Case Studies in Uncommon Headache Disorders [1 ed.] 9789354650529, 9789352706716
This book discusses on case studies in uncommon headache disorders. Headaches still remain the commonest complaint for w
135 25 8MB
English Pages 241 Year 2019
Polecaj historie


![Case Studies in Communication Sciences and Disorders, Second Edition [1 ed.]
9781630913038, 9781630913021](https://dokumen.pub/img/200x200/case-studies-in-communication-sciences-and-disorders-second-edition-1nbsped-9781630913038-9781630913021.jpg)




![Clinical Case Studies in Home Health Care (Case Studies in Nursing) [1st ed.]
0813811864, 9781118278161, 9780813811864](https://dokumen.pub/img/200x200/clinical-case-studies-in-home-health-care-case-studies-in-nursing-1stnbsped-0813811864-9781118278161-9780813811864.jpg)
![Case Studies in Uncommon Headache Disorders [1 ed.]
9789354650529, 9789352706716](https://dokumen.pub/img/200x200/case-studies-in-uncommon-headache-disorders-1nbsped-9789354650529-9789352706716.jpg)
Citation preview
Case Studies in UNCOMMON HEADACHE DISORDERS
~PRELIMS.indd 1
12/8/2018 11:20:48 AM
~PRELIMS.indd 2
12/8/2018 11:20:48 AM
Case Studies in UNCOMMON HEADACHE DISORDERS
Author Ambar Chakravarty MD FRCP Honorary Professor and Emeritus Consultant in Neurology Vivekananda Institute of Medical Science Kolkata, West Bengal, India
Foreword G Arjundas
JAYPEE BROTHERS MEDICAL PUBLISHERS The Health Sciences Publisher New Delhi | London | Panama
~PRELIMS.indd 3
12/8/2018 11:20:48 AM
Jaypee Brothers Medical Publishers (P) Ltd Headquarters Jaypee Brothers Medical Publishers (P) Ltd 4838/24, Ansari Road, Daryaganj New Delhi 110 002, India Phone: +91-11-43574357 Fax: +91-11-43574314 Email: [email protected] Overseas Offices J.P. Medical Ltd 83 Victoria Street, London SW1H 0HW (UK) Phone: +44 20 3170 8910 Fax: +44 (0)20 3008 6180 Email: [email protected]
Jaypee-Highlights Medical Publishers Inc City of Knowledge, Bld. 235, 2nd Floor, Clayton Panama City, Panama Phone: +1 507-301-0496 Fax: +1 507-301-0499 Email: [email protected]
Jaypee Brothers Medical Publishers (P) Ltd 17/1-B Babar Road, Block-B, Shaymali Mohammadpur, Dhaka-1207 Bangladesh Mobile: +08801912003485 Email: [email protected]
Jaypee Brothers Medical Publishers (P) Ltd Bhotahity, Kathmandu, Nepal Phone: +977-9741283608 Email: [email protected]
Website: www.jaypeebrothers.com Website: www.jaypeedigital.com © 2019, Jaypee Brothers Medical Publishers The views and opinions expressed in this book are solely those of the original contributor(s)/author(s) and do not necessarily represent those of editor(s) of the book. All rights reserved. No part of this publication may be reproduced, stored or transmitted in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, without the prior permission in writing of the publishers. All brand names and product names used in this book are trade names, service marks, trademarks or registered trademarks of their respective owners. The publisher is not associated with any product or vendor mentioned in this book. Medical knowledge and practice change constantly. This book is designed to provide accurate, authoritative information about the subject matter in question. However, readers are advised to check the most current information available on procedures included and check information from the manufacturer of each product to be administered, to verify the recommended dose, formula, method and duration of administration, adverse effects and contraindications. It is the responsibility of the practitioner to take all appropriate safety precautions. Neither the publisher nor the author(s)/editor(s) assume any liability for any injury and/or damage to persons or property arising from or related to use of material in this book. This book is sold on the understanding that the publisher is not engaged in providing professional medical services. If such advice or services are required, the services of a competent medical professional should be sought. Every effort has been made where necessary to contact holders of copyright to obtain permission to reproduce copyright material. If any have been inadvertently overlooked, the publisher will be pleased to make the necessary arrangements at the first opportunity. The CD/DVD-ROM (if any) provided in the sealed envelope with this book is complimentary and free of cost. Not meant for sale. Inquiries for bulk sales may be solicited at: [email protected] Case Studies in Uncommon Headache Disorders / Ambar Chakravarty First Edition: 2019 ISBN: 978-93-5270-671-6
~PRELIMS.indd 4
12/8/2018 11:20:48 AM
Dedication To the memory of Professor Shyamal Kumar Das (1954–2018) a dear friend and a very learned colleague
~PRELIMS.indd 5
12/8/2018 11:20:48 AM
~PRELIMS.indd 6
12/8/2018 11:20:48 AM
Contributors AUTHOR Ambar Chakravarty MD FRCP Honorary Professor and Emeritus Consultant in Neurology Vivekananda Institute of Medical Science Kolkata, West Bengal, India
CO-AUTHORS Angshuman Mukherjee MD DM Professor and Head Department of Neurology Vivekananda Institute of Medical Science Kolkata, West Bengal, India
Debasish Roy MD DM Professor Department of Neurology Vivekananda Institute of Medical Science Kolkata, West Bengal, India
~PRELIMS.indd 7
12/8/2018 11:20:48 AM
~PRELIMS.indd 8
12/8/2018 11:20:48 AM
Foreword Headaches still remain the commonest complaint for which patients seek neurologist advice. The fear of brain lesions is very high and rightly so. And yet the detailed histories and deductions, both from patients and busy neurologists are not intense and quick.
