓
✓
—
—
Yohimbine
—
—
?
—
—
—
DCS
—
✓
✓
?
?
?
CBM-A
✓
✓
?
?
—
?
CBM-I
✓
?
—
—
—
?
ICT
✓
✓
✓
✓
?
✓
✓ indicates that trials to date have supported effectiveness of this intervention; ? indicates insufficient or mixed evidence from trials to date; —indicates that this intervention has not been studied in relation to this disorder.
translational framework to capitalize on our growing understanding of the anxiety disorders, and extend our reach with further novel augmentative approaches. A particular emphasis should be placed on understanding the effects of interventions on underlying fear neurocircuitry, the ways in which this circuitry may differ among individuals with anxiety disorders, and which aspects may be modified to produce therapeutic outcomes. Furthermore, there is now a growing and substantial body of evidence concerning the role of genetic and environmental factors in the etiology and maintenance of anxiety (as reviewed in Hamilton and Fyer, 2009). As research in this area expands, a better understanding of the interactions between genetic and environmental risk factors in the neuroplasticity changes that underpin pathological anxiety will facilitate the delivery of preventative and early-stage interventions targeted toward at-risk groups. Such early-stage interventions are a critical step in improving the outcomes of anxiety treatment. For both existing and future treatment approaches, these interindividual genetic and neurobiological differences are likely to be a key predictor of treatment response, providing a potential means to target efficacious interventions to the right individuals. DISCLOSURES The chapter authors have no conflicts of interest to declare. REFERENCES Aerni, A., Traber, R., et al. (2004). Low-dose cortisol for symptoms of posttraumatic stress disorder. Am J Psychiatry 161(8):1488–1490. Alvarez, R.P., Biggs, A., et al. (2008). Contextual fear conditioning in humans: cortical-hippocampa and amygdala contributions. J Neurosci 28:6211–6219. Andreatta, M., Leombruni, E., et al. (2015). Generalization of contextual fear in humans. Behavior Therapy 46:583–596. Bandelow, B., Sher, L., et al. (2012). Guidelines for the pharmacological treatment of anxiety disorders, obsessive–compulsive disorder and posttraumatic stress disorder in primary care. Int J Psychiatry Clin Pract 16(2):77–84.
Bar-Haim, Y., Lamy, D., et al. (2007). Threat-related attentional bias in anxious and nonanxious individuals: a meta-analytic study. Psychol Bull 133(1):1–24. Barlow, D. (2002). Anxiety and its disorders: the nature and treatment of anxiety and panic. New York: Guildford Press. Beard, C. (2011). Cognitive bias modification for anxiety: current evidence and future directions. Exp Rev Neurother 11(2):299–311. Bishop, S.J. (2007). Neurocognitive mechanisms of anxiety: an integrative account. Trends Cogn Sci 11(7):307–316. Boje, K.M., Wong, G., et al. (1993). Desensitization of the NMDA receptors complex by glycinergic ligands in cerebellar granule cell cultures. Brain Res 603(2):207–214. Browning, M., Holmes, E., Harmer, C. (2010a). The modification of attentional bias to emotional information: a review of the techniques, mechanisms, and relevance to emotional disorders. Cogn Affect Behav Neurosci 10(1):8–20. Browning, M., Holmes, E.A., Murphy, S.E., (2010b). Lateral prefrontal cortex mediates the cognitive modification of attentional bias. Biol Psychiatry 67(10):919–925. Brettschneider, M., Neumann, P., et al. (2015). Internet-based interpretation bias modification for social anxiety: A pilot study. J Behav Ther Exp Psychiatry 49:21–29. Butler, E., Mobini, S., et al. (2015). Enhanced effects of combined cognitive bias modification and computerised cognitive behavior therapy on social anxiety. Cogent Psychol 2: 1–13. Cain, C.K., Blouin, A.M., et al. (2004). Adrenergic transmission facilitates extinction of conditional fear in mice. Learn Mem 11(2):179–187. Cain, C.K., Maynard, G.D., et al. (2012). Targeting memory processes with drugs to prevent or cure PTSD. Expert Opin Investig Drugs 1323–1350. Carlbring, P., Apelstrand, M., et al. (2012). Internet-delivered attention bias modification training in individuals with social anxiety disorder: a double blind randomized controlled trial. BMC Psychiatry 12:66–80. Carleton, R.N., Teale Sapach, M.J., et al. (2015). A randomized controlled trial of attention modification for social anxiety disorder. J Anxiety Disord 33:35–44. Cisler, J.M., and Koster, E.H. (2010). Mechanisms of attentional biases towards threat in anxiety disorders: an integrative review. Clin Psychol Rev 30(2):203–216. Clark, D.A., and Beck, A.T. (2010). Cognitive theory and therapy of anxiety and depression: convergence with neurobiological finidings. Trends Cog Sci 14:418–424. Cristea, I. A., Kok, R. N., and Cuijpers, P. (2015). Efficacy of cognitive bias modification interventions in anxiety and depression: meta- analysis. Br J Psychiatry 206: 7–16. de Kleine, R., Hendriks, G.-J., et al. (2012). A randomized placebo- controlled trial of d-cycloserine to enhance exposure therapy for posttraumatic stress disorder. Biol Psychiatry 71(11):962–968.
C urrent T reatments nxiety Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis 4 S.0. Charney, et al., Oxford University Press USAfor - OSO,A 2018. 15:10:22.
de Quervain, D.J.F., Aerni, A., et al. (2009). Glucocorticoids and the regulation of memory in health and disease. Front Neuroendocrinol 30(3):358–370. de Quervain, D.J.F., Bentz, D., et al. (2011). Glucocorticoids enhance extinction-based psychotherapy. Proc Natl Acad Sci 108(16):6621. Ganasen, K.A., Ipser, J.C., et al. (2010). Augmentation of cognitive behavioural therapy with pharmacotherapy. Psychiatr Clin N Am 33(3):687–699. Guastella, A.J., and Alvares, G. (2012). D-Cycloserine. In: Hofmann, S., ed. Psychobiologial approaches for anxiety disorders: treatment combination strategies (pp. 75–90). West Sussex, UK: Wiley-Blackwell. Guastella, A.J., Richardson, R. et al. (2008). A randomized controlled trial of d-cycloserine enhancement of exposure therapy for social anxiety disorder. Biol Psychiatry 63:544–549. Hakamata, Y., Lissek, S., et al. (2010). Attention bias modification treatment: a meta-analysis toward the establishment of novel treatment for anxiety. Biol Psychiatry 68(11):982–990. Hallion, L.S., and Ruscio, A.M. (2011). A meta-analysis of the effect of cognitive bias modification on anxiety and depression. Psychol Bull 137(6):940–958. Hamilton, S., and Fyer, A.J. (2009). The molecular genetics of anxiety disorders. In: Charney, D.S., and Nestler, E.J., eds. Neurobiology of Mental Illness, 3rd Edition (pp. 585–602). New York: Oxford University Press. Heeren, A., Mogoaşe, C., et al. (2015). Attention bias modification for social anxiety: a systematic review and meta-analysis. Clin Psychol Rev 40:76–90. Herry, C., Bach, D.R., et al. (2007). Processing of temporal unpredictability in human and animal amygdala. J Neurosci 27:5958–5966. Herry C., Ferraguti F., et al. (2010). Neuronal circuits of fear extinction. Eur J Neurosci 31:599–612. Hofmann, S.G. (2007). Enhancing exposure-based therapy from a translational research perspective. Behav Res Therapy 45:1987–2001. Hofmann, S.G., Pollack, M.H., et al. (2006). Augmentation treatment of psychotherapy for anxiety disorders with D-cycloserine. CNS Drug Reviews 12(3–4):208–217. Hofmann, S. G., Smits, J et al. (2013). D-cycloserine as an augmentation strategy with cognitive-behavioral therapy for social anxiety disorder. Am J Psychiatry 170 (7): 751–758. Otto M.W., Kredlow, M.A. (2016) Enhancement of psychosocial treatment with d-cycloserine: models, moderators, and future directions. Biol Psychiatry 80(4):274–283. Holmes, A., and Quirk, G. J. (2010). Pharmacological facilitation of fear extinction and the search for adjunct treatments for anxiety disorders: the case of yohimbine. Trends Pharmacol Sci 31(1):2–7. Koster, E.H., Baert, S., et al. (2010). Attentional retraining procedures: manipulating early or late components of attentional bias? Emotion 10(2):230–236. Linetzky, M., Pergamin-Hight, L., et al. (2015). Quantitative evaluation of the clinical efficacy of attention bias modification treatment for anxiety disorders. Depress Anxiety 23:383–391. Macleod, C., and Mathews, A. (2012). Cognitive bias modification approaches to anxiety. Annu Rev Clin Psychol 8:189–217. Mathews, A., and MacLeod, C. (2005). Cognitive vulnerability to emotional disorders. Annu Rev Clin Psychol 1:167–195. Meyerbroeker, K., Powers, M.B., et al. (2012). Does yohimbine hydrochloride facilitate fear extinction in virtual reality treatment of fear of
flying? A randomized placebo-controlled trial. Psychother Psychosom 81(1):29–37. Mogoaşe, C., David, D., et al. (2014). Clinical efficacy of attentional bias modification procedures: an updated meta-analysis. J Clin Psychol 70(12):1133–1157. Morris, R.W., and Bouton, M.E. (2007). The effect of yohimbine on the extinction of conditioned fear: a role for context. Behav Neurosci 121(3):501. Myers, K.M., and Davis, M. (2007). Mechanisms of fear extinction. Mol Psychiatry 12:120–150. Norberg, M.M., Krystal, J.H., et al. (2008). A meta- analysis of D- cycloserine and the facilitation of fear extinction and exposure therapy. Biol Psychiatry 63(12):1118–1126. Ouimet, A.J., Gawronski, B., and Dozois, D.J. (2009). Cognitive vulnerability to anxiety: a review and an integrative model. Clin Psychol Rev 29(6):459–470. Porto, P.R., Oliveira, L., et al. (2009). Does cognitive behavioral therapy change the brain? A systematic review of neuroimaging in anxiety disorders. J Neuropsychiatry Clin Neurosci 21(2):114–125. Powers, M.B., Smits, J.A.J., et al. (2009). Facilitation of fear extinction in phobic participants with a novel cognitive enhancer: a randomized placebo controlled trial of yohimbine augmentation. J Anxiety Disord 23(3):350–356. Quartermain D., Mower J., et al. (1994). Acute but not chronic activation of NMDA-coupled glycine receptor with D-cycloserine facilitates learning and retention. Eur J Pharmacol 257(1-2):7–12. Quirk, G.J., and Mueller, D. (2008). Neural mechanisms of extinction learning and retrieval. Neuropsychopharmacology 33:56–72. Rapee, R.M., MacLeod, C., et al. (2013). Integrating cognitive bias modification into a standard cognitive behavioural treatment package for social phobia: a randomized controlled trial. Behav Res Ther 51:207–215. Ravindran, L.N., and Stein, M.B. (2010). The pharmacologic treatment of anxiety disorders: a review of progress. J Clin Psychiatry 71:839–854. Ressler, K.J., Rothbaum, B.O., et al. (2004). Cognitive enhancers as adjuncts to psychotherapy: use of D-cycloserine in phobic individuals to facilitate extinction of fear. Arch Gen Psychiatry 61(11):1136–1144. Salemink, E., Kindt, M., et al. (2014). Internet-based cognitive bias modification of interpretations in patients with anxiety disorders: a randomised controlled trial. J Behav Ther Exp Psychiatry 45:186–195. Singewald, N., Schmuckermair, C., et al. (2015). Pharmacology of cognitive enhancers for exposure-based therapy of fear, anxiety and trauma- related disorders. Pharmacol Ther 149:150–190. Smits, J.A., Rosenfield D., et al., (2014). Yohimbine enhancement of exposure therapy for social anxiety disorder: a randomized controlled trial. Biol Psychiatry 75:840–846. Soravia, L.M., Heinrichs, M., et al. (2006). Glucocorticoids enhance in vivo exposure-based therapy of spider phobia. Depress Anxiety 31:429–435. Taylor, S., Abramowitz, J., et al. (2012). Non-adherence and non-response in the treatment of anxiety disorders. J Anxiety Disord 26(5):583–589. Tsigos, C., and Chrousos, G.P. (2002). Hypothalamic-pituitary-adrenal axis, neuroendocrine factors and stress. J Psychosom Res 53(4):865–871. Van Bockstaele, B., Verschuere, B., et al. (2014). A review of current evidence for the causal impact of attentional bias on fear and anxiety. Psychol Bull 140(3):682–721. Wolf, O.T. (2008). The influence of stress hormones on emotional memory: relevance for psychopathology. Acta Psychol 127(3):513–531.
• A 544 nxiety isorders Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University PressD USA - OSO, 2018. 15:10:22.
SECTION 5 SUBSTANCE USE DISORDER S
Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press USA - OSO, 2018. 15:12:18.
Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press USA - OSO, 2018. 15:12:18.
41. EPIDEMIOLOGY OF SUBSTANCE USE DISORDER S Denise B. Kandel, Mei-Chen Hu, Pamela C. Griesler, Bradley T. Kerridge, and Bridget F. Grant
INTRODUCTION The epidemiology of drug use in the general population includes two distinct streams of research. The more common stream measures consumption patterns by asking individuals whether they have ever used specific classes of drugs, and, if so, how frequently they have done so. The second stream, and one implemented more rarely, measures the extent of problematic drug use by asking individuals about behaviors and symptoms that meet criteria for a substance use disorder. Important changes have been made in the definition of substance use disorders since the prior edition of this chapter, replacing in 2013 the DSM-IV criteria that had been used since 1994 with DSM-5 criteria (Hasin et al., 2013). To date, DSM-5 criteria have been operationalized in only one national survey of the US population 18 years and older, the 2012–2013 National Epidemiologic Survey on Alcohol and Related Conditions-III (NESARC-III) (Grant et al., 2016). Thus, while previously it was possible to compare rates of substance use disorder across several studies, and compare adolescents with adults, these comparisons based on the new definitions cannot be implemented. The ongoing National Survey on Drug Use and Health (NSDUH; Center for Behavioral Health, 2014) annually provides data on patterns of drug use and DSM-IV diagnoses for persons 12 years of age and older and makes possible comparisons of adolescents with adults. In this chapter, we present data on the epidemiology and phenomenology of substance use disorders from comparative and developmental perspectives. We discuss six issues: • The DSM-5 definitions and measurement of substance use disorders and differences from the DSM-IV • The prevalence of substance use and DSM-5 substance use disorders for legal drugs (cigarettes, alcohol), marijuana, illicit drugs (e.g., cocaine and nonmedical use of prescribed psychoactive drugs) among adults, and DSM-IV disorders among adults and adolescents • The prevalence of DSM-5 and DSM-IV substance use disorders by age, gender, and race/ethnicity • The comorbidity of DSM-5 substance use disorders with psychiatric disorders by gender and by race/ethnicity
• Developmental stages of involvement in drugs, including underlying biological processes • Adolescence as a critical exposure period The epidemiological data presented in the chapter are based on publications from NESARC-III and NSDUH, and secondary analyses of these datasets that we implemented when the appropriate documentation was not available in published reports. DEFINITION AND ME ASUREMENT O F S U B S TA N C E U S E D I S O R D E R S : D S M-I V A N D D S M-5 The diagnostic criteria for substance use disorders specified by the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders in 1994 (American Psychiatric Association, 1994) covered two maladaptive patterns of substance use: abuse and dependence. Abuse was conceptualized as being less severe than dependence and was diagnosed only if criteria for dependence were not met. Three of seven criteria needed to be experienced within a 12-month period in order for the diagnosis of DSM-IV substance dependence to be made: (1) tolerance; (2) withdrawal; (3) impaired control, the substance taken in larger amounts or over a longer period than intended; (4) unsuccessful quit attempts; (5) much time spent obtaining, using the substance, or recovering from its effects; (6) neglect of important social, occupational, or recreational activities; (7) continued use despite persistent or recurrent physical or psychological problems caused or exacerbated by the substance. Withdrawal was not included as a criterion for cannabis, inhalants, and hallucinogens, although a cannabis withdrawal syndrome has been established (Budney et al., 2003). As noted by Hughes (Hughes, 2006), generic criteria were based in part on shared genotype across different drugs, common underlying neurobiological processes, and by common behavioral correlates such as antisocial syndromes (Compton et al., 2005). DSM-IV abuse was a distinct diagnostic category that excluded individuals who met criteria for dependence, and required recurrent substance use during a 12-month period resulting in at least one of four harmful consequences: (1)
5 4 7 USA - OSO, 2018. Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press 15:12:18.
failure to fulfill major role obligations at work, school, or home; (2) hazardous use, such as driving an automobile or operating a machine when impaired by substance use; (3) legal problems, for example, arrests for substance-related disorderly conduct; and (4) continued use despite social or interpersonal problems caused by the substance. For tobacco (nicotine), the dependence criteria were the same as for alcohol and illicit drugs, but abuse criteria were not applied. These definitions differ substantively from those in the fifth edition (DSM-5) of the American Psychiatric Association, which became the standard as of 2013. The DSM-5 definitions were based on literature reviews and extensive secondary analyses of large-scale epidemiological datasets of the general population and clinical samples of adults and adolescents (Hasin et al., 2013; Hasin, 2015). The most important change was the combination of abuse and dependence criteria into a single substance use disorder. Craving was added as a criterion, while legal difficulties was eliminated, leaving a total of 11 criteria. Withdrawal syndromes were added for cannabis. Criteria for nicotine use disorder were aligned with those for other substance use disorders. Thus, the same criteria apply to disorders across substances (Shmulewitz et al., 2015). For all substances, including nicotine, the criteria for disorder became two or more out of 11 criteria (Hasin et al., 2013; O’Brien, 2011). A severity indicator was specified, with mild indexed by two to three criteria, moderate by four to five, and severe by six or more criteria. The methods used to determine the relationship between abuse and dependence included severity factor analysis to establish unidimensionality, item response theory to assess the relationship of abuse to dependence criteria, criterion/item characteristic curves to examine the severity and discrimination of each criterion relative to each other, and total information curves to allow comparisons of two or more sets of criteria (Hasin, 2015; Hasin et al, 2012; Saha et al., 2012). The evidence indicated that abuse and dependence formed one disorder. All the DSM-IV abuse and dependence criteria, except legal problems, aligned along a single dimension and were interspersed across the range of severity (Hasin et al., 2013). Furthermore, except for legal problems, the likelihood of endorsing the criteria did not vary by age, gender, or race/ethnicity (Hasin, 2015). In analyses of existing datasets, the new diagnostic definition of substance use disorder based on two or more criteria generated overall rates of substance use disorders similar to those derived from combining rates of DSM-IV dependence and abuse (Hasin et al., 2013; Hasin, 2015; Goldstein et al., 2015). However, there were differences across specific drugs. Comparisons of DSM-IV dependence and DSM- 5 substance use disorders found optimal concordance at a higher threshold than two DSM-5 criteria, namely four+ criteria, for alcohol, opioids, and cocaine, and six+ criteria for cannabis (Hasin, 2015; Compton et al., 2013). The inclusion of cannabis withdrawal in the DSM-5 definition of cannabis disorder but not the DSM-IV definition of cannabis dependence accounted for the lower overall concordance between DSM-IV and DSM-5 cannabis diagnosis than other diagnoses (Compton et al., 2013). Because DSM-5 combined abuse and dependence criteria, the rates of DSM-5 substance use
disorders presented in this chapter are higher than the rates of DSM-IV dependence discussed in the prior edition. T H E S U RVEYS : N E S A R C -I I I AND NSDUH At this time only a single study, NESARC-III, provides national data for DSM-5 based diagnoses among adults. To obtain insights into disorders among adolescents compared to adults, DSM-IV data need to be examined in the ongoing National Survey on Drug Use and Health of the population 12 years old and over (NSDUH [SAMHSA, 2015]). By contrast, four national surveys provided data on DSM-IV defined substance use disorders in the prior edition of this chapter: the 2010 NSDUH; the National Epidemiological Survey on Alcohol and Relates Conditions of adults 18 years old and over, carried out in 2001–2002 (Compton et al., 2005; Conway et al., 2006; Grant et al., 2004b); the National Comorbidity Survey Replication (NCS-R) study of adults 18 years old and over, carried out in 2001–2003 (Kessler et al., 2005a); and the National Comorbidity Survey for Adolescents 13–18 years old, carried out in 2001–2004 (NCS-A) (Kessler et al., 2012a). Comparisons across studies revealed substantial variations in prevalence due to differences among the surveys regarding the measurement of drug use, drug abuse, and DSM-IV drug dependence. In NESARC-III, respondents were asked which illicit drugs they had ever used from a list of ten drug classes. Either sedatives or tranquilizers was the first drug listed; the last class included “any other medicines or drugs (not otherwise defined).” More detailed questions about drug-specific patterns of use were then asked for each drug reported to have been used. Symptoms of DSM-5 substance use disorder were ascertained first without reference to any drugs. Respondents were then asked which “medicines or drugs did this happen with?” during the last 12 months, and before 12 months ago. The NSDUH asked about DSM-IV abuse and dependence symptoms experienced in the last 12 months but not lifetime for all substances, except nicotine. For nicotine, symptoms of nicotine dependence were ascertained for the last 30 days with the Nicotine Dependence Syndrome Scale (NDSS) (Shiffman et al., 2004). In NESARC-III, being a smoker was defined as having ever smoked at least 100 cigarettes, or 50 cigars, or smoked a pipe 50 times, or used snuff, or used e-cigarettes/e- liquid. The nicotine use disorder questions were ascertained in this restrictive group of smokers, whereas the NSDUH asked the nicotine-related dependence questions of anyone who had ever smoked cigarettes, even if only a puff. The two surveys have different strengths and weaknesses. NESARC-III has the most systematic assessment of DSM- 5 substance use and psychiatric disorders for past year, prior to past year and lifetime periods. The annual NSDUH surveys provide detailed repeated data on patterns of use of legal and illegal drugs in the population and also include detailed DSM-IV assessments of abuse and dependence on alcohol, specific illicit drugs, and the nonmedical use of medically prescribed drugs for the last 12 months. Anonymity in NSDUH
• Oxford 548 S ubstance UUSA se D isorders Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., University Press - OSO, 2018. 15:12:18.
may have led to higher rates of self-reported drug use than in NESARC-III, whereas differences in instrumentation may have led to higher rates of last 12-month substance use disorder among the self-acknowledged drug users in NESARC- III than NSDUH. The NSDUH surveys respondents as of age 12, making possible comparisons between adolescents and adults. There are slight differences in the classification of selected drugs between the surveys. Ecstasy/MDMA were included under club drugs in NESARC, but under hallucinogens in NSDUH. We implemented extensive secondary analyses of the two datasets to supplement published results. For reasons of confidentiality, the public-use 2014 NSDUH data include only 81.4% of the original sample, so that in certain instances the figures in this chapter differ very slightly from published ones. We included DSM-IV nicotine dependence or DSM- 5 tobacco use disorder (nicotine use disorder) in summary measures of drug use disorder for the two surveys.