This leads to premature and nonlogical resort to expensive imaging and other tests.
Conditions like chronic daily headaches, primary increased intracranial tension and migraine syndromes can almost be resolved with experience-based algorithms and minimal tests especially for those who are unable to afford expensive tests. Case-based studies by senior neurologists and headache centers will be of great help to younger and less experienced neurologists than didactic reviews and updates to a clinician. Professor Ambar Chakravarty and his colleagues are bringing out this most important volume on this very basis to help enlarge more accurate algorithms in headaches based on case reports of difficult cases of headaches of various etiologies.
It will help all neurologists as a referral book in practice.
It will enable logical choices for investigations and treatments and finally help the patients. Professor G Arjundas Chennai, India
~PRELIMS.indd 9
12/8/2018 11:20:48 AM
~PRELIMS.indd 10
12/8/2018 11:20:48 AM
Preface The present volume is a unique one, the type of which is being published for the first time from India and contributed solely by Indian authors about cases encountered by them in their practice in India. This would be a case-based study being written about 51 uncommon cases of headache disorders, the types of which are not encountered in routine day-to-day practice by most neurologists. In addition, there are 10 commentaries, incorporating most recent information on subjects relevant to the cases discussed. The cases are discussed in a very interactive way with the case history and findings detailed first followed by the investigations performed and the results of therapy, when applicable. This clinical note is followed by a series of questions which are likely to crop up in the minds of the readers after going through the case. The final section is the discussion, embedded in which would lie the answers to all the questions raised, along with other relevant and up to date information on the subject discussed. Not very detailed referencing had been done considering the time constraint for busy medical practitioners and trainees, and only few major ones are listed at the end of each case/ chapter for those interested in more detailed discourses. All cases have been discussed in conformity with the current classification proposed by the International Headache Society in the International Classification of Headache Disorders (ICHD-3 2018) and published in Cephalalgia 2018; 38(1):1-211. This reference will not be repeated again and again in the text. I have no hesitation in admitting that in preparation of this book, I had been influenced by a somewhat similar style adopted by Professor Alan Purdy of Nova Scotia, Canada and his colleagues in their book “Advanced Treatment of Migraine” written quite a few years back and currently not available in the market. I felt this would be the best form of learning for busy practicing clinicians and the trainees. Headache medicine is becoming more and more popular in India and I am confident the present volume would be a source of inspiration for our younger generation to take up this subspeciality to master in. An attempt will be made to distribute this book free of any charge to all members of the Indian Academy of Neurology and to all residents in Neurology in the country to this end. I am grateful to my collaborators Dr Angshuman Mukherjee and Dr Debasish Roy for their part contribution and constructive criticism of my thinking and writing. I must also thank the Publishers for their untiring efforts to bring out the volume in time as desired by me. Lastly, I must pay my tribute and thanks to Professor G Arjundas for kindly writing the Foreword of the book highlighting the very reason for publishing such a volume.
~PRELIMS.indd 11
Ambar Chakravarty
12/8/2018 11:20:48 AM
~PRELIMS.indd 12
12/8/2018 11:20:48 AM
Contents SECTION 1: THE MIGRAINES Commentary 1: Chronology of Acute Migraine Attack
1
CASE 1
A Young Boy with Recurrent Headaches and Visual Loss
8
CASE 2
A Middle-aged Man with Headache, Visual Disturbance and Recurrent Episodes of Confusion and Altered Sensorium
12
Commentary 2: The Genetics of Familial Hemiplegic Migraine
17
CASE 3
A Young Girl with Transient Limb Weakness
21
CASE 4
Can Hemiplegic Migraine Occur without Any Headache?
25
CASE 5
Neurology after an Airplane Flight
29
CASE 6
The Lady Who Fooled the Surgeon!