P R E VA L E N C E O F S U B S TA N C E U S E A N D S U B S TA N C E U S E D I S O R D E R S P R EVA L E N C E A MO N G A D U LTS
The lifetime and last 12-month prevalence of use of specific substances in the NSDUH and NESARC-III for persons aged 18 and over are presented in the first two panels of Table 41.1. The rates of alcohol use are very similar across the two studies, whereas those for nicotine (tobacco) and illicit drugs are much higher in NSDUH than NESARC-III (Table 41.1, Panels 1 and 2). The discrepancy for nicotine is explained by the fact that, in NESARC-III, smoking at least 100 cigarettes lifetime was required to be defined as a smoker. Yet, 36% of smokers in NSDUH never smoked 100 cigarettes, reflecting the inclusion of those who have had little experience with smoking. When restricted to those who smoked at least 100 cigarettes, the rates in both studies are almost identical. It is not clear why the overall rates of lifetime or last-year illicit drug use in NESARC-III are at least 20% lower than those in NSDUH, except for stimulants and nonmedical prescription opioids. For instance, 47.1% in NSDUH report having ever used marijuana compared to 32.1% in NESARC-III; 16.3% and 9.9%, respectively, report having ever used cocaine; 14.3% and 11.3%, respectively, report having ever used prescription opioids nonmedically. Lack of anonymity may be one explanation for these discrepancies (Grucza et al., 2007). Despite these differences in absolute rates across the two studies, the relative rankings for overall prevalence of substance use are the same in both. Alcohol is the substance that is used most widely, followed by nicotine and illicit drugs. As per NSDUH, half the adults 18 and over in the United States have used an illicit drug, including nonmedical use of a prescribed drug, representing 125 million individuals in 2014. Of these drugs, marijuana is the most prevalent, followed by cocaine and hallucinogens. Almost three times as many individuals have ever used marijuana as have used cocaine or hallucinogens (Table 41.1, Panel 1). The
higher rates in NSDUH than NESARC-III increase the base of individuals eligible for being asked the questions relevant to substance abuse and dependence or substance use disorders and the absolute number identified as meeting these criteria. Lifetime and last 12-month rates of substance use disorders in the total adult population, lifetime rates among lifetime users of each drug class, last 12-month rates among last 12-month users, and last 12-month rates among those meeting criteria for a lifetime substance use disorder are presented for DSM-5 in NESARC-III, and last 12-month rates only for DSM-IV in NSDUH in Table 41.2. The conditional rates among users specify the risk of developing a substance use disorder on a drug among those who consumed the drug in their lifetime or the last 12 months. The conditional rates of last 12-month disorder among those who met lifetime criteria index chronicity of disorder. None of the published reports from the studies include nicotine use disorder in any substance use disorder. This is a serious omission inasmuch as tobacco is one of the two most addictive substances that are used, higher than heroin in NESARC-III, second to heroin in NSDUH. Table 41.2 presents rates of any substance use disorder excluding nicotine, as typically reported in the literature (Row 14), and rates including nicotine use disorder (Row 15). Rates of last 12-month disorder are consistently the lowest in NSDUH (Table 41.2, Panels 2 and 4). In NESARC, 43.1% of the population 18 years old and over ever met criteria for a substance use disorder, including nicotine; 27.9% met criteria for a nicotine use disorder, 29.1% for an alcohol use disorder, and 9.9% for an illicit drug disorder (Table 41.2, Panel 1). The 12-month rates were 61% to 28% lower than lifetime rates. Close to 30% of the population met criteria for a substance use disorder within the last 12 months in NESARC-III, a rate that is twice as high as in NSDUH (Table 41.2, Panel 2). The proportion meeting criteria for disorder on a given drug among individuals who used the drug varied greatly across drug classes. Conditional upon lifetime use, nicotine emerged as the most addictive of substances, with 60.8% of nicotine users in NESARC-III meeting criteria for lifetime nicotine disorder. This compares to 32.7% for alcohol use disorder among drinkers and 29.6% among heroin users (Table 41.2, Panel 3). Among last 12-month users, however, nicotine (73.7%) and heroin (63.4%) emerged as the most addictive substances by far. Conditional rates of other substance use disorders among last 12-month users were half to a third those of nicotine and heroin (Table 58412, Panel 4). Substance use disorders are chronic. As illustrated by NESARC-III, two-thirds (67.1%) of those who met criteria for a lifetime substance use disorder on any substance still experienced these symptoms within the last year (Table 41.2, Panel 5). Nicotine is by far the most chronic of the addictions, with 71.9% of nicotine users meeting criteria for last 12- month disorder among those who ever met lifetime criteria. Chronicity is higher for an alcohol (47.7%) than an illicit drug (39.2%) disorder (Table 41.2, Panel 5). Chronicity of disorder is also relatively high among those who consume prescribed drugs nonmedically, especially opioids (43.3%). These rates could not be calculated for NSDUH, which only measured last 12-month abuse and dependence.
E pS.idemio oOxford gy of S ubstance U se D Charney and Nestler's Neurobiology of Mental Illness, edited by 41. Dennis Charney, et l al., University Press USA - OSO, 2018. 15:12:18.
9
Table 41.1 LIFETIME AND LAST 12-M ONTH PREVALENCE OF SUBSTANCE USE AMONG PERSONS AGED 18 AND OLDER IN NESARC-I II (N = 36,309), NSDUH 2014 (N = 41,671), AND AMONG PERSONS AGED 12–17 IN NSDUH 2014 (N = 13,600) (1) LIFETIME RATES AMONG PERSONS 18+
(2) LAST 12-M ONTH RATES AMONG PERSONS 18+
(3) LIFETIME (4) LAST 12-M ONTH RATES AMONG RATES AMONG PERSONS 12–17 PERSONS 12–17
NESARC-III % (95% CI)
NSDUH % (95% CI)
NESARC-III % (95% CI)
NSDUH % (95% CI)
NSDUH % (95% CI)
NSDUH % (95% CI)
Alcohol
88.9 (88.0–89.8)
87.6 (87.1–88.0)
72.7 (71.4–73.9)
71.0 (70.3–71.8)
29.8 (28.9–30.7)
24.2 (23.5–25.2)
Nicotinea
45.8 (44.7–47.0)
71.4 (70.7–72.1)
27.2 (26.3–28.1)
32.6 (31.9–33.3)
18.8 (17.9–19.7)
13.0 (12.3–13.8)
Cigarettes
–
66.1 (65.4–6 6.9)
–
26.7 (26.1–27.3)
14.4 (13.6–15.3)
9.0 (8.3–9.7)
Cigarettes (100+ ever)
42.0 (40.9–43.1)
42.2 (41.6–43.2)
23.5 (22.7–24.3)
23.1 (22.5–23.7)
2.9 (2.6–3.3)
2.8 (2.4–3.1)
Any Illicit Drugb
36.8 (35.6–37.9)
51.9 (51.1–52.7)
13.3 (12.7–13.9)
16.7 (16.3–17.1)
23.3 (22.4–24.2)
17.6 (16.9–18.4)
Marijuana (Cannabis)
32.1 (31.1–33.2)
47.1 (46.4–47.9)
9.5 (9.0–10.1)
13.4 (13.0–13.8)
16.5 (15.7–17.3)
13.3 (12.6–14.0)
Cocaine
9.9 (9.5–10.5)
16.3 (15.8–16.8)
1.0 (0.9–1.2)
1.9 (1.7–2.0)
0.9 (0.7–1.2)
0.7 (0.6–1.0)
Heroin
1.6 (1.5–1.8)
2.0 (1.8–2.1)
0.2 (0.2–0.3)
0.4 (0.3–0.5)
0.2 (0.1–0.3)
0.1 (0.1–0.2)
Inhalants/Solvents
3.1 (2.9–3.4)
8.3 (8.0–8.7)
0.2 (0.2–0.3)
0.5 (0.4–0.5)
5.1 (4.8–5.6)
2.0 (1.7–2.3)
Hallucinogens
9.3 (8.8–9.8)
16.4 (15.8–17.0)
0.6 (0.5–0.8)
1.7 (1.5–1.8)
2.5 (2.1–2.9)
1.7 (1.4–2.1)
Opioids (Nonmedical)
11.3 (10.6–12.0)
14.3 (13.7–14.8)
4.1 (3.8–4.4)
3.8 (3.6–4.0)
7.3 (6.8–7.9)
4.8 (4.4–5.3)
Sedatives/Tranquilizersc
7.5 (7.0–8.0)
11.3 (10.9–11.8)
2.3 (2.1–2.6)
2.1 (1.9–2.3)
3.1 (2.7–3.5)
2.3 (1.9–2.3)
Sedatives
–
3.1 (2.9–3.4)
–
0.3 (0.2–0.3)
0.8 (0.6–1.1)
0.5 (0.3–0.7)
Tranquilizers
–
10.1 (9.8–10.5)
–
2.0 (1.8–2.1)
2.5 (2.2–2.9)
1.6 (1.3–1.9)
Stimulants
8.3 (7.9–8.8)
8.3 (7.9–8.7)
1.2 (1.1–1.4)
1.2 (1.1–1.4)
2.1 (1.8–2.5)
1.5 (1.2–1.8)
Club Drugsd
4.4 (4.1–4.8)
–
0.7 (0.6–0.8)
–
–
–
Other Drugse
0.8 (0.7–1.0)
–
0.3 (0.2–0.3)
–
–
–
SUBSTANCE USE
Based on having ever smoked at least 100 cigarettes, or 50+ cigars, or 50+ times pipes, or used 20+ times snuff or chewing tobacco, or used e-cigarettes/e-liquid in NESARC-III; any tobacco product use in NSDUH. a
Any of 10 drugs: (1) marijuana (cannabis), (2) cocaine, (3) heroin, (4) inhalants/solvents, (5) hallucinogens, (6) opioids other than heroin, (7) sedatives/tranquilizers, (8) stimulants, (9) club drugs, (10) any other drug. b
Sedatives and tranquilizers were asked about separately in NSDUH, but as one category in NESARC-III.
c
Club drugs (MDMA, Ecstasy, GHB, Rohypnol, Ketamine, Special K, XTC, Roofies) were listed in NESARC-III. No separate category for club drugs in NSDUH, and MDMA and Ecstasy were included in hallucinogens. d
Any other medicines or drugs, e.g., steroids, Elavil, Thorazine or Haldol were listed in NESARC-III. No separate category for other drugs in NSDUH. Elavil, Thorazine, and Haldol were listed in other opioids, tranquilizers, or stimulants. e
Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press USA - OSO, 2018. 15:12:18.
Table 41.2 LIFETIME AND LAST 12-M ONTH PREVALENCE OF DSM-5 SUBSTANCE USE DISORDERS IN NESARC-I II (N = 36,309) AND LAST 12-M ONTH PREVALENCE OF DSM-I V SUBSTANCE USE DISORDERS IN NSDUH 2014 (N = 41,671) AMONG PERSONS AGED 18 AND OLDER (3) LIFETIME RATES AMONG LIFETIME (1) LIFETIME USERS RATES (2) LAST 12-M ONTH RATES
(4) LAST 12-M ONTH RATES AMONG LAST 12-M ONTH USERS b
Substance Use Disorder
NESARC- III % (95% CI)
NESARC- III % (95% CI)
NSDUH % (95% CI)
Alcohol
29.1 (28.2–30.1)
13.9 (13.3–14.5)
6.8 (6.5–7.1)
32.7 (31.7–33.7)
19.1 (18.3–19.9)
9.6 (9.1–10.0)
47.7 (46.1–49.3)
Nicotinea
27.9 (26.9–28.9)
20.0 (19.2–20.9)
–
60.8 (59.5–62.1)
73.7 (72.3–75.1)
–
71.9 (70.3–73.4)
–
–
8.7 (8.4–9.1)
–
–
32.7 (31.6–33.9)
–
Any Illicit Drugc
9.9 (9.4–10.4)
3.9 (3.6–4.2)
2.6 (2.4–2.8)
26.9 (25.6–28.3)
29.3 (27.5–31.1)
15.5 (14.5–16.6)
39.2 (37.2–41.2)
Marijuana (Cannabis)
6.3 (5.8–6.7)
2.5 (2.3–2.8)
1.5 (1.3–1.6)
19.5 (18.3–20.8)
26.7 (24.9–28.6)
10.9 (10.0–11.9)
40.5 (38.0–43.1)
Cocaine
2.4 (2.2–2.6)
0.3 (0.3–0.4)
0.4 (0.3–0.5)
24.0 (22.2–25.8)
33.7 (27.7–4 0.2)
20.4 (17.4–23.8)
14.6 (12.1–17.4)
Heroin
0.5 (0.4–0.6)
0.1 (0.1–0.2)
0.2 (0.2–0.3)
29.6 (25.1–34.5)
63.4 (49.4–75.5)
57.7 (47.6–67.2)
27.5 (18.6–38.7)
Inhalants/Solvents
0.2 (0.1–0.2)
0.04 (0.02–0.09)
0.02 (0.01–0.04)
5.2 (3.7–7.3)
19.8 (9.3–37.4)
4.8 (2.4–9.3)
25.5 (12.2–45.9)
Hallucinogens
0.6 (0.5–0.7)
0.05 (0.03–0.08)
0.08 (0.06–0.11)
6.4 (5.4–7.6)
7.8 (4.7–12.9)
4.9 (3.5–6.7)
8.1 (4.8–13.5)
Opioids (Nonmedical)
2.1 (1.9–2.3)
0.9 (0.8–1.0)
0.7 (0.6–0.8)
18.2 (16.4–20.1)
21.7 (19.1–24.5)
18.8 (16.7–21.2)
43.3 (39.5–47.2)
Sedatives/Tranquilizers
1.1 (0.9–1.2)
0.4 (0.3–0.5)
0.2 (0.1–0.2)
14.2 (12.4–16.2)
16.1 (13.5–19.0)
8.7 (7.0–10.6)
35.2 (29.9–4 0.9)
Stimulants
1.7 (1.5–1.9)
0.3 (0.3–0.4)
0.2 (0.1–0.2)
20.6 (18.5–22.9)
26.1 (20.7–32.4)
16.0 (9.0–26.9)
18.7 (15.0–23.1)
Any Substance Use Disorder, not including Nicotine
31.6 (30.6–32.6)
15.7 (15.0–16.3)
8.4 (8.1–8.7)
35.2 (34.2–36.3)
21.2 (20.3–22.0)
11.9 (11.5–12.4)
49.6 (48.1–51.2)
Any Substance Use Disorderd
43.1 (42.1–4 4.2)
28.9 (28.1–29.8)
15.4 (15.0–15.9)
47.5 (46.4–48.6)
37.1 (36.0–38.1)
20.0 (19.5–20.6)
67.1 (65.9–68.3)
Cigarettesb
NESARC-III % NESARC- NSDUH % (95% CI) III % (95% CI) (95% CI)
(5) LAST 12-M ONTH RATES AMONG LIFETIME DISORDER
NESARC-III % (95% CI)
Ever smoked at least 100 cigarettes, or 50+ cigars, or 50+ times pipes, or used 20+ times snuff or chewing tobacco, or used e-cigarettes/e-liquid.
a
b
Nicotine dependence on cigarettes last 30 days as measured by the NDSS.
Any of 10 drugs: (1) marijuana (cannabis), (2) cocaine, (3) heroin, (4) inhalants/solvents, (5) hallucinogens, (6) opioids other than heroin, (7) sedatives/tranquilizers, (8) stimulants, (9) club drugs, (10) any other drug. c
Includes alcohol, nicotine, any illicit drug.
d
P R EVA L E N C E A MO N G A D O L E S C E N TS
The behavior of adults 18 years old and over could be compared with that of adolescents 12–17 years old in NSDUH. For substance use disorders, this comparison was based on the DSM-IV definitions which combined abuse and dependence. The prevalence of lifetime use of various substances is consistently lower among adolescents than adults, with wide
differences across substances (Table 41.1, Panels 3 versus 1, 4 versus 2). The lifetime adolescent rates for alcohol are about 34% of those observed among adults, those for any nicotine are 26% lower, those for having smoked at least 100 cigarettes are 7% of those for adults, and those for any illicit drug are 45% of those observed among adults. There are great variations across specific illicit drugs in the ratio of adolescent to
E pS.idemio oOxford gy of S ubstance U se D Charney and Nestler's Neurobiology of Mental Illness, edited by 41. Dennis Charney, et l al., University Press USA - OSO, 2018. 15:12:18.
adult lifetime prevalence rates. Inhalants is the drug class for which the lifetime rates are the least different. With respect to last 12-month use, the age patterns are reversed for illicit drugs overall: adolescents have slightly higher rates than adults, 17.6% versus 16.7%. The differences are relatively greater among adolescents than adults for inhalants (2.0% versus 0.5%) and nonmedical prescription opioids (4.8% versus 3.8%). The rates for marijuana and hallucinogens are similar. The last 12-month rates of any DSM-IV alcohol and illicit drug use disorder (abuse/ dependence) among 12- month users are higher among adolescents (11.5% alcohol, 20.2% illicit drug) than adults (9.6% alcohol, 15.5% illicit drug) in the NSDUH. The rates of nicotine dependence among cigarette users are higher among adults (32.7%) than adolescents (11.5%) (Table 41.2, Panel 4; Figure 41.1C). Persistence of disorder could not be compared among adolescents and adults because NSDUH does not ascertain lifetime substance use disorder. C O M O R B I D I T Y O F S U B S TA N C E U S E A N D D S M- 5 S U B S TA N C E U S E D I S O R D E R S AC R O S S S U B S TA N C E S Consideration of each drug class by itself underestimates the extent of drug use in the population, because many individuals use more than one class of drugs. In 2014, only 8.8% of persons aged 18 and over had not experimented with any substance; 43.4% had experimented with all three major classes: alcohol, nicotine, and illicit drugs (based on NSDUH 2014). Similarly, substance use disorders tend to co-occur. In NESARC-III, 42.2% of individuals 18 and over who met criteria for a substance use disorder on one drug class also met criteria for at least one other drug disorder; 12.8% met criteria for two other substance use disorders. The highest comorbidity was between an illicit drug disorder and alcohol (75.0%) or nicotine (70.2%) disorder. Yet, only a minority of addicted individuals have been treated for their addiction: 13.5% of persons with a 12-month substance use disorder received any treatment, including treatment from a health professional, attending 12-step groups, or an outpatient or rehabilitation facilities. This proportion increased only to 19.5% among those with a moderate to severe disorder (Grant et al., 2013). P R E VA L E N C E O F S U B S TA N C E U S E A N D S U B S TA N C E U S E D I S O R D E R S BY AG E , G E N D E R , R AC E /ET H N I C I T Y There are important differences in the prevalence of use and substance use disorders in different subgroups in the population, but the patterns are not consistent across surveys. AG E
Differences between adolescents and adults were discussed earlier. Adulthood itself can be differentiated into ages 18–25,
26–34, 35–49, and 50 and over. Rates of last 12-month use by age in the population are presented in Figure 41.1A–B, and rates of last 12-month disorder among last 12-month users are presented in Figure 41.1C–D. Age-related trends are presented for cigarette users in NSDUH and for those who used nicotine in NESARC-III. Age-related patterns are very similar across the two surveys, although the absolute rates of use or disorder may differ. The prevalence of substance use varies greatly by age. With the exception of nicotine (cigarettes), age-related differences are stronger for use in the population than for disorder among those who used a particular substance. Rates of use of all substances increase sharply throughout adolescence, and decline also sharply as of ages 18–25 for illicit drugs (Figure 41.1A– B). In NSDUH, any use of cigarettes declines more slowly. In NESARC, the decline for those who used nicotine begins at ages 26–34. The prevalence of drinking alcohol remains at fairly stable levels from ages 18 to 49, when rates start to decline. Among last 12-month users, age-related patterns for substance use disorder differ from those for use (Figure 41.1C–D). For cigarette users in NSDUH, conditional rates of nicotine dependence rise sharply from adolescence to the mid-thirties and then more slowly thereafter (Figure 41.1C). Rates of nicotine disorder remain flat in NESARC-III (Figure 41.1C–D). The rates of alcohol disorder decline consistently as of ages 18–25 in both surveys. The conditional rates of any illicit drug disorder among last 12-month users decline as of ages 12–17 in NSDUH and ages 18–25 in NESARC-III. Rates of nonmedical opioid use disorder increase as of ages 18–25 in NSDUH but do not vary with age in NESARC-III (Figure 41.1C–D). GENDER
Gender patterns for substance use and substance use disorders are similar in NESARC-III and NSDUH (Table 41.3). For all substances, males have consistently higher rates of use in the population than females, with the rates higher by about 10% for alcohol, and by 42%–60% for nicotine and all illicit drugs combined. Gender differences are especially pronounced for marijuana and cocaine. There are fewer gender differences in rates of substance use disorder among users than in rates of use. The rates of nicotine disorder in NESARC-III are slightly higher for females than males (Table 41.3). In both surveys, rates of alcohol and any illicit drug disorders (marijuana in particular) are higher for males than females. However, rates of cocaine and nonmedical prescription opioid disorders are the same for both genders. R AC E/E T H N I C I T Y
Racial/ethnic differences in patterns of substance use in the population are similar in NESARC-III and NSDUH, but differ for substance use disorder (Table 41.4). In both surveys, Asians have the lowest rates of use for every drug class, but not the lowest rates of disorder. Whites have the highest rates of use of any substance, especially alcohol. In NESARC-III, African Americans have the highest rate of any group for
• Oxford 552 S ubstance U USA se D isorders Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., University Press - OSO, 2018. 15:12:18.
(b)
NSDUH-TOTAL SAMPLE
NESARC-III -TOTAL SAMPLE
90
90
80
80
70
70
Last 12-Month Use (%)
Last 12-Month Use (%)
(a)
60 50 40 30 20 10 0 12–17
60 50 40 30 20 10
18–25
26–34
35–49
0 12–17
50+
18–25
Age NSDUH-AMONG LAST 12-MONTH USERS
(d) 90
80
80
70 60 50 40 30 20 10 18–25
Alcohol
26–34 Age Cigarettes
50+
NESARC-III -AMONG LAST 12-MONTH USERS
90
0 12–17
35–49
Age
Last 12-Month DSM-5 Disorder (%)
Last 12-Month DSM-IV Disorder (%)
(c)
26–34
35–49
50+
Nicotine
70 60 50 40 30 20 10 0 12–17
18–25
Nonmedical Prescription Opioids
26–34 Age
35–49
50+
Any Illicit Drugs
Figure 41.1
Prevalence of last 12-month use of alcohol; cigarettes (NSDUH 2014); any nicotine (at least 100 cigarettes, or 50+ cigars, or 50+ times pipes, or used 20+ times snuff or chewing tobacco, or used e-cigarettes/e-liquid in NESARC-III); nonmedical prescription opioids and any illicit drugs by age in (A) NSDUH 2014, (B) NESARC-III; and prevalence of last 12-month substance use disorders by age among last 12-month users in (C) NSDUH 2014, (D) NESARC-III.
any substance use disorder (40.7%) and alcohol use disorder (21.7%). African Americans and Hispanics have the highest rates for any illicit drug disorder. In NSDUH, ethnic patterns are less consistent. Whites have the highest rates of nicotine dependence among last 12-month smokers; African Americans have a higher rate of any illicit drug disorder than whites. C O M O R B I D I T Y O F S U B S TA N C E USE DISORDER S WITH P SYC H I AT R I C D I S O R D E R S There is extensive comorbidity between addiction and mental illness, as documented by NESARC-III. The associations between psychiatric and substance use disorders are highly statistically significant for all classes of psychiatric disorders and all substances. The associations are somewhat higher with mood than anxiety disorders, and much higher—by a factor of two or three—with antisocial personality than mood or
anxiety disorders, with odds ratios ranging from 6 to 13 with illicit drugs (Table 41.5). Among individuals with a diagnosis of substance use disorder on illicit drugs, 49.6% met criteria for a mood disorder (odds ratio = 3.5,95%CI = 3.2-3.9), 35.3% for an anxiety disorder (odds ratio = 3.1,95%CI = 2.8– 3.5), 18.3% for antisocial personality disorder (odds ratio = 7.8,95%CI = 6.8-8.8), and 64.7% for any psychiatric disorder (odds ratio = 4.2,95%CI = 3.8–4.7) (Table 41.5). The comorbidity rates among those with an alcohol or nicotine disorder were similar and lower than the rates for the six classes of illicit drugs that were considered (Table 41.5). Alcohol and nicotine, the two drugs with the highest prevalence of disorder in the population, had the lowest comorbidity with psychiatric disorders (see also Compton et al., 2005; Conway et al., 2006). As suggested by Compton et al. (Compton et al., 2005), the strong association with antisocial personality disorder across various substances may reflect an underlying comorbidity factor rather than substance specific links. This has important
E pS.idemio oOxford gy of S ubstance U se D Charney and Nestler's Neurobiology of Mental Illness, edited by 41. Dennis Charney, et l al., University Press USA - OSO, 2018. 15:12:18.
Table 41.3 PREVALENCE OF LAST 12-M ONTH SUBSTANCE USE AND DSM-5 SUBSTANCE USE DISORDERS IN NESARC-I II (N = 36,309) AND DSM-I V SUBSTANCE USE DISORDERS IN NSDUH 2014 (N = 41,671) AMONG LAST 12-M ONTH USERS AGED 18 AND OLDER , BY GENDER NESARC-III
NSDUH
MALES LAST 12-M ONTH
FEMALES
MALES
%
(95% CI)
%
(95% CI)
76.7
(75.4–77.9)
69.0
33.1
(32.0–34.2)
21.7
FEMALES
%
(95% CI)
%
(95% CI)
(67.5–70.5)***
74.2
(73.0–75.4)
68.1
(67.0–69.2)***
(20.7–22.7)
40.6
(39.5–41.6)
25.2
24.2–26.0)***
–
30.1
(29.3–31.0)
23.5
(22.7–24.3)***
Substance Use Alcohol Nicotine
a
Cigarettes
***
–
Any Illicit Drugb
15.7
(14.9–16.7)
11.0
(10.3–11.7)***
20.2
(19.6–20.9)
13.4
(12.9–14.1)***
Marijuana (Cannabis)
12.3
(11.5–13.1)
6.9
(6.4–7.5)
16.9
(16.3–17.6)
10.1
(9.6–10.6)***
Cocaine
1.4
(1.2–1.6)
0.7
(0.5–0.9)***
2.5
(2.3–2.8)
1.3
(1.1–1.5)***
Opioids (Nonmedical)
4.4
(4.0–4.8)
3.8
(3.5–4.3)*
4.4
(4.0–4.7)
3.3
(3.0–3.6)***
Any Substance Use
82.3
(81.3–83.3)
74.2
(72.9–75.5)
80.4
(79.5–81.4)
73.8
(72.6–74.9)***
c
Total N
(15,862)
***
***
(20,447)
(19,412)
(22,259)
DSM-5/DSM-IV Substance Use Disorder among Last 12-Month Users of Each Substance Alcohol
23.0
(22.0–24.1)
15.0
(14.2–16.0)***
Nicotinea
70.3
(68.5–72.0)
78.5
(76.8–80.2)***
Cigarettesd
—
12.2
(11.6–13.1)
6.7
(6.3–7.3)***
—
32.0
(30.4–33.6)
33.7
(32.3–35.2)
—
—
Any Illicit Drugb
30.9
(28.7–33.2)
27.1
(24.6–29.7)*
17.0
(15.4–18.6)
13.5
(12.2–14.8)***
Marijuana
28.4
(26.0–30.9)
24.0
(21.4–26.8)*
12.3
(10.0–13.9)
8.7
(7.8–9.7)***
Cocaine
33.2
(26.3–41.0)
34.4
(25.2–45.0)
18.7
(14.6–23.6)
23.7
(17.9–30.6)
20.9
(17.9–24.3)
22.5
(18.6–26.8)
18.8
(15.6–22.5)
18.8
(16.1–21.8)
41.5
(40.1–42.8)
32.5
(31.3–33.8)
23.2
(22.3–24.1)
16.9
(16.2–17.6)***
Opioids (Nonmedical) Any Substance Use Disorder
c
***
*p= 60 Years in GBD 61 studies from Western Europe, 34 studies from East Asia, Regions. Adapted from Prince et al., 2013. • DPress ementia Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford678 University USA - OSO, 2018. 15:41:51.