34
CASE 7
A Middle-aged Lady with Migraine with Aura and Rapidly Progressive Dementia
35
CASE 8
A Case of Headache and Vertigo
41
CASE 9
Another Case of Headache and Vertigo
45
CASE 10
A Devastating Episode in a Football Ground
49
Commentary 3: Migraine, Stroke and Other Related Issues
52
CASE 11
A Young Girl with Migraine Who Lost her Vision
58
CASE 12
A Middle-aged Lady with Recurrent Ophthalmoplegia
60
Commentary 4: Use of Calcitonin Gene-related Peptide Antagonists in Migraine Treatment
65
SECTION 2: MIGRAINE AND EPILEPSY Commentary 5: Migraine and Epilepsy
69
CASE 13
Migraine Epilepsy Interface
80
CASE 14
Another Case of Migraine-Epilepsy Interface
81
CASE 15
More Epilepsy Migraine Interface
83
~PRELIMS.indd 13
12/8/2018 11:20:49 AM
Case Studies in Uncommon Headache Disorders
CASE 16
Yet Another Case of Headache-Epilepsy Interface
84
CASE 17
Yet Another Case of Seizure and Headache
86
SECTION 3: TRIGEMINAL AUTONOMIC CEPHALALGIAS Commentary 6: Clinical Assessment of Patients with Headache and Autonomic Symptoms
87
Commentary 7: Trigeminal Autonomic Cephalalgia: Pathophysiology and Treatment of Intractable Cases
92
CASE 18
An Elderly Man with Intractable Ocular Jabs with a Red Eye and Tearing
101
CASE 19
A Lady with Unilateral Jabs with Tearing from Ipsilateral Eye
109
CASE 20
An Elderly Man with Severe Throat Pain Shooting up to Ipsilateral Eye and Temple with ANS Features including Salivation
113
A Young Girl with Intractable Headache and Severe Photophobia which Changed Pattern over the Years
116
CASE 22
A Young Boy with Side-locked Headache and Restlessness
121
CASE 23
Does Cluster Migraine Exist?
123
CASE 24
A Lady with Side Locked and Time Locked Headache: A Diagnostic and Therapeutic Dilemma
125
Yet Another Case of Hemiplegia with Severe Headache and Autonomic Features
130
CASE 26
Traps in Trigeminal Autonomic Cephalalgias—A Doctor’s Mistake!
133
CASE 27
A Man with an Intractable Abdominal Pain
135
CASE 28
A Lady with Side Shifting Headaches
137
CASE 29
A Young Man with Cluster Headaches, Sleep Disturbance and Sulfa Drug Allergy
138
CASE 21
CASE 25
Commentary 8: TACs and LASH: A Spectrum Disorder
142
SECTION 4: OTHER PRIMARY HEADACHE DISORDERS
xiv
Introduction
144
Commentary 9: Thunderclap Headache
146
CASE 30
Headache in the Shower
152
CASE 31
Another Case of Headache in the Shower
152
CASE 32
Yet Another Case of Headache in the Shower
155
~PRELIMS.indd 14
12/8/2018 11:20:49 AM
Contents
CASE 33
A Middle-aged Lady with Bursting Headache Following Micturition
158
CASE 34
A Pregnant Lady with Headache and Convulsion
159
CASE 35
Alarm Clock Headache that Woke Her Up from Sleep Every Night
164
CASE 36
A Lady Who Had Hemicranial Headache on Coughing
167
SECTION 5: SECONDARY AND OTHER HEADACHE DISORDERS AND CRANIAL NEURALGIAS Commentary 10: Secondary Headaches: An Introduction
171
CASE 37
An Elderly Man with an Intractable Headache
177
CASE 38
An Elderly Man Who Woke Up with a Headache and Visual Loss
178
CASE 39
A Middle-aged Man with Recurrent Fever and Transient Neurological Deficits Who Developed an Iatrogenic Complication
182
CASE 40
A Young Lady with an Intractable Head and Face Pain
188
CASE 41
A Young Girl with an Apparently Serious Illness with Spontaneous Improvement
191
CASE 42
A Middle-aged Lady with Intractable Headache
193
CASE 43
A Middle-aged Man with an Explosion in the Head
195
CASE 44
Another Case of Explosion in the Head
196
CASE 45
A Young Boy with Recurrent Headaches and Falls
198
CASE 46
A Young Lady with Unilateral Eye Pain and Tenderness
203
CASE 47
A Lady with a Linear Burning Sensation on the Face
204
CASE 48
Recurrent Eye/Periorbital Pain and Visual Loss: Could It have been Prevented?
207
An Elderly Man with Facial Twitching and Burning Tongue
208
CASE 49
SECTION 6: TRAPS IN HEADACHE DIAGNOSIS CASE 50
An Elderly Man Who Woke Up with Severe Headache and Visual Loss
213
CASE 51
A Middle-aged Lady with Left Hemicranial Headache and a Red Eye
214
INDEX
217
xv
~PRELIMS.indd 15
12/8/2018 11:20:49 AM
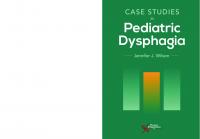
PLATE 1
FIG. 1: Ictal EEG showing right hemispheric epileptiform discharges during a spell of right hemicranial headache (Commentary 5).
A
B
FIG. 1: Transcutaneous electrical stimulation with Cefaly device in progress (Commentary 7).
FIG. 1: Temporal artery biopsy. Hematoxylin and eosin (H&E) stain: shows transmural inflammatory and giant cells infiltration in Case 37 (Commentary 10).
~Plates_.indd 1
12/6/2018 3:08:27 PM
Section 1: The Migraines COMMENTARY 1 Chronology of Acute Migraine Attack
INTRODUCTION The International Headache Society defines migraine as a recurrent primary headache disorder resulting in attacks that last 4–72 hours. Typically, the headache is unilateral, pulsating, moderate or severe in intensity, aggravated by routine physical activity and associated with nausea or photophobia and phonophobia. In the western world approximately one-third of individuals with migraine, some attacks are associated with an aura phase, comprised of visual, sensory and language or brainstem disturbances. Four stages are involved to lead up to the acute attack which is followed by a postdrome.
Preparatory Stage This stage defines subjects who are prone to develop acute migraine attacks because of their genetic constitution which makes their brains hyperexcitable. So when acted upon by an attack provoking stimulus or trigger, a cascade of events ensue leading first to an aura and then the headache.
NEURONAL HYPEREXCITABILITY AND ITS GENETICS Neurophysiological studies have shown that the migraine brain is characterized by general neuronal hyperexcitability. Evoked and event-related potential studies have shown increased excitability in patients with migraine in response to a wide range of stimuli including visual, somatosensory and auditory, as well as brainstem reflexes in response to nociceptive stimuli. Functional imaging studies have also shown that the migraine brain is hyperresponsive to sensory stimuli during the interictal phase. It is thought that this general neuronal hyperexcitability may explain the increased sensitivity to sensory stimuli seen in patients with migraine during the interictal phase. It has also been proposed that this hyperresponsiveness may contribute to the development of central sensitization, since patients with migraine show greater activation in pain-facilitating regions and decreased activation in pain-inhibiting regions at resting state and in response to painful stimuli, compared to healthy controls. Some genetic variations found to be possibly associated with migraine may provide insights into the mechanism(s) for the generalized neuronal hyperexcitability seen in these patients. The most important single gene migrainous disorder is familial hemiplegic migraine, an autosomal dominant disorder which may involve at least three different genetic mutations which all have been characterized and discussed
Commentary_01.indd 1
12/7/2018 3:39:42 PM
SECTION 1: The Migraines
in detail in the next section. The genes identified for FHM all encode for proteins that ultimately modulate the availability of glutamate at synaptic terminals, thus increasing neuronal excitability. Since the identification of the FHM genes, 12 genetic loci have been identified that are associated with increased susceptibility for migraine, with or without aura, three of which increase activity in glutaminergic systems. This leads to increased transmission of pain signals, allodynia and central sensitization. Large genome-wide association studies (GWASs) have identified genetic loci that predict for susceptibility to migraine of various types. Among the identified susceptibility gene variants, some may regulate glutamate neurotransmission (MTDH, LRP1 and MEF2D), while others modulate synaptic functions and plasticity (ASTN2 and FHL5) and ion channels (KCNK5 and TRPM8) as well as ion homeostasis (SLC24A3, near ITPK1 and near GJA1). A new K+ channel gene TRESK has been found to be associated with migraine with aura (MA) occurring in members of a single family only. In a metaanalysis of 22 GWAS, a number of migraine associated single nucleotide polymorphisms were identified that modulate both arterial and smooth muscle function, suggesting that alterations in vascular and smooth muscle function are likely to play a major role in migraine pathogenesis. This is in keeping with the increased risk of vascular disease (ischemic stroke and cardiovascular disease) in migraine, especially with aura. This is also related with the primacy of the central neuronal mechanisms involved in migraine in view of the intimate anatomical and physiological relationship between the blood vessel and neuronal and glial cells within the neurovascular unit.