Persons with dementia (in millions)
120 100 80 60 40 20 0
2010
2030
2050
Year High Income Regions Figure 50.2
Low/middle Income Regions
Projected Prevalence of Dementia.
in dementia prevalence results from increases in developing countries. In contrast, projections for developed regions have predicted either a moderate proportionate increase or even a decline. Specifically, in 2005, based on data between 1982 and 1999 from the National Long-Term Care Surveys, scientists from the Duke Center for Demographic Studies reported a decline in the prevalence of severe cognitive impairment in the United States (Manton et al., 2005). Since then, other groups have reported similar estimates for some Western countries, with the latest study published by researchers from the Framingham Heart Study which observed a decline in dementia incidence based on data from 1975 to the present, namely a 20% decrease in incidence in each decade (Satizabal et al., 2016). The most likely explanations for this observed decline in industrialized regions are increased economic wealth, better levels of education, and effects of primary and secondary prevention of risk factors, in particular vascular disease, including the use of statins, antihypertensive agents, and nonsteroidal anti-inflammatory drugs, although decline in these factors do not fully explain the decrease in dementia incidence (Satisabal et al., 2016). As described, predictions of growth for sub-Saharan Africa, a region with persistently high child mortality and effects of fatal epidemics, remain as expected modest, with prevalence estimates of 2%–4%. Despite this observed decline in Western countries and the limited growth for regions with persistently high child mortality and fatal epidemics, the global prevalence over the four coming decades is still projected to quadruple due to the high burden of disease contributed by developing regions. When interpreting these data it is important to recognize their limitations. In general, derivation of accurate data about the courses of chronic diseases is difficult. As described, data from many world regions were sparse. Second, the estimations of prevalence and incidence rely on demographic statistics, which might not be accurate for many parts of the world, especially for older age groups. Third, temporal trends are best derived through continuous monitoring for new cases in a representative community-based sample over an extended observation period, with the use of consistent diagnostic criteria. However, most studies conducted were based on
comparisons of prevalence data ascertained at multiple time points, and potentially modified diagnostic criteria. While the longitudinal data by the Framingham Heart Study overcome this limitation, this study reflects only a single population sample. Fourth, since trajectories of chronic disease incidence reflect interactions of various causal factors, it remains uncertain whether decreases will continue or reverse. For example, the notable increases in obesity and diabetes in Western countries could halt or even reverse the observed decline in dementia incidence. Finally, if populations age, the prevalence of dementia can increase even if the incidence decreases; and if the size of the elderly population grows, the absolute number of people with dementia can increase even if both incidence and prevalence decrease. Consequently, the prevalence of dementia is expected to escalate as societies age, and therapies that delay onset even only slightly could considerably reduce age-specific prevalence and public health burden. N O N G E N ET I C R I S K A N D P R OT E C T I VE FAC TO R S Epidemiological studies have implicated several factors (both risk or protective) in cognitive function, dementia, and/or AD. “Risk factors” are defined as precursors of at least a part of the disease pathway, and can be associated with the etiology or the outcome of a disease. They may be used to assess disease risk, but they do not exhibit adequate sensitivity and/or specificity to be employed as diagnostic markers. “Protective factors” are conditions or elements that alleviate or eliminate disease risk and increase health. R I S K FAC TO R S
Several risk factors have been linked to the risk of dementia and/or AD. Among the strongest risk factors are several vascular risk factors associated with coronary artery disease and stroke (i.e., diabetes, hypertension, obesity) and cerebrovascular disease itself. However, while vascular risk factors and cerebrovascular disease are clearly associated with vascular dementia and are associated with AD, the molecular pathways underlying their individual association with AD remain to be determined.
Cerebrovascular Disease A variety of cerebrovascular changes including hemorrhagic infarcts, small and large ischemic cortical infarcts, vasculopathies, and white matter changes have been demonstrated to heighten the risk of dementia. In aging demented patients, cerebrovascular alterations induced by a sustained process of vascular remodeling, with disrupted blood vessel integrity caused by insults to the macro-and microvasculature, are a common characteristic neuropathological finding. While the specific molecular mechanisms underlying the associations between cerebrovascular disease and cognitive impairment remain to be fully clarified, there is evidence for various etiologic mechanisms. First, a cerebral insult can cause direct damage to brain
D S. iagnosis E pidemiology D Charney and Nestler's Neurobiology of Mental Illness, edited by 50. Dennis Charney, et al.,and Oxford University Press USA - OSO,of 2018. 15:41:51.
regions essential for proper memory function, such as the hippocampus or the thalamocortical projections. Second, cerebrovascular disease might trigger the deposition of Aβ, which in turn can lead to cognitive decline. Third, cerebrovascular disease might trigger inflammatory responses impairing cognitive function. The recent genomic studies have clearly implicated inflammation and immune response as a major etiologic mechanism in AD (Lambert et al., 2013; Jonsson et al., 2013; Guerreiro et al., 2013). Finally, there is data suggesting that cerebral hypoperfusion can lead to overexpression of cyclin- dependent kinase 5 (CDK5), a serine–threonine kinase critical to synapse formation and synaptic plasticity. It is clear that abnormal CDK5 activation is associated with neuronal apoptosis and death (Weishaupt et al., 2003). Furthermore, CDK5 might also be involved in the abnormal phosphorylation of tau, thereby contributing to the formation of neurofibrillary tangles (Wen et al., 2007), and might be a key protein linking tangle and β-amyloid pathology.
Type 2 Diabetes Besides cerebrovascular disease, Type 2 diabetes (T2D) is the vascular risk factor most consistently associated with AD in observational studies. It is regarded as clearly implicated in disease etiology. T2D nearly doubles the risk of AD (Leibson et al., 1997; Luchsinger et al., 2001; Ott et al., 1999). Several molecular mechanisms might underlie this association. First, diabetes and impairment of glucose tolerance trigger the formation of advanced glycosylation end products (AGEs). Amyloid plaques and NFTs contain receptors for AGEs (RAGEs), and glycation of Aβ enhances its tendency to aggregate (Yamaguchi et al., 2005). In addition, RAGEs may facilitate the neuronal damage caused by Aβ, as the latter is a high-affinity ligand for cell-surface RAGEs. Second, when diabetes is accompanied by hyperinsulinemia, insulin might compete with Aβ for the insulin degrading enzyme (IDE), thereby hindering Aβ clearance from the brain (Craft, 2007). In addition, there is evidence from histopathological studies of hippocampal tissue from AD patients and healthy controls that IDE expression and IDE messenger RNA levels in AD brain tissue from carriers of the APOEe4 allele is reduced compared to cases without APOEe4 alleles or controls, suggesting that IDE may interact with APOE status to affect Aβ metabolism (Cook et al., 2003). Finally, adipose tissue produces cytokines involved in inflammation. Recent genomic studies on AD clearly implicate inflammation as a major etiologic pathway in AD (Lambert et al., 2013).
Blood Pressure The conducted cross- sectional and longitudinal studies examining the effect of late-life blood pressure on cognitive function and dementia have been largely inconsistent (Glynn et al., 1999; Possner et al., 2002; Skoog et al., 1996; Reitz et al., 2007). To some extent these discrepancies can be explained by differences in study design, in particular the age at which blood pressure and the dementia outcome were assessed, as well as variation in the time between
measurement of blood pressure and assessment of cognitive function or dementia. In contrast to the results of studies in late life, data from observational studies assessing the relation between elevated levels of blood pressure in midlife (40–6 0 years of age) and cognitive function in late life have been largely in agreement (Kivipelto et al., 2001; Launer et al., 1995; Swan et al., 1998). In middle-aged individuals, higher blood pressure clearly increases risk of cognitive impairment, dementia, and AD. It is possible that high blood pressure reduces the vascular integrity of the blood–brain barrier, which then leads to protein extravasation into brain tissue causing cell damage, a reduction in neuronal or synaptic function, apoptosis, and an increase in Aβ accumulation. Studies conducted in later life suggest that with increasing age, the effect of elevated blood pressure on AD risk diminishes and may even become inverted, with an increase in blood pressure showing a protective effect in some studies. This observation might be explained by the fact that following the onset of AD, blood pressure begins to decrease, possibly as a result of vessel stiffening, weight loss, and changes in the autonomic regulation of blood flow. The randomized, placebo-controlled trials (RCTs) that have evaluated the benefit of antihypertensive treatments in patients with cognitive impairment have been inconsistent (Forette et al., 2002; Tzourio et al, 2003; Starr et al., 1996; Prince et al., 1996; SHEP Cooperative Research Group, 1991; Lithell et al., 2003) and failed to clarify the effect of blood-pressure-lowering medication on cognitive decline. Additional randomized controlled trials with longer periods of follow-up are needed to clarify this issue.
Plasma Lipid Levels While dyslipidemia increases the risk of vascular disease, which in turn is associated with an increased risk of AD, the published observational study data on the relationship between dyslipidemia and cognitive impairment or AD are conflicting. While some studies observe an association, other studies with similar study design remained negative (Muckle and Roy, 1985; Kuo et al., 1998; Michikawa, 2003; Wieringa et al., 1997; Lesser et al., 2001). In people at risk of cardiovascular and cerebrovascular disease, statins remain the first-line treatments for reducing cholesterol levels. Various RCTs involving participants aged 50–90 years have explored the effect of statins on AD risk ( Jones et al., 2008; Simons et al., 2002; Sparks et al., 2006). Overall, these studies were inconsistent and yielded insufficient evidence for a beneficial effect of statins on AD risk. This observation is in line with a recent Cochrane Database Review, which concluded that statins given in late life to people at risk for vascular disease do not seem to prevent cognitive decline or AD (McGuinness et al., 2016). It is important to note that recent genomic studies on AD clearly implicated lipid metabolism as an etiologic pathway in AD (Lambert et al., 2013). Several lines of evidence indicate that altered brain lipid metabolism may contribute to the pathogenesis of AD. The fact that lipids are ubiquitously present within amyloid plaques has triggered
• DPress ementia Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford680 University USA - OSO, 2018. 15:41:51.
exhaustive investigation of their functional involvement in Aβ generation, clearance, and deposition. Amyloid precursor protein (APP) is proteolytically cleaved by via two routes, the nonamyloidogenic and amyloidogenic pathways. In the amyloidogenic pathway, APP is cleaved by β-(BACE1) and, subsequently γ-secretase to generate neurotoxic Aβ1–40 and Aβ1–42. A significant pool of BACE1 is localized to lipid rafts, mainly through palmitoylation of its transmembrane and cytoplasmic domains. Cholesterol depletion decreases the association of BACE1 with lipid rafts, leading to decreased amyloidogenic processing of APP. In contrast, acute cell exposure to cholesterol promotes the co-clustering of APP and BACE1 in lipid raft domains, their rapid endocytosis, and an increase in APP processing. Core components of the γ-secretase complex, including presenilins, are also associated with lipid rafts, and inhibition of γ-secretase activity leads to the accumulation of APP carboxy-terminal products in lipid rafts. Further, Aβ peptide itself can interact with various lipids and lipid raft components such as gangliosides, phospholipids, and cholesterol, promoting its aggregation on cell membranes and leading to perturbation of membrane integrity and signaling properties. This in turn might subsequently affect intracellular calcium homeostasis and trigger neurotoxic cascades in AD. Finally, there is also evidence that brain lipid metabolism modulates the aggregation of hyperphosphorylated tau. One of the strongest genetic risk factors for late-onset AD is the ɛ4 allele of the ApoE (ApoE4), which is implicated in the transport and delivery of cholesterol in the brain. ApoE is known to interact with Aβ, or compete with it for binding to lipoprotein receptors. It is well established that ApoE can significantly influence Aβ clearance and aggregation in an isoform-dependent manner, and ApoE4 has impaired abilities to clear Aβ in the brain. The protein encoded by the AD risk gene TREM2 (Triggering Receptor Expressed on Myeloid cells 2) might act as a regulator of the microglial response through lipid sensing around senile plaques in an AD mouse model (Wang et al., 2015). The ABC transporter encoded by AD risk gene ABCA7 (ATP Binding Cassette Subfamily A Member 7) is involved in regulating lipid homeostasis, phospholipids, and cholesterol transport across cell membranes to ApoA and ApoE, as well as lipidation of ApoE. ABCA7 is highly expressed in the brain. Overexpression of ABCA7 in cell lines expressing human βAPP resulted in decreased Aβ levels, whereas deletion of ABCA7 impaired Aβ uptake in vitro. A recent study also showed that overexpression of ABCA7 was neuroprotective against AD (Kim et al., 2013), whereas deletion of ABCA7 increased amyloid plaque burden in the brain of βAPP transgenic mice due to reduced phagocytic clearance of Aβ (Kim et al., 2013).
Body Weight Suggesting a U- shaped relationship between weight and cognitive performance (Gufstafson et al., 2003; Razay and Vreugdenhil, 2005; Stewart et al., 2005), prospective studies have linked both low and high body weight to an increased risk of AD and cognitive impairment. The association of body
weight with the risk of AD seems to be driven by central obesity (Tezapsidis et al., 2009) and clearly depends on the age at which body weight is recorded. In addition, there is evidence for reverse causation in the years preceding dementia onset, meaning that cognitive impairment during the prodromal phase of dementia results in the loss of body weight (Gufstafson et al., 2009). In a meta-analysis of 21 epidemiological longitudinal studies in participants without cognitive impairment and aged 30 or over at baseline assessment with at least two years of follow-up, obesity before the age of 65 years increased the risk of AD by 41%, while beyond 65 years a relative risk of 0.83 was observed (Pedditizi et al., 2016).
Metabolic Syndrome Instead of individually exploring the effect of its subcomponents, several studies have assessed the relationship between metabolic syndrome as a whole and the risk of AD or cognitive decline. Most of these investigations demonstrated a positive association between the presence of this syndrome and cognitive dysfunction (Raffaitin et al., 2009; Solfrizzi et al., 2010; Yaffe et al., 2009).
Smoking The relationship between smoking and cognitive decline remains uncertain. The early case–control studies have largely suggested that smoking lowers the risk of AD (Tyas, 1996; Brenner et al., 1993), whereas prospective studies have shown that smoking increases this risk (Merchant et al., 1999; Launer et al., 1999) or has no effect on the probability of developing AD (Doll et al., 2000; Hebert et al., 1992). A meta-analysis that examined the relationship between smoking and AD while accounting for tobacco-industry affiliation found that the combined results of 18 cross-sectional studies without industry affiliations yielded no association. By contrast, data from eight cross-sectional studies with tobacco-industry affiliations suggested that smoking protected against AD. Analysis of 14 cohort studies without tobacco-industry affiliations yielded a significant increase in the risk of AD in smokers (Cataldo et al., 2010). Smoking could affect the risk of AD via several mechanisms. Smoking may increase the generation of free radicals, leading to high oxidative stress, or affect the inflammatory immune system, leading to activation of phagocytes and further oxidative damage (Traber et al., 2000). In addition, smoking may promote cerebrovascular disease. Evidence also exists, however, that smoking can have a protective effect against AD. Nicotine has been suggested to induce an increase in the level of nicotinic acetylcholine receptors, thereby counterbalancing the loss of these receptors and subsequent cholinergic deficits observed in AD.
Depressive Symptoms Depressive symptoms occur in 40%–50% of patients with AD. Some longitudinal and case–control studies have found an increase in the risk of AD or MCI in individuals with a
DS. iagnosis E pidemiology D Charney and Nestler's Neurobiology of Mental Illness, edited by 50. Dennis Charney, et al.,and Oxford University Press USA - OSO,of 2018. 15:41:51.
history of depression ( Jorm, 2001; Barnes et al., 2006), but other studies have been unable to link AD with this mood disorder (Becker et al., 2009; Panza et al., 2008). The potential mechanisms underlying the possible association between these conditions might involve vascular pathways and effects of depression on the hippocampal formation or the hypothalamic–pituitary–adrenal axis.
Traumatic Brain Injury Over the past 30 years, research has linked moderate and severe traumatic brain injury to a greater risk of developing AD. Retrospective studies (Mayeux et al., 1995; Fleminger et al., 2003) suggested that individuals with a history of traumatic brain injury (TBI) had a higher risk of dementia than individuals with no history of such injury. Prospective studies of the relationship between TBI and AD have proved inconsistent (Guo et al., 2000; Mehta et al., 1999; Plassman et al., 2000), but postmortem and experimental studies support a link between these conditions. Evidence also exists that after human brain injury, the extent of Aβ pathology and tau pathology increases in brain tissue, CSF Aβ levels are elevated, and APP is overproduced (Franz et al., 2003). P ROT E C T I VE FAC TO R S
Diet In a largely consistent manner, prospective epidemiologic studies have provided evidence for a beneficial impact of a Mediterranean-type diet (MeDi) on cognitive decline, risk of progression from MCI to AD, and risk of AD. While the Mediterranean diet has heterogeneous characteristics among countries residing in the Mediterranean basin, it is in general characterized by high intake of vegetables, fruits, cereals, pulses, nuts, and seeds; moderate consumption of dairy products, fish, poultry, eggs, and unsaturated fats, such as olive oil as the primary source of monounsaturated fat for cooking and dressing; low to moderate intake of wine during meals; and low intake of red, processed meats and saturated fats. In addition to its effect on clinically measured cognitive impairment and AD, MeDi adherence has also been reported to be associated with less brain atrophy, a reduced risk of stroke, and a reduced risk of depression among older adults (Psaltopoulou et al., 2013).
account the age of the individuals. This finding is in line with an earlier systematic review of 15 longitudinal studies totaling ~34,000 cognitively healthy subjects, which observed that even a low to moderate level of activity was associated with a 35% lower risk of cognitive decline when compared to the sedentary subjects (Sofi et al., 2011).There are several mechanisms through which physical activity could affect cognition. Proposed pathways include increased neurogenesis and neuroplasticity, particularly that associated with brain derived neurotrophic factor (BDNF), improvements in cardiovascular function and the associated influence on the cerebrovascular system, reduction in stress and anxiety, reduced inflammation, and improved insulin sensitivity. Experimental studies conducted in rodents further suggest that physical activity might reduce the rate of amyloid plaque formation.
Intellectual Activity Following initial reports that elderly people with higher levels of education had a lower incidence of dementia than individuals with no education, cognitive activity was suggested to decrease the risk of cognitive decline by increasing cognitive reserve. Several prospective studies subsequently found that both young (Carlson et al., 2008; Fratiglioni and Wang, 2007) and old people who engage in cognitively stimulating activities such as learning, reading, or playing games were less likely to develop dementia than individuals who did not engage in these activities. Some RCTs have shown a beneficial effect of intellectual interventions on cognitive function in elderly dementia-free individuals (Acevedo and Loewenstein, 2007). The benefits of cognitive training seem to be domain specific, however. Several trials found that while cognitive training can improve memory, reasoning, and mental processing speed in older adults, cognitive training did not have an effect on all cognitive domains and did not affect day-to-day functioning (Ball et al., 2002). In addition, one study found that among elderly individuals, those with memory impairment showed less improvement in cognition through memory training than those without such impairment (Unverzagt et al., 2007). Consequently, in elderly people the effect of cognitive training on the risk of dementia is unclear, but several trials are underway.
Physical Activity
C O N C LU S I O N
There is a substantial body of evidence suggesting that physical exercise can promote health and functionality of the central nervous system, including a reduction of age- related cognitive decline and reduction of the risk of cognitive impairment and dementia. A recent meta-analysis of 37 longitudinal studies concluded that there was a negative relationship between physical activity and dementia and cognitive decline (Blondell et al., 2014), specifically a 14% reduction in those with higher levels of physical activity compared to less physically active persons taking into
The described diagnostic criteria, estimates on dementia prevalence and incidence, and summarized data on nongenetic modifiable risk and protective factors reflect the best current basis for planning and allocation of health and welfare resources in dementia care. Future projections of numbers of people with dementia might be modified substantially by preventive interventions lowering incidence, improvements in treatment and care prolonging survival, and disease-modifying interventions preventing or slowing progression.
• DPress ementia Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford682 University USA - OSO, 2018. 15:41:51.