MIGRAINE CASCADE Premonitory Stage—Hypothalamus, Autonomic Nervous System and Mechanism of Triggering
2
The premonitory phase of migraine can begin as early as 3 days before a migraine headache and allows some patients to correctly predict migraine headache up to 12 hours before its onset. Common symptoms felt during this phase, like fatigue, mood changes, food cravings, yawning, muscle tenderness and photophobia, all point to the involvement of the hypothalamus, brainstem, limbic system and certain cortical areas during the early stages of an attack. Migraine may also display a diurnal periodicity and is commonly triggered by alterations in homeostasis. These findings suggest the involvement of chronobiological mechanisms in migraine pathogenesis and have led to the studies of the hypothalamus as a potential site of origin of the migraine attack. Functional magnetic resonance imaging (fMRI) studies provide evidence of the involvement of the hypothalamus during the premonitory phase. In a positron emission tomography study using cerebral blood flow as a marker of neuronal activity in patients with induced migraine attacks, activations were found in the posterolateral hypothalamus as well as in the midbrain tegmental area, periaqueductal gray, dorsal pons, and various cortical areas during the premonitory phase. A second study used fMRI during the interictal phase (the period between migraine attacks). Imaging revealed stronger functional connections between the hypothalamus and areas of the brain related to pain transmission and autonomic function in patients with migraine compared with non-migrainous controls, which
Commentary_01.indd 2
12/7/2018 3:39:42 PM
COMMENTARY 1: Chronology of Acute Migraine Attack
may account for some of the autonomic symptoms experienced during the interictal and premonitory phases. With evidence pointing toward the involvement of the hypothalamus during the early stage of migraine, it has been postulated that the hypothalamus may play a key role in facilitating or amplifying pain transmission during an attack. The main theories postulated for this mechanism include; increased parasympathetic tone activating meningeal nociceptors and the other involving modulation of nociceptive signals from the trigeminal nucleus complex (TNC) to supratentorial structures involved in pain processing. Many features of migraine, such as nausea, vomiting and thirst and also cranial autonomic symptoms such as lacrimation, nasal congestion and rhinorrhea are indicative of altered autonomic function in the central nervous system (CNS). As such, it has been shown that alterations in sympathetic and parasympathetic tone can be found from the premonitory phase through postdrome. It has been proposed that migraine triggers, such as stress, awakening or other changes in physiological or emotional homeostasis, activate nociceptive pathways through increased parasympathetic tone. Other pathways may also play a role in the provocation of migraine by stress. Sympathetic outflow into the meninges involving norepinephrine release has been shown in experimental models to contribute to pronociceptive signaling through actions on dural afferents and dural fibroblasts. Activation of the kappa-opioid system in response to stress-induced corticotropinreleasing hormone and dynorphin release may also play a role in stress-induced migraine. These physiological mechanisms, involving networks which project to preganglionic parasympathetic neurons in the superior salivary nucleus, may result in peripheral nociceptor activation through the release of neuropeptide transmitters contained within parasympathetic efferents that innervate the meninges and meningeal blood vessels.
Modulation of Nociceptive Signals and Role of Cyclical Brainstem Activity Nociceptive trigeminovascular signals reaching the thalamus may be modulated by the release of excitatory and inhibitory neuropeptides/neurotransmitters from hypothalamic and brainstem neurons. The balance of these neurotransmitters regulates the firing of relay trigeminovascular neurons. If the neurotransmitter is excitatory, it can shift the firing of thalamic trigeminovascular neurons from burst to tonic mode. If the converging inputs from hypothalamic and brainstem neurons are inhibitory, the shift is from tonic to burst mode. The high and low set points for the allostatic load (the amount of physiological or emotional stress that can be managed by the brain) in patients who experience migraine and thus determine whether nociceptive signals are transmitted to the cortex. Whether the premonitory phase passes into the headache phase may also be determined by the current circadian phase of cyclical brainstem activity. If cyclical brainstem activity is high, the threshold is raised for transmission of nociceptive trigeminovascular signals, and nociceptive signals are inhibited. If cyclical brainstem activity is low, the threshold is lowered for the transmission of nociceptive signals and thus a migraine headache may occur. This may in part
Commentary_01.indd 3
3
12/7/2018 3:39:42 PM
SECTION 1: The Migraines
explain why same migraine triggers (both external and internal) do not always cause an attack every time, as this may largely depend on the present state of cyclic brainstem rhythm and on the degree of modulation of trigeminovascular nociceptive signals.
Aura Stage Cortical Spreading Depression Cortical spreading depression (CSD) is thought to be the neurophysiological correlate of migraine and was first described by Aristides Leao in 1944. It is characterized by a slowly (3–5 mm/min) propagating wave of depolarization in neuronal and glial cell membranes that is followed by inhibition of cortical activity for up to 30 minutes, coinciding with the initiation and progression of aura symptoms. This wave of spreading depression is also associated with a wave of hyperemia, followed by a prolonged phase of cortical oligemia. CSD is initiated by local elevations in extracellular potassium (K+) that chronically depolarize neurons for approximately 30–50 seconds. It has been suggested that the initial accumulation of extracellular K+ occurs as a result of repeated depolarization and repolarization of hyperexcitable neurons in the cerebral cortex and that this accumulation of extracellular K+ then further depolarizes the cells from which it was released. This large efflux of K+ is associated with a major disruption of cell membrane ionic gradients, influx of sodium (Na+) and calcium (Ca2+) and release of glutamate. The propagation of CSD is still not fully understood and several hypotheses exist. Originally, the interstitial diffusion of either K+ or glutamate was thought to lead to the propagation of CSD, but later theories suggest that the propagation is mediated via gap junctions between glial cells or neurons. Increasing evidence from animal studies supports the assumption that CSD can activate trigeminal nociception and thus trigger headache mechanisms. The question is does CSD cause the aura symptoms? Probably so. The hypoperfusion of CSD in some way induces both the positive as well as the negative components of the aura. The next question that arises is whether CSD occurs in subjects with migraine without aura (MO). CSD generation is an integral part of the migraine cascade and probably activates meningeal inflammation and trigeminal nociception through release of noxious chemicals. So it must occur in subjects with MO as well. It was suggested earlier that CSD in MO principally occurs in silent or non-eloquent areas of the cortex and hence no aura symptoms are produced. More recent thoughts are that the CSD in MO does not reach the threshold to produce focal neurological features which we call aura. Two other aspects about CSD propagation need to be considered. CSD spread does not follow vascular territory but stops at major sulci. However, it can bypass major sulcus as well by travelling deep into the depths of the sulcus and then coming back on surface travelling up along the cortex on the other side of the deep sulcus. This can explain the development of both motor and sensory symptoms in subjects with hemiplegic migraine where CSD crosses the central sulcus, involving both motor and sensory cortical areas by this mechanism.