REFERENCES
Guerreiro, R., Wojtas, A., et al. (2013). TREM2 variants in Alzheimer’s disease. N Engl J Med 368(2):117–127. Acevedo, A., and Loewenstein, D.A. (2007). Nonpharmacological cogni- Guo, Z., Cupples, L.A., et al. (2000). Head injury and the risk of AD in the MIRAGE study. Neurology 54(6):1316–1323. tive interventions in aging and dementia. J Geriatr Psychiatry Neurol Gustafson, D., Rothenberg, E., et al. (2003). An 18-year follow-up of 20(4):239–249. overweight and risk of Alzheimer disease. Arch Intern Med 163(13): Albert, M.S., DeKosky, S.T., et al. (2011). The diagnosis of mild cogni1524–1528. tive impairment due to Alzheimer’s disease: recommendations from Gustafson, D.R., Backman, K., et al. (2009). Adiposity indicators and the National Institute on Aging-Alzheimer’s Association workgroups dementia over 32 years in Sweden. Neurology 73(19):1559–1566. on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement Hebert, L.E., Scherr, P.A., et al. (1992). Relation of smoking and alco7(3):270–279. hol consumption to incident Alzheimer’s disease. Am J Epidemiol Alzheimer’s Association. (2011). 2011 Alzheimer’s disease facts and fig135(4):347–355. ures. Alzheimers Dement 7(2):208–244. Ball, K., Berch, D.B., et al. (2002). Effects of cognitive training inter- Hu, W.T., Rippon, G.W., et al. (2009). Alzheimer’s disease and corticobasal degeneration presenting as corticobasal syndrome. Mov Disord ventions with older adults: a randomized controlled trial. JAMA 24(9):1375–1379. 288(18):2271–2281. Hurd, M.D., Martorell, P., et al. (2013). Monetary costs of dementia in the Barnes, D.E., Alexopoulos, G.S., et al. (2006). Depressive symptoms, United States. N Engl J Med 368(14):1326–1334. vascular disease, and mild cognitive impairment: findings from the Hyman, B.T., Phelps, C.H., et al. (2012). National Institute on Aging- Cardiovascular Health Study. Arch Gen Psychiatry 63(3):273–279. Alzheimer’s Association guidelines for the neuropathologic assessBecker, J.T., Chang, Y.F., et al. (2009). Depressed mood is not a risk facment of Alzheimer’s disease. Alzheimers Dement 8(1):1–13. tor for incident dementia in a community-based cohort. Am J Geriatr Jansen, W.J., Ossenkoppele, R., et al. (2015). Prevalence of cerebral amyPsychiatry 17(8):653–663. loid pathology in persons without dementia: a meta-analysis. JAMA Blondell, S.J., Hammersley-Mather, R., Veerman, J.L. (2014). Does phys313(19):1924–1938. ical activity prevent cognitive decline and dementia?: a systematic Jones, R.W., Kivipelto, M., et al. (2008). The Atorvastatin/Donepezil in review and meta-analysis of longitudinal studies. BMC Public Health Alzheimer’s Disease Study (LEADe): design and baseline characteris14:510. tics. Alzheimers Dement 4(2):145–153. Brenner, D.E., Kukull, W.A., et al. (1993). Relationship between cigarette smoking and Alzheimer’s disease in a population-based case-control Jonsson, T., Stefansson, H., et al. (2013). Variant of TREM2 associated with the risk of Alzheimer’s disease. N Engl J Med 368(2):107–116. study. Neurology 43(2):293–300. Cacace, R., Sleegers, K., Van Broeckhoven, C. (2016). Molecular genet- Jorm, A.F. (2001). History of depression as a risk factor for dementia: an updated review. Aust N Z J Psychiatry 35(6):776–781. ics of early-onset Alzheimer’s disease revisited. Alzheimers Dement Kim, W.S., Li, H., et al. (2013). Deletion of Abca7 increases cerebral 12(6):733–748. amyloid-beta accumulation in the J20 mouse model of Alzheimer’s Carlson, M.C., Helms, M.J., et al. (2008). Midlife activity predicts risk of disease. J Neurosci 33(10):4387–4394. dementia in older male twin pairs. Alzheimers Dement 4(5):324–331. Kivipelto, M., Helkala, E.L., et al. (2001). Midlife vascular risk factors Cataldo, J.K., Prochaska, J.J., Glantz, S.A. (2010). Cigarette smoking is a and late-life mild cognitive impairment: a population-based study. risk factor for Alzheimer’s disease: an analysis controlling for tobacco Neurology 56(12):1683–1689. industry affiliation. J Alzheimers Dis 19(2):465–480. Chare, L., Hodges, J.R., et al. (2014). New criteria for frontotemporal Kuo, Y.M., Emmerling, M.R., et al. (1998). Elevated low-density lipoprotein in Alzheimer’s disease correlates with brain abeta 1-42 levels. dementia syndromes: clinical and pathological diagnostic implicaBiochem Biophys Res Commun 252(3):711–715. tions. J Neurol Neurosurg Psychiatry 85(8):865–870. Lambert, J.C., Ibrahim-Verbaas, C.A., et al. (2013). Meta-analysis of Cook, D.G., Leverenz, J.B., et al. (2003). Reduced hippocampal insulin- 74,046 individuals identifies 11 new susceptibility loci for Alzheimer’s degrading enzyme in late-onset Alzheimer’s disease is associated with disease. Nat Genet 45(12):1452–1458. the apolipoprotein E-epsilon4 allele. Am J Pathol 162(1):313–319. Craft, S. (2007). Insulin resistance and Alzheimer’s disease pathogen- Launer, L.J., Andersen, K., et al. (1999). Rates and risk factors for dementia and Alzheimer’s disease: results from, EURODEM pooled analyses. esis: potential mechanisms and implications for treatment. Curr EURODEM Incidence Research Group and Work Groups. European Alzheimer Res 4(2):147–152. Studies of Dementia. Neurology 52(1):78–84. Crutch, S.J., Schott, J.M., et al. (2013). Shining a light on posterior cortical Launer, L.J., Masaki, K., et al. (1995). The association between midlife atrophy. Alzheimers Dement 9(4):463–465. blood pressure levels and late-life cognitive function. The Honolulu- Doll, R., Peto, R., et al. (2000). Smoking and dementia in male British Asia Aging Study. JAMA 274(23):1846–1851. doctors: prospective study. BMJ 320(7242):1097–1102. Leibson, C.L., Rocca, W.A., et al. (1997). The risk of dementia among perFerri, C.P., Prince, M., et al. (2005). Global prevalence of dementia: a sons with diabetes mellitus: a population-based cohort study. Ann N Y Delphi consensus study. Lancet 366(9503):2112–2117. Acad Sci 826:422–427. Fleminger, S., Oliver, D.L., et al. (2003). Head injury as a risk factor for Alzheimer’s disease: the evidence 10 years on; a partial replication. J Lesser, G., Kandiah, K., et al. (2001). Elevated serum total and LDL cholesterol in very old patients with Alzheimer’s disease. Dement Geriatr Neurol Neurosurg Psychiatry 74(7):857–862. Cogn Disord 12(2):138–145. Folstein, M.F., Folstein, S.E., and McHugh, P.R. (1975). “Mini-mental Lithell, H., Hansson, L., et al. (2003). The Study on Cognition and state”. A practical method for grading the cognitive state of patients for Prognosis in the Elderly (SCOPE): principal results of a randomized the clinician. J Psychiatr Res 12(3):189–198. double-blind intervention trial. J Hypertens 21(5):875–886. Forette, F., Seux, M.L., et al. (2002). The prevention of dementia with antihypertensive treatment: new evidence from the Systolic Hypertension Luchsinger, J.A., Tang, M.X., et al. (2001). Diabetes mellitus and risk of Alzheimer’s disease and dementia with stroke in a multiethnic cohort. in Europe (Syst-Eur) study. Arch Intern Med 162(18):2046–2052. Am J Epidemiol 154(7):635–641. Franz, G., Beer, R., et al. (2003). Amyloid beta 1-42 and tau in cerebrospinal Manton, K.C., Gu, X.L., Ukraintseva, S.V. (2005). Declining prevafluid after severe traumatic brain injury. Neurology 60(9):1457–1461. lence of dementia in the U.S. elderly population. Adv Gerontol 16: Fratiglioni, L., and Wang, H.X. (2007). Brain reserve hypothesis in 30–37. dementia. J Alzheimers Dis 12(1):11–22. Glynn, R.J., Beckett, L.A., et al. (1999). Current and remote blood pres- Mayeux, R., Ottman, R., et al. (1995). Synergistic effects of traumatic head injury and apolipoprotein-epsilon 4 in patients with Alzheimer’s dissure and cognitive decline. JAMA 281(5):438–445. ease. Neurology 45(3 Pt 1):555–557. Gorno-Tempini, M.L., Brambati, S.M., et al. (2008). The logopenic/ phonological variant of primary progressive aphasia. Neurology McGuinness, B., Craig, D., et al. (2016). Statins for the prevention of dementia. Cochrane Database Syst Rev 2016(1):CD003160. 71(16):1227–1234. D S. iagnosis E pidemiology D Charney and Nestler's Neurobiology of Mental Illness, edited by 50. Dennis Charney, et al.,and Oxford University Press USA - OSO,of 2018. 15:41:51.
McKeith, I., Mintzer, J., et al. (2004). Dementia with Lewy bodies. Lancet Neurol 3(1):19–28. McKhann, G., Drachman, D., et al. (1984). Clinical diagnosis of Alzheimer’s disease: report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology 34(7):939–944. McKhann, G.M., Knopman, D.S., et al. (2011). The diagnosis of dementia due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement 7(3):263–269. Mehta, K.M., Ott, A., et al. (1999). Head trauma and risk of dementia and Alzheimer’s disease: The Rotterdam Study. Neurology 53(9): 1959–1962. Merchant, C., Tang, M.X., et al. (1999). The influence of smoking on the risk of Alzheimer’s disease. Neurology 52(7):1408–1412. Michikawa, M. (2003). Cholesterol paradox: is high total or low HDL cholesterol level a risk for Alzheimer’s disease? J Neurosci Res 72(2):141–146. Muckle, T.J., and Roy, J.R. (1985). High-density lipoprotein cholesterol in differential diagnosis of senile dementia. Lancet 1(8439):1191–1193. Okamura, N., Harada, R., et al. (2016). Advances in the development of tau PET radiotracers and their clinical applications. Ageing Res Rev 30:107–113. Ossenkoppele, R., Pijnenburg, Y.A., et al. (2015). The behavioural/dysexecutive variant of Alzheimer’s disease: clinical, neuroimaging and pathological features. Brain 138(Pt 9):2732–2749. Ott, A., Stolk, R.P., et al. (1999). Diabetes mellitus and the risk of dementia: The Rotterdam Study. Neurology 53(9):1937–1942. Panza, F., Capurso, C., et al. (2008). Impact of depressive symptoms on the rate of progression to dementia in patients affected by mild cognitive impairment. The Italian Longitudinal Study on Aging. Int J Geriatr Psychiatry 23(7):726–734. Pedditizi, E., Peters, R., Beckett, N. (2016). The risk of overweight/obesity in mid-life and late life for the development of dementia: a systematic review and meta-analysis of longitudinal studies. Age Ageing 45(1):14–21. Plassman, B.L., Havlik, R.J., et al. (2000). Documented head injury in early adulthood and risk of Alzheimer’s disease and other dementias. Neurology 55(8):1158–1166. Posner, H.B., Tang, M.X., et al. (2002). The relationship of hypertension in the elderly to AD vascular dementia and cognitive function. Neurology 58(8):1175–1181. Prince, M.J., Bird, A.S., et al. (1996). Is the cognitive function of older patients affected by antihypertensive treatment? Results from 54 months of the Medical Research Council’s trial of hypertension in older adults. BMJ 312(7034):801–805. Psaltopoulou, T., Sergentanis, T.N., et al. (2013). Mediterranean diet, stroke, cognitive impairment, and depression: A meta-analysis. Ann Neurol 74(4):580–591. Raffaitin, C., Gin, H., et al. (2009). Metabolic syndrome and risk for incident Alzheimer’s disease or vascular dementia: the Three-City Study. Diabetes Care 32(1):169–174. Ramirez-Bermudez, J. (2012). Alzheimer’s disease: critical notes on the history of a medical concept. Arch Med Res 43(8):595–599. Razay, G., and Vreugdenhil, A. (2005). Obesity in middle age and future risk of dementia: midlife obesity increases risk of future dementia. BMJ 331(7514):455; author reply. Reitz, C., Tang, M.X., Manly, J., et al. (2007). Hypertension and the risk of mild cognitive impairment. Arch Neurol 64(12):1734–1740. Satizabal, C.L., Beiser, A.S., et al. (2016). Incidence of dementia over three decades in the Framingham Heart Study. N Engl J Med 374(6):523–532. Savica, R., Grossardt, B.R., et al. (2013). Incidence of dementia with Lewy bodies and Parkinson disease dementia. JAMA Neurol 70(11):1396–1402. SHEP Cooperative Research Group. (1991). Prevention of stroke by antihypertensive drug treatment in older persons with isolated systolic hypertension. Final results of the Systolic Hypertension in the Elderly Program (SHEP). JAMA 265(24):3255–3264. Simons, M., Schwarzler, F., et al. (2002). Treatment with simvastatin in normocholesterolemic patients with Alzheimer’s disease: A 26-week
randomized, placebo- controlled, double- blind trial. Ann Neurol 52(3):346–350. Skoog, I., Lernfelt, B., et al. (1996). 15-year longitudinal study of blood pressure and dementia. Lancet 347(9009):1141–1145. Sofi, F., Valecchi, D., et al. (2011). Physical activity and risk of cognitive decline: a meta-analysis of prospective studies. J Intern Med 269(1):107–117. Solfrizzi, V., Scafato, E., et al. (2010). Metabolic syndrome and the risk of vascular dementia: the Italian Longitudinal Study on Ageing. J Neurol Neurosurg Psychiatry 81(4):433–440. Sousa, R.M., Ferri, C.P., et al. (2009). Contribution of chronic diseases to disability in elderly people in countries with low and middle incomes: a 10/66 Dementia Research Group population-based survey. Lancet 374(9704):1821–1830. Sousa, R.M., Ferri, C.P., et al. (2010). The contribution of chronic diseases to the prevalence of dependence among older people in Latin America China and India: a 10/66 Dementia Research Group population- based survey. BMC Geriatr 10:53. Sparks, D.L., Connor, D.J., et al. (2006). Circulating cholesterol levels, apolipoprotein E genotype and dementia severity influence the benefit of atorvastatin treatment in Alzheimer’s disease: results of the Alzheimer’s disease cholesterol-lowering treatment (ADCLT) trial. Acta Neurol Scand Suppl 185:3–7. Starr, J.M., Whalley, L.J., Deary, I.J. (1996). The effects of antihypertensive treatment on cognitive function: results from the HOPE study. J Am Geriatr Soc 44(4):411–415. Stewart, R., Masaki, K., et al. (2005). A 32-year prospective study of change in body weight and incident dementia: the Honolulu-Asia Aging Study. Arch Neurol 62(1):55–60. Swan, G.E., Carmelli, D., Larue, A. (1998). Systolic blood pressure tracking over 25 to 30 years and cognitive performance in older adults. Stroke 29(11):2334–2340. Tezapsidis, N., Smith, M.A., Ashford, J.W. (2009). Central obesity and increased risk of dementia more than three decades later. Neurology 72(11):1030–1031; author reply 1. Traber, M.G., van der Vliet, A., et al. (2000). Tobacco-related diseases. Is there a role for antioxidant micronutrient supplementation? Clin Chest Med 21(1):173–187, x. Tyas, S.L. (1996). Are tobacco and alcohol use related to Alzheimer’s disease? A critical assessment of the evidence and its implications. Addict Biol 1(3):237–254. Tzourio, C., Anderson, C., et al. (2003). Effects of blood pressure lowering with perindopril and indapamide therapy on dementia and cognitive decline in patients with cerebrovascular disease. Arch Intern Med 163(9):1069–1075. Unverzagt, F.W., Kasten, L., et al. (2007). Effect of memory impairment on training outcomes in ACTIVE. J Int Neuropsychol Soc 13(6): 953–960. Wang, Y., Cella, M., et al. (2015). TREM2 lipid sensing sustains the microglial response in an Alzheimer’s disease model. Cell 160(6): 1061–1071. Watson, R., and Colloby, S.J. (2016). Imaging in dementia with Lewy bodies: an overview. J Geriatr Psychiatry Neurol 29(5):254–260. Weishaupt, J.H., Kussmaul, L., et al. (2003). Inhibition of CDK5 is protective in necrotic and apoptotic paradigms of neuronal cell death and prevents mitochondrial dysfunction. Mol Cell Neurosci 24(2):489–502. Wen, Y., Yang, S.H., et al. (2007). Cdk5 is involved in NFT-like tauopathy induced by transient cerebral ischemia in female rats. Biochim Biophys Acta 1772(4):473–483. Wieringa, G.E., Burlinson, S., et al. (1997). Apolipoprotein E genotypes and serum lipid levels in Alzheimer’s disease and multi-infarct dementia. Int J Geriatr Psychiatry 12(3):359–362. Yaffe, K., Weston, A.L., et al. (2009). The metabolic syndrome and development of cognitive impairment among older women. Arch Neurol 66(3):324–328. Yamagishi, S., Nakamura, K., et al. (2005). Serum or cerebrospinal fluid levels of glyceraldehyde-derived advanced glycation end products (AGEs) may be a promising biomarker for early detection of Alzheimer’s disease. Med Hypotheses 64(6):1205–1207.
• DPress ementia Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford684 University USA - OSO, 2018. 15:41:51.
51. GENETICS OF DEMENTIA Alan E. Renton and Alison M. Goate
INTRODUCTION Dementia is defined as cognitive impairment severe enough to impair daily life. Dementia is a central phenotypic feature of several progressive and fatal neurodegenerative disorders: Alzheimer’s disease (AD), frontotemporal dementia (FTD), Parkinson’s disease dementia (PDD), dementia with Lewy bodies (DLB), progressive supranuclear palsy (PSP), corticobasal degeneration (CBD), lysosomal storage diseases (LSDs), leukodystrophies, and transmissible spongiform encephalopathies (TSEs). These conditions are characterized by the age-dependent accumulation of central nervous system protein aggregates, many of which are encoded by genes that drive disease risk and lend their names to neuropathological diagnoses (e.g., amyloidosis, tauopathy, synucleinopathy). Most dementia cases are sporadic and complex, in that they occur randomly within the community due to the delicate interplay of multiple genetic variants and environmental factors. But a subset of affected individuals display a positive family history, and many of these familial cases exhibit Mendelian inheritance patterns caused by highly penetrant disease- segregating alleles in a single gene (i.e., pathogenic mutations). Due to the aging global population, dementia prevalence is set to increase significantly through the 21st century and this surge will disproportionately impact developing countries. This chapter summarizes published genetics literature for the most important neurodegenerative dementias. Early 21st century neurogenetics is a rapidly moving field undergoing seismic shifts as it matures in the post-genomics era. Our intention is to focus on the most salient findings, both classical and cutting edge, in order to provide a clear synthesis for students of medicine and the neurosciences. This overview will not cover every disease, nor will it be an exhaustive account of the selected disorders. We will use representative examples to describe the fundamentals of dementia genetics and illuminate the big picture. Our aim is to empower the reader to dive more deeply into the most stimulating areas, and we suggest starting with several recent reviews (Collins and Gray, 2016; Cuyvers and Sleegers, 2016; Götzl et al., 2016; Hernandez et al., 2016; Karch et al., 2014; Kobayashi et al., 2015; Lloyd and Collinge; 2013; Lloyd- Evens and Haslett, 2016; Mackenzie and Neumann, 2016; Schmitz et al., 2016; Scholz and Bras, 2015; Singleton and Hardy, 2016; Weishaupt et al., 2016).
T H E G E N ET I C A R C H I T E C T U R E OF DEMENTIA A vast literature demonstrates that the genetic architecture of human disease comprises risk and protective alleles spanning a range of population frequencies and effect sizes. This idea was crystallized into an elegant framework by Manolio and colleagues (2009), and we will use that to structure our discussion of dementia genetics. Modern human disease genetics began in the 1980s with the linkage era. Rare alleles (population minor allele frequency [MAF] < 0.01) of large effect size were demonstrated to segregate with disease in multiplex Mendelian pedigrees (e.g., Amyloid Beta Precursor Protein [APP]). Despite their sparse coverage, microsatellite markers are scattered genome- wide, enabling relatively unbiased detection of linkage between their genotypes and the phenotypic trait, followed by positional cloning and Sanger sequencing to isolate the pathogenic mutation. Increased application of linkage analysis facilitated the identification of common alleles (population MAF > 0.05) with large effect size (e.g., Apolipoprotein E [APOE]). The genome-wide association study (GWAS) era dawned in the mid-2000s. Association analysis of increasingly large case-control complex disease cohorts established a role for common alleles (population MAF > 0.05) of small effect size (e.g., Bridging Integrator 1 [BIN1]). This systematic approach relies on relatively unbiased genome-wide microarrays that genotype thousands of densely distributed single nucleotide variant (SNV) markers. Twin studies have been used to estimate narrow-sense heritability (h2), which is the proportion of phenotypic variation due to additive genetic factors. However, it became clear that for numerous complex traits, significant genetic loci identified in the largest GWASs only explain a small proportion of this heritability, and the disparity was termed the missing heritability problem (Manolio et al., 2009). The sequencing era, which began in the late 2000s, was spurred on by technological development and the missing heritability problem. The revolutionary rise of second generation sequencing (such as short read exome, genome, and targeted sequencing) has evolved the enterprise, enabling identification of low frequency (0.01 < population MAF < 0.05) and rare
6 8 5 USA - OSO, 2018. Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press 15:41:51.
(population MAF < 0.01) alleles with moderate effect size (e.g., Triggering Receptor Expressed On Myeloid Cells 2 [TREM2]). Despite being in their infancy, these studies are rapidly generating a growing body of evidence indicating that low frequency and rare variation contribute to the genetic architecture of human disease. A L Z H E I M E R’S D I S E A S E
Alzheimer’s disease, the most common form of neurodegenerative dementia, is a progressive and fatal illness typified by deficits in memory, problem solving, and language. Neuropathologically it is characterized by neuronal loss, cortical atrophy, gliosis, lipid granules, and the presence of two protein aggregate classes: extracellular amyloid plaques (containing β-amyloid [Aβ], a cleavage product of APP protein) and intracellular neurofibrillary tangles (containing hyperphosphorylated tau, which is encoded by Microtubule Associated Protein Tau [MAPT]). Hence AD is thought of as both an amyloidosis and a tauopathy (Cuyvers and Sleegers, 2016). Based on observed inheritance patterns, AD is divided into Mendelian familial (autosomal dominant and autosomal recessive), non-Mendelian familial, and sporadic. The majority of cases are sporadic, followed by non-Mendelian familial, with Mendelian familial accounting for only ~1% of AD. Based on symptomatic presentation with the cutoff generally at 65 years, cases are labeled as either early-onset Alzheimer’s disease (EOAD) or late-onset Alzheimer’s disease (LOAD). Mendelian familial AD is skewed toward early onset, whereas non-Mendelian familial and sporadic AD tend to be late onset (Cuyvers and Sleegers, 2016). It is well understood that AD risk is driven by a substantial genetic component, but despite notable progress a significant proportion of this genetic architecture remains unresolved. The largest twin study examined 392 elderly Swedish pairs with at least one affected member. When shared environmental factors are considered, it estimated h2 (i.e., “twin heritability”) as 0.58 (95% confidence interval [CI] = 0.19 –0.87) (Gatz et al., 2006). However, this is probably an underestimate, as longitudinal follow up tends to show that some discordant twins become concordant over time. Maximum likelihood analysis of GWAS datasets can assess the additive heritability attributable to genotyped variants on a genome-wide scale, known as hg2 (i.e., “chip heritability”). This approach was recently applied to Caucasian non-Hispanic LOAD data that had been imputed with 1000 Genomes for dense coverage of common and low frequency alleles (AD = 3877; controls = 5822). The analysis estimated LOAD hg2 as 0.53 (standard error [SE] = 0.04). Within this genetic risk signal, 0.37 (SE = 0.04) was explained by unknown variation, with 0.22 (SE = 0.04) of that residing outside of loci currently implicated by genome-wide association or sequencing studies (Ridge et al., 2016). The largest published LOAD GWAS was sufficiently powered to find the majority of common variants with low but appreciable effect (Lambert et al., 2013). Hence much of the unknown AD genetic architecture is most likely low frequency/rare alleles with low to moderate effect, which will be amenable
to large sequencing studies; and numerous common variants, each making a very small contribution, which will be difficult to ever conclusively prove. In addition, other genetic factors inadequately captured by hg2 may play a role, and several are active areas of investigation, such as these overlapping categories: rare or extremely rare alleles, structural variation, de novo variation, aneuploidy, somatic mosaicism, and multiplicative effects (e.g., gene–gene [i.e., epistatic] or gene–environment interactions). It remains unclear to what extent the situation differs across populations, and large studies of underrepresented minorities are greatly needed. Moreover, we have not touched on strictly nongenetic factors that could influence AD susceptibility, such epigenetics or the environment, but those are beyond the scope of this discussion. In summary, the genetic architecture of AD is polygenic and complex. Some of the overall genetic risk burden is now captured by known alleles demonstrating association or segregation. But the remainder is most likely constructed from a constellation of unknown variants with effect sizes ranging from moderate to extremely small. FRO N TOT E M P O R A L D E M E N T I A
Frontotemporal dementia, the third most common neurodegenerative dementia, is typified by combinatorial changes in behavior, personality, and language. Familial and sporadic FTD are of approximately equal prevalence, and onset is usually late. This progressive and fatal disorder is clinically divided into behavior-variant frontotemporal dementia (bvFTD) and primary progressive aphasia (PPA), with the latter split into nonfluent (nfvPPA) and semantic (svPPA) variants. Characteristic neuropathological changes include neuronal loss, gliosis, intracellular protein aggregates, and frontal and temporal atrophy; clinical FTD is associated with the neuropathological diagnosis frontotemporal lobar degeneration (FTLD) (Mackenzie and Neumann, 2016). Depending on the identity of the predominant accumulated protein (in parentheses), FTLD is classified into at least three subtypes: FTLD-TDP (transactive response DNA-binding protein [TDP-43]), FTLD-tau (tau), and FTLD-FET (fused in sarcoma [FUS], Ewing’s sarcoma [EWS], TATA-binding protein-associated factor 15 [TAF15]). By far the most common subtypes are FTLD-TDP (~50% of cases) and FTLD- tau (~40% of cases). Significant clinical, neuropathological, and genetic overlap exists between FTD and the neuromuscular condition amyotrophic lateral sclerosis (ALS). Indeed, many investigators consider these two neurodegenerative disorders as part of the same disease spectrum, known as either FTD-ALS or ALS-FTD (Mackenzie and Neumann, 2016). PA R K I NS O N ’S D I S E A S E , L EWY B O DY D E M E N T I A , A N D AT Y P I C A L PA R K I NS O N I S M
Parkinson’s disease, the most common neurodegenerative movement disorder, is characterized clinically by bradykinesia, resting tremor, muscular rigidity, and postural instability (symptoms collectively known as parkinsonism). Onset tends to be late, and most cases are sporadic. The neuropathological
• DPress ementia Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford686 University USA - OSO, 2018. 15:41:51.