4
Commentary_01.indd 4
12/7/2018 3:39:42 PM
COMMENTARY 1: Chronology of Acute Migraine Attack
Phase 3: Headache The characteristic throbbing pain of migraine headache is widely accepted to be the result of trigeminovascular pathway activation. The trigeminovascular pathway is well characterized and its anatomy and physiology explain the distribution of pain seen in migraine.
Trigeminovascular Pathway The trigeminovascular pathway conveys nociceptive information from the meninges to the central areas of the brain and subsequently to the cortex. Nociceptive fibers originating from the trigeminal ganglion innervate the meninges and large cerebral arteries. This nociceptive innervation occurs mainly through the ophthalmic branch of the trigeminal nerve. Afferent projections from the trigeminal ganglion converge with inputs from adjacent skin, pericranial and paraspinal muscle and other C1C2 innervated tissues before synapsing on second-order neurons in the trigeminal cervical complex (TCC), which encompasses the TNC and the dorsal horn of the upper cervical spinal cord (C1-C2). The convergence of afferent projections with neurons from extracranial structures accounts for referred pain perception in the periorbital, occipital and cervical regions. Ascending pathways from the TCC transmit signals to multiple brainstem, thalamic, hypothalamic and basal ganglia nuclei. These nuclei project to multiple cortical areas (cortical pain matrix) including the somatosensory, insular, motor, parietal association, retrosplenial, auditory, visual and olfactory cortices that are involved in processing the cognitive, emotional and sensory-discriminative aspects of the nociceptive signals and give rise to some of the associated symptoms that are characteristic of the attacks and the syndrome, such as photophobia, phonophobia, cognitive dysfunction, osmophobia and allodynia.
Activation of the Trigeminovascular Pathway The activation of migraine pain begins peripherally when nociceptive neurons that innervate the dura mater are stimulated and release vasoactive neuropeptides such as calcitonin gene-related peptide (CGRP) and pituitary adenylate cyclase-activating polypeptide (PCAP), causing signaling along the trigeminovascular pathway— the extent to which arterial vasodilatation, mast cell degranulation and plasma extravasation are involved remains unclear. Some believe that CSD initiates the activation of meningeal nociceptors. Molecules such as ATP, glutamate, K+, hydrogen ions, CGRP, and nitrous oxide that are released locally during a CSD are thought to diffuse toward and activate meningeal nociceptors. Focal stimulation of the rat visual cortex was shown to induce CSD and lead to long-lasting activation of meningeal nociceptors. In addition, this neuronal activation occurred approximately 14 minutes after the induced CSD, consistent with the time delay between onset of aura and onset of migraine headache. It has also been shown in experimental studies, that CSD can lead to ongoing increased activity in central trigeminovascular neurons in the spinal trigeminal nucleus, supporting the theory that CSD results in sequential activation of peripheral and then central trigeminovascular neurons. Preclinical evidence also suggests that CSD may directly activate or disinhibit central trigeminal sensory
Commentary_01.indd 5
5
12/7/2018 3:39:42 PM
SECTION 1: The Migraines
neurons by mechanism intrinsic to the CNS. In these experiments, sensory blockade of the trigeminal ganglion did not disrupt CSD-induced activation of second order trigeminovascular neurons in the TCC. This suggests that CSD does not act to increase central trigeminovascular traffic by a peripheral action alone and that, therefore, the pain of migraine may also arise by a central mechanism. This may explain, e.g. several clinical observations including the development of mechanical allodynia (neck discomfort) prior to the development of headache that occurs in some patients. However, the majority of migraine attacks are not preceded by clinical symptoms of aura; aura may occur after the headache phase has already begun and patients may experience aura but not the subsequent headache. Many patients report migraine symptoms such as nausea, photophobia, phonophobia and headache during the aura phase and some report the headache as starting simultaneously with the aura. It has been suggested therefore, that aura may instead be the result of an aberrant “brain state” that occurs in a genetically susceptible individual during a migraine attack and that physiological events occurring during the premonitory phase (which occurs earlier than aura) may be the primary cause of both trigeminovascular pathway activation and cortical neuronal/glial activity.