hallmarks of this progressive and fatal illness are loss of dopaminergic neurons in the substantia nigra pars compacta, gliosis, and widespread subcortical and cortical intracellular protein aggregates called Lewy bodies (containing α-synuclein, which is encoded by Synuclein Alpha [SNCA]). Hence PD is known as a synucleinopathy (Hernandez et al., 2016). Meta-analysis of Caucasian non-Hispanic GWAS data estimated PD hg2 as 0.27 (95% CI = 0.17 –0.38) (PD = 7,096; controls = 19,455). Known genome-wide significant loci explain about one-tenth of this, suggesting that much additive genetic architecture remains undiscovered (Keller et al., 2012). Although PD is classically defined by its motor symptoms, cognitive impairment occurs frequently, and if sufficiently severe leads to a diagnosis of PDD. The related condition DLB is the second most common neurodegenerative dementia, and this disorder is largely late-onset sporadic. It is characterized by parkinsonism, dementia, visual hallucinations, substantia nigra neuronal loss, and Lewy bodies. Collectively known as Lewy body dementia (LBD), the synucleinopathies PDD and DLB involve heterogeneous mixtures of motor and cognitive features, and their ideal nosological relationship is a matter of debate. Furthermore, most DLB patients also exhibit amyloid plaques and neurofibrillary tangles. These overlapping features support a continuous clinicopathological framework where PDD and DLB sit on a spectrum between PD and AD (Scholz and Bras, 2015). Analysis of Caucasian non-Hispanics recently estimated DLB hg2 as 0.31 (SE = 0.03) (DLB = 788; controls = 1403), but this value should be considered preliminary until larger cohorts are investigated (Guerreiro et al., 2016). Atypical parkinsonism, such as the fatal neurodegenerative movement disorders PSP and CBD, also contributes to dementia burden. The vast majority of PSP and CBD cases are sporadic and late onset. Progressive supranuclear palsy is typified by gait impairment, parkinsonism, ataxia, slow vertical saccades, pseudobulbar palsy, cognitive dysfunction, and intracellular tau-positive neurofibrillary tangles. Corticobasal degeneration is characterized by parkinsonism, dystonia, myoclonus, apraxia, cognitive impairment, and intracellular tau-positive plaques. Hence PSP and CBD are classed as tauopathies. In addition, subcortical and cortical atrophy is observed in both conditions (Scholz and Bras, 2015). LY S O S O M A L S TO R AG E D I S E A S E S A N D L EU KO DY S T RO P H I E S
Lysosomal storage diseases are a collection of rare conditions typified by accumulated macromolecules resulting from defective lysosomes. Many LSDs are fatal child-onset monogenic recessive disorders caused by highly penetrant biallelic mutations (i.e., homozygous or compound heterozygous) whose phenotypes include neurodegeneration, dementia, dyskinesia, ataxia, and sensory loss. Well-known examples are Gaucher’s disease (GD), neuronal ceroid lipofuscinosis (NCL), and Niemann-Pick type C (Lloyd-Evans and Haslett, 2016). Leukodystrophies are a group of rare neurodegenerative diseases defined by brain demyelination. Many leukodystrophies are fatal young-onset monogenic recessive conditions,
with phenotypes such as dementia, parkinsonism, seizures, and sensory loss. Examples include Nasu- Hakola disease (NHD), leukoencephalopathy with vanishing white matter, and Canavan disease (Mackenzie and Neumann, 2016). T R A NS M I S S I B L E S P O N G I F O R M E N C E P H A L O PAT H I E S
TSEs, also known as prion diseases, are a family of fatal and extremely rare neurodegenerative disorders. Their neuropathological characteristics include neuronal loss, spongiosis, gliosis, and aggregation of the prion protein (which is encoded by Prion Protein [PRNP]) misfolded from its normal (PrpC) into its pathogenic (PrpSc) conformation. Several TSEs have been described, such as Creutzfeldt-Jakob disease (CJD), Gerstmann-Sträussler-Scheinker syndrome (GSS), fatal familial insomnia (FFI), and kuru. Clinical symptoms encompass memory impairment, confusion, aphasia, ataxia, apraxia, myoclonus, parkinsonism, autonomic dysfunction, sleep disturbance, spatial disorientation, and hallucinations. The majority of cases are late-onset sporadic (Lloyd et al., 2013; Schmitz et al., 2016). The etiology of TSEs can be Mendelian (e.g., familial Creutzfeldt-Jakob disease [fCJD]), sporadic (e.g., sporadic Creutzfeldt-Jakob disease [sCJD]), or acquired through exposure to the PrpSc protein infectious agent (e.g., variant Creutzfeldt-Jakob disease [vCJD]). Acquired TSEs have been attributed to iatrogenic events, for example iatrogenic CJD (iCJD) caused by accidental transfusion of infected blood, as well as cultural practices, such as vCJD resulting from dietary exposure to livestock affected with the TSE bovine spongiform encephalopathy, or kuru, caused by endocannabilistic consumption of infected brain tissue during Papua New Guinean mortuary feasts (Lloyd and Collinge, 2013; Schmitz et al., 2016). The pathogenesis of TSEs involves the misfolding and polymerization of PrpC initiated by PrpSc seeds (i.e., permissive templating). This groundbreaking observation, the first of its kind in neurodegenerative disease, was highly influential on the field. Mechanisms involving “prion- like” cell–cell seeding and permissive templating have subsequently been proposed to explain the progressive deposition of aggregated protein that defines other neuropathological diagnoses (e.g., amyloidosis, tauopathy, and synucleinopathy) (Lloyd and Collinge, 2013; Schmitz et al., 2016). R ARE ALLELES WITH HIGH EFFECT SIZE AU TO S O M A L D O M I NA N T A N D AU TO S O M A L R EC E S S I VE A L Z H E I M E R’S D I S E A S E : A PP, PS E N1, PS E N2
The discovery that rare APP, Presenilin 1 (PSEN1), and Presenilin 2 (PSEN2) alleles are highly penetrant in autosomal dominant AD kindreds from several populations identified the first genes linked to this disorder (Goate et al., 1991; Levy-Lahad et al., 1995; Rogaev et al., 1995; Sherrington et al., 1995). Co-segregating pathogenic mutations in these three
GOxford enetics D USA ementia Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney,51. et al., Universityof Press - OSO, 2018.• 15:41:51.
genes explain almost all known autosomal dominant EOAD pedigrees, with PSEN1 contributing significantly more disease burden (~80%) than APP (~14%) or PSEN2 (~5%). The majority of EOAD APP alleles are dominant heterozygous missense mutations located in or near the Aβ domain (e.g., Val717Ile [a variant that is absent from ExAC]). However, dominant whole gene duplication mutations, recessive homozygous missense mutations (e.g., Ala673Val [absent from ExAC]), and de novo variants have also been detected in EOAD (Karch et al., 2014). Dominant heterozygous EOAD PSEN1 and PSEN2 mutations are scattered throughout these genes, with some clustering in their transmembrane domains. Interestingly, sequencing studies investigating multiplex European-, Hispanic-, and African-American LOAD families have discovered APP, PSEN1, and PSEN2 partially penetrant risk variants (e.g., PSEN1 Glu318Gly [ExAC non-Finnish European MAF = 0.021]) and/or segregating mutations, and sequencing analysis of Icelandic LOAD identified an APP Ala673Thr variant (ExAC non-Finnish European MAF = 5.39 x 10−4) that protects against disease (Karch et al., 2014), indicating that these three loci also harbor rare and low frequency alleles of moderate effect size. Based on genetic, biochemical, and neuropathological evidence, the amyloid hypothesis posits that Aβ aggregation is critical for instigating AD pathogenesis. Central to this theory is APP proteolysis. The bulk of APP is processed via the anti- amyloidogenic pathway, which involves sequential cleavage by α-then γ-secretase to produce secreted amyloid precursor protein-α (sAPPα), p3, and amyloid precursor protein intracellular domain (AICD). However, APP can also undergo the mutually exclusive amyloidogenic pathway: sequential proteolysis by β-then γ-secretase, generating secreted amyloid precursor protein-β (sAPPβ), Aβ peptides, and AICD (Karch et al., 2014) (see Gan et al. for more details on Chapter 54). Some APP mutations enhance total Aβ levels, such as missense alleles that alter β-secretase activity or duplications that increase APP gene dosage and expression. Furthermore, the integral membrane proteins PSEN1 and PSEN2 are essential components of the γ-secretase complex. Presenilin mutations modify γ-secretase activity via several biochemical mechanisms that impact the efficiency of Aβ aggregation (Karch et al., 2014). Hence in the context of the amyloid hypothesis, pathogenic APP, PSEN1, and PSEN2 alleles demonstrate the importance of APP processing and/or Aβ aggregation to AD pathophysiology. AU TO S O M A L D O M I NA N T F RO N TOT E M P O R A L D E M E N T I A : C9O RF72 , GRN, MA PT
The heterozygous Chromosome 9 Open Reading Frame 72 (C9orf72) repeat expansion mutation co-segregates in multiple European ancestry pedigrees afflicted with autosomal dominant FTD and/or ALS. The nature of this mutation is massive expansion of a noncoding GGGGCC hexanucleotide, and affected individuals carry thousands of repeats. In European descent populations, the expansion is the most frequent cause of not only familial FTD and ALS, but also the sporadic forms of these disorders (DeJesus-Hernandez et al.,
2011; Renton et al., 2011). Building on previous clinicopathological and genetic evidence, this discovery cemented the nascent notion that these conditions are not separate but part of the same FTD-ALS disease spectrum. Indeed, the expansion gives rise to considerable phenotypic heterogeneity. Age at onset is wide-ranging, and clinical outcomes can vary even within the same family. Neuropathological characteristics of C9orf72-linked FTD include FTLD-TDP, intracellular TDP-43-negative dipeptide repeat protein aggregates, and intracellular RNA inclusions containing C9orf72 expanded repeat transcripts and RNA-binding proteins (Mackenzie and Neumann, 2016). Highly penetrant Granulin (GRN) alleles constitute the second largest cause of familial FTD in populations of European descent (Baker et al., 2006; Cruts et al., 2006). Almost all FTD-segregating GRN mutations are autosomal dominant, heterozygous, and loss of function (LOF) (i.e., nonsense, splice site, or frameshift [also known as disruptive]). Clinical presentation is heterogeneous even within the same family, encompassing bvFTD, nfvPPA, and moderate parkinsonism. However, the neuropathological pattern is consistently FTLD-TDP (Mackenzie and Neumann, 2016). Mutations in MAPT co-segregate in multiple European and Japanese ancestry autosomal dominant pedigrees displaying FTD with and without parkinsonism (Hutton et al., 1998). Most penetrant MAPT alleles are dominant heterozygous missense, deletion, or splice site mutations, and many are clustered in the microtubule binding repeats domain. Affected individuals develop behavioral or personality changes, cognitive dysfunction, atypical parkinsonism, and FTLD-tau (Mackenzie and Neumann, 2016). Moreover, sequencing studies have identified GRN and MAPT segregating mutations and/or partially penetrant risk variants in clinically diagnosed LOAD families. Such cases most likely represent misdiagnosed FTD, nevertheless it is clear these loci also harbor rare alleles of moderate effect size (Karch et al., 2014). Taken together, these findings demonstrate that pathogenic mutations in a particular gene can result in phenotypic pleiotropy (i.e., disparate clinical outcomes). Despite accumulating insight, it remains unclear how mutations in C9orf72, GRN, and MAPT cause disease. The C9orf72 repeat expansion appears to drive multiple pathogenic mechanisms, both gain and loss of function. In vitro and in vivo experimental evidence already implicates defects in RNA metabolism, nucleocytoplasmic shuttling, the autophagosome- lysosome system, and the ubiquitin- proteasome system (Götzl et al., 2016). Given the unpredictable consequences of inserting large amounts of GC-rich DNA, it’s probable that additional effects on cellular physiology await discovery. The full picture of C9orf72-linked neurodegeneration will likely describe a rich and complicated pathomechanistic heterogeneity whose elucidation may explain the extensive clinical variability. Granulin is a secreted growth factor involved in inflammation, neuroprotection, and wound repair, and most FTD-segregating GRN mutations reduce mRNA and/or protein levels in patient blood and/ or cerebrospinal fluid (CSF), causing haploinsufficiency (i.e., functional impairment due to loss of gene or protein expression from the variant allele). Interestingly, several lines of evidence
• DPress ementia Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford688 University USA - OSO, 2018. 15:41:51.
indicate GRN deficiency may impact the autophagosome- lysosome system. A homozygous frameshift GRN mutation segregates with the LSD NCL in one family, and GRN-linked FTD cases and knockout mouse models exhibit elevated levels of lysosomal marker proteins in their brains Götzl et al., 2016). Tau stabilizes and binds microtubules. This protein is hyperphosphorylated and aggregated in AD neurofibrillary tangles and FTLD-tau inclusions. Studies show that many pathogenic missense or splice site MAPT alleles can alter tau aggregation efficiency and microtubule binding activity, with potential impacts on inclusion burden, vesicular transport, and the autophagosome-lysosome system (Götzl et al., 2016; see Gan et al. for more details on Chapter 54). In summary, research suggests that autophagosome-lysosome impairment is a recurrent theme underlying the death of frontotemporal cortical neurons. AU TO S O M A L D O M I NA N T PA R K I N S O N ’S D I S E A S E , L EWY B O DY D E M E N T I A , A N D AT Y P I C A L PA R K I N S O N I S M : S NC A
Highly penetrant alleles in several genes, such as Leucine-Rich Repeat Kinase 2 (LRRK2), Parkin RBR E3 Ubiquitin Protein Ligase (PARK2), Parkinsonism Associated Deglycase (PARK7), and PTEN Induced Putative Kinase 1 (PINK1), cause autosomal dominant or recessive PD. Collectively these four genes explain the bulk of monogenic PD, however they do not elicit significant cognitive impairment and are beyond the scope of this discussion. Mutations in SNCA co-segregate in autosomal dominant European and Asian ancestry PD pedigrees. All pathogenic SNCA alleles are dominant heterozygous missense mutations or dominant copy number changes (Collins and Williams-Gray, 2016; Hernandez et al., 2016). Examples include Glu46Lys (absent from ExAC) and triplication, which result in early-onset parkinsonism, dementia, hallucinations, autonomic dysfunction, extensive Lewy bodies, and clinical diagnoses ranging from PD to DLB (Singleton et al., 2003; Zarranz et al., 2004). Interestingly, allele dosage correlates with age at onset and disease severity in SNCA copy number families. This gene encodes α-synuclein, which aggregates into the Lewy bodies that neuropathologically define familial and sporadic parkinsonian disorders. This synaptic protein is poorly understood, but appears to play a role in vesicular transport. These findings demonstrate that copy number variants can have dose-dependent effects on the severity of clinical phenotypes (Hernandez et al., 2016). AU TO S O M A L R EC E S S I VE LYS O S O M A L S TO R AG E D I S E A S E S A N D L EU KO DY S T RO P H I E S : GB A , T RE M2
Gaucher’s disease is a recessive LSD caused by biallelic coding (i.e., missense, nonsense, splice site, or frameshift) mutations in Glucosylceramidase Beta (GBA). Onset ranges from neonatal to adult. Patients can develop hepatosplenomegaly, anemia, thrombocytopenia, and bone disease, as well as various neurological outcomes including neurodegeneration, dementia, dysphagia, supranuclear gaze palsy, ataxia, and seizures.
Interestingly, GD cases and their unaffected heterozygous relatives exhibit elevated rates of comorbid PD. The prevalence of GD is especially high in the Ashkenazi Jewish population, most likely due to founder effects. The majority of pathogenic alleles severely impair GBA enzyme function, resulting in lysosomal defects including accumulation of the sphingolipid glucosylceramide (Lloyd-Evans and Haslett, 2016; Sidransky et al., 2009). Nasu-Hakola disease (also known as polycystic lipomembranous osteodysplasia with sclerosing leukoencephalopathy) is a fatal recessive leukodystrophy caused by homozygous missense, nonsense, and splice site mutations in TREM2. After onset in adolescence to young adulthood, NHD cases develop pain in hands, feet, and joints, polycystic bone lesions and recurrent fractures, personality changes, seizures, and dementia Paloneva et al., 2002). Consistent neuropathological features include myelin loss, axonal spheroids, and accumulated pigment in glia and macrophages (Mackenzie and Neumann, 2016). AU TO S O M A L D O M I NA N T T R A NS M I S S I B L E S P O N G I F O R M E N C E P H A L O PAT H I E S : PRN P
Heterozygous missense and nonsense mutations in PRNP segregate with several TSEs (e.g., fCJD, GSS, FFI) in autosomal dominant families from several populations (Goldgaber et al., 1989; Hsiao et al., 1989; Mead et al., 2013; Medori et al., 1992). This groundbreaking discovery identified the first gene linked to neurodegenerative dementia. Heterozygous PRNP indels modifying the number of octapeptide repeats display apparent co-segregation (Collinge et al., 1989; Owen et al., 1989), but some of these indels have been detected at low frequencies in controls from several ethnicities, hence their penetrance might vary depending on the exact alteration (Lloyd and Collinge, 2013). Pathogenic alleles are scattered throughout this gene. PrpC is a membrane-anchored glycoprotein whose physiological functions are unclear but may include synaptic plasticity (Schmitz et al., 2016).
COMMON ALLELES WITH HIGH EFFECT SIZE AU TO S O M A L S E M I-D O M I NA N T A L Z H E I M E R’S D I S E A S E : A P O E
Early linkage studies in LOAD and EOAD pedigrees provided the first evidence implicating a region on chromosome 19q in this disorder. Subsequent association analysis in multiple populations has convincingly demonstrated that APOE variation is the strongest genetic risk factor for sporadic and familial AD (Farrer et al., 1997; Pericak-Vance et al., 1991; Saunders et al., 1993). The APOE protein exists in three common isoforms, known as ε2, ε3, and ε4. These alleles are defined by the combination of two common missense SNVs: Cys112Arg (ExAC non-Finnish European MAF = 0.208) and Arg158Cys (ExAC non- Finnish European MAF = 0.106) (codon numbering
GOxford enetics D USA ementia Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney,51. et al., Universityof Press - OSO, 2018.• 15:41:51.
Member 2 (FERMT2), Major Histocompatibility Complex, Class II, DR Beta 5-Major Histocompatibility Complex, Class II, DR Beta 1 (HLA–DRB5-HLA–DRB1), Inositol Polyphosphate- 5-Phosphatase D (INPP5D), Myocyte Enhancer Factor 2C (MEF2C), Membrane Spanning 4-Domains A6A (MS4A6A), NME/NM23 Family Member 8 (NME8), Phosphatidylinositol Binding Clathrin Assembly Protein (PICALM), Protein Tyrosine Kinase 2 Beta (PTK2B), Solute Carrier Family 24 Member 4- Ras And Rab Interactor 3 (SLC24A4-RIN3), Sortilin-Related Receptor, L(DLR Class) A Repeats Containing (SORL1), Zinc Finger CW-Type And PWWP Domain Containing 1 (ZCWPW1) (Lambert et al., 2013). Most of these loci were replicated in stage 2 or a subsequently published independent cohort, although DSG2 appears to be spurious. The CD33 Molecule (CD33) locus was slightly subthreshold in stage 1 and its veracity as a robust AD locus remains uncertain. Like GWASs in other complex traits, most of the association signals were characterized by low effect sizes, with OR values generally ranging from 0.75 to 1.2. However, the observed APOE locus association was considerably stronger (OR ≈ 7). Consistent with earlier studies, population-attributable/preventive fraction analysis indicated that APOE has markedly more impact on disease susceptibility than any other locus. Interestingly, the minor allele conferred reduced AD risk for roughly half the associated loci (Lambert et al., 2013). The well-powered IGAP GWAS demonstrates that low effect size common variation is an important component of AD genetic architecture (Figure 51.1). Subsequent European ancestry GWASs investigating specific AD sub-cohorts have yielded interesting findings. Given the large contribution of the APOE locus, additional loci affecting disease risk could be missed due to genetic heterogeneity. C O M M O N A L L E L E S W I T H L OW One report filtered the IGAP dataset to retain only subjects EFFECT SIZE negative for the ε4 allele, and used a two-stage design as before. In the combined meta-analysis, the 17q21 MAPT H1 haploA L Z H E I M E R’S D I S E A S E : G E N O M E -WI D E type was associated in the ε4-negative stratum (AD = 7,902; A S S O C I AT I O N S T U D I E S controls = 28,667; OR = 0.73 [95% CI = 0.65 –0.81]; p = 5.8 The largest GWAS of LOAD susceptibility to date, known as x 10−9) ( Jun et al., 2016), and this hit has since been independthe International Genomics of Alzheimer’s Project (IGAP), ently replicated. The restriction of this signal to ε4-negative brought together case-control and family cohorts collected AD raises the intriguing possibility that these individuals repby four consortia in the United States and Europe. Stage 1 resent a pathologically distinct disease entity. Indeed, the same entailed imputation of European ancestry GWAS data and haplotype increases risk for several neurodegenerative diseases meta- analysis of 7,055,881 common variants (primary dis- that tend to lack amyloidosis, including PD, PSP, and CBD covery cohort: AD = 17,008; controls = 37,154). In stage 2, (Höglinger et al., 2011; Kouri et al., 2015; Nalls et al., 2014). 11,632 variants with p < 1 x 10−3 were genotyped in an inde- Many GWASs examine clinically diagnosed patients and so pendent case-control sample drawn from 11 populations of can be underpowered due to phenotypic heterogeneity. The European descent (replication cohort: AD = 8,572 cases; con- largest published GWAS of neuropathologically confirmed trols = 11,312) and subjected to meta-analysis. Stage 2 was used LOAD (AD = 3,887; controls = 1,027) found that 13 of 22 to replicate association signals observed in stage 1, and subse- IGAP loci were nominally significant, with nine displaying quently both stages underwent combined meta-analysis (sec- stronger effect sizes than reported by IGAP (ABCA7, BIN1, ondary discovery cohort: AD = 25,580; controls = 48,466) CASS4, CD33, MEF2C, MS4A6A, PICALM, SORL1, and (Lambert et al., 2013). Twenty-one loci achieved genome- ZCWPW1) (Beecham et al., 2014). These sub-cohort analyses wide significance (p < 5 x 10−8) in either stage 1 or the com- suggest that the increased statistical power bestowed by genetic bined analysis: ATP Binding Cassette Subfamily A Member stratification or rigorous phenotyping can improve our under7 (ABCA7), APOE, BIN1, Cas Scaffolding Protein Family standing of disease biology and generate nosological insights. Minority population GWASs indicate that AD genetic Member 4 (CASS4), CUGBP, Elav-Like Family Member 1 (CELF1), Clusterin (CLU), Complement Component 3b/4b architecture is characterized by inter-ethnic similarities and Receptor 1 (CR1), CD2-Associated Protein (CD2AP), Desmoglein differences, but analyses have been hindered by limited sam2 (DSG2), EPH Receptor A1 (EPHA1), Fermitin Family ple sizes. The largest African-American LOAD GWAS to date based on removal of the 18 residue signal peptide). The ε3 allele is most frequent, although this can vary markedly across ethnicities. The common ε4 allele raises AD susceptibility and lowers age at onset in a dose-dependent manner in multiple populations (Karch et al., 2014). For example, a large retrospective study of LOAD in European ancestry populations (AD = 7,531; controls = 10,132) found that ε4 heterozygosity increases risk 3.63-fold (95% CI = 3.37 –3.90), and ε4 homozygosity increases risk 14.49-fold (95% CI = 11.91 –17.64) as compared to ε3 homozygotes (the standard referent genotype). Age-stratified analyses found lower odds ratios (ORs) before 60 years and after 80 years, underlining the prime window in which ε4 exerts its effects (Genin et al., 2011). Furthermore, the protective ε2 allele reduces LOAD susceptibility and delays age at onset (Karch et al., 2014). Given its powerful effect on AD, APOE-ε4 has been described as a moderately penetrant allele with semi-dominant inheritance (Genin et al., 2011). More than 20 years have passed since APOE was linked to AD, yet its role in pathophysiology is still poorly understood. This gene encodes a lipid-binding glycoprotein expressed in liver, brain, and innate immune cells. The APOE protein is involved in many processes, including cholesterol redistribution, neuronal growth, and the immune system. The ε4 and ε3 alleles appear to differ in their ability to influence Aβ aggregation and amyloid formation (Karch et al., 2014). However, this is unlikely to be the full story, and recent research suggests the pathogenic mechanisms of APOE may also encompass lipid metabolism and innate immunity (Keren-Shaul et al., 2017; Yeh et al., 2016).
• DPress ementia Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford690 University USA - OSO, 2018. 15:41:51.