Calcitonin Gene-related Peptide Calcitonin gene-related peptide is a 37 amino acid neuropeptide encoded by the calcitonin gene (CALCA) which plays a role in cardiovascular, digestive and sensory functions. CGRP and its receptor are expressed throughout the body, particularly in the central and peripheral nervous systems, the cardiovascular system and the gastrointestinal system. The somatosensory function of CGRP has been implicated in the development of neuronal sensitization and pain generation, most notably in migraine. Considerable evidence points toward CGRP as a key player in migraine pathogenesis—CGRP is a potent vasodilator and is present in afferents innervating meningeal blood vessels. CGRP is also a neurotransmitter that can enhance synaptic transmission mediated by glutamatergic signaling; elevations of CGRP can be detected in jugular venous blood during migraine attacks. Intravenous injection of CGRP triggers migraine in patients with migraine, but not in healthy volunteers. CGRP is thought to act at multiple sites along the trigeminovascular pathway. Peripheral release of CGRP in the meninges causes arterial vasodilatation and may result in sterile inflammation and activation of meningeal nociceptors. CGRP acts indirectly in the periphery to cause plasma extravasation by further increasing substance P release. CGRP acts centrally within the trigeminal ganglion, where it may be involved in signaling between trigeminal ganglion neurons. In addition, CGRP has also been implicated in neuronal-glial cell signaling within the trigeminal ganglion, which may contribute to peripheral sensitization. Release of CGRP in the TCC may facilitate nociceptive transmission by increasing the release of neurotransmitters from adjacent primary afferent terminals.
Peripheral Sensitization 6
Once activated by endogenous mediators, peripheral trigeminovascular neurons become sensitized to dural stimuli, meaning their threshold for response decreases
Commentary_01.indd 6
12/7/2018 3:39:42 PM
COMMENTARY 1: Chronology of Acute Migraine Attack
and the magnitude of their response increases. Peripheral sensitization is likely responsible for the characteristic throbbing pain of migraine and the exacerbation of pain by bending over or coughing. This increased sensitivity to sensory stimulation is thought to be caused by hyperresponsiveness within primary afferent fibers and/ or central neurons. The precise inflammatory mediators that promote activation and sensitization of peripheral trigeminovascular neurons remains to be fully understood. Mast cell degranulation produces long-lasting activation and sensitization of dural nociceptors. Several animal studies implicate CGRP release in the initiation and maintenance of peripheral sensitization. Following repeated CGRP injection into rats’ paws, the response threshold to a noxious mechanical stimulus was significantly lowered as a result of peripheral sensitization.
Central Sensitization Sensitization of central trigeminovascular neurons in the TCC and thalamic nuclei are responsible for cephalic and extracephalic allodynia. Sensitization causes an increase in spontaneous neuronal activity and a heightened response to innocuous cephalic and extracephalic stimuli. Cephalic allodynia, resulting from sensitization in the spinal trigeminal nucleus, includes signs of scalp and cephalic muscle tenderness and an aversion to touch. Thalamic sensitization develops after approximately 2–4 hours and is responsible for extracephalic allodynia. There is evidence that cutaneous allodynia may be a risk factor for migraine progression. It is thought that this may occur through repeated activation and sensitization of the central trigeminovascular pathways and eventually persistent central sensitization. This mechanism may be involved in the genesis of chronic migraine.
Migraine Postdrome Non-headache symptoms may persist for 1–2 days after the headache has resolved in the postdrome or recovery phase. Postdromal symptoms, identified by retrospective recall of typical experiences, include tiredness, impaired concentration and reduced mood. The postdrome, while disabling for many patients, has not been prospectively documented and is not defined in the International Classification of Headache Disorders (ICHD). The persistence of non-headache symptoms throughout all phases of the migraine attack supports the hypothesis of persistent brain changes in the attack. An altered functional state may develop during the premonitory period and persist throughout the headache phase into the postdrome.
CONCLUDING REMARKS Migraine is an inherited neurological disorder characterized by an underlying state of increased responsiveness of cortical and subcortical networks that amplify the intensity of sensory stimuli in genetically susceptible individuals. Some such genetic aberrations have been identified and probably account for the neuronal hyperexcitable state which can be identified by electrophysiological means. This constitutes the preparatory stage. Migraine attacks are evolutive and generally involve a premonitory, headache pain and postdromal phase and in some, reversible visual,
Commentary_01.indd 7
7
12/7/2018 3:39:42 PM
SECTION 1: The Migraines
sensory and language symptoms (aura phase). The premonitory phase appears to involve the hypothalamus and its functional connections to specific brainstem nuclei and cortical regions, whereas migraine headache pain involves increased sensory processing within peripheral and central trigeminovascular pathways. In the present authors opinion, it is unwise to discuss migraine pathophysiology purely as a vascular or neural phenomenon, it is indeed a neurovascular act played on the backdrop of a genetically determined hyperexcitable cerebral cortical state. It is worth noting that one of the key players in this act CGRP is indeed a potent vasodilator. This certainly is going to be the major target for therapeutic intervention in future.