Risk of disease
Causes disease
PSEN1 PSEN2 APP
High risk
Med risk
APOE4
Low risk
3
4
5
6
7
8
9 10 11 12 13 14
20
30
Rare
40
50
Common Frequency in the population (%) REPLICATED AD LOCI
UNREPLICATED AD LOCI
Genetic Architecture of Alzheimer’s Disease. Genetic loci influencing AD risk are shown. Loci acting at multiple places in frequency– effect size space are displayed more than once. Fill colors indicate whether loci have demonstrated robust replication. AD = Alzheimer’s disease. Figure 51.1
(AD = 1,968; controls = 3,928) demonstrated association at APOE (OR = 2.31 [95% CI = 2.19 –2.42]; p = 5.5 x 10−47) and ABCA7 (OR = 1.78 [95% CI = 1.28 –1.82]; p = 1.4 x 10−6). The latter became genome-wide significant after adjustment for ε4 allele dosage (OR = 1.79 [95% CI = 1.47 –2.12]; p = 2.21 x 10−9). Varying degrees of association were also seen at the 5q35, Engulfment And Cell Motility 1 (ELMO1), SRY- Box 13 (SOX13), BIN1, CD33, CR1, and EPHA1 loci, though further studies in better-powered African-American cohorts will be required to build confidence in the novel association signals (Reitz et al., 2013). Compared to IGAP, effect sizes in African Americans were markedly lower at APOE but marginally higher at other loci (e.g., ABCA7), and at each locus association signals were usually attributed to different variants in the different populations. These observations are likely due to inter-ethnic differences in haplotypic structure and/or the presence of population-specific risk variants (Reitz et al., 2013). A Japanese LOAD GWAS demonstrated genome-wide association at APOE with similar effect size to Caucasian non-Hispanics (AD = 1,008; controls = 1,016; OR = 5.5 [95% CI = 4.4 –6.9]; p = 2.46 x 10−49). Several other known loci were at least nominally significant (ABCA7, BIN1, CR1, CLU, PICALM, SLC24A4-RIN3), but larger sample sizes will be required to thoroughly elucidate AD genetic architecture in Asian populations. However, meta-analysis of SORL1 variants in Japanese, Korean, and European-American cohorts
achieved genome-wide significance (AD = 14,072; controls = 14,061; OR = 0.81 [95% CI = 0.75 –0.87]; p = 2.2 x 10−9) (Miyashita et al., 2013). Due to an established role in APP metabolism, candidate gene studies predating GWASs had already investigated SORL1. Variants and haplotypes were tentatively associated and replicated in sporadic case-control and familial LOAD cohorts drawn from European-American, African-American, Caribbean-Hispanic, and Arab-Israeli populations (Rogaeva et al., 2007). Taken together with IGAP, these findings suggest that SORL1 common alleles influence AD risk worldwide. It is essential to remember that GWASs identify loci, not genes. This powerful and relatively unbiased technique detects association between the phenotype of interest and haplotype blocks of linkage disequilibrium (LD), not specific genes or variants. The gene used to label any GWAS locus is usually a placeholder selected for its central location within the associated LD block. Hence additional research is required to pinpoint the gene or genes implicated by an association signal, and leverage GWAS findings to elucidate mechanisms driving disease risk. Functional and biomarker studies already incriminate ABCA7, CD33, CR1, SORL1, and Spi-1 Proto-Oncogene (SPI1) (which resides in the CELF1 locus), but further work is needed to clarify how these genes contribute to AD pathogenesis (Cuyvers and Sleegers, 2016; Huang et al., 2017). Meanwhile, large-scale efforts to tackle this sizable problem are already underway.
GOxford enetics DUSA ementia Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney,51. et al., Universityof Press - OSO, 2018.• 15:41:51.
p = 1.08 x 10−11). Sub-cohort and conditional analyses found this signal in both GRN mutation-positive and negative FTLD- TDP, and indicated that the TMEM106B locus is a genetic modifier of GRN-linked disease. Functional studies showed the most significant variant is also an eQTL for TMEM106B in human frontal cortex, and these experiments suggest that TMEM106B overexpression increases FTLD-TDP risk (Van Deerlin et al., 2010). The largest FTD GWAS to date entailed imputation and separate analyses of clinical subtype European ancestry cohorts (bvFTD, nfvPPA, svPPA, FTD-ALS) followed by meta-analysis of all FTD. Genome-wide signals were detected and replicated in the bvFTD analysis at RAB38, Member RAS Oncogene Family- Cathepsin C (RAB38-CTSC) (bvFTD = 1,377; controls = 2,754; OR = 0.730 [95% CI = 0.65 –0.82]; p = 2.02 x 10−8), and in the all FTD meta-analysis at Major Histocompatibility Complex, Class II, DR Alpha-Major Histocompatibility Complex, Class II, F RO N TOT E M P O R A L D E M E N T I A : DR Beta 5 (HLA–DRA-HLA–DRB5) (all FTD = 2,154; conG E N O M E -W I D E A S S O C I AT I O N S T U D I E S trols = 4,308; OR = 1.331 [95% CI = 1.22 –1.45]; p = 1.65 x The first large FTD GWAS analyzed a cohort of European 10−10). The other subtype analyses did not yield genome-wide descent with case inclusion restricted to neuropathologically significant loci, probably due to lack of power. Data mining indidiagnosed FTLD-TDP. Cases with and without GRN muta- cated that the bvFTD analysis top hit is also an eQTL for RAB38 tions were present, and some subjects exhibited comorbid ALS. in human monocytes (Ferrari et al., 2014). The TMEM106B, Genome-wide association was identified and replicated at the RAB38, and CTSC proteins are involved in lysosomal biology; Transmembrane Protein 106B (TMEM106B) locus (FTLD- hence together these results support the notion that lysosomal TDP = 515; controls = 2,509; OR = 0.61 [95% CI = 0.53 –0.71]; dysfunction contributes to FTD pathophysiology (Figure 51.2). Investigators use various statistical tools, such as expression quantitative trait locus (eQTL), pathway, and network co- expression analysis, to integrate multiple layers of genetic and functional data. Several reports indicate that lipid metabolism, innate immunity, endocytosis, and the ubiquitin-proteasome system are central to AD etiology (International Genomics of Alzheimer’s Disease Consortium, 2015; Jones et al., 2010). Moreover, there is strong evidence that microglia and/or other myeloid-lineage cells play a critical role in functionally mediating the genetic architecture of this disorder, potentially through efferocytosis, which is the phagocytosis of lipid rich dying cell debris by innate immune cells (Huang et al., 2017; Raj et al., 2014; Zhang et al., 2013). Nevertheless, these early forays into systems genomics have just scratched the surface.
Causes disease
Risk of disease
High risk
Med risk
Low risk
3 Rare
4
5
6
7
8
9 10 11 12 13 14
Frequency in the population (%) FTD LOCI
20
30
40
50
Common
ALS LOCI
Genetic Architecture of Frontotemporal Dementia and Amyotrophic Lateral Sclerosis. Genetic loci influencing risk of FTD and ALS are shown. Loci acting at multiple places in frequency–effect size space are displayed more than once. Fill colors indicate predominant disease phenotype(s) influenced by each locus. Loci circled in red have not demonstrated robust replication. ALS = amyotrophic lateral sclerosis; FTD = frontotemporal dementia. Figure 51.2
• DPress ementia Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford692 University USA - OSO, 2018. 15:41:51.
penetrant alleles that cause Mendelian parkinsonism (e.g. LRRK2, MAPT, SNCA, and VPS13C), validating Singleton & Hardy’s prediction that individual neurological disease loci are likely to be pleomorphic (i.e., contain risk alleles spread across frequency-effect size space) (Hernandez et al., 2016; The largest PD GWAS to date was a two-stage imputed meta- Singleton and Hardy, 2016). Overall these findings suggest analysis conducted in European ancestry populations by the that PD mechanistic architecture coalesces around pathInternational Parkinson’s Disease Genomics Consortium ways involving the autophagosome-lyososome system, innate (IPDGC) (PD = 13,708; controls = 95,282). Replicated immunity, the cytoskeleton, and mitochondria (Figure 51.3). association was demonstrated for 28 independent genome- Investigation of LBD common genetic architecture is still wide signals in 24 loci, including Family With Sequence in its infancy. Though not technically a GWAS, the largest Similarity 47 Member E-Scavenger Receptor Class B Member 2 association study to date selected 54 loci demonstrating asso(FAM47E-SCARB2), Glucosylceramidase Beta-Synaptotagmin ciation in the IPDGC (32 PD loci) or IGAP studies (22 AD 11 (GBA-SYT11), LRRK2, MAPT, SNCA, and Vacuolar loci) and systematically screened them in a neuropathological Protein Sorting 13 Homolog C (VPS13C). Multiple indeand clinical DLB cohort of European descent (DLB = 788; pendent signals were found in four loci, including SNCA and controls = 2,624). Study-wide significance (p < 3.7 x 10−5) was GBA-SYT11. The strongest common genetic risk factors for observed at APOE, SCARB2, and SNCA (Bras et al., 2014). PD are SNCA (OR = 0.737; p = 3.23 x 10−67) and MAPT The APOE signal (OR = 2.786 [95% CI = 2.397 –3.239]; (OR = 0.771; p = 4.86 x 10−37). Interestingly, the MAPT p = 1.52 x 10−40) had been seen in previous DLB association association detected the 17q21 MAPT H1 haplotype, which studies and is driven by the ε4 allele. This is the strongest comincreases PD susceptibility (Nalls et al., 2014). This region mon genetic risk factor for DLB, but its effect size is lower contains a ~900 kb inversion polymorphism encompassing than for AD in the same population. Despite their biological the MAPT gene which has diverged into two common haploplausibility, the other two loci await replication. The potential type lineages (H1 and H2) (Stefansson et al., 2005). Several of for bias notwithstanding, these data indicate DLB shares elethese confirmed PD risk loci contain genes known to harbor ments of its genetic architecture with AD and PD, and imply PA R K I N S O N ’S D I S E A S E , L EWY B O DY D E M E N T I A , A N D AT Y P I C A L PA R K I N S O N I S M : G E N O M E -WI D E A S S O C I AT I O N S T U D I E S
Causes disease
Risk of disease
High risk
Med risk
Low risk
3 Rare
4
5
6
7
8
9 10 11 12 13 14
20
30 40 Common
50
Frequency in the population (%) PD LOCI
DLB or PDD LOCI
Genetic Architecture of Parkinson’s Disease, Parkinson’s Disease Dementia, and Dementia with Lewy Bodies. Genetic loci influencing risk of PD, PDD, and DLB are shown. Loci acting at multiple places in frequency-effect size space are displayed more than once. Fill colors indicate predominant disease phenotype(s) influenced by each locus. Loci circled in red have not demonstrated robust replication. DLB = dementia with Lewy bodies; PD = Parkinson’s disease; PDD = Parkinson’s disease dementia. Figure 51.3
GOxford enetics D USA ementia Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney,51. et al., Universityof Press - OSO, 2018.• 15:41:51.
that lysosomal/vesicular and Aβ mechanisms both contribute to DLB pathophysiology. Interestingly, the MAPT locus was not associated with DLB (Bras et al., 2014). However, an ongoing prospective incident cohort study of PD shows that MAPT H1 homozygosity significantly increases the risk of progression to PDD, and this effect on cognitive decline seems to be greater earlier in the disease course (Collins and Williams-Gray, 2016). Atypical parkinsonism has been interrogated using separate two- stage GWASs examining neuropathologically diagnosed PSP (PSP = 1,114; controls = 3,287) and CBD (CBD = 152; controls = 3,311) cohorts of mostly European descent. The 17q21 MAPT H1 haplotype was detected and replicated in both disorders. This is by far the strongest common genetic risk factor for PSP (OR = 5.50 [95% CI = 4.40 – 6.86]; p = 2.1 x 10−51) and CBD (OR = 3.45 [95% CI = 2.25 – 9.34]; p = 6.71 x 10−9). The PSP study identified and/or replicated additional genome-wide signals at Myelin- Associated Oligodendrocyte Basic Protein (MOBP), Syntaxin 6 (STX6), and Eukaryotic Translation Initiation Factor 2 Alpha Kinase 3 (EIF2AK3). For CBD, genome-wide significance was identified at Kinesin Family Member 13B (KIF13B), and suggestive signals were observed at MOBP and SOS Ras/R ac Guanine Nucleotide Exchange Factor 1 (SOS1) (Höglinger et al., 2011; Kouri et al., 2015). Perhaps unsurprisingly, these
results place MAPT common variation and the cytoskeleton at the heart of tauopathy pathogenesis (Figure 51.4). T R A NS M I S S I B L E S P O N G I F O R M E N C E P H A L O PAT H I E S : G E N O M E -WI D E A S S O C I AT I O N S T U D I E S
Extremely low disease prevalence has limited the statistical power of TSE association studies. The first large TSE GWAS investigated sCJD, vCJD, iCJD, fCJD, and kuru in cohorts from the United Kingdom, Germany, and Papua New Guinea. The only locus demonstrating robust association across several TSE cohorts was PRNP (all CJD subtypes and kuru resistant = 1,406; controls = 6,301; OR = 0.77; p = 6.58 x 10−7), and conditional analyses suggested this is explained by the common variant Met129Val (ExAC non- Finnish European MAF = 0.335) (Mead et al., 2012). A GWAS of sCJD in cohorts drawn from multiple European populations (sCJD = 1,543; controls = 11,424) detected association at PRNP (beta coefficient = 0.2927 [SE = 0.0528]; p = 3.00 x 10−8) and Glutamate Receptor Metabotropic 8 (GRM8) (beta coefficient = –0.1837 [SE = 0.0447]; p = 3.91 x 10−5) (Sanchez-Juan et al., 2015). Both studies found suggestive signals at additional loci, but these await exploration in better- powered cohorts (Mead et al., 2012; Sanchez-Juan et al., 2015).
Causes disease
Risk of disease
High risk
Med risk
Low risk
3
4
5
6
7
8
9 10 11 12 13 14
Rare
20
30
40
50
Common Frequency in the population (%) PSP LOCI
CBD LOCI
Genetic Architecture of Progressive Supranuclear Palsy and Corticobasal Degeneration. Genetic loci influencing risk of PSP and CBD are shown. Loci acting at multiple places in frequency-effect size space are displayed more than once. Fill colors indicate predominant disease phenotype(s) influenced by each locus. Loci circled in red have not demonstrated robust replication. PSP = progressive supranuclear palsy; CBD = corticobasal degeneration. Figure 51.4
• DPress ementia Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford694 University USA - OSO, 2018. 15:41:51.
Hence TSE genetic architecture is dominated by the PRNP locus, but several other regions probably make at least minor contributions. Other reports indicate that PRNP common missense variation modifies TSE outcomes and phenotypes, as exemplified by Met129Val. Met/Met and/ or Val/Val homozygosity are overrepresented in sCJD, iCJD, vCJD, and kuru, implying that Met/ Val heterozygosity protects against TSEs. Furthermore, Met/Val kuru patients display later age at onset and longer disease duration. These findings suggest codon 129 heterozygosity ameliorates permissive templating. The situation for PRNP-linked Mendelian TSE is more complicated. Carriers of mutations mostly seen in European ancestry patients (e.g., Glu200Lys [absent from ExAC]) are similarly depleted for Met/Val heterozygosity. However, carriers of mutations mostly found in Japanese cases (e.g., Val180Ile [ExAC East Asian MAF = 3.47 x 10−4]) are enriched for Met/ Val heterozygosity (Kobayashi et al., 2015). Thus additional research is required to elucidate the role of PRNP common variation in TSE pathogenesis. R A R E A N D L OW F R E Q U E N C Y A L L E L E S W I T H M O D E R AT E EFFECT SIZE OVE RVI EW
Many genes likely contain rare and low frequency variants that influence neurodegenerative dementia susceptibility. Several of these genes reside in loci where common variation also associates with similar neurological disease phenotypes, confirming the existence of pleomorphic risk loci (Singleton and Hardy, 2016). However, the sequencing era is young and still very much a work in progress, technologically and statistically. Early optimism that effect sizes would be substantial (e.g., OR > 5) has been tempered by the sobering subtlety of many rare variants (e.g., OR > 2). Hence considerably larger cohorts (e.g., potentially more than 50,000 subjects) will be required to convincingly demonstrate that rare variation is a significant driver of neurodegenerative dementia risk. A L Z H E I M E R’S D I S E A S E
ADAM10 Sanger sequencing showed that the rare ADAM Metal lopeptidase Domain 10 (ADAM10) variants Gln170His (ExAC non-Finnish European MAF = 1.23 x 10−3) and Arg181Gly (ExAC non-Finnish European MAF = 1.95 x 10−4) display partial but unconvincing segregation with LOAD in several European-American pedigrees. Incomplete penetrance was observed, indicating these alleles are risk factors rather than sufficient to cause disease (Kim et al., 2009). Sequencing 305 neuropathologically proven sporadic AD cases and 271 controls identified no ADAM10 coding variants associated with disease. Indeed, this study demonstrated
that spurious association for Leu9Val (ExAC non-Finnish European MAF = 2.00 x 10−3) was actually due to enrichment in the Ashkenazi Jewish population, highlighting the need to be wary of population stratification in rare variant analysis (Cai et al., 2012). No further sequencing studies have been reported, suggesting that ADAM10 rare variation is not a substantial component of AD genetic architecture. The ADAM10 enzyme is a metalloprotease that regulates shedding of extracellular domains from cell surface proteins. It mediates α-secretase activity that cleaves APP to generate sAPPα and block the production of Aβ, thereby driving the anti-amyloidogenic pathway. The Gln170His and Arg181Gly variants are located in the prodomain which regulates ADAM10 enzymatic activity. These alleles reduce anti- amyloidogenic pathway fragments and enhance Aβ levels in cell and mouse models (Karch et al., 2014).
SORL1 The IGAP GWAS confirmed that SORL1 common variation drives AD susceptibility (Lambert et al., 2013), and considerable evidence indicates that rare and low frequency alleles at the same locus increase AD risk across multiple populations. However, definitively pathogenic variants remain elusive, and gene level association signals are just shy of multiple testing correction thresholds, highlighting the need for larger sample sizes. Exome sequencing identified seven rare coding variants in 29 autosomal dominant EOAD familial cases originating from France, Italy, Portugal, United Kingdom, and Algeria. One missense variant (Gly511Arg [absent from ExAC]) was also present in an affected relative, but segregation analysis was not possible (Pottier et al., 2012). Exome and targeted sequencing studies in larger autosomal dominant EOAD case-control cohorts implicate SORL1 rare coding variation. Gene aggregation analysis in a French population including subjects from the previous report showed association for variants predicted as protein-damaging (AD = 484; controls = 498; OR = 5.03 [95% CI = 2.02 –14.99]; p = 7.49 x 10−5), and this signal was enhanced by restriction to familial cases (AD = 205; controls = 498; OR = 8.78 [95% CI = 3.22 –23.93]; p = 2.19 x 10−5) (Nicolas et al., 2016). Aggregated coding variants were associated in a meta-analysis of populations drawn from Belgium, Spain, Portugal, Italy, and Sweden (AD = 1085; controls = 1752; variant enrichment in AD = 1.7-fold; p = 1 x 10−4) (Verheijen et al., 2016). Furthermore, targeted sequencing and genotyping in a cohort comprising American-Hispanic and Caribbean-Hispanic families and unrelated controls suggests that rare and low frequency SORL1 alleles also modify LOAD risk. After prioritizing 17 coding variants by a combined association and linkage approach, aggregation analysis excluding noncarrier families found modest association (families = 87; AD = 350; familial controls = 114; unrelated controls = 498; p = 7.9 x 10−3). Rare 17-variant haplotypes were associated with LOAD (n = 933; OR = 1.9; p = 6.9 x 10−5), and three missense variants (Glu270Lys [ExAC Hispanic MAF = 0.013], Ala528Thr [ExAC Hispanic MAF = 0.116], and Thr947Met
GOxford enetics D USA ementia Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney,51. et al., Universityof Press - OSO, 2018.• 15:41:51.
[ExAC Hispanic MAF = 4.32 x 10−4]) were enriched in disease cases across multiple families. Interestingly, Glu270Lys and Ala528Thr appear to reside on a common haplotype previously associated with AD in Caribbean- Hispanic populations, but are not in LD with the European ancestry IGAP GWAS signal (Vardarajan et al., 2015a). The SORL1 protein redirects APP away from cell surface endosome- lysosome transport, recycling it toward the Golgi via the retromer pathway. This reduces amyloidogenic processing, as corroborated by increased Aβ levels after SORL1 ablation in vitro and in vivo (Cuyvers and Sleegers, 2016; Karch et al., 2014). Sequencing studies have identified coding variants spanning all SORL1 protein domains. Interestingly, multiple rare SORL1 LOF variants were found exclusively in affected individuals. These are absent from the ExAC database, and in patient blood samples some elicited haploinsufficiency, supporting the notion that rare SORL1 LOF alleles can increase AD risk via impaired APP recycling (Nicolas et al., 2016; Verheijen et al., 2016; Vardarajan et al., 2015a). As is often the case for sequencing data, SORL1 rare and low frequency missense variation is more difficult to interpret. Indeed, many variants were also seen in controls, suggesting they are neutral or risk factors with incomplete penetrance (Nicolas et al., 2016; Verheijen et al., 2016; Vardarajan et al., 2015a). Nevertheless, cell culture experiments have been informative. Gly511Arg impairs SORL1-Aβ binding thereby reducing SORL1-mediated lysosomal degradation of Aβ, whereas Glu270Lys, Ala528Thr, and Thr947Met exhibit reduced APP binding as well as enhanced Aβ release and cell surface APP (Cuyvers and Sleegers, 2016; Vardarajan et al., 2015a). Overall, these findings suggest that rare and low frequency SORL1 alleles influence AD risk via multiple mechanisms.
TREM2 A large body of evidence convincingly demonstrates that rare and low frequency TREM2 alleles influence AD susceptibility in populations of European descent, but larger analyses of underrepresented minorities are warranted. Two independent studies employing different combinations of sequencing (exome, genome, Sanger), imputation, and genotyping in LOAD and EOAD cohorts drawn from multiple European ancestry populations were the first to implicate TREM2 rare coding variation. Notably these reports observed cases with heterozygous NHD variants (e.g., Gln33Ter [1 allele in ExAC; non-Finnish European MAF = 1.54 x 10−5]) and showed that Arg47His (ExAC non-Finnish European MAF = 2.60 x 10−3) raises disease risk (Guerreiro et al., 2013; Jonsson et al., 2013). Several publications subsequently replicated this association. The largest study to date recently meta-analyzed cohorts of European descent and found that Arg47His increases AD susceptibility with moderate effect size (AD = 24,086; controls = 148,993; OR = 2.71 [95% CI = 2.24 –3.28]; p = 4.67 x 10−25) (Lill et al., 2015). Targeted sequencing and gene aggregation analysis in European-American familial and sporadic LOAD cohorts (AD = 2,082; controls = 1,648) demonstrated TREM2 rare and low frequency coding variation is associated
with disease (OR = 2.55 [95% CI = 1.80 –3.67]; p = 5.37 x 10−7). This remained significant after excluding Arg47His (OR = 2.47 [95% CI = 1.62 –3.87]; p = 7.72 x 10−5), but not both Arg47His and the low frequency variant Arg62His (ExAC non-Finnish European MAF = 0.011) (OR = 2.95 [95% CI = 1.23 –8.09]; p = 0.09), suggesting most of the statistical signal arises from these variants, but that additional rare alleles may also be involved. Indeed, Arg62His alone was shown to increase AD risk (OR = 2.36 [95% CI = 1.47 – 3.80]; p = 2.36 x 10−4) ( Jin et al., 2014). Sequencing and genotyping of TREM2 in clinically ascertained African- American sporadic and familial LOAD cohorts (AD = 906; controls = 2,487) detected trending association signals for Leu211Pro (ExAC African MAF = 0.128) (OR = 1.27 [95% CI = 1.05 – 1.54]; p = 0.01) and Trp191Ter (ExAC African MAF = 0.039) (OR = 1.35 [95% CI = 0.97 –1.87]; p = 0.08). These results await further exploration, but conditional analyses suggested that Leu211Pro could account for the Trp191Ter signal. Interestingly, Arg47His and Arg62His displayed no association, possibly due to their rarity in this population ( Jin et al., 2015). Taken together, these results indicate that multiple TREM2 coding alleles contribute to AD genetic architecture. Implicated variants are scattered across this gene, but their relative impact varies by population, with ethnicity- dependent clustering in the extracellular (European ancestry) and cytoplasmic (African ancestry) domains. The pathogenic mechanisms mediating TREM2 risk are largely unclear and under intense investigation. The TREM2 protein is a transmembrane receptor expressed on the surface of myeloid cells. It binds lipids and lipidated APOE and regulates phagocytosis and inflammation (Karch et al., 2014). Functional experiments suggest that AD-associated rare TREM2 coding variants in the extracellular domain alter ADAM protease-dependent TREM2 shedding and the phagocytic activity of TREM2-positive cells (Cuyvers and Sleegers, 2016). Interestingly, the IGAP GWAS found subthreshold association near Triggering Receptor Expressed On Myeloid Cells Like 2 (TREML2) within the TREM gene cluster, whereby the minor allele has a protective effect, hinting that common variation in this region may also influence AD susceptibility (Lambert et al., 2013). Exome sequencing followed by meta-analysis of imputed European ancestry LOAD GWAS data demonstrated that the risk-reducing common variant Ser144Gly (ExAC non-Finnish European MAF = 0.299) in TREML2 could explain the IGAP signal (AD = 16,254; controls = 20,052; OR = 0.93 [95% CI = 0.89 –0.96]; p = 8.66 x 10−5). Furthermore, conditional analyses indicated TREML2 Ser144Gly and TREM2 Arg47His are independent of each other with regard to their effects on susceptibility (Benitez et al., 2014). These data suggest the TREM gene cluster harbors rare and common variants that modify AD risk in a complex manner.
ABCA7 The European ancestry IGAP and African-American GWASs both implicated ABCA7 common variation in AD (Lambert et al., 2013; Reitz et al., 2013), and several studies show that
• DPress ementia Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford696 University USA - OSO, 2018. 15:41:51.
rare alleles at this locus influence disease susceptibility. One report used genome and Sanger sequencing data to impute and validate rare variant genotypes in an Icelandic cohort. Gene aggregation analysis demonstrated that ABCA7 rare LOF alleles increase AD risk (AD = 3,419; controls = 151,805; OR = 2.12; p = 2.2 x 10−13), and this was replicated in European ancestry cohorts. Interestingly, the LOF variants driving this effect were not in LD with the IGAP GWAS variant, suggesting these rare alleles act independently from that common signal (Steinberg et al., 2015). Targeted sequencing and gene aggregation analysis in a Belgian cohort found that ABCA7 rare LOF variation associates with AD (AD = 772; controls = 757; relative risk [RR] = 4·03 [95% CI = 1.75 – 9.29]; p = 2 x 10−4), and the effect was enhanced by restriction to familial cases (AD = 146; controls = 757; RR = 8.55 [95% CI = 3.29 – 22.26]; p < 10−5). This cohort harbored the rare frameshift variant Glu709fs (ExAC non-Finnish European MAF = 4.92 x 10−3), and all carriers shared a common haplotype implying a single founder. In one pedigree this allele segregated with AD or cognitive impairment in an autosomal dominant fashion. Expression analysis in Glu709fs carrier postmortem prefrontal cortex tissue indicated this variant causes haploinsufficiency (Cuyvers et al., 2015). Targeted sequencing in African-American LOAD (AD = 40; controls = 37) detected the common frameshift variant Arg578fs (ExAC African MAF = 0.078). This 44 bp deletion is in near perfect LD with the African-American GWAS risk allele and increases disease susceptibility in African-American LOAD cohorts (AD = 978; controls = 1,407; OR = 1.81 [95% CI = 1.38 –2.37]; p = 1.41 x 10−5), suggesting Arg578fs underlies this GWAS signal, and potentially explaining the higher effect size than observed in IGAP. This frameshift exhibited autosomal dominant segregation with AD or mild dementia in one Caribbean-Hispanic family, but is almost nonexistent in non-Hispanic Caucasian cases. Blood expression analysis indicated the Arg578fs allele produces stable RNA lacking the deleted sequence (Cukier et al., 2016). The role of ABCA7 in AD pathogenesis is poorly understood. The ABCA7 protein regulates phagocytosis, transmembrane phospholipid efflux to APOE, and microglial clearance of Aβ. Knockout mice display elevated Aβ levels in their brains (Cuyvers and Sleegers, 2016; Karch et al., 2014). These findings indicate that ABCA7 variation can enhance AD risk via LOF mechanisms, although some associated alleles appear to be largely ethnic-specific.
AKAP9, CLU, EPHA1, PLD3, TM2D3, TTC3, TYROBP, UNC5C Co-segregation or association with AD has been observed for rare coding variants in A-Kinase Anchoring Protein 9 (AKAP9), CLU, EPHA1, Phospholipase D Family Member 3 (PLD3), TM2 Domain Containing 3 (TM2D3), Tetratricopeptide Repeat Domain 3 (TTC3), TYRO Protein Tyrosine Kinase Binding Protein (TYROBP), and Unc-5 Netrin Receptor C (UNC5C) (Bettens et al., 2012; Cruchaga et al., 2014; Jakobsdottir et al., 2016; Kohli et al., 2016; Logue et al., 2014; Pottier et al., 2016; Vardarajan et al., 2015b; Wetzel-Smith et al., 2014).
However, these discoveries await robust replication. Additional genetic evidence is required before concluding that these genes make significant contributions to AD rare genetic architecture. FRO N TOT E M P O R A L D E M E N T I A , PA R K I NS O N ’S D I S E A S E , L EWY B O DY D E M E N T I A , A N D AT Y P I C A L PA R K I NS O N I S M
MAPT The common 17q21 MAPT H1 haplotype has been associated with PD, PDD, PSP, CBD, and APOE-ε4-negative AD (Collins and Williams-Gray, 2016; Jun et al., 2016; Höglinger et al., 2011; Kouri et al., 2015; Nalls et al., 2014), and rare alleles at this locus also influence neurodegenerative dementia susceptibility. The rare MAPT variant Ala152Thr (ExAC non- Finnish European MAF = 1.67 x 10−3), which resides on the H1 haplotype, was genotyped in neuropathological and clinical cohorts of mostly European descent. This analysis showed that Ala152Thr increases the risk of FTD/PSP/CBD (disease = 2,139; controls = 9,047; OR = 3.0 [95% CI = 1.6 –5.6]; p = 5 x 10−4) and AD (AD = 3,345; controls = 9,047; OR = 2.3 [95% CI = 1.3 –4.2]; p = 4 x 10−3). Similar Ala152Thr MAF values were observed for FTD (0.004), PSP/CBD (0.005), and AD (0.003) (Coppola et al., 2012). Moreover in non- Hispanic Caucasian cohorts, Ala152Thr was associated with clinical DLB (DLB = 442 [MAF = 0.007]; controls = 2,456; OR = 5.76 [95% CI = 1.62 –20.51]; p = 7 x 10−3) but not clinical PD (PD = 3,229 [MAF = 0.003]; controls = 2,456; OR = 1.37 [95% CI = 0.63 –2.98]; p = 0.42) (Labbé et al., 2015). In vitro experiments indicate that Ala152Thr alters tau aggregation and impairs microtubule assembly (Coppola et al., 2012). Overall, these data suggest that rare MAPT alleles modify susceptibility to tauopathies but their role in synucleinopathies remains unclear.
TBK1, OPTN Exome sequencing and gene aggregation analysis in a familial ALS-FTD cohort drawn from European populations demonstrated that rare and low frequency TANK Binding Kinase 1 (TBK1) LOF variants increase disease risk (ALS-FTD = 252; controls = 827; p = 1.6 x 10−7). In multiple pedigrees, LOF alleles exhibited partial segregation with incomplete penetrance, and cognitive impairment was frequently observed, often with progression to FTD. Expression analysis in patient cell lines indicated that several TBK1 LOF variants result in haploinsufficiency, and brain autopsy of one frameshift carrier discovered temporal lobe FTLD-TDP (Freischmidt et al., 2015). Optineurin (OPTN) rare variation has mainly been implicated in ALS, a disorder characterized by loss of upper and lower motor neurons. However, genome sequencing of 104 mostly European ancestry disease cases neuropathologically diagnosed with FTLD-TDP identified five TBK1 and OPTN rare variant carriers. Two of these were compound heterozygotes involving LOF alleles (TBK1 LOF- OPTN LOF; OPTN LOF-OPTN missense), and neither subject
GOxford enetics D USA ementia Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney,51. et al., Universityof Press - OSO, 2018.• 15:41:51.
displayed motor neuron loss (Pottier et al., 2015). The TBK1 and OPTN proteins bind each other to regulate autophagy, and functional studies of ALS-FTD TBK1 variants imply that impaired TBK1-OPTN binding is an important pathogenic mechanism (Freishmidt et al., 2015). Once again, these findings implicate autophagosome-lysosome system dysfunction in FTD pathophysiology.
CI = 0.77 –0.82]; sensitivity = 0.704; specificity = 0.703; p < 10−94) (Escott-Price et al., 2015). Another publication used stepwise analysis to identify a minimal set of parameters able to predict PD in European ancestry cohorts. One parameter was PRS calculated from genotypes at the 28 IPDGC genome-wide significant common loci, and at the PD-associated rare variants GBA Asn370Ser and LRRK2 Gly2019Ser (ExAC non-Finnish European MAF = 6.29 x 10−4). The resulting model integrating PRSs, olfactory funcGBA tion, PD family history, age, and sex was remarkably successGlucosylceramidase Beta common variation is associated with ful at predicting PD status in test (PD = 367; controls = 165; PD (Nalls et al., 2014), and rare alleles at this locus also con- AUC = 0.923 [95% CI = 0.900 –0.926]) and validation tribute to synucleinopathy genetic architecture. Given that (PD = 453; controls = 156; AUC = 0.894 [95% CI = 0.867 – GD patients are susceptible to comorbid parkinsonism, a large 0.921]) cohorts. However, due to the low prevalence of PD international multicenter study undertook GBA genotyp- this model would have limited positive predictive value in the ing and Sanger sequencing in PD cohorts of European, East general population, and greatest utility in subjects at high risk Asian, Ashkenazi Jewish, and Hispanic descent. Rare cod- of disease (Nalls et al., 2015). These predictive models await ing GBA variants were demonstrated to increase disease risk validation and refinement in large prospective studies of AD (PD = 4,846; controls = 3,879; OR = 5.43 [95% CI = 3.89 – and PD. Nevertheless, these findings demonstrate the promise 7.57]). The alleles Asn370Ser (ExAC non-Finnish European of clinicogenetic statistical approaches for predicting disease MAF = 3.63 x 10−3) and Leu444Pro (ExAC non-Finnish outcomes. European MAF = 3.92 x 10−3) (codon numbering based on removal of the 39 residue signal peptide) were observed most G E N ET I C A R C H I T E C T U R E frequently. In addition, PD cases carrying a rare GBA variant S H A R E D AC R O S S T R A I T S were more likely to be familial (n = 4401; p = 6 x 10−3) or cognitively impaired (n = 1948; p = 7 x 10−3) (Sidransky et al., 2009). Sanger sequencing and genotyping in clinical and neuropath- Several publications have systematically evaluated whether ological cohorts of mostly European ancestry showed that common genetic architecture is shared across neurological GBA rare coding variation associates with DLB (DLB = 721; phenotypes, but to date only a few diseases have been comcontrols = 1,962; OR = 8.66 [95% CI = 4.49 –17.71]; p = 5.11 pared. The recently developed LD score regression method x 10−10) and PDD (PDD = 151; controls = 1,962; OR = 3.82 estimates hg2 using LD relationship information between [95% CI = 1.45 –10.05]; p = 5.77 x 10−3) (Nalls et al., 2015). genotyped variants and their neighbors. This approach has Taken together, these results indicate that GBA rare variation been adapted for cross-trait LD score regression, which esticonstitutes the strongest genetic risk factor for PD and DLB, mates the genetic correlation between a pair of phenotypes and support the notion that GBA alleles increase dementia (i.e., their shared genetic architecture). The Brainstorm consortium has undertaken a large cross-trait LD score regresincidence in parkinsonian synucleinopathies. sion study of multiple brain disorders and traits of interest in mostly European ancestry cohorts. Several psychiatric illnesses appeared to share considerable heritability. However, P O LYG E N I C R I S K S C O R E S neurological diseases such as AD (cases = 17,008; conThe polygenic risk score (PRS) is calculated from GWAS trols = 37,154) and PD (cases = 5,333; controls = 12,019), data in order to quantify the degree of genetic risk burden exhibited little or no significant overlap with each other or a specific individual carries for a specific disorder. Several with psychiatric conditions (Anttila et al., 2016). A different reports have evaluated the ability of statistical models built study used the standard maximum likelihood approach to from PRSs and clinical parameters to accurately predict neu- estimate hg2 for genetic correlations between AD (cases = 959; rological disease outcomes. This can be quantified using the controls = 1,403), DLB (cases = 788; controls = 1,403), and area under the receiver operating characteristic curve (AUC) PD (cases = 804; controls = 1,403) cohorts of European parameter, with AUC > 0.9 viewed as highly predictive. One descent. Consistent with LD score regression analysis, there study divided the IGAP AD dataset into two sub-cohorts and was almost no overlap between AD and PD. However, signifcalculated PRSs from variants with p ≤ 0.5 in the first group icant correlations were observed for AD/DLB and DLB/PD, (AD = 13,831; controls = 29,877). These PRS alleles were and the AD/DLB correlation was diminished but remained highly enriched in cases from the second group (AD = 3,177; significant after exclusion of the APOE locus (Guerreiro et al., controls = 7,277; beta coefficient = 0.327 [SE = 0.0310]; 2016). Overall, these data provide genetic evidence supporting p = 4.9 x 10−26). Furthermore, a model incorporating PRSs, the existence of an AD-DLB-PDD-PD disease spectrum, but genotypes at 20 IGAP genome-wide significant loci, APOE- tentatively suggest that many neurological conditions do not ε4 and ε2 allele dosages, age, and sex could predict AD status share substantial common heritability. On the other hand, moderate/high effect rare genetic with relatively high accuracy in a subset of the second group (AD = 3,049 cases; controls = 1554; AUC = 0.782 [95% architecture clearly indicates certain neurodegenerative • DPress ementia Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford698 University USA - OSO, 2018. 15:41:51.
alleles are known to elicit clinical heterogeneity, and this has generated nosological insight, but many neurological diseases apparently do not share significant common genetic architecture. Third, intra-disease mechanistic heterogeneity is the norm, and inter-disease overlaps occur often. The genetic architecture of each disorder implicates multiple biological pathways in its pathogenesis. Functional themes recurring across conditions include the autophagosome-lysosome system, innate immunity, lipid metabolism, the cytoskeleton, and the ubiquitin-proteasome system. In the near future, various parallel trends are likely to develop in neurodegenerative genetics research. First, the sequencing era will take hold, but GWAS analysis will continue for some time. Falling sequencing costs, new technologies, and improved computation will eventually foster mass adoption of large-scale genome sequencing. With significantly bigger cohorts than today, these studies will enable widespread interrogation of noncoding variation and genetic epistasis. Third generation sequencing will mature, generating long reads able to elucidate the impact of structural variation with unprecedented resolution. However, genotyping arrays and GWAS analysis will remain important during this process, especially when coupled with powerful imputation panels. Second, underrepresented minority population studies will expand massively. Genetic architecture can vary between populations, both because of differing effect sizes (e.g., APOE-ε4 in AD) C O N C LU S I O N S A N D F U T U R E P E R S P E C T I VE S and ethnicity-specific risk alleles (e.g., ABCA7 Arg578fs in AD), and only a fraction of total extant human genetic variaDecades of neurogenetics research are finally paying divi- tion has been identified. These gaps will be addressed through dends. Application of GWAS to increasingly large cohorts large projects analyzing diverse populations collected worldhas lifted replicated risk loci from the murk of statistical noise, wide. Third, nosology will evolve. Despite the widespread and second generation sequencing is revealing rare alleles with use and demonstrated utility of the sporadic/familial classifidiverse effect sizes. These concrete and laudable advances have cation, clinical variation in familial clustering and symptom begun to paint meaningful patterns attempting to describe onset is considerable. Moreover, phenotypic pleiotropy is a the mechanistic architecture of neurodegenerative demen- well-known phenomenon that disrupts traditional diagnostic tia. Yet this success must be placed in context. The majority boundaries. Genetic and neuropathological evidence increasof genetic architecture remains unresolved for most of these ingly indicates these lines are blurred. Individual pleomorphic diseases, and even less is understood about the roles known risk loci contribute to the architecture of both sporadic and variants play in pathophysiology. familial disease (e.g., SNCA in PD and SORL1 in AD), and This large body of work generates clear conclusions about rare variants can exhibit both sporadic association and familneurodegenerative dementia. First, the genetic architecture ial segregation (e.g., ABCA7 Glu709fs in AD and LRRK2 of these disorders is likely to be polygenic and complex. Most Gly2019Ser in PD), potentially due to genetic factors that of the known risk burden arises from low effect size com- modify penetrance in specific pedigrees. Furthermore, pathomon variation in multiple loci (notwithstanding the notable genic mutations can cause multiple diseases (e.g., C9orf72 in exception of APOE), with some input from a handful of low/ ALS and FTD), and associated loci can influence the risk moderate effect size rare variants. The unknown component is of several traits (e.g., APOE in AD and DLB). Similar neuprobably a combination of many low/moderate effect size rare ropathological patterns occur across sporadic and familial alleles and vast numbers of extremely low effect size common cases (e.g., amyloidosis in AD) and are observed in multiple variants, although their relative contributions are currently clinical diagnostic categories (e.g., tauopathy in AD and PSP). unclear. Some susceptibility loci are pleomorphic, harbor- The ability to reveal pathophysiological subtleties could be ing risk-modifying alleles spread across frequency–effect size improved by conducting genetic analyses using continuous space, although these different variant classes may engage dif- rather than dichotomous phenotypes (Guerreiro et al., 2016), ferent pathomechanisms. Indeed, some rare risk alleles reside such as quantitative measures of cognitive impairment and on common associated haplotypes (e.g., MAPT Ala152Thr neuropathological burden. One natural extension of this and H1 in PSP), whereas at other pleiomorphic loci rare and argument is eventual dissolution of phenotypic dividing lines common associated variants are genetically independent (e.g., and substitution with continuous clinicopathogenetic models ABCA7 Glu709fs and ABCA7 locus in AD). Second, phe- of neurodegenerative disease, such as AD-DLB-PDD-PD or notypic pleiotropy is relevant but its extent is unclear. Rare FTD-ALS disease spectra. This might accompany transition disorder genes display phenotypic pleiotropy. This is best illustrated by the C9orf72 repeat expansion mutation, which in the same individual or pedigree can cause ALS, FTD, or both conditions. Coexistence of these two phenotypes in expansion carrier families is the norm rather than the exception (DeJesus- Hernandez et al., 2011; Renton et al., 2011). This FTD-ALS disease spectrum reflects a fundamental shared genetic link that initiates pathophysiological pleiotropy (i.e., either several pathogenic processes or one process able to destroy several neuronal types). Other genes implicated in multiple disorders each represent currently ill-defined combinations of true pathophysiological pleiotropy, actual disease spectra, and misdiagnosis, such as GRN (FTD, AD), MAPT (FTD, AD, PSP, CBD, DLB), and GBA (PD, PDD, DLB) (Karch et al., 2014; Sidransky et al., 2009; Coppola et al., 2012; Labbé et al., 2015; Nalls et al., 2013). Discussions of pathophysiological pleiotropy versus disease spectra can become circular and might be dismissed as mere semantics. However, these issues highlight real-world diagnostic grey areas that clinicians face. Moreover, as we significantly deepen our knowledge of genotypes and the traits they influence, genetics will mature into a powerful toolkit with the potential to improve diagnostic accuracy and reframe nosological concepts.
GOxford enetics D USA ementia Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney,51. et al., Universityof Press - OSO, 2018.• 15:41:51.
to gene-or pathway-centric nosological frameworks, wherein disease is primarily conceptualized according to etiological molecular dysfunction, for example lysosomopathy or efferocytopathy. It is tempting to speculate about broader long-term trends that might emerge as we progress through the 21st century. First, the environmental architecture of neurodegenerative disorders could be subjected to systematic analysis. It almost certainly plays a role in most diseases, but meaningful systematic interrogation of that role is currently beyond us. In time, technological developments (e.g., wearable devices) may enable longitudinal study designs simultaneously collecting environmental exposure data across multiple modalities (i.e., the exposome). Second, systems genomics could generate transformational insights into the mechanistic architecture of neurodegenerative disease and may precipitate a post-reductionist revolution in biology. Prospective cohort studies spanning decades could harness advanced computational capabilities to integrate multimodal omics data collected from vast cohorts and generate models that enable emergent properties analysis, fundamentally shifting us toward a holistic multilevel systems perspective of health and disease (Woese, 2004).
Cuyvers, E., and Sleegers, K. (2016). Genetic variations underlying Alzheimer’s disease: evidence from genome-wide association studies and beyond. Lancet Neurol 15:857–868. Cuyvers, E., De Roeck, A., et al. (2015). Mutations in ABCA7 in a Belgian cohort of Alzheimer’s disease patients: a targeted resequencing study. Lancet Neurol 14:814–822. DeJesus- Hernandez, M., Mackenzie, I.R., et al. (2011). Expanded GGGGCC hexanucleotide repeat in noncoding region of C9ORF72 causes chromosome 9p-linked FTD and ALS. Neuron 72:245–256. Escott- Price, V., Sims, R., et al. (2015). Common polygenic variation enhances risk prediction for Alzheimer’s disease. Brain 138: 3673–3684. Farrer, L.A., Cupples, L.A., et al. (1997). Effects of age, sex, and ethnicity on the association between apolipoprotein E genotype and Alzheimer disease. A meta-analysis. APOE and Alzheimer Disease Meta Analysis Consortium. JAMA 278:1349–1356. Ferrari, R., Hernandez, D.G., et al. (2014). Frontotemporal dementia and its subtypes: a genome-wide association study. Lancet Neurol 13:686–699. Freischmidt, A., Wieland, T., et al. (2015). Haploinsufficiency of TBK1 causes familial ALS and fronto-temporal dementia. Nat Neurosci 18:631–636. Gatz, M., Reynolds, C.A., et al. (2006). Role of genes and environments for explaining Alzheimer disease. Arch Gen Psychiatry 63:168–174. Genin, E., Hannequin, D., et al. (2011). APOE and Alzheimer disease: a major gene with semi-dominant inheritance. Mol Psychiatry 16:903–907. Goate, A., Chartier-Harlin, M.C., et al. (1991). Segregation of a missense mutation in the amyloid precursor protein gene with familial REFERENCES Alzheimer’s disease. Nature 349:704–706. Goldgaber, D., Goldfarb, L.G., et al. (1989). Mutations in familial Anttila, V., Bulik-Sullivan, B., et al. (2016). Analysis of shared heritability Creutzfeldt-Jakob disease and Gerstmann-Sträussler-Scheinker’s synin common disorders of the brain. bioRxiv 48991. drome. Exp Neurol 106:204–206. Baker, M., Mackenzie, I.R., et al. (2006). Mutations in progranulin cause Götzl, J.K., Lang, C.M., et al. (2016). Impaired protein degradation in tau- negative frontotemporal dementia linked to chromosome 17. FTLD and related disorders. Ageing Res Rev 32:122–139. Nature 442:916–919. Guerreiro, R., Wojtas, A., et al. (2013). TREM2 variants in Alzheimer’s Beecham, G.W., Hamilton, K., et al. (2014). Genome-wide association disease. N Engl J Med 368:117–127. meta-analysis of neuropathologic features of Alzheimer’s disease and Guerreiro, R., Escott-Price, V., et al. (2016). Genome-wide analysis of related dementias. PLoS Genet 10:e1004606. genetic correlation in dementia with Lewy bodies, Parkinson’s and Benitez, B.A., Jin, S.C., et al. (2014). Missense variant in TREML2 proAlzheimer’s diseases. Neurobiol Aging 38:214.e7–e10. tects against Alzheimer’s disease. Neurobiol Aging 35:1510.e19–e26. Hernandez, D.G., Reed, X., and Singleton, A.B. (2016). Genetics in Bettens, K., Brouwers, N., et al. (2012). Both common variations and rare Parkinson disease: Mendelian versus non-Mendelian inheritance. J non-synonymous substitutions and small insertion/deletions in CLU Neurochem 139(Supp 1):59–74. are associated with increased Alzheimer risk. Mol Neurodegener 7:3. Höglinger, G.U., Melhem, N.M., et al. (2011). Identification of common Bras, J., Guerreiro, R., et al. (2014). Genetic analysis implicates APOE, variants influencing risk of the tauopathy progressive supranuclear SNCA and suggests lysosomal dysfunction in the etiology of dementia palsy. Nat Genet 43:699–705. with Lewy bodies. Hum Mol Genet 23:6139–6146. Hsiao, K., Baker, H.F., et al. (1989). Linkage of a prion protein missense Cai, G., Atzmon, G., et al. (2012). Evidence against a role for rare variant to Gerstmann-Sträussler syndrome. Nature 338:342–345. ADAM10 mutations in sporadic Alzheimer disease. Neurobiol Aging Huang, K., Marcora, E., et al. (2017). A common haplotype lowers PU.1 33:416–417.e3. expression in myeloid cells and delays onset of Alzheimer’s disease. Nat Collinge, J., Harding, A.E., et al. (1989). Diagnosis of Gerstmann- Neurosci Jun 19: Epub ahead of print. Sträussler syndrome in familial dementia with prion protein gene Hutton, M., Lendon, C.L., et al. (1998). Association of missense and 5’- analysis. Lancet (London, England) 2:15–17. splice-site mutations in tau with the inherited dementia FTDP-17. Collins, L.M., and Williams-Gray, C.H. (2016). The genetic basis of Nature 393:702–705. cognitive impairment and dementia in Parkinson’s disease. Front International Genomics of Alzheimer’s Disease Consortium (IGAP). psychiatry 7:89. (2015). Convergent genetic and expression data implicate immunity Coppola, G., Chinnathambi, S., et al. (2012). Evidence for a role of in Alzheimer’s disease. Alzheimers Dement 11:658–671. the rare p.A152T variant in MAPT in increasing the risk for FTD- Jakobsdottir, J., van der Lee, S. J., et al (2016). Rare functional variant in spectrum and Alzheimer’s diseases. Hum Mol Genet 21:3500–3512. TM2D3 is associated with late-onset Alzheimer’s disease. PLOS Genet Cruchaga, C., Karch, C.M., et al. (2014). Rare coding variants in the 12:e1006327. phospholipase D3 gene confer risk for Alzheimer’s disease. Nature Jin, S.C., Benitez, B.A., et al. (2014). Coding variants in TREM2 increase 505:550–554. risk for Alzheimer’s disease. Hum Mol Genet 23:5838–5846. Cruts, M., Gijselinck, I., et al. (2006). Null mutations in progranulin cause Jin, S.C., Carrasquillo, M.M., et al. (2015). TREM2 is associated with ubiquitin-positive frontotemporal dementia linked to chromosome increased risk for Alzheimer’s disease in African Americans. Mol 17q21. Nature 442:920–924. Neurodegener 10:19. Cukier, H.N., Kunkle, B.W., et al. (2016). ABCA7 frameshift deletion Jones, L., Holmans, P.A., et al. (2010). Genetic evidence implicates the associated with Alzheimer disease in African Americans. Neurol Genet immune system and cholesterol metabolism in the aetiology of 2:e79. Alzheimer’s disease. PLoS One 5:e13950.