SUGGESTED READING 1. Charles A. The evolution of a migraine attack—a review of recent evidence. Headache. 2013;53(2): 413-9. 2. Dodick DW. A Phase-by-Phase Review of Migraine Pathophysiology. Headache. 2018;58(Suppl 1): 4-16. 3. Goadsby PJ, Holland PR, Martins-Oliveira M, et al. Pathophysiology of Migraine: A Disorder of Sensory Processing. Physiol Rev. 2017;97(2):553-622. 4. Russo A, Silvestro M, Tedeschi G, et al. Physiopathology of Migraine: What Have We Learned from Functional Imaging? Curr Neurol Neurosci Rep. 2017;17(12):95.
CASE 1
A Young Boy with Recurrent Headaches and Visual Loss CASE HISTORY
A 16-year-old boy was seen in 2001 with 15 days history of recurrent blurring of vision in both eyes lasting 10–15 minutes followed by moderately severe holocranial throbbing headache associated with photo and phonophobia and nausea, no vomiting but some unsteadiness in walking. All symptoms would subside in about 3 hours time. He felt very sleepy afterward. He had a total of six attacks at presentation. One attack was witnessed by the resident. His visual acuity was down to perception of light and projection of rays only. Pupils were of normal size and reactive. However he could read looking through a pinhole of 2 mm diameter. His fundi were normal. Tandem walking was abnormal. His routine investigations were normal. Magnetic resonance imaging (MRI) of brain and MR angiography were normal.
QUESTIONS
8
1. 2. 3. 4.
What was the headache diagnosis according to ICHD-3? Why did he have blurring of vision in both eyes and what was the localization? Why he could read through a pinhole? What are the uses of the pinhole test?
Commentary_01.indd 8
12/7/2018 3:39:42 PM
COMMENTARY 1: Chronology of Acute Migraine Attack
5. What are the different types of visual auras encountered in migraine? 6. How does cortical spreading depression (CSD) create visual symptoms? Does CSD occur in both migraine without aura (MO) and with aura (MA)? 7. Is CSD a unilateral or bilateral phenomenon?
DISCUSSION This young boy had half a dozen episodes of holocranial pulsatile headaches associated with photo and phonophobia with nausea. Clearly he had new onset attacks of migraine. All these episodes were preceded by blurring of vision in both eyes and unsteadiness in gait. Clearly he had associated focal anatomically localizable transient neurological phenomena and hence he certainly had MA. On the single episode when he could be examined during an episode, his pupillary reaction and fundi were normal when he had the visual blurring, suggesting that he had transient bilateral occipital cortical dysfunction. Furthermore although his acuity was down to perception of light and projection of rays, he could clearly read through a pinhole. Reading through a pinhole of 2 mm diameter tests the macular, i.e. central vision which localizes in the macular area of the cortex which lies on the lips of the calcarine sulcus in the occipital pole. This is classical of macular sparing due to hypoperfusion or ischemia of the bilateral occipital cortices which are supplied by the two posterior cerebral arteries, terminal branches of the basilar arteries. The macular area, on the other hand is supplied from a posterior branch of the middle cerebral artery. The pinhole test has great utility in ophthalmology. Correction of acuity on reading through a pinhole suggests a defect in the ocular media, e.g. from refractive error. Secondly as already stated, it can test central vision, i.e. macular vision. Thirdly in uniocular diplopia, persistence of diplopia on looking through a pinhole with the other eye closed, suggests either a psychogenic diplopia or a rare parietal lobe disorder called cerebral polyopia. Coming back to the case, in addition to the visual disturbance, the boy had unsteadiness of gait suggesting brainstem-cerebellar dysfunction. In all, preceding his migrainous headache, he had posterior (basilar) circulation hypoperfusion related visual disturbance and ataxia—a possible brainstem– cerebellar dysfunction. Originally described by Bickerstaff in 1961 as Basilar Artery Migraine, the current ICHD-3 terminology for the condition is Migraine with Brain Stem Aura and the “diagnostic criteria” include: “A. Attacks fulfilling criteria for 1.2 migraine with aura and criterion B below B. Aura with both of the following: 1. At least two of the following fully reversible brainstem symptoms: • Dysarthria • Vertigo • Tinnitus • Hypoacusis • Diplopia • Ataxia not attributable to sensory deficit • Decreased level of consciousness (GCS 4 hours and CH lasts for