• DPress ementia Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford700 University USA - OSO, 2018. 15:41:51.
Jonsson, T., Stefansson, H., et al. (2013). Variant of TREM2 associated with the risk of Alzheimer’s disease. N Engl J Med 368:107–116. Jun, G., Ibrahim-Verbaas, C.A., et al. (2016). A novel Alzheimer disease locus located near the gene encoding tau protein. Mol Psychiatry 21:108–117. Karch, C.M., Cruchaga, C., and Goate, A.M. (2014). Alzheimer’s disease genetics: from the bench to the clinic. Neuron 83:11–26. Keller, M.F., Saad, M., et al. (2012). Using genome-wide complex trait analysis to quantify ‘missing heritability’ in Parkinson’s disease. Hum Mol Genet 21:4996–5009. Keren-Shaul, H., Spinrad, A., et al. (2017). A unique microglia type associated with restricting development of Alzheimer’s disease. Cell 69(7):1276–1290. Kim, M., Suh, J., et al. (2009). Potential late-onset Alzheimer’s disease- associated mutations in the ADAM10 gene attenuate {alpha}-secretase activity. Hum Mol Genet 18:3987–3996. Kobayashi, A., Teruya, K., et al. (2015). The influence of PRNP polymorphisms on human prion disease susceptibility: an update. Acta Neuropathol 130:159–170. Kohli, M.A., Cukier, H.N., et al. (2016). Segregation of a rare TTC3 variant in an extended family with late-onset Alzheimer disease. Neurol Genet 2:e41. Kouri, N., Ross, O.A., et al. (2015). Genome-wide association study of corticobasal degeneration identifies risk variants shared with progressive supranuclear palsy. Nat Commun 6:7247. Labbé, C., Ogaki, K., et al. (2015). Role for the microtubule-associated protein tau variant p.A152T in risk of α-synucleinopathies. Neurology 85:1680–1686. Lambert, J.C., Ibrahim-Verbaas, C.A., et al. (2013). Meta-analysis of 74,046 individuals identifies 11 new susceptibility loci for Alzheimer’s disease. Nat Genet 45:1452–1458. Levy-Lahad, E., Wasco, W., et al. (1995). Candidate gene for the chromosome 1 familial Alzheimer’s disease locus. Science 269:973–977. Lill, C.M., Rengmark, A., et al. (2015). The role of TREM2 R47H as a risk factor for Alzheimer’s disease, frontotemporal lobar degeneration, amyotrophic lateral sclerosis, and Parkinson’s disease. Alzheimers Dement 11:1407–1416. Lloyd, S.E., Mead, S., and Collinge, J. (2013). Genetics of prion diseases. Curr Opin Genet Dev 23:345–351. Lloyd-Evans, E., and Haslett, L.J. (2016). The lysosomal storage disease continuum with ageing-related neurodegenerative disease. Ageing Res Rev 32:104–121. Logue, M.W., Schu, M., et al. (2014). Two rare AKAP9 variants are associated with Alzheimer’s disease in African Americans. Alzheimers Dement 10:609–618.e11. Mackenzie, I.R.A., and Neumann, M. (2016). Molecular neuropathology of frontotemporal dementia: insights into disease mechanisms from postmortem studies. J Neurochem 138 Supp 1:54–70. Manolio, T.A., Collins, F.S., et al. (2009). Finding the missing heritability of complex diseases. Nature 461:747–753. Mead, S., Uphill, J., et al. (2012). Genome-wide association study in multiple human prion diseases suggests genetic risk factors additional to PRNP. Hum Mol Genet 21:1897–1906. Mead, S., Gandhi, S., et al. (2013). A novel prion disease associated with diarrhea and autonomic neuropathy. N Engl J Med 369: 1904–1914. Medori, R., Tritschler, H.J., et al. (1992). Fatal familial insomnia, a prion disease with a mutation at codon 178 of the prion protein gene. N Engl J Med 326:444–449. Miyashita, A., Koike, A., et al. (2013). SORL1 is genetically associated with late-onset Alzheimer’s disease in Japanese, Koreans and Caucasians. PLoS One 8:e58618. Nalls, M.A., Duran, R., et al. (2013). A multicenter study of glucocerebrosidase mutations in dementia with Lewy bodies. JAMA Neurol 70:727–735. Nalls, M.A., Pankratz, N., et al. (2014). Large-scale meta-analysis of genome-wide association data identifies six new risk loci for Parkinson’s disease. Nat Genet 46:989–993.
Nalls, M.A., McLean, C.Y., et al. (2015). Diagnosis of Parkinson’s disease on the basis of clinical and genetic classification: a population-based modelling study. Lancet Neurol 14:1002–1009. Nicolas, G., Charbonnier, C., et al. (2016). SORL1 rare variants: a major risk factor for familial early-onset Alzheimer’s disease. Mol Psychiatry 21:831–836. Owen, F., Poulter, M., et al. (1989). Insertion in prion protein gene in familial Creutzfeldt-Jakob disease. Lancet 1:51–52. Paloneva, J., Manninen, T., et al. (2002). Mutations in two genes encoding different subunits of a receptor signaling complex result in an identical disease phenotype. Am J Hum Genet 71:656–662. Pericak-Vance, M.A., Bebout, J.L., et al. (1991). Linkage studies in familial Alzheimer disease: evidence for chromosome 19 linkage. Am J Hum Genet 48:1034–1050. Pottier, C., Hannequin, D., et al. (2012). High frequency of potentially pathogenic SORL1 mutations in autosomal dominant early-onset Alzheimer disease. Mol Psychiatry 17:875–879. Pottier, C., Bieniek, K.F., et al. (2015). Whole-genome sequencing reveals important role for TBK1 and OPTN mutations in frontotemporal lobar degeneration without motor neuron disease. Acta Neuropathol 130:77–92. Pottier, C., Ravenscroft, T. A., et al. (2016). TYROBP genetic variants in early-onset Alzheimer’s disease. Neurobiol Aging 48:222.e9–222.e15. Raj, T., Rothamel, K., et al. (2014). Polarization of the effects of autoimmune and neurodegenerative risk alleles in leukocytes. Science 344:519–523. Reitz, C., Jun, G., et al. (2013). Variants in the ATP-binding cassette transporter (ABCA7), apolipoprotein E ϵ4,and the risk of late-onset Alzheimer disease in African Americans. JAMA 309:1483–1492. Renton, A.E., Majounie, E., et al. (2011). A hexanucleotide repeat expansion in C9ORF72 is the cause of chromosome 9p21-linked ALS-FTD. Neuron 72:257–268. Ridge, P.G., Hoyt, K.B., et al. (2016). Assessment of the genetic variance of late-onset Alzheimer’s disease. Neurobiol Aging 41:200.e13–e20. Rogaev, E.I., Sherrington, R., et al. (1995). Familial Alzheimer’s disease in kindreds with missense mutations in a gene on chromosome 1 related to the Alzheimer’s disease type 3 gene. Nature 376:775–778. Rogaeva, E., Meng, Y., et al. (2007). The neuronal sortilin-related receptor SORL1 is genetically associated with Alzheimer disease. Nat Genet 39:168–177. Sanchez-Juan, P., Bishop, M.T., et al. (2015). A genome wide association study links glutamate receptor pathway to sporadic Creutzfeldt-Jakob disease risk. PLoS One 10:e0123654. Saunders, A.M., Strittmatter, W.J., et al. (1993). Association of apolipoprotein E allele epsilon 4 with late-onset familial and sporadic Alzheimer’s disease. Neurology 43:1467–1472. Schmitz, M., Dittmar, K., et al. (2016). Hereditary human prion diseases: an update. Mol Neurobiol Jun 20:Epub ahead of print. Scholz, S.W., and Bras, J. (2015). Genetics underlying atypical parkinsonism and related neurodegenerative disorders. Int J Mol Sci 16:24629–24655. Sherrington, R., Rogaev, E.I., et al. (1995). Cloning of a gene bearing missense mutations in early-onset familial Alzheimer’s disease. Nature 375:754–760. Sidransky, E., Nalls, M.A., et al. (2009). Multicenter analysis of glucocerebrosidase mutations in Parkinson’s disease. N Engl J Med 361:1651–1661. Singleton, A., and Hardy, J. (2016). The evolution of genetics: Alzheimer’s and Parkinson’s diseases. Neuron 90:1154–1163. Singleton, A.B., Farrer, M., et al. (2003). alpha-Synuclein locus triplication causes Parkinson’s disease. Science 302:841. Stefansson, H., Helgason, A., et al. (2005). A common inversion under selection in Europeans. Nat Genet 37:129–137. Steinberg, S., Stefansson, H., et al. (2015). Loss-of-function variants in ABCA7 confer risk of Alzheimer’s disease. Nat Genet 47:445–447. Van Deerlin, V.M., Sleiman, P.M.A., et al. (2010). Common variants at 7p21 are associated with frontotemporal lobar degeneration with TDP-43 inclusions. Nat Genet 42:234–239.
GOxford enetics DUSA ementia Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney,51. et al., Universityof Press - OSO, 2018.• 15:41:51.
Vardarajan, B.N., Zhang, Y., et al. (2015a). Coding mutations in SORL1 and Alzheimer disease. Ann Neurol 77:215–227. Vardarajan, B.N., Ghani, M., et al. (2015b). Rare coding mutations identified by sequencing of Alzheimer disease genome-wide association studies loci. Ann Neurol 78:487–498. Verheijen, J., Van den Bossche, T., et al. (2016). A comprehensive study of the genetic impact of rare variants in SORL1 in European early-onset Alzheimer’s disease. Acta Neuropathol 132:213–224. Weishaupt, J.H., Hyman, T., and Dikic, I. (2016). Common molecular pathways in amyotrophic lateral sclerosis and frontotemporal dementia. Trends Mol Med 22:769–783. Wetzel-Smith, M.K., Hunkapiller, J., et al. (2014). A rare mutation in UNC5C predisposes to late-onset Alzheimer’s disease and increases neuronal cell death. Nat Med 20:1452–1457.
Woese, C.R. (2004). A new biology for a new century. Microbiol Mol Biol Rev 68:173–186. Yeh, F.L., Wang, Y., et al. (2016). TREM2 binds to apolipoproteins, including APOE and CLU/APOJ, and thereby facilitates uptake of amyloid-beta by microglia. Neuron 91: 328–40. Zarranz, J.J., Alegre, J., et al. (2004). The new mutation, E46K, of alpha- synuclein causes Parkinson and Lewy body dementia. Ann Neurol 55:164–173. Zhang, B., Gaiteri, C., et al. (2013). Integrated systems approach identifies genetic nodes and networks in late-onset Alzheimer’s disease. Cell 153:707–720.
• DPress ementia Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford702 University USA - OSO, 2018. 15:41:51.
52. NEUROIMAGING AND CEREBROSPINAL FLUID BIOMARKER S OF ALZHEIMER’S DISEASE Brian A. Gordon, Stephanie J.B. Vos, and Anne M. Fagan
INTRODUCTION The neuropathological hallmarks of Alzheimer’s disease (AD) include aggregation of the beta-amyloid (Aβ) peptide into extracellular amyloid plaques and the accumulation of intraneuronal neurofibrillary tangles (NFT), primarily composed of hyperphosphorylated tau protein (Braak and Braak, 1991). Until recently such pathology was observable only at autopsy. As a result, the original diagnostic guidelines for AD were based primarily on a physician’s clinical judgment guided by interviews, cognitive testing, and neurological assessment (McKhann et al., 1984) and could only be rendered when the disease had progressed to the point of significant disability where the criterion was met for dementia. The clinical diagnosis of AD was designated as “probable” until AD pathology was confirmed postmortem. In the ensuing three decades great strides have been made in our understanding of the pathobiology of AD, driven in large part by methodological breakthroughs for measuring AD pathologies in vivo. Reflecting these advancements, updated guidelines for diagnosing AD in both research and clinical settings have been proposed that incorporate new insights and technological innovations to improve diagnosis (McKhann et al., 2011; Dubois et al., 2014). These guidelines overwhelmingly support the incorporation of biomarkers to increase the certainty of a clinical diagnosis and formally recognize AD as a progressive neurodegenerative disease in which pathology begins well before the appearance of clinical symptoms. Thus, AD is now viewed as a continuous disease that is comprised of an asymptomatic, preclinical stage during which there is evidence of pathology prior to any cognitive symptoms, a pre-dementia phase (often denoted as mild cognitive impairment [MCI] due to AD, or prodromal AD) with progressive pathology and initial cognitive disruption, and an end stage during which there is a clinical designation of dementia. The evolving course of the disease can be assessed using in vivo biomarkers while simultaneously utilizing cognitive and neurological assessments to detect the emergence of the deficits in memory and executive function that classically represent AD. The use of fluid and imaging biomarkers has become commonplace in research and certain clinical settings for both diagnostic and prognostic applications. Their usage now extends even further as a selection tool for enrolling
participants into clinical trials testing disease-modifying therapies, as well as endpoints to demonstrate therapeutic efficacy. This chapter will broadly describe the current state of the field for fluid and imaging biomarkers as they relate to AD. A D N E U R O PAT H O L O GY AD is a dynamic disease characterized by multiple pathologies that evolve over the course of decades in specific anatomical and temporal patterns. The rare, early-onset form of autosomal dominant AD (ADAD) caused by mutations in the amyloid precursor protein (APP), presenilin 1 (PSEN1), and presenilin 2 (PSEN2) genes (Bateman et al., 2011), is caused by an overproduction of Aβ species (notably the 42 amino acid form, Aβ42) that leads to increased amyloid plaque formation in the brain. The ε4 allele of apolipoprotein E (APOE) is the strongest genetic risk factor for the more common late- onset form of the disease (Corder et al., 1993) and is involved, among other things, in Aβ trafficking (see Chapter 51 for more detailed review of AD genetics). Increased plaque deposition in late-onset AD (LOAD) is primarily believed to be caused by a reduced clearance of Aβ from the brain. The overwhelming data from genetic studies points to a dysregulation of Aβ metabolism as the initiating, or at least very early, event in the disease cascade leading to AD dementia (Hardy and Higgins, 1992). Amyloid plaques in AD are primarily composed of Aβ42 and can be “diffuse” in form (lacking an identifiable substructure), fibrillar (a central mass and spoke-like extensions), or dense-cored/neuritic (a compact central mass surrounded by an outer shell typically associated with dystrophic neurites) (Dickson and Vickers, 2001). Roughly one-third of cognitively normal older adults have ß-amyloid pathology at autopsy (Morris et al., 1996), and increased Aβ plaque formation can occur decades before the onset of clinical symptoms (Bateman et al., 2012; Jack et al., 2013; Vos et al., 2013). NFTs are believed to be downstream of the initial Aβ plaque formation and emerge later in the course of the disease. Tangles are also observed in the normal aged brain, but their distribution is primarily confined to the medial temporal lobe in normal aging. In AD, the density of tangles observed postmortem strongly correlates with synapse loss and neuronal cell death, which are associated with cognitive impairment (Terry et al.,
7 0 3 USA - OSO, 2018. Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford University Press 15:41:51.
M A R K E R S O F B ETA-A M Y L O I D PAT H O L O GY I N A L Z H E I M E R DISEASE
1991; Giannakopoulos et al., 2003). AD brains also exhibit significant neuroinflammation, although, like neuronal death and dysfunction, this feature is not specific to AD. IDENTIFYING AD BIOMARKER S Optimal biomarkers should be related to specific underlying disease processes, have disease selectivity, be highly reliable, predict future occurrence of disease symptoms in asymptomatic individuals, and be easily integrated into clinical settings. Biomarkers can be used in both a confirmatory manner (e.g., cerebrospinal fluid [CSF] analysis for meningitis) and exclusionary manner (e.g., ruling out a B12 deficiency causing memory impairment). Fluid and imaging biomarkers of AD pathology have been sought to confirm a clinical dementia diagnosis but, critically, also to identify individuals in the prodromal and even preclinical stages when therapeutic interventions may be most effective. AD biomarkers generally measure one of two classes of pathology: beta-amyloid and neuronal injury. The vast majority of AD biomarkers are assessed by CSF assays or neuroimaging scans. CSF is an ideal source of biomarkers, as it is in direct contact with the extracellular space and therefore reflects pathological processes in the brain. CSF is obtained via standard lumbar puncture procedures, and analytes (e.g., proteins, lipids, etc.) are measured by quantitative assays. Common neuroimaging biomarkers include those evaluated by positron emission tomography (PET) and magnetic resonance imaging (MRI). PET uses a radioactive labeled tracer that is designed to bind to a specific molecule in the brain (e.g., aggregated Aβ or tau) or is a labeled molecule that is naturally used by the body (e.g., glucose or O2). MRI uses magnetic fields and pulses of radio frequency energy to generate images of the brain. MRI can be used to make static structural images of the brain as well as functional images that are sensitive to changes in blood flow. CSF and imaging techniques each have their own strengths and weaknesses in terms of quantification, contraindications, risk, availability, and cost that will likely need to be considered when determining clinical feasibility (Table 52.1).
Aβ is naturally produced mostly by platelets and neurons, and its level in the brain is regulated by synaptic activity (Cirrito et al., 2005). Aβ is derived from its precursor protein, APP, through sequential cleavage by two enzyme complexes, β-secretase and γ-secretase. Depending upon the exact point of cleavage by γ-secretase, Aβ can be up to 43 amino acids in length. Aβ can exist as monomeric forms that, at sufficient concentrations, will transform into oligomers that are prone to aggregate further into an insoluble form of amyloid. Compared to the more abundantly produced Aβ38 and Aβ40 peptides, Aβ42 is much more prone to oligomerize and aggregate. C E R E B R O S P I N A L F LU I D Levels of Aβ40 and Aβ42 peptides are measured in the CSF by either immunoassay or mass spectrometry. In a seminal study, CSF from individuals diagnosed with AD were reported to contain lower levels of Aβ42 than controls or individuals with non-AD neurodegenerative diseases (Motter et al., 1995). This reduction (~50%) has been confirmed in scores of subsequent studies and is considered to be the CSF signature of Aβ associated with AD (Olsson et al., 2016) (Table 52.2). This reduction occurs very early in the disease process; it is observed in individuals with MCI who later progress to AD (Shaw et al., 2009), and even in cognitively normal individuals (preclinical) that ultimately develop dementia due to either ADAD (Bateman et al., 2012) or LOAD (Vos et al., 2013). Known to be a risk factor for AD (Corder et al., 1993), the presence of an APOE ε4 allele is associated with lower levels of CSF Aβ42 across the disease spectrum, whereas levels of other forms of Aβ (e.g., Aβ38, Aβ40) are relatively unchanged (Weiner et al., 2013; Fagan et al., 2009). Low levels of CSF Aβ42 are associated with amyloid plaques in autopsy-confirmed cases of AD (Shaw et al., 2009) and amyloid PET in vivo (Fagan et al., 2006).
Table 52.1 STRENGTHS AND WEAKNESSES OF USING CSF VERSUS NEUROIMAGING BIOMARKERS CSF
NEUROIMAGING MRI
PET
Reported values
Quantitative
Qualitative or quantitative
Qualitative or quantitative
Spatial info on brain changes
No
Yes
Yes
Costs
Low
Higher
Higher
Contraindications
Few
More common
More common
Radioactivity
No
No
Yes
Invasiveness
Higher
Low
Low
Side-effects
Post-LP headaches
None
None
Worldwide availability
Intermediate
High
Low
• DPress ementia Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. Charney, et al., Oxford704 University USA - OSO, 2018. 15:41:51.
Table 52.2 OVERVIEW DIAGNOSTIC AND PROGNOSTIC ACCURACY OF WELL-E STABLISHED AND EMERGING CSF AD BIOMARKERS BASED ON A META-A NALYSIS ANALYTE
# OF STUDIES
# OF SUBJECTS
EFFECT SIZE
P VALUE
AD VS. CTL AD
CTL
Aβ42
142
9949
6841
0.561
1 Mb) are observed in four to five times as many instances of ID-related phenotypes than in ASD, although the distinction between syndromic and nonsyndromic forms of ID are not always made, and there could be more CNVs associated with syndromic ID (or ASD). Overall, rare CNVs (seen in roughly 2% of the general population) are observed in 10% of ASD cases and 16% of ID. A more modest, roughly twofold excess of rare CNVs has also been observed in ADHD (Williams et al., 2010, 2012). Thus, emerging data suggest a convincing role for rare, primarily spontaneous, CNVs but to significantly varying degrees. The highest frequency is in ID, then to lesser degrees respectively in ASD plus ID, ASD alone, ADHD, and likely other less deleterious childhood phenotypes. Although it is still early in the use of many genomic analysis techniques (e.g., GWAS, genome sequencing), it seems plausible that these observations represent the relative contribution of extremely rare and de novo variation versus more common, older inherited variation across these phenotypes. Two other important observations, which also likely extend to other variation types, have been made convincingly as sample sizes and studies have grown across many distinct clinical end points. First, the majority of CNVs that have been associated with ASD have independently been demonstrated to confer risk to other, apparently unrelated, phenotypes, such as schizophrenia or epilepsy (Sebat et al., 2009; Pinto et al., 2010, 2014; Perkins et al., 2016). This suggests pointedly that most of these mutations confer risk to a very broad set of phenotypes, rather than a clinically specific one. Second, for most of these CNVs, healthy adult controls are also occasionally seen bearing the mutations. Accordingly, although risk conferred is quite high (approximate odds ratios of 10 to 20), the penetrance for any specific outcome is generally less than 50%. In these two properties, the risk variants discovered in large case-control studies (generally focusing on large, idiopathic population samples of cases) seem distinct from those relevant to the rare Mendelian genomic syndromes. Such syndromes are usually caused by high-penetrance events and have an extremely specific set of comorbidities and features that often make them clinically recognizable in advance of conclusive genetic testing. Related to this, a considerable number of specific, single- gene genetic syndromes have been described that feature unusually high rates of ID or ASD (Betancur, 2011). Although some of these are rare and apparently fully penetrant entities such as Rett syndrome, a severe form of autism most often caused by mutations in one copy of MECP2 or CDKL5
• Petediatric P sychiatric D isorders Charney and Nestler's Neurobiology of Mental Illness, edited by Dennis S. 790 Charney, al., Oxford University Press USA - OSO, 2018. 15:43:54.
on one X chromosome in girls (these mutations are usually lethal prenatally in boys), most have far less than complete penetrance. Noteworthy examples among these in the case of ASD include fragile X and tuberous sclerosis complex (TSC) (Folstein and Piven, 1991), specific and long-identified Mendelian syndromes with high rates of ASD. Similar to the CNVs described previously, however, fewer than 50% of cases manifest ASD. Although many such rare genetic syndromes are now identified, taken in total they likely explain only a small percentage of idiopathic ASD. Figure 58.1 shows the relationship between effect size and frequency for CNVs associated to ASD and the first common variants identified in schizophrenia at genome-wide significance. The CNVs clearly confer much greater risk, but are only present in a small fraction of cases. The common variants are selected from schizophrenia to illustrate the effect sizes of common variants typical of psychiatric phenotypes. As sample sizes continue to increase for GWAS for these traits, further clues are likely to be revealed in the biological basis of these diseases. The massively parallel genome-sequencing technologies that have become available since 2010 have made it possible to sequence the roughly 1% of the human genome that encodes proteins (the exome). ASD is among the first disorders for which this approach has been utilized in substantial numbers of cases; indeed, by genetic sequencing of parents and children, recent studies have documented excesses of de novo loss-of-function mutations in cases when compared with either control individuals (Sanders et al., 2012) or mutational expectations (Neale et al., 2012; O’Roak et al., 2012). Although such studies suggest that only a minority
